Obesity Rates Among Children: A Closer Look at Implications for Children Covered by Medicaid
Obesity in children is caused by a multitude of socioecological, environmental, and genetic factors and has increased in recent decades, with child obesity rates now three times higher than they were in the 1970s. Obesity is a risk factor for many chronic diseases and has been linked to future physical and mental health challenges and increased health care costs. Though obesity has historically been stigmatized as a result of personal choices, there have been recent actions to reduce that stigma and weight bias and increase obesity screening and treatment options. New FDA weight-loss drugs have entered the market, and the American Academy of Pediatrics (AAP) released a new set of clinical practice guidelines for evaluating and treating obesity in early 2023. While addressing obesity among children with all forms of insurance coverage is important, Medicaid is particularly relevant since it now covers half of children in the U.S., including 8 in 10 children living in poverty and over half of Black, Hispanic, and American Indian/Alaska Native children. Obesity prevalence is higher for these groups. This brief examines the share of children with obesity, how obesity screening and treatment is covered under Medicaid for children, and what recent changes may mean for Medicaid programs and enrollees in the future.
What is the share of children with obesity?
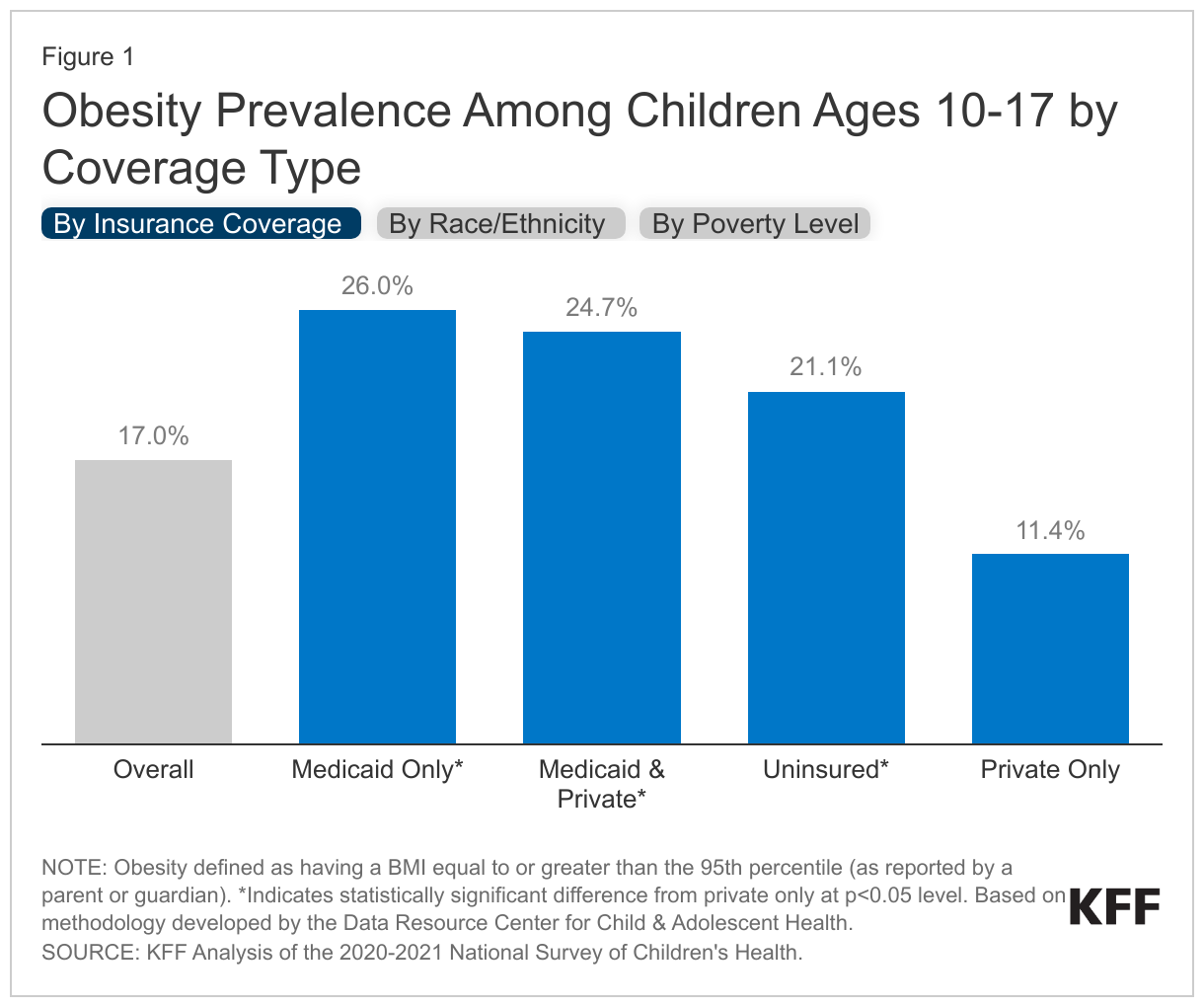
KFF analysis of federal survey data show more than one in six children have obesity, with obesity rates varying by insurance coverage type, race and ethnicity, and household income. Based on data from the 2020-2021 National Survey of Children’s Health (NSCH), 17% of children ages 10-17 in the U.S. have obesity (Figure 1). Obesity in children is typically defined as having a Body Mass Index (BMI) equal to or greater than the 95th percentile for their age and sex, although there has been recent pushback on BMI as a screening tool, and research has shown it can incorrectly classify individuals as overweight or obese, especially for people of color. Children with Medicaid are more than two times as likely to have obesity than those with private insurance: Over one-quarter (26.0%) of Medicaid children have obesity compared with 11.4% of children with private insurance alone. Obesity prevalence is also higher for Black, Hispanic, and children of other or multiple races compared with White children as well as for children with lower household incomes compared with children in the highest income households (Figure 1). These disparities in obesity reflect a variety of factors, including social and economic factors such as higher rates of food insecurity, more limited access to healthy food options, more limited time and access to opportunities for physical activity and recreation, and experiences with discrimination and stigma.
What other chronic conditions do Medicaid children with obesity have?
Children’s obesity rates in Medicaid claims data are lower than survey estimates of obesity prevalence. In 2019, 7.4% of Medicaid children ages 10-17 had an obesity diagnosis clinically identified in the Medicaid claims data (T-MSIS), suggesting that obesity in children may be undertreated. Other research has found that obesity is generally under-reported in claims data, and when it is reported, it is more likely to identify individuals with morbid obesity or comorbidities than individuals with more moderate obesity. Several factors could be contributing to low rates of reporting including the relative newness in viewing obesity as a disease, interventions being time intensive and difficult for clinicians to implement in a time limited primary care visit, or limited provider reimbursement for obesity treatment services. While there are limitations, analysis of claims data can help to identify the extent to which other chronic health conditions accompany obesity.
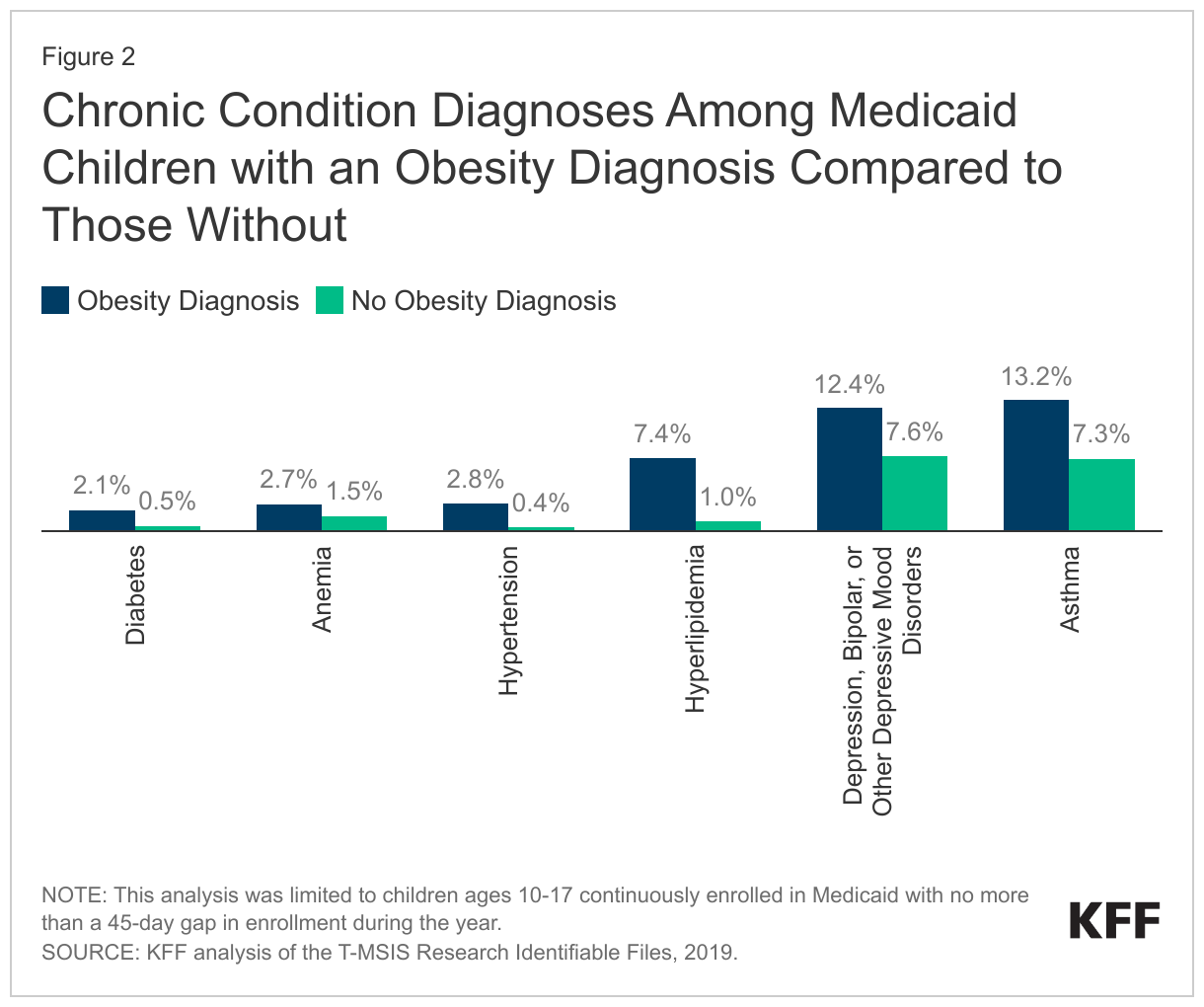
For Medicaid children ages 10-17 with an obesity diagnosis, the most common co-occurring chronic condition (across a set of 30 chronic conditions, see Methods for more information) is asthma, followed by certain mental health conditions, hyperlipidemia, anemia, hypertension, and diabetes (Figure 2). Children with obesity are also more likely to have these conditions compared with children without an obesity diagnosis. For example, 13.2% of children with an obesity diagnosis also have an asthma diagnosis compared with 7.3% of children without obesity. Similarly, 12.4% of children with an obesity diagnosis also experience mental health challenges including depression, bipolar disorder, and other depressive mood disorders compared with 7.6% of children without obesity. These findings mirror a body of research that has found a link between childhood obesity and asthma as well as various mental health challenges including depression and anxiety, lower self-esteem and increased bullying. One recent study of Medicaid expenditures also found inpatient and outpatient mental health services were a primary driver of spending among children with obesity. Overall, over one-third (35.6%) of children with an obesity diagnosis have at least one other co-occurring chronic condition (across a set of 30 chronic conditions).
What obesity treatment and services does Medicaid cover for children?
Obesity services can include screening, behavioral and nutritional counseling, anti-obesity medications, and bariatric surgery, and these services are covered for children under Medicaid’s Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) program. EPSDT is a Medicaid benefit for children under 21 that provides comprehensive treatment and preventive care. Under EPSDT, states are required to cover all screening services for children as well as any services “necessary… to correct or ameliorate” a child’s physical or mental health condition. EPSDT also allows for unique state flexibility in addressing the range of other factors connected to obesity, including providing behavioral health services and addressing adverse childhood experiences (ACEs) and social determinants of health (SDOH) such as housing, finances, and safety.
While children have access to obesity treatment though EPSDT, it is less clear how states are implementing and covering these services in practice. One old study, from 2010, only found conclusive evidence from 10 states that they were covering obesity-related behavioral and nutritional counseling services. While additional states are likely to have started covering obesity-related services since then, other research has found that some Medicaid-covered children do not receive recommended EPSDT screenings and services. Data from the 2020 Child Core Set, which includes data from participating states on children in Medicaid or the Children’s Health Insurance Program (CHIP), found a median of 73% of children ages 3 to 17 with a primary care visit had evidence of BMI screening, 63% received nutrition counseling, and 59% received physical activity counseling though these rates varied across states.
What to watch looking ahead?
While data indicate a majority of Medicaid children are being screened for obesity, it is difficult to know how many children are receiving recommended services. Research also indicates there are racial disparities in access to obesity treatments. When the Child Core Set quality measures—which include measures related to obesity— become mandatory in 2024, states and health plans will have data on rates of screening and counseling for obesity. Access to such data may prompt the states and health plans to encourage more proactive screening and treatment by pediatricians. Provisions included in recent legislation to bolster Medicaid’s EPSDT benefit may also help more Medicaid-covered children receive all recommended screenings and services, including obesity screening and counseling.
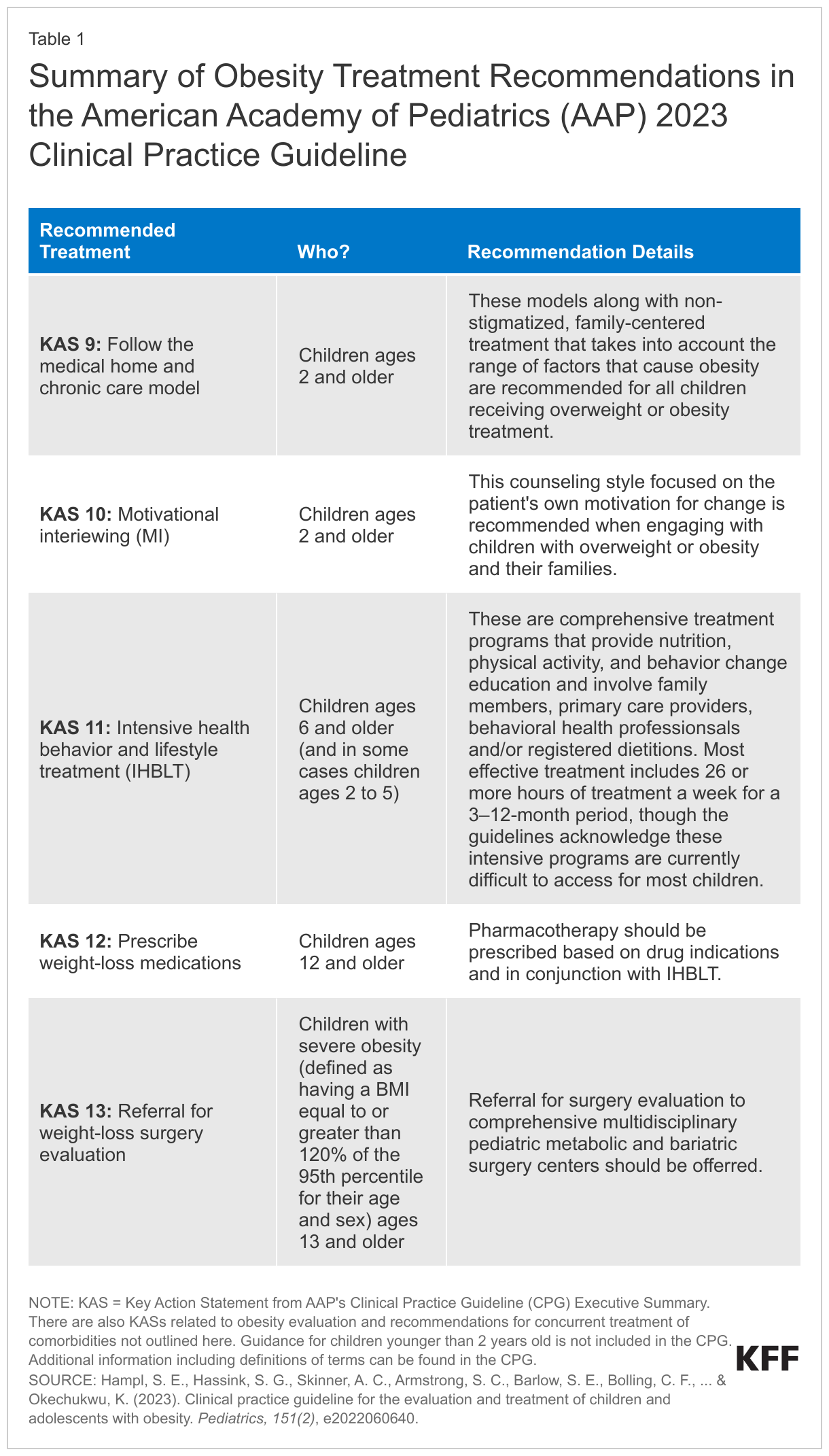
The AAP released a new set of clinical practice guidelines for evaluating and treating obesity and associated conditions in early 2023. The guidelines outline and describe evidence-based screening procedures, comorbidity evaluation and treatment for children ages 2 and older, and recommended obesity treatments (for treatment details, see Table 1). The guidelines emphasize early and intensive treatment, and note the importance of a non-stigmatized, family-centered approach that takes the range of factors that cause obesity into account. The guidelines are not mandatory, and it remains to be seen how quickly and to what extent the guidelines will be adopted by clinicians. There has been some pushback on the intensity of the new guidelines and the potential to cause eating disorders. Concerns with new medications for weight loss include some side effects and studies show people regain the weight if they stop taking the medications. Despite increasing prescribing rates of medications for adults, it is expected that providers may be slower to prescribe children anti-obesity medications .
With Medicaid now covering half of all children in the U.S., and an even larger percentage of children who are likely to be obese, changes in physicians’ practice stemming from the updated treatment recommendations could have a sizable effect on Medicaid programs and enrollees. However, the extent to which the new, more intensive treatment recommendations are considered medically necessary for children may vary by state and provider. While there is evidence that payment rates for obesity treatment, access to IHBLT, and take up of anti-obesity medications is currently limited, there could also be spending implications for Medicaid if more children begin to receive recommended obesity treatments including anti-obesity medications or bariatric surgery.
Methods
Data: This analysis used the 2019 T-MSIS Research Identifiable Files. More specifically, the analysis used the inpatient (IP), long-term care (LT), and other services (OT) claims files merged with the demographic-eligibility (DE) files from the Chronic Condition Warehouse (CCW) to include beneficiary demographic and enrollment information.
Identifying an Obesity Diagnosis: An obesity diagnosis was identified if any enrollee had any claims across the IP, LT, and OT files during the year with ICD-10 diagnosis codes within E66.0, E66.1, E66.2, E66.8, E66.9, Z68.3, Z69.4, Z68.54. This code set was based on previous KFF analysis and other sources.
Chronic Conditions: 30 chronic conditions were identified in this analysis including anemia, asthma, diabetes, depression, bipolar, or other depressive mood disorders, hypertension, and hyperlipidemia, using ICD-10 codes from the CCW Chronic Condition Algorithm. A condition was identified as present if an enrollee had any claims across the IP, LT, and OT files during the year with any of the relevant diagnosis codes listed in the CCW algorithm.
Enrollee Exclusion Criteria: This analysis was limited to children ages 10-17 continuously enrolled in Medicaid with no more than a 45-day gap in enrollment during the year. This definition of continuous enrollment was chosen to align with previous KFF analysis and CMS’ Child Set Core Measures, specifically, those around children’s preventive care, and to give people sufficient time in Medicaid to utilize services.
State Exclusion Criteria: We excluded the following states from our analysis due to concerns with the quality of their enrollment data: Florida, Kentucky, Rhode Island, and Oklahoma. Based on a previous KFF analysis, we relied on data quality assessments from the DQ Atlas to exclude states. We exclude states based on (1) Number of Enrollment Spans – % of Beneficiaries with Only One Enrollment Span in Year ≥ 99.8 (Florida, Kentucky, Rhode Island), (2) Enrollment Patterns Over Time: Number of Enrollment Spans – % Beneficiaries with 3 or More Enrollment Spans in Year ≥ 5% (Oklahoma).
At the state level, we also examined claims volume, the share of children with no health care utilization, and benchmarked the share of children with a well-child visit in 2019 to the 2019 Child Core Set measure for the percentage of children with at least 1 well-care visit with a primary care practitioner or obstetrician/gynecologist. We did not find any significant state outliers across those measures.