The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR)
Editorial Note: Originally published in November 2009, this resource is updated as needed to reflect the latest developments.
Key Facts
- Although the U.S. has been involved in efforts to address the global AIDS crisis since the mid-1980s, the creation of the President’s Emergency Plan for AIDS Relief (PEPFAR) in 2003 marked a significant increase in funding and attention to the epidemic. Now, more than 20 years in, PEPFAR reports saving an estimated 26 million lives and is currently providing HIV prevention and treatment services to millions.
- PEPFAR has been the largest commitment by any nation to address a single disease in the world, credited with not only saving millions of lives but also helping to change the trajectory of the global HIV epidemic.
- PEPFAR funding is comprised of U.S. bilateral funding and U.S. contributions to multilateral organizations addressing HIV, primarily the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund).1
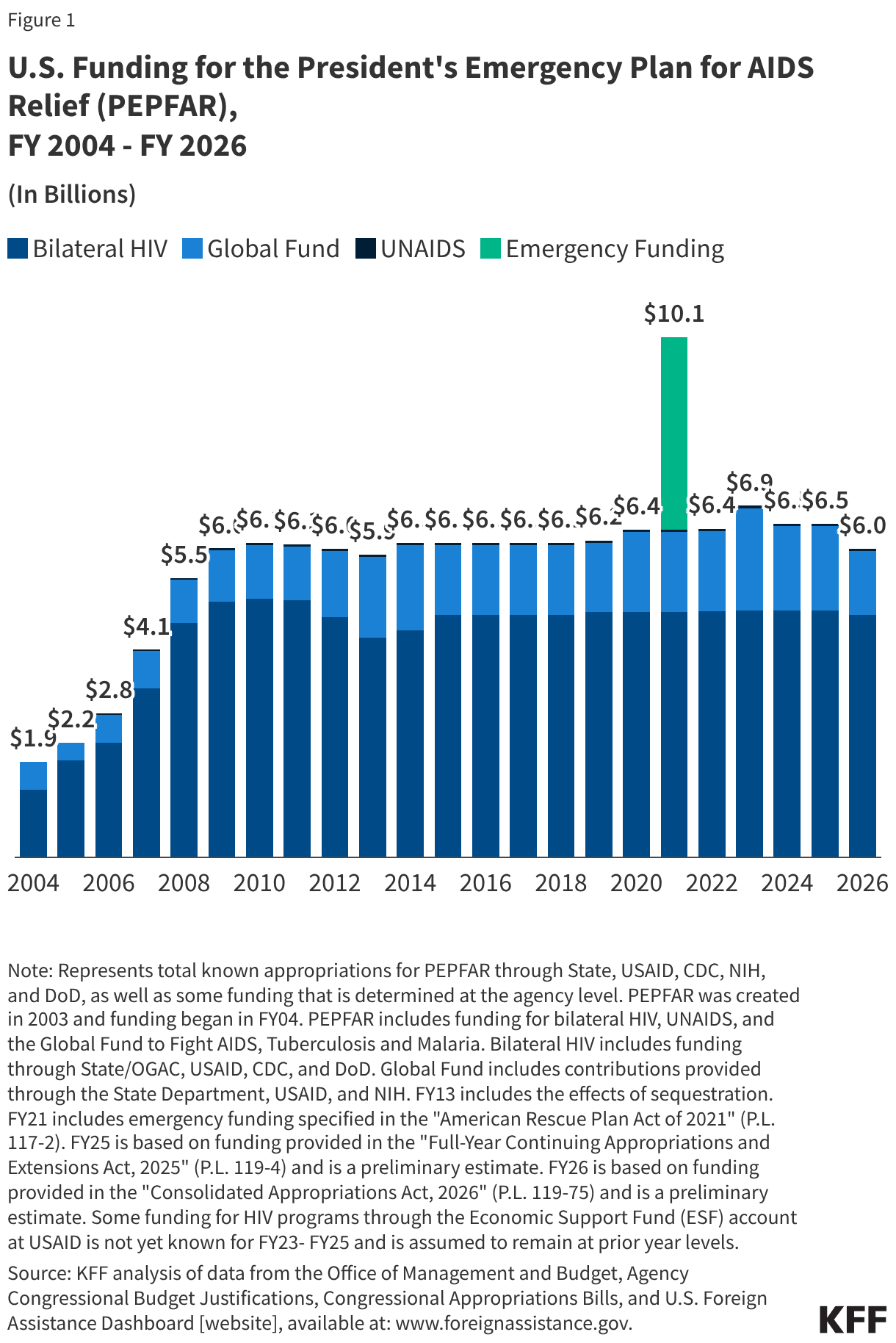
- To date, U.S. funding appropriated by Congress for PEPFAR has totaled over $130 billion, growing from $1.9 billion in FY 2004 to $6 billion in FY 2026; in FY 2026, funding includes $4.7 billion provided for bilateral HIV efforts and $1.3 billion for multilateral efforts ($45 million for UNAIDS and $1.25 billion for the Global Fund).2
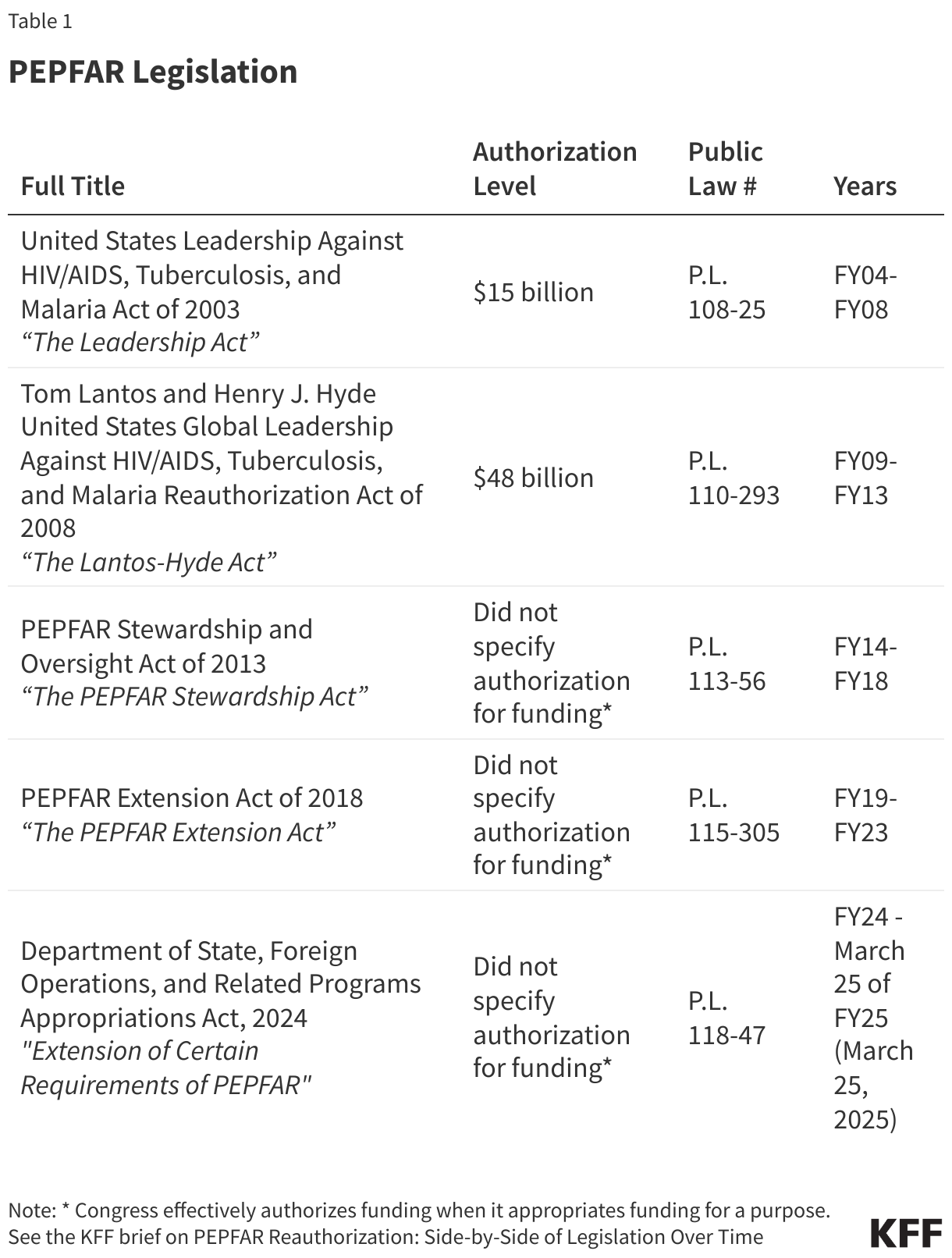
- PEPFAR has been reauthorized by Congress four times, most recently in March 2024 for one year. Although that authorization expired on March 25, 2025, PEPFAR is a permanent part of U.S. law and, other than a now-expired set of eight time-bound provisions, continues as long as Congress appropriates funding for the program.
- At the same time, changes made by the Trump administration starting in 2025 (including a reorganization of foreign assistance, reductions in funding, and cancellation of programs) have fundamentally altered the global health landscape generally and PEPFAR specifically. As part of its new America First Global Health Strategy, anchored in bilateral health agreements with countries, HIV services will be integrated into country health systems, and the U.S. will aim to reduce its funding over time.
Global Situation
HIV, the virus that causes AIDS (“acquired immunodeficiency syndrome” or Advanced HIV Disease), has become one of the world’s most serious health and development challenges. Today, there are approximately 40.8 million people living with HIV, and tens of millions of people have died of AIDS-related causes since the beginning of the epidemic (see the KFF fact sheet on the global HIV epidemic).3
Box 1: Snapshot of Global Epidemic Today
- Number of people living with HIV: 40.8 million
- Number of people newly infected with HIV: 1.3 million
- Number of AIDS-related deaths: 630,000
- Number of people with HIV on treatment: 31.6 million
Notes: Reflects 2024 data.
U.S. Government Efforts
Although the U.S. had been involved in efforts to address the global HIV/AIDS crisis since the mid-1980s,4 the creation of the President’s Emergency Plan for AIDS Relief (PEPFAR) in 2003 marked a significant increase in funding and attention to the epidemic.5 PEPFAR, the U.S. government’s global effort to combat HIV and the largest global health program devoted to a single disease, is credited with saving millions of lives and helping to change the trajectory of the global HIV epidemic. It was announced in January 2003 during President George W. Bush’s State of the Union and authorized by Congress that same year through the Leadership Act. The Leadership Act governs PEPFAR’s HIV response, as well as U.S. participation in the Global Fund (an independent, international multilateral financing institution that provides grants to countries to address HIV, TB, and malaria) and bilateral assistance for TB and malaria programs.6 Congress has updated, extended, and made changes to the program through the Lantos-Hyde Act of 2008, the PEPFAR Stewardship Act of 2013, the PEPFAR Extension Act of 2018, and more recently, a short-term reauthorization of PEPFAR in early 2024 that extended certain timebound provisions through late March 2025, which have since lapsed (see Table 1 and the KFF brief on PEPFAR reauthorization legislation over time). This short term reauthorization signaled a departure from the program’s long history of strong bipartisan support across multiple Congresses and administrations when, in an increasingly partisan environment, PEPFAR was caught up in the broader U.S. political debate over abortion (see the KFF brief on PEPFAR’s short term reauthorization). This and other developments, including the Trump administration’s review of foreign assistance and new America First Global Health Strategy, have fundamentally altered PEPFAR and introduced significant uncertainty about its future.
Organization
PEPFAR’s original authorization established new structures and authorities, consolidating all U.S. bilateral and multilateral activities and funding for global HIV/AIDS.7 Historically, PEPFAR has been overseen by the U.S. Global AIDS Coordinator, who is appointed by the President, confirmed by the Senate, and reports directly to the Secretary of State, as established through PEPFAR’s authorizing legislation.8 The Coordinator holds the rank of Ambassador and leads the Office of the Global AIDS Coordinator (OGAC) at the Department of State.9 The Coordinator has primary responsibility for the oversight and coordination of all U.S. global HIV activities and funding across U.S. implementing agencies and departments. In addition, the Coordinator serves as the U.S. Government’s board member to the Global Fund (the U.S. Government holds a permanent seat on the Global Fund’s Board). The Coordinator is dual-hatted as the U.S. Special Representative for Global Health Diplomacy and also leads the broader Bureau of Global Health Security and Diplomacy (GHSD), which brings together PEPFAR with global health security and global health diplomacy functions.10 Currently, the President has not yet nominated a Coordinator, and it is unclear when or whether someone will be nominated.
In addition to the Department of State, other implementing departments and agencies for HIV activities have included: the U.S. Agency for International Development (USAID), PEPFAR’s largest government implementing agency (the Trump administration dissolved USAID and integrated remaining USAID global health activities into GHSD); the Department of Health and Human Services, primarily through the Centers for Disease Control and Prevention (CDC), which has also gone through staff reductions and seen a diminished role under the Trump administration; the Departments of Labor, Commerce, and Defense (DoD); and the Peace Corps.11 Currently, however, most PEPFAR activity is being managed out of the State Department as it transitions programs and services to country governments.
Key Activities and Results
PEPFAR reports having saved an estimated 26 million lives, focusing on expanding access to HIV prevention, treatment, and care interventions. This has included provision of antiretroviral treatment, pre-exposure prophylaxis, voluntary male circumcision, condoms, and other commodities related to HIV services, although some of these services have now been scaled back or discontinued by the administration.12 In addition, PEPFAR launched specific initiatives in key strategic areas. For example, in 2015, PEPFAR launched DREAMS, a public-private partnership that aimed to reduce HIV infections in adolescent girls and young women; the DREAMS program has been discontinued.
In FY 2024, the last full year of data reported, PEPFAR indicated that it had supported testing services for 83.8 million people; prevented 7.8 million babies from being born with HIV, who would have otherwise been infected; provided care for more than 6.6 million orphans, vulnerable children (OVC), and their caregivers; supported training for nearly 342,000 new health care workers; and supported antiretroviral treatment for 20.6 million people.13 However, more recent data is mixed. For example, analysis of data from Quarter 4 of FY 2025 found that while the number of people on antiretroviral therapy was stable compared to Quarter 4 of FY 2024, the number newly enrolled on antiretroviral therapy, the number tested, and the number receiving PrEP, dropped significantly.14
Since the beginning of the second Trump administration, numerous actions have already had a significant impact on PEPFAR operations and programmatic outcomes), including the following:
- the administration’s foreign aid review and funding freeze, announced in 2025, which limited PEPFAR’s activities to those defined in a limited waiver, significantly scaling back PEPFAR’s scope to what the waiver defines as “life-saving HIV services,” which include only certain activities: HIV treatment and care, prevention of mother-to-child transmission (PMTCT), pre-exposure prophylaxis (PrEP) for pregnant and breastfeeding women, and HIV testing, but even after the initial period, not all of these services have been continued;
- the administration’s September 2025 announcement that PEPFAR would partner with the Global Fund to provide long-acting injectable PrEP, reaching up to 2 million people in high-burden HIV countries through 2028, and then more recently in April 2026, the announcement of an expanded commitment to reach an additional 1 million people, bringing the total to 3 million people; and
- the administration’s September 2025 release of its new America First Global Health Strategy, which provides a framework for global health efforts in countries receiving PEPFAR assistance through bilateral health agreements that aim to reduce U.S. funding over time. Under the agreements, the U.S. plans to provide 100% of current levels of PEPFAR funding for commodities and frontline healthcare workers in 2026 and reduced funding thereafter. More broadly, HIV services will be integrated into country health systems, as the U.S. reduces its funding and direct implementation role.
Countries Reached
Historically, PEPFAR bilateral programs were carried out in more than 50 countries.15 Additional countries are reached through U.S. contributions to the Global Fund. Prior to the second Trump administration, PEPFAR required 25 countries16 and the Asia, Western Hemisphere, and West Africa regional programs to develop “Country Operational Plans” (COPs) and “Regional Operational Plans” (ROPs), respectively, to document annual investments and anticipated results.17 OGAC reviewed and the Global AIDS Coordinator approved COP/ROPs. Currently, this process has been replaced by new bilateral global health agreements with partner countries, which are not specific to PEPFAR or HIV and which require partner countries to increasingly co-invest domestic government resources while the U.S. decreases its health assistance over time. (See the KFF tracker on bilateral global health agreements for more details.)
Funding18
Total PEPFAR funding19 includes bilateral funding to U.S. agencies for HIV activities as well as U.S. contributions to the Global Fund and UNAIDS,20 as specified by Congress for PEPFAR in annual appropriations bills.21 It has represented the majority of U.S. global health funding (ranging from 53-55% in recent years22) and is the largest commitment by any nation to address a single disease in the world. To date, funding appropriated for PEPFAR totals more than $130 billion, with funding reaching $6 billion in FY 2026 (see figure).
PEPFAR’s creation marked a significant increase in the amount of funding provided by the U.S. for HIV. Trends in funding for bilateral programs and contributions to multilateral organizations are as follows (see the KFF fact sheet on the U.S. Global Health Budget: Global HIV Funding, Including PEPFAR and U.S. Global Health Budget: The Global Fund):
- Bilateral HIV Funding: The majority of PEPFAR funding (ranging from 70-79% each year over the past decade) is provided for bilateral programs through the State Department (most of which had been transferred to other agencies – particularly USAID and CDC – but now is managed by the State Department). Bilateral funding rose rapidly from $822 million in FY 2003 (the year before PEPFAR) to a peak of $5.0 billion in FY 2010. Between FY 2010 and FY 2013, it declined by more than $750 million. While it has risen since then, funding leveled off for several years, and in FY 2026, appropriations totaled $4.7 billion ($316 million below its peak level).
- Multilateral Funding: The U.S. also supports global HIV efforts through contributions to the Global Fund and UNAIDS. Support for the Global Fund, which accounts for most of the multilateral contributions, increased rapidly in its early years and fluctuated over time; it reached its highest level to date ($2.0 billion) in FY 2023. In FY 2026, Congressionally-appropriated funding for the Global Fund was $1.25 billion, $400 million less than the FY 2025 level, though Congress noted that this funding is intended for the first installment of the $4.6 billion U.S. pledge to the Global Fund’s eighth funding replenishment period (2026-2028).23 The U.S. contribution to UNAIDS has fluctuated between $45 and $50 million; it was $45 million in FY 2026.
- Emergency COVID-19 Funding: In FY 2021, an additional $3.8 billion in emergency supplemental funding was provided for bilateral HIV ($250 million) and the Global Fund ($3.5 billion) to address COVID-19.24
Spending Directives25
PEPFAR has included several spending directives, or earmarks, from Congress over the course of its history, many of which have changed over time:
- The Leadership Act, PEPFAR’s original authorization, included the following spending directives: 55% of funds were to be spent on treatment; 15% on palliative care; 20% on prevention, of which at least 33% be spent on abstinence-until-marriage programs; and 10% on OVC. While these were included as “sense of Congress” recommendations, the treatment, OVC, and abstinence-until-marriage earmarks were made requirements as of FY 2006.
- The Lantos-Hyde Act relaxed some of these directives for the FY 2009 – FY 2013 period: while still requiring that 10% of funds be spent on programs targeting OVC, it changed the treatment earmark from 55% to requiring that at least half of bilateral HIV assistance be spent on treatment and care. It removed the 33% abstinence-until-marriage directive and replaced it with a requirement of “balanced funding” for prevention to be accompanied by a report to Congress if less than half of prevention funds were spent on abstinence, delay of sexual debut, monogamy, fidelity, and partner reduction activities in any host country with a generalized (high prevalence) epidemic.
- The PEPFAR Stewardship Act, The PEPFAR Extension Act, and recent short-term reauthorization have maintained the language in the Lantos-Hyde Act. With the expiration of the short-term reauthorization in 2025, eight timebound provisions have now lapsed, although PEPFAR is a permanent part of U.S. law.
PEPFAR & The Global Fund
The U.S. is the single largest donor to the Global Fund. Appropriations for the U.S. contribution to the Global Fund totaled almost $33 billion from FY 2001 through FY 2026 (including emergency funding for COVID-19).26
The Global Fund provides another mechanism for U.S. support by funding programs developed by recipient countries, reaching a broader range of countries, and supporting TB, malaria, and health systems strengthening (HSS) programs in addition to (and beyond their linkage with) HIV.27 To date, over 120 countries28 have received Global Fund grants. Most Global Fund support (52%) has been signed and approved by the Board for HIV and HIV/TB programs,29 followed by 29% to malaria, 15% to TB, and 5% to other health issues.30 The original authorization of PEPFAR, and subsequent reauthorizations, included a limit on annual U.S. contributions to the Global Fund that prevented them from causing cumulative U.S. contributions to exceed 33% of the Global Fund’s total contributions (see the KFF fact sheet on the Global Fund). 31
Endnotes
- KFF analysis of The Global Fund: https://data-service.theglobalfund.org/downloads. ↩︎
- Totals represent funding specified by Congress in annual appropriations bills and/or identified by agencies for the Department of State, USAID, CDC, and DoD. In addition, international HIV research activities are supported by the NIH Office of AIDS Research (OAR) through its annual appropriated budget, but these amounts are not considered part of PEPFAR. See KFF's “Breaking Down the U.S. Global Health Budget by Program Area” for additional information. ↩︎
- UNAIDS. 2025 UNAIDS Global AIDS Update: AIDS, Crisis and the Power to Transform; July 2025. ↩︎
- The U.S. first provided funding to address the global HIV epidemic in 1986. Then, in 1999, President Bill Clinton announced the Leadership and Investment in Fighting an Epidemic (LIFE) Initiative to address HIV in 14 African countries and in India. Later, in 2002, President George W. Bush announced the International Mother and Child HIV Prevention Initiative focused on 12 African and two Caribbean countries. ↩︎
- PEPFAR. 2009 Annual Report to Congress; Jan. 2009. ↩︎
- U.S. Congress. P.L. 108-25; May 27, 2003. ↩︎
- KFF. The U.S. Government and Global Health, Sep. 2022. CRS. PEPFAR Reauthorization: Key Policy Debates and Changes to U.S. International HIV/AIDS, Tuberculosis, Malaria and Programs and Funding; Jan. 2009. ↩︎
- U.S. Congress. Public Law No: 108-25; May 27, 2003. ↩︎
- U.S. Department of State. “Leadership – Bureau of Global Health Security and Diplomacy” webpage, https://www.state.gov/leadership-bureau-of-global-health-security-and-diplomacy. ↩︎
- Department of State. “ Leadership – Bureau of Global Health Security and Diplomacy,” webpage, https://www.state.gov/leadership-bureau-of-global-health-security-and-diplomacy/. ↩︎
- PEPFAR. “About Us,” webpage, https://www.state.gov/about-us-pepfar/. ↩︎
- KFF. Funding for Key HIV Commodities in PEPFAR Countries; July 2021. ↩︎
- PEPFAR. PEPFAR Latest Global Results; December 2024. ↩︎
- KFF. What We Know from the Latest PEPFAR Data: Analysis of FY 2025 Quarter 4 Results; April 2026. ↩︎
- PEPFAR, “Where We Work” webpage, https://www.state.gov/where-we-work-pepfar/; PEPFAR 2023 Country Operational Plan Guidance for all PEPFAR Countries; and CDC’s “Where We Work” webpage, https://www.cdc.gov/global-hiv-tb/php/where-we-work/. ↩︎
- The 25 countries that were required to complete a FY23 COP are Angola, Botswana, Burundi, Cameroon, Cote d’Ivoire, Democratic Republic of the Congo, Dominican Republic, Eswatini, Ethiopia, Haiti, Kenya, Lesotho, Malawi, Mozambique, Namibia, Nigeria, Rwanda, South Africa, South Sudan, Tanzania, Uganda, Ukraine, Vietnam, Zambia, and Zimbabwe. PEPFAR. “Where We Work” webpage, https://www.state.gov/where-we-work-pepfar/. ↩︎
- PEPFAR. 2023 Country and Regional Operational Plan Guidance and Technical Considerations; Feb. 2023. ↩︎
- U.S. Congress. Public Law No: 112-25; Aug. 2, 2011. White House Office of Management and Budget (OMB). OMB Report to the Congress on the Joint Committee Sequestration for Fiscal Year 2013; March 1, 2013. KFF analysis of data from: Congressional appropriations bills and reports; Federal Agency Budget and Congressional Justification documents; ForeignAssistance.gov; KFF personal communication with the Office of Management and Budget. ↩︎
- Overall PEPFAR funding technically includes support for bilateral HIV and TB activities, as well as contributions to multilateral organizations (specifically, the Global Fund and UNAIDS). This analysis only focuses on bilateral funding for HIV and contributions to multilateral organizations. ↩︎
- UNAIDS is the Joint United Nations Programme on HIV/AIDS, the U.N. system’s coordinating body that serves to help galvanize worldwide attention to AIDS. ↩︎
- Totals represent funding specified by Congress for PEPFAR in annual appropriations bills and/or identified by agencies for the Department of State, USAID, CDC, and DoD. In addition, international HIV research activities are supported by the NIH Office of AIDS Research (OAR) through its annual appropriated budget, but these amounts are not considered part of PEPFAR. See KFF's “Breaking Down the U.S. Global Health Budget by Program Area” for additional information. ↩︎
- Includes bilateral funding for HIV as well as U.S. contributions to UNAIDS and the Global Fund to Fight AIDS, Tuberculosis and Malaria through regular appropriations. ↩︎
- U.S. Congress. Public Law No: 119-75; February 2026. The explanatory statement accompanying the FY 2026 conference agreement notes that the U.S. contribution supports the $4.6 billion U.S. pledge to the eighth replenishment and that the $1.25 billion provided in the agreement is for the first installment of the replenishment. The explanatory statement also states that the “funds shall be contributed to the Global Fund on a quarterly basis to the fullest extent practicable” and that “sufficient unobligated balances [that] exist[ed] from prior Acts to fully fund the first installment of the eighth replenishment and to fulfill the United States pledge for the seventh replenishment” are to be provided in a “timely manner.” ↩︎
- KFF analysis of data from the “American Rescue Plan Act of 2021” (P.L. 117-2). ↩︎
- U.S. Congress. Public Law No: 108-25; May 27, 2003. U.S. Congress. Public Law No: 110-293; July 30, 2008. U.S. Congress. Public Law No: 113-56; Dec. 2, 2013. U.S. Congress. Public Law No: 115-305; Dec. 11, 2018. U.S. Congress. Public Law No: 118-47; March 23, 2024. ↩︎
- Includes funding through regular appropriations and emergency supplemental funding. KFF analysis of data from: Congressional appropriations bills and reports; Federal Agency Budget and Congressional Justification documents; ForeignAssistance.gov; KFF personal communication with the Office of Management and Budget. KFF analysis of data from the “American Rescue Plan Act of 2021” (P.L. 117-2). ↩︎
- Congress states that the Global Fund is the multilateral component of PEPFAR in the following: U.S. Congress. Public Law No: 110-293; July 30, 2008. U.S. Congress. Public Law No: 113-56; Dec. 2, 2013. ↩︎
- Does not include countries that may have received funding through multi-country or regional programs. Additional countries may be reached through multi-country or regional programs. ↩︎
- Of the 52% committed to HIV and HIV/TB programs, 38% was for HIV activities and 14% was for HIV/TB activities. ↩︎
- Percentages may not sum due to rounding. In 2020, some donor governments provided COVID-specific emergency contributions to the Global Fund in addition to their contributions to core activities. For the purposes of this fact sheet, these COVID-specific amounts have been excluded as they cannot be attributed to a specific area, such as HIV, TB, or malaria. The Global Fund. Data Explorer; accessed January 2026: https://data.theglobalfund.org/. ↩︎
- U.S. Congress. Public Law No: 108-25; May 27, 2003. U.S. Congress. Public Law No: 110-293; July 30, 2008. U.S. Congress. Public Law No: 113-56; Dec. 2, 2013. U.S. Congress. Public Law No: 118-47; March 23, 2024. KFF. PEPFAR Reauthorization: Side-by-Side of Legislation Over Time. ↩︎