Why Affordability Is the Big Tent

What does the public care about most when it comes to health care? Answer: Out-of- pocket costs followed by, well, out-of-pocket costs. Far down the list after that is everything else: Medicare solvency, value, state Medicaid spending, employer premiums, and down near the bottom is a big one, national health spending. Sure, people are just trying to make ends meet and expressing that to us when we poll. And experts will be quick to tell you that out-of-pocket spending has not changed much as a share of total health spending. But between a quarter and a half of all Americans report real problems paying their medical bills depending on how sick they are. People are not economists, and they don’t think about out-of-pocket costs as a share of spending. People experience them as bills they often can’t afford to pay. The salience of out-of- pocket costs matters for elections, policy, experts, polling and how we in health policy frame the issue to garner public support.
What this means is that affordability is now the theme that will resonate most with voters, whether candidates are talking about health on the campaign trail, or policymakers are advancing policy proposals. That doesn’t mean that other themes like “universal coverage” or health care as a “right” (if you lean liberal), or “choice” or “competition” (if you lean more conservative), don’t work with large segments of the population. But with 92% of the population now covered and so many people struggling with medical bills and medical debt, affordability is the big tent theme that will connect with the most Americans. Here’s more on the data and a few more implications.
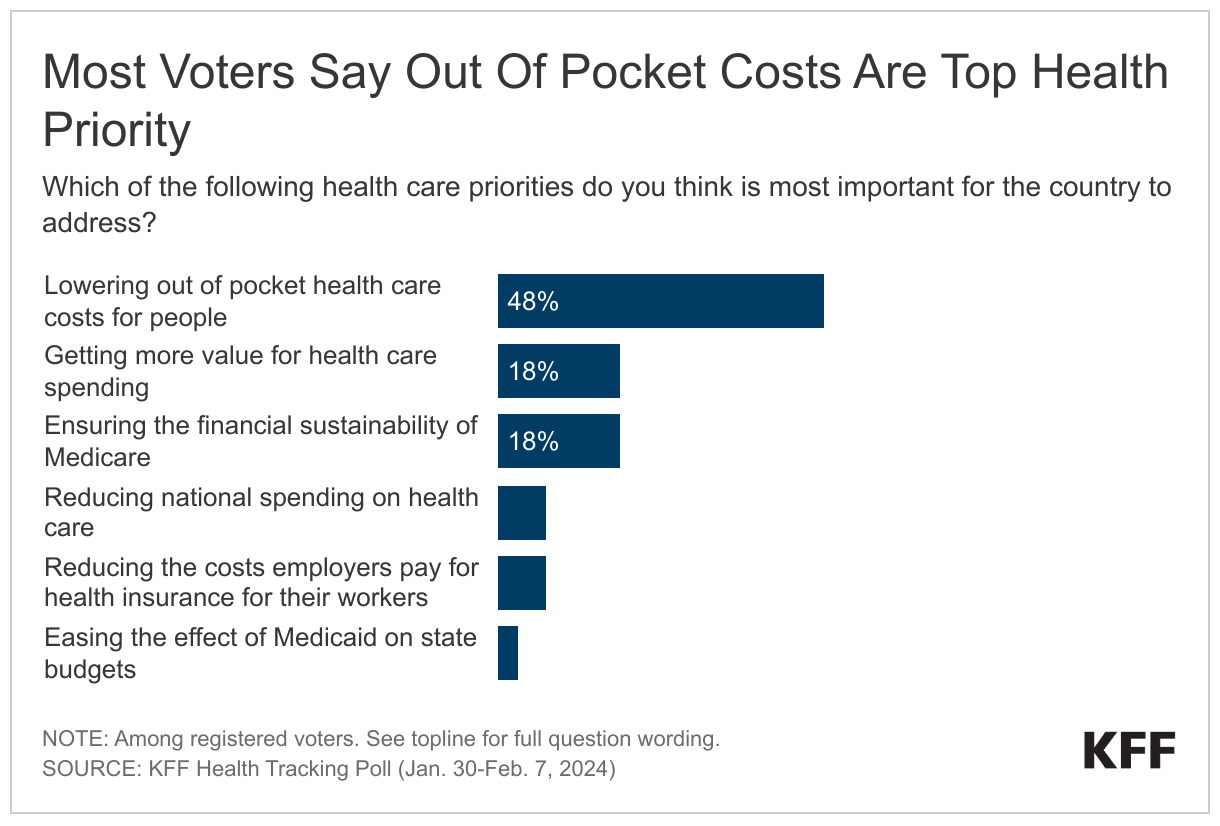
We recently added a polling question to one of our tracking polls to get new data on how the public ranks the various dimensions of the health cost problem, which I wrote about in a recent column. We focused on registered voters since we are in an election year. Far and away the “winner” was “lowering out of pocket costs for people,” picked by 48% of voters, leading reducing national health spending (7%) by a health policy mile. Other prominent concerns, such as keeping Medicare solvent and getting more value for the health care dollar (both 18%), registered with voters but with relatively lackluster impact, while Medicaid spending and employer health costs (surprisingly to me) didn’t make much of an impression. Unlike almost everything we poll about these days, there were no real differences between Republicans and Democrats; to borrow a favorite health care term, concern about out-of-pocket costs is universal.
The fact that people view health care costs as mostly about their own medical bills helps explain another series of findings we see in our polls. Health care is mostly an economic issue to voters; one dimension of their economic concerns. We saw this again in a recent poll that found that, remarkably, “the affordability of health care” just barely trailed “inflation, including the rising cost of household expenses,” as an issue for candidates to talk about. We see it in another way with a different question in a new tracking poll that we’ll release tomorrow, where the cost of health care was right in the mix of reasons people give for rating the economy poorly.
The salience of affordability has implications for the role of health in the election. With no big health reform debate in front of the country, this is not a “health care election.” Abortion is far and away the health care issue most likely to influence voters at the polls in November. Still, it looks like there is untapped potential to appeal to voters who are concerned about the affordability of health care, by talking more about it, and by making proposals that voters may perceive as helping them pay their medical bills. This is true for Democrats who might talk about strengthening the ACA, or doing more on drug costs, or adding vision and hearing benefits to Medicare, or expanding Medicaid to help people afford care. It is also true for Republicans who can trot out their list of policy proposals aimed at costs, such as skinnier health plans, association health plans, health savings accounts, and various transparency proposals they favor. Sometimes policies aimed at affordability can have bipartisan appeal, as did the recent No Surprises Act. Another example is legislation to strengthen transparency rules currently percolating on Capitol Hill.
There are also implications for polling. If you watch John King at CNN or Steve Kornacki at MSNBC display the polls, you will generally see “health” or “health care” ranking pretty far down the issue priority list these days (after all, there is no big national health reform debate to make health care top of mind for voters). They are reporting the polling with complete accuracy. However, if pollsters asked more often “what do you mean by ‘the economy” or “what are your economic concerns?” health care costs would be right up in the mix with inflation and other everyday family economic worries. Drug costs would not be too far behind. It would be clear that what appears separately as “health care” on polls is also a significant dimension of the public’s economic concerns. And if pollsters asked the public to rank “their health care costs” or just “health care costs” as an issue rather than the vague and more general “health” or “health care,” the issue overall would rank higher. Pollsters are doing nothing wrong. Their polls are not health policy polls and they have only so much time and space on most national polls, especially much more limited exit polls. There is, however, more to the story than you get from the polls you see on TV or read online about how the voters think about health and health costs. (That is not to say that this issue or any issue will be decisive in this presidential election cycle, largely a contest between Biden and Trump and not fundamentally about issues.)
Finally, there are implications for the “value” movement. Much of the R&D enterprise now in health services research and health policy focuses on ways to change payment and delivery to get more value for the health spending we do. The primary constituencies for this work are payers, purchasers, and providers, all looking for ways to lower costs and improve quality. However, the polling suggests there is a ways to go before people see “value” as relevant to them. This matters as long as value-based payment remains a central strategy in health care. If consumers do not see these efforts as lowering their costs and improving their care, they will see only high prices and continue to believe no effort is being made to make health care more affordable for them by the institutions that serve them. There are many ways employers or hospital systems or government agencies can approach the challenge of making the value movement more relevant to consumers (spoiler alert: none of them involve marketing “value-based payment” as a concept itself to consumers). How to talk about value and make it more real for people is definitely a subject for another column.
Stay tuned for new KFF polling data that we’ll release tomorrow on people’s cost problems and why health care is an economic issue for voters.
