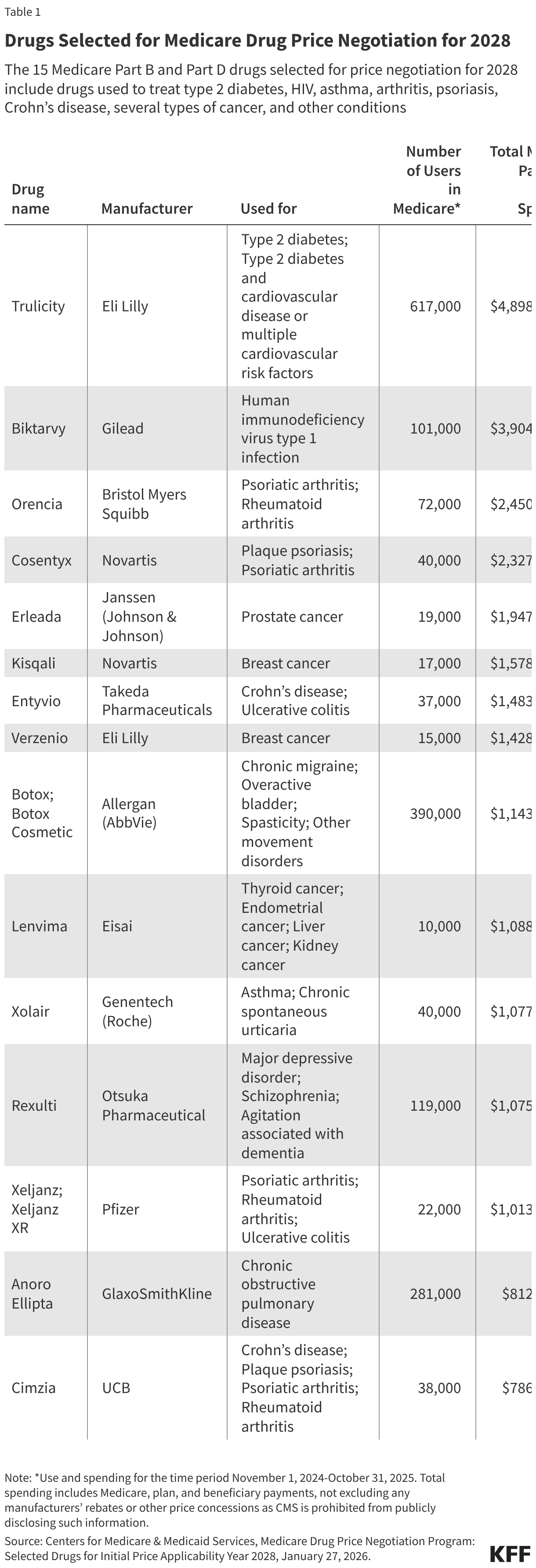
Fifteen drugs covered under Medicare Part B, which covers physician-administered drugs, or Medicare Part D, Medicare’s outpatient prescription drug benefit program, were selected for price negotiation in 2026, with Medicare’s negotiated prices for these drugs taking effect on January 1, 2028 (Table 1). These 15 drugs include treatments for type 2 diabetes, HIV, asthma, arthritis, psoriasis, Crohn’s disease, several types of cancer, and other conditions (See Table 1). Total gross Medicare spending on these 15 drugs between November 2024 and October 2025 was $27 billion, with 1.8 million Medicare beneficiaries using these medications during that time. Starting in 2027 and in each subsequent year, up to 20 additional drugs covered under Part B or Part D will be selected for negotiation. The number of drugs with negotiated prices available will accumulate over time.