Medicaid Coverage of Behavioral Health Services in 2022: Findings from a Survey of State Medicaid Programs
Medicaid plays a key role in covering and financing care for people with behavioral health conditions. Nearly 40% of the nonelderly adult Medicaid population (13.9 million enrollees) had a mental health or substance use disorder (SUD) in 2020. Most enrollees with behavioral health conditions qualify for Medicaid because of their low incomes. Behavioral health services are not a specifically defined category of Medicaid benefits: some may fall under mandatory Medicaid benefit categories (e.g., psychiatrist services may be covered under the “physician services” category), and states may also cover behavioral health benefits through optional benefit categories (e.g., case management services, prescription drugs, and rehabilitative services). Behavioral health services for children are particularly comprehensive due to Medicaid’s EPSDT benefit for children: children diagnosed with behavioral health conditions receive any service available under federal Medicaid law necessary to correct or ameliorate the condition. However, the same is not required for adults.
To better understand the variation in access to behavioral health services for adults in Medicaid, KFF surveyed state Medicaid officials about behavioral health benefits covered for adult enrollees in their fee-for-service (FFS) programs. These questions were part of KFF’s Behavioral Health Survey of state Medicaid programs, fielded as a supplement to the 22nd annual budget survey of Medicaid officials conducted by KFF and Health Management Associates (HMA). A total of 45 states (including the District of Columbia) responded to the behavioral health benefits survey. This issue brief uses the survey data to describe the landscape of behavioral health service coverage across states, including themes across and within service categories. Additional state-by-state detail is available in KFF’s Medicaid Behavioral Health Services data collection. Further policy context is available in a series of behavioral health briefs that can be accessed in the “Behavioral Health Supplemental Survey” section on this page.
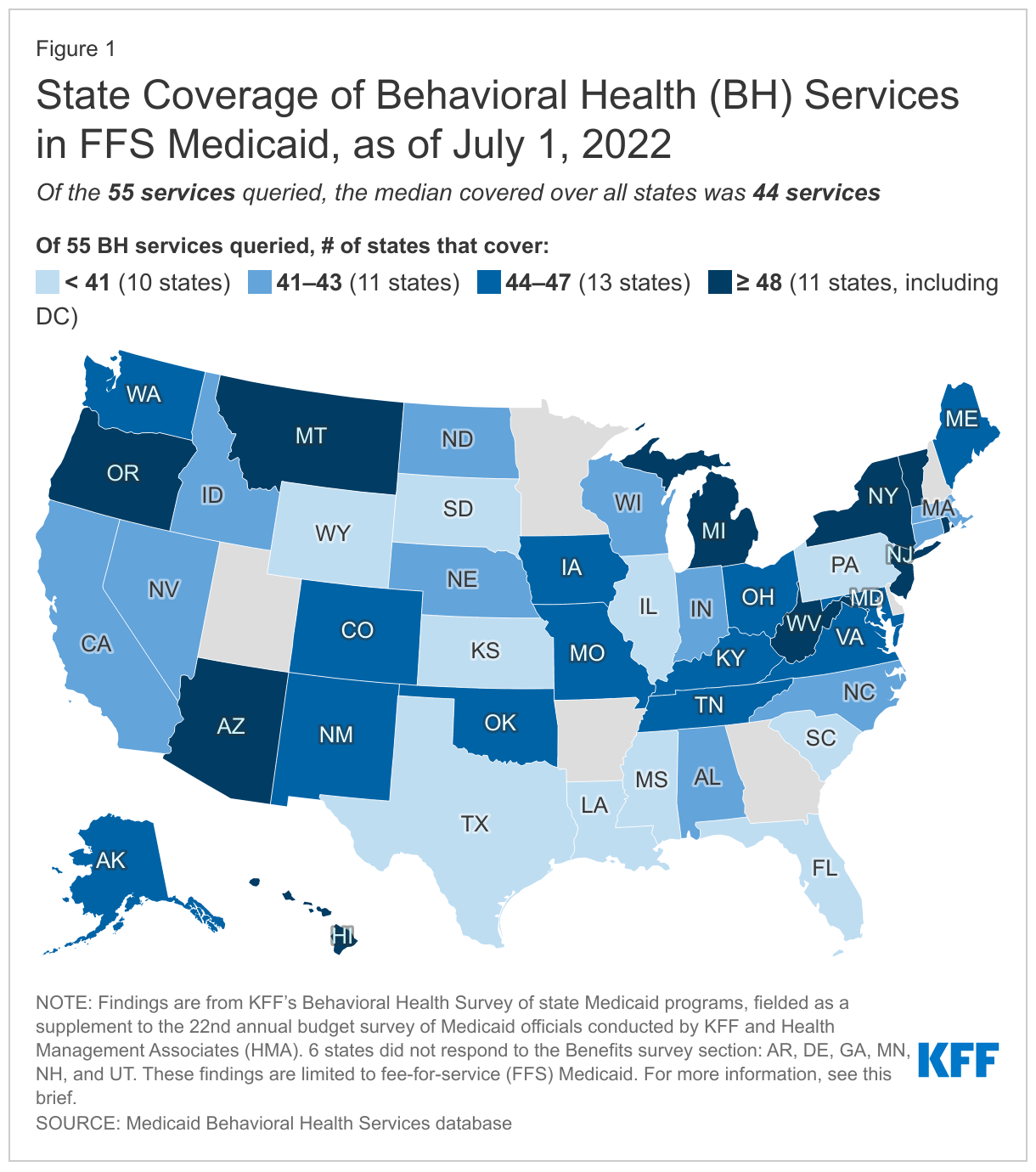
Medicaid coverage of behavioral health services varied moderately across states, with the median number of covered services at 44 of the 55 services queried (Figure 1). We provided state Medicaid officials with a list of 55 behavioral health benefits and asked them to indicate which were covered under their FFS Medicaid programs for adults, as of July 1, 2022 (for more information on survey methods, see Appendix A). We grouped the benefits queried by service category: institutional care/intensive, outpatient, SUD, naloxone (without prior authorization), crisis, integrated care, and other services. Notably, all but one state (SC) reported coverage of at least half of all services queried, with a median coverage rate of four-fifths of all services (44 of 55). These high rates of coverage reflect state trends in recent years to expand Medicaid services across the behavioral health care continuum—however, coverage of services may not translate into access to care, particularly given workforce shortages that make accessibility a challenge for Medicaid enrollees (as well as people with private insurance). We also asked states that reported coverage of each service to indicate any copay requirements as well as notable limits on the services (such as day limits or other utilization controls, including prior authorization requirements).1 Across services, most states reported no copay requirements, but limits were more common.
These findings are limited to FFS Medicaid and do not comprehensively capture variation in coverage for managed care organizations (MCOs) or Section 1115 waivers. Within each service category, we asked states to note differences in coverage for populations receiving services from MCOs or through Section 1115 waivers. Most states continue to rely on MCOs to deliver inpatient and outpatient behavioral health services, and these MCOs may offer services to their adult enrollees that differ from those available on a FFS basis. States also may use Section 1115 waivers to operate their Medicaid programs in ways that differ from what is required by federal statute; these can include “comprehensive” waivers that make broad changes in Medicaid benefits and other program rules or more targeted demonstrations. For state-specific information on behavioral health benefit coverage variation in MCOs or Section 1115 waivers as reported by states, see footnotes on indicators in the data collection. See also Appendix A for a summary of survey methods.
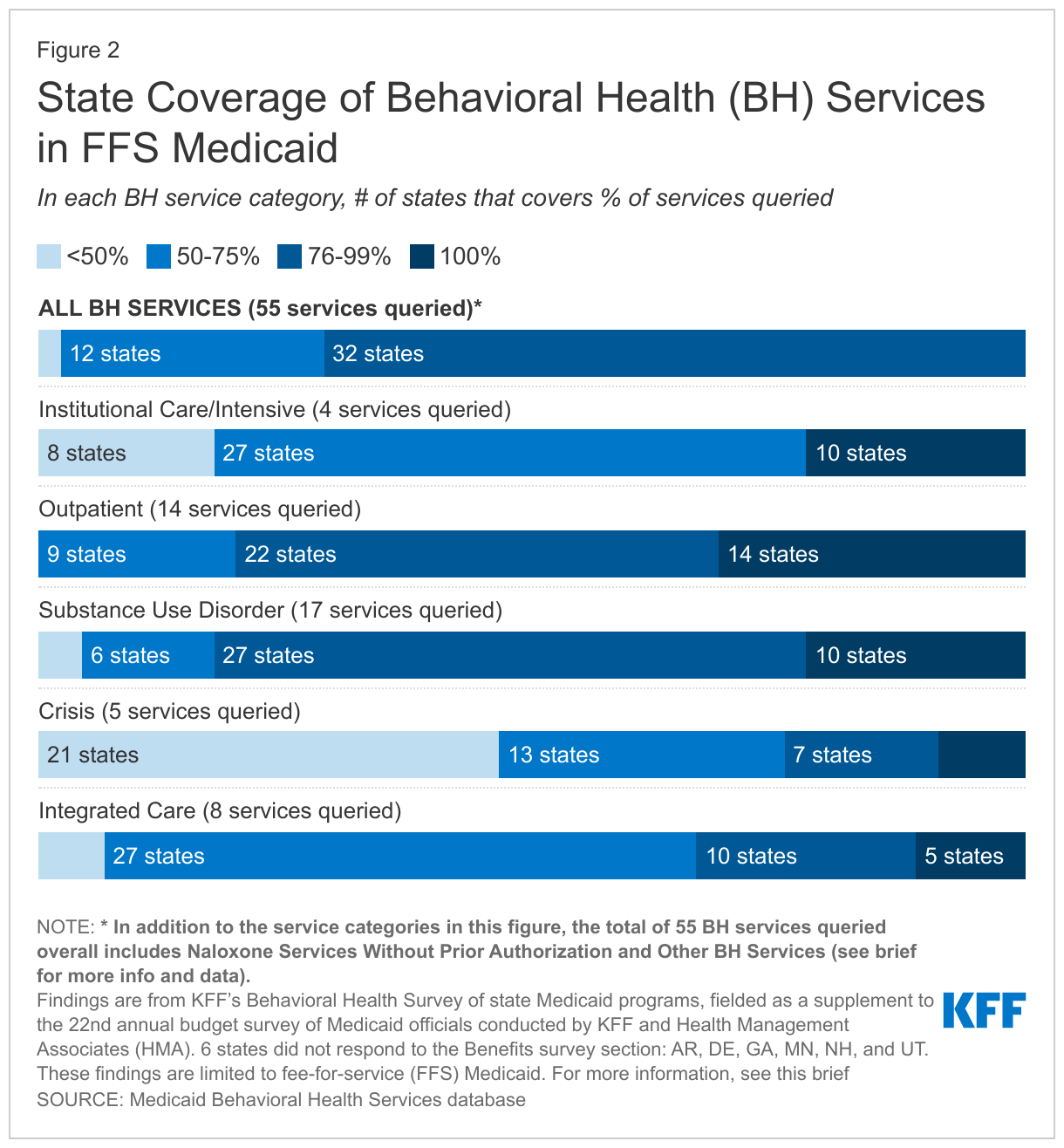
Across responding states, coverage rates were highest for SUD and outpatient services and lowest for crisis services (Figure 2). As indicated in Figure 2, for each service category, the majority of responding states covered more than 50% of the services queried, with at least a few states reporting coverage of 100% of services queried. Some states reported high coverage rates across service categories, including six states that cover more than 90% of all services queried: NY, AZ, OR, MI, NJ, and WV. Each of these states cover all services in multiple of the categories: for example, MI and OR each cover 100% of the services queried in the institutional, outpatient, SUD, and integrated care categories.2
Additional detail on definitions of and trends within each service category, including copays and limits, is included in the bullets below. For a detailed table showing the number of states with coverage of each individual benefit, see Appendix B.
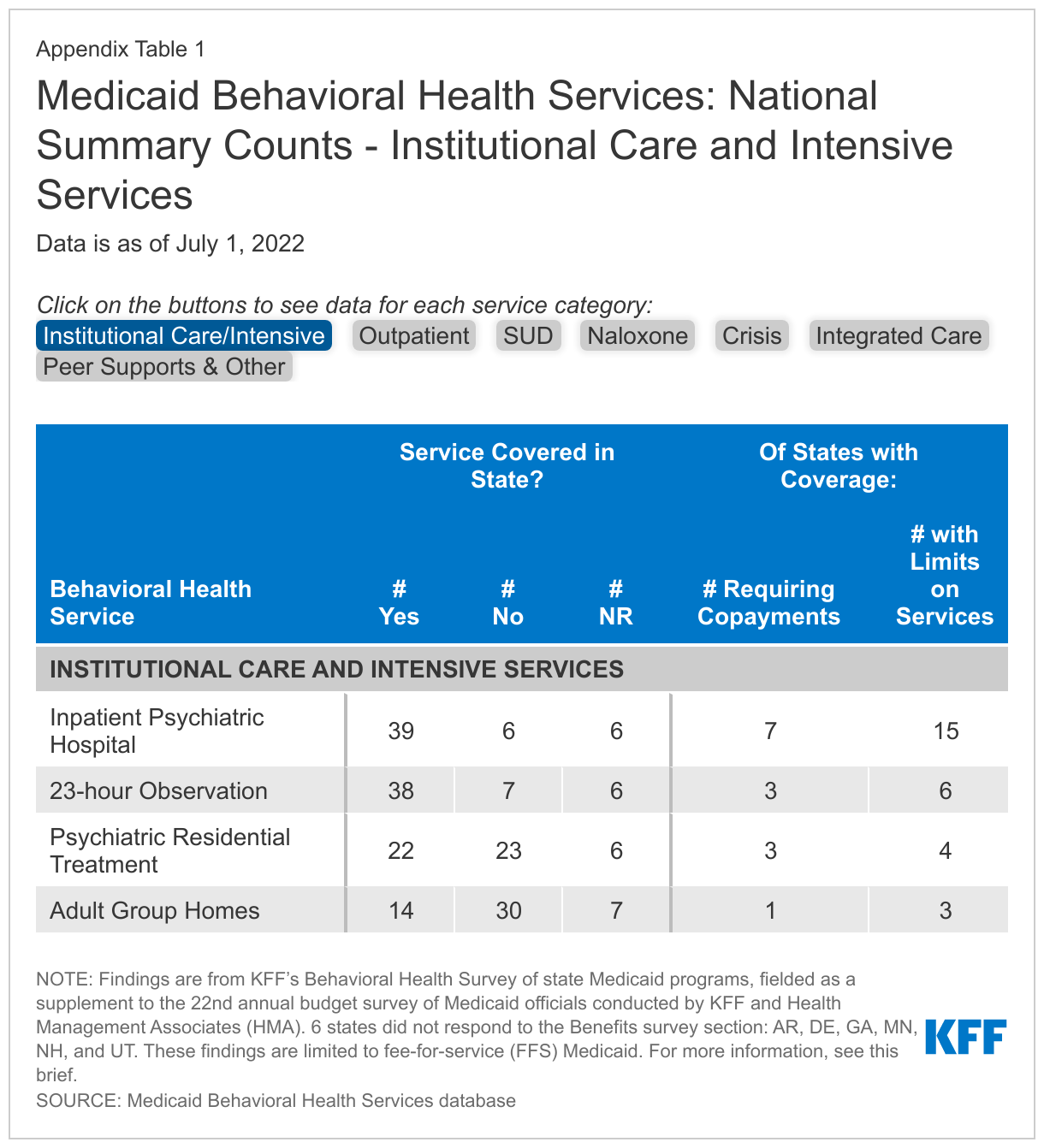
- Institutional care and intensive services are typically reserved for situations that require a higher level of care and monitoring, such as behavioral health emergencies or long-term treatment for those with ongoing needs. Although a large majority of responding states report coverage of inpatient psychiatric hospital services and 23-hour observation, fewer than half of states report coverage of psychiatric residential treatment and adult group homes. Within this category, limits and copays are most common for psychiatric inpatient care, with more than one-third of covering states reporting limits and nearly one-fifth reporting copays. In states without Section 1115 waivers of the IMD payment exclusion, the number of psychiatric or residential care facilities that accept Medicaid may be restricted.
- Outpatient services include a wide range of psychiatric services provided in outpatient settings. Services in this category range from psychiatric testing—which may be used to inform diagnosis of mental health conditions—to more intensive services, like partial hospitalization services—a more intensive treatment that occurs multiple times a week on an outpatient basis. While all or nearly all states cover evaluation and testing services as well as individual, family, and group therapy, there is more variation in coverage of ADL/Skills training, case management, and day treatment services. Within this category, states were most likely to report limits for case management and copays for therapy (individual, family, or group).
- Services to treat SUD were queried in categories that follow the level of care criteria from the American Society of Addiction Medicine (ASAM), ranging from early intervention to more intensive services, such as medically monitored intensive inpatient services (which may be subject to the IMD exclusion). Most states reported the highest coverage rates for SUD services compared to the other categories, likely bolstered by provisions in the SUPPORT Act. Within this category, nearly all states cover outpatient SUD treatment, while states were least likely to cover clinically managed high intensity residential services. As services grow in intensity, the number of states placing limits on the service also increases. Also within this service category, all or nearly all states reported coverage of medications for SUD treatment, including buprenorphine, naltrexone, and methadone. About one-third of states report limits for buprenorphine, but fewer limits are reported for naltrexone, which is not a controlled substance. For most SUD medications, about one-quarter of states report copay requirements (whereas fewer states report copays for services across the ASAM levels).
- We also asked states to report coverage of naloxone (without prior authorization requirements), which is used to reverse an opioid overdose and is prescribed to people with opioid use disorder, but may be available over the counter in the future. Nearly all states cover at least one formulation of naloxone without a prior authorization. A handful of states place other limits on these prescriptions and fewer than one-third of states require copays. (Data for this service category is not shown in Figure 2, but can be found in Appendix B.)
- Crisis services provide specialized responses to enrollees experiencing behavioral health emergencies. These services aim to reduce the reliance on law enforcement professionals, emergency departments, and other organizations staffed by people who are not behavioral health professionals. States were less likely to cover crisis services compared to other categories: for most states, crisis services was the category for which the state reported the lowest coverage rate, including several states that reported covering none of the crisis services queried. In contrast, four states (AZ, NM, NY, and TN) reported covering every crisis service queried. The wide range of coverage across states may reflect the emerging nature of crisis management in behavioral health. Within this category, states most frequently covered mobile crisis services (about three-quarters of responding states). This relatively higher coverage rate could be in part connected to the American Rescue Plan Act’sprovision of a new option and enhanced funding for states to provide community-based mobile crisis intervention services.
- Integrated care services provide behavioral health care in conjunction with physical health care. Examples include mental health screening in primary care settings and psychiatric evaluation with medical services. Traditionally, physical and behavioral health services have been delivered separately, but a growing body of evidence supports their integration. Coverage of services in this category varies; collaborative care model services are covered least frequently and psychiatric evaluations with medical services, as well as Medicaid individual/family counseling, are covered most often. For most integrated care services, few states reported copays, and limits were somewhat more common (fewer than one-fifth of states).
We also asked states to report coverage of a few additional behavioral health benefits in an “other” category. For example, more than four-fifths of responding states cover peer support services, which are provided by individuals who have personally experienced behavioral health challenges. These professionals may help enrollees with emotional support or navigation of health care or other social services. Peer supports has been identified as one method that states are using to extend the Medicaid behavioral health workforce.
Looking ahead, states may continue the trend of expanding Medicaid behavioral health benefits and may also enhance access to behavioral health care through other programs or policies. Since FY 2016, behavioral health benefits have been the most frequent category of service expansions reported on KFF’s annual Medicaid budget survey. For example, in FY 2022 and/or FY 2023, a number of states reported expanding coverage of crisis services and/or of services aimed to improve the integration of physical and behavioral health care. As access to behavioral health care is a key Medicaid priority at both the state and federal levels, these trends are likely to continue into the future. Notably, comprehensive coverage of behavioral health services has been linked to higher Medicaid acceptance rates by providers. In addition to further expanding coverage of behavioral health services, states may take additional policy actions to increase access and improve outcomes for enrollees with behavioral health conditions. For example, states may pursue initiatives to address behavioral health workforce shortages, such as by adopting permanent expansions of behavioral health telehealth policy to facilitate access to care. State Medicaid agencies may also play a role in developing, implementing, and helping to fund a statewide crisis system, including 988 crisis hotline services. KFF surveyed states on these and other behavioral health policies, with the results to be published in a series of briefs that can be accessed in the “Behavioral Health Supplemental Survey” section on this page. Finally, in addition to state Medicaid policy, federal legislation could continue to shape the behavioral health landscape for Medicaid enrollees.
This work was supported in part by Well Being Trust. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
This brief draws on work done under contract with Health Management Associates (HMA) consultants Angela Bergefurd, Gina Eckart, Kathleen Gifford, Roxanne Kennedy, Gina Lasky, and Lauren Niles.
Appendix A: Methodology
KFF contracted with Health Management Associates (HMA) to survey Medicaid directors in all 50 states and the District of Columbia to identify those behavioral health services covered for adult beneficiaries in their programs. The survey instrument captured information about services covered, copay requirements, and notable limits on those services as of July 1, 2022. The survey data is summarized in this brief and published on a state-by-state basis in KFF’s Medicaid Behavioral Health Services data collection. This data reflects what the states reported on the survey; responses vary in level of detail and were not verified through another source.
The survey asked states to report coverage of services in their fee-for-service (FFS) programs for categorically needy (CN) traditional Medicaid adults ages 21 and older. The survey did not ask about service coverage for medically needy (MN) coverage groups, which may differ from the state’s CN benefit package. Children were excluded from the survey because all children under age 21 enrolled in Medicaid through the categorically needy pathway are entitled to the Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) benefit, which requires states to cover all screening services for children as well as any services “necessary… to correct or ameliorate” a child’s physical or mental health condition (regardless of whether the service is covered for adults). All but six states (AR, DE, GA, MN, NH, UT) submitted survey responses, though in some instances a responding state may have left a particular service row blank. The territories are not included in the data.
We provided states with a list of 55 optional Medicaid behavioral health services. For each service, the state selected from a yes/no dropdown menu on the survey to indicate whether the service was covered. The list of behavioral health services included in this survey was based on the services queried by KFF in a similar 2018 survey; the 2018 data is available in the data collection. While we have posted data for both years, the data should not be compared across years as a trend due to changes in question phrasing over time.
Note that while this survey focused on coverage in FFS, most states continue to rely on MCOs to deliver inpatient and outpatient behavioral health services, and these MCOs may offer services to their adult enrollees that differ from those available on a FFS basis. States had an opportunity on the survey to note differences in required minimum benefits for MCOs, as well as differences in benefit coverage under Alternative Benefit Plans (benefit plans that Medicaid expansion states are required to design, in line with federal guidelines, for newly eligible ACA expansion adults) or Section 1115 waiver programs. To the extent that they were reported, these notes are included in the data collection as state-specific footnotes. However, the level of comprehensiveness of states’ responses in capturing these differences varies, and the level of information provided is likely inconsistent across states. Therefore, while the state-specific footnotes may provide useful context about coverage in an individual state, they should not be taken as a complete list of differences in benefit coverage under managed care, Alternative Benefit Plans, or Section 1115 waiver programs nationally.
Additional information on Medicaid coverage of behavioral health services is available here and here.
Appendix B: Summary Table
- Specifically, we asked states to describe any “notable limits on services or days or other utilization controls.” This question was open to state interpretation, so limits may not be consistently reported across states. ↩︎
- Also, NY covers all services in the crisis, SUD, and integrated care categories; AZ covers all services in the institutional, outpatient, crisis, and SUD categories; NJ covers all services in the institutional, outpatient, and integrated care categories; and WV covers all services in the outpatient and SUD categories. ↩︎