PEPFAR Reauthorization: Side-by-Side of Legislation Over Time
Overview
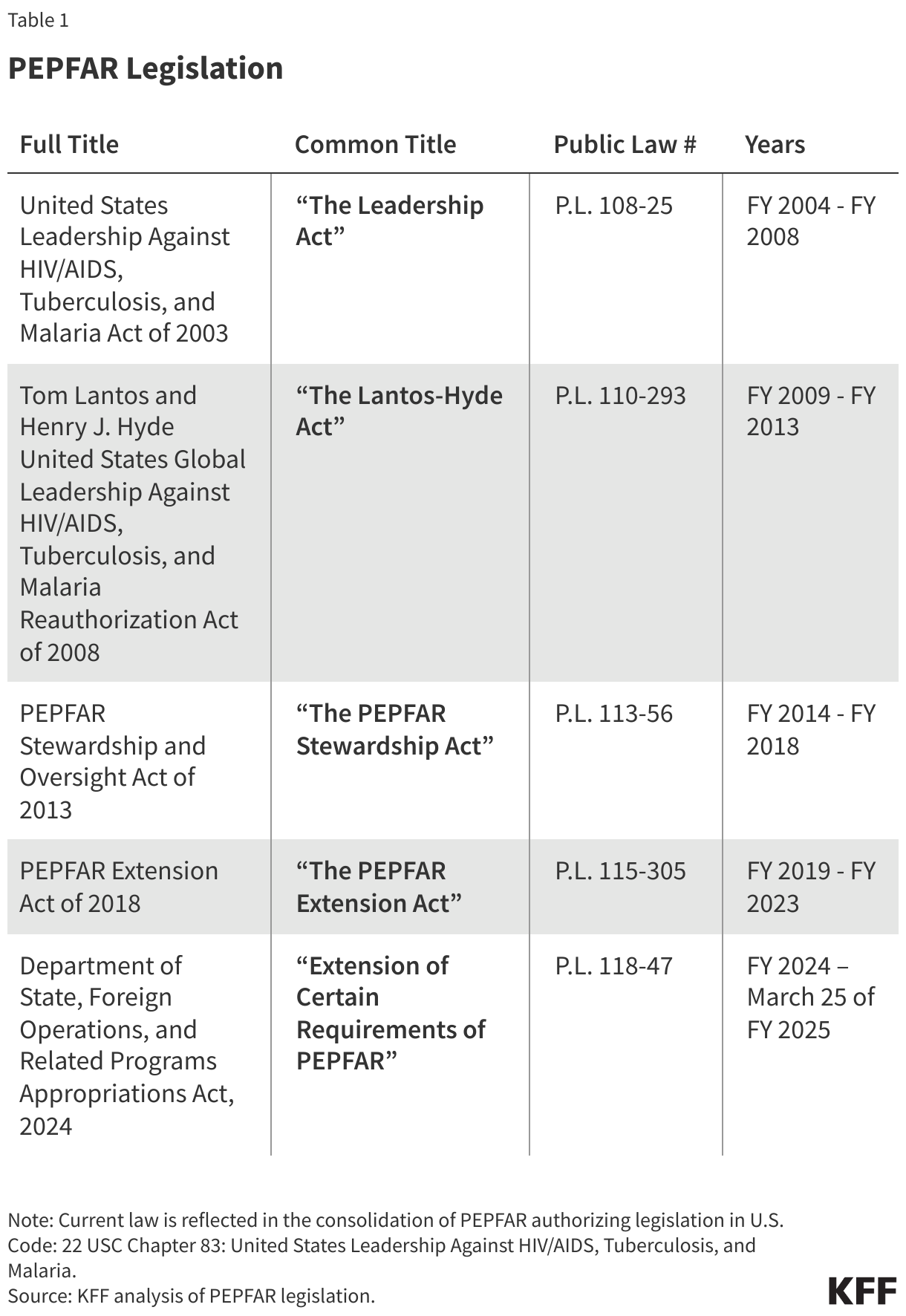
The President’s Emergency Plan for AIDS Relief (PEPFAR) is the U.S. government’s global effort to combat HIV and the largest global health program in the world devoted to a single disease (for more information, see PEPFAR). First proposed by President George W. Bush in 2003, PEPFAR was authorized that same year and has been reauthorized four times since, including its latest – a short-term extension that marks a significant departure from past five-year PEPFAR reauthorizations (see Table 1). PEPFAR’s authorizing legislation governs the U.S. bilateral HIV response, as well as participation in the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) and bilateral assistance for tuberculosis (TB) and malaria programs. These legislative vehicles have permanently authorized most of the program within U.S. law but have also created some time-bound provisions; other than these time-bound provisions, PEPFAR does not need to be reauthorized to continue to operate, as long as Congress appropriates funding for the program. The recent short-term reauthorization extended the program until March 25, 2025, but since its timebound provisions have now lapsed, what happens after this point is uncertain and likely to be affected by the ongoing Trump administration actions related to global health as well as the current complex outlook for PEPFAR. This brief provides a detailed comparison of PEPFAR’s authorizing legislation over time and highlights those authorities that are time-bound (see Tables 2 and 3).
Legislative Changes to PEPFAR Over Time
After first setting the broad parameters for PEPFAR and creating its main structures in 2003, PEPFAR’s subsequent authorizing legislation has made several key changes to the program, as the HIV response has evolved and as PEPFAR has moved from an emergency response to one supporting longer-term sustainability and epidemic control. These include changes to funding authorization levels and spending directives, as well as requirements for reporting and oversight. Among the major changes over time are:
- Funding authorization levels: The Leadership Act authorized $15 billion during PEPFAR’s first five-year period (FY 2004 – FY 2008), which marked a significant increase in funding for HIV by the U.S. government. The Lantos-Hyde Act authorized even more, with $48 billion over the next five-year period (FY 2009 – FY 2013). Subsequent reauthorizations have not included specific authorization of funding amounts.
- Spending directives: Congress has provided several spending directives to PEPFAR through its authorizing legislation, although these have generally been relaxed over time. For example, in the Leadership Act, Congress required that at least 33% of prevention funds be spent on abstinence-until-marriage programs during the FY 2004 – FY 2009 period. This was relaxed in the Lantos-Hyde Act, which removed the 33% directive and replaced it with a requirement of “balanced funding” for prevention, to be accompanied by a report to Congress if less than half of prevention funds were spent on abstinence, delay of sexual debut, monogamy, fidelity, and partner reduction activities in any host country with a generalized epidemic.
- Reporting, monitoring, and transparency: Each of the authorizing bills has included reporting requirements to provide Congress and others with data and information about the program and to support oversight and evaluation. For example, the Leadership Act and the Lantos-Hyde Act required the Institute of Medicine to conduct evaluations of PEPFAR; however, this has not been included in subsequent reauthorizations. On the other hand, all authorizations have required the Inspectors General of several U.S. agencies (the Department of State, the Department of Health and Human Services, and the U.S. Agency for International Development) to jointly develop coordinated annual plans for overseeing U.S. government global HIV, TB, and malaria programs.
It is important to note that Congress has also made changes to PEPFAR through other legislative vehicles. For example, Congress has used appropriations legislation in certain years to change the amount of withholding required from the annual U.S. contribution to the Global Fund, pending certification of certain benchmarks by the Secretary of State. Still, by the time of the Stewardship Act in 2013, a decade after PEPFAR’s creation, most changes have been relatively minor, focused on adding new or refining existing reporting requirements.
Permanent and Time-Bound Authorities
PEPFAR operates largely under permanent authorities of U.S. law that allow for ongoing funding and the continuation of the major structures of the program, such as the Office of the Global AIDS Coordinator at the Department of State (now within the Bureau of Global Health Security and Diplomacy) as well as the position of Global AIDS Coordinator, U.S. participation in the Global Fund, and annual reporting on PEPFAR efforts. Absent a reauthorization, the PEPFAR program would continue, provided funds are appropriated. At the same time, a subset of PEPFAR’s congressionally-mandated requirements are time-bound and are currently lapsed, having been extended through only March 25, 2025 (approximately midway through FY 2025). Of these, two relate to how HIV funding is allocated, four specify requirements related to the U.S. contribution to the Global Fund, and two address reporting or oversight (see Table 2).

Detailed Comparison
Table 3 provides a detailed comparison of PEPFAR’s authorizing legislation over time, by key topic. Time-bound provisions are specified. The recent short-term reauthorization’s extension of these provisions is reflected in The PEPFAR Extension Act column.
