Five Things to Know About Medicare Site-Neutral Payment Reforms
Amid rising concerns about health care spending and voters’ worries about health care affordability, there is growing, bipartisan interest in proposals to align Medicare payments for outpatient services across care settings, otherwise known as “site neutral” payments. The goal of this approach would be for Medicare to pay the same rate for the same service, whether it is provided in a hospital outpatient department (HOPD), ambulatory surgical center (ASC), or freestanding physician office, subject to patient safety and quality safeguards. Private payers could also achieve savings if they adopt similar payment policies. Policymakers have been focusing recently on site-neutral payment reform in response to concerns about health care costs and the rapid pace of consolidation, given that the differences in payment across settings for the same service create a financial incentive for hospitals to acquire physician practices.
Site-neutral payment reforms would lower costs by reducing the amount Medicare pays for certain services when conducted in more expensive settings and could also lower costs by reducing incentives for hospitals to buy up physician practices, a pattern which has also been associated with higher commercial prices. Through legislation and rulemaking, Medicare has moved incrementally forward by aligning payments for clinic visits provided at off-campus HOPDs and for all other services provided at off-campus HOPDs that started billing on or after November 2, 2015, with some exceptions. Some policymakers are pressing to broaden the reach of site-neutral payment reforms to include additional settings, such as on-campus HOPDs and off-campus HOPDS that were grandfathered and exempted from certain site-neutral payments under current law. In December 2023, for example, the House of Representatives passed the Lower Costs, More Transparency Act on a bipartisan basis, which would align Medicare payments for drug administration services in off-campus HOPDs, including those exempt under prior reforms.
Opponents, principally in the hospital industry, argue that site-neutral payment reforms would adversely affect patients’ access to services by reducing hospital revenues, raising particular concerns about access for rural and low-income populations. They also suggest that the higher payments for services in hospital outpatient settings are justified by the level of care patients need, the higher costs of providing care in hospitals (e.g., due to regulatory requirements), and the costs of maintaining emergency care and standby capacity.
This issue brief describes five things to know about Medicare site-neutral payment reforms for outpatient services. It does not discuss a related set of proposals to regulate outpatient facility fees charged by hospitals and other institutional providers in commercial markets, such as a bill introduced in the Senate. Those options are intended to achieve similar policy goals but are more complicated, in part, because prices in commercial markets are determined through negotiations between payers and providers rather than being set by the government.
1. Medicare often pays more for the same service when provided in a hospital outpatient department versus other settings
Traditional Medicare generally pays more for outpatient services when provided in HOPDs than in ASCs or freestanding physician offices—which is usually the least-expensive setting. For example, one report estimated that payments for initial preventive exams were 51 percent higher in 2023 when provided in an HOPD than in a freestanding physician office, based on national payment amounts. Another estimated that average reimbursement for drug administration services was 129 to 211 percent higher in HOPDs than in freestanding physician offices in 2021. (Both sets of number exclude HOPDs that are subject to existing site-neutral reforms).
Medicare generally pays the same amount for services provided by HOPDs whether the HOPD is on the main campus of the hospital—i.e., “on-campus”—or off-campus. Off-campus HOPDs often resemble physician offices and may have previously been freestanding physician offices that were acquired by a hospital.
Traditional Medicare Payment System for Outpatient Services by Care Setting*
Hospital outpatient department (HOPD). Under the standard reimbursement approach, Medicare makes one payment to the hospital under the outpatient prospective payment system (OPPS)—sometimes referred to as a “facility fee”—and a separate payment to clinicians using the physician fee schedule (PFS) rate for facility settings. Some hospitals are excluded from the OPPS, such as critical access hospitals (CAHs), which receive cost-based reimbursement.
Ambulatory surgical center (ASC). Medicare generally uses a similar approach to reimburse services provided in ambulatory surgical centers (ASC) as it does for services provided in HOPDs but with a facility fee that is lower than the OPPS rate.
Freestanding physician office. Medicare makes a single payment to the clinician using the physician fee schedule (PFS) rate for nonfacility settings.
*Traditional Medicare uses the same payment system across settings for outpatient therapy services, mammography tests, dialysis services, and clinical lab tests. Provider reimbursement under Medicare Advantage is negotiated between plans and providers, is not public, and may or may not differ from traditional Medicare rates.
Differences in Medicare payments across settings result in higher costs for Medicare and its beneficiaries. Differences in Medicare payments mean that, by definition, program spending is higher than it would have been if the program reimbursed for services based on the least-expensive setting. Higher Medicare spending leads to higher Part B deductibles and cost-sharing amounts in traditional Medicare. For example, MedPAC estimated that aligning Medicare payment rates for a set of outpatient service categories (described below) would have reduced total traditional Medicare Part B spending by $6.0 billion in 2021 and beneficiary cost sharing by $1.5 billion. Higher Part B spending would also contribute to higher premiums for beneficiaries, because Medicare premiums are based on total Part B spending.
Savings for beneficiaries attributable to site-neutral payment reforms would vary, in part, depending on the amount of outpatient services they use and where they receive their care. For instance, one recent study estimated that aligning reimbursement for drug administration services between off-campus HOPDs and freestanding physician services would have reduced cost sharing for traditional Medicare beneficiaries by about $1 on average in 2021 but $1,055 among beneficiaries with the greatest use of chemotherapy who receive care at off-campus HOPDs that are not subject to existing site-neutral reforms (in addition to reducing the standard Part B premium by about $1).
As with Medicare, prices paid by private plans for outpatient services can also vary across care settings. Research from the Blue Cross Blue Shield Association found that average prices paid for a large commercial population were 31% higher for clinic visits in 2022 when provided in an HOPD versus a freestanding physician office, 238% higher for chest x-rays, and 563% higher for prostate biopsies, among other differences. These differences could in part reflect Medicare’s reimbursement system to the extent that commercial payers are benchmarking to Medicare rates.
Higher commercial prices attributable to differences in payments by site of care lead to higher costs for employers, higher premiums and cost sharing for workers and other health plan enrollees, and potentially higher spending or lower revenues for the federal government. A CBO report discussing policies to reduce commercial prices stated that they would “would mainly affect the budget by lowering federal subsidies for health insurance.”
Higher Medicare payments for services provided in HOPDs than in freestanding physician offices create a financial incentive for hospitals to acquire physician practices, which could lead to higher costs. Both the CBO and MedPAC have observed that Medicare’s reimbursement system creates an incentive for hospitals to acquire physician practices. Doing so allows providers to bill Medicare at the higher rates for the same services when provided in an HOPD, leading to higher costs. Some studies provide evidence that differences in payments across settings have led to increases in consolidation of physician practices with hospitals and that consolidation has led to higher spending in Medicare and commercial markets, with unclear effects on quality.
2. While Congress enacted legislation in 2015 to align Medicare payments across settings in certain circumstances, there is interest in adopting additional site-neutral payment reforms
Proponents say that site-neutral payment reforms would reduce Medicare program and beneficiary spending, lead to spillover effects that reduce spending in commercial markets, and further decrease commercial prices by slowing the pace of consolidation. Through legislation and rulemaking, Medicare has aligned payments for clinic visits at off-campus HOPDs as well as for all other services at off-campus HOPDs that started billing on or after November 2, 2015, with some exceptions. More recently, policymakers have expressed some interest in applying these reforms to additional services and settings, based on Congressional hearings and legislation that passed the House of Representatives in 2023.
The Bipartisan Budget Act (BBA) of 2015 introduced site-neutral payment reforms for services provided at relatively new off-campus HOPDs. Under this change, Medicare began to pay for services in some HOPDs at a lower amount more closely aligned with what would be paid in a freestanding physician office. The BBA provisions applied to off-campus HOPDs that started to bill Medicare under the OPPS on or after the date that the law was enacted (November 2, 2015), while grandfathering off-campus HOPDs that existed and billed earlier. The BBA of 2015 and subsequent legislation (the 21st Century Cures Act of 2016) created additional exemptions for off-campus HOPDs, including for those that are dedicated emergency departments, are related to a dedicated cancer hospital, or were under construction when the BBA was enacted. Under current law, exempt off-campus HOPDs are permitted to bill under the OPPS for new services provided, for example, as a result of incorporating additional physician practices.
In 2015, the CBO estimated that the BBA site-neutral payment reforms would save about $9 billion over ten years. CMS implemented this reform by reducing facility fees for affected services to 50% of OPPS rates beginning in 2017 and to 40% beginning in 2018, with the intent of aligning payment in these settings with freestanding physician offices.
In practice, this reform has been relatively modest in scope. According to MedPAC, services provided in non-exempt off-campus HOPDs and paid at lower amounts account for less than one percent of all OPPS spending.
In 2019, CMS extended Medicare’s site-neutral payments to cover clinic visits at all off-campus HOPDs that submit claims to Medicare under the OPPS. This includes all off-campus HOPDs that were exempt under the BBA of 2015. CMS reduced the facility component of reimbursement for clinic visits to 40% of OPPS rates, which it intended to phase in over 2019 and 2020. Implementation was temporarily interrupted when the American Hospital Association (AHA) and others filed a lawsuit against the Department of Health and Human Services, arguing that CMS had exceeded its authority. However, a federal appeals court rejected the industry’s claim in 2020 and the Supreme Court declined to consider an appeal in 2021, which allowed CMS to fully implement the rule. In 2022, CMS announced that rural sole community hospitals would be exempted from this site-neutral payment reform beginning in 2023.
Two-thirds of HOPD clinic visits are provided in on-campus HOPDs and so are not subject to the lower rates.
Given the limited reach of current site-neutral payment policies, MedPAC and others have recommended that Congress implement additional site-neutral reforms for outpatient services. MedPAC’s recommendation is that Congress “more closely align payment rates across ambulatory settings for selected services that are safe and appropriate to provide in all settings and when doing so does not pose a risk to access,” with CMS choosing the services. MedPAC presented one approach that would align HOPD and ASC payment rates with freestanding physician offices for 57 service categories that are most commonly provided in that setting, which the Commission views as an indication that they can be safely provided there. This includes services such as clinic visits, drug administration, and certain imaging services. MedPAC’s approach would also align HOPD payment rates with ASCs for 9 service categories that are most commonly provided in that setting, such as certain types of colonoscopies. The approach would increase aligned payments when related to emergency visits or trauma care. Site-neutral payment reforms have also been endorsed by groups from across the political spectrum— including Families USA, Americans for Prosperity, the Bipartisan Policy Center, and former Secretaries of Health and Human Services (HHS) Kathleen Sebelius and Alex Azar—as well as by the Government Accountability Office and the HHS Office of Inspector General.
In December of 2023, the House of Representatives passed legislation to apply Medicare site-neutral payments to drugs administered in an outpatient setting. The House of Representatives passed the Lower Costs, More Transparency Act (320-71) in December 2023, which would align Medicare payments for drug administration services—such as for chemotherapy—in off-campus HOPDs with rates for freestanding physician offices. Policymakers have considered a variety of other proposals, including proposals to apply site-neutral reforms to cancer diagnosis and treatment services at off-campus HOPDs, all services provided at off-campus HOPDs, or services provided at all HOPDs (off-campus and on-campus) and ASCs when they are most commonly provided in less expensive settings, such as freestanding physician offices (in line with the MedPAC approach). Former President Trump’s 2021 budget proposal included relatively broad site-neutral payment reforms (as described below). President Biden did not include similar proposals in the Administration’s budgets for 2022 through 2025.
Despite bipartisan interest, and a House-passed bill, site-neutral payment reforms were considered but ultimately excluded from a government spending package that was enacted in March 2024. Proponents are pushing for these reforms to be included in a year-end spending package.
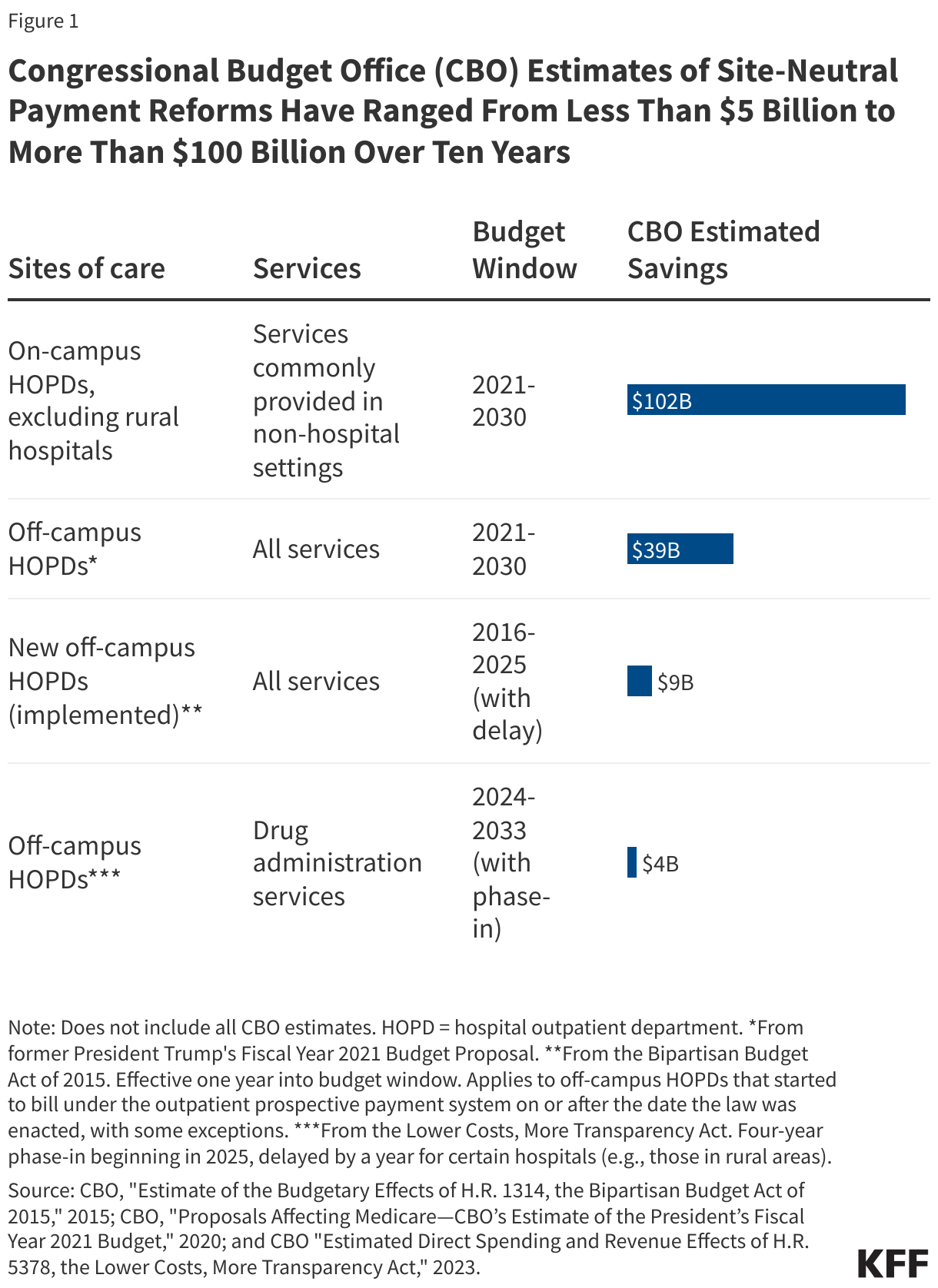
3. Site-neutral payment proposals vary in scope, with CBO estimates of savings ranging from less than $5 billion to more than $100 billion over ten years
Estimated savings from proposed site-neutral payment reforms vary widely (see Figure 1). For example, CBO estimated that the provision in the Lower Costs, More Transparency Act that would align payments for drug administration services in off-campus HOPDs would save $4 billion over ten years. In contrast, in their evaluation of former President Trump’s 2021 budget proposal, CBO estimated that a proposal to extend reforms to all services in off-campus HOPDs would have saved $39 billion over ten years. The Trump budget proposal to align payments for on-campus HOPDs for services commonly provided in non-hospital settings would have saved $102 billion over ten years. Differences in savings to the government would also correspond to varying savings for beneficiaries.
Large differences in expected savings reflect the varying scope of site-neutral payment reforms:
- Which sites of care are covered? Proposals vary based on whether they would apply to off-campus HOPDs alone or all HOPDs. Site-neutral payment reforms for a given set of services could lead to substantially larger savings if they were also applied to on-campus HOPDs. One study estimated that on-campus HOPDs accounted for 87 percent of Medicare’s spending on hospital outpatient services in 2022 and, as noted above, on-campus HOPDs account for two-thirds of clinic visits provided at HOPDs. Another study estimated that aligning payments for the services identified by MedPAC would save Medicare $18 billion over ten years if applied to off-campus HOPDs alone but $127 billion over ten years if on-campus HOPDs were also included.Nonetheless, most reforms have focused on off-campus HOPDs, which may be less controversial given that off-campus HOPDs often resemble physician offices (and may have been freestanding physician offices that were acquired by a hospital). While several options would align rates in HOPDs with freestanding physician offices, some would align rates in HOPDs with ASCs and in ASCs with freestanding physician offices for certain services, resulting in additional savings.
- What services would be covered? Proposals vary in the services that would be covered, which in turn affects the estimated savings. For example, proposals relating to off-campus HOPDs vary in whether they would align payment for cancer diagnosis and treatment, drug administration (estimated by one group to save Medicare $5 billion over ten years), services most commonly provided in less expensive settings as identified by MedPAC (estimated to save $18 billion over ten years), or all services (estimated to save $28 billion over ten years). Recent proposals relating to on-campus HOPDs have focused on services commonly provided outside of hospitals. Proposals also vary in terms of whether they would carve out or augment payments for services related to emergency care or that are provided in dedicated emergency departments.
- Which providers would be given special consideration or exempted? Proposals vary in whether they include provisions to limit or offset the impact on certain providers, such as by excluding rural hospitals, capping losses for hospitals that care for a relatively large number of low-income patients, or targeting new resources to safety-net or rural hospitals.
- Are proposals designed to be budget neutral? Site-neutral payment reforms are often designed to reduce government spending but could be pursued in a budget neutral manner. For example, MedPAC noted that its recommendation to Congress would not have an immediate effect on total OPPS spending due to budget neutrality requirements under current law, which would result in offsetting increases in reimbursement for hospital outpatient services that are not affected by site-neutral reforms. However, policies that are implemented in a budget neutral fashion may nonetheless lower Medicare spending over time by reducing the incentive for hospitals to acquire physician practices.
- Timing. Proposals vary in how quickly they would be implemented and whether they would be phased in over time.
Some site-neutral reform proposals would require that off-campus HOPDs provide a separate, unique identifier from the main campus when submitting claims, which is expected to produce modest savings. This provision would make it easier for private insurers to identify and prohibit facility fees and could improve the accuracy of Medicare payments to off-campus HOPDs. CBO estimated that one version of this proposal would reduce federal spending by about $2 billion over ten years, primarily through its effect on commercial markets.
4. Opponents say site-neutral reforms would adversely affect patient care
Critics of site-neutral payment reforms, primarily hospital industry representatives, have voiced concern about the likely impact on hospital revenues and patient care. Opponents warn that decreases in Medicare reimbursement attributable to site-neutral reforms could lead some hospitals to scale back or eliminate services that they offer in HOPDs or other departments. Just as reforms could lead to savings for the government and patients, they could also lead to decreases in revenues for hospitals. For example, MedPAC estimated that its approach—i.e., aligning payments for services provided in on- and off-campus HOPDs and ASCs that are mostly commonly provided in less-expensive settings—would reduce Medicare revenues among OPPS hospitals by about 3.8% if implemented without budget neutrality requirements. Critics say that the revenue losses would be especially challenging for hospitals in light of financial challenges facing the sector, including higher costs due to labor shortages. Hospital employment now exceeds pre-pandemic levels, and industry reports indicate that finances have been improving, though some hospitals continue to struggle.
Revenue losses would be larger for some hospitals than for others. For example, MedPAC estimated that its approach would lead to relatively large decreases in Medicare revenues for smaller and rural hospitals. Other research has found that off-campus HOPDs—the focus of some reforms—account for a smaller share of total hospital or facility outpatient revenues in rural versus urban areas. Relatedly, according to research supported by the AHA, Medicare beneficiaries treated in HOPDs are more likely than those treated in physician offices to be dual-eligible individuals.
The potential impact of site-neutral payment reforms on rural hospitals has been a sticking point for some Members of Congress amid broader concerns about the financial stability of these facilities. As described below, some have proposed options that are intended to soften the impact on hospital finances and mitigate access concerns. Previous site-neutral payment reforms and many proposals to expand upon these reforms do not apply to Critical Access Hospitals (CAHs)—which are typically in rural areas—because these facilities are reimbursed by Medicare under a separate payment system.
Critics of site-neutral payment reforms say that higher payment rates for outpatient hospital services are justified by higher overhead costs (including those due to stricter regulatory requirements for hospitals) and higher costs associated with maintaining certain essential services, including 24/7 emergency care and standby capacity for public health crises and other emergencies. Proponents counter that rates should not be based on hospital costs but on the costs of providing the service in the least-expensive setting that is safe and appropriate. Some have proposed to refine payments to provide a mechanism to pay for emergency care and standby services, rather than building in the cost of these services through higher reimbursement for outpatient services more generally.
Opponents of site-neutral payment reforms have also suggested that reimbursement should be higher for HOPDs because they care for patients with more complex care needs who are more costly to treat. For example, research supported by the AHA found that Medicare beneficiaries treated in HOPDs are more likely than those treated in physician offices to have a major complication and comorbidity or have had a recent emergency department visit or hospital stay. However, another analysis found that differences in patient severity across HOPDs and physician offices are small. MedPAC has also noted that the services they have focused on typically have low complexity—and may not necessarily cost more to provide for sicker patients—and that hospitals can often bill for additional services under the OPPS if patients need them.
In addition, physician groups and others suggest that Medicare reimbursement rates under the physician fee schedule—i.e., the basis for aligned payment rates—are inadequate. The preponderance of research finds that Medicare beneficiaries do not have problems accessing clinicians, although the AHA argues that hospital acquisitions of physician practices have helped preserve access. Some have raised the option of using savings from site-neutral reforms to increase payment rates for physicians, which could help to mitigate these concerns.
5. Site-neutral payment reforms could be designed to limit or offset the impact on certain providers, such as rural or safety-net hospitals
To address concerns about the effect of site-neutral payment reforms on hospital finances and the implications for access to care and quality, policymakers could include provisions that limit or offset the impact on vulnerable hospitals, such as rural or safety-net hospitals. Options include the following:
- Use savings to fund targeted assistance to vulnerable hospitals. Examples of targeted assistance include increasing reimbursement for rural or safety-net hospitals for services, delaying scheduled cuts to Medicaid Disproportionate Share Hospital (DSH) payments, increasing and improving the targeting of Medicare uncompensated care and DSH payments, extending Medicare payment designations for Medicare Dependent Hospitals and Low-Volume Hospitals, expanding Medicare Critical Access Hospital (CAH) designations to additional facilities, and investing in the rural health care workforce.
- Cap losses for vulnerable hospitals. An alternative approach would limit the reduction in Medicare revenues to a specified percent for any given hospital meeting certain criteria (e.g., that care for a relatively large share of low-income beneficiaries) on a temporary or permanent basis. One tradeoff of this approach is that it would retain some of the incentives under Medicare’s current reimbursement system to acquire physician practices, as the effect of the reform would be eliminated above the cap. One approach for addressing this would be to calculate what the offset would have been prior to implementation and then using that amount as the basis for future offsets (which would therefore not be affected by later acquisitions).
- Exclude certain hospitals altogether. Previous site-neutral payment reforms and many proposals to expand upon these reforms do not apply to CAHs, which accounted for 61 percent of rural hospitals in 2021. Former President Trump’s 2021 budget proposal would have excluded rural hospitals from proposed site-neutral reforms for on-campus HOPDs, without defining how broadly this exemption would be applied. Excluding hospitals would reduce the savings, although extending the policy to on-campus HOPDs produces substantially larger savings than policies that are limited to off-campus HOPDs. One study estimated that off-campus HOPDs affiliated with rural facilities would account for about six percent of traditional Medicare program and beneficiary savings under the Lower Costs, More Transparency Act's site-neutral payment reform. The tradeoff of excluding rural hospitals altogether is that it would necessarily eliminate the potential benefits of site-neutral payment reform for rural areas, such as lower spending for beneficiaries and reduced consolidation.
Key terms
Ambulatory surgical center (ASC). ASCs are distinct health care providers that mostly provide outpatient surgical procedures to patients who do not need to stay overnight.
Critical access hospital (CAH). More than 1,300 hospitals are designated as a CAH by Medicare on the basis of having 25 or fewer beds and meeting other requirements. Medicare reimburses CAHs based on costs, rather than under the inpatient or outpatient prospective payment systems. CAHs are typically in rural areas.
Facility fee. Fees charged by hospitals and other institutional providers that are meant to cover the operational costs of running the facility. These are distinct from professional fees for the care provided by physicians and other health care professionals.
Freestanding physician office. Freestanding physician offices operate independently from a hospital. Services in freestanding physician offices are reimbursed by Medicare using the physician fee schedule (PFS). When a hospital acquires a freestanding physician office, the same services can be billed under Medicare’s reimbursement system for care provided in hospital outpatient departments, which generally results in higher payments. In that scenario, Medicare makes a payment to the clinician under the PFS at a rate that is typically lower than for freestanding physician offices but also makes a separate payment to the hospital under the outpatient prospective payment system (OPPS).
Hospital outpatient department (HOPD). Hospital departments that provide outpatient services, such as clinic visits, injections, and outpatient surgeries. There has been a large increase in Medicare spending on HOPD services over time as care has shifted from inpatient to outpatient settings and as hospitals have acquired physician practices and directly employed more physicians.
Off-campus HOPD. HOPDs that are not part of the hospital campus (i.e., are not physically close to the main hospital buildings). Off-campus HOPDs often resemble physicians’ offices and may have previously been freestanding physician offices that were acquired by a hospital.
On-campus HOPD. HOPDs that are part of the hospital campus (i.e., are part of or physically close to the main hospital buildings).
Outpatient prospective payment system (OPPS). The payment system that Medicare generally uses to cover hospitals’ costs for HOPD services, such as for nursing services, medical supplies, equipment, and rooms. OPPS rates vary geographically and based on the complexity of the service, among other things. Medicare also provides a separate payment to clinicians under the PFS for services provided in an HOPD.
Physician fee schedule (PFS). Medicare’s payment system for physician and other health care professional services. This accounts for clinicians’ labor, practice expenses (such as for rent, equipment, and staff), and malpractice insurance. The PFS includes separate rates for facility and nonfacility settings. The PFS rate for services provided in HOPDs (the rate for facility settings) is typically smaller than for services provided in freestanding physician offices (the rate for nonfacility settings), which reflects the fact that HOPDs cover many expenses otherwise incurred by clinicians in freestanding offices and are reimbursed for these costs under the OPPS.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.