State Policies for Expanding Medicaid Coverage of Community Health Worker (CHW) Services
Many states use community health worker (CHW) services to address the health needs of targeted populations, including enrollees with chronic conditions or complex behavioral or physical health needs. Services provided by CHWs may include culturally appropriate health promotion and education, assistance in accessing medical and non-medical services, translation services, care coordination, and social support. Research evidence indicates CHW interventions can be effective in reducing health disparities in communities of color and promoting health equity.1 ,2 ,3 These interventions have also been shown to be effective in improving health for individuals with a wide range of chronic conditions.4 Though few studies have focused on CHW programs serving Medicaid beneficiaries, some evidence exists that these interventions can reduce health care costs and improve outcomes.5 CHW services may also potentially play a role in helping individuals access health care in areas with provider shortages.6 In September 2022, the Biden Administration announced that it was awarding $225 million in American Rescue Plan funding to train over 13,000 CHWs, the largest ever one-time federal investment in the CHW workforce. The Consolidated Appropriations Act of 2023 also authorized $50 million annually to build CHW workforce capacity from state fiscal year (FY) 2023 through FY 2027.7 These investments represent growing interest among federal and state policymakers in the potential role of CHWs in strengthening population health.
KFF’s 22nd annual Medicaid budget survey (conducted in 2022) asked states about CHW coverage policies in place as of July 1, 2022 (the beginning FY 2023 for most states)8 and planned for FY 2023. Key findings from the survey (supplemented by other available research) include:
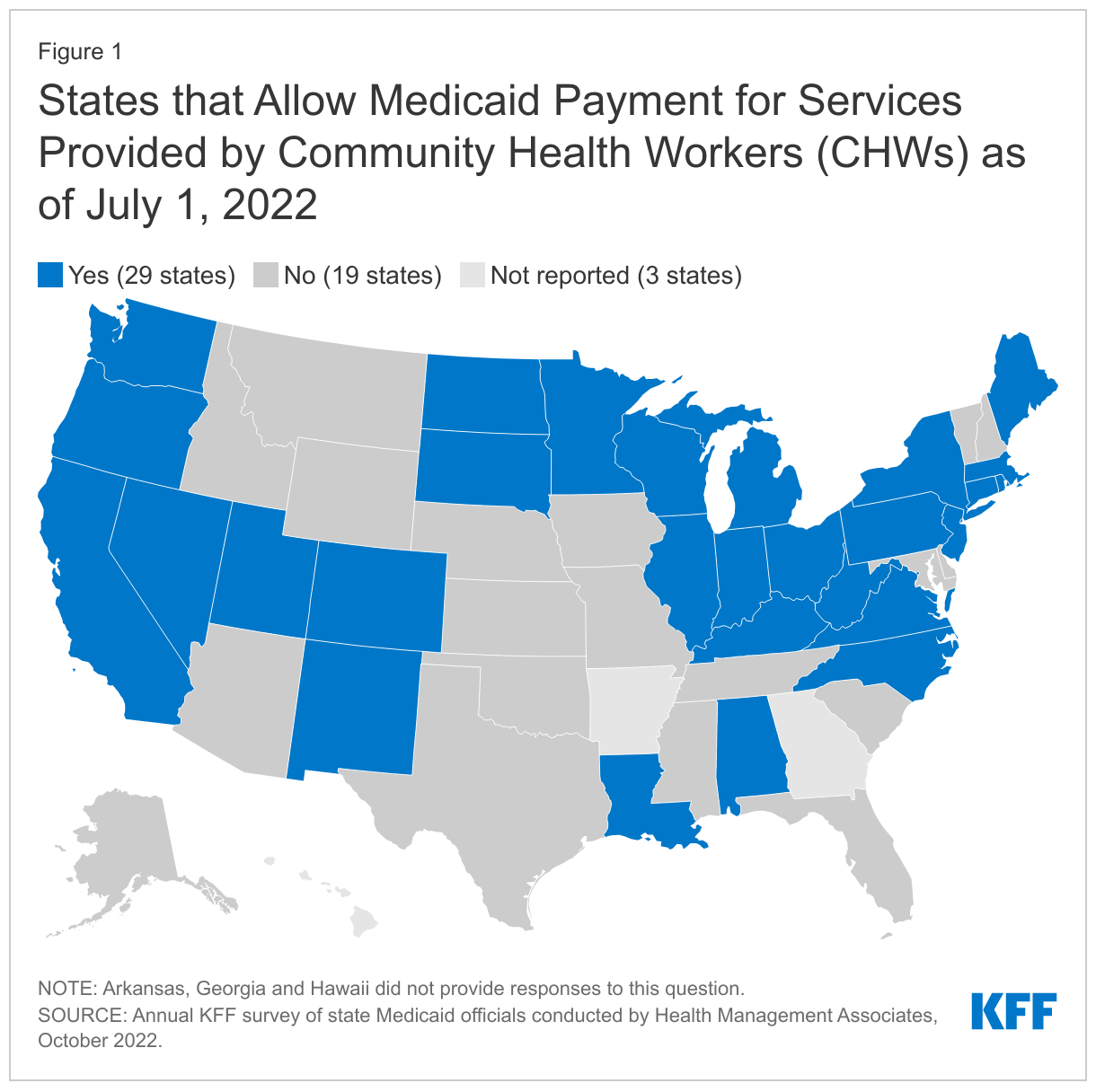
- Medicaid payment for CHW services: As of July 1, 2022, over half of responding states (29 of 48) reported allowing Medicaid payment for services provided by CHWs.9
- CHW coverage changes planned for FY 2023: A number of states reported plans to implement Medicaid coverage/payment of CHW services under state plan authority or through other coverage pathways, including under Section 1115 authority. Notably, a few states reported planning to target CHW interventions to pregnant and postpartum populations.
- Certification and training. Though the survey did not include questions about CHW certification and training programs, several states reported plans to introduce new certification and/or standardized training programs for CHWs in FY 2023.
- Efforts to expand CHW workforce. States also reported working with stakeholders to identify best practices for expanding the number of CHWs and for supporting broader acceptance of CHWs by Medicaid providers, health plans, and enrollees.
Background
Community Health Workers (CHWs) are frontline workers who have close relationships with the communities they serve, allowing them to better liaise and connect community members to health care systems.10 They often share life experiences, language, socioeconomic status, and race/ethnicity with members of the communities in which they work, allowing them to foster greater trust between community members and the health care system.11 As of May 2021, there were an estimated 61,010 CHWs working in the United States.12
CHW examples include care coordinators, community health educators, outreach and enrollment agents, patient navigators, and peer educators. Services provided by CHWs may include culturally appropriate health promotion and education, assistance in accessing medical and non-medical services, translation services, care coordination, patient advocacy, home visits, and social support.13 CHWs have also played an important role in trying to mitigate the spread of COVID-19.14 Training and certification requirements for CHWs vary widely, depending on the specific role/responsibilities and employer (e.g., community-based organizations, federally qualified health centers (FQHCs), health departments, or hospitals). No national curriculum or core training exists; however, in recent years, some states have developed standardized core competency trainings and certification requirements for CHWs.15 The move to greater standardization of the CHW role may carry some trade-offs, as some studies have found that more explicitly defining the role of CHWs and introducing certification can create new barriers to entry into the profession, undermining the grassroots nature of the workforce.16 ,17
Historically, most CHW programs have been run and funded through community health centers and other community-based organizations.18 States may authorize Medicaid payment for certain CHW services under state plan or Section 1115 demonstration authority. States may allow or require managed care organizations (MCOs) to provide CHW services or include CHWs in care teams. Many states use CHW services to address the health needs of targeted populations including enrollees with chronic conditions or complex behavioral or physical health needs, enrollees receiving targeted case management services, or frequent users of health care services.19
Findings
MEDICAID CHW SERVICE coverage approaches
States can take a variety of approaches to authorize payment for or encourage use of CHW services within Medicaid programs. State approaches to covering CHW services may be influenced by state specific factors including existing delivery systems and payment models and state policy and program goals. Primary coverage approaches and general considerations are outlined below:
- State plan coverage. States can authorize Medicaid payment for CHW services under different state plan benefits including under the preventive services benefit20 or outpatient services benefit. Requirements for authorizing coverage vary by specific state plan benefit.21 Generally, Medicaid payment is authorized for a specific set of services, provided under the supervision of a physician or licensed provider. States may also define CHW certification and training requirements.22 Federal Medicaid rules require services authorized under state plan to be available to all full benefit Medicaid beneficiaries (with certain exceptions).
- ACA Health Home option. The Medicaid health homes state plan option (created under Section 2703 of the Affordable Care Act (ACA))23 allows states to establish health homes to coordinate care for individuals with chronic conditions. States may encourage or require use of CHWs as part of a Health Homes care team. States receive a 90% federal match rate for qualified Health Home service expenditures for the first eight quarters under each Health Home state plan amendment (SPA);24 states can (and have) created more than one Health Home program to target different populations. As of September 2022, 19 states (including DC) had a total of 33 approved Medicaid health home models.
- Managed care arrangements. Some states provide CHW services through Medicaid managed care arrangements, including by adding requirements related to CHWs in MCO contracts. CHW services may be reflected in the medical component of the MCO capitation rate (e.g., if these services are specifically authorized under the state plan and the MCO is required to provide them, or if services fall under care coordination provisions25 ). MCOs may also choose to provide CHW services as “value-added” services even when they are not covered under the state plan (or factored into the capitation rate).26 As of July 2022, 41 states (including DC) contract with comprehensive, risk-based managed care plans to provide care to at least some of their Medicaid beneficiaries.
- Section 1115 demonstration waivers. Under Section 1115 waiver authority certain Medicaid requirements can be waived and states can be permitted to use federal Medicaid funds in ways that federal rules do not otherwise allow. For example, states may cover CHW services under Section 1115 demonstration authority by allowing CHWs to provide services to Medicaid certain enrollees (e.g., as part of a pilot program), through authorizing incentive payments for CHW-related activities, or by providing funding for CHW infrastructure. Alternative delivery system models requiring team-based care may also allow for more flexibility in paying for CHW services. CHW provisions may be part of broader (and often complex) state Section 1115 waivers which usually involve a lengthy approval (and negotiation) process with the Centers for Medicare and Medicaid Services (CMS). Section 1115 waivers are generally approved for five years and are subject to transparency, public notice, evaluation, and other federal requirements.
As of July 1, 2022, over half of responding states (29 of 48) reported allowing Medicaid payment for services provided by CHWs (Figure 1).27 ,28 Coverage approaches vary and may include payment authorized under state plan, CHWs included as part of a Health Home program care team, CHWs included as members of interdisciplinary teams or networks under a Section 1115 demonstration waiver, or CHW services provided by MCOs.29
CHW COVERAGE UNDER STATE PLAN AUTHORITY
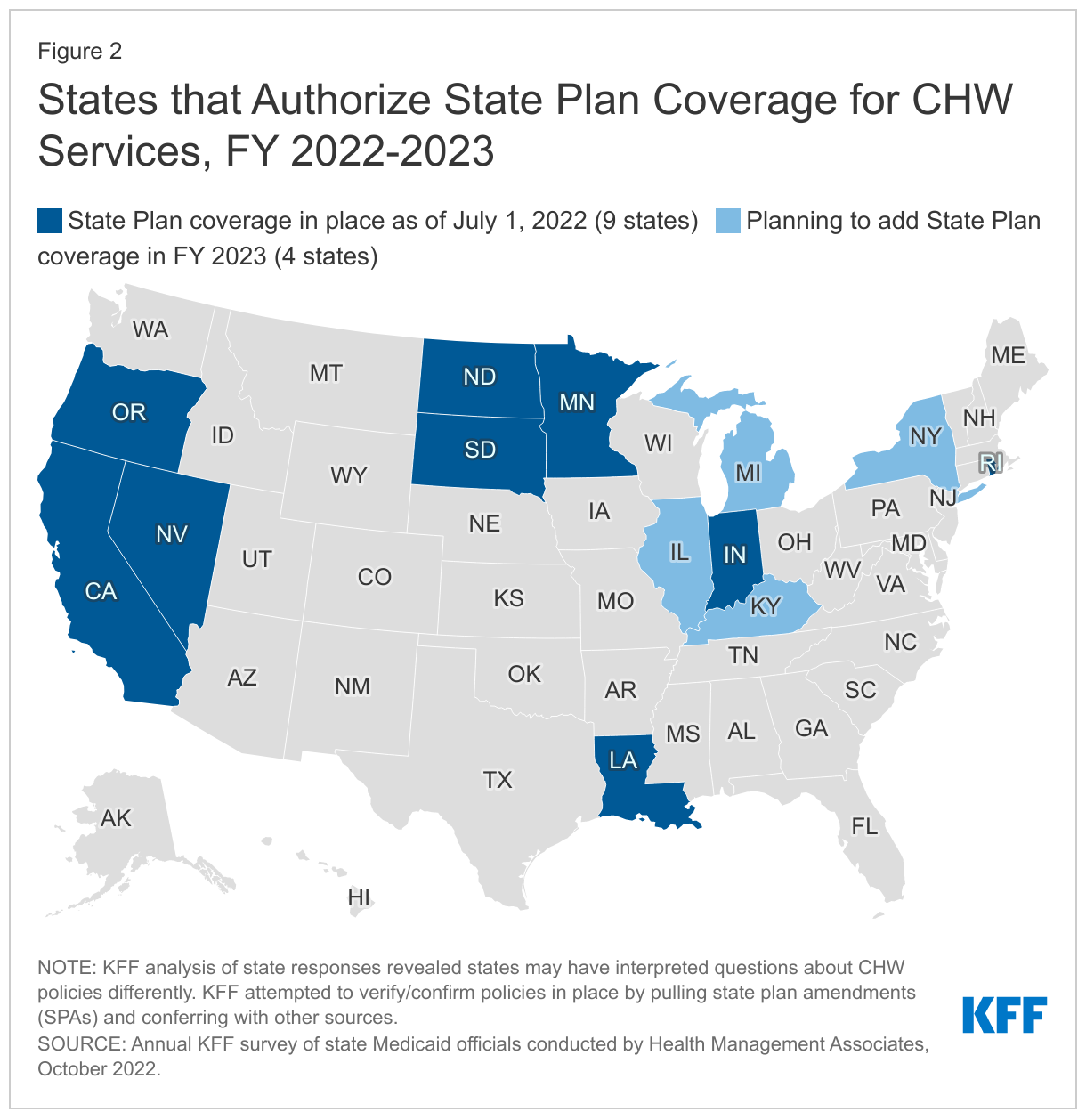
Nine states (California, Indiana, Louisiana, Minnesota, North Dakota, Nevada,30 Oregon, Rhode Island, and South Dakota) reported payment is authorized under the Medicaid state plan for a specific set of services provided by CHWs as of July 1, 2022.31 , 32 ,33 , 34 This includes four states (California, Louisiana, Nevada, and Rhode Island) that implemented coverage in 2022 (FY 2022 or the beginning of FY 2023). Four additional states (Illinois, Kentucky, Michigan, and New York) reported plans to implement coverage of CHW services under state plan authority in FY 2023.
The table below summarizes features of a few recently implemented CHW state plan amendments.
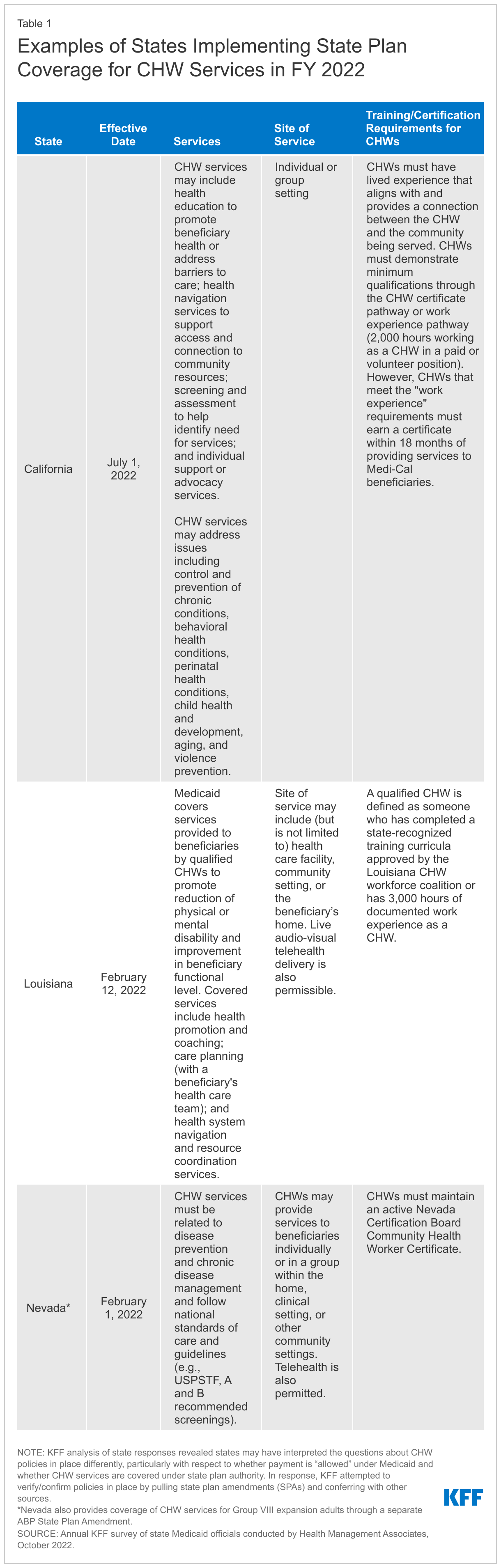
At least four additional states reported plans to implement Medicaid coverage/payment of CHW services under state plan authority (as a covered benefit) in FY 2023, including:
- In Illinois, CHWs are currently funded through Medicaid MCO administrative dollars and through the Healthcare Transformation Collaborative. Medicaid MCOs may employ CHWs or pay for CHW services with administrative dollars. Healthcare Transformation Collaboratives are provider-led collaboratives focused on innovative and equity-focused solutions to reimagine healthcare in Illinois; many have incorporated CHWs in their proposals. The state is working to add certified CHWs as a Medicaid provider type and covered Medicaid service through a state plan amendment; this will allow CHWs to bill Medicaid directly and be reimbursed for services. A CHW certification is under development.
- Kentucky currently has a CHW program funded with state dollars. It is a collaboration between the Department for Public Health and the University of Kentucky. State legislation was passed in the 2022 Kentucky legislative session mandating that the Department for Medicaid Services reimburse for CHWs and work with other stakeholders to create a public/private partnership that expands CHWs throughout the state. The Department is currently working with stakeholders to identify best practices and reimbursement models to expand the CHW footprint in 2023.
- Michigan Medicaid has developed and enhanced contract requirements for MCOs relative to the provision of CHW services, while direct reimbursement mechanisms have not (to date) been defined or implemented through program policy. MCOs have been required to ensure they meet the contractually defined ratio of CHWs to members which has evolved from a volume ratio of 1:20,000 to 1:5,000 over time. In FY 2023, Michigan will be exploring opportunities to leverage learnings from the CHW services through MCOs and identifying appropriate policy, coverage, and reimbursement methodology to support broader acceptance and use of CHWs across all managed care programs and fee-for service. The state reported plans to add CHW services as a covered benefit in FY 2023.
- New York will seek a state plan amendment to add coverage of CHWs for pregnant and postpartum individuals in 2023.
CHW COVERAGE INITIATIVES under DEMONSTRATION AND Other authorities
Several states reported other CHW coverage initiatives planned for FY 2023 including under Section 1115 demonstration authority or planned as part of a CMS Center for Medicare and Medicaid Innovation (CMMI) model. Examples include:
- As part of the MassHealth Section 1115 demonstration, Massachusetts has provided delivery system reform incentive payment (DSRIP) funding to accountable care organizations (ACOs) to hire CHWs and has funded CHW core competency trainings (which align with CHW core competencies developed by the Massachusetts Department of Public Health and enable CHWs to meet one of the qualifications for CHW certification). The state has also developed and funded advanced CHW trainings in mental health, substance use disorder, and telehealth and trainings for CHW supervisors. As of July 2022, 600 health care workers had participated in the CHW core competency and CHW supervisor trainings. As part of their next Section 1115 waiver, the state has authority to sub-capitate primary care within ACO models, which will allow financing of team-based care for primary care services in a non-FFS model. These sub-capitation funds can be used to hire CHWs in support of the team-based care model. The state will also be funding additional core competency and advanced trainings in mental health, substance use disorder, and telehealth trainings for CHWs during the next waiver period.
- Maine plans to add CHWs to its maternal opioid model of care early FY 2023. This model is a Center for Medicare and Medicaid Innovation (CMMI) initiative that supports the delivery of integrated physical and behavioral health care and wrap-around services for pregnant and postpartum women with opioid use disorder and their infants. Maine’s model provides a team-based approach to care for the eligible population, currently including a perinatal provider, substance use counselor, patient navigator, nurse care manager, recovery coach, and perinatal provider.
- The New Jersey Division of Medical Assistance and Health Services (DMAHS), in partnership with the state Department of Health (DOH), have identified CHWs as a promising resource to enhance care coordination, address disparities, and improve outcomes for Medicaid beneficiaries. To support and advance this work, the state has requested expenditure authority as part of its Section 1115 renewal application to support a set of CHW pilots, to be administered by interested MCOs in collaboration with DMAHS and the NJ DOH's Colette Lamothe-Galette Community Health Worker Institute.35 (The goal of the Institute is to create a standardized community health worker training and certification program, resulting in a robust CHW workforce.) DMAHS also participates in a CHW sustainability workgroup led by DOH members from the Institute.
- North Carolina will incorporate CHWs as “care management extenders” within their “Tailored Plan” care management model. The state will launch its “Tailored Plans” on April 1, 2023, offering integrated services to enrollees with significant behavioral health needs and intellectual/developmental disabilities (I/DD). Care management extenders can support care managers in delivering care management and meeting member contact requirements.36 CHWs that have completed the NC CHW standardized core competency training meet extender qualification requirements. North Carolina Medicaid is also preparing to leverage existing contract authority with its “Standard Plans” to expand the number of CHWs used throughout its Medicaid managed care system by establishing a CHW staffing requirement ratio. The state is also considering how health plan-level requirements filter down to providers with local care management responsibilities and how to encourage community-based organization partnership and deployment of CHWs.
Looking Ahead
In this year’s 22nd annual budget survey, states reported focusing on both longstanding issues and new priorities, including new and expanded initiatives to improve equity and reduce health disparities, improve behavioral health access and supports, and address workforce challenges. Many states also reported new and expanded benefits related to enrollees’ social needs. Research indicates community health workers can play a role in reducing racial and ethnic health disparities and addressing health-related social needs among Medicaid beneficiaries. CHWs may also potentially play a role in helping individuals access health care in areas with provider shortages.37 As states look to expand the use of CHWs in the future, evidence from recently implemented and existing CHW programs and from the infusion of ARPA and other federal funds to increase CHW workforce capacity may provide important experience and lessons to inform these efforts.
- Chidinma A. Ibe, Debra Hickman and Lisa A. Cooper, “To Advance Health Equity During COVID-19 and Beyond, Elevate and Support Community Health Workers,” JAMA Health Forum 2, no.7 (July 2021), https://doi.org/10.1001/jamahealthforum.2021.2724. ↩︎
- Sonia Ahmed, et al. “Community health workers and health equity in low- and middle-income countries: systematic review and recommendations for policy and practice,” International Journal for Equity in Health 21, no. 49 (April 2022), https://doi.org/10.1186/s12939-021-01615-y. ↩︎
- Miya L. Barnett, et al. “Mobilizing Community Health Workers to Address Mental Health Disparities for Underserved Populations: A Systematic Review” Administration and Policy in Mental Health and Mental Health Services Research 45, (July 2017), https://doi.org/10.1007/s10488-017-0815-0. ↩︎
- Richard Crespo et al. “An Emerging Model for Community Health Worker–Based Chronic Care Management for Patients With High Health Care Costs in Rural Appalachia.” Preventing Chronic Disease 17 (February 2020), http://dx.doi.org/10.5888/pcd17.190316. ↩︎
- Erica T. Marshall, et al, “Home Visits for Children With Asthma Reduce Medicaid Costs.” Preventing Chronic Disease 17 (February 2020), http://dx.doi.org/10.5888/pcd17.190288. ↩︎
- Tanekwah Hinds, Community Health Workers Bridge the Gap for Providers and Communities. (Community Catalyst, April 2022), https://www.communitycatalyst.org/blog/community-health-workers-bridge-the-gap-for-providers-and-communities#.Y5N4uvfMI2w. ↩︎
- Consolidated Appropriations Act, 2023 (P.L. 117-328). ↩︎
- State fiscal years begin on July 1 except for these states: New York on April 1; Texas on September 1; Alabama, District of Columbia, and Michigan on October 1. ↩︎
- States were asked, “As of July 1, 2022, does your state allow for Medicaid payment for services provided by a CHW – i.e., an individual who serves as a liaison between the community and health care and social services including, for example, promotoras, care coordinators, community health educators, outreach and enrollment agents, patient navigators, etc. (but excluding doulas and peer educators)?” ↩︎
- Community Health Workers (American Public Health Association), https://www.apha.org/apha-communities/member-sections/community-health-workers ↩︎
- Role of Community Health Workers (National Heart, Lung and Blood Institute, June 2014), https://www.nhlbi.nih.gov/health/educational/healthdisp/role-of-community-health-workers.htm. ↩︎
- Occupational Employment and Wage Statistics, May 2021 (U.S. Bureau of Labor Statistics, May 2021), https://www.bls.gov/oes/current/oes211094.htm. ↩︎
- Role of Community Health Workers (National Heart, Lung and Blood Institute, June 2014), https://www.nhlbi.nih.gov/health/educational/healthdisp/role-of-community-health-workers.htm. ↩︎
- Elinor Higgins, States Engage Community Health Workers to Combat COVID-19 and Health Inequities (National Academy for State Health Policy, June 2020), https://www.nashp.org/states-engagecommunity-health-workers-to-combat-covid-19-and-health-inequities/ ↩︎
- Statewide Training Approaches for Community Health Workers (National Association of Community Health Workers, August 2021), https://nachw.org/wp-content/uploads/2021/09/8.25.21StatewideTraining.pdf. ↩︎
- Theresa H. Mason, Carl H. Rush and Meredith K. Sugarman, Statewide Training Approaches for Community Health Workers. (National Association of Community Health Workers, August 2021), https://nachw.org/wp-content/uploads/2021/09/8.25.21StatewideTraining.pdf. ↩︎
- Megan Coffinbargar, April J. Damian and John M. Westfall, “Risks and Benefits to Community Health Worker Certification.” Health Affairs Forefront (July 2022), doi: 10.1377/forefront.20220705.856203. ↩︎
- Medicaid Coverage of Community Health Worker Services (Medicaid and CHIP Payment and Access Commission, April 2022), https://www.macpac.gov/wp-content/uploads/2022/04/Medicaid-coverage-of-community-health-worker-services-1.pdf. ↩︎
- Ibid. ↩︎
- A 2014 update to the Center for Medicare and Medicaid Services’ (CMS) regulatory definition of preventive services allows these services to be provided by non-licensed providers, including CHWs. ↩︎
- For example, to add coverage under the preventive services benefit, states need to submit a state plan amendment (SPA) that describes the specific CHW services to be delivered, qualifications for practitioners who will deliver the services, limitations on services, and payment methodology. For CHW services covered under the outpatient hospital services benefit, states are not required to identify these services in the state plan. https://www.macpac.gov/wp-content/uploads/2022/04/Medicaid-coverage-of-community-health-worker-services-1.pdf ↩︎
- Medicaid Coverage of Community Health Worker Services (Medicaid and CHIP Payment and Access Commission, April 2022), https://www.macpac.gov/wp-content/uploads/2022/04/Medicaid-coverage-of-community-health-worker-services-1.pdf. ↩︎
- ACA, P.L. 111-148, as amended ↩︎
- For substance use disorder (SUD) Health Homes approved on or after October 1, 2018, the SUPPORT Act extends the enhanced federal match rate from eight to ten quarters. ↩︎
- 42 CFR § 438.208(b)(2) ↩︎
- Medicaid Coverage of Community Health Worker Services (Medicaid and CHIP Payment and Access Commission, April 2022), https://www.macpac.gov/wp-content/uploads/2022/04/Medicaid-coverage-of-community-health-worker-services-1.pdf. ↩︎
- States were asked, “As of July 1, 2022, does your state allow for Medicaid payment for services provided by a CHW – i.e., an individual who serves as a liaison between the community and health care and social services including, for example, promotoras, care coordinators, community health educators, outreach and enrollment agents, patient navigators, etc. (but excluding doulas and peer educators)?” ↩︎
- KFF analysis of state responses revealed states may have interpreted questions about CHW policies differently. KFF attempted to verify/confirm policies in place by pulling state plan amendments (SPAs) and conferring with other sources. ↩︎
- KFF count of states that “allow Medicaid payment” for CHW services may differ from and include more states than reported by other sources, as KFF broadly defined related Medicaid CHW coverage approaches to include coverage under Medicaid state plan authority (see EN 31 below), CHWs as part of a Health Home program care team (allowed or required by state), CHWs included as members of interdisciplinary team or network under Section 1115 waiver (allowed or required by state), and CHW services provided by MCOs (allowed or required by state). KFF count may include states that allow MCOs to provide CHW services using administrative funds or as “value-added” services. ↩︎
- Nevada also provides coverage of CHW services for Group VIII expansion adults through a separate ABP State Plan Amendment. ↩︎
- States were asked “As of July 1, 2022, is payment authorized under the State Plan for a specific set of services provided by CHWs under the supervision of, or recommended by, a physician or other licensed provider?” ↩︎
- Alaska provides state plan coverage for Community Health Aides/Practitioners (CHA/Ps) but the state confirmed CHA/Ps are service providers, not public health workers and do not fit the definition of CHW established by the APHA. However, Alaska may be counted as a state that allows payment for CHW services in other sources. ↩︎
- KFF analysis of state responses revealed states may have interpreted questions about CHW policies differently. KFF attempted to verify/confirm policies in place by pulling state plan amendments (SPAs) and conferring with other sources. ↩︎
- Several states reported that they authorize payment under the state plan for a specific set of services provided by CHWs but are not reflected in our count / here. These states were excluded because we were unable to identify/locate the corresponding state plan amendment. These states may have been referencing coverage under the ACA Health Homes state plan option. States that were excluded from the state plan authority count were not reported by other sources as reimbursing for CHW services under state plan authority. ↩︎
- Colette Lamothe-Galette Community Healthworker Institute (State of New Jersey Department of Health), https://www.nj.gov/health/fhs/clgi. ↩︎
- Tailored plan members have access to a dedicated care manager who will work with a multidisciplinary team to deliver integrated, whole-person care. ↩︎
- Tanekwah Hinds, Community Health Workers Bridge the Gap for Providers and Communities. (Community Catalyst, April 2022), https://www.communitycatalyst.org/blog/community-health-workers-bridge-the-gap-for-providers-and-communities#.Y5N4uvfMI2w. ↩︎