President Trump has increased immigration enforcement activity to support mass deportation and detention. The administration has shifted enforcement actions from focusing on criminals and recent border crossers to prioritizing all of the estimated 14 million undocumented immigrants for deportation, even though many who have some form of temporary deportation protections. As a result, there has been a significant increase in the number of immigrants detained in Immigration and U.S. Customs Enforcement (ICE) detention facilities, which have a history of inadequate compliance with health and safety standards, insufficient health care, and limited oversight.
The extent to which President Trump will be able to implement interior enforcement policies in the face of potential court challenges remains uncertain. Meanwhile, Congressional Republicans and President Trump passed the tax and spending law in July 2025, which included $191 billion for the Department of Homeland Security (DHS) to support immigration enforcement and expand detention capacity. This brief provides an overview of recent trends in detention using ICE detention data and health care risks and challenges facing those held in detention facilities. These efforts also have broader ramifications for the nation’s workforce and economy given the role immigrants play.
Detention Policies under the Trump Administration
President Trump has identified deportation as a key priority and enhanced interior immigration enforcement efforts since taking office though some policies face legal challenges. President Trump has prioritized all undocumented immigrants for deportation and rescinded numerous Biden-era policies, including a policy that protected against enforcement in “sensitive areas,” such as schools and health care facilities; a ban on collateral arrests, which will allow ICE to pursue arrests without a warrant; and deportation protections for immigrants with humanitarian parole and Temporary Protected Status from numerous countries. The 2025 tax and spending law appropriated $191 billion to DHS to support these actions and increase detention capacity.
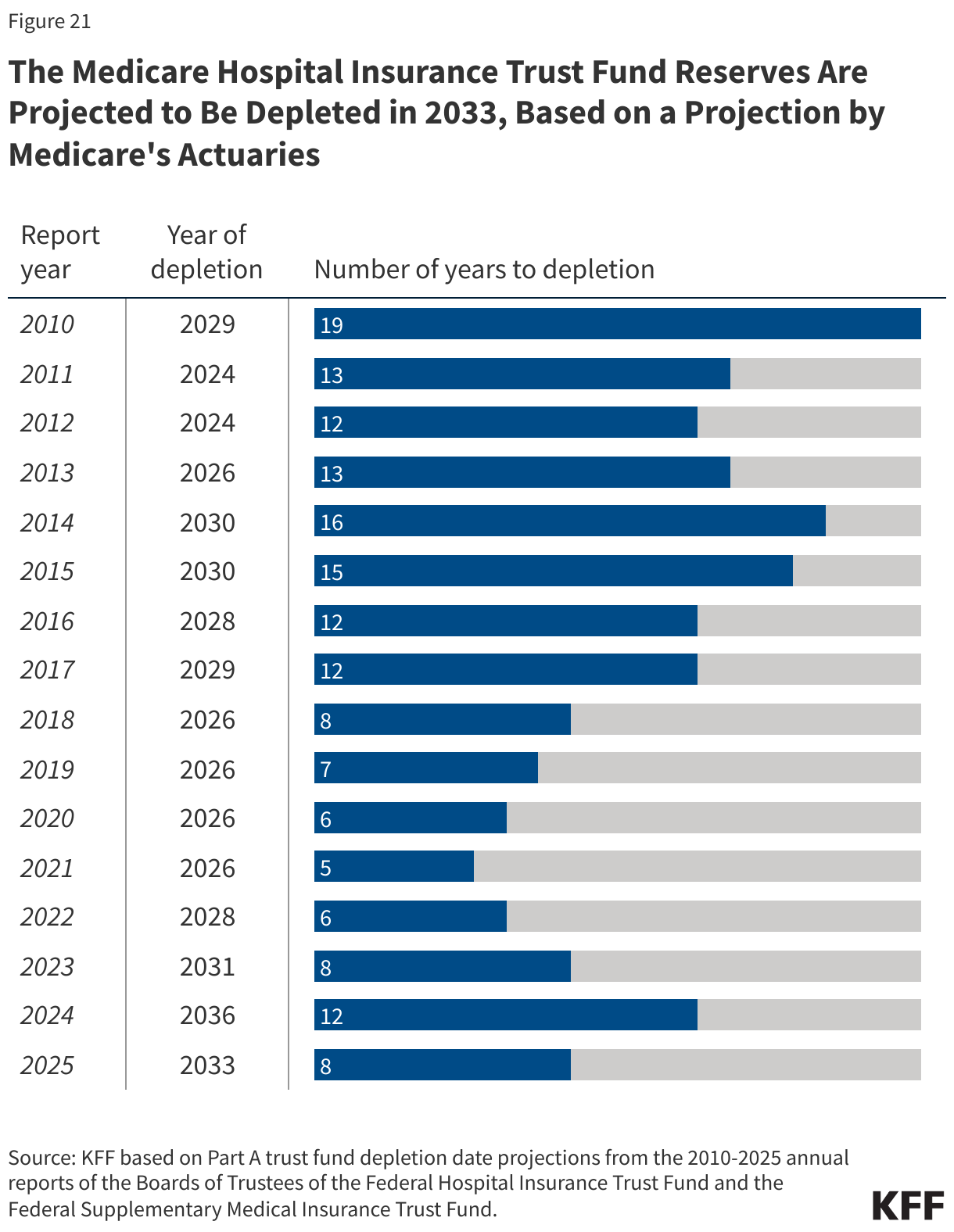
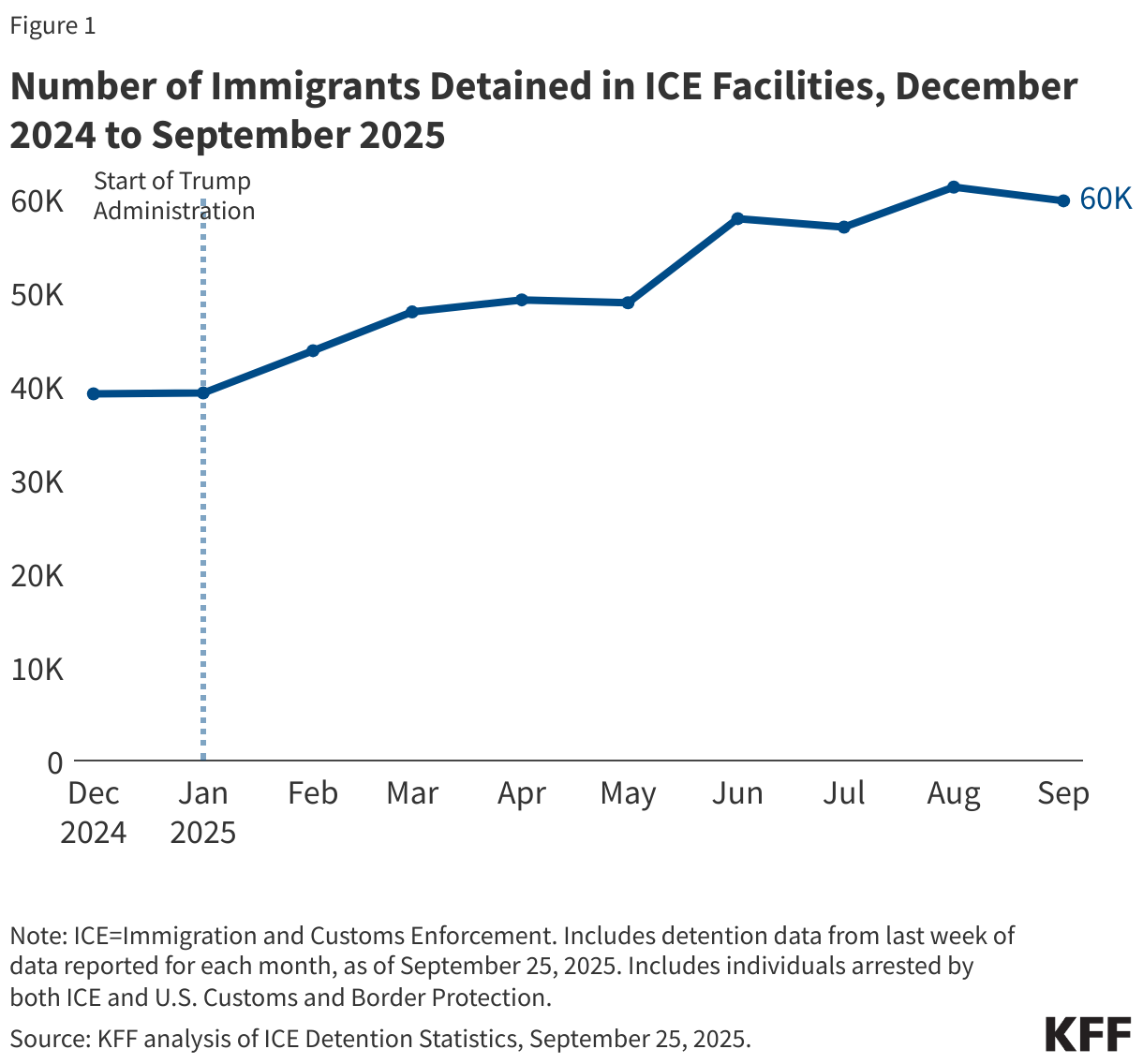
As of September 2025, the Trump administration has nearly 60,000 immigrants held in ICE detention facilities, a 50% increase from 39,000 immigrants held in ICE facilities at the end of the Biden administration in December 2024 (Figure 1). The number of immigrants held in detention increased slightly during the first few months of the year and then saw a sharp uptick in June 2025 due to heightened interior enforcement activity by ICE. ICE detention statistics likely undercount the number of immigrants held in detention due to reporting methodology issues and because they do not include immigrants held by local authorities on detainer requests, where local jails may detain immigrants upon request until they can be transferred to ICE. An analysis of ICE facilities in July 2025 found that many facilities were at or exceeded contractual capacity, which can lead to overcrowding conditions if deportations do not keep up with the pace of arrests. Due to facilities operating at capacity limits, ICE has expanded detaining immigrants in facilities such as hotels and military bases that may be excluded from public reporting. Reflecting the shift to prioritize all undocumented immigrants for deportation, seven in ten (72%) of immigrants in detention facilities have no criminal convictions as of September 2025. The number of immigrants held in detention varies by state, reflecting a combination of where immigrants live, logistics of ICE deportation operations, and the extent to which local laws support coordination with ICE.
Health Care Risks and Challenges for Immigrants in Detention Facilities
ICE is responsible for oversight and management of detention facilities, but it has a history of inadequate compliance with detention standards and insufficient health care, and research shows that immigrants in detention experience widespread health risks. ICE has published health care and safety standards for detention centers, including those that are privately run. As part of its published standards, immigrants arriving at detention facilities must undergo an initial health screening and have access to 24-hour emergency care, daily sick calls, and comprehensive health services including prevention, health education, screening, diagnosis, and treatment. However, ICE provides little to no publicly available data on health care use, quality, and outcomes, and oversight reporting is inconsistent. According to a Congressional Research Service (CRS) report, there is a history of inadequate health care standard compliance in ICE facilities. The Government Accountability Office (GAO) reported on the lack of informed consent for immigrants when receiving offsite medical care, and a DHS report found instances where ICE did not establish medical necessity for surgical procedures, including when performing sterilization procedures on migrant women. Research shows that detainees, including pregnant people and children, can receive inadequate care in detention facilities, and that most detention center deaths were associated with ICE violating their own medical standards. A study on LGBT detainees found they experienced higher rates of harassment than non-LGBT detainees. Immigrants in detention are increasingly being placed in solitary confinement, which can worsen mental health and tends more frequently utilized for those with serious mental illness. The suicide rate also significantly increased from 2010-2020 among immigrants in ICE facilities. Further, a study of immigrants released from detention found significantly higher likelihood of poor or fair self-rated health, mental illness, and PTSD among those detained 6 months or longer compared to those detained less than 6 months. Research also shows that family separation policies while in detention worsened the mental health of both children and caregivers.
The Trump administration has reduced oversight of operations in immigration detention facilities, which may have negative implications for conditions and health risks in detention centers, including for children and families in detention. The Trump administration has shut down watchdog agencies in DHS, including the Immigration Detention Ombudsman office that conducted oversight on conditions at immigration detention centers. Fewer watchdog agencies may further limit transparency and oversight of ICE operations, including on issues such as overcrowding and inadequate medical care. The administration has also attempted to terminate the Flores Settlement Agreement, which set standards for the detention, treatment, and release of immigrant children in federal custody, but federal court recently upheld the settlement. The settlement requires the government to hold minors in the least restrictive settings, prioritize release to family members, and ensure access to basic necessities like food, medical care, and sanitation. Minors may be held with their families in ICE family detention centers, while unaccompanied minors are sent to other facilities when their parents are detained or deported. The tax and spending law approved funds for indefinite family detention, which may be in violation of the Flores Settlement Agreement.
Recent reports suggest immigrants in detention facilities are facing poor and sometimes dangerous conditions for extended periods of time. Some immigrants may be held in holding facilities while they are processed, such as local jails and field offices not designed for long-term detention, and they may not be included in ICE detention statistics. An analysis of ICE detention found that most facilities exceeded contractual capacity, which can lead to overcrowding conditions if deportations do not keep up with the pace of arrests. ICE inspectors found that immigrants held in an unfinished Texas facility still under construction violated many detention standards and failed to properly treat medical conditions. Recent reports have also detailed how immigrants in detention face poor living conditions, including inadequate meals and sanitation, lack of ventilation, and exposure to extreme temperatures. Immigrants held in a Florida detention facility experienced severe overcrowding and a lack of food, and those in Texas and Louisiana experienced extreme cold that the facilities were not equipped to handle. A judge ordered a facility in New York to improve conditions after reports of immigrants being in overcrowded conditions deprived of showers, meals, and bedding. Immigrants held in detention facilities across states reported not receiving adequate meals and foodborne illnesses spreading due to poor hygiene. Families and children in a Texas family detention center reported experiencing extreme temperatures and lacked access to showers or toilets. As of September 2025, 15 immigrants have died in detention, compared to 8 deaths in all of 2024 and the most seen under ICE custody since 2020.
Mass detention efforts may lead to increased fears among immigrant families, which can have negative mental and physical health impacts on immigrants across statuses and their children. As of 2023, 19 million, or one in four, children in the U.S. had an immigrant parent, including one in ten (12%) who are citizen children with a noncitizen parent. An estimated 4.6 million U.S.-born children live with an undocumented immigrant parent. Enforcement efforts have increased worries about detention and deportation among immigrants, including among naturalized citizens, and worsened the mental health and well-being of immigrant families with undocumented immigrants. KFF survey data from March 2025 find that about a third (32%) of immigrants overall say they have experienced negative health repercussions due to worries about their own or a family member’s immigration status. Immigrants also reported they avoided seeking health care due to concerns about costs and fears, were fearful of accessing public programs, and were confused whether these programs can negatively impact immigration status. Research has found that living near areas subject to immigration enforcement raids increased the risk of negative mental health among children of immigrants and worse birth outcomes among both Hispanic immigrant mothers as well as U.S.-born Hispanic mothers as compared to non-Hispanic White mothers. Education outcomes also worsened among Hispanic children in areas impacted by raids compared to White children. Studies have also found that children and caregivers impacted by family separations experience worse mental health, including anxiety, depression, and posttraumatic stress disorder. Family separations can also lead to financial challenges for mixed-status households due to loss of income. Mass detention efforts may also have negative impacts on the nation’s economy and workforce given the outsized role immigrants play in certain industries, including health care. Over 1 million immigrants are estimated to have left the workforce since January 2025.

 Mollyann Brodie
Mollyann Brodie  Liz Hamel
Liz Hamel  Ashley Kirzinger
Ashley Kirzinger  Kaye Pestaina
Kaye Pestaina  Rayna Wallace
Rayna Wallace  Michelle Long
Michelle Long 
 Jared Ortaliza
Jared Ortaliza  Matt McGough
Matt McGough  Cynthia Cox
Cynthia Cox 
 Jennifer Tolbert
Jennifer Tolbert  Clea Bell
Clea Bell  Sammy Cervantes
Sammy Cervantes  Rakesh Singh
Rakesh Singh 
 Emma Wager
Emma Wager  Stephanie Oum
Stephanie Oum  Kellie Moss
Kellie Moss  Jennifer Kates
Jennifer Kates 


 Larry Levitt
Larry Levitt  Juliette Cubanski
Juliette Cubanski  Meredith Freed
Meredith Freed  Nancy Ochieng
Nancy Ochieng  Alex Cottrill
Alex Cottrill  Jeannie Fuglesten Biniek
Jeannie Fuglesten Biniek  Tricia Neuman
Tricia Neuman