Title 42 and its Impact on Immigration and Migrant Families
Introduction
Title 42 of the Public Health Services Act is a public health authority that authorizes the Director of the Centers for Disease Control and Prevention (CDC) to suspend entry of individuals into the U.S. to protect public health. This rarely utilized authority was implemented by the Trump administration in March 2020 in response to the COVID-19 pandemic to allow for quick expulsion of migrants, including asylum seekers, seeking entry into the U.S. at the land borders. After a series of delays due to court challenges, the restrictions were lifted when the Biden Administration declared an end to the COVID-19 public health emergency (PHE) on May 11, 2023. The Biden administration subsequently took increasingly restrictive executive action to restrict border entry.
Land border entries into the U.S. decreased as a result of Title 42 since individuals who had border encounters under this authority were immediately expelled due to the public health threat outlined by the Trump administration. However, research suggests that Title 42 restrictions did not result in a “better managed border” and increased cases of unauthorized re-entry, and public health experts stated that it put the health and well-being of migrants at risk. Recent reports suggest President-elect Trump may reinvoke Title 42 restrictions during his second term to close the border between the U.S. and Mexico, along with a number of other actions to restrict immigration.
This brief provides an explanation of Title 42 and its application in border regions, the impact of Title 42 on border expulsions and the health and well-being of migrants during COVID-19, and a discussion of the potential implications of reinvoking Title 42 restrictions for immigration and the health of migrants.
What are policies for migrants seeking entry at the U.S. border?
Under U.S. immigration law, individuals have a legal right to claim asylum when presenting at U.S. ports of entry. An asylee is an individual already present in the U.S. or seeking admission at a port of entry who is seeking protection based on “persecution or a well-founded fear of persecution on account of their race, religion, nationality, membership in a particular social group, or political opinion.” In fiscal year (FY) 2023, the U.S. granted asylum to over 54,000 individuals from close to a dozen different countries. However, as of October 2024, over 90% of asylum cases filed in FY 2023 were still pending with only 2% being granted approval due to immigration backlogs.
Migrants encountered at the border are processed and screened for asylum under Title 8 of the U.S. Code addressing “Aliens and Nationality.” Under Title 8, those determined to have a credible fear of persecution or other threats in their home country are either held in custody or released into the U.S. while their case is pending in immigration court. Those who the U.S. Citizenship and Immigration Services (USCIS) determine not to have a credible fear are permitted to appeal this decision to an immigration judge. If an individual chooses not to appeal or the immigration judge did not find fear, then the individual is removed.
In June 2024, the Biden administration took executive action to suspend and limit the entry of migrants at the southern border, including asylum seekers, to “address the historic levels of migration and more efficiently process migrants arriving at the southern border.” Under this rule, the suspension of entry will go into effect immediately after there have been 2,500 or more average daily border encounters (not including unaccompanied children) over seven consecutive days and can be lifted once there have been fewer than 1,500 average daily border encounters over seven consecutive days. As of April 2024, there were about 4,000 average daily border encounters, leaving the restrictions in place. U.S. Customs and Border Patrol (CBP) data show that border encounters following the executive order were at a three-year low with there being a 29% reduction in encounters between May and June 2024.
How did Title 42 change policy for migrants seeking entry at the border during the COVID-19 pandemic?
In March 2020, the Trump administration implemented Title 42 under the Public Health Service Act, which allowed for the immediate expulsion of migrants without screening for asylum. This order applied to all migrants arriving to the U.S. from Canada or Mexico regardless of their country of origin who would otherwise be held in a congregate setting at a port of entry or border patrol station. It did not apply to lawful permanent residents and their families, members of the armed forces or their families, or people who hold valid travel documents such as tourists or those in a visa waiver program. Officials also had authority to make exceptions for individuals on a case-by-case basis. Under this order, the CDC Director was authorized to “suspend the introduction of persons into the United States” and CBP officials were directed to process migrants promptly (within 15 minutes in an outdoor setting) without screening for asylum and expel them back to Mexico or Canada or their country of origin. The CDC stated the purpose of the order was to protect CBP personnel, U.S. citizens, lawful permanent residents, and other individuals from an increase in COVID-19 spread at land ports of entry, Border Patrol stations, and in the interior of the country. The order pointed to the introduction of individuals into congregate settings at the border and the increased strain this would put on the U.S. health care system during a public health emergency as primary reasons for implementing the restrictions on entry.
Title 42 continued to be enforced under the Biden administration until the end of the COVID-19 PHE declaration in May 2023. However, unaccompanied minors were exempted from the order based on a district court ruling in November 2020 and by a CDC order issued under the Biden administration in February 2021. The CDC order continued to apply the original Title 42 order to single adults and families. After facing legal challenges, Title 42 restrictions were lifted in May 2023 following the end of the COVID-19 PHE declaration.
How did implementation of Title 42 impact immigration and the health of migrants?
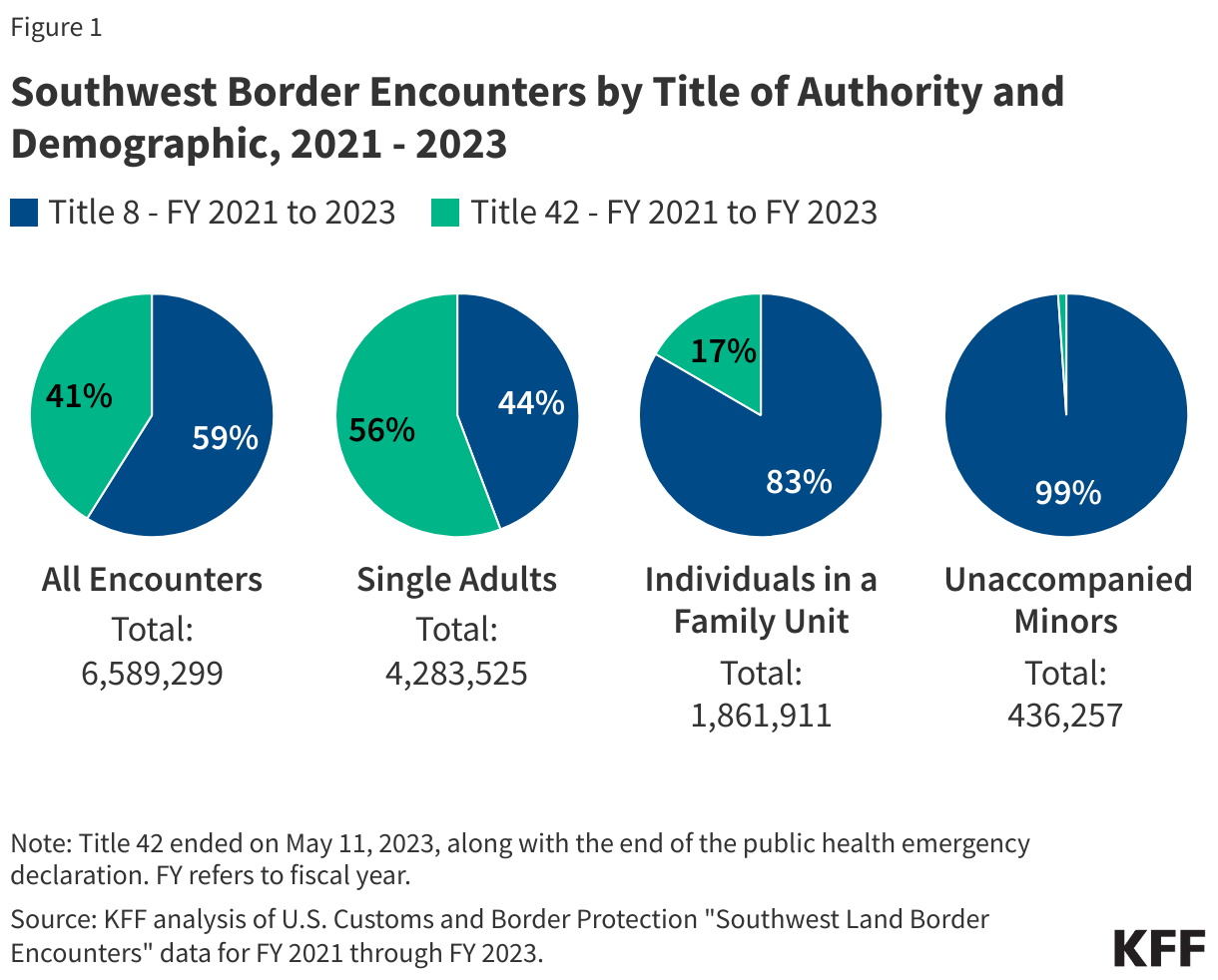
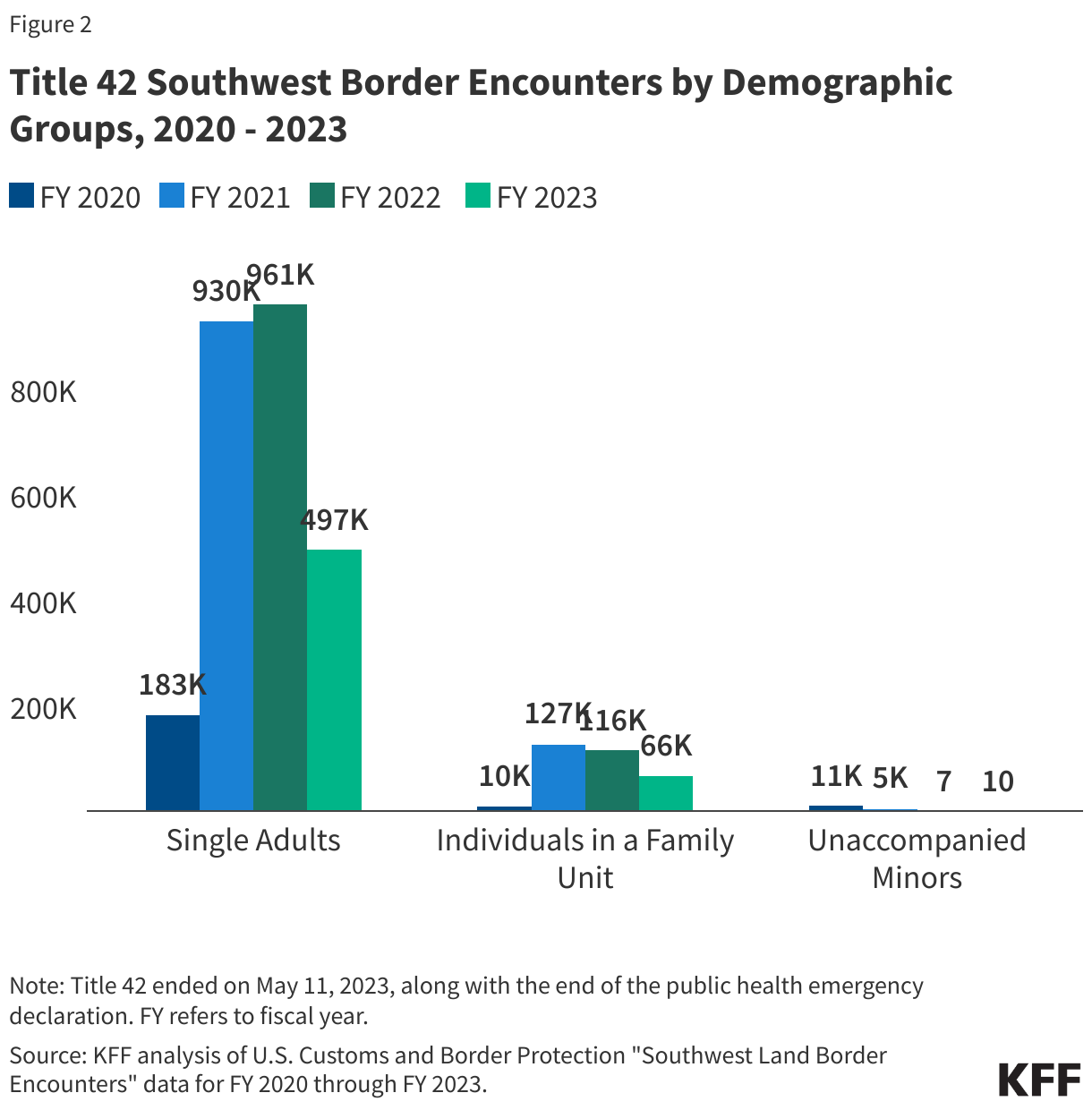
Between FY 20211 and 2023, there were over 6.5 million encounters at the Southwest land border of which about four in ten (41%) were under Title 42 authority. Enforcement encounters refer to “apprehensions or inadmissibles processed under CBP’s immigration authority;” these include individuals apprehended under Title 8 as well as individuals expelled under Title 42. While Title 42 applies to both the Northern and Southwestern Borders, nearly all Title 42 encounters occurred at the Southwestern Border. Between FY 2021 and FY 2023, Title 42 encounters at the Southwest Border accounted for about four in ten (41%) of all Southwest Border encounters. The share of encounters that were under Title 42 varied by demographic group with Title 42 accounting for a majority (56%) of single adult encounters and one in six (17%) family encounters, while Title 8 accounted for virtually all (99%) encounters with unaccompanied minors reflecting their exemption from expulsion under Title 42 (Figure 1).
As of May 2023, there were over 2.5 million single adult expulsions, nearly 320,000 expulsions of individuals in a family unit, and nearly 16,000 expulsions of unaccompanied minors under Title 42. The number of family expulsions under Title 42 grew between FY 2020 and FY 2021, while expulsions of unaccompanied minors decreased, reflecting their exemption beginning in February 2021. These encounter counts reflect repeat encounters with individuals, as each attempt by the same individual to cross the border is counted as a new encounter.
Data indicate that Title 42 did not lead to a reduction in border encounters, but border entries into the U.S. went down due to the nature of the authority. While Title 42 was intended to reduce COVID-19 exposure risk at the border, it led to an increasing number of encounters at the border largely due to repeat encounters. This is in large part because, unlike Title 8, migrants apprehended under Title 42 were immediately expelled and those with repeat encounters did not face any penalties. Data from 2020 through 2023 suggest that while there were close to 3 million Southwest border expulsions under Title 42 authority, many of those expulsions were of the same individuals making repeated attempts to cross the border. In the last 6 months of 2021, a quarter of the encounters under Title 42 were of the same individuals on multiple occasions, with recidivism rates under the authority being at their highest levels in over a decade. In addition, there has not been a significant increase in border encounters since Title 42 was lifted with border encounters in FY 2024 (2.1 million) being lower than border encounters in FY 2022 (2.4 million) and FY 2023 (2.5 million). However, entries into the U.S. through land borders decreased as a result of Title 42 since individuals who had border encounters under this authority were immediately expelled due to the public health threat outlined by the Trump administration.
Research suggests Title 42 expulsions negatively impacted the health and well-being of migrant families while having little to no impact on preventing the spread of COVID-19 in the U.S. Physicians, epidemiologists, and public health experts repeatedly stated that Title 42 was counterproductive to preserving health and protecting individuals from COVID-19. Physicians suggested that being in close proximity with other individuals while being temporarily detained or transported back to Mexico, lack of medical screenings, and lack of provision of necessary medication could have adverse impacts on physical and mental health. Typically, the CDC recommends that asylees be provided an initial medical screening within 30-60 days of arriving in the U.S., but since Title 42 called for immediate expulsion, such screenings were not provided. Interviews conducted with over two dozen asylum seekers who were expelled under Title 42 authority found that a vast majority reported symptoms of depression, anxiety, and post-traumatic stress disorder (PTSD), and many reported that their children’s mental health was also impacted. Sending individuals back to potentially dangerous situations they were fleeing also poses risks. Title 42 may also have contributed to increases in family separations at the border. Media reports suggested that some families were separating from their children so that the children could seek entry as unaccompanied minors, who were exempt from Title 42 expulsions. These separations may have led to children facing dangerous situations traveling to the border and expose them to trauma and toxic stress. The impact of Title 42 on migrant families may also have been exacerbated by the “Remain in Mexico” or Migrant Protection Protocols program implemented under the first Trump administration, which required thousands of migrants (including children) to wait for their U.S. immigration court hearings in Mexican border towns that can be dangerous and unsafe. Close to 80% of migrants receiving medical treatment from Doctors without Borders/Medecins Sans Frontieres at border locations in Nuevo Laredo, Mexico, reported being victims of violence, with many experiencing depression, severe anxiety, and post-traumatic stress.
What are the potential implications of reinvoking Title 42?
The incoming Trump administration has indicated plans to reinvoke Title 42. President-elect Trump has proposed an array of policies focused on restricting immigration. Recent reports suggest that the incoming Trump administration is planning to reinvoke Title 42 to restrict immigration under the rubric of public health protection. Experiences during COVID-19 suggest Title 42 was not effective at reducing border encounters or preventing COVID-19 and had negative health impacts for migrants. Reinvocation of such a policy also raises questions about its use as a border enforcement tool and could potentially fuel xenophobic sentiment towards immigrants.
- U.S. Customs and Border Protection, “Nationwide Enforcement Encounters: Title 8 Enforcement Actions and Title 42 Expulsions Fiscal Year 2021”. Accessed January 2025. ↩︎



 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma