What are the Implications of New Anti-Obesity Drugs for Racial Disparities?
Recently medications have emerged that offer new opportunities for obesity treatment. The surge of interest in these drugs also raises questions about who can access them and the potential impacts on racial health disparities. These drugs, including Novo Nordisk’s Ozempic and Wegovy (semaglutide) and Eli Lilly’s Mounjaro (tirzepatide) were initially approved to treat type 2 diabetes, but have also been proven effective in helping people lose weight. Reductions in obesity could help reduce risks for chronic diseases associated with obesity, such as heart disease, type 2 diabetes, and types of cancer, as well as health care costs. However, these medications may not be appropriate for all patients, there are side effects associated with the medications, and studies suggest that most people regain weight if they stop taking them. Moreover, access to these medications varies and they remain unaffordable for many individuals given that they currently are excluded from Medicare coverage, coverage through Medicaid and private plans remains limited, and out-of-pocket costs without coverage can be in excess of $1,300 per month.
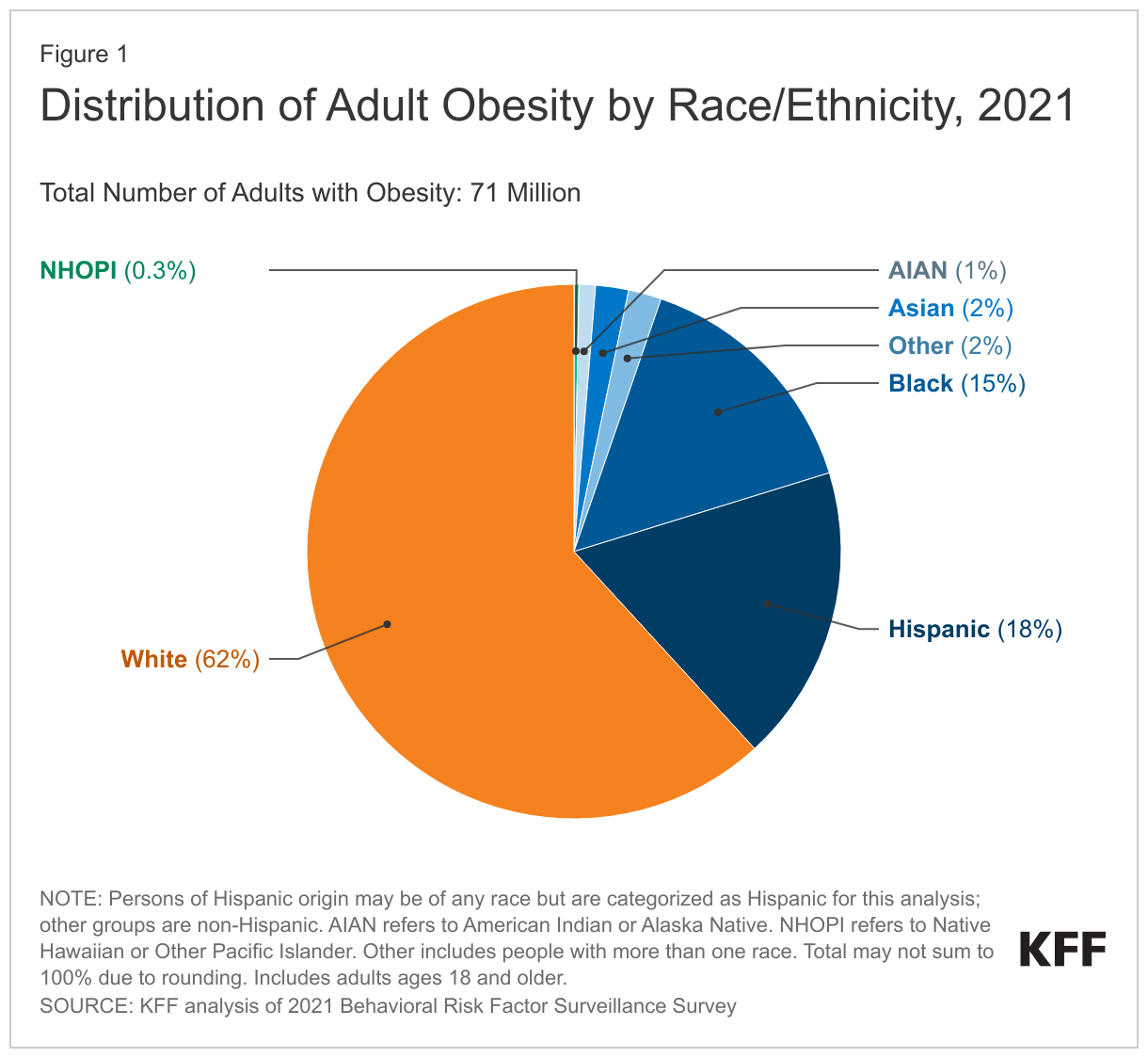
As of 2021, roughly 71 million people or one third of the total US adult population were classified as obese, that is having a body mass index (BMI) of over 30 according to self-reported survey data. (Other data based on physical examinations suggest higher prevalence of obesity, although recent data from this source are not available due to pandemic collection issues.) The majority of people with obesity are White (62%), while another 18% are Hispanic, 15% are Black, 2% are Asian, 1% are American Indian or Alaska Native (AIAN), and less than 1% are Native Hawaiian or Other Pacific Islander (NHOPI) (Figure 1).
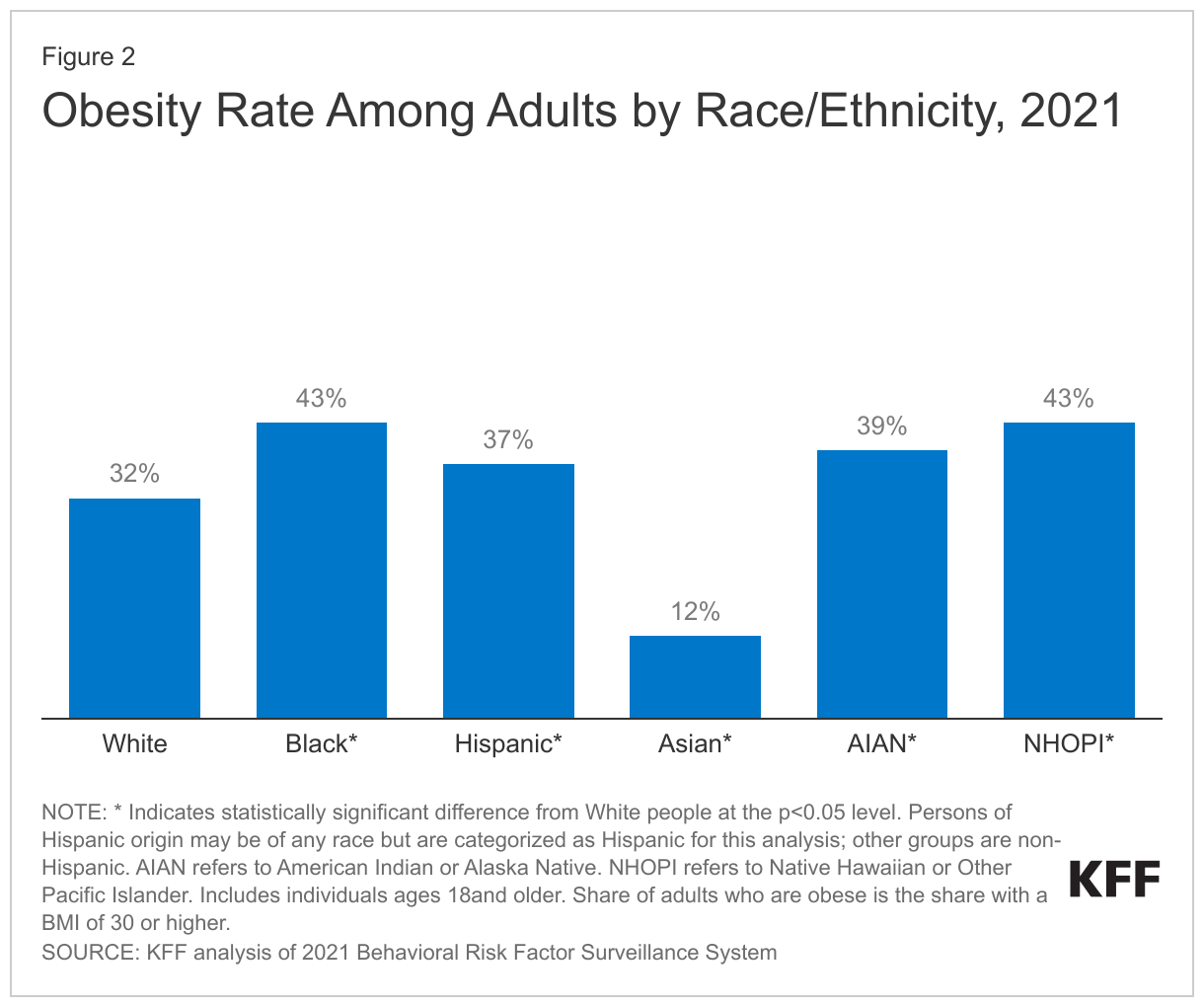
Although most people with obesity are White, many people of color are at increased risk for obesity. As of 2021, Black (43%), NHOPI (43%), AIAN (39%), and Hispanic (37%) adults all had higher obesity rates than White adults (32%), while Asian adults had a lower obesity rate at 12% (Figure 2). These disparities in obesity reflect a variety of factors, including more limited access to health care as well as social and economic factors, including higher rates of food insecurity, more limited access to healthy food options, more limited time and access to opportunities for physical activity and recreation.
Given higher rates of obesity among people of color, they could particularly benefit from new treatment options. However, they also are more likely than their White counterparts to face barriers to affording and accessing the new medications. AIAN, Hispanic, NHOPI, and Black nonelderly people are more likely to be uninsured and have lower incomes than their White counterparts. Moreover, growing shortages of the medications may further limit access to people with resources and time to navigate systems to identify availability.
Going forward, the new weight loss medications provide an additional tool for obesity prevention and treatment but may remain unaffordable for some patients. Expanded coverage of these medications may help to address some disparities in access. There is interest in expanding coverage under Medicare, including the Treat and Reduce Obesity Act reintroduced to the Senate and House in July 2023, and many private insurance plans and employers are actively considering how to approach coverage of these drugs. Some states also are examining approaches to cover obesity treatment including prescription drugs under Medicaid, which covers a disproportionate share of people of color relative to other payers. Expanded coverage would likely improve access but also increase costs to public payers and private plans, although there is a possibility of a downward effect on health care costs if use of the medications lowers the risk of chronic illnesses associated with obesity. However, even with expanded coverage of these medications, people of color would still face disparities in access given their higher uninsured rates. Moreover, the medications may not be an appropriate treatment option for all patients. Consideration of actions to provide equitable access to these medications, other prevention and treatment strategies, as well as other medical advancements will be important given the ongoing racial disparities in obesity and other health outcomes.