Section 1115 Waiver Watch: Medicaid Pre-Release Services for People Who Are Incarcerated
Note: For the latest information on states with approved pre-release waivers, view our Section 1115 tracker “Key Themes Maps.”
In April 2023, the Centers for Medicare and Medicaid Services (CMS) released guidance encouraging states to apply for a new Section 1115 demonstration opportunity to test transition-related strategies to support community reentry for people who are incarcerated. This demonstration allows states a partial waiver of the “inmate exclusion policy,” which prohibits Medicaid from paying for services provided during incarceration (except for inpatient services). Justice-involved people are disproportionately low-income and often have complex and/or chronic conditions, including behavioral health needs (mental health conditions and/or substance use disorder (SUD)). Reentry services aim to improve care transitions and increase continuity of health coverage, reduce disruptions in care, improve health outcomes, and reduce recidivism rates.
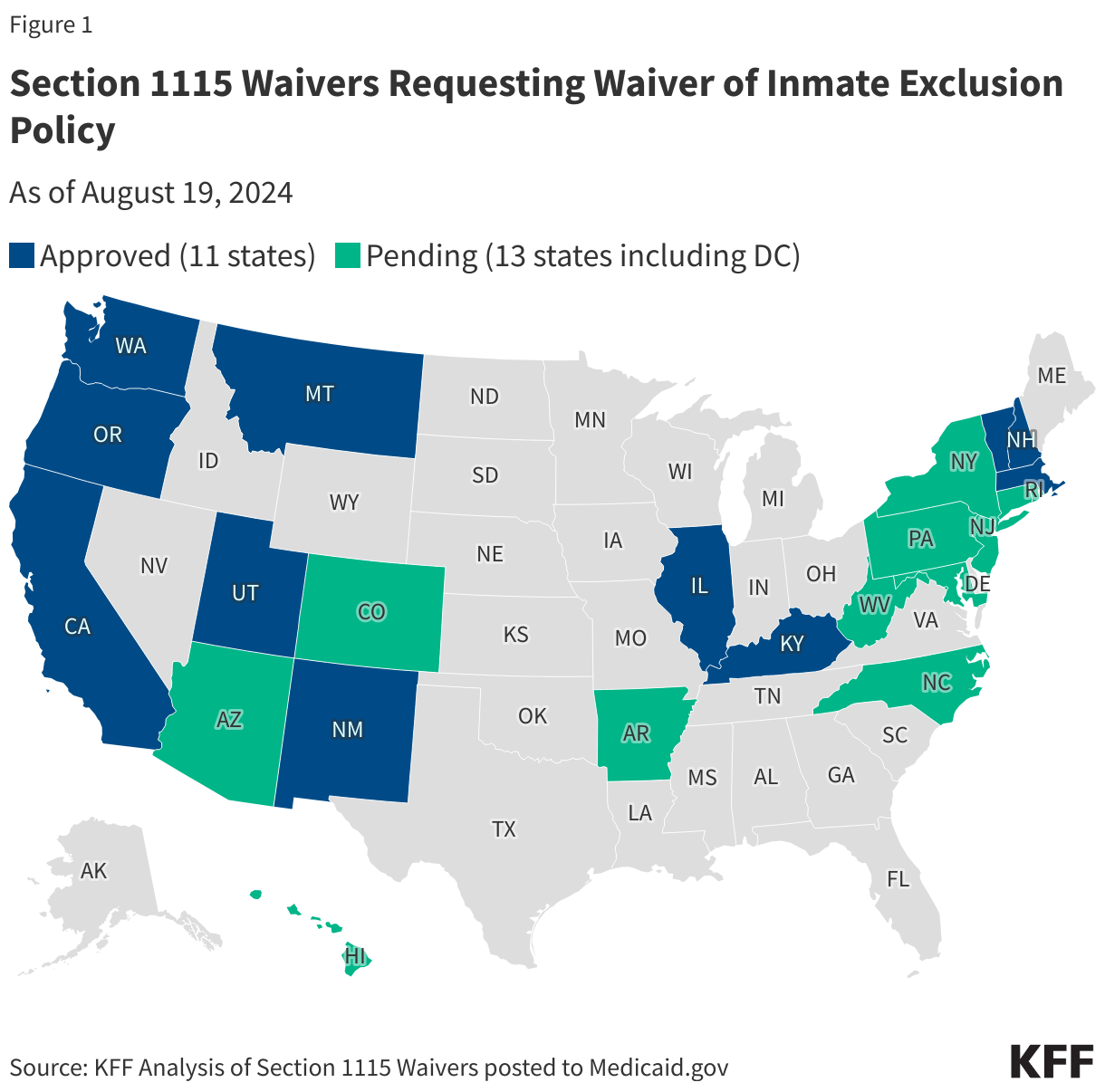
As of August 19, 2024, CMS has approved Section 1115 reentry waiver requests from 11 states, while 13 additional reentry waivers remain pending. In July 2024, CMS announced it had developed a standard demonstration application and special terms and conditions to expedite the review and approval of reentry waiver requests (approving 7 reentry waivers in July). States with governors across political parties have pursued these waivers. California will be the first state to implement its reentry demonstration in October 2024 (after gaining approval in January 2023); California’s experience may inform other states’ implementation efforts. This Waiver Watch reviews CMS guidance and summarizes key features of the eleven approved 1115 reentry waivers.
What are the demographics and health needs of people who are incarcerated?
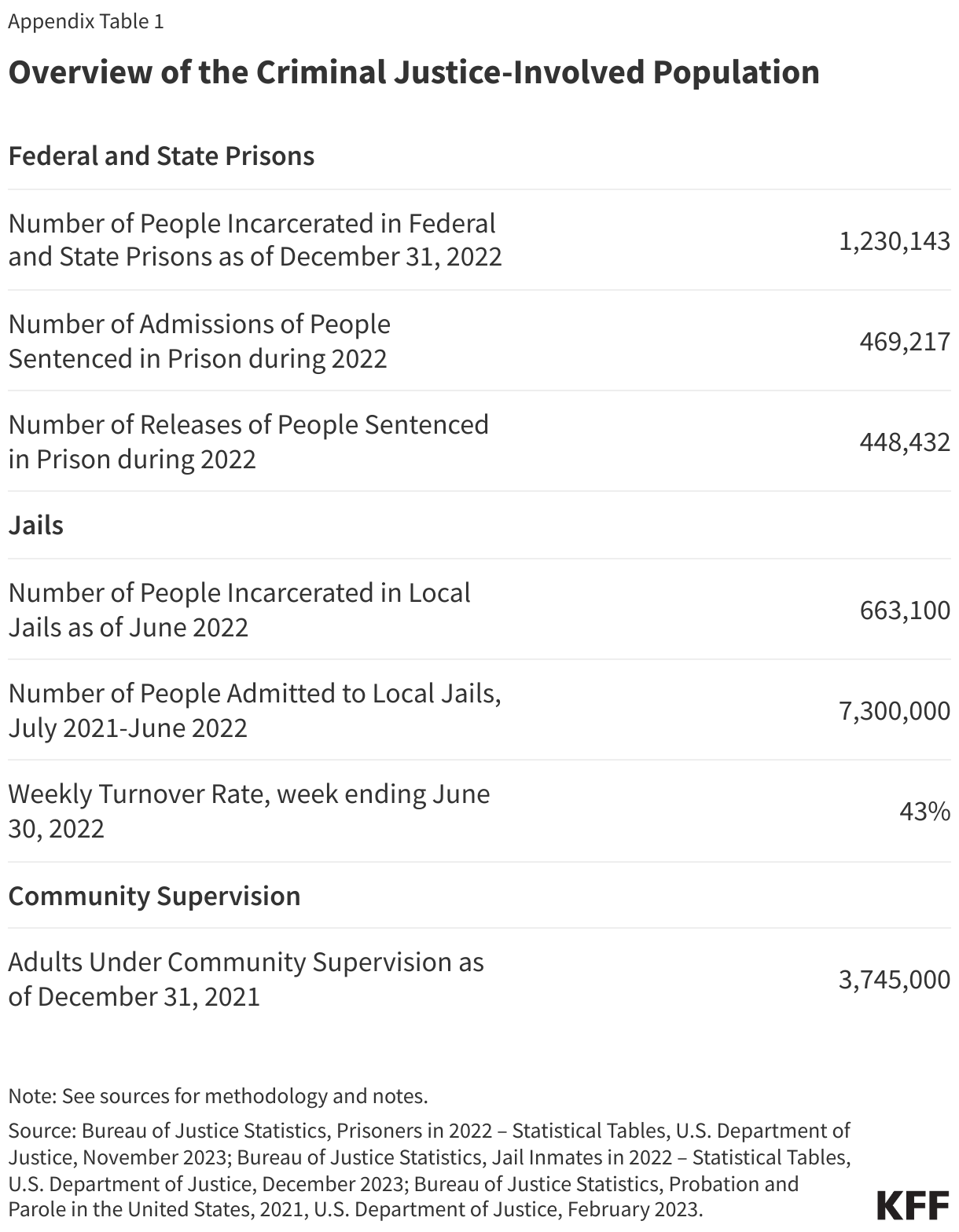
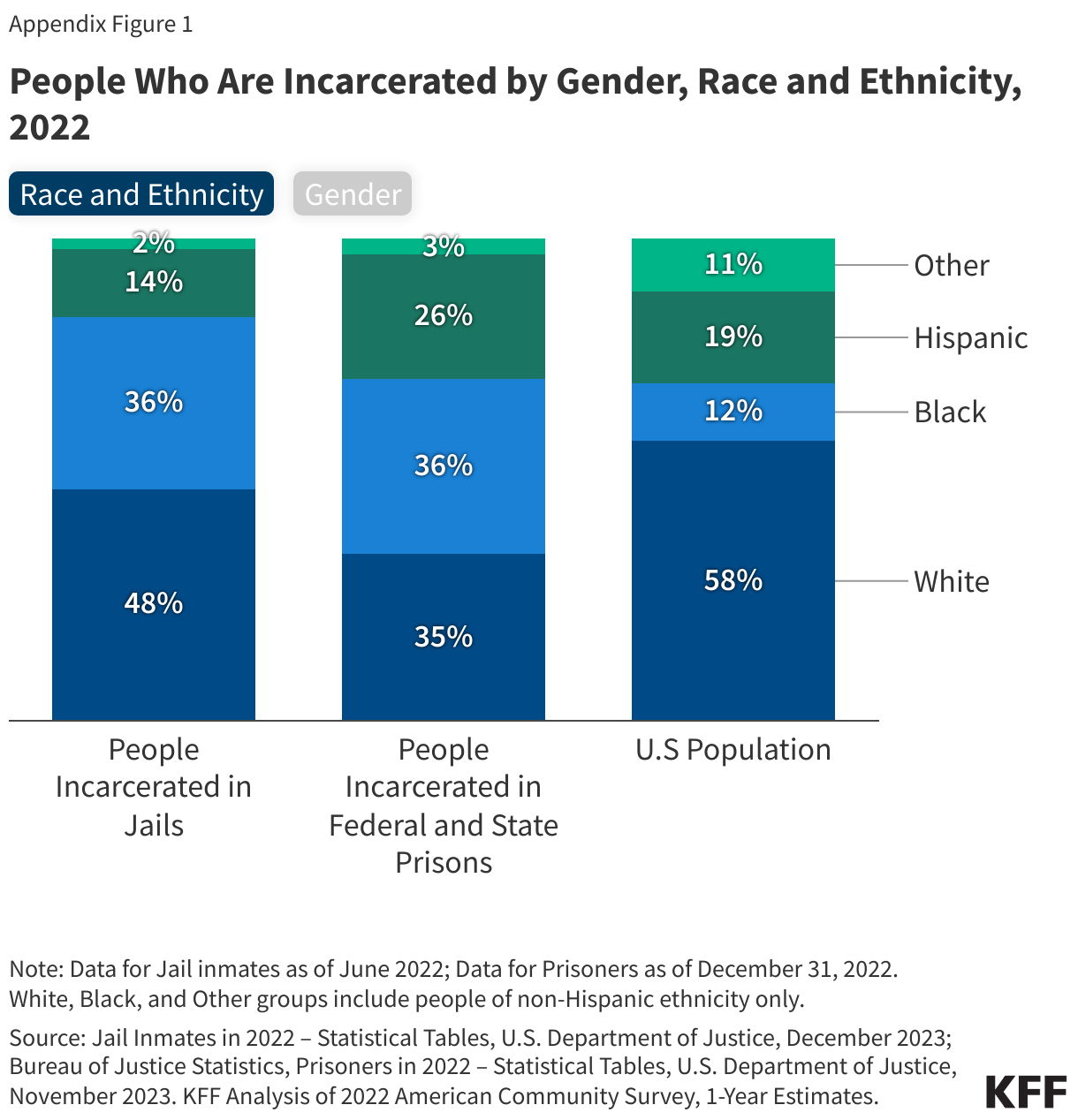
About 1.2 million people were incarcerated in federal and state prisons as of the end of 2022 and 660,000 people were held in local jails as of mid-year 2022. However, millions more interact with the correctional system each year (Appendix Table 1). The vast majority of people who are incarcerated in prisons and jails are male and over half of all people who are incarcerated are people of color (Appendix Figure 1). Hispanic and Black people are disproportionately represented among the carceral population (i.e., compared to their representation in the general population). Black people are incarcerated in prisons at nearly five times the rate of White people, and in jails more than three times the rate of White people. Racial disparities in incarceration further exacerbate health disparities.
Individuals who are incarcerated have higher rates of mental illness, substance use disorder, and chronic and physical health care needs than the general population and are particularly vulnerable upon release. These individuals have higher rates of chronic diseases such as hypertension, tuberculosis, hepatitis, and HIV/AIDS than the general population and also have significant behavioral health needs. An estimated 65% of people incarcerated in prisons (across the U.S.) have an active substance use disorder. Despite the high rates of physical and behavioral health needs among people who are incarcerated, access to health care services in prisons and jails is variable and may be limited. The U.S. Department of Justice issued guidance in 2022 indicating that preventing individuals who become incarcerated from continuing medication assisted treatment for opioid use disorder (prescribed before their detention) is a violation of the Americans with Disabilities Act (ADA). Upon release, people who were formerly incarcerated experience significant obstacles, including poverty, homelessness, stigma, legal barriers (e.g., to obtaining housing, employment etc.), and challenges accessing health care. When people leave incarceration, they are at greater risk of overdose death and suicide compared to the general population, as well as other adverse outcomes like increased risk for emergency department use, hospitalization, and recidivism.
What is the role of Medicaid for enrollees who are incarcerated?
The Affordable Care Act (ACA) Medicaid expansion provided new opportunities to connect enrollees leaving incarceration to coverage and services. The ACA expanded Medicaid eligibility to nearly all adults with incomes at or below 138% FPL ($20,783 for an individual in 2024) in the 41 states that have adopted the expansion. Previously, many adults who were incarcerated did not qualify for Medicaid due to restrictions that excluded low-income adults without dependent children from the program.
The “inmate exclusion” policy limits Medicaid coverage available to people who are incarcerated, but states have used various strategies to help maintain eligibility and coordinate care for people transitioning from incarceration. Current rules allow people to be enrolled in Medicaid while incarcerated, but the Medicaid “inmate exclusion” policy limits Medicaid reimbursement for incarcerated individuals to inpatient care provided at facilities that meet certain requirements. Most states facilitate access to Medicaid coverage by suspending rather than terminating coverage for enrollees who become incarcerated. Suspending eligibility expedites access to federal Medicaid funds if people receive inpatient care while incarcerated and allows coverage to be active immediately upon release, which facilitates access to health care services in the community. States have also adopted other strategies to coordinate care pre-release, including developing managed care requirements and fee-for-service initiatives.
Justice-Involved Youth
While the number of youth in juvenile detention and correctional facilities has fallen since 2000, 25,014 youth (under age 21) were in juvenile residential facilities in 2020. 2,250 juveniles (under 18) were incarcerated in adult prisons and jails in 2021. Justice-involved youth report high rates of adverse childhood experiences that research demonstrates is linked to poor health outcomes, including heart disease, substance use disorders, sexually transmitted diseases, and premature death among adults. Approximately two-thirds of justice-involved youth have diagnosable mental health or substance use disorders. As many as 50% of youth referred to the juvenile justice system are also involved with the child welfare system.
Current Requirements: The SUPPORT Act prohibits states from terminating Medicaid eligibility for individuals under age 21 or former foster care youth under age 26 while incarcerated. The Consolidated Appropriations Act (CAA) of 2023 extended this requirement to CHIP as well.
New Requirements: The 2023 CAA required states to implement 12-month continuous eligibility for children in Medicaid and CHIP as of January 1, 2024; CMS guidance on implementing this requirement includes considerations for specific populations, including children who become incarcerated. Starting January 1, 2025, the 2023 CAA requires Medicaid and CHIP to cover medically necessary screenings (including medical, dental, and behavioral health), diagnostic services, and case management for all eligible youth (under age 21 and former foster care youth under age 26) in public institutions (including state prisons, local jails, tribal jails and prisons, and all juvenile detention and youth correctional facilities) 30 days prior to release. States must continue to provide case management services for at least 30 days post-release. Some states are using 1115 waivers to provide pre-release services to incarcerated youth beyond minimum CAA requirements. The 2023 CAA also gives states an option to provide Medicaid or CHIP services (full benefits) to all youth (under age 21 and former foster care youth under age 26) in public institutions pending disposition of charges (i.e., awaiting the outcome of charges).
What are 1115 waiver options to provide Medicaid coverage for individuals pre-release from carceral settings?
The 2018 SUPPORT Act directed CMS to issue guidance on how waivers can improve care transitions for people who are incarcerated but otherwise eligible for Medicaid. The SUPPORT Act required the Secretary of Health and Human Services (HHS) to convene a group of stakeholders to help inform the design of a demonstration opportunity to improve care transitions for people leaving incarceration. Findings from that convening were summarized in a report from the Office of the Assistant Secretary for Planning and Evaluation (ASPE) and referenced in the waiver guidance issued by CMS. The report identifies promising practices to connect people to health care who are reentering the community after incarceration and summarizes the research evidence. Evidence suggests medication-assisted treatment (MAT) for opioid use disorder during incarceration and after release is associated with lower overdose and mortality rates and in-reach by peer navigators is associated with greater engagement in care following release. Other research suggests that Medicaid coverage can reduce recidivism.
In April 2023, CMS released guidance on the new Medicaid Reentry Section 1115 demonstration opportunity. The guidance summarizes CMS goals as well as demonstration features and minimum requirements, including:
- Carceral Settings. States participating in the demonstration may provide coverage for certain pre-release services to people incarcerated in state and/or local jails, prisons, and/or youth correctional facilities. States have discretion to identify the specific carceral settings eligible to participate and may set limitations on facility participation.
- Medicaid Eligibility and Enrollment. States are expected to suspend (rather than terminate) Medicaid eligibility when an adult Medicaid enrollee becomes incarcerated. States that do not currently suspend eligibility will be expected to fully implement suspension policies within two years. States are expected to work with corrections partners to assist people who are incarcerated but not already enrolled in Medicaid to apply for Medicaid upon or during incarceration, but no later than 45 days before expected release. States may consider using “presumptive eligibility” for individuals anticipated to have short incarceration stays.
- Eligibility for Pre-Release Services. States have the flexibility to define target populations (e.g., those with specific health conditions) and establish eligibility criteria. CMS encourages states to propose broadly defined populations of people soon-to-be released from incarceration who are otherwise Medicaid eligible.
- Minimum Benefits. CMS expects state proposals will include benefits “sufficiently robust” to be likely to improve care transitions, covering at least a minimum set of pre-release services:
- Case management to assess physical, behavioral health, and health-related social needs (HRSN) and assist people who are incarcerated in obtaining both pre- and post- release services (including setting up post-release appointments);
- MAT for all types of substance use disorders, with accompanying counseling; and
- A 30-day supply of all prescription medications at the time of release.
States may request to cover other services including, for example, family planning services, behavioral health or preventive services (including peer support), and/or Hepatitis C treatment.
- Pre-Release Timeframe. States may offer coverage of pre-release services 30 to 90 days before the expected date of release.
- Provider Requirements. States may choose to offer in-person or telehealth services. CMS indicates a preference for “in reach” by community-based providers. If states rely on carceral health care providers, they must comply with Medicaid participation policies set by the state.
- Capacity Building Funds. CMS will consider state requests for time-limited federal matching funds for certain new expenditures (e.g., development of new business and operational practices and related IT, workforce development, and outreach and stakeholder convening) to support the implementation of reentry demonstration waivers.
- Reinvestment Requirements. States must agree to reinvest federal matching funds received for carceral health care services currently funded with state/local dollars into activities that increase access or improve the quality of health care services for people who are incarcerated or were recently released or for health-related social services that may help divert people released from incarceration from criminal justice involvement.
What is the current landscape of pre-release waivers?
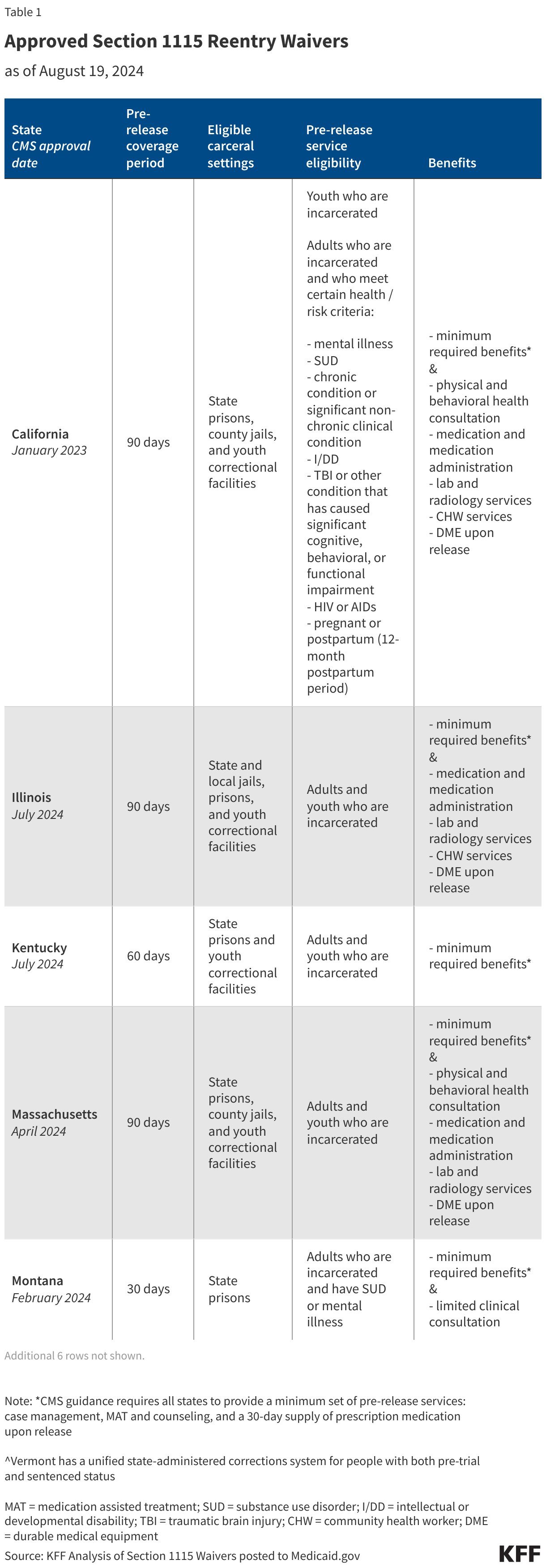
As of August 2024, eleven states have approval to provide pre-release services to certain incarcerated, Medicaid eligible individuals (Figure 1). CMS has developed a standard demonstration application and special terms and conditions (STCs) to expedite the approval of pre-release waiver requests (approving 7 waivers in July 2024). Features of the approved demonstrations (i.e., eligible carceral settings, pre-release coverage period, eligibility criteria for pre-release services, and benefits) vary across states (Table 1). The number of people potentially affected by these initiatives will vary based on each state’s incarcerated population as well as other state specific factors/decisions (e.g., eligibility criteria for services, state/corrections efforts to identify and enroll Medicaid-eligible individuals). California, for example, estimated in its initial application that approximately 200,000 people each year will be eligible to receive pre-release services under the demonstration waiver, while Washington estimated 4,000 people will receive pre-release services each year (both states’ estimates assume about half of all individuals released from incarceration will be eligible for pre-release services). Section 1115 waivers must be “budget neutral” for the federal government (i.e., costs under a waiver must not exceed what federal costs would have been for a state without the waiver). In its approvals, CMS has established per member per month spending caps for reentry services and aggregate (annual) spending caps for reentry planning and implementation activities.
As of August 2024, thirteen additional states (including DC) have pre-release waivers pending review at CMS. These pending requests vary in scope by pre-release period, eligibility, and benefits. Many of these requests were submitted prior to the release of the April 2023 CMS guidance. States with pending requests may need to make changes to conform with the new guidance and requirements.
What to watch?
Reentry initiatives are often part of broader reforms included in state 1115 waivers. States may currently be pursuing other policies and initiatives aimed at supporting individuals following release from correctional settings. For example, a few states have or are seeking approval to implement 12-month continuous eligibility for certain adults, including individuals released from corrections facilities, to promote continuity of coverage. Additionally, CMS recently expanded tools available to states to address enrollee health-related social needs, including approving coverage (under 1115 authority) of rent/temporary housing and utilities for up to 6 months as well as other housing and nutrition supports. Target populations include individuals experiencing high-risk care transitions—including from corrections facilities and the child welfare system. The outcome of the 2024 presidential election may affect states’ ability to continue to pursue some of these initiatives, as Section 1115 waivers generally reflect administrative priorities.
Implementation of pre-release services will require forging new partnerships with and providing significant technical assistance to corrections agencies, health care providers, and community-based organizations. CMS recognizes the operational complexities involved with providing services to an incarcerated population. States must submit reentry implementation plans to CMS for approval. Approved reentry waivers include authority to spend federal Medicaid funds on activities that support implementation, including planning activities, staff recruitment and training, and IT infrastructure. State Medicaid agencies will need to work closely with corrections agencies including to ensure access to demonstration-covered services, to facilitate access into carceral facilities for community-based health care providers and case managers, and to ensure systems are in place to share data and information. In April 2024, the Health Resources and Services Administration (HRSA) announced new funding for community health centers to support transitions in care for people leaving incarceration along with draft policy guidance. Community health centers provide comprehensive primary and behavioral health care services to individuals in medically underserved communities and may play an important role in post-release care delivery.
Section 1115 demonstration waivers are subject to regular reporting, monitoring, and evaluation requirements. As a condition of approval, states must submit a monitoring protocol, quarterly and annual reports, a mid-point assessment report, an evaluation design, and interim/summative evaluation reports. Information and analyses from independent evaluations will help answer questions about the impact of these initiatives on continuity of coverage, management of serious behavioral health conditions, and health outcomes (e.g., post-release overdose deaths, suicide, and other adverse outcomes); however, these evaluations will not be available for a number of years. In the meantime, initial implementation plans and regular state monitoring reports may yield important operational details, implementation information (including challenges and mid-course corrections), as well as preliminary enrollment and pre-release service utilization data. California will be the first state to implement its reentry demonstration in October 2024 (after gaining approval in January 2023). California’s experience may inform other states’ implementation efforts.
Federal legislation may further impact Medicaid coverage and access for people who are incarcerated and state capacity to support community transition. The Consolidated Appropriations Act of 2024, signed into law in March 2024, requires states to suspend rather than terminate Medicaid coverage for all individuals who are incarcerated starting January 1, 2026 (this suspension requirement is already in place for youth). The legislation includes $113.5 million in appropriated funds to help states meet the new requirement. It also directs CMS to issue guidance (within 18 months) on strategies and best practices to address implementation and operational challenges to ensure access to and continuity of care for Medicaid and CHIP beneficiaries before, during, and after incarceration. These efforts could supplement ongoing state approaches and federal investments to expand access to substance use disorder treatment. Other legislation introduced at the federal level in 2023 (e.g., SUPPORT ACT reauthorization, the Reentry Act, and the Due Process Continuity of Care Act) would expand Medicaid coverage for people who are incarcerated if passed.
Appendix Tables