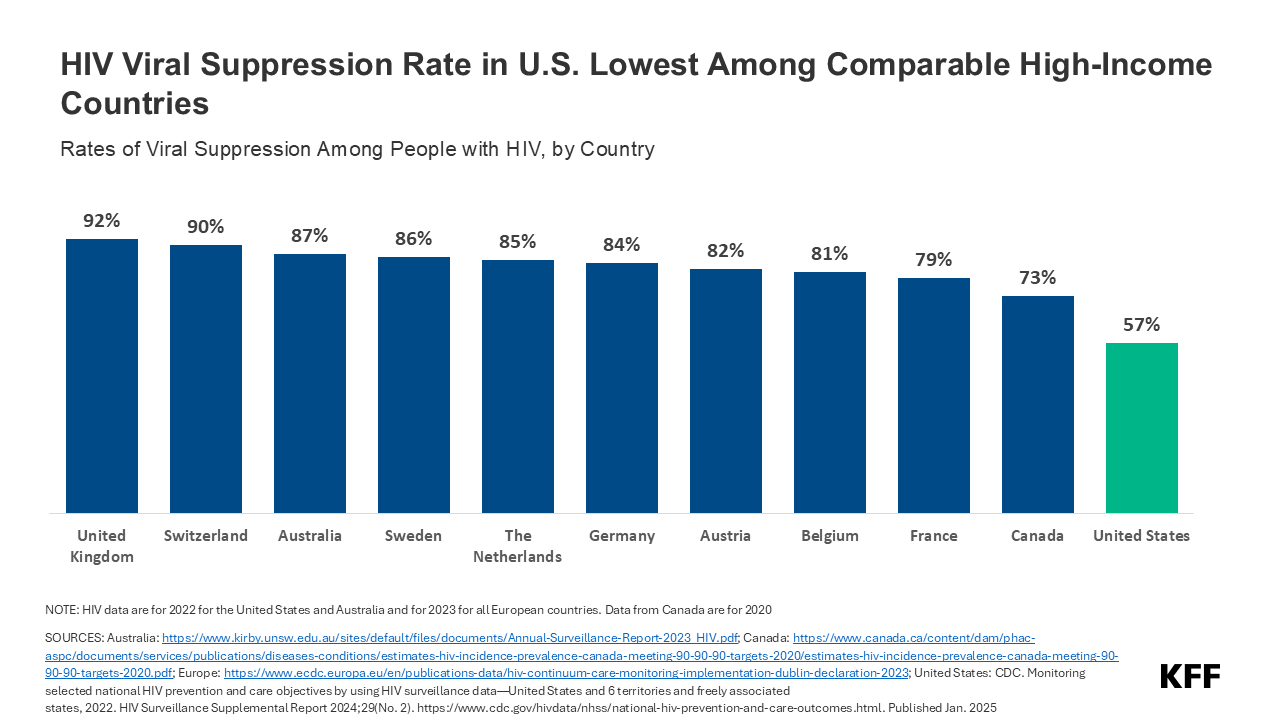
HIV Viral Suppression Rate in U.S. Lowest Among Comparable High-Income Countries
The independent source for health policy research, polling, and news.
Section 1115 Medicaid demonstration waivers offer states an avenue to test new approaches in Medicaid that differ from what is required by federal statute, if [in the HHS Secretary’s view] the approach is likely to “promote the objectives of the Medicaid program.” They can provide states additional flexibility in how they operate their programs, beyond the considerable flexibility that is available under current law. Waivers generally reflect priorities identified by states as well as changing priorities from one presidential administration to another. Nearly all states have at least one active Section 1115 waiver and some states have multiple 1115 waivers. This brief explains what Section 1115 waivers are and how they are used, summarizes key waiver requirements, and outlines the application and approval process.
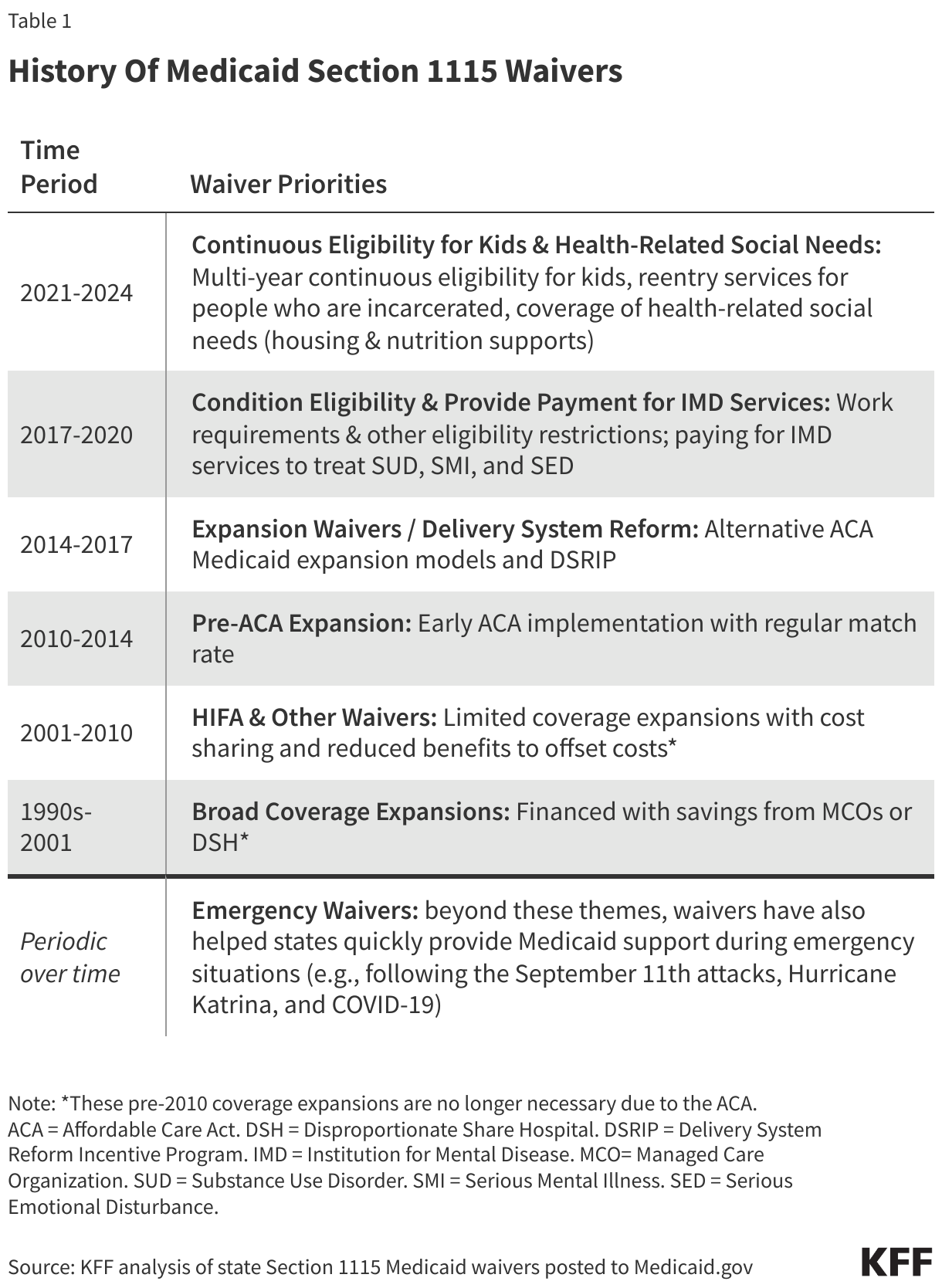
Authority & Purpose. Under Section 1115 of the Social Security Act, the Secretary of Health and Human Services (HHS) can waive certain federal Medicaid requirements.1 In addition, the Secretary may permit states to use federal Medicaid funds in ways that are not otherwise allowed. Each administration has some discretion over which waivers to approve and encourage (Table 1). While the Secretary’s waiver authority is broad, it is not unlimited. Section 1115 waivers have been challenged in court. The Secretary does not have authority to waive some elements of the program, such as the federal matching payment system for states, or requirements that are rooted in the Constitution, such as the right to a fair hearing.2
Waiver Scope/Use. Waivers have been used to expand coverage or benefits, change policies for existing Medicaid populations (e.g., testing premiums or other eligibility requirements), modify delivery systems, restructure financing or authorize new payments (e.g., supplemental payments or incentive-based payments), as well as make other program changes. Waivers vary in size and scope. States can obtain “comprehensive” Section 1115 waivers that make broad program changes or narrow waivers focused on a specific population. Some policies introduced through 1115 waivers can only be implemented through Section 1115 authority while others could be implemented under other authorities (e.g., State Plan authority or 1915(c)). MACPAC analysis found about half of all Medicaid spending (in FY 2019) was authorized under Section 1115 demonstrations, but most of that spending could have been covered without an 1115 waiver. States may seek to include some populations or services in Section 1115 waivers that could be covered under other authorities to capture “budget neutrality” savings (discussed in more detail below). For example, although states can implement mandatory managed care for most populations under other authorities (e.g., State Plan or 1915(b)), states may implement managed care under 1115 authority to show budget neutrality savings, which can be used to finance other waiver costs that are not otherwise covered / allowed by Medicaid. In addition, many states have comprehensive waivers that make broad and intertwined program changes and may include both provisions that require 1115 authority as well as provisions that could be implemented without a waiver.
Financing. Under long-standing policy and practice (although not required by statute), waivers must be “budget neutral” to the federal government over the course of the waiver. In other words, federal costs under an 1115 waiver may not exceed what they would have been for that state without the waiver. Typically, budget neutrality calculations are determined on a per enrollee basis—so, per enrollee spending over the course of the waiver cannot exceed the projected per enrollee spending calculated in the “without-waiver baseline” (putting states at risk for the costs per individual but not for the number of individuals enrolled). Waiver budget neutrality—measured against the estimated without-waiver baseline over the entire demonstration period—is not the same as a federal per enrollee limit on spending set at rates lower than expected under current law to generate federal savings. Budget neutrality calculations and the use of “budget neutrality savings” (to fund the federal share of costs not otherwise allowed) are negotiated between states and CMS (and the Office of Management and Budget (OMB)).
Because Section 1115 budget neutrality is not defined in statute or regulations, CMS agency policy and guidance to states has changed over time. For example, the Trump administration made changes to 1115 waiver budget neutrality policy in 2018, limiting the amount of federal funds that could be used for waiver spending. Later, the Biden administration made changes to Section 1115 budget neutrality policies that could provide greater flexibility for states to design and implement 1115 demonstration programs, including health-related social needs initiatives.
Waiver Timeframe. Section 1115 waivers generally are approved for an initial five-year period and can be renewed, typically for three-to-five-year periods. Some waivers have been continually renewed over many periods, allowing waiver operations to continue for many years. Under the Trump administration, in a departure from prior policy, CMS approved waiver extension requests for up to 10 years.
Incoming administrations may let waivers expire, choosing not to renew certain waiver provisions if they don’t align with the administration’s waiver priorities or if they determine the provisions do not promote the objectives of the Medicaid program. Additionally, outlined in waiver approval terms and conditions, CMS reserves the right to withdraw Section 1115 waiver or expenditure authorities at any time (including those already in operation under an active/approved waiver). The Biden administration withdrew Medicaid work requirement waivers in all states that had approvals, concluding that the provisions do not promote the objectives of the Medicaid program. States can appeal withdrawal decisions to the HHS Department Appeals Board and/or challenge recissions in court.
Transparency, Public Input, and Evaluation. The Affordable Care Act (ACA) made Section 1115 waivers subject to new rules about transparency, public input, and evaluation.3 Regulations require public notice and comment periods to occur at the state and federal levels before CMS approves new Section 1115 waivers and extensions of existing waivers. Although the final regulations on public notice do not require a state-level public comment period for amendments to existing/ongoing demonstrations, CMS has historically applied these regulations to amendments as well. The Trump administration did not enforce state-level public notice and comment procedures maintained by previous administrations for certain 1115 waiver requests, including waivers that proposed significant changes.
The ACA also implemented new evaluation requirements for Section 1115 waivers, including that states must have a publicly available, CMS-approved evaluation strategy. States have traditionally also been required to submit quarterly reports as well as an annual report to HHS that describes the changes occurring under the waiver and their impact on access, quality, and outcomes.
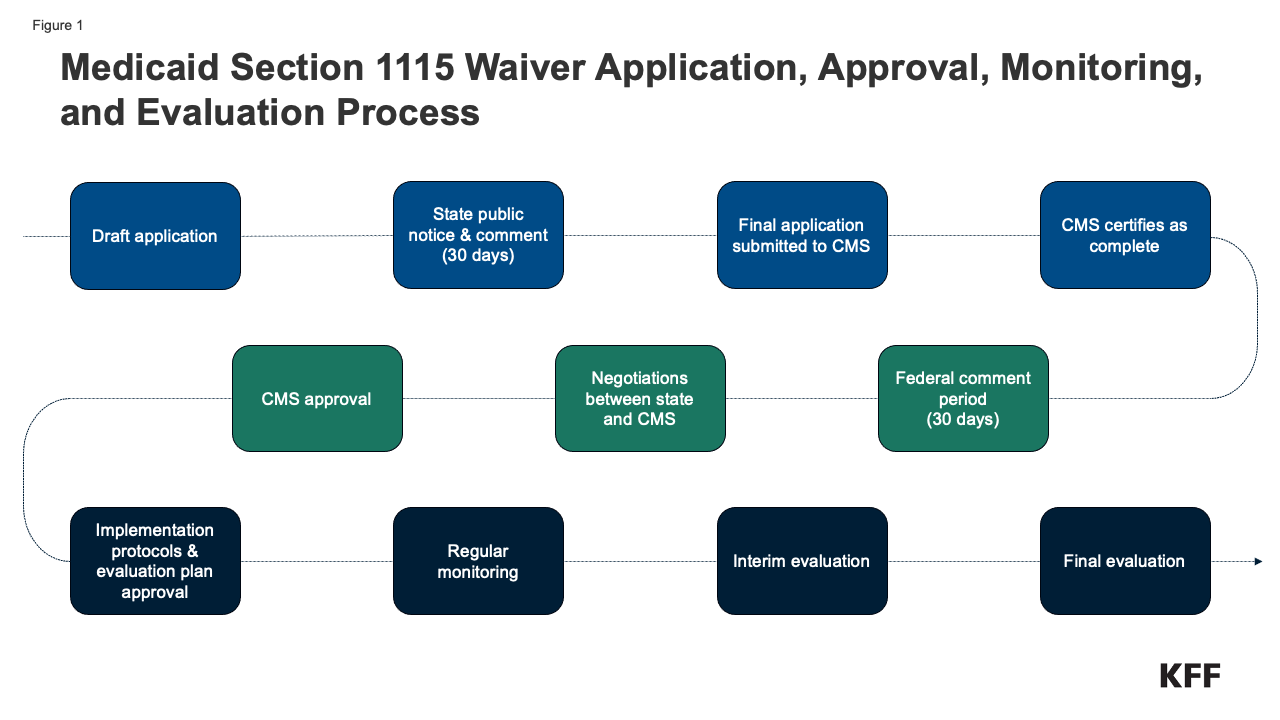
Waiver Application, Monitoring, and Evaluation Process. Medicaid policy changes, including through Section 1115 waivers, may require state legislative action or may be authorized at the direction of the governor. Once proposed policy changes have been formulated, a demonstration waiver proposal must be drafted. Key steps in the waiver process include (Figure 1):
*State waiver applications (including amendment and renewal requests), CMS issued approval documents, required implementation plans and protocols, and monitoring and evaluation reports are made publicly available on Medicaid.gov (search by state).
At the start of 2025, many issues are at play that could affect Medicaid coverage, financing, and access to care. Medicaid is the primary program providing comprehensive health and long-term care to one in five people living in the U.S. While Medicaid was not discussed much on the campaign trail, there are expectations that big changes will likely be proposed through executive actions by the Trump administration and as part of a tax and spending debate in Congress. Even without Congressional action, the Trump administration can make significant programmatic changes through administrative action (including state demonstration waivers, regulations, and other guidance). Other areas to watch with Medicaid implications include state budgets and long-term care workforce challenges.
The most significant changes to Medicaid in 2025 could include federal funding cuts and financing reforms. According to documents reported on by Politico, House Republicans are considering $2.3 trillion in Medicaid cuts from policy changes that include: imposing a per capita cap on federal Medicaid spending, reducing the federal government’s share of costs for the Affordable Care Act (ACA) expansion group, imposing Medicaid work requirements, reducing the minimum federal matching rate for Medicaid expenditures, changing the match rate for the District of Columbia, and repealing the incentive for states to newly adopt the Medicaid expansion that was passed in the American Rescue Plan Act. These policy changes would fundamentally alter how Medicaid financing works and federal spending reductions of this magnitude would put states at significant financial risk, likely forcing them to cut the number of people covered, cover fewer benefits, and cut payment rates for physicians, hospitals, and nursing homes. If the House and Senate pass a budget resolution with a $2.3 trillion target for Medicaid, Congress will need to come up with detailed legislative policy proposals to hit that target through the budget reconciliation process.
Under current law states are guaranteed federal matching dollars without a cap for qualified services provided to eligible enrollees. The match rate (the share that the federal government pays, known as the federal medical assistance percentage or “FMAP”) varies across states based on per capita income. States receive a higher match rate for some services and populations, most notably, the 90% enhanced match for the ACA expansion population, and sometimes, Congress adjusts the match rate upwards during economic downturns.
With a second Trump administration and Republican control of Congress, work requirements are likely to be back on the agenda—through federal legislation or state Medicaid waivers. During the first Trump administration, 13 states received 1115 waiver approval to condition Medicaid coverage on meeting work and reporting requirements. Only Arkansas implemented work and reporting requirements with consequences for noncompliance; however, the waiver ended in 2019 when a federal court found the work requirement approval unlawful. 18,000 people lost coverage in Arkansas, primarily due to failure to regularly report the fact that they were working or document eligibility for an exemption. These approvals were either rescinded by the Biden administration or withdrawn by states, and Georgia is the only state with a work requirement waiver in place (following litigation over the Biden Administration’s attempt to stop it). Several states have continued to pursue work requirement waivers despite data showing that most Medicaid adults are working or face barriers to work. Among adults with Medicaid who are under age 65 and do not have Medicare or Supplemental Security Income (SSI), 91% are working, or are not working due to an illness, caregiving responsibilities, or school attendance. A Congressional Budget Office analysis of a recent work requirement proposal shows that the policy would reduce federal spending due to reductions in enrollment and increase the number of people without health insurance but would not increase employment.
Beyond work requirements, the previous Trump administration’s Section 1115 waiver policy emphasized eligibility restrictions and capped financing. Eligibility restrictions included permitting states to charge premiums and lock out enrollees who are disenrolled for unpaid premiums. Waiver priorities shift across presidential administrations and the new Trump administration’s waiver priorities will likely differ significantly from those of the Biden administration; however, it is unclear how the Trump administration will treat certain waivers promoted and approved by the Biden administration, such as those focused on addressing health-related social needs, multi-year continuous eligibility primarily for children, and leveraging Medicaid to help individuals leaving incarceration transition to the community. The Trump administration could choose not to approve waivers that remain pending, rescind existing waiver guidance, and withdraw approved waivers, although some of these waivers, particularly those that are using Medicaid to assist with reentry from incarceration, have been pursued by both Republican and Democratic governors.
Trump administration could delay implementation of new regulations or issue new rules or guidance related to access, managed care, and enrollment processes. The Biden administration finalized a number of major Medicaid regulations designed to promote quality of care and advance access to care for Medicaid enrollees as well as to streamline eligibility and enrollment processes in Medicaid and the Children’s Health Insurance Program (CHIP). These rules are complex and are set to be implemented over several years. Congress may consider legislation to overturn these rules, without legislation, the Trump administration could delay implementation of certain provisions or could issue new regulations that would undo these final rules. (Rules related to long-term care are discussed below). Finally, the Trump administration could issue guidance and implement policy to make it more difficult for people to obtain and maintain coverage, which would reduce enrollment and spending. Previously, the Trump administration sought to reduce Medicaid enrollment by encouraging states to conduct eligibility verification processes in between annual renewal periods.
State fiscal conditions remained stable at the beginning of state FY 2025, but the longer term fiscal outlook is less certain. Heading into FY 2025, revenue collections had begun to stabilize and states were returning to more “normal” state budget environments, following multiple years of high revenue and spending growth as well as pandemic-related volatility and unpredictability. States appeared to be in a stable fiscal position, though there is variation across states. According to FY 2025 enacted budgets, most states anticipated revenue growth would continue to flatten and state general fund spending growth would slow. While states have made a number of Medicaid investments in recent years, including to expand access to behavioral health services, improve Medicaid reimbursement rates (particularly for long-term care), and to use Medicaid to help address social determinants of health, and reduce health disparities, expectations of reduced revenue collections beyond 2025 may dampen enthusiasm for further investments in Medicaid and could even prompt spending reductions. Reduced state revenues may be tied to implementation of state tax cuts, the expiration of pandemic-era federal funding, and other macroeconomic uncertainties Any reductions in federal Medicaid spending would put further pressure on state budgets and lead to program cuts.
It is unknown whether new administrative actions will undermine efforts to bolster the long-term care workforce. There are also longstanding challenges finding enough workers to provide long-term care for people who need such services, and the COVID-19 pandemic exacerbated those issues considerably. As of February 2024, employment levels in most long-term care settings remained below pre-pandemic levels. The Biden Administration finalized two rules intended to address those challenges and increase access to services. The Administration finalized a rule that would create new staffing requirements in nursing facilities, require state Medicaid agencies to report on the percent of Medicaid payments for institutional long-term care that are spent on compensation for direct care workers and support staff, and provide funding for individuals to enter careers in nursing facilities. The rule will increase the number of staff in many nursing facilities, but also increase Medicaid spending. The Administration also finalized a rule aimed at ensuring access to Medicaid services, which included several provisions aimed specifically at home care, which is long-term care provided in home and community environments. The “access” rule requires states to spend least 80% of total payments for certain home care services on compensation for direct care workers. It’s unknown whether the Trump Administration will implement those rules or revise them, and it is possible Congress will overturn them.
Cuts to Medicaid and changes in immigration policy may exacerbate workforce challenges, reduce payment rates for long-term care workers, and erode supports to family caregivers. In response to workforce challenges, many states have adopted payment rate increases for nursing facilities and home care providers with the goal of boosting staffing levels. All states have also created supports for family caregivers, recognizing that caregiving can be very demanding, particularly when there are shortages of paid caregivers. Those initiatives may be impossible to sustain if federal support for Medicaid is reduced by one third. Beyond reducing Medicaid resources, President Trump’s planned crackdown on immigration may further strain the long-term care workforce, which relies heavily on foreign-born workers.
The issues identified in this policy watch could have major implications for Medicaid coverage, financing, and access to care. As these issues play out, the following key questions will be at the forefront:
With President Trump now in office, his cabinet nominees continue to testify at congressional hearings as part of the nomination process. Robert F. Kennedy Jr. is the nominee to be the secretary of the Department of Health and Human Services (HHS), and his nomination hearings will spotlight a range of HHS activities but may not touch on the full scope of the department’s responsibilities. To better understand HHS’s impact on the health care system and the American people’s coverage, public health, safety, and well-being, what follows is an overview of the activities of the department.
The Department of Health, Education, and Welfare was established in 1953 and evolved into the Department of Health and Human Services in 1980 after the Department of Education was established as an independent entity. A relatively new department of the 15 current executive branch departments, HHS has a Fiscal Year (FY) 2024 budget funding estimated at $1.7 trillion, and the department’s budget is about a quarter of the total FY 2024 U.S. federal budget. It has the largest budget of any federal agency and is the largest grant-making agency.
Most federal executive branch health policy is implemented and managed within HHS, though the White House typically plays a major role in policymaking. The department has 13 operating divisions, most of which have a health focus in areas of coverage, research, regulation, resource delivery, and training. Others are focused on social assistance and support for families and communities in need. More than 80,000 HHS employees are located across the U.S. and the world and half of the workforce is outside the greater Washington, D.C. area.
The Public Health Service (PHS) predates HHS and now exists across ten of the 13 operating divisions within the department:
Led by the Assistant Secretary of Health and the U.S. Surgeon General, the more than 6,000 United States Public Health Service Corps work across HHS and several other federal departments in everyday roles involving their health expertise, but they are also the country’s frontline workers for emergency response including public health emergencies.
The largest division of HHS is the Centers for Medicare and Medicaid Services (CMS), responsible for administering or overseeing health insurance coverage for Medicare, Medicaid, the Children’s Health Insurance Program, and the Affordable Care Act’s Health Insurance Marketplaces. Together, these programs provide health coverage access to 170 million Americans—more than half the population. However, the impact of HHS on the nation’s health insurance system goes well beyond the programs it administers, as it is heavily involved in the federal regulation of private health insurance, including employer-sponsored health insurance covering more than 150 million people, in conjunction with the Departments of Labor and the Treasury.
Beyond the core health insurance programs CMS administers, HHS also supports access to health care services in several other ways. Community health centers provide primary care and some additional services to low-income and uninsured populations and often serve special populations, e.g., people experiencing homelessness, migratory agricultural workers, and rural residents. HHS has a central role in setting standards and providing significant funding through various sources. HHS also provides medical and public health care to American Indians and Alaskan Natives through a network of providers run or contracted by the Indian Health Service. It has programs addressing the needs of specific populations, including the Ryan White HIV/AIDS program, refugee health, mental health and substance use treatment programs, and maternal and child health, to name a few.
The public health role of HHS has been in the spotlight due to the COVID-19 pandemic, but its role during the crisis was based on pre-existing infrastructure and routine activities that adapt to the needs of the day. The department has a long-standing role in monitoring, preventing, and reducing the spread of infectious and non-communicable diseases. Its role encompasses a wide range of responsibilities, including research, screening, policy development and guidance, public education, treatment, and funding for state and local health departments.
Aside from COVID-19, HHS has been active in addressing infectious disease outbreaks of H5N1 avian flu, mpox, and hepatitis A in the past five years and works on long-term challenges like the HIV/AIDS epidemic. The role of HHS in vaccination dates back to the 1950s polio vaccine and it continues to have a substantial role in influencing the country’s vaccine policy.
The routine health activities of HHS often merge with its role in addressing the health impacts of public emergencies and disasters. Events like the September 11, 2001, terrorist attacks, the opioid epidemic, the Flint, Michigan water crisis, natural disasters of hurricanes, tornadoes, and wildfires, and disease outbreaks have all triggered an HHS response in conjunction with other federal agencies.
HHS has provided emergency coordination and strategic planning to set up shelters for acute medical care and mental health support, sometimes utilizing the National Disaster Medical System, accessed stockpiles of critical equipment and medicine, led investigations and expanded on testing and monitoring activities, and assisted with survivor and community recovery including continuity of health care services.
Arguably, the broadest touch point for HHS’ impact on Americans’ daily lives is its role in food safety. The Food and Drug Administration (FDA) oversees most food safety aside from meat and poultry and shares responsibility for egg products with the Department of Agriculture. It also regulates the information about dietary supplements provided to consumers, though it does not have authority to approve them for safety and effectiveness. Among the activities related to food safety are conducting inspections of facilities, labeling requirements, issuing food recalls and alerts, and ensuring imported food meets U.S. standards. However, the FDA isn’t the only HHS agency that plays a significant role in food safety, as the Centers for Disease Control’s broad role of monitoring and responding to disease outbreaks also includes those related to consuming contaminated food.
HHS has a major role in regulating medical drugs and devices, mainly through the FDA. This includes pre-market testing for the safety and effectiveness of a product’s intended use, monitoring of approved products for any harm to consumers, and regulations for producing and labeling such products.
HHS, primarily through the National Institutes of Health, is the world’s largest public funder of health research. While the research often conducted can center on the basics of science and biomedicine, it has led to breakthroughs like the first successful polio vaccine, treatments for cancer and HIV/AIDs, the development of MRI technology, and the ability to personalize medicine because of the mapping of the human genome.
The health of individuals can be impacted by several non-medical factors often categorized as social determinants of health. HHS has a range of social service programs that may not be typically considered health services, but usually factor in the stability of individual and family lives.
Financial assistance for low-income families with children has long been a federal program, and Temporary Assistance for Needy Families (TANF) is the primary cash assistance program for this population. TANF is administered by the HHS Administration of Children and Families (ACF) which also has programs related to child support enforcement, foster care, adoption, and child care. It also promotes early childhood development in low-income children under the age of five through Head Start.
One element of the department’s support services that has gained significant attention over the past decade, particularly as refugee resettlement submissions to the U.S. have sharply increased, is the array of services offered by the Office of Refugee Resettlement (ORR). Established 45 years ago, ORR aims to integrate individuals, including unaccompanied minors, and families into American society and provide a pathway to self-sufficiency. Services offered include financial assistance, housing, medical care, and employment services.
Medicare provides health insurance coverage to 67 million adults—20% of the U.S population—and is a major source of revenue for physicians and other health providers. In 2024, Medicare spending on Part B services (including physician services, outpatient services, and physician-administered drugs) accounted for nearly half (49%) of total Medicare benefit spending. Physicians are not required to participate in Medicare, though the vast majority of them choose to do so.
In recent years, physician groups and some policymakers have raised concerns that physicians would opt out of Medicare due to reductions in Medicare payments for many Part B services, potentially leading to a shortage of physicians willing to treat people with Medicare. Medicare payments are lower, on average, than payments from private insurers and are not automatically indexed to keep pace with inflation in medical practice costs. Every year, as required by law, the Centers for Medicare & Medicaid Services (CMS) updates Medicare payments to physicians under the physician fee schedule through rulemaking. Since 2021, Congress has enacted four temporary, one-year increases to physician payment rates to soften scheduled cuts. However, Congress has not enacted a payment increase for 2025, and a 2.93% drop in average Medicare payments to physicians went into effect on January 1.
Despite these ongoing concerns, virtually all (98%) of non-pediatric physicians participate in the Medicare program. Furthermore, Medicare beneficiaries report access to physician services that is equal to, or better than, that of privately-insured individuals, with similar shares reporting delays in needed care or difficulty finding a physician who takes their insurance.
This brief uses the most recent CMS data to document the extent to which non-pediatric physicians have opted out of Medicare, by specialty and by state, as of November 2024, updating prior KFF analyses. (See Methods for details).
Key Takeaways:
Currently, physicians and other health providers seeking payment from Medicare for Part B services must enroll as a Medicare provider. Physicians may either agree to be a participating provider or non-participating provider. Providers who do not want to enroll in Medicare or receive Medicare payments are required to sign an “opt out” agreement with their patients.
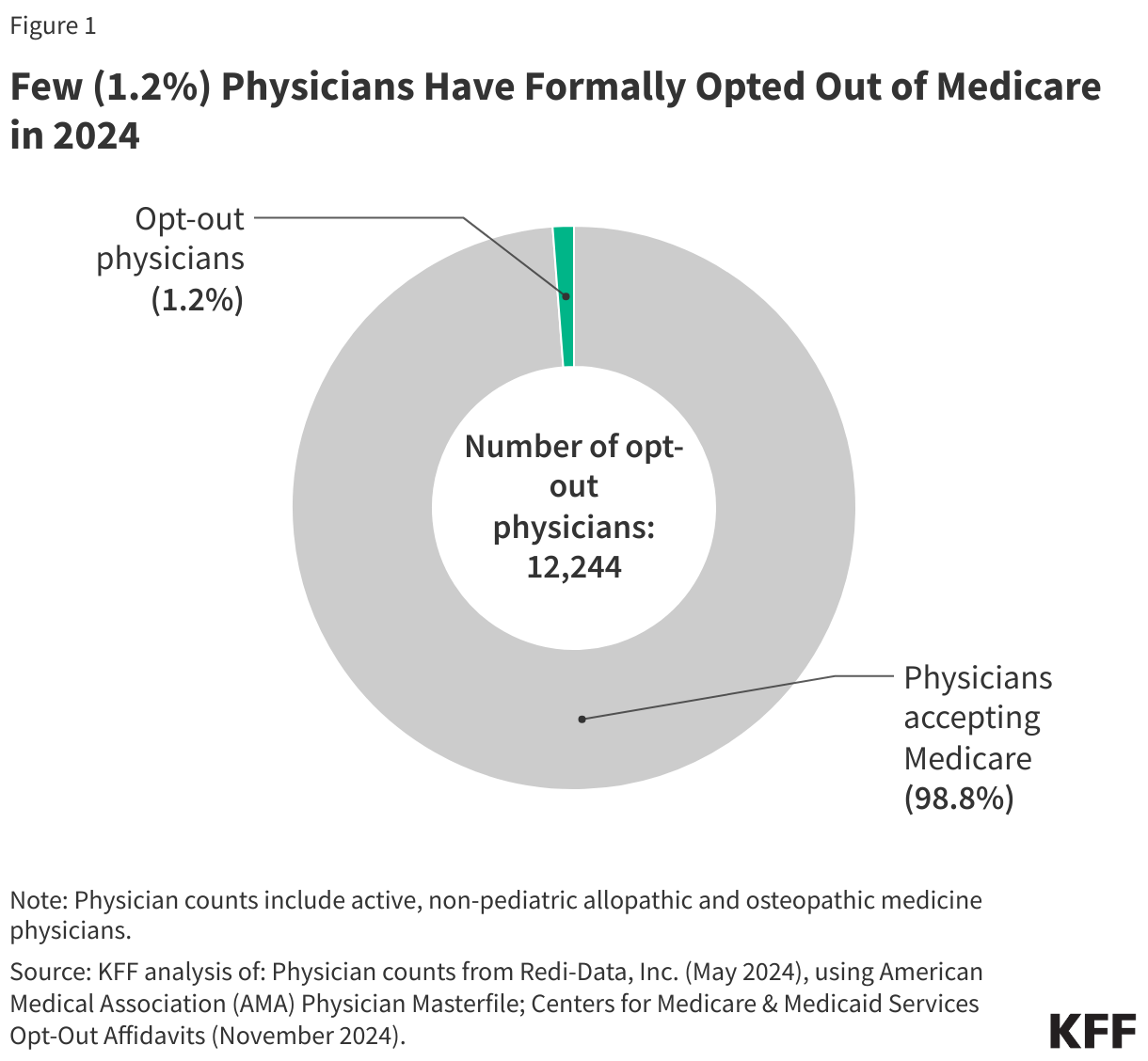
1.2 percent of non-pediatric physicians have formally opted out of the Medicare program. As of November 2024, 12,244 non-pediatric physicians have opted out of Medicare, representing a very small share (1.2%) of the total number active physicians, similar to the shares reported in 2013 and 2022 (Figure 1).
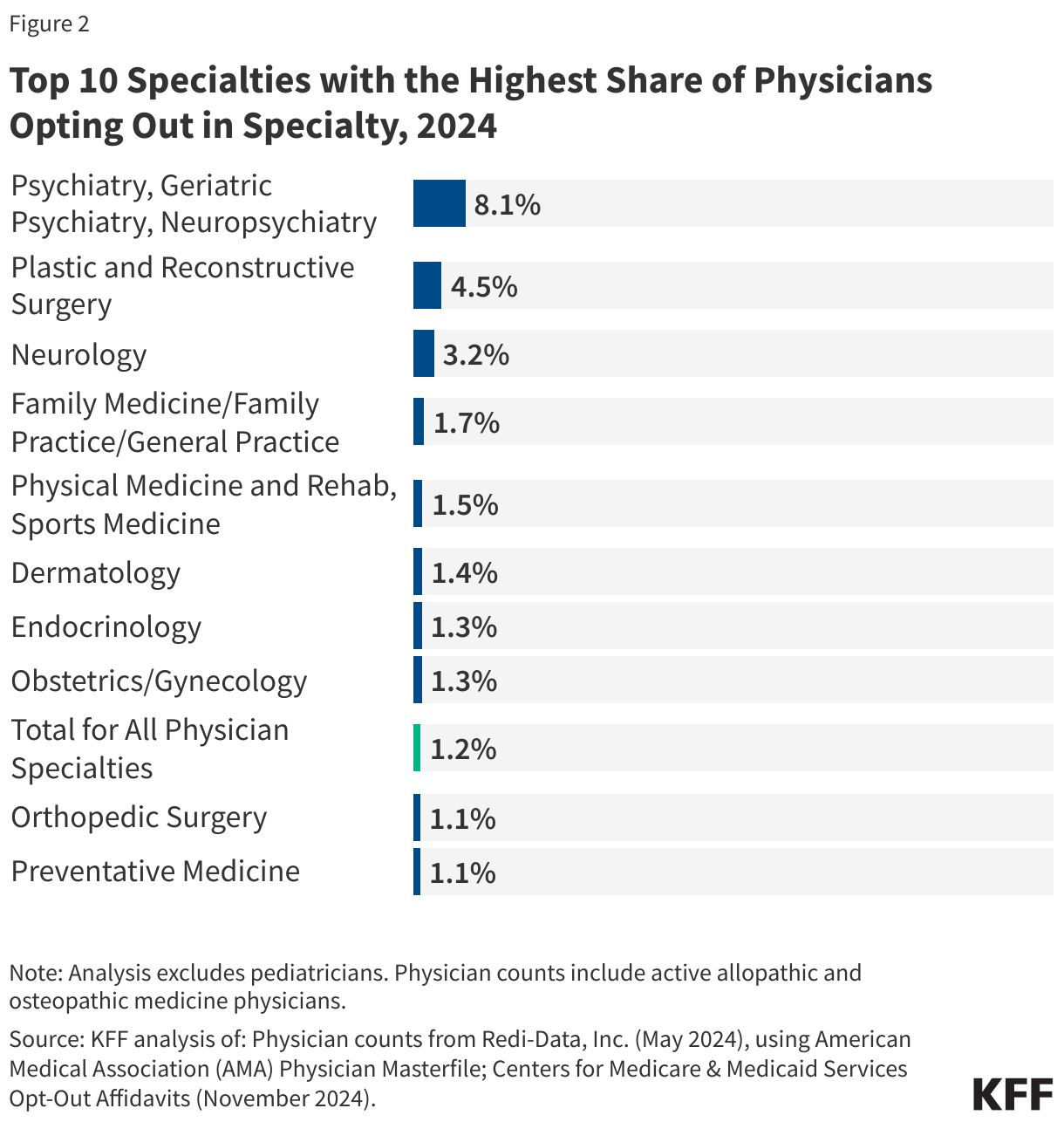
While the overall opt-out rate is low, opt-out rates are somewhat higher for certain specialties, such as psychiatry and plastic and reconstructive surgery. In 2024, 8.1% of psychiatrists have opted out of Medicare, followed by 4.5% of physicians specializing in plastic and reconstructive surgery and 3.2% of physicians specializing in neurology (Figure 2).
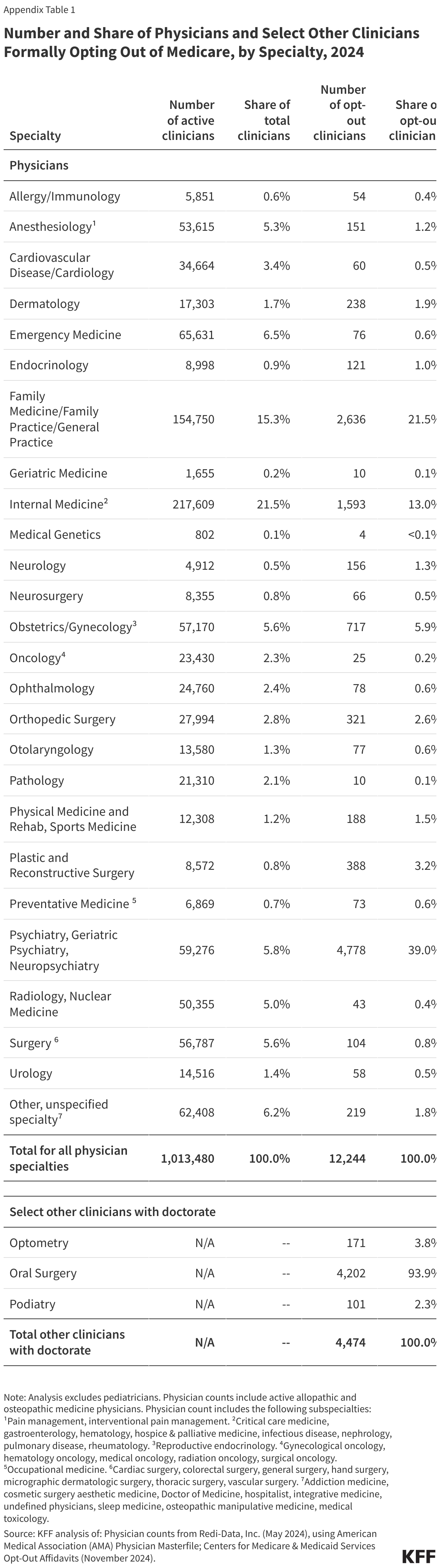
On the other hand, of the 26 specialty groups included in this analysis, 11 have opt-out rates that are 0.5% or lower, with the lowest rates seen among physicians specializing in emergency medicine (0.1%), oncology (0.1%), radiology (0.1%), and pathology (<0.1%) (Appendix Table 1).
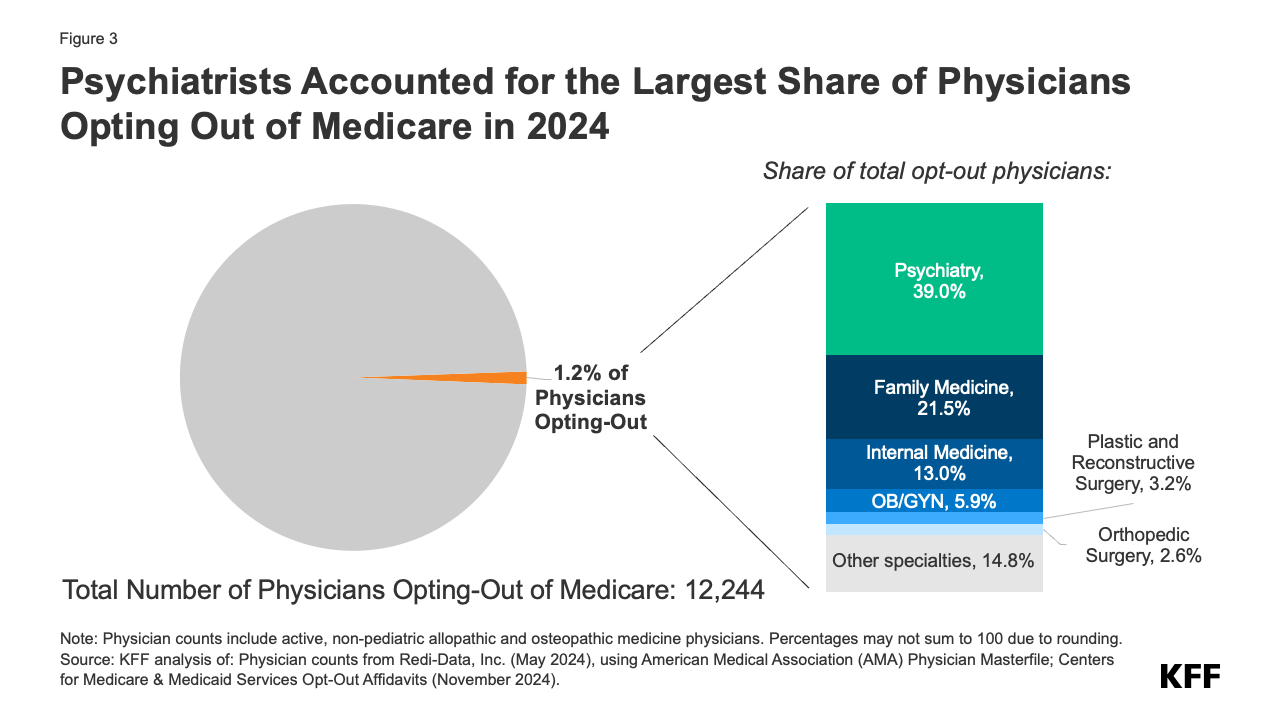
Psychiatrists are disproportionately represented among the 1.2 percent of active physicians who have opted out of Medicare. Psychiatrists account for the largest share (39.0%) of opt-out physicians, followed by physicians in family medicine (21.5%), internal medicine (13.0%), and obstetrics/gynecology (5.9%) (Figure 3). This is consistent with prior analyses that found that psychiatrists are less likely than other physician specialties to accept new patients with Medicare or private insurance, suggesting that psychiatrists may prefer to be paid directly by their patients, in order to avoid the administrative burden of submitting claims to insurers and maintain the flexibility to charge higher fees.
In addition to physicians, another 4,474 select clinical professionals with doctorate degrees (i.e. oral surgeons, podiatrists, and optometrists) have also opted out of the Medicare program, with oral surgeons accounting for the vast majority (93.9%) of this group (Appendix Table 1).
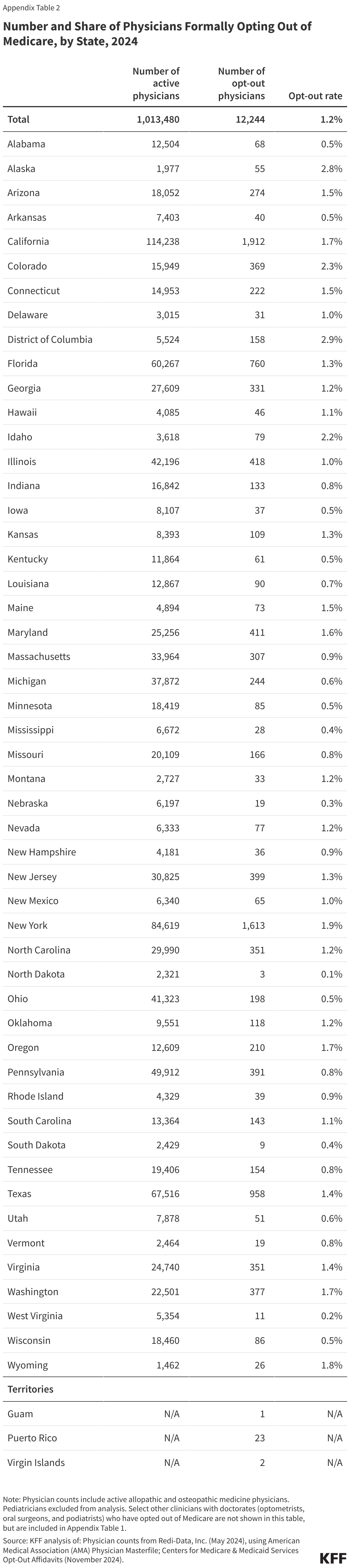
Less than two percent of physicians have opted out of Medicare in all but three states and the District of Columbia. As of November 2024, the District of Columbia (2.9%), Alaska (2.8%), Colorado (2.3%), and Idaho (2.2%) have the highest rates of non-pediatric physicians who have opted out of Medicare (Figure 4). In twelve states (Alabama, Arkansas, Iowa, Kentucky, Minnesota, Mississippi, Nebraska, North Dakota, Ohio, South Dakota, West Virginia, and Wisconsin) the opt-out rate is 0.5% or lower (Appendix Table 2).
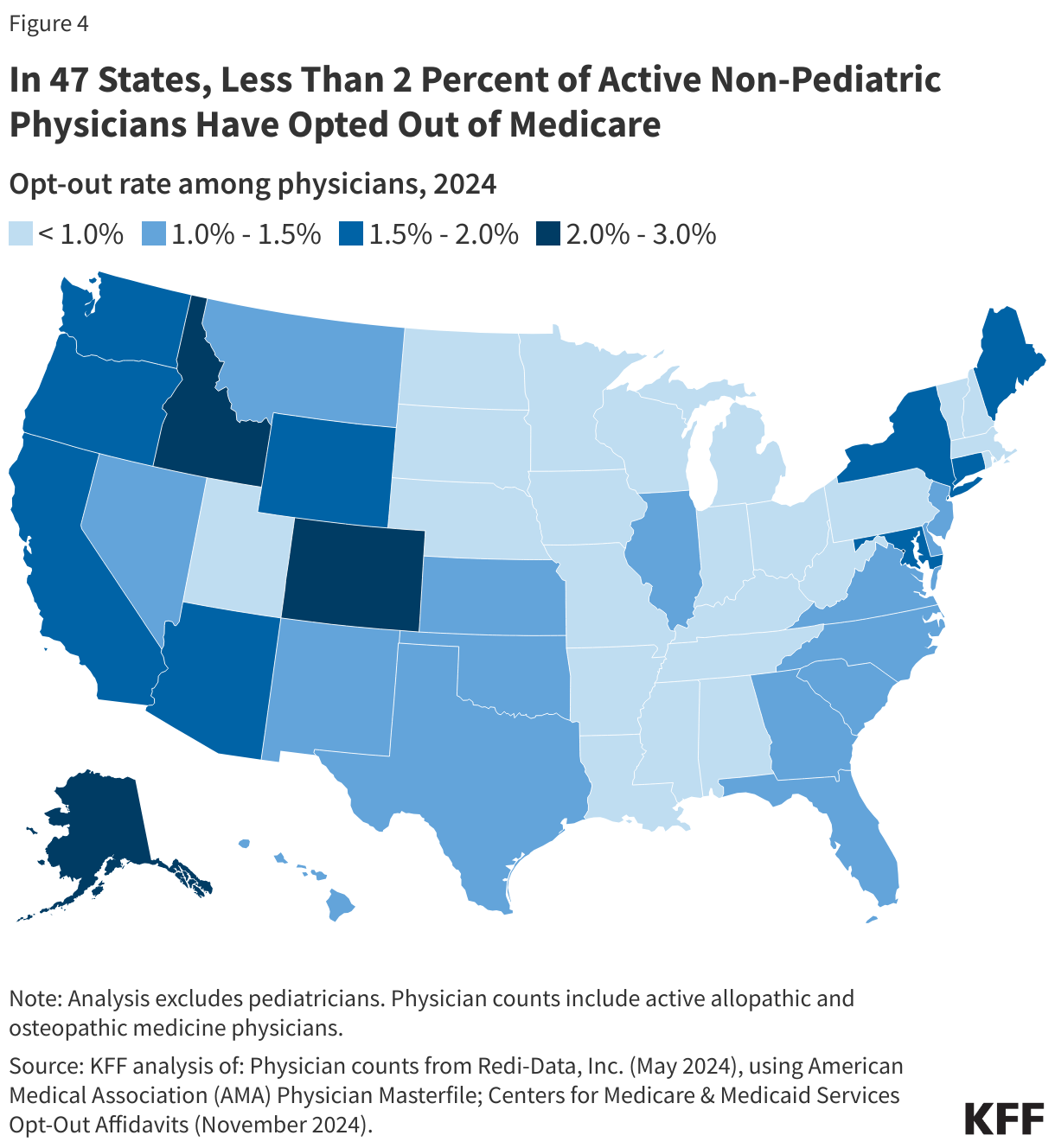
Due to data limitations, this analysis only includes opt-out rates at the state level. Opt-out rates may vary based on rural status and other county-level factors, and some counties may have opt-out rates that are higher than the state average.
Methods
This analysis uses Medicare opt-out affidavit data from the Centers for Medicare & Medicaid Services (CMS), as of November 2024. The scope of this analysis was limited to non-pediatric physicians, given its Medicare focus, as well as a select group of other clinicians with doctorates: optometrists, oral surgery, and podiatrists. Therefore, pediatricians and other non-physician specialists, such as certified nurse midwives, clinical social workers, and physician assistants, were excluded from the total number of opt-out physicians. Of note, while some clinicians under the oral surgery specialty group may also hold a medical degree (MD or DO), for the purpose of this analysis, these physicians were grouped in accordance with the primary specialty (oral surgery) associated with their National Provider Identifier (NPI) in CMS’ opt-out file.
This analysis obtained data on the number of active allopathic and osteopathic physicians by specialty and state from Redi-data, Inc, which utilizes data from the American Medical Association (AMA) Physician Masterfile. One limitation of this analysis is that due to data source limitations, it was not possible to exclude active physicians involved in professional activities other than patient care, such as research and administration. We were also unable to examine opt-out rates based on the ownership characteristics of physicians (e.g., hospital-owned vs physician-owned practices). Further, we were unable to examine out-out rates by rural status due to lack of county-level opt-out data.
The specific physician specialty groups identified in this analysis were selected if they were included in the list of opt-out providers provided by CMS. In order to gain a more complete picture of the distribution of opt-out providers in each specialty category, this analysis grouped some subspecialties under a broader specialty category, consistent with the specialty cross-walk provided by Redi-Data, Inc. More specifically, anesthesiology includes pain management and interventional pain management, obstetrics and gynecology includes reproductive endocrinology, and preventive medicine includes occupational medicine. The internal medicine category includes the following subspecialties: internal medicine (not otherwise specified), critical care medicine, gastroenterology, hematology, hospice & palliative medicine, infectious disease, nephrology, pulmonary disease, and rheumatology. The surgery category includes the following subspecialties: cardiac surgery, colorectal surgery, general surgery, hand surgery, micrographic dermatologic surgery, thoracic surgery, and vascular surgery. The following subspecialties are included in the “other” category: addiction medicine, cosmetic surgery aesthetic medicine, Doctor of Medicine, hospitalist, integrative medicine, undefined physicians, sleep medicine, osteopathic manipulative medicine, and medical toxicology.
Title 42 of the Public Health Services Act is a public health authority that authorizes the Director of the Centers for Disease Control and Prevention (CDC) to suspend entry of individuals into the U.S. to protect public health. This rarely utilized authority was implemented by the Trump administration in March 2020 in response to the COVID-19 pandemic to allow for quick expulsion of migrants, including asylum seekers, seeking entry into the U.S. at the land borders. After a series of delays due to court challenges, the restrictions were lifted when the Biden Administration declared an end to the COVID-19 public health emergency (PHE) on May 11, 2023. The Biden administration subsequently took increasingly restrictive executive action to restrict border entry.
Land border entries into the U.S. decreased as a result of Title 42 since individuals who had border encounters under this authority were immediately expelled due to the public health threat outlined by the Trump administration. However, research suggests that Title 42 restrictions did not result in a “better managed border” and increased cases of unauthorized re-entry, and public health experts stated that it put the health and well-being of migrants at risk. Recent reports suggest President-elect Trump may reinvoke Title 42 restrictions during his second term to close the border between the U.S. and Mexico, along with a number of other actions to restrict immigration.
This brief provides an explanation of Title 42 and its application in border regions, the impact of Title 42 on border expulsions and the health and well-being of migrants during COVID-19, and a discussion of the potential implications of reinvoking Title 42 restrictions for immigration and the health of migrants.
Under U.S. immigration law, individuals have a legal right to claim asylum when presenting at U.S. ports of entry. An asylee is an individual already present in the U.S. or seeking admission at a port of entry who is seeking protection based on “persecution or a well-founded fear of persecution on account of their race, religion, nationality, membership in a particular social group, or political opinion.” In fiscal year (FY) 2023, the U.S. granted asylum to over 54,000 individuals from close to a dozen different countries. However, as of October 2024, over 90% of asylum cases filed in FY 2023 were still pending with only 2% being granted approval due to immigration backlogs.
Migrants encountered at the border are processed and screened for asylum under Title 8 of the U.S. Code addressing “Aliens and Nationality.” Under Title 8, those determined to have a credible fear of persecution or other threats in their home country are either held in custody or released into the U.S. while their case is pending in immigration court. Those who the U.S. Citizenship and Immigration Services (USCIS) determine not to have a credible fear are permitted to appeal this decision to an immigration judge. If an individual chooses not to appeal or the immigration judge did not find fear, then the individual is removed.
In June 2024, the Biden administration took executive action to suspend and limit the entry of migrants at the southern border, including asylum seekers, to “address the historic levels of migration and more efficiently process migrants arriving at the southern border.” Under this rule, the suspension of entry will go into effect immediately after there have been 2,500 or more average daily border encounters (not including unaccompanied children) over seven consecutive days and can be lifted once there have been fewer than 1,500 average daily border encounters over seven consecutive days. As of April 2024, there were about 4,000 average daily border encounters, leaving the restrictions in place. U.S. Customs and Border Patrol (CBP) data show that border encounters following the executive order were at a three-year low with there being a 29% reduction in encounters between May and June 2024.
In March 2020, the Trump administration implemented Title 42 under the Public Health Service Act, which allowed for the immediate expulsion of migrants without screening for asylum. This order applied to all migrants arriving to the U.S. from Canada or Mexico regardless of their country of origin who would otherwise be held in a congregate setting at a port of entry or border patrol station. It did not apply to lawful permanent residents and their families, members of the armed forces or their families, or people who hold valid travel documents such as tourists or those in a visa waiver program. Officials also had authority to make exceptions for individuals on a case-by-case basis. Under this order, the CDC Director was authorized to “suspend the introduction of persons into the United States” and CBP officials were directed to process migrants promptly (within 15 minutes in an outdoor setting) without screening for asylum and expel them back to Mexico or Canada or their country of origin. The CDC stated the purpose of the order was to protect CBP personnel, U.S. citizens, lawful permanent residents, and other individuals from an increase in COVID-19 spread at land ports of entry, Border Patrol stations, and in the interior of the country. The order pointed to the introduction of individuals into congregate settings at the border and the increased strain this would put on the U.S. health care system during a public health emergency as primary reasons for implementing the restrictions on entry.
Title 42 continued to be enforced under the Biden administration until the end of the COVID-19 PHE declaration in May 2023. However, unaccompanied minors were exempted from the order based on a district court ruling in November 2020 and by a CDC order issued under the Biden administration in February 2021. The CDC order continued to apply the original Title 42 order to single adults and families. After facing legal challenges, Title 42 restrictions were lifted in May 2023 following the end of the COVID-19 PHE declaration.
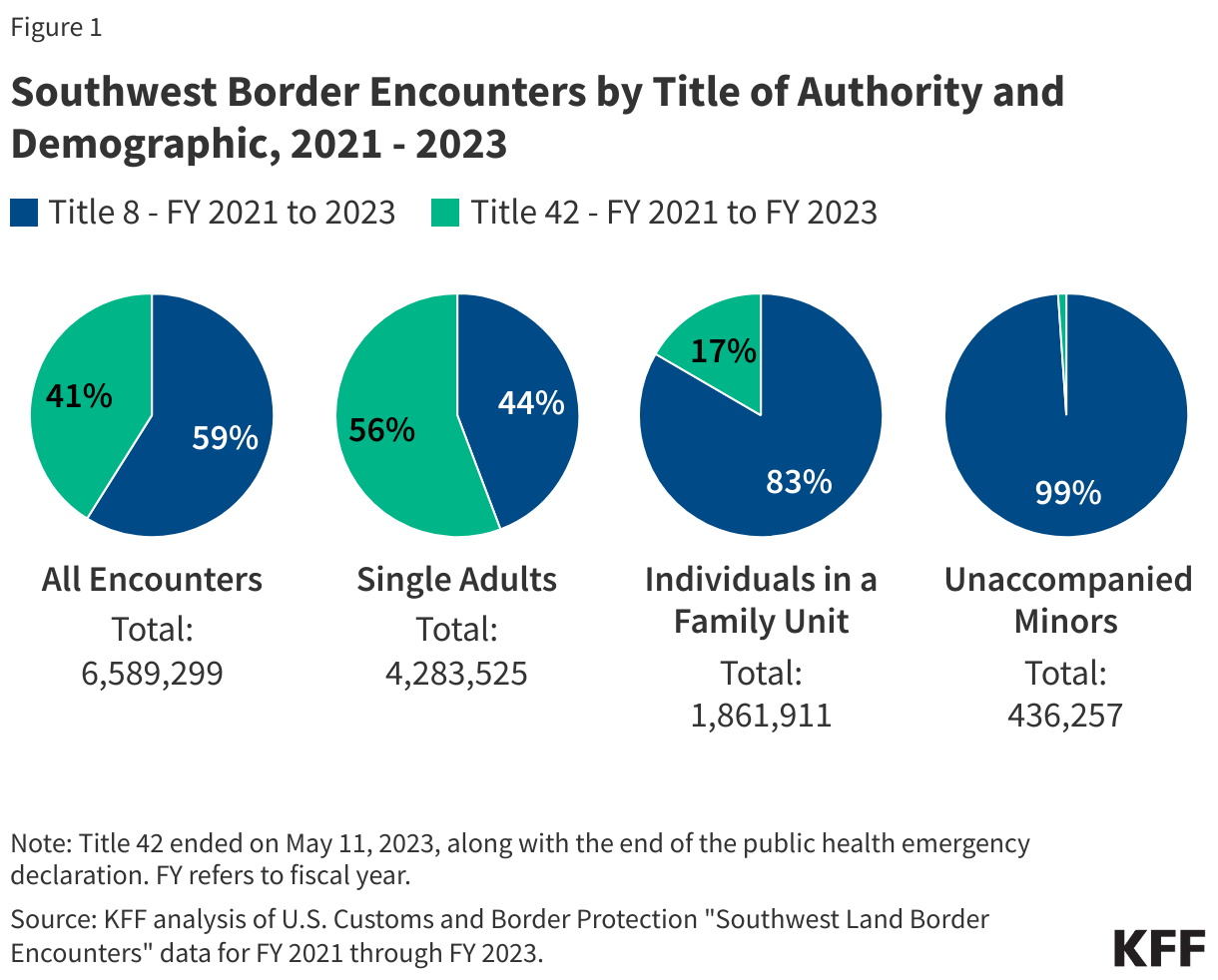
Between FY 20211 and 2023, there were over 6.5 million encounters at the Southwest land border of which about four in ten (41%) were under Title 42 authority. Enforcement encounters refer to “apprehensions or inadmissibles processed under CBP’s immigration authority;” these include individuals apprehended under Title 8 as well as individuals expelled under Title 42. While Title 42 applies to both the Northern and Southwestern Borders, nearly all Title 42 encounters occurred at the Southwestern Border. Between FY 2021 and FY 2023, Title 42 encounters at the Southwest Border accounted for about four in ten (41%) of all Southwest Border encounters. The share of encounters that were under Title 42 varied by demographic group with Title 42 accounting for a majority (56%) of single adult encounters and one in six (17%) family encounters, while Title 8 accounted for virtually all (99%) encounters with unaccompanied minors reflecting their exemption from expulsion under Title 42 (Figure 1).
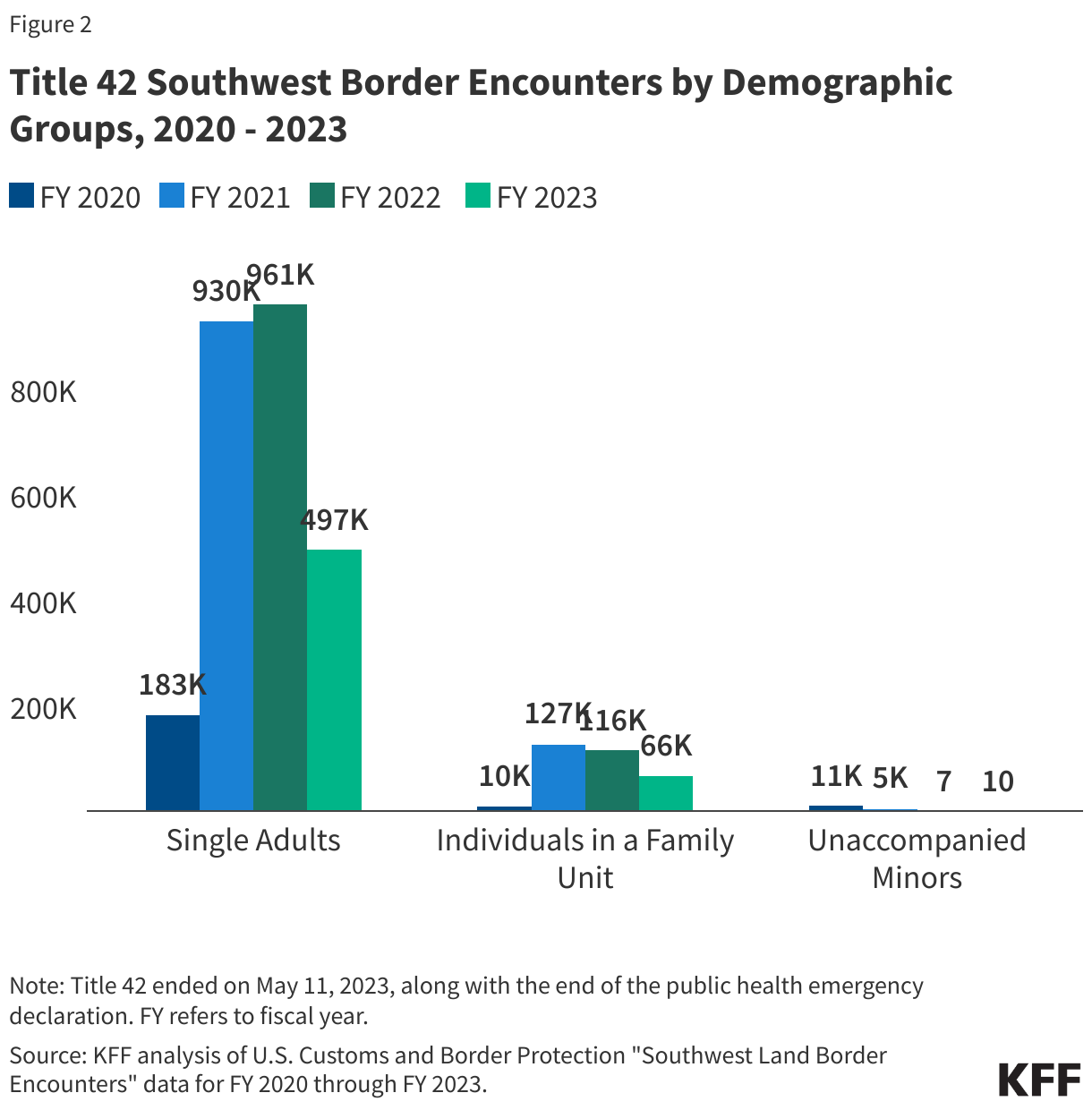
As of May 2023, there were over 2.5 million single adult expulsions, nearly 320,000 expulsions of individuals in a family unit, and nearly 16,000 expulsions of unaccompanied minors under Title 42. The number of family expulsions under Title 42 grew between FY 2020 and FY 2021, while expulsions of unaccompanied minors decreased, reflecting their exemption beginning in February 2021. These encounter counts reflect repeat encounters with individuals, as each attempt by the same individual to cross the border is counted as a new encounter.
Data indicate that Title 42 did not lead to a reduction in border encounters, but border entries into the U.S. went down due to the nature of the authority. While Title 42 was intended to reduce COVID-19 exposure risk at the border, it led to an increasing number of encounters at the border largely due to repeat encounters. This is in large part because, unlike Title 8, migrants apprehended under Title 42 were immediately expelled and those with repeat encounters did not face any penalties. Data from 2020 through 2023 suggest that while there were close to 3 million Southwest border expulsions under Title 42 authority, many of those expulsions were of the same individuals making repeated attempts to cross the border. In the last 6 months of 2021, a quarter of the encounters under Title 42 were of the same individuals on multiple occasions, with recidivism rates under the authority being at their highest levels in over a decade. In addition, there has not been a significant increase in border encounters since Title 42 was lifted with border encounters in FY 2024 (2.1 million) being lower than border encounters in FY 2022 (2.4 million) and FY 2023 (2.5 million). However, entries into the U.S. through land borders decreased as a result of Title 42 since individuals who had border encounters under this authority were immediately expelled due to the public health threat outlined by the Trump administration.
Research suggests Title 42 expulsions negatively impacted the health and well-being of migrant families while having little to no impact on preventing the spread of COVID-19 in the U.S. Physicians, epidemiologists, and public health experts repeatedly stated that Title 42 was counterproductive to preserving health and protecting individuals from COVID-19. Physicians suggested that being in close proximity with other individuals while being temporarily detained or transported back to Mexico, lack of medical screenings, and lack of provision of necessary medication could have adverse impacts on physical and mental health. Typically, the CDC recommends that asylees be provided an initial medical screening within 30-60 days of arriving in the U.S., but since Title 42 called for immediate expulsion, such screenings were not provided. Interviews conducted with over two dozen asylum seekers who were expelled under Title 42 authority found that a vast majority reported symptoms of depression, anxiety, and post-traumatic stress disorder (PTSD), and many reported that their children’s mental health was also impacted. Sending individuals back to potentially dangerous situations they were fleeing also poses risks. Title 42 may also have contributed to increases in family separations at the border. Media reports suggested that some families were separating from their children so that the children could seek entry as unaccompanied minors, who were exempt from Title 42 expulsions. These separations may have led to children facing dangerous situations traveling to the border and expose them to trauma and toxic stress. The impact of Title 42 on migrant families may also have been exacerbated by the “Remain in Mexico” or Migrant Protection Protocols program implemented under the first Trump administration, which required thousands of migrants (including children) to wait for their U.S. immigration court hearings in Mexican border towns that can be dangerous and unsafe. Close to 80% of migrants receiving medical treatment from Doctors without Borders/Medecins Sans Frontieres at border locations in Nuevo Laredo, Mexico, reported being victims of violence, with many experiencing depression, severe anxiety, and post-traumatic stress.
The incoming Trump administration has indicated plans to reinvoke Title 42. President-elect Trump has proposed an array of policies focused on restricting immigration. Recent reports suggest that the incoming Trump administration is planning to reinvoke Title 42 to restrict immigration under the rubric of public health protection. Experiences during COVID-19 suggest Title 42 was not effective at reducing border encounters or preventing COVID-19 and had negative health impacts for migrants. Reinvocation of such a policy also raises questions about its use as a border enforcement tool and could potentially fuel xenophobic sentiment towards immigrants.
As President-elect Trump takes office on January 20th with Republican majorities in both chambers of Congress, the public is sending mixed messages on how they prioritize key components of the Trump administration’s health agenda. While Americans across partisanship largely embrace prioritizing increased regulation and oversight such as boosting price transparency rules and setting stricter limits on chemicals in the food supply, there are other aspects of the Republican agenda the public does not support – most notably, reducing federal funding to Medicaid.
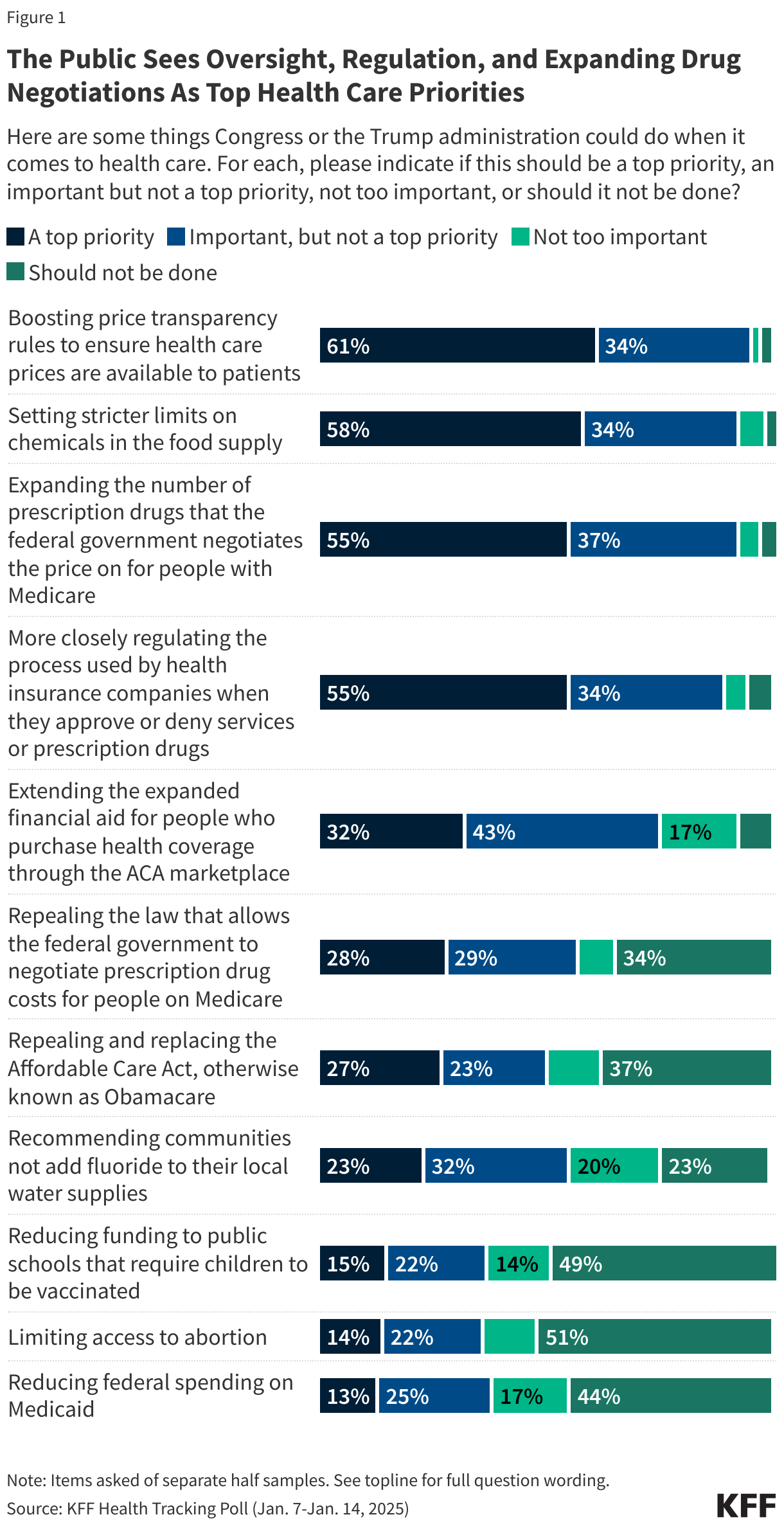
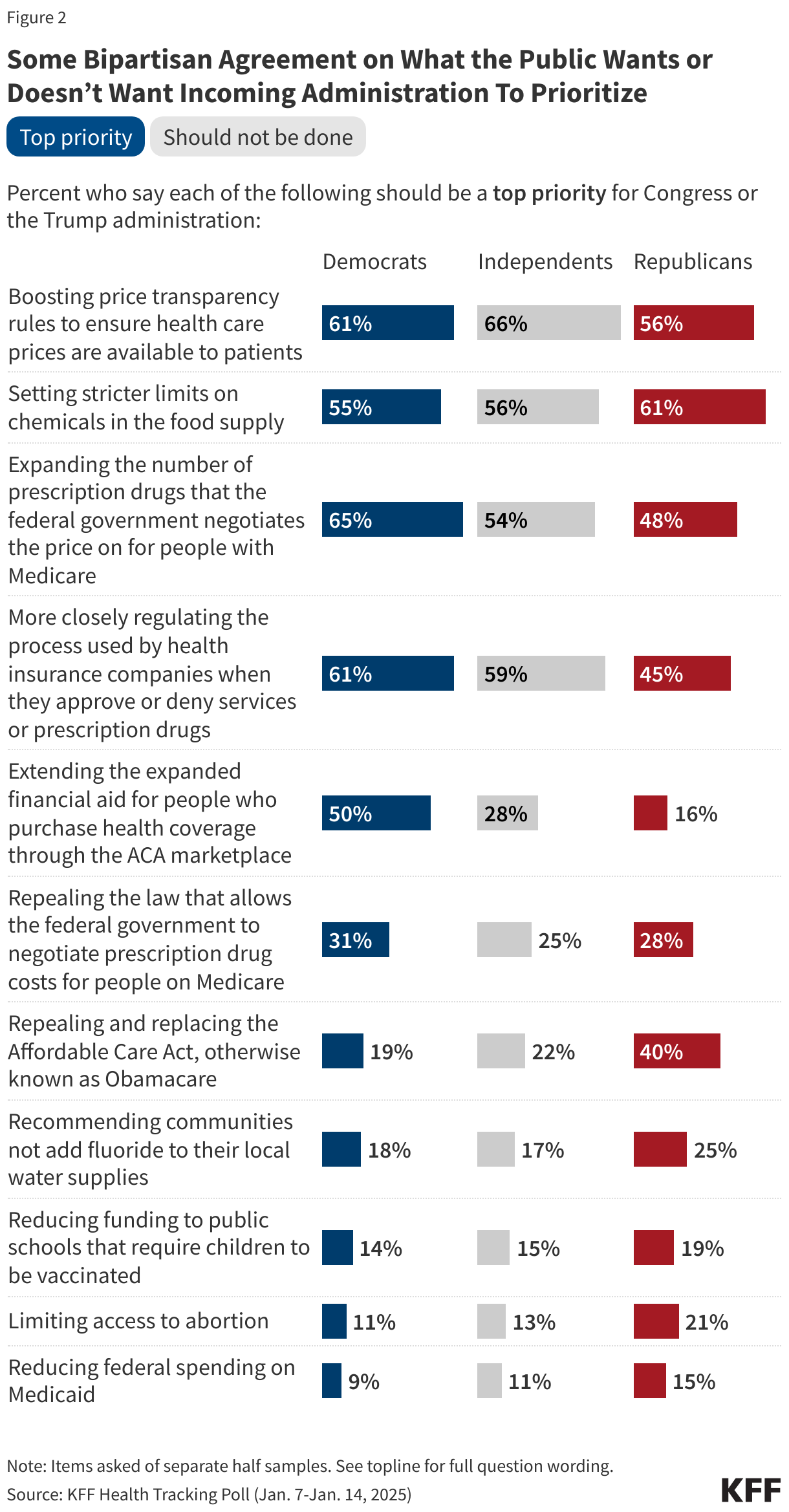
When asked about a variety of health care proposals, including those put forth by Republican and Democratic lawmakers, about six in ten say boosting price transparency rules to ensure health care prices are available to patients (61%) should be a “top priority,” and a similar share say the same about setting stricter limits on chemicals found in the food supply (58%). A majority (55%) also say more closely regulating the process used by health insurance companies when they approve or deny services or prescription drugs is a top priority. Overall, while health care ranks lower than other policy areas such as immigration, foreign policy, and the economy; majorities of the public – including half or more across partisanship – say each of these should be a “top priority” for Congress and the new Trump administration.
When it comes to proposed changes to two key health care legislations: the Inflation Reduction Act’s provisions to allow the federal government to negotiate the Medicare price of prescription drugs as well as the 2010 Affordable Care Act (ACA), larger shares of the public support actions to expand or strengthen these laws rather than repealing them. More than half of the public (55%) say expanding the number of prescription drugs subject to Medicare price negotiation should be a top priority, twice the share who prioritize rolling back this provision (28%). On the ACA, about a third (32%) prioritize extending the enhanced subsidies for people who buy their own health coverage while a quarter of the public (27%) say repealing and replacing the ACA is a top priority.
Other health care issues, many of which may be the focus of the Trump administration, are seen as even lower priorities for the incoming administration with substantial shares of the public saying they “should not be done.” Less than a quarter of the public think changing recommendations for fluoride in local water supplies (23%) should be a “top priority,” which is identical to the share who say it should not be done. Less than one in eight say reducing federal funding to schools that require vaccinations (15%), limiting abortion access (14%), and reducing federal funding on Medicaid (13%) should be top priorities. At least four in ten of the public say each of these “should not be done” by Congress or the Trump administration.
Robert F. Kennedy Jr., President Trump’s choice for head of the Department of Health and Human Services has long touted the need for a complete overhaul of U.S. food policy including cracking down on ultra-processed foods and food dyes. This focus on limiting chemicals in the public’s food supply is echoed in the public’s list of top health care priorities, with majorities across partisans saying it should be a top priority for the new Trump administration and Congress. More than half of Republicans (61%), independents (56%), and Democrats (55%) say setting stricter limits on chemicals in the food supply should be a “top priority” for Congress or the Trump administration.
Majorities of Democrats and independents also say oversight – both boosting price transparency rules to ensure health care prices are available to patients and more closely regulating health insurance companies’ approval or denial of care – should be a top priority for lawmakers. This increased oversight on hospital pricing and insurance companies is also seen as a priority among large shares Republicans (56% and 45%, respectively). Partisans also hold similar views on whether expanding the number of drugs subject to Medicare price negotiation should be a priority, with about half of Republicans (48%) saying this should be a “top priority,” as do nearly two-thirds of Democrats (65%).
There is also bipartisan agreement on what shouldn’t be a top health care priority for lawmakers. Few Democrats, independents, or Republicans think the incoming administration should prioritize changing recommendations for fluoride in local water supplies, reducing federal funding to schools that require vaccinations, limiting abortion access, or reducing federal funding for Medicaid.
On the other hand, views on the future of the 2010 Affordable Care Act continue to be partisan. Repealing the ACA continues to rank as a priority for Republicans (40% say it is a “top priority” in the most recent tracking poll), but it has dropped as priority among the total public (down 10 percentage points), and among Republicans specifically (down 23 percentage points), since the start of the first Trump administration. Democrats, on the other side of the political aisle, are more likely to prioritize extending the Biden-era enhanced ACA marketplace subsidies. Half of Democrats say this should be a “top priority” compared to just about one in six Republicans.
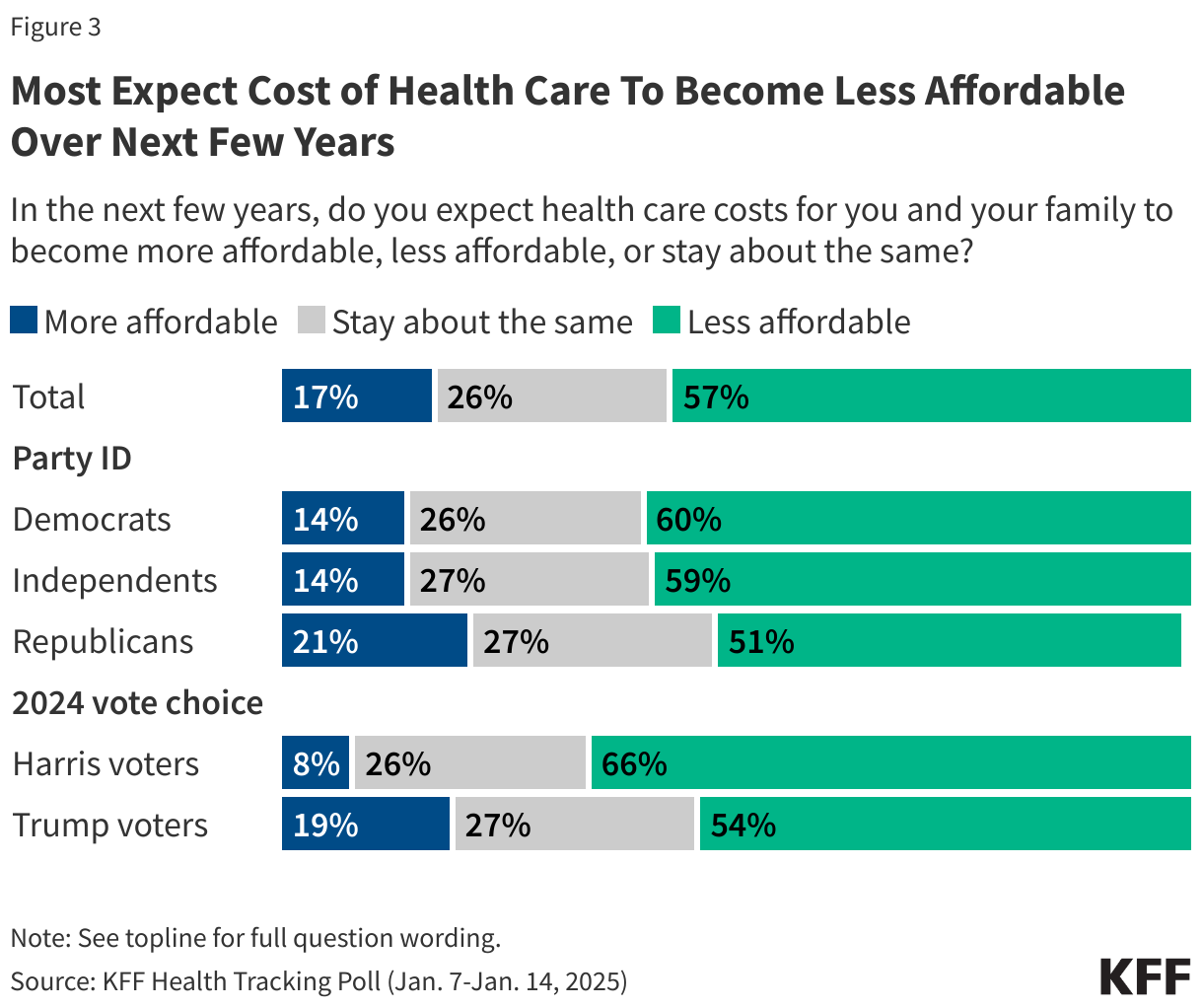
Throughout the 2024 presidential campaign, voters consistently said they were most interested in electing a candidate who could reduce their health care costs. President Trump largely capitalized on voters’ economic concerns and his own record to convince voters that he was the candidate most adept at taking on the high cost of health care. Yet, few Americans now expect health care costs for them and their family members to become more affordable over the next few years. In fact, more than half (57%) of the public – including 54% of Trump voters – say they expect the cost of health care to become “less affordable.” Majorities of Democrats (60%), independents (59%), as well as half of Republicans (51%) all expect health care costs for them and their family members to become less affordable in the coming years.
With the Trump administration’s focus on tax cuts and border security, House Republicans have been coming up with plans to pay for these which may include reducing spending on government health programs such as Medicare, Medicaid, and the Affordable Care Act. Yet, changes to these programs may run up against public sentiment according to the latest KFF Tracking Poll.
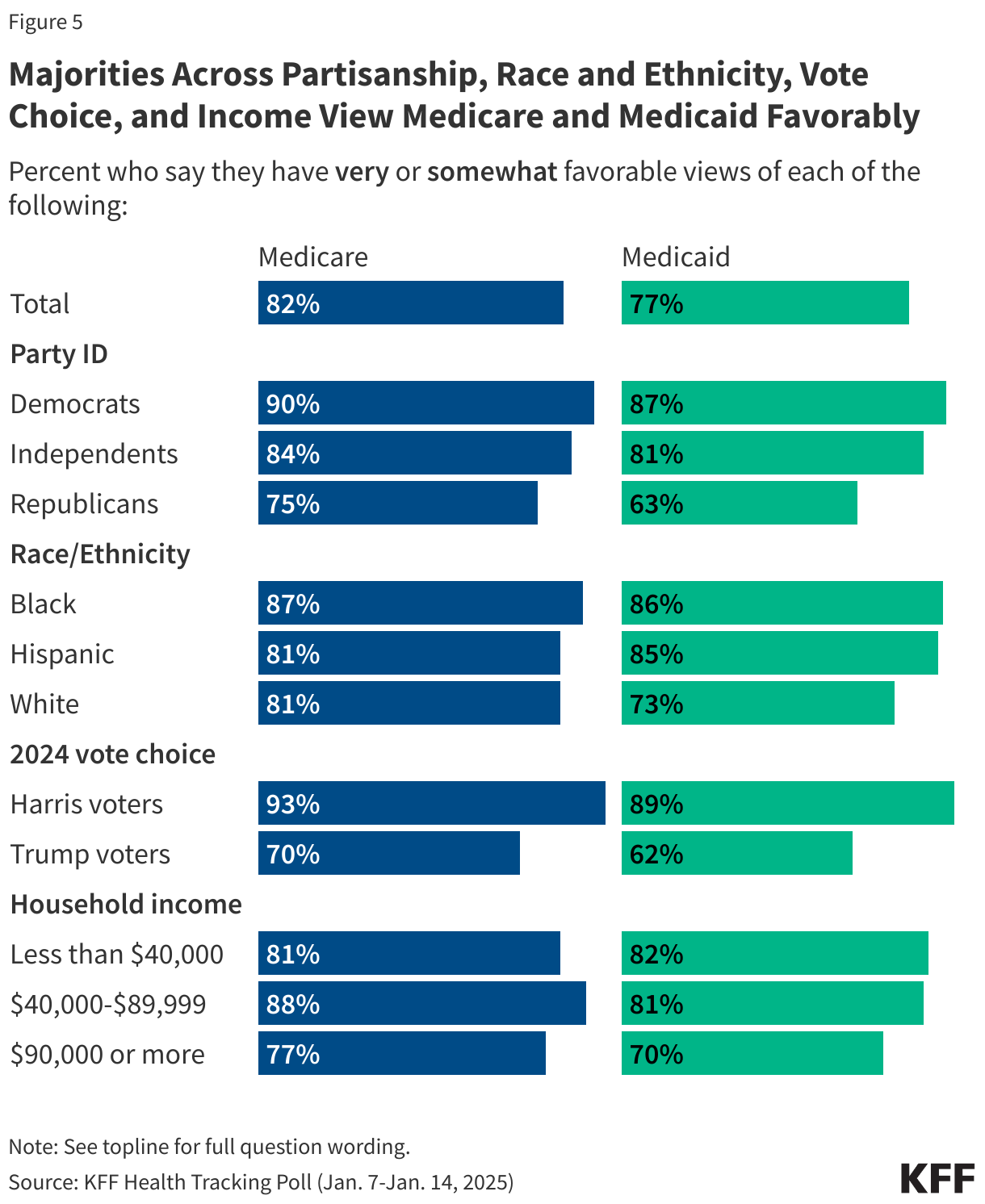
KFF has asked the public about their attitudes about both Medicaid and Medicare for more than two decades, and these two programs continue to be overwhelmingly popular among the public. In the most recent poll, about eight in ten (82%) Americans hold favorable views of Medicare and more than three-fourths (77%) hold favorable views of Medicaid.
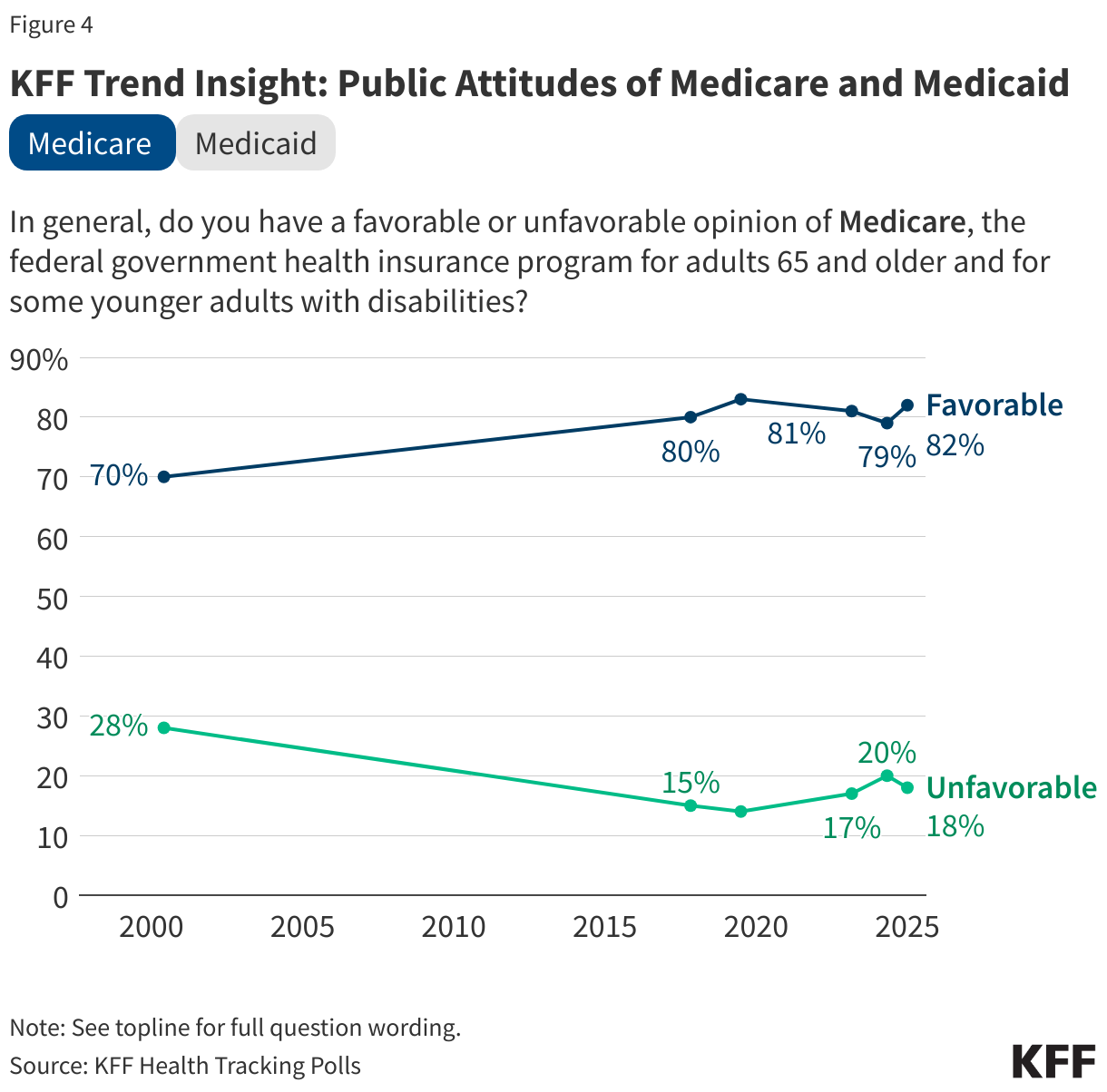
Medicare, the federal government health insurance program for adults 65 and older and some younger adults with disabilities, has maintained favorability among eight in ten adults for nearly a decade. In the January KFF Health Tracking Poll, the share who say they view the program favorably includes three-fourths of Republicans (75%) and more than eight in ten independents (84%), and Democrats (90%). This also includes 94% of the individuals who are currently enrolled in the Medicare program.
Similarly, Medicaid, the federal-state government health insurance program for certain low-income individuals and long-term care program, is also very popular with three-fourths of adults (77%) holding favorable views, including six in ten Republicans (63%), and at least eight in ten independents (81%) and Democrats (87%). Medicaid is also popular among those enrolled in the program with 84% saying they view the program favorably.
Notably, both programs are also viewed favorably by a majority of voters who say they voted for President Trump in the 2024 election.
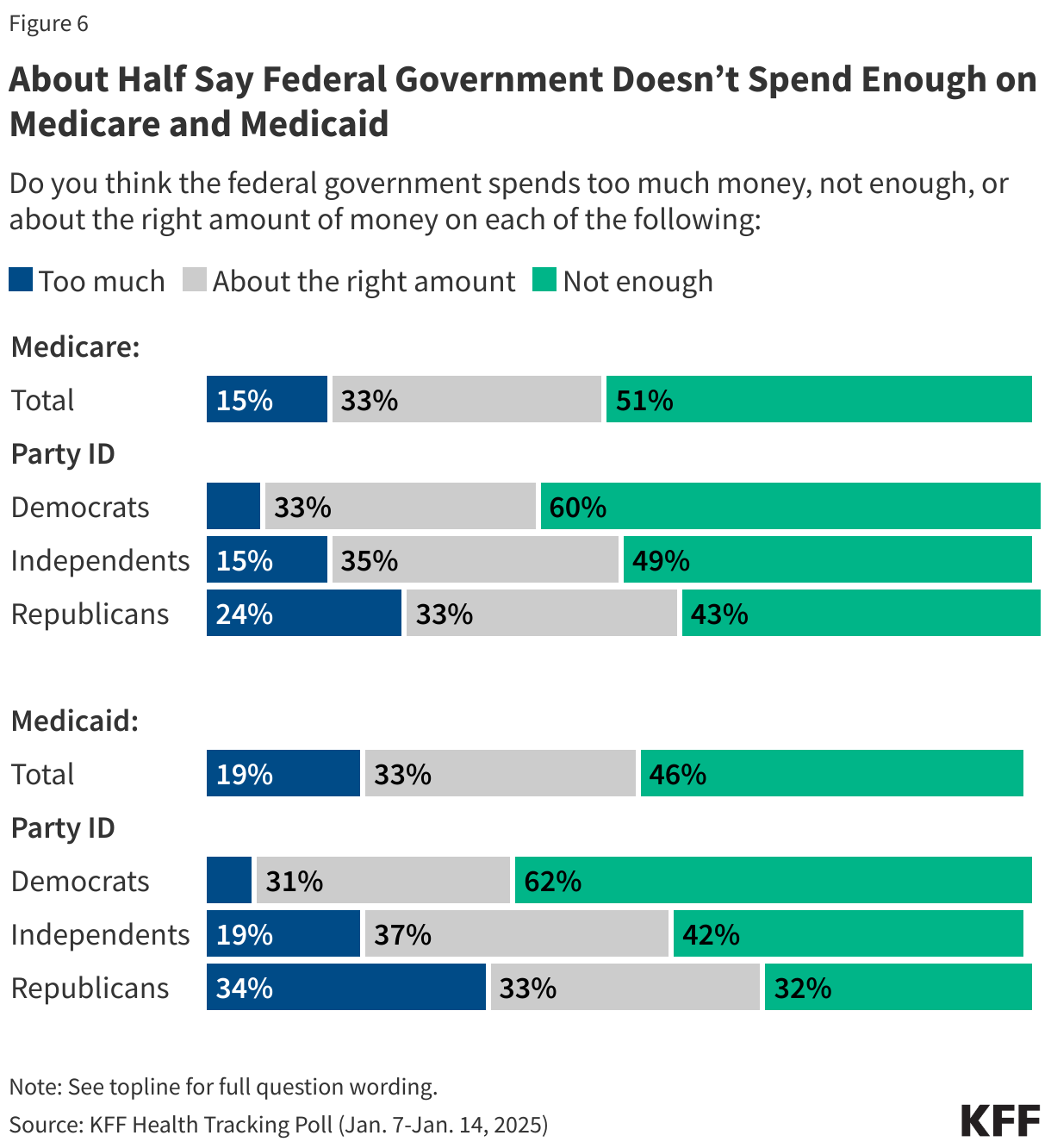
While lawmakers are discussing changes to these programs including significant cuts to Medicaid, about half of the public actually think the federal government isn’t spending enough on either of these programs. About half of the public (51%) say the federal government spends “not enough” on Medicare, while one-third say the government spends “about the right amount” and about one in seven (15%) say the government spends “too much.” A majority of Democrats (60%) and pluralities of independents (49%) and Republicans (43%) say the federal government doesn’t spend enough on Medicare.
Nearly half (46%) say the federal government doesn’t spend enough on the Medicaid program, with another third saying it spends “about the right amount” and around one in five (19%) saying it spends “too much.” While most Democrats (62%) say the federal government doesn’t spend enough, Republicans are a bit more divided with about similar shares of Republicans saying the government spends “too much” (34%), “not enough” (32%), or “about the right amount” (33%) on Medicaid.
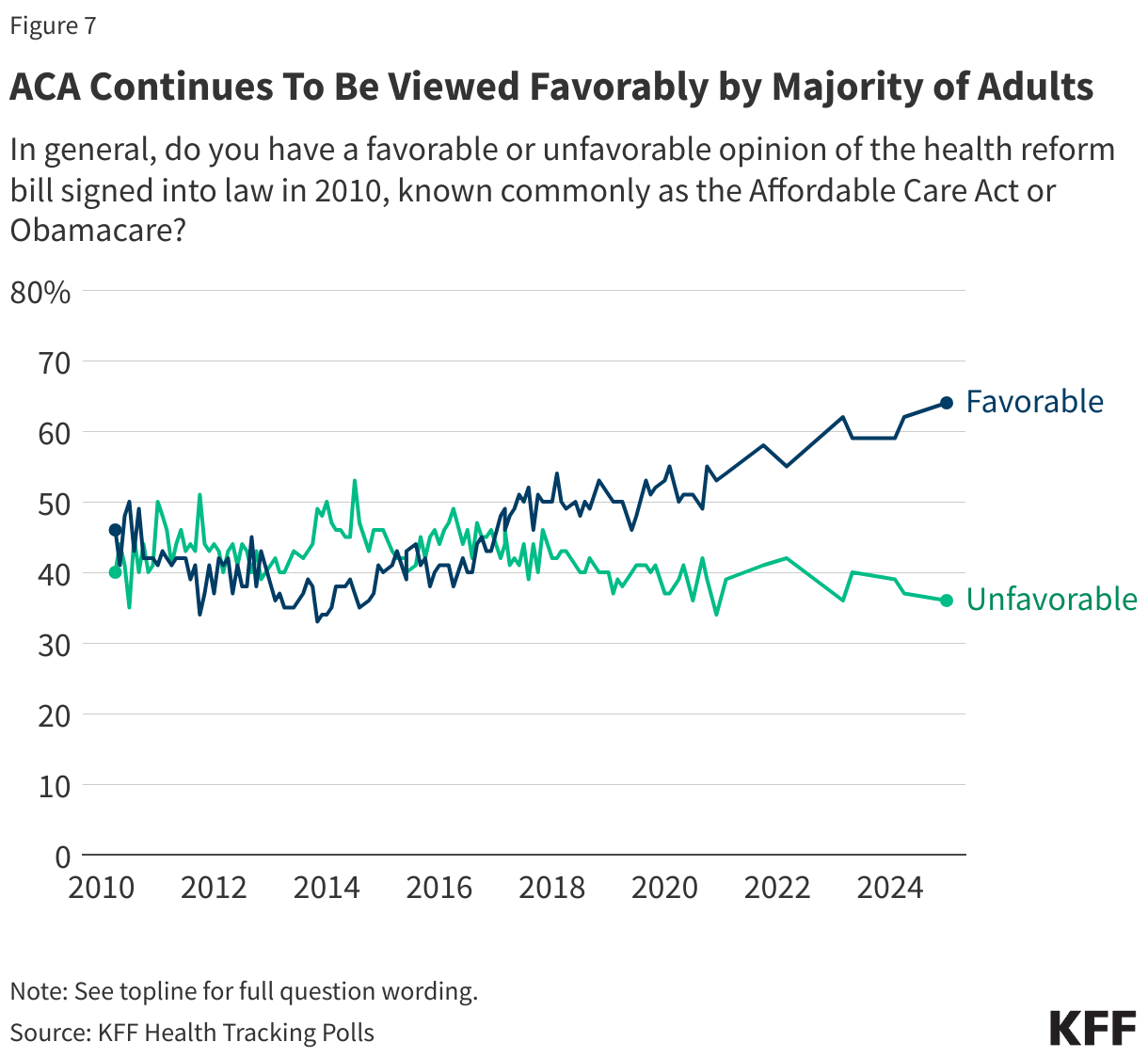
The Affordable Care Act, the Obama-administration health insurance program that was a frequent target of the first Trump administration, also continues to be popular – although to a somewhat lesser degree than Medicaid or Medicare. Nearly two-thirds of the public (64%) view the 2010 ACA favorably while less than four in ten (36%) say they hold an unfavorable view of the law. The share of the public who views the law unfavorably continues to be largely made up of Republicans, with about three-fourths (72%) saying they have an unfavorable view. ACA favorability increased substantially during the 2017 repeal efforts, and has maintained majority support throughout the past four years of the Biden administration.
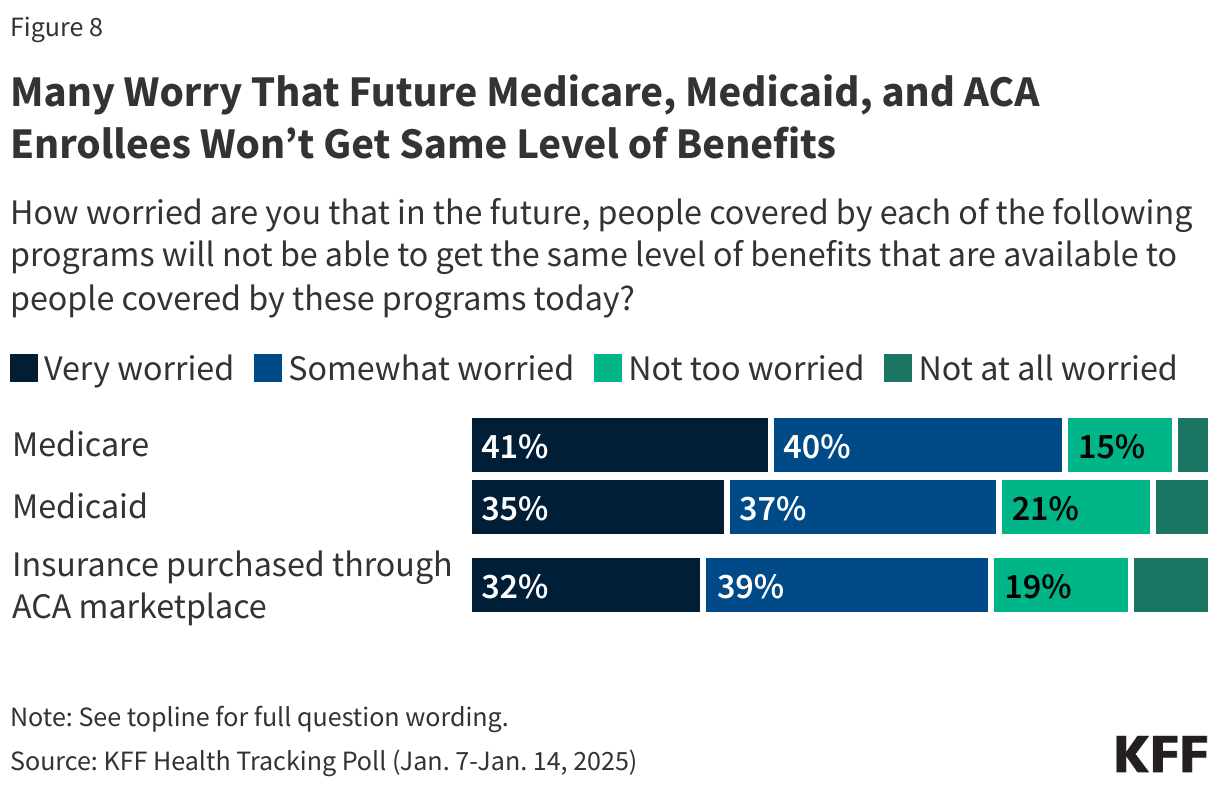
With possible changes to all three government health programs, the public is worried that people covered by each of these programs in the future will not be able to get the same level of benefits that are available today. About eight in ten (81%) say they are either “very worried” or “somewhat worried” that Medicare enrollees will not get the same level of benefits in the future. This includes more than eight in ten (82%) individuals who are currently covered by the program as well as about nine in ten adults (88%) who will be eligible for the program in the coming years, those between the ages of 50 and 64.
In addition, seven in ten are worried about the level of benefits that will be available to people covered by Medicaid (72%) and people who buy their own coverage through the ACA marketplaces (70%). Both Medicaid and the ACA have repeatedly been discussed as possible focuses of the incoming Trump administration and Congressional Republicans.
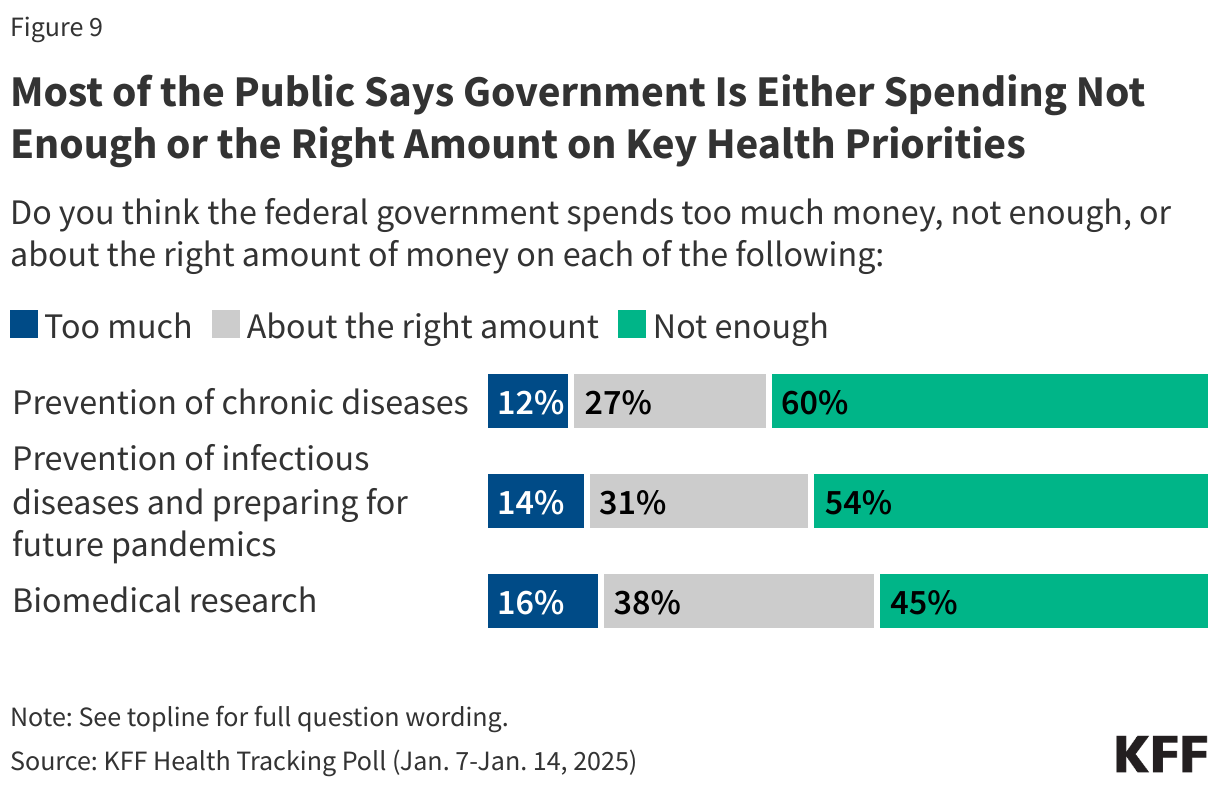
As the Trump administration is balancing spending priorities, the public thinks the government isn’t spending enough on many facets of public health, including both the priorities of RFK Jr, Trump’s pick to lead HHS, and the priorities of Congressional Republicans.
Most of the public says the government is spending “not enough” on the prevention of chronic diseases (60%) or prevention of infectious diseases and preparing for future pandemics (54%). More than four in ten said the government was spending “not enough” (45%) on biomedical research, while 38% said it was spending “about the right amount.” Smaller shares say the federal government is spending “too much” on each of the key health priorities asked about.
One of the Trump administration’s promises has been to cut excessive government spending, including reducing fraud and waste across various sectors of the government. As the newly-formed “Department of Government Efficiency” or DOGE begins work, the public is concerned about the impact that government efficiency efforts will have on people who get their health insurance through Medicare or Medicaid.
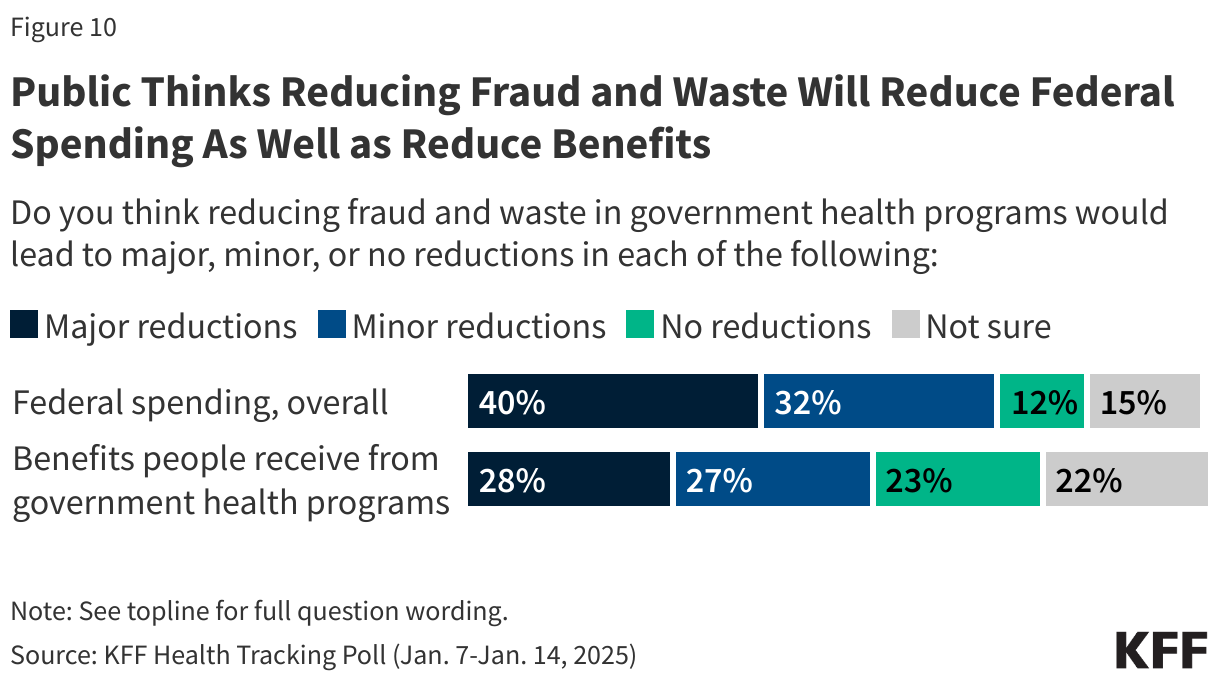
Overall, the public thinks that reducing fraud and waste in government health programs could lead to reductions in overall federal spending – which is the goal of the government efficiency program, but many also think it will result in a reduction of benefits. Four in ten say reducing fraud and waste in government health programs could lead to “major reductions” in federal spending with an additional third (32%) saying it could lead to “minor reductions.” This includes majorities across partisans (80% of Republicans, 68% of Democrats, and 72% of independents) who say reducing fraud and wasted could reduce overall federal spending.
Yet, more than half (55%) of the public also say reducing fraud and waste could lead to reductions in the benefits people receive from the programs. More than a quarter (28%) of the public say that reducing fraud and waste will lead to “major reductions,” with an additional quarter who say it will lead to “minor reductions” in benefits. Once again, more than half across partisans (60% of Republicans, 55% of Democrats, and 51% of independents) say that reducing fraud and waste will lead to reduced benefits.
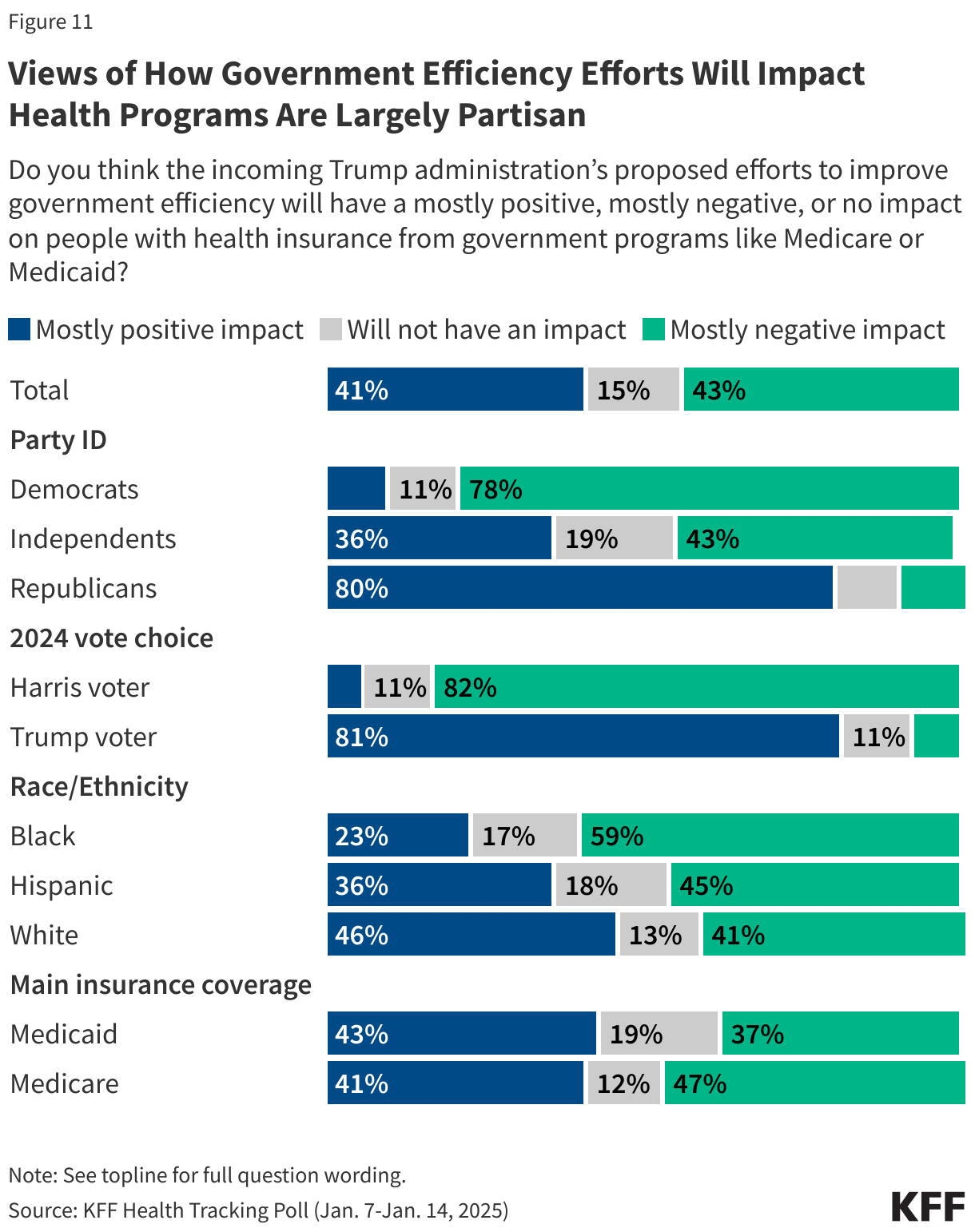
The public is largely divided on whether the incoming Trump administration’s proposed efforts to improve government efficiency will have a negative or positive impact on people who get health coverage through Medicare or Medicaid. Similar shares say the impact will be “mostly negative” (43%) and “mostly positive” (41%), while 15% say there won’t be any impact. Views of the impact are highly partisan, with large majorities of Democrats (78%) saying there will be a mostly negative impact, and most Republicans (80%) say there will be a mostly positive impact. Independents are more divided, but a larger share say there will be a mostly negative impact (43%).
This KFF Health Tracking Poll was designed and analyzed by public opinion researchers at KFF. The survey was conducted January 7-14, 2025, online and by telephone among a nationally representative sample of 1,310 U.S. adults in English (1,233) and in Spanish (77). The sample includes 1,024 adults (n=48 in Spanish) reached through the SSRS Opinion Panel either online (n=999) or over the phone (n=25). The SSRS Opinion Panel is a nationally representative probability-based panel where panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails.
Another 286 (n=29 in Spanish) interviews were conducted from a random digit dial telephone sample of prepaid cell phone numbers obtained through MSG. Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity groups within each frame.
Respondents in the phone samples received a $15 incentive via a check received by mail. SSRS Opinion panelists who completed the survey by phone were offered $10 via a mailed check and those who completed online received $5 via e-gift card. In order to ensure data quality, cases were removed if they failed two or more quality checks: (1) attention check questions in the online version of the questionnaire, (2) had over 30% item non-response, or (3) had a length less than one quarter of the mean length by mode. Based on this criterion, no cases were removed.
The combined cell phone and panel samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2024 Current Population Survey (CPS), September 2023 Volunteering and Civic Life Supplement data from the CPS, and the 2024 KFF Benchmarking Survey with ABS and prepaid cell phone samples. The demographic variables included in weighting for the general population sample are sex, age, education, race/ethnicity, region, civic engagement, frequency of internet use, political party identification by race/ethnicity, and education. The weights account for differences in the probability of selection for each sample type (prepaid cell phone and panel). This includes adjustment for the sample design and geographic stratification of the cell phone sample, within household probability of selection, and the design of the panel-recruitment procedure.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. KFF public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
| Group | N (unweighted) | M.O.S.E. |
| Total | 1,310 | ± 3 percentage points |
| . | ||
| Party ID | ||
| Democrats | 403 | ± 6 percentage points |
| Independents | 383 | ± 6 percentage points |
| Republicans | 383 | ± 6 percentage points |
With the incoming Trump administration and Republican-led Congress looking to ways to reduce federal spending, a new KFF Health Tracking Poll finds that the Medicare and Medicaid programs remain broadly popular, and more people favor more spending on those programs than less spending.
About eight in 10 Americans overall view Medicare (82%) and Medicaid (77%) favorably. This includes majorities across partisans, including most Republicans (75% view Medicare favorably and 63% view Medicaid favorably).
About half (46%) of the public say the federal government doesn’t spend enough on Medicaid, more than twice the share (19%) who say the government spends “too much.” The gap is even larger for Medicare, with half (51%) of the public saying the government doesn’t spend enough compared to 15% who say the government spends too much.

The Affordable Care Act (ACA), sometimes called Obamacare, also remains popular, with nearly two thirds (64%) of the public holding favorable views, though with more of a partisan divide. Most Democrats and independents hold favorable views of the ACA, while about three quarters of Republicans (72%) hold unfavorable views.
Large majorities also say they are “very” or “somewhat” worried that people covered by each of the three programs in the future won’t get the same benefits available today. This includes 81% who say so about Medicare, 72% who say so about Medicaid, and 70% who say so about the ACA marketplaces. Republicans are less worried than other partisans about Medicaid and the ACA.
Ahead of President Trump’s inauguration, the poll also assesses how the public prioritizes 11 potential actions on health that the new administration and Congress could take.
About six in 10 say that boosting price transparency rules (61%) and limiting chemicals in the food supply (58%) are both a “top priority.” This includes majorities of Republicans, independents and Democrats.
During his first administration, President Trump issued federal regulations establishing price transparency requirements for hospitals and insurers, and Robert F. Kennedy Jr., his pick to head the U.S. Department of Health and Human Services, has long advocated against chemicals in food.
In contrast, few among the public rank several other health policies associated with President Trump and his allies as top priorities.
For example, about one in seven say that reducing federal spending on Medicaid (13%) or limiting access to abortion (14%) is a top priority, while much larger shares say each of these “should not be done” (44% and 51%, respectively). Other low-ranking priorities include cutting funding to schools that require students to get vaccinated (15%), encouraging communities not to add fluoride to their water supply (23%), and repealing and replacing the ACA (27%).
Among other health priorities:
The incoming Trump administration has established a new “Department of Government Efficiency,” or DOGE, charged with developing plans to cut federal spending and reduce regulations.
Most Americans (73%) say that reducing fraud and waste in government health programs would lead to “major” or “minor” reductions in federal spending overall. This includes most Republicans (80%), independents (72%), and Democrats (68%).
At the same time, more than half (55%) of the public also say that reducing fraud and waste would lead to reductions in the benefits that people receive from government health programs. At least half of Republicans (60%), Democrats (55%), and independents (51%) hold this view.
Other findings include:
Designed and analyzed by public opinion researchers at KFF. The survey was conducted Jan. 7-14, 2025, online and by telephone among a nationally representative sample of 1,310 U.S. adults in English and in Spanish. The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on other subgroups, the margin of sampling error may be higher.
VOLUME 14
This is Irving Washington and Hagere Yilma. We direct KFF’s Health Information and Trust Initiative and on behalf of all our colleagues at KFF, we’re pleased to bring you this edition of our bi-weekly Monitor.
This volume examines misleading claims about birth control, focusing on the distortion of emergency contraceptives, such as Plan B, as abortifacients. It also explores how social media and patient-provider communication shape perceptions of hormone-based contraceptives’ safety and effectiveness, particularly in response to online messaging that inaccurately promotes fertility awareness methods as safer alternatives.

Emergency contraception (EC) and intrauterine devices (IUDs) are safe, effective methods for preventing pregnancy, but some anti-abortion groups misrepresent these methods, particularly EC, as abortifacients. These claims are rooted in the misconception that these methods can terminate an existing pregnancy, prevent the implantation of a fertilized egg, or affect a developing embryo. Despite the FDA clarifying in 2022 on the Plan B label that it does not block implantation, misinformation persists. This narrative has fueled opposition to policies that expand access to contraceptives, with some lawmakers claiming to support birth control but also embracing policies rooted in these false claims. KFF policy experts explain that these misconceptions underpin legal and legislative challenges. For example, in the Supreme Court case Burwell v. Hobby Lobby Stores, Inc. (2014), the plaintiffs successfully argued that covering IUDs and EC under the ACA violated their religious beliefs, claiming that they “believed” that these methods are abortifacients. In 2024, similar misinformation threatened the adoption of state legislation in Missouri and Louisiana aimed at improving contraception access, as some lawmakers expressed concerns these methods may induce abortions. The Missouri legislation ultimately passed after delays attributed to concerns from anti-abortion groups, but the proposed Louisiana law failed to advance after its introduction.
KFF Data Insights:
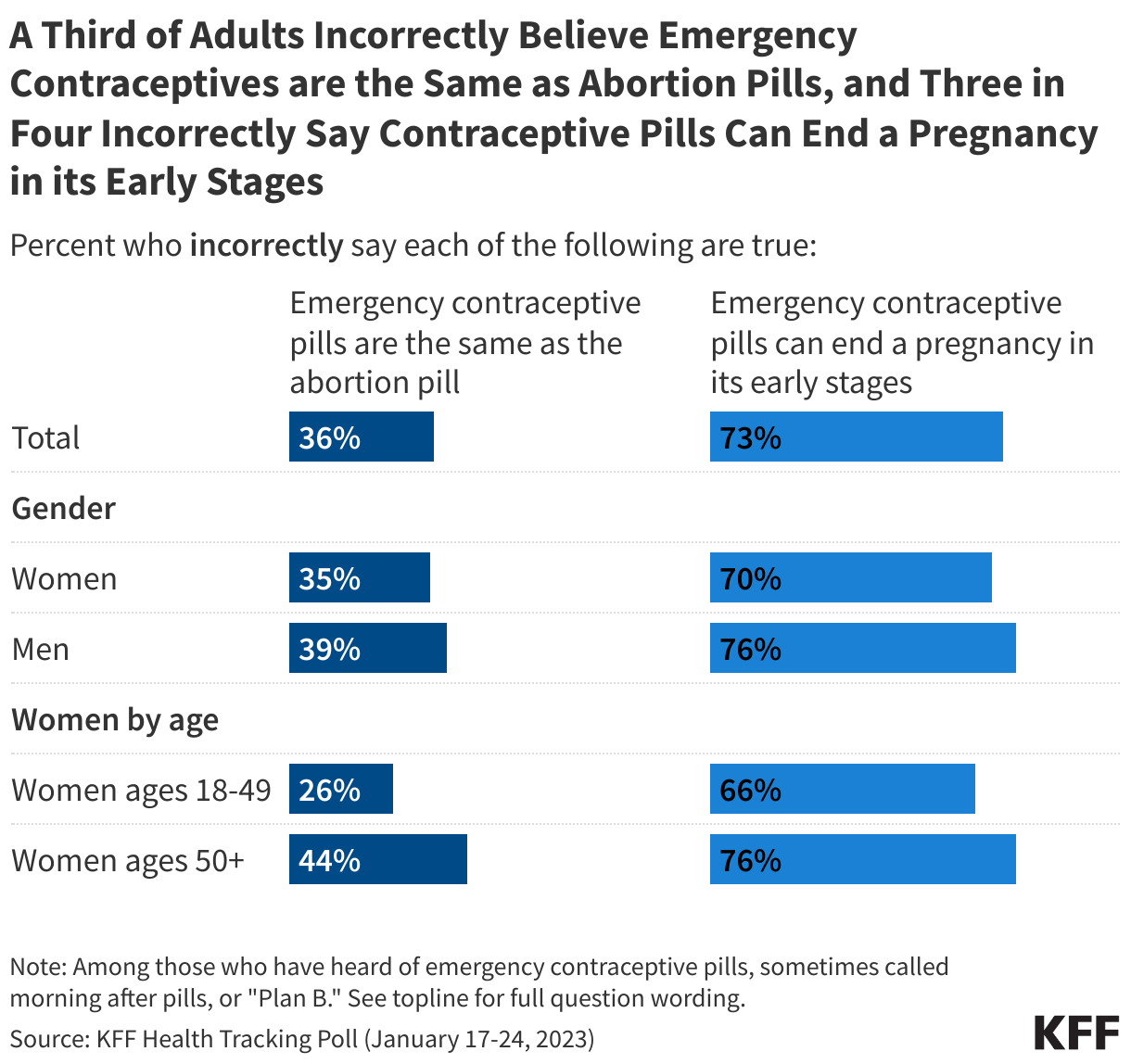
KFF polling has found that while the vast majority of U.S. adults (93%) have heard of emergency contraceptive (EC) pills, sometimes called the morning after pill or “Plan B,” knowledge gaps remain when it comes to accessing the medication and how it works.
One-third of adults who have heard of EC pills (including similar shares of women and men) incorrectly say that “emergency contraceptive pills are the same as the abortion pill,” and about three in four (including similar shares of women and men) incorrectly say that “emergency contraceptive pills can end a pregnancy in its early stages.” Women ages 18 to 49 are less likely than older women to say these false statements are true, though a majority (66%) still incorrectly believe that emergency contraceptive pills can end a pregnancy in its early stages.
Abortion bans have created uncertainty among providers and patients about the legality of EC in some states. According to a KFF issue brief, many bans define pregnancy as beginning at fertilization and effectively grant personhood to fertilized eggs. Combined with misconceptions that some contraceptives are abortifacients, this language can lead to abortion bans being interpreted as restricting access to contraceptives. KFF polling from 2023 finds that about half of women in states where abortion is banned either believe EC is illegal or are unsure of its legality. This uncertainty extends to providers, who may delay or deny services like IUDs and EC out of fear their actions could be misinterpreted as inducing abortion.

Misleading claims about contraceptive safety and effectiveness on social media could be driven by a number of factors including lack of high-quality contraceptive counseling, lack of knowledge of potential side effects, as well as wellness influencers who speak out against hormones. Social media platforms like TikTok, YouTube, and X amplify this misinformation with content creators frequently sharing unsubstantiated claims about the harms of hormonal contraceptives. These posts, often part of a broader trend against synthetic hormones, link hormonal contraceptive use to infertility, mental health challenges, and other health concerns. Personal anecdotes about side effects, coupled with critiques of pharmaceutical companies and the healthcare system, fuel these narratives. By sharing personal experiences and presenting themselves as relatable and independent, influencers are able to establish trust in a way that traditional health experts may not.
KFF Data Insights:
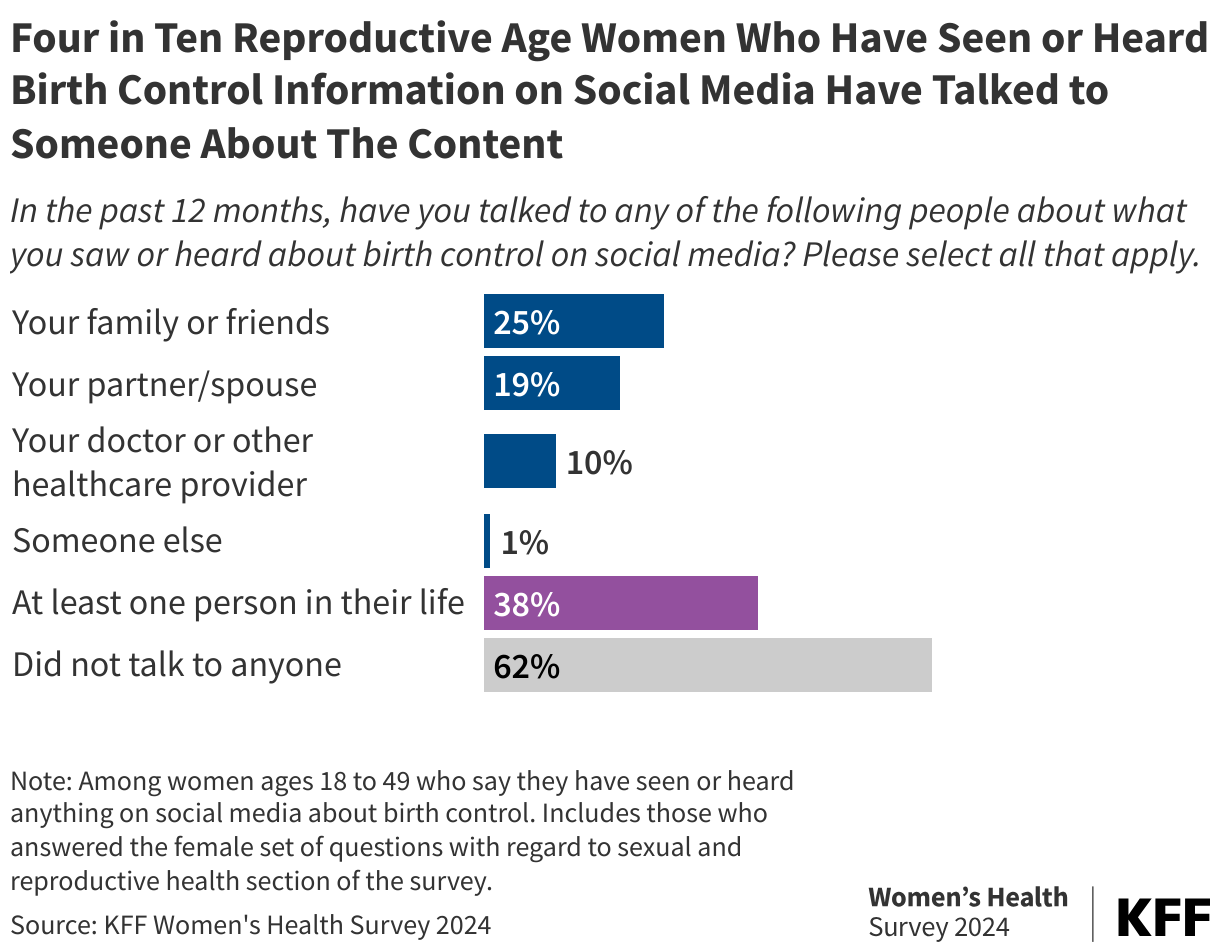
A November 2024 analysis of the KFF Women’s Health Survey examined women's experiences with contraception and the impact of contraceptive information on social media. The analysis found that approximately four in ten (39%) women of reproductive age report having encountered content related to birth control on social media in the past year. However, few women reported making or considering changes to their birth control method based on social media content.
Among those who have seen or heard birth control-related content on social media, 38% reported discussing the content with somebody in their lives. This includes about a quarter (25%) who had conversations with family or friends, 19% with their spouse or partner, and 10% who discussed the content with a doctor or healthcare provider.
Some content creators who advocate for avoiding synthetic hormones promote “natural” family planning methods—such as fertility awareness, cycle tracking, or the rhythm method—as healthier alternatives. These methods involve monitoring the menstrual cycle and avoiding intercourse or using non-hormonal birth control on fertile days. However, these approaches are generally less effective than hormonal contraceptives due to their reliance on precise knowledge and consistent application. Despite the proven effectiveness of hormonal contraceptives in preventing pregnancy, there are anecdotal reports of some women discontinuing their use, in part due to non-evidence-based fears fueled by such misinformation. While hormonal contraception may not be suitable for everyone, many individuals using “natural” family planning methods face challenges from a lack of proper guidance and difficulties with consistent use.

Health professionals have an opportunity to address questions or concerns about side effects outside of social media. The 2022 KFF Women’s Health Survey found that healthcare providers are both the primary (57%) and preferred source (74%) of information for many reproductive-age women using contraception. The main area of desired information is side effects with about half (52%) of reproductive-age women using contraception reporting wanting more information about additional side effects of their chosen contraceptive method.
An example where social media spurred a change in clinical practice relates to IUD insertions. After a number of people spoke about and recorded their painful experiences with IUD insertions on social media, the CDC issued new guidance for clinicians to ensure pain management is offered and covered by insurance during IUD insertions.
In recent decades, clinicians have prioritized getting their patients on the most effective contraceptive methods without centering patient needs and preferences, while downplaying their experiences and side effects. This has led to distrust and opened the door for social media content to fill a void on contraception information, but at a cost. There have been recent efforts to prioritize and center counseling and contraceptive options based on patient choices rather than focused on effectiveness alone. In addition to counseling in a clinical setting, reliable and trusted organizations are increasingly using social media to discuss and educate people about contraceptive methods, side effects, and effectiveness as a countervailing force to address misinformation.

Research published in the American Journal of Obstetrics & Gynecology surveyed physicians at the University of Wisconsin to examine their beliefs about contraception, particularly regarding misconceptions that methods like IUDs and ECs cause abortion. While most physicians surveyed correctly identified that pills, implants, and injections do not cause abortion, 17% believed IUDs and 39% thought EC were abortifacients. Male physicians and those with higher religiosity were more likely to hold these misconceptions. Obstetricians, gynecologists, and physicians who had some abortion education during training were less likely to believe IUDs and EC cause abortion compared to other specialties or those without training.
Source: Swan, L. E., Cutler, A. S., Lands, M., Schmuhl, N. B., & Higgins, J. A. (2023). Physician beliefs about contraceptive methods as abortifacients. AJOG, 78(1), 33-34.

An article in Human Communication Research introduces the Misinformation Resilience and Response Model (MRRM), which explains how individuals respond to misinformation. When faced with conflicting information, people experience cognitive dissonance and are motivated to resolve it. If they recognize misinformation, they may use strategies like counterarguing or avoidance, which can change their attitudes, emotions, or behaviors, such as sharing misinformation or altering health or political views. This model highlights the need for targeted intervention strategies to address misinformation effectively, but future research could help refine these strategies and improve their practical applications.
Source: Amazeen, M. A. (2024). The misinformation recognition and response model: an emerging theoretical framework for investigating antecedents to and consequences of misinformation recognition. Human Communication Research, 50(2), 218-229.

AI-powered chatbots show potential in addressing health misinformation by encouraging user engagement and reflection, but a 2023 systematic review on contraceptive knowledge found mixed results on their effectiveness. Some studies reviewed indicated increased contraception uptake in certain groups, while others saw no change in knowledge or intentions. This suggests that while chatbots offer convenience, their lack of emotional sensitivity and limited competency can hinder their effectiveness. A more recent study in the Harvard Misinformation Review also explored AI interventions aimed at addressing misinformation, but this time around belief in conspiracy theories. The study found that using an AI chatbot to prompt individuals to reflect on the reasons for their beliefs led to a reduction in the strength of that belief. However, this effect was less pronounced among individuals with strongly held beliefs, highlighting the challenge of changing deeply entrenched views. These findings point to the need for further research to determine the features that make AI chatbots effective in countering health misinformation.
This edition was created in close collaboration with KFF’s Women’s Health Policy team.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.

The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Sign up to receive KFF Monitor
email updates
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The Public Good Projects (PGP) provides media monitoring data KFF uses in producing the Monitor.
A new KFF analysis finds that there were 44 million people enrolled in health coverage through the Affordable Care Act’s Marketplaces and its expansion of the Medicaid program in 2024. That represents about 1 in every 6 people under age 65, or 16.4%.
There was significant variation in ACA enrollment across states, ranging from about 1 in 4 nonelderly people in Louisiana, Oregon, Florida, and New York to fewer than 1 in 10 in Tennessee, Alabama, Wyoming, Kansas, and Wisconsin, according to the analysis.
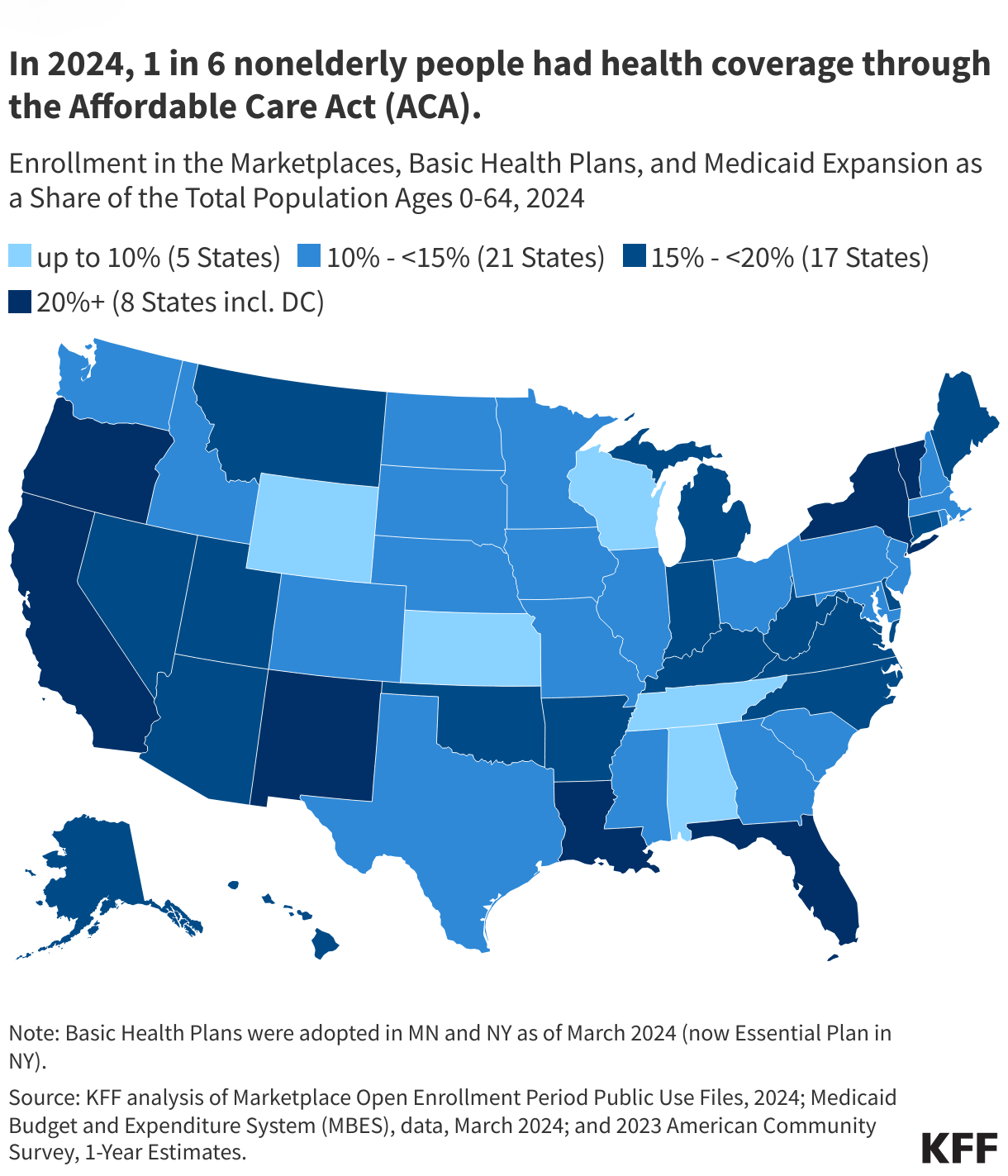
With the exception of Florida, the states with the largest ACA-related enrollment as a share of population had adopted the Medicaid expansion, while all five states with the lowest share of enrollment were non-expansion states. (The data includes enrollment in the Basic Health Program, an option offered by some states under the ACA to provide coverage for low-income residents who would otherwise be eligible to obtain coverage through the Marketplace. There were 1.3 million people enrolled in this option in 2024.)
The new analysis helps illustrate how many people could potentially be affected by the anticipated policy debates in Congress, including whether to allow enhanced ACA Marketplace subsidies to expire this year, whether to reduce the federal share of Medicaid expansion funding, or whether to enact deeper spending cuts to ACA subsidies and Medicaid to help pay for expected tax cuts.
From 2020 to 2024, total enrollment in ACA programs (Medicaid, Marketplace, and Basic Health Plan) increased by nearly 60%, with the largest increase among Marketplace enrollees, helping to drive the uninsured rate down to historic lows. The number of Marketplace enrollees increased by 10 million people nationally, almost doubling, over the period, and the number of Medicaid expansion enrollees increased by 6.2 million people. States with the largest increases in enrollment, in percentage terms, included Missouri (243%), Oklahoma (227%), Texas (212%), Mississippi (190%), North Carolina (185%) and Georgia (186%).
Growth in Marketplace enrollment over the period can be largely attributed to the temporary enhanced subsidies that were made available in 2021, which were extended through 2025. Marketplace enrollment climbed to a new record high in 2025, with nearly 24 million people signing up for plans during the current enrollment period. Marketplace enrollment was 21.4 million in 2024.
Medicaid expansion enrollment increased due to more states implementing expansion (seven states—Idaho, Missouri, Nebraska, North Carolina, Oklahoma, South Dakota, and Utah—implemented Medicaid expansion during or after 2020) and because of the pause in disenrollments from the pandemic-era continuous enrollment provision. Medicaid expansion enrollment totaled 21.3 million people in 2024. Even with the unwinding of the continuous enrollment provision that was still in play through March 2024, overall enrollment in Medicaid expansion is higher than in 2020.


 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma