How Medicare’s New Drug Price Negotiation Program Could Expand Access to Selected Drugs
Medicare recently announced the first 10 Part D drugs selected for negotiation under Medicare’s new drug price negotiation program. These drugs were identified as the 10 top spending drugs covered under Medicare Part D without generic or biosimilar equivalents that have been on the market for at least seven years and also meet other selection criteria. The 10 drugs selected for the first round of negotiations include treatments for several medical conditions, including diabetes (Farxiga, Fiasp/NovoLog, Januvia, Jardiance), blood clots (Eliquis, Xarelto), heart failure (Entresto, Farxiga), psoriasis (Stelara, Enbrel), rheumatoid arthritis (Enbrel), Crohn’s disease (Stelara), and blood cancers (Imbruvica) (Appendix Table 1). Between June 2022 and May 2023, 8.3 million Medicare Part D enrollees used one or more of these medications. Negotiated prices for these 10 drugs will be available on January 1, 2026.
Much of the discussion around Medicare’s new drug price negotiation program has been about the details of the negotiation process, whether or not it will impact future drug development, and the several lawsuits that have been filed by drug manufacturers seeking to block its implementation. But scant attention has been paid to the ways in which the new negotiation program could affect access to and utilization of selected drugs for Medicare Part D enrollees:
- The law requires all Medicare Part D plans to cover each of the selected drugs, including all dosages and forms, when negotiated prices take effect in 2026.
- The Centers for Medicare & Medicaid Services (CMS) will require Part D plans to justify formulary placement of selected drugs on non-preferred tiers, where cost sharing is typically higher than for preferred tiers.
- CMS will scrutinize plans’ use of utilization management tools, such as prior authorization requirements, applied to selected drugs, which could remove administrative barriers to accessing these medications.
- Along with improved access, Part D enrollees could see lower out-of-pocket costs due to lower negotiated prices, particularly for drugs with coinsurance requirements, which could increase utilization.
This brief examines how Part D enrollees’ access to and utilization of the first set of 10 selected drugs could be affected by the new Part D coverage and formulary requirements for selected drugs established by the Inflation Reduction Act and in CMS guidance, as well as the potential for lower out-of-pocket costs, based on analysis of current (2023) Part D formulary coverage, tier placement, and utilization management requirements for these 10 drugs.
The Inflation Reduction Act requires Part D plans to cover all selected drugs, including all dosages and forms, when negotiated prices are in effect
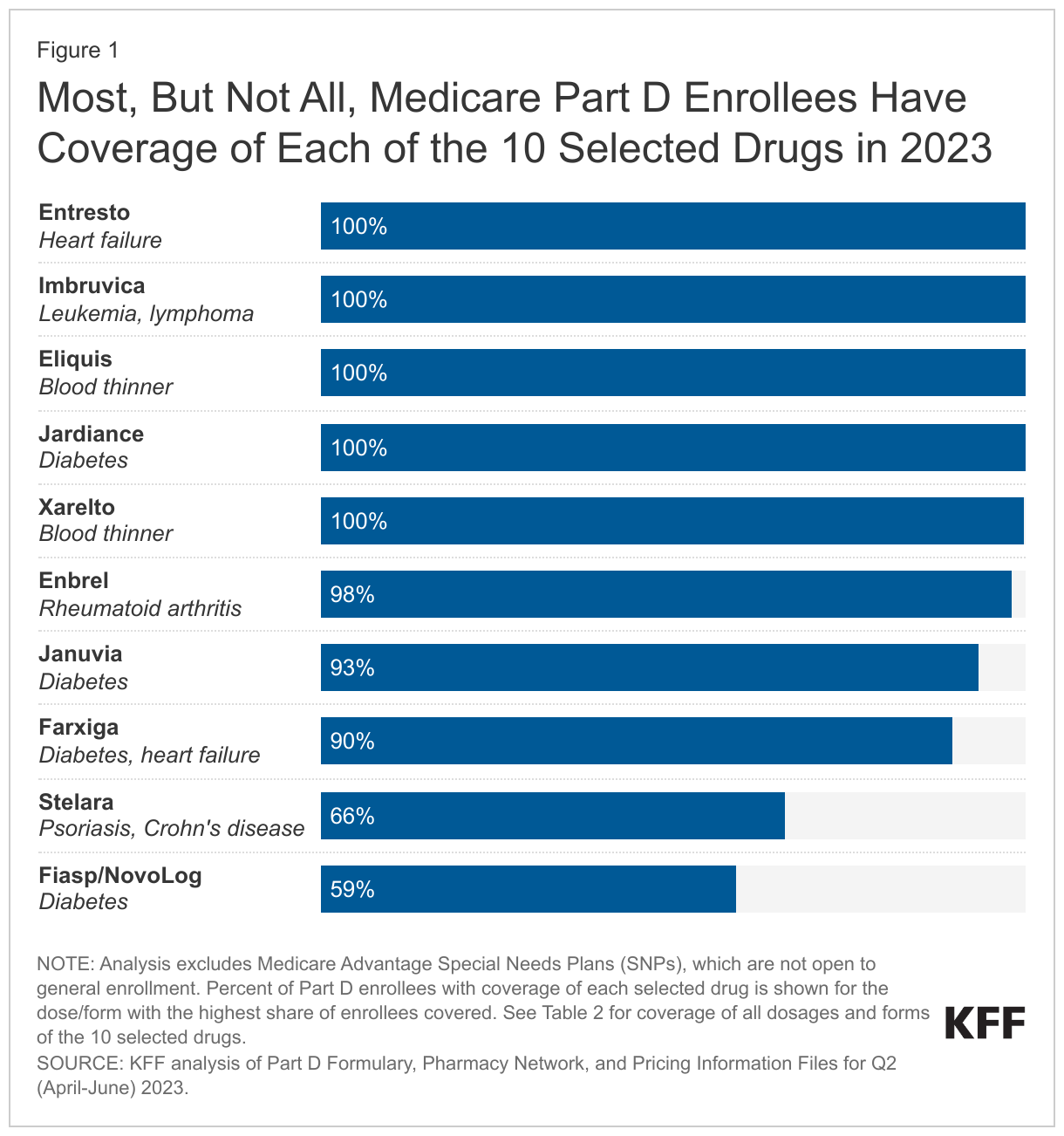
Not all Medicare Part D enrollees have coverage of each of the 10 selected drugs in 2023. The statutory coverage requirement will have the effect of improving access to the selected drugs that are not currently universally covered, in particular the insulin product Fiasp/NovoLog and the psoriasis drug Stelara. The share of Part D enrollees with coverage of any form of these 10 drugs ranges from less than 60% for Fiasp/NovoLog and 66% for Stelara to 100% for Eliquis, Entresto, Imbruvica, Jardiance, and Xarelto (Figure 1). (Imbruvica is an antineoplastic, a type of medication used to treat cancer, which is one of six so-called protected classes where all or substantially all drugs are required to be covered by all Part D plans.)
For Part D enrollees with coverage of the selected drugs in 2023, plans generally cover all or nearly all dosages and forms, but there is a small amount of variation in coverage for seven of the 10 selected drugs. For example, the blood thinner Xarelto is covered in tablet form for virtually all Part D enrollees, but the share of enrollees with coverage of the oral suspension falls to 78%. For the cancer drug Imbruvica, all enrollees have coverage of the 140mg oral capsule but that share drops to 77% for the 280mg oral tablet (Appendix Table 2).
CMS will require Part D plans to justify formulary placement of selected drugs on non-preferred tiers
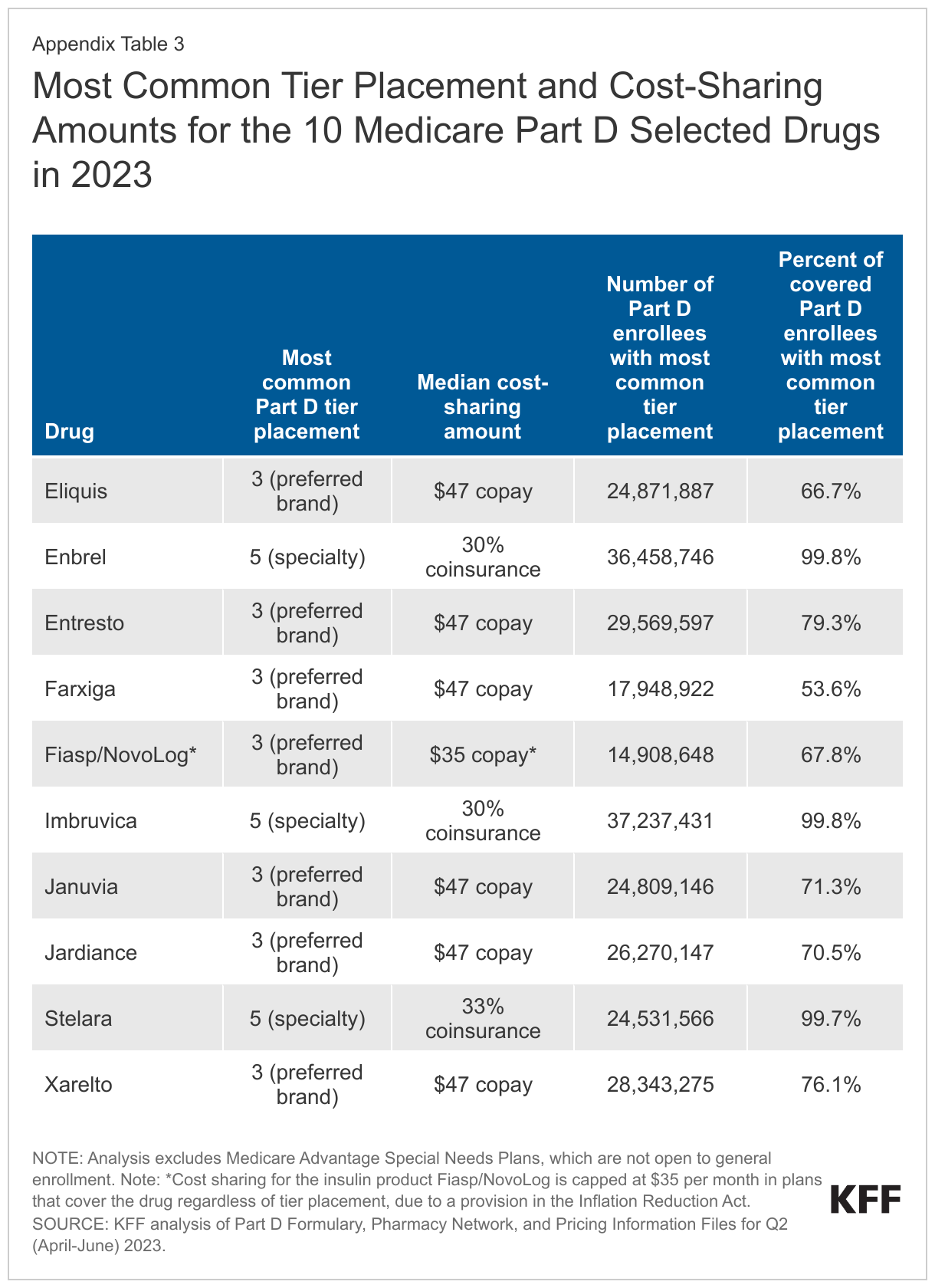
As of 2023, placement of the 10 selected drugs on non-preferred tiers is not common (although whether CMS will consider the specialty tier a non-preferred tier for this purpose is unknown); if coverage of selected drugs shifts to preferred tiers, that could lower Part D enrollees’ out-of-pocket costs. In 2023, three of the 10 selected drugs – the rheumatoid arthritis drug Enbrel, the cancer drug Imbruvica, and the psoriasis drug Stelara – are placed on the specialty tier in virtually all Part D plans that cover these drugs, with median coinsurance of 30-33% in the initial coverage phase (Figure 2, Appendix Table 3). This coinsurance rate is applied to the price of each drug to determine an enrollee’s monthly out-of-pocket cost. Currently, list prices, which do not take into account manufacturer rebates or other price concessions, are generally used in determining patient out-of-pocket costs for drugs with coinsurance. This means that a lower negotiated price would result in lower out-of-pocket costs for selected drugs with coinsurance requirements. In turn, lower out-of-pocket costs could lead to higher utilization of selected drugs.
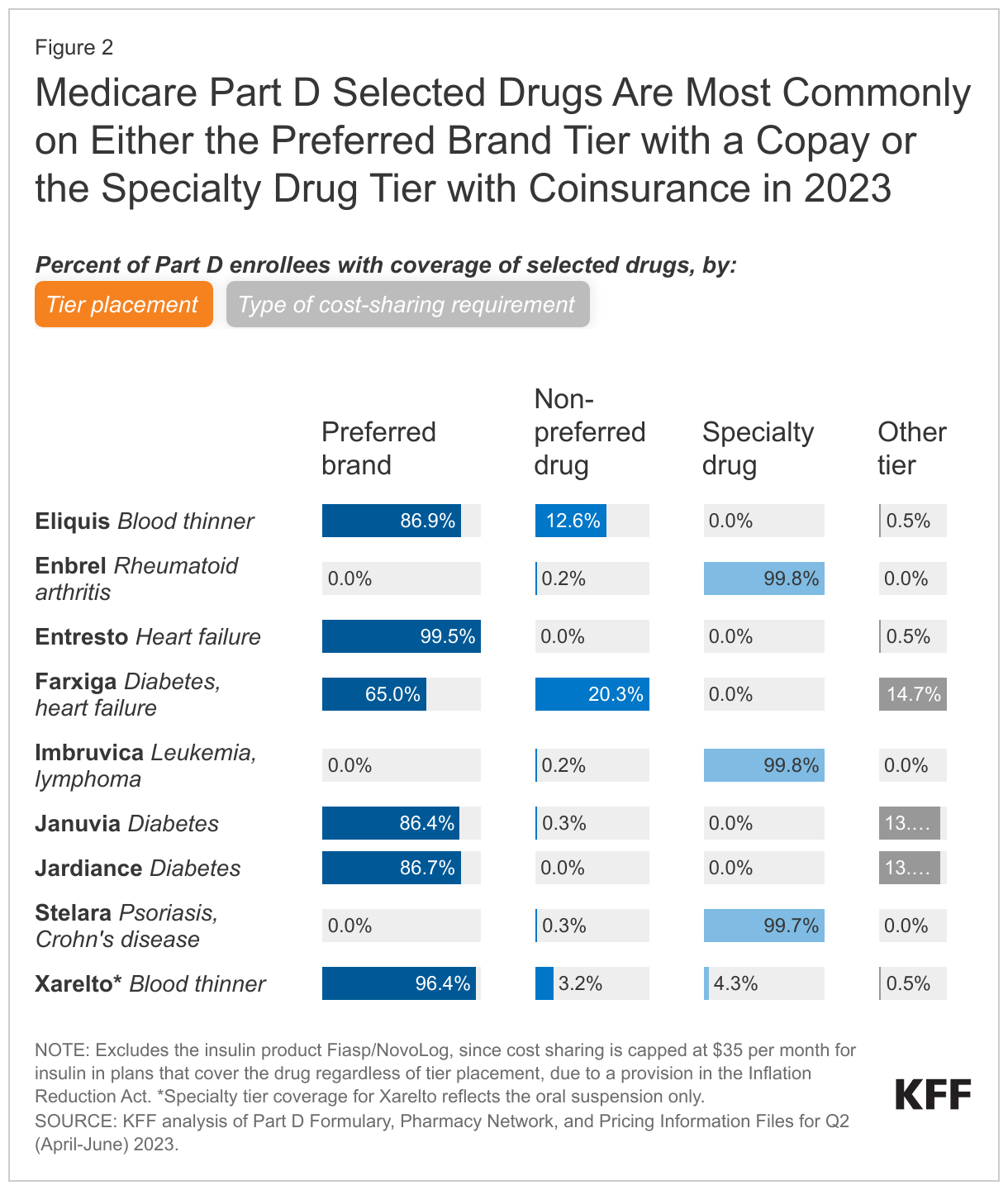
Six of the 10 selected drugs (Entresto, Eliquis, Farxiga, Januvia, Jardiance, and Xarelto) are more commonly placed on a preferred brand tier in 2023, with a median copayment of $47 per month – an out-of-pocket amount that is fixed rather than being a percentage of the drug’s list price (Figure 2, Appendix Table 3).
But some Part D enrollees with coverage of these six drugs in 2023 have coverage on a non-preferred tier, where cost sharing is higher than for drugs on preferred tiers, and enrollees may face coinsurance of up to 50% rather than fixed copayments. For example, roughly 13% of Part D enrollees whose plans cover the blood thinner Eliquis have coverage on a non-preferred tier and face coinsurance of 50% (9.5% of enrollees) or a monthly copayment of $100 (3% of enrollees). If coverage of these drugs shifts to preferred tiers, that could lower Part D enrollees’ out-of-pocket costs.
For the insulin product Fiasp/NovoLog, the most common tier placement in 2023 is on a preferred brand tier, but regardless of tier placement, monthly cost sharing is capped at $35 in plans that cover this product. This is due to a provision of the Inflation Reduction Act, where, starting in 2023, Part D plans are not allowed to charge a copayment of more than $35 per month for covered insulin products.
CMS expects Part D plans to provide justification if more restrictive utilization management is applied to selected drugs relative to non-selected drugs in the same class
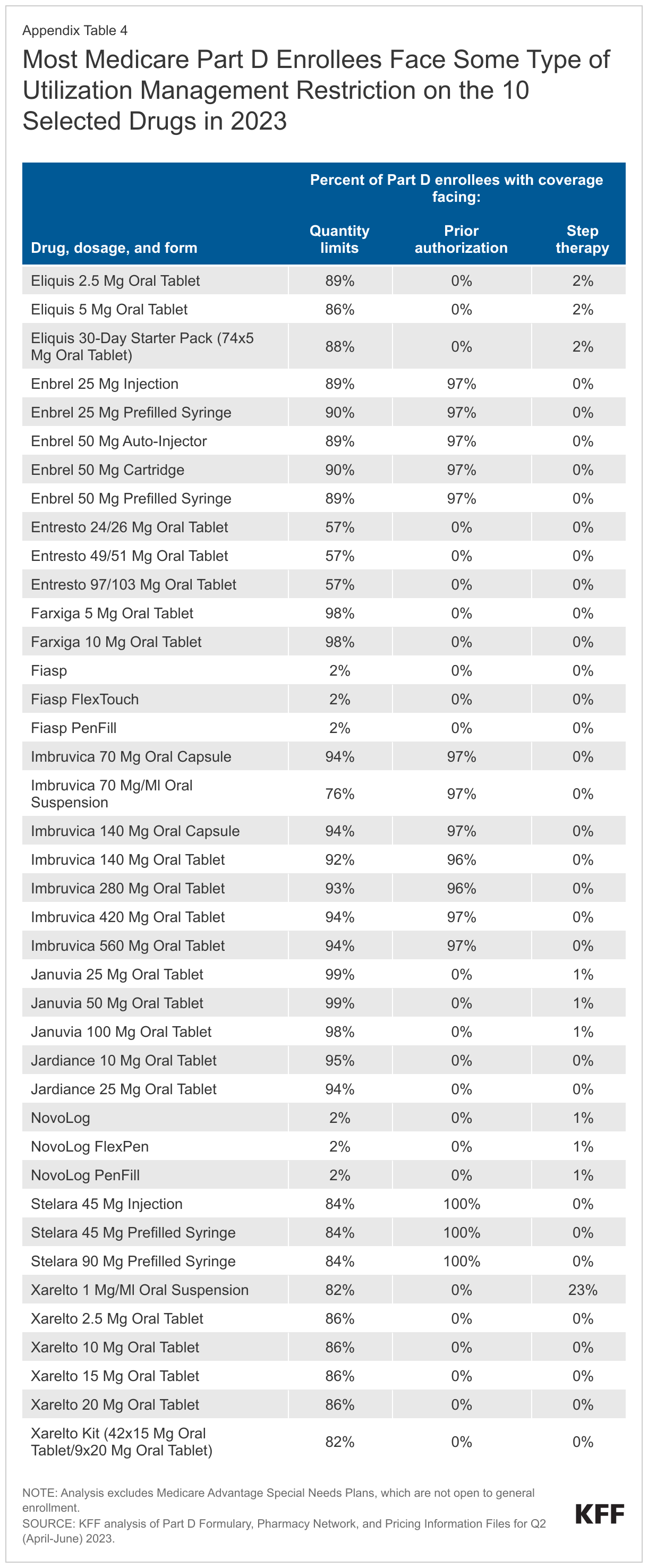
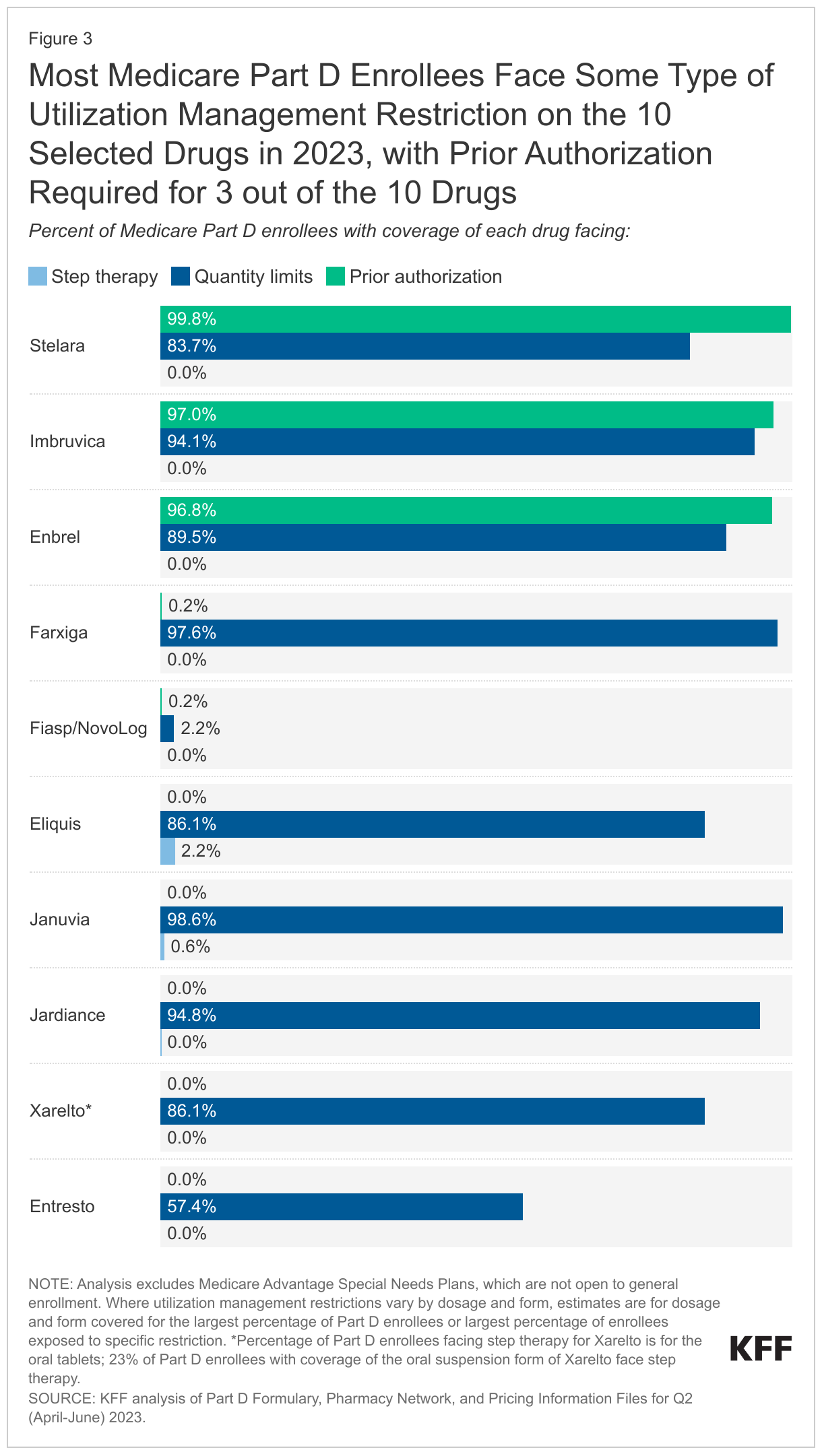
Most Part D enrollees face some type of utilization management restriction on the 10 selected drugs in 2023. Prior authorization requirements are applied to virtually all Part D enrollees who have coverage of Enbrel, Imbruvica, and Stelara in 2023, meaning that nearly all enrollees would need to get prior authorization from their plan prior to initiating treatment with any of these three drugs (Figure 3, Appendix Table 4). The most common utilization management restriction applied to the 10 selected drugs is quantity limits, ranging from around 2% of Part D enrollees who have coverage for the insulin product Fiasp/NovoLog to nearly all enrollees with coverage of Januvia and Jardiance. Step therapy requirements are rarely applied to these 10 drugs.
This analysis did not examine utilization management restrictions applied to other drugs in the same classes as selected drugs to assess whether utilization management applied to selected drugs in 2023 is comparatively more restrictive. But if CMS’s justification requirement leads to less frequent application of utilization management tools on selected drugs by Part D plans, utilization could increase.
Conclusion
While Medicare’s new drug price negotiation program is projected to lower Medicare spending on drugs selected for negotiation, less attention has been given to its potential to expand access to and utilization of selected drugs for Part D enrollees. In part, this could result from a requirement in the Inflation Reduction Act that all Part D plans cover all selected drugs once negotiated prices take effect. This requirement will have the effect of expanding coverage for the selected drugs that are not currently universally covered by all plans, in particular Fiasp/NovoLog and Stelara. This requirement could have a larger impact in future years, depending on formulary coverage of drugs selected for price negotiation in the future. CMS has also stated that it intends to use the annual formulary review process to ensure that all Part D plans cover all dosages and forms of selected drugs during the year that the negotiated prices apply. This level of coverage currently is not standard.
CMS has stated that it will also require plans to justify formulary placement of selected drugs on non-preferred tiers, where cost sharing is typically higher than when drugs are on preferred tiers. As of 2023, placement of the 10 selected drugs on non-preferred tiers is not common, but some Part D enrollees have coverage on a non-preferred tier and face higher cost-sharing requirements than for drugs on preferred tiers. If coverage of selected drugs shifts to preferred tiers, that could lower Part D enrollees’ out-of-pocket costs. And for drugs with coinsurance requirements, a lower negotiated price would result in lower out-of-pocket costs. In turn, lower out-of-pocket costs could lead to higher use of selected drugs.
Finally, CMS has stated that it expects plans to provide a justification if more restrictive utilization management is applied to selected drugs relative to non-selected drugs in the same class, or if utilization management restrictions that are not based on medical appropriateness are applied to selected drugs. If CMS’s justification requirement leads to less frequent application of utilization management tools on selected drugs by Part D plans, utilization could increase.
It should be noted that if manufacturers of selected drugs do not want to participate in price negotiations, they are required to withdraw their drugs from coverage under Medicare and Medicaid or face an excise tax on sales of the selected drug to Medicare beneficiaries. Withdrawal of products from coverage under the Medicare and Medicaid program would affect access to these medications, but would also mean that manufacturers would forfeit the revenue from sales of all of their products in these programs.
Taken altogether, the formulary and coverage requirements for selected drug in the Inflation Reduction Act and CMS guidance are likely to increase access to selected drugs for Medicare Part D enrollees and could also lower Part D enrollees’ out-of-pocket costs, which could increase utilization of these drugs and revenues for their manufacturers.
Juliette Cubanski and Tricia Neuman are with KFF. Anthony Damico is an independent consultant.
Methods
This analysis is based on KFF analysis of the Part D Formulary, Pharmacy Network, and Pricing Information Files for Q2 (April-June) 2023. Part D formulary files were used for analysis of formulary coverage, tier placement, cost-sharing amounts, and utilization management restrictions. The formulary analysis includes 4,281 Part D plans, both stand-alone prescription drug plans and Medicare Advantage drug plans, covering 37.3 million enrollees. Analysis excludes Medicare Advantage Special Needs Plans (SNPs), which are not open to general enrollment (1,144 plans covering 5.7 million enrollees).
Formulary tiers with tier number 3 were categorized as preferred brands, tier number 4 as non-preferred drugs, and tier number 5 as specialty drugs; all other tier numbers were categorized as other tier. Cost sharing is based on standard (i.e., non-preferred) 30-day cost-sharing requirements and is enrollment weighted.
Appendix