The Impact of the COVID-19 Recession on Medicaid Coverage and Spending
Unlike previous recessions in modern history, this past recession was spurred by the spread of a virus (COVID-19), which created a public health crisis with unique health implications. Understanding the impact past recessions have had on Medicaid programs, early in the pandemic we began tracking employment and state revenue indicators, which can signal changes to Medicaid enrollment and have implications for state budgets. Medicaid is a counter-cyclical program, meaning that more people become eligible and enroll during economic downturns; at the same time, states may face declines in revenues that make it difficult to fund the state share of funding for the program. However, the pandemic-induced recession looked different from historical recessions in a number of ways. This brief describes the broader impacts of this most recent recession — which lasted from February 2020 to April 2020 — and also explores how trends in Medicaid spending and enrollment differed from past recessions and what that might mean for state Medicaid programs moving forward. Key differences between the Great Recession and the COVID-19 recession are highlighted in Table 1.
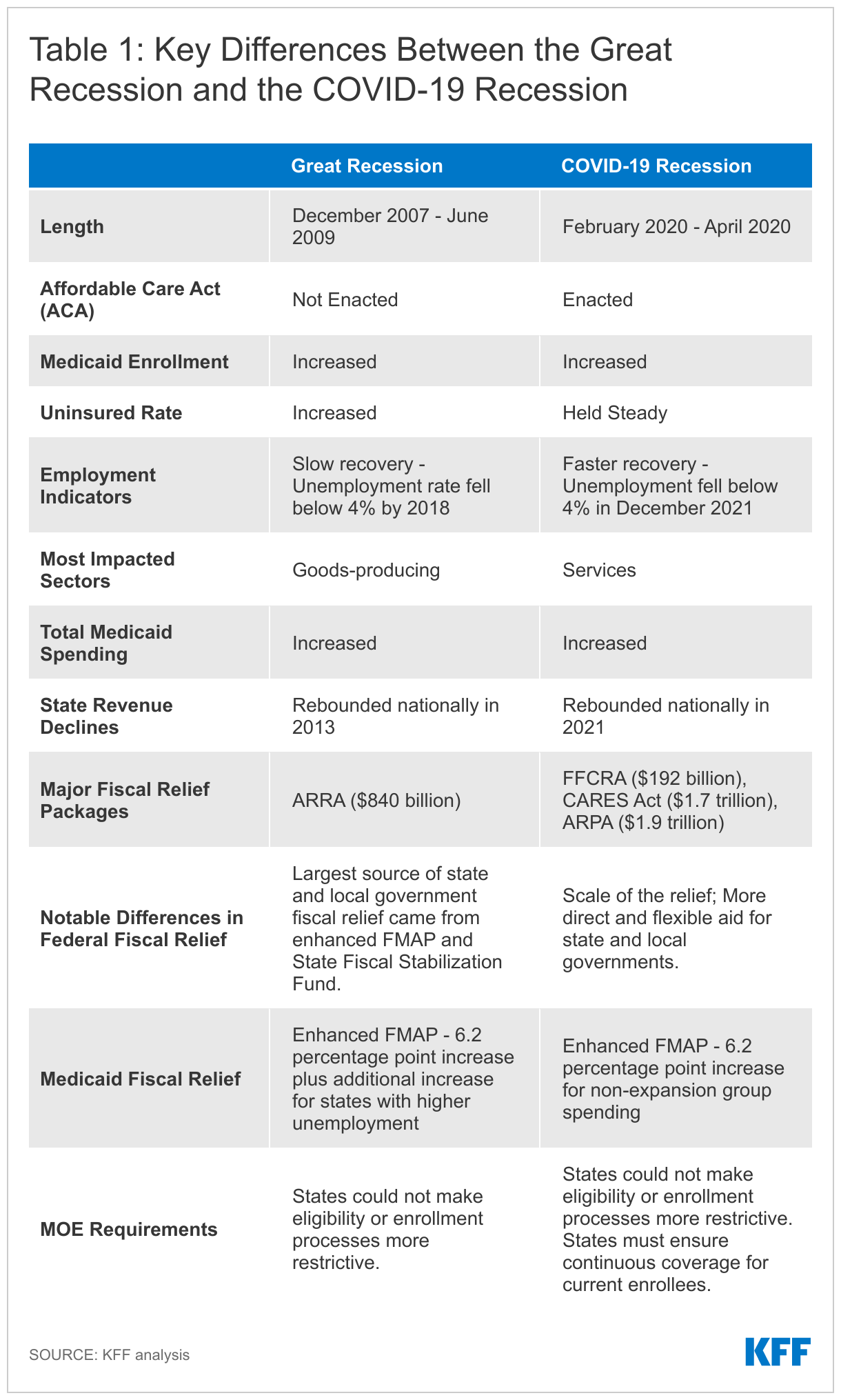
How were the effects of this recession different from the Great Recession?
This recession was the first recession since the passage of the Affordable Care Act (ACA), which created new coverage options in Medicaid and through the ACA marketplace (Table 1). Following the implementation of the ACA, the non-elderly uninsured rate dropped by the largest amount ever recorded, and recent data show the number of people who were uninsured and the uninsured rate held steady in 2020, the first year of the pandemic. In comparison, during the Great Recession, the non-elderly uninsured rate grew significantly by 1.9 percentage points from 2007 to 2010.
Numerous legislative actions were taken to combat the health and economic effects of the pandemic (Table 1). Congress passed the Families First Coronavirus Response Act (FFCRA), which among other provisions, authorized a 6.2 percentage point increase in the federal Medicaid match rate (“FMAP”) for states that meet certain “maintenance of eligibility” (MOE) requirements with the goal of providing broad fiscal relief to states and supporting increases in Medicaid enrollment. The additional funds were retroactively available to states beginning January 1, 2020 and continue through the quarter in which the Public Health Emergency (PHE) period ends. Congress also passed the Coronavirus Aid, Relief, and Economic Security Act (CARES Act) and later the American Rescue Plan Act (ARPA), which provided unprecedented fiscal relief, increasing the speed and strength of the economic recovery and providing support to families facing household hardships in the wake of the pandemic, including increased premium assistance for ACA marketplace enrollees. Overall, the scale of federal fiscal relief authorized during the pandemic was much larger compared to the Great Recession, providing more direct fiscal relief to families including three rounds of stimulus checks and more flexible relief for state and local governments.
What happened to Medicaid enrollment during the public health crisis and COVID-19 recession?
Medicaid enrollment has increased by over 12 million, or by more than 17 percent through July 2021 (Figure 1). Many factors likely contributed to Medicaid enrollment growth during the pandemic including the MOE and other economic factors. The MOE continuous eligibility requirement kept people enrolled in the program irrespective of changes in income and halted churn, which is when individuals temporarily lose Medicaid coverage and disenroll and then re-enroll within a short period of time. A recent KFF analysis found one in ten Medicaid/CHIP enrollees disenrolled and then re-enrolled within a year. Churn can occur when enrollees face barriers to maintaining coverage despite remaining eligible due to renewal processes and periodic eligibility checks. Churn can also occur because enrollees experience short-term income fluctuations that make them temporarily ineligible; however, much of the federal income support provided during the pandemic, like the $600 additional unemployment benefit, did not count toward Medicaid eligibility.
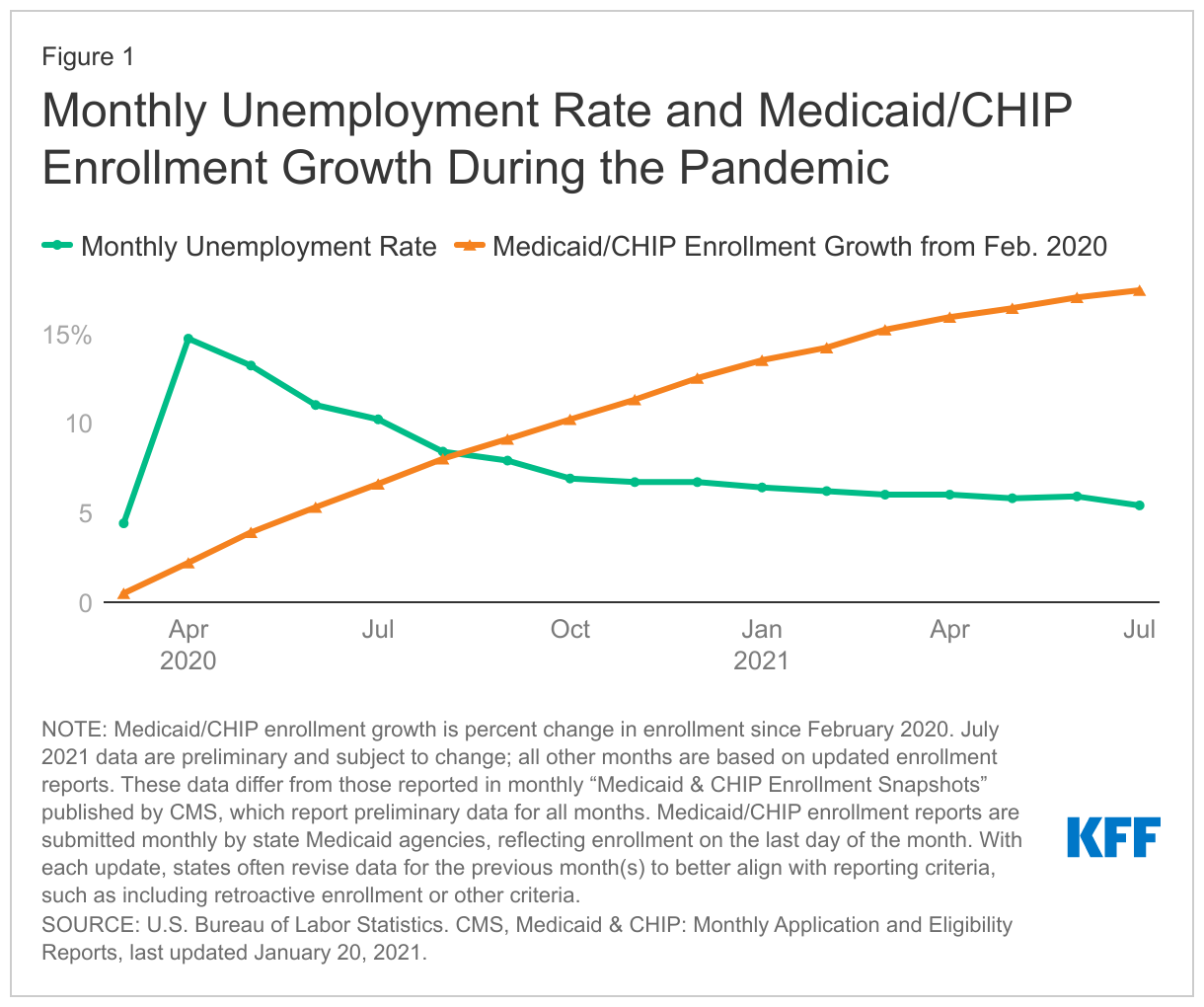
Despite a historical relationship between the national unemployment rate and Medicaid enrollment, studies have shown that, during the COVID-19 pandemic, increases in Medicaid enrollment have not been directly associated with increases in unemployment.1 ,2 ,3 Employment indicators, such as the unemployment rate, have historically signaled changes to Medicaid enrollment. Following the onset of the pandemic, national employment indicators quickly worsened, creating one of the deepest recessions on record. The unemployment rate soared to a peak of 14.7% in April 2020, which is higher than the highest unemployment rate during the Great Recession (10.0% in October 2009) (Figure 1). Unemployment claims also spiked, and the employment-to-population ratio, which captures what share of the population is working overall, plummeted. While this recession was deep, it was the shortest on record at two months. National economic indicators have improved in recent months, with the national unemployment rate and monthly unemployment claims nearing pre-pandemic levels. However, the employment-to-population ratio, remains below pre-pandemic levels, signaling labor force participation remains depressed. Beyond national indicators, some states are still experiencing unemployment rates higher than the national rate.
Populations and industries affected by the recession were more likely to include people already eligible or enrolled in Medicaid. Job losses were concentrated among low-income workers, as well as workers identifying as Black or Hispanic and younger workers. While national employment indicators have improved, jobs recovery has been slower for low-wage workers compared to higher-wage workers as well as Black and Hispanic workers compared to White workers. So, even without the continuous coverage requirements, it is not clear how many Medicaid enrollees would be experiencing changes or increases in income.
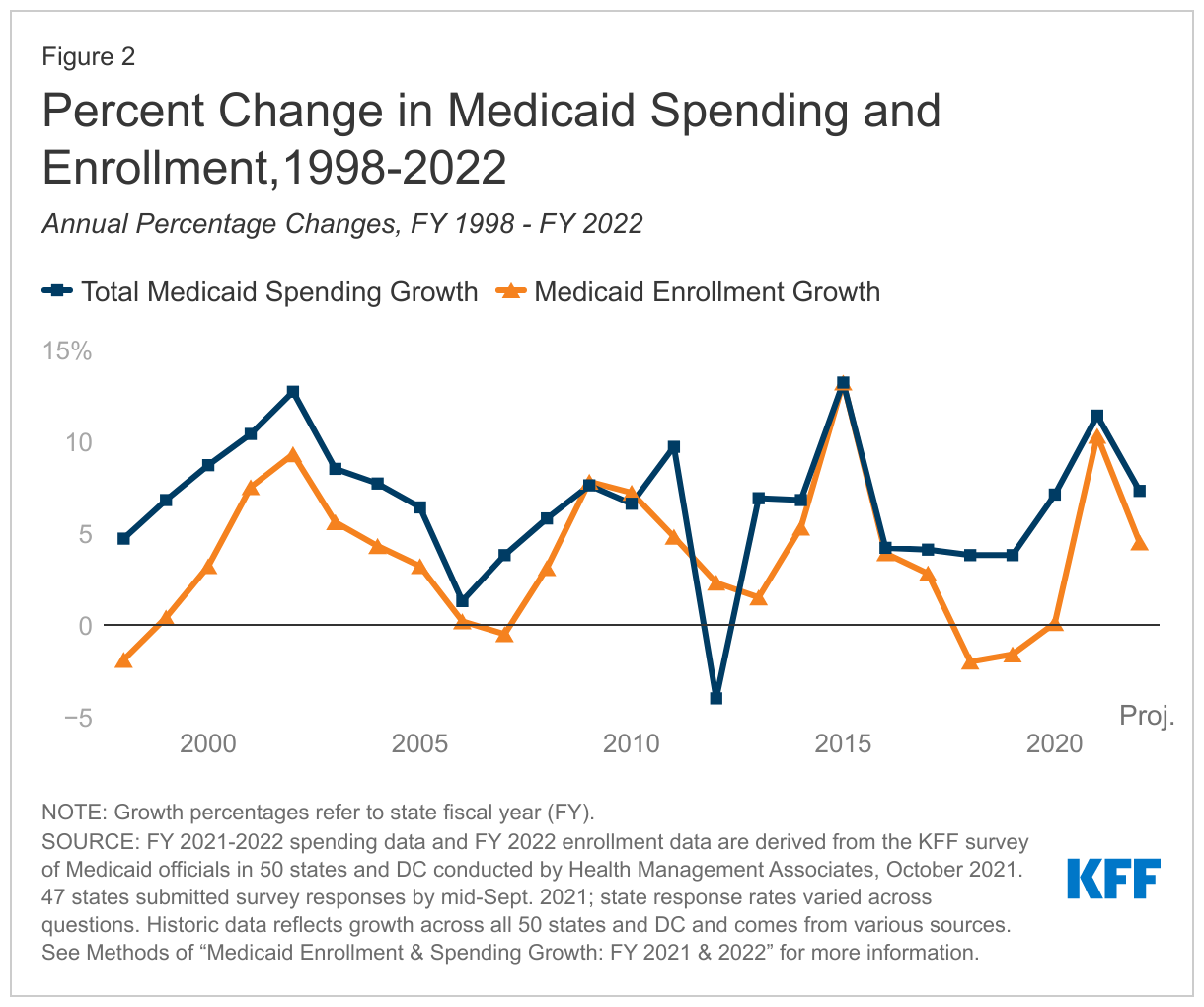
The COVID-19 recession had different implications for Medicaid compared to the Great Recession. While Medicaid enrollment growth spiked during the Great Recession (Figure 2), the MOE requirements tied to the fiscal relief during the Great Recession did not include a continuous enrollment requirement, though states could not make eligibility or enrollment processes more restrictive. As noted above, the unemployment rate peak in April 2020 exceeded the highest unemployment rate during the Great Recession; however, the Great Recession spanned a much longer timeframe with broader changes in income. The Great Recession widely impacted goods-producing industries, with the largest employment losses among the construction and manufacturing sectors, while service sectors, like leisure and hospitality, experienced the largest employment losses during the pandemic-induced recession (Table 1). During the first year of the pandemic, more women than men left the labor force, which contrasts trends seen in the Great Recession, when more men left the labor force. The Great Recession also predated the ACA, including expanded Medicaid eligibility and premium assistance for people buying individual insurance through the ACA marketplace.
What happened to Medicaid spending?
As during previous recessions, total Medicaid spending growth increased following the onset of the pandemic (Figure 2). In KFF’s annual budget survey, states identified enrollment growth as the primary driver of spending growth, and noted the end of the PHE and the MOE requirements and enhanced FMAP that are tied to the PHE will have significant implications for Medicaid spending and enrollment. Total Medicaid spending also increased during the early 2000s recession and the Great Recession, as more people experienced job or income loss and became eligible for Medicaid and enrolled. However, as the result of enhanced FMAP, state spending on Medicaid declined in 2020 as federal support increased (Figure 3). When fiscal relief expires, the state share and federal shares of Medicaid spending are expected to shift. During the Great Recession, state spending for Medicaid also declined in FY 2009 and FY 2010 due to fiscal relief from a temporary FMAP increase provided in the American Recovery and Reinvestment Act (ARRA). State spending increased sharply when that fiscal relief ended.
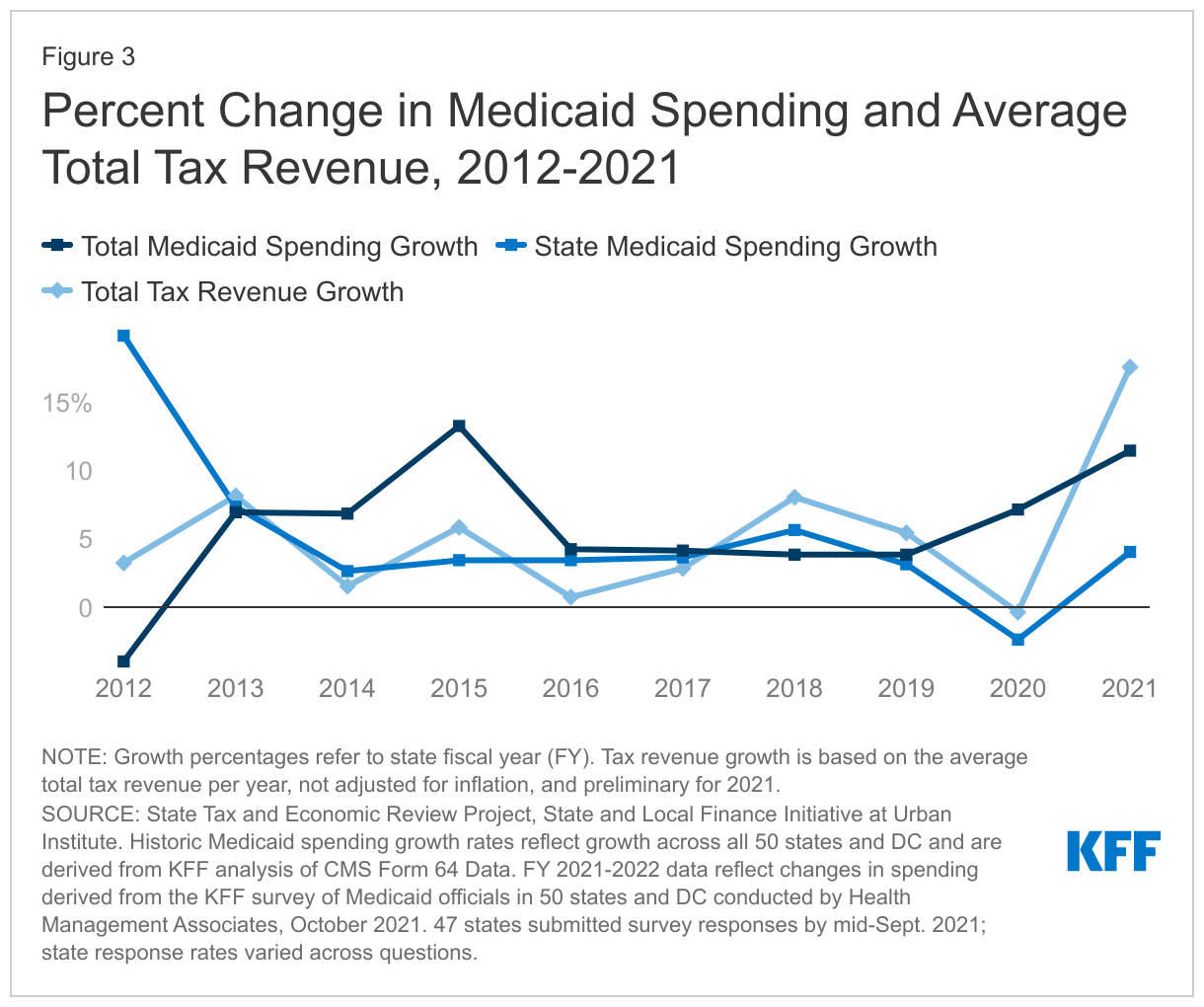
Improving state economic conditions as well as federal fiscal relief mitigated the need for the widespread spending cuts experienced in prior recessions. Early in the pandemic, steep state budget shortfalls were projected for FY 2020 and FY 2021 and states adopted conservative FY 2021 budgets. However, revenue declines were not as deep as projected and national tax revenue rebounded in 2021, with some declines in revenue attributed to states delaying their 2020 income tax collections from April to July (the start of FY 2021 for most states) (Figure 3). The quick rebound is due, in part, to federal aid provided to states, improved state sales tax collections on online purchases, and smaller personal income tax revenue declines due to the disproportionate impact of the pandemic on low-income workers. Revenue impacts and the speed of recovery has varied by state depending on state characteristics such as tax structure, industry reliance, social distancing policies and behaviors, and virus transmission. In contrast to budgets adopted for FY 2021, proposed FY 2022 state budgets reflected improving economic conditions, and most states enacted FY 2022 budgets with increased state spending and revenue. State revenues were slow to rebound following the Great Recession, with national revenues remaining depressed until mid-2013, though the recovery varied drastically from state to state (Table 1). Medicaid programs experienced more drastic spending cuts in previous economic downturns, including provider payment cuts, benefit restrictions, and/or eligibility restrictions.
Looking ahead
While national employment indicators show vast improvement from the start of the pandemic, there is variation across states and job sectors that may suggest slower recovery for low-wage workers; so, even after the end of the continuous coverage requirements it is unclear if Medicaid enrollment patterns will reflect broader national economic indicators. It remains unclear how long the period of recovery will last, what will happen once federal fiscal relief ends, and what longer term effects the pandemic-induced recession will have on the economy. For example, shifts in consumer and business behavior, changes in the composition of the labor force, rising inflation, and the Russian invasion of Ukraine may have future impacts on the economy.
Governors have started to propose their FY23 budgets, and their proposals will likely reflect improving fiscal conditions, with some states considering a range of tax cuts in light of improved revenue collections. During this budget season, states will likely grapple with the uncertainty of the duration of the PHE and the fiscal relief tied to the PHE, which was extended to mid-April 2022. The Biden Administration has said that it will give states a 60 day notice before the PHE expires. Since that notice was not issued in February, it is expected that the PHE will be extended again.
The end date of the PHE will have significant implications for Medicaid enrollment and spending. When the continuous enrollment requirements end, states will begin processing redeterminations and renewals and millions of people could lose coverage if they are no longer eligible or face administrative barriers during the process despite remaining eligible. The Build Back Better Act (BBBA) – which has passed the House but faces uncertain prospects in the Senate – included provisions that would phase-out the continuous enrollment requirement with rules about disenrolling people tied to a phased down enhanced match rate through FY 2022. Within parameters set by the Administration, or legislation if enacted, states will largely be responsible for managing the unwinding of the continuous enrollment requirement, which could lead to variation in practices and in how many people are able to maintain Medicaid coverage, transition to other coverage or become uninsured.
- Peggah Khorrami and Benjamin Sommers, “Changes in US Medicaid Enrollment During the COVID-19 Pandemic”, JAMA Network Open 4(5):e219463 (2021), doi:10.1001/jamanetworkopen.2021.9463 ↩︎
- Chris Frenier, Sayeh Nikpay, and Ezra Golberstein, “COVID-19 Has Increased Medicaid Enrollment, But Short-Term Enrollment Changes Are Unrelated To Job Losses”, Health Affairs 39,10 (2020): 1822-1831, https://www.healthaffairs.org/doi/10.1377/hlthaff.2020.00900. ↩︎
- Laura Dague, Nicolás Badaracco, and Thomas DeLeire, et al., “Trends in Medicaid Enrollment and Disenrollment During the Early Phase of the COVID-19 Pandemic in Wisconsin”, JAMA Health Forum 3(2):e214752 (2022), doi:10.1001/jamahealthforum.2021.4752. ↩︎