How Have States Used Medicaid Emergency Authorities During COVID-19 and What Can We Learn?
In response to the COVID-19 public health emergency, states and the federal government took a range of actions in Medicaid to enhance capacity to respond to the public health and economic crises. The COVID-19 pandemic had wide ranging effects across Medicaid, impacting providers, beneficiaries, and long-term services and supports (LTSS). States were able to use Medicaid emergency authorities to address specific challenges and make necessary changes as circumstances evolved and new challenges emerged.
Although the federal public health emergency (PHE) remains in place, as vaccine rates increased and COVID-19 cases declined earlier this year, many state-level emergency declarations expired and states started to terminate some Medicaid flexibilities beginning in late Spring and early Summer of 2021. However, the Delta variant and low vaccination rates in some areas may present additional challenges. The Biden Administration has indicated it intends to extend the public health emergency until at least the end of calendar year 2021, but a continued wave of infections, hospitalizations, and deaths could lead to further extensions and continued emergency authorities in Medicaid.
This brief summarizes how states have used Medicaid emergency authorities related to the COVID-19 PHE, providing potential lessons for future public health and economic crises.
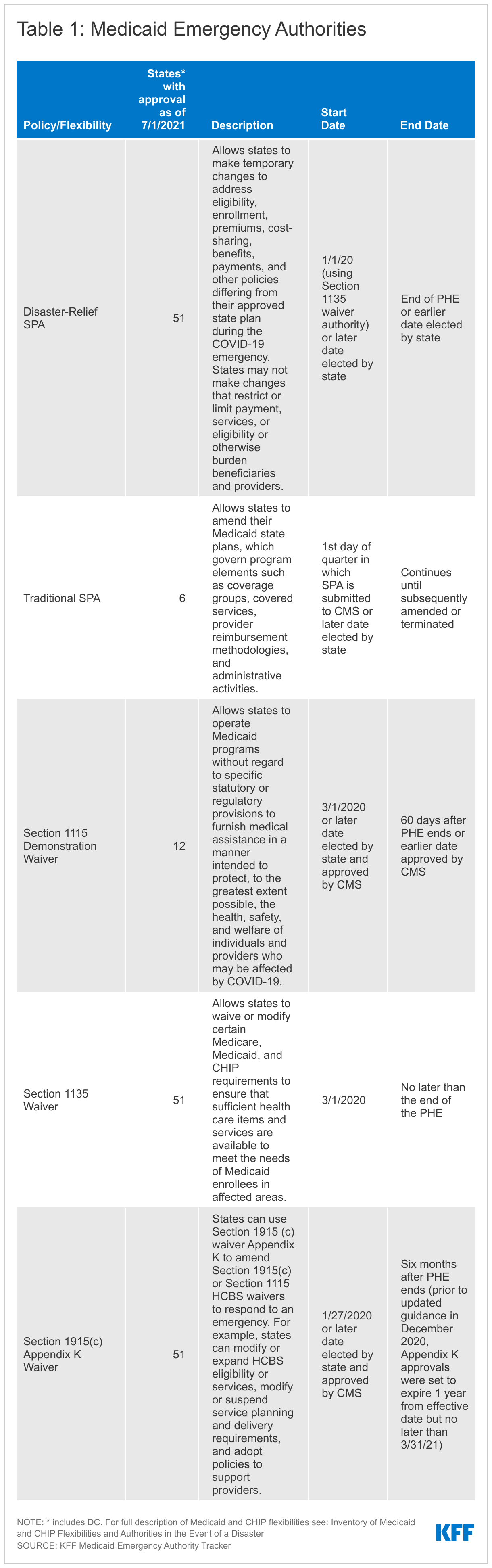
The declarations of a national disaster and a public health emergency allow for the use of a range of Medicaid emergency authorities. These authorities include Disaster-Relief state plan amendments (SPAs), Section 1135 waivers, Section 1915(c) Appendix K waivers, and Section 1115 waivers. States can also make Medicaid program changes during a PHE using existing administrative authorities and traditional SPAs. In addition, Congress enacted major federal legislation to respond to the COVID-19 emergency, including funding to support Medicaid and increase access to Medicaid coverage. The PHE began on January 27, 2020, and the most recent declaration extended the PHE through October 18, 2021, however; the Biden administration has indicated it will continue to renew the PHE through the end of 2021 and that states will receive 60 days’ notice prior to its expiration or termination.
The unprecedented nature of the COVID-19 pandemic resulted in wide adoption by states of available Medicaid emergency authorities to expand Medicaid capacity and target services, providers, and enrollees that were impacted by the coronavirus emergency. Based on our tracking between March 2020 and July 2021, all 50 states and DC received approval to make changes through Disaster-Relief state plan amendments (SPAs), Section 1135 waivers and Section 1915(c) Appendix K waivers. Additionally, twelve states received approval for changes through a Section 1115 waiver and six states made changes through regular SPAs. States adopted many policies through these existing authorities similar to previous disasters, including to connect individuals to coverage more quickly and to address needs of affected populations.
States used Medicaid emergency authorities to make changes across a number of policy areas during the COVID-19 PHE to address the effects of the emergency. We analyzed specific state actions in more detail in a series of briefs, linked below. State actions included:
- Facilitating access to Medicaid and/or CHIP coverage. As people lost jobs and income due to the COVID-19 emergency and associated economic downturn, a growing number became eligible for Medicaid. To make it easier for individuals to enroll, states made changes to expand eligibility and/or modify eligibility rules, eliminate or waive premiums, and streamline application and enrollment processes. Federal legislation also created a new optional Medicaid eligibility pathway available to all states, with 100% federal matching funds, for states to cover coronavirus testing and testing-related services for uninsured individuals. However, only about a third of states adopted this eligibility group and some states rescinded the policy later after adoption.
- Expanding LTSS eligibility and benefits. The COVID-19 pandemic had a disproportionate impact on nursing homes, congregate settings, and other LTSS providers and services. In response, states expanded eligibility criteria for seniors and people with disabilities, reduced premium and/or cost-sharing requirements for these populations, and provided new LTSS benefits to meet enrollee needs during the emergency.
- Supporting providers across service type and authority, most commonly by increasing payment rates and making retainer payments.The coronavirus pandemic resulted in financial strain for Medicaid providers. Forty-one states increased provider payment rates for state plan services through Disaster-Relief SPA or other administrative authority, 40 states did so for home and community-based services (HCBS) waiver services specifically using Appendix K, and two states received approval for Section 1115 waivers that increased payment rates for HCBS.
- Increasing beneficiary access to medications. Medicaid beneficiaries with chronic conditions faced barriers to obtaining needed medications during social distancing and stay-at-home orders. To allow beneficiaries to have more of their medication on hand and reduce the barriers to receiving medication, states relaxed restrictions on quantity limits, allowed early refills, suspended prior authorization requirements and increased the availability of mail delivery.
- Increasing access to telehealth. To increase health care accessibility and limit risk of viral exposure, states took steps to expand coverage and access to services delivered via telehealth. For example, states newly allowed certain services to be delivered via telehealth and established payment parity for these services as compared to face-to-face services. States also broadened the provider types that may provide services via telehealth, including by adding new providers and waiving licensing requirements.
Use of Medicaid emergency Section 1115 authority differed from previous emergencies. Historically, states have used Section 1115 authority to expand coverage and/or provide uncompensated care to address the direct impact of natural disasters and public health emergencies (like New York City after 9/11, Hurricane Katrina, and Flint Michigan) on state Medicaid and Children’s Health Insurance Program (CHIP) programs. In response to the COVID-19 PHE, however, CMS targeted the emergency Section 1115 waiver demonstration opportunity to HCBS flexibilities. While states initially submitted Section 1115 waivers with a broader approach, CMS approved few waivers and mostly limited the scope to authorities in the application template.
Medicaid emergency authorities related to the PHE expire at different times, but states can choose to continue some of these changes even after the PHE ends (Table 1). The PHE ends when the Secretary declares that the emergency no longer exists, or after 90 days from the last PHE extension, whichever happens first. As noted above, the Biden Administration has indicated the PHE will last at least through 2021. Policy changes such as streamlining eligibility and enrollment, adding benefits and increasing provider rates that were made through Disaster-Relief SPAs can be continued after the emergency through regular SPA authority. Similarly, states may submit 1915(c) waiver amendment requests to continue some Appendix K options (such as expanded telehealth, new services, and increased ability to pay family caregivers) after the PHE. States may also submit Section 1115 requests to continue some emergency flexibilities.
Lessons learned from Medicaid’s response to the COVID-19 PHE can inform continued pandemic response and recovery as well as future emergencies. To facilitate states’ adoption of emergency authorities during the COVID-19 PHE, the federal government issued templates, guidance documents and held state calls to communicate with states. These weekly state calls helped to provide timely guidance and to answer emerging questions as the federal government and states were moving quickly to implement new legislative provisions as well as emergency authorities designed to facilitate enrollment, access to care and reimbursement for providers. Preprint templates allowed states to quickly apply for and adopt flexibilities specifically addressed to COVID-19 challenges, especially given that states faced staffing shortages due to social distancing and illness. Once adopted, states and the federal government communicated with providers and enrollees to inform those impacted by the policy changes and to ensure that additional resources were utilized. Policy flexibilities during the COVID-19 PHE strengthened Medicaid’s ability to serve as a safety net during the pandemic and economic downturn by providing coverage to individuals who lost their jobs and supporting providers who experienced reduced income. The Biden Administration has indicated a continued focus on Medicaid as a key part of the social safety net during the COVID-19 recovery and beyond, including increasing support for HCBS services and increasing adoption of the Medicaid expansion. Going forward, understanding how the process of adopting and implementing changes during the pandemic worked and what could be improved will be important in continuing to respond to the current emergency and the Delta variant as well as future emergencies.
Looking ahead, some states had begun to unwind emergency authorities and were planning for a return to normal operations; however, they may face challenges due to rising cases as a result of the Delta variant and low vaccination rates in some areas. The Biden Administration recently updated previous guidance to states on the end of the PHE on transitioning to normal operations, allowing additional time for states to complete renewals and redeterminations once the PHE ends. States began to roll back emergency authorities and plan for normal operations beginning in late Spring and early Summer of 2021 as vaccination levels increased and cases declined. More recently, however, states are again seeing increased cases due to the Delta variant. States with areas of low vaccination rates in particular may face challenges and disruptions similar to those experienced earlier in the pandemic. If states have terminated emergency Medicaid flexibilities that increased access to coverage and care, they may have reduced ability to address the effects of the Delta variant on providers and individuals. Increased case levels due to coronavirus variants may result in the Biden Administration continuing to extend the PHE into 2022, which would also have implications for maintenance of effort requirements for states, further extending the time which they must provide continuous Medicaid coverage and keeping many emergency authorities in place longer.