KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
A new KFF brief provides a comprehensive overview of the coverage and use of fertility services in the United States, highlighting cost and insurance coverage gaps as key barriers faced by low-income people, Black and Hispanic people, LGBTQ individuals, infertile couples and single individuals seeking these services.
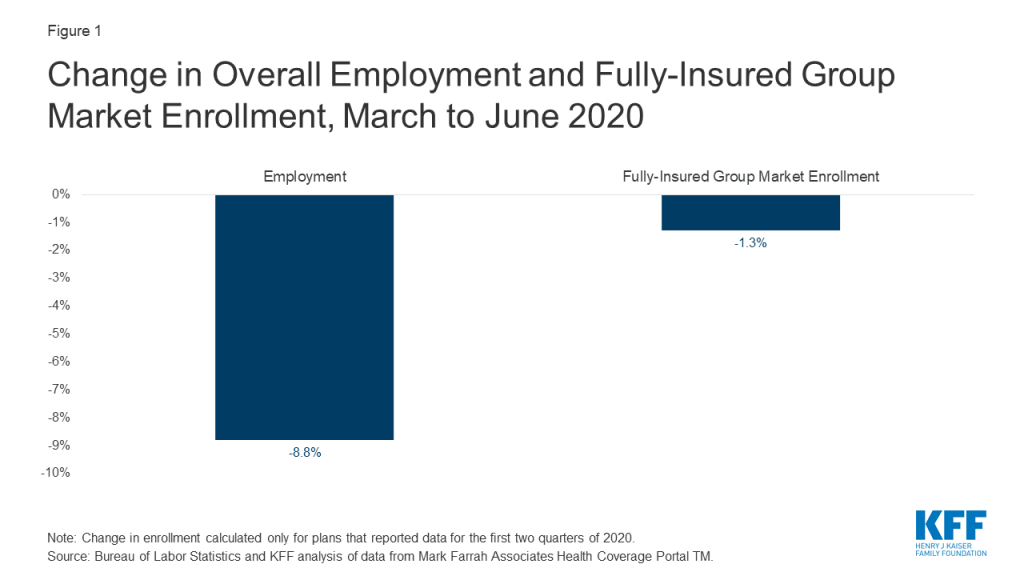
The coronavirus pandemic has worsened the availability of medical services and the financial situations of many Americans. Utilization of fertility services has declined, and medical professional societies issued guidelines earlier this year to stop new fertility treatment cycles, non-urgent diagnostic procedures and the criteria to resume such care. However, even before the pandemic several populations experienced disparities in access to such services.
Most patients pay out of pocket for fertility services which typically range in costs based on treatment and duration from the low thousands to tens of thousands of dollars. There is limited coverage of such services by private insurance plans and Medicaid. Fifteen states have laws requiring certain private insurers to cover some infertility treatments and these laws vary widely in the populations eligible and services covered. Only one state, New York, requires its Medicaid program to cover fertility treatment and eight states cover some diagnostic services. Additionally, surveys indicate that about 1 in 5 employers cover some form of infertility treatments.
Many people require fertility assistance. This includes men and women with infertility, many LGBTQ individuals, and single individuals who desire to raise children. An estimated 10% of women report that they or their partners have ever received medical help to become pregnant.
Despite a need for fertility services, fertility care in the U.S. is inaccessible to many due to the cost. More often than not, fertility services are not covered by public or private insurers. Fifteen states require some private insurers to cover some fertility treatment, but significant gaps in coverage remain. Only one state Medicaid program covers any fertility treatment, and no Medicaid program covers artificial insemination or in-vitro fertilization.
Most patients pay out of pocket for fertility treatment, which can amount to well over $10,000 depending on the services received. This means that in the absence of insurance coverage, fertility care is out of reach for many people.
Fewer Black and Hispanic women report ever having used medical services to become pregnant than White women. This is a result of many factors, including lower incomes on average among Black and Hispanic women as well as barriers and misconceptions that may dissuade women from seeking assistance with fertility.
LGBTQ individuals also face heightened barriers to accessing fertility care, as they often do not meet definitions of “infertility” that would qualify them for covered services. Transgender individuals undergoing gender-affirming care may also not meet criteria for “iatrogenic infertility” that would qualify them for covered fertility preservation.
Introduction
Many people require fertility assistance to have children. This could either be due to a diagnosis of infertility, or because they are in a same-sex relationship or single and desire children. While there are several forms of fertility assistance, many services are out of reach for most people because of cost. Fertility treatments are expensive and often are not covered by insurance. While some private insurance plans cover diagnostic services, there is very little coverage for treatment services such as IUI and IVF, which are more expensive. Most people who use fertility services must pay out of pocket, with costs often reaching thousands of dollars. Very few states require private insurance plans to cover infertility services and only one state requires coverage under Medicaid, the health coverage program for low-income people. This widens the gap for low-income people, even when they have health coverage. This brief examines how access to fertility services, both diagnostic and treatment, varies across the U.S., based on state regulations, insurance type, income level and patient demographics.
Diagnosis and Treatment Services
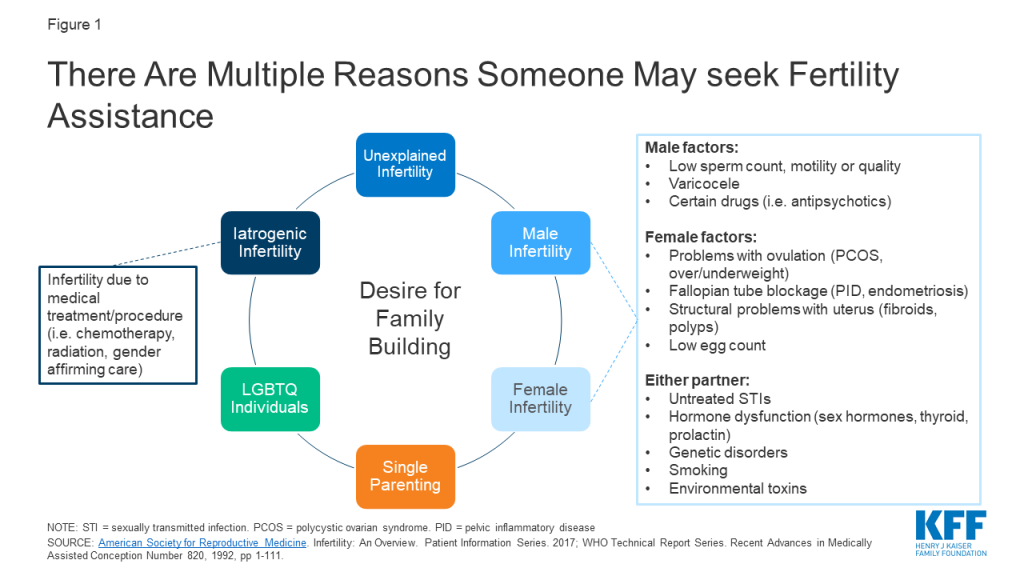
Infertility is most commonly defined1 as the inability to achieve pregnancy after 1 year of regular, unprotected heterosexual intercourse, and affects an estimated 10-15% of heterosexual couples. Both female and male factors contribute to infertility, including problems with ovulation (when the ovary releases an egg), structural problems with the uterus or fallopian tubes, problems with sperm quality or motility, and hormonal factors (Figure 1). About 25% of the time, infertility is caused by more than one factor, and in about 10% of cases infertility is unexplained. Infertility estimates, however do not account for LGBTQ or single individuals who may also need fertility assistance for family building. Therefore, there are varied reasons that may prompt individuals to seek fertility care.
Figure 1: There Are Multiple Reasons Someone May seek Fertility Assistance
A broad array of diagnostic and treatment services may be necessary to assist in fertility (Table 1). Diagnostics typically include lab tests, a semen analysis and imaging studies or procedures of the reproductive organs. If a probable cause of infertility is identified, treatment is often directed at addressing the source of the problem. For example, if someone has abnormal thyroid hormone levels, thyroid medications may help the patient achieve pregnancy. If a patient has large fibroids distorting the uterine cavity, surgical removal of these benign tumors may allow for future pregnancy. Other times, other interventions are needed to help the patient achieve pregnancy. For example, if a semen analysis reveals poor sperm motility or the fallopian tubes are blocked, the sperm will not be able to fertilize the egg, and intrauterine insemination (IUI) or in-vitro fertilization (IVF) may be necessary. These procedures also facilitate family building for LGBTQ and single individuals, with use of donor egg or sperm, with or without a gestational carrier (surrogacy).
NOTES: This is not an exhaustive list of infertility services.SOURCE: ACOG. Evaluating Infertility. 2017; ACOG. Treating Infertility. 2019; American Society for Reproductive Medicine. Infertility: An Overview. Patient Information Series. 2017
Utilization of Fertility Services
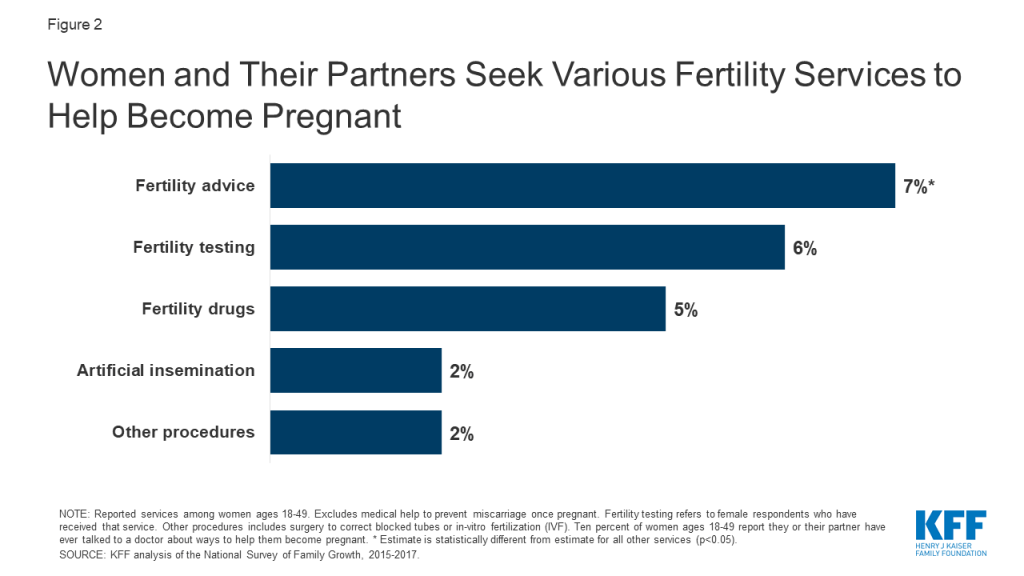
Our analysis of the 2015-2017 National Survey of Family Growth (NSFG) finds that 10% of women2 ages 18-49 say they or their partner have ever talked to a doctor about ways to help them become pregnant (data not shown).3 Among women ages 18-49, the most commonly reported service is fertility advice (Figure 2).
Figure 2: Women and Their Partners Seek Various Fertility Services to Help Become Pregnant
The CDC finds that use of IVF has steadily increased since its first successful birth in 1981. According to the most recent data, an estimated 1.8% of U.S. infants are conceived annually using assisted reproductive technology (ART) (e.g., IVF and related procedures).4 The proportions are highest in the Northeast (MA 4.7%, CN 3.9%, NJ 3.9%), and lower in the South and Southwest (NM 0.4%, AR 0.6%, MS 0.6%).
Utilization of fertility services has dropped drastically during the COVID-19 public health emergency. On March 17, 2020 the American Society for Reproductive Medicine (ASRM) issued guidelines to stop all new fertility treatment cycles and non-urgent diagnostic procedures. Since then, ASRM has provided updated guidance on what conditions should be met and measures should be taken before safely resuming fertility care. During this time, a study by Strata Decision Technology of 228 hospitals across 40 states found patient encounters for infertility services were down 83% from March 22 to April 4, 2020 compared to this time the year prior.
Cost of Services
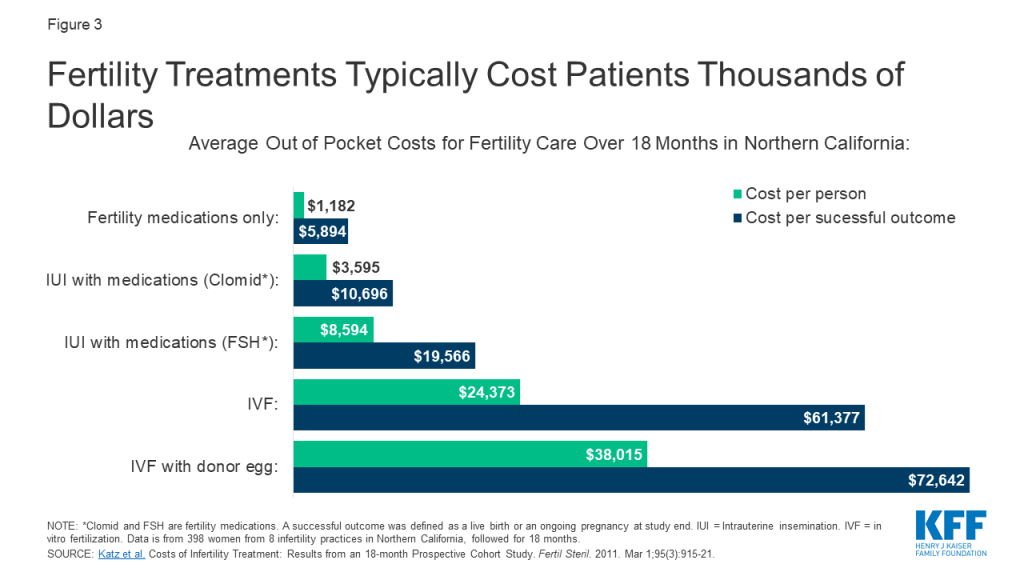
Many patients lack access to fertility services, largely due to its high cost and limited coverage by private insurance and Medicaid. As a result, many people who use fertility services must pay out of pocket, even if they are otherwise insured. Out of pocket costs vary widely depending on the patient, state of residence, provider and insurance plan. Generally, diagnostic lab tests, semen analysis and ultrasounds are less expensive than diagnostic procedures (e.g., HSG) or surgery (e.g., hysteroscopy, laparoscopy). Meanwhile treatment using fertility medications is less expensive than IUI and IVF, but even the less costly treatments can still result in thousands of dollars of out of pocket costs. Many people must try multiple treatments before they or their partner can achieve a pregnancy (typically medication first, followed by surgery or fertility procedures if medications are unsuccessful). A study of nearly 400 women undergoing fertility care in Northern California demonstrates this overall trend, with the lowest out of pocket spending on treatment with medication only and the highest costs for IVF services (Figure 3). Prior research showed the cost of just one standard cycle of IVF was approximately $12,500 in 2009, but is likely higher today due to rising health care costs overall. Furthermore, many patients require several rounds of treatment before achieving a pregnancy, with costs accruing each cycle making these interventions financially inaccessible for many. In addition to costs for the actual treatment, patients can be saddled with out of pocket expenses for office visits, diagnostic tests/procedures, genetic testing, donor sperm/egg use and storage fees and wages lost from time off work.
Figure 3: Fertility Treatments Typically Cost Patients Thousands of Dollars
Insurance Coverage
Insurance coverage of fertility services varies by the state in which the person lives and, for people with employer-sponsored insurance, the size of their employer. Many fertility treatments are not considered “medically necessary” by insurance companies, so they are not typically covered by private insurance plans or Medicaid programs. When coverage is available, certain types of fertility services (e.g., testing) are more likely to be covered than others (e.g., IVF). A handful of states require coverage of fertility services for some fully-insured private plans, which are regulated by the state. These requirements, however, do not apply to health plans that are administered and funded directly by employers (self-funded plans) which cover six in ten (61%) workers with employer-sponsored health insurance. States also have purview over the benefits covered by their Medicaid programs. The federal government has authority over benefit requirements in federal health coverage programs, including Medicare, the Indian Health Service (IHS) and military health coverage.
Private Insurance
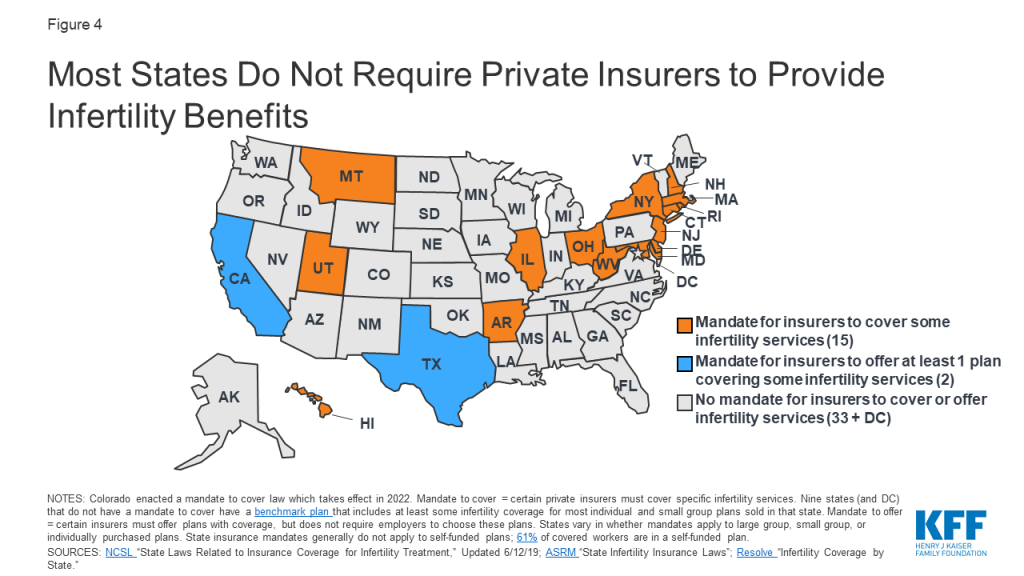
Fifteen states have laws in effect requiring certain health plans to cover at least some infertility treatments (a “mandate to cover”) (Figure 4). Additionally, Colorado recently enacted a requirement for individual and group health benefit plans to cover infertility diagnosis, treatment and fertility preservation for iatrogenic infertility, effective January 2022. Among states that do not have a mandate to cover, nine states5 and DC have a benchmark plan that includes coverage for at least some infertility services (diagnosis and/or treatment) for most individual and small group plans sold in that state.6 Two states (CA and TX7 ) require group health plans to offer at least one policy with infertility coverage (a “mandate to offer”), but employers are not required to choose these plans.
Figure 4: Most States Do Not Require Private Insurers to Provide Infertility Benefits
However, in states with “mandate to cover” laws, these only apply to certain insurers, for certain treatment services and for certain patients, and in some states have monetary caps on costs they must cover (Appendix 1). For example, in OH and WV, the requirement to cover infertility services only applies to health maintenance organizations (HMOs). In other states, almost all insurers and HMOs are included in the mandate. Many states provide exemptions for small employers (<50 employees) or religious employers. In addition, state laws do not apply to self-funded (or self-insured) employer plans, which are regulated by federal law. Sixty-one percent of covered workers are enrolled in a self-funded plan.
Even in states with coverage laws, not all patients are eligible for infertility treatment. In HI, someone with unexplained infertility only qualifies for IVF after five years of infertility. In others, patients are eligible after 1 year. Some states place age limits on female patients who can access these services (e.g., ineligible if 46 or older in NJ or if under age 25 or older than 42 in RI). Others place restrictions based on marital status; for example, until May 2020, IVF benefits were only available to married women in MD. Recently enacted legislation now expands coverage to unmarried women. Additionally, it is not always made clear if LGBTQ individuals meet eligibility criteria for these benefits, without a diagnosis of infertility. Furthermore, many costs associated with surrogacy are often not covered by insurance.
States also vary in which treatment services they require plans to cover. Some states mandate insurers to cover cryopreservation for persons with iatrogenic infertility, while others do not. Four states with insurer mandates do not cover IVF. Eleven states do, but with a dollar limit on coverage (e.g., $15,000 lifetime max in AR and $100,000 in MD and RI) or a limit on the number of cycles they will cover (e.g., one cycle of IVF in HI and three cycles in NY).
Do state mandates for IVF coverage affect use of services?
IVF utilization appears to be higher in states with mandated IVF coverage. CDC data from 2016 showed that in three of the four states deemed by the CDC to have “comprehensive coverage”8 for IVF (IL, MA, NH), use of assisted reproductive technology was 1.5 times higher than the national rate. Similarly, a national study found that IVF availability and utilization9 were significantly higher in states with mandated IVF coverage. A study in MA found IVF utilization increased after implementation of their IVF mandate, but overutilization by patients with a low chance of pregnancy success was not found. State level mandates can also help reduce inequities in access. For example, a recent bill proposed in the CA legislature would reverse existing limitations on fertility coverage and make the benefit available to single women and women in same sex relationships.
What does it cost to cover fertility benefits?
While the costs of fertility treatments can be very expensive for those who lack coverage, the cost of covering fertility benefits varies depending on the services covered and utilization with implications for state budgets, employers, and policy holders. For example, in 2019, New York passed a bill to require IVF and fertility preservation services for comprehensive private health insurance policies. The New York State Department of Financial Services estimated that premiums would increase 0.5% to 1.1% due to mandating IVF coverage, and 0.02% for mandating fertility preservation for iatrogenic infertility (caused by medical treatments).
An analysis of a bill proposed in CA to require private plans and Medi-Cal managed care plans to cover IVF services estimated that per member per month premiums would increase by approximately $5 in the private market and less than a $1.00 for Medi-Cal plans. Overall though, out of pocket spending for individuals seeking services would decrease substantially.
Data from MA, CT and RI suggest that mandating coverage does not appear to raise premiums significantly. All three states have been mandating infertility benefits for over 30 years, and estimate the cost of infertility coverage to be less than 1% of total premium costs. In 2017, California was considering a more limited bill that would require fertility preservation for iatrogenic infertility in certain individual and group health plans. As the bill was introduced, it was estimated to result in a net annual increase of $2,197,000 in premium costs or 0.0015% for enrollees in plans subject to the mandate.
While these costs could be modest in comparison to the costs of paying out-of-pocket for these services, there are other costs to coverage mandates. The ACA requires states to offset some of the costs for any state mandated benefits beyond essential health benefits (EHBs) in the individual and small group market. This requirement was estimated to cost NY $59 to $69 million per year if covering one cycle or $98 to $116 million per year if covering unlimited cycles of IVF.
What share of employers offer fertility benefits?
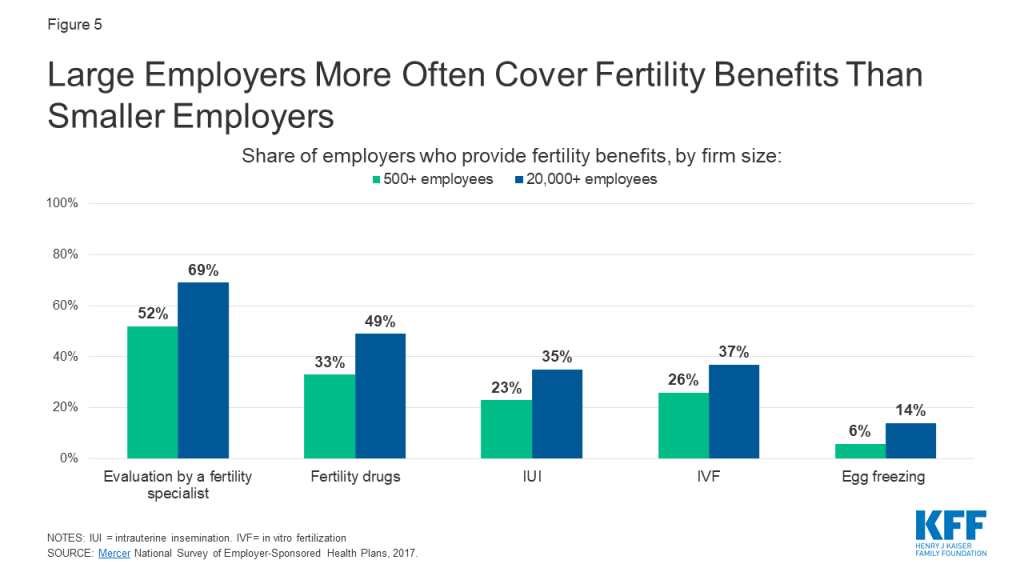
Large employers are more likely than smaller employers to include fertility benefits in their employer-sponsored health plans. According to Mercer’s 2017 National Survey of Employer-Sponsored Health Plans, 56% of employers with 500 or more employees cover some type of fertility service, but most do not cover treatment services such as IVF, IUI, or egg freezing. Coverage is higher for diagnostic evaluations and fertility drugs. Coverage is more common among the largest employers and those that offer higher wages (Figure 5).
Figure 5: Large Employers More Often Cover Fertility Benefits Than Smaller Employers
Public Coverage
Medicaid
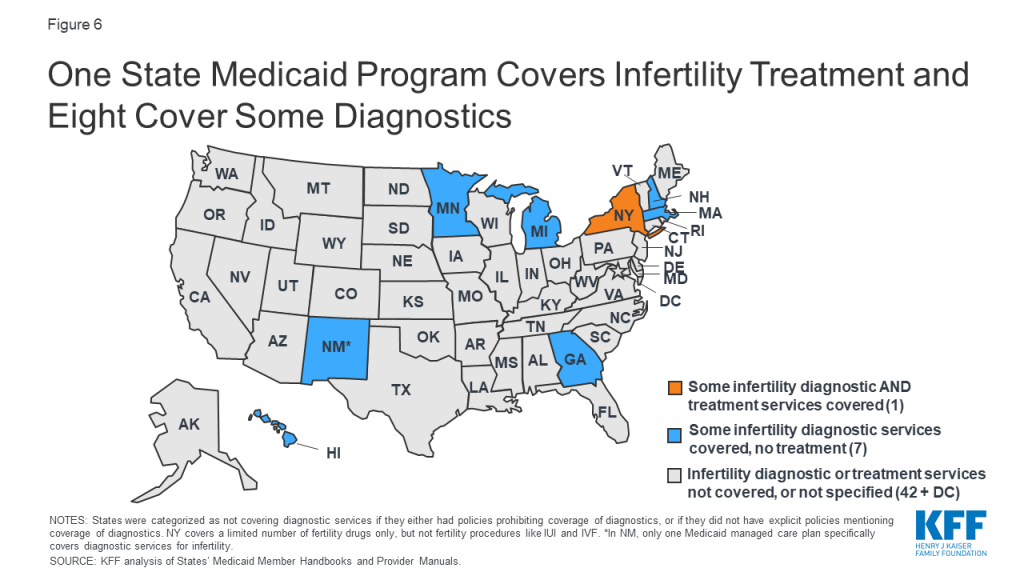
NSFG data show that significantly fewer women with Medicaid have ever used medical services to help become pregnant compared to women with private insurance. As of January 2020, our analysis of Medicaid policies and benefits reveal only one state, New York, specifically requires their Medicaid program to cover fertility treatment (limited to 3 cycles of fertility drugs) (Figure 6). However, some states may require Medicaid to cover treatments for conditions that impact fertility, while not directly stated in their policies. For example, states may cover thyroid medications, or cover surgery for fibroids, endometriosis or other gynecologic abnormalities if causing pelvic pain, abnormal bleeding or another medical problem, other than infertility. No state Medicaid program currently covers artificial insemination (IUI), IVF, or cryopreservation (Appendix 2).
Some states specifically cover infertility diagnostic services; GA, HI, MA, MI, MN, NH, NM and NY all offer at least one Medicaid plan with this benefit, but the range of diagnostics covered varies. For example, New York Medicaid specifically covers office visits, HSGs, pelvic ultrasounds and blood tests for infertility. Meanwhile, the infertility assessment covered by Georgia Medicaid includes lab testing, but not imaging or procedural diagnostics. Other states specifically do not cover infertility diagnostics, or more generally do not cover “infertility services,” which likely includes diagnostics. Others do not mention infertility diagnostics in their Medicaid policies, meaning the beneficiary would need to check with their Medicaid program to see if these services are covered (Appendix 2).
The Medicaid program’s lack of coverage of fertility assistance has a disproportionate impact on women of color. Among reproductive age women, the program covers three in ten (30%) who are Black and one quarter who are Hispanic (26%), compared to 15% who are White. Because eligibility for Medicaid is based on being low-income, people enrolled in the program likely could not afford to pay for services out of pocket.
The relative lack of Medicaid coverage for fertility services stands in stark contrast to Medicaid coverage for maternity care and family planning services. Nearly half of births in the U.S. are financed by Medicaid, and the program finances the majority of publicly-funded family planning services. Therefore, while there is broad coverage of many services for low-income people during pregnancy and to help prevent pregnancy, there is almost no access to help low-income people achieve pregnancy.
Figure 6: One State Medicaid Program Covers Infertility Treatment and Eight Cover Some Diagnostics
Medicare
While most beneficiaries of Medicare are over the age of 65+, Medicare also provides health insurance to approximately 2.5 million reproductive age adults with permanent disabilities. According to the Medicare Benefit policy manual, “reasonable and necessary services associated with treatment for infertility are covered under Medicare.” However, specific covered services are not listed, and the definition of “reasonable and necessary” are not defined.
Military
TRICARE: TRICARE, the insurance program for military families, will cover some infertility services, if deemed “medically necessary” and if pregnancy is achieved through “natural conception,” meaning fertilization occurs through heterosexual intercourse. Diagnostic services are covered, including lab testing, genetic testing, and semen analysis. Treatment to correct physical causes of infertility are also covered. However, IUI, IVF, donor eggs/sperm and cryopreservation are not typically covered, unless the service member had a serious injury while on active duty resulting in infertility.
Veterans Affairs (VA): Infertility services are covered by the VA medical benefits package, if infertility resulted from a service-connected condition. This includes infertility counseling, blood tests, genetic counseling, semen analysis, ultrasound imaging, surgery, medications and IVF (as of 2017). However, the couple seeking services must be legally married, and the egg and sperm must come from said couple (effectively excluding same sex couples). Donor eggs/sperm, surrogacy or obstetrical care for non-Veteran spouses are not covered.
Infertility Services In Publicly Funded Clinics
The CDC’s and Office of Population Affairs’ (OPA) Quality Family Planning recommendations address provision of basic infertility services. Family planning providers are recommended to provide at minimum patient education about fertility and lifestyle modifications, a thorough medical history and physical exam, semen analysis, and if indicated, referrals for lab testing of hormone levels, additional diagnostic tests (endometrial biopsy, ultrasound, HSG, laparoscopy) and prescription of medications to promote fertility. However, studies of publicly funded family planning clinics suggest that availability of infertility services is uneven. In a 2013-2014 study of 1615 publicly funded clinics, a high share reported offering preconception care (94% for women and 69% for men), but fewer offered any basic infertility services (66% for women and 45% for men). Provision of any infertility treatment was uncommon (16% of clinics), likely requiring referrals to specialists who may not accept Medicaid or uninsured patients.10 The majority of patients who rely on publicly funded clinics are low-income and would not likely be able to afford infertility services and treatments once diagnosed.
Per the Indian Health Services (IHS) provider manual, basic infertility diagnostics should be made available to women and men at IHS facilities, including a history, physical exam, basal temperature charting (to predict ovulation), semen analysis and progesterone testing. In facilities with OBGYNs, HSG, endometrial biopsy and diagnostic laparoscopy should also be available. However, it is unclear how accessible these services are in practice, and provision of infertility treatment is not mentioned.
Key Populations
Racial and ethnic minorities
The ability to have and care for the family that you wish for is a fundamental tenet of reproductive justice. For those who need it, this includes access to fertility services. The share of racial and ethnic minorities who utilize medical services to help become pregnant is less than that of non-Hispanic White women, despite research that has found higher rates of infertility among women who are Black and American Indian / Alaska Native (AI/AN). Our analysis of 2015-2017 NSFG data shows that while 13% of non-Hispanic White women reported ever going to a medical provider for help getting pregnant, just 6% of Hispanic women and 7% of non-Hispanic Black women did so (Figure 7). A higher share of Black and Hispanic women are either covered by Medicaid or uninsured than White women and more women with private insurance sought fertility help than those with Medicaid or the uninsured. A variety of factors, including differences in coverage rates, availability of services, income, and service‐seeking behaviors, affect access to infertility care. Furthermore, other societal factors also play a role. Misconceptions and stereotypes about fertility have often portrayed Black women as not requiring fertility assistance. Combined with the history of discriminatory reproductive care and harm inflicted upon many women of color over decades, some may delay seeking infertility care or may not seek it at all.
Figure 7: Women Seeking Help to Become Pregnant Tend to Be Age 35+, White, Higher Income, and Privately Insured
Other research has found that use of fertility testing and treatment also varies by race. An analysis of NSFG data found that among women who reported using medical services to help become pregnant, similar shares of Black (69%), Hispanic (70%) and White (75%) women received fertility advice. However, less than half (47%) of Black and Hispanic women who used medical services to become pregnant reported receiving infertility testing, compared to 62% of White women, and even fewer women of color received treatment services. According to an analysis of surveillance data of IVF services, use is highest among Asian and White women and lowest among American Indian / Alaska Native (AI/AN) women. Racial inequities may exist for fertility preservation as well; a study of female patients in NY with cancer found disproportionately fewer Black and Hispanic patents utilized egg cryopreservation compared to White patients. On average, more Black, Hispanic, and AI/AN people live below the federal poverty level than people who are White or of Asian/Pacific Islander descent. The high cost and limited coverage of infertility services make this care inaccessible to many people of color who may desire fertility preservation, but are unable to afford it.
Iatrogenic Infertility
Iatrogenic, or medically induced, infertility refers to when a person becomes infertile due to a medical procedure done to treat another problem, most often chemotherapy or radiation for cancer. In these situations, persons of reproductive age may desire future fertility, and may opt to freeze their eggs or sperm (cryopreservation) for later use. The American Society for Reproductive Medicine (ASRM) encourages clinicians to inform patients about fertility preservation options prior to undergoing treatment likely to cause iatrogenic infertility.
However, the cost of egg or sperm retrieval and subsequent cryopreservation can be prohibitive, particularly if in the absence of insurance coverage. Only a handful of states (CT, DE, IL, MD, NH, NJ, NY, and RI) specifically require private insurers to cover fertility preservation in cases of iatrogenic infertility. No states currently require fertility preservation in their Medicaid plans.
LGBTQ populations
LGBTQ people may face heightened barriers to fertility care, and discrimination based on their gender identity or sexual orientation. Section 1557 of the Affordable Care Act (ACA) prohibits discrimination in the health care sector based on sex, but the Trump Administration has eliminated these protections through regulatory changes. Without the explicit protections that have been dropped in the current rules, LGBTQ patients may be denied health care, including fertility care, under religious freedom laws and proposed changes to the ACA. However, these changes are being challenged in the courts because they conflict with a recent Supreme Court decision stating that federal civil rights law prohibits discrimination based on sexual orientation and gender identity.
In a committee opinion, ASRM concluded it is the ethical duty of fertility programs to treat gay and lesbian couples and transgender persons, equally to heterosexual married couples. They write that assisted reproductive therapy should not be restricted based on sexual orientation or gender identity, and that fertility preservation should be offered to transgender people before gender transitions. This allows transgender individuals the ability to have biological children in the future if desired. Despite this recommendation, in aforementioned states with mandated fertility preservation coverage for iatrogenic infertility, it remains unclear if this benefit extends to transgender individuals, whose gender affirming care can result in infertility. Additionally, many state laws regarding mandates for infertility treatment contain stipulations that may exclude LGBTQ patients. For example, in Arkansas, Hawaii and Texas and at the VA, IVF services must use the couple’s own eggs and sperm (rather than a donor), effectively excluding same sex couples. In other states, same-sex couples do not meet the definition of infertility, and thus may not qualify for these services. Data are lacking to fully capture the share of LGBTQ individuals who may utilize fertility assistance services. Research studies on family building are often not designed to include LGBTQ respondents’ fertility needs.
Single Parents
Single persons are often excluded from access to infertility treatment. For example, the same IVF laws cited above that require the couple’s own sperm and egg, effectively exclude single individuals too, as they cannot use donors. Some grants and other financing options also stipulate funds must go towards a married couple, excluding single and unmarried individuals. This is in opposition to the ASRM committee opinion, which states that fertility programs should offer their services to single parents and unmarried couples, without discrimination based on marital status.
Looking Forward
On a federal level, efforts to pass legislation to require insurers to cover fertility services are largely stalled. The proposed Access to Infertility Treatment and Care Act (HR 2803 and S 1461), which would require all health plans offered on group and individual markets (including Medicaid, EHBP, TRICARE, VA) to provide infertility treatment, is still in committee (and never made it out of committee when proposed during the 115th congress). There has been some more movement on the state level. Some states require private insurers to cover infertility services, the most recent of which was NH in 2020. Currently, NY continues to be the first and only state Medicaid program to cover any fertility treatment.
For those who desire to have children, obtaining fertility care can be a stressful process. Stigma around infertility, intensive and sometimes long or painful treatment regimens, and uncertainty about success can take a toll. On top of that, in the absence of insurance coverage, infertility care is cost prohibitive for most, particularly for low-income people and for more expensive services, like IVF or fertility preservation. Significant disparities exist within access to infertility services across, dictated by state of residence, insurance plan, income level, race/ethnicity, sexual orientation and gender identity. Achieving greater equity in access to fertility care will likely depend on addressing the needs faced by low-income persons, people of color and LGBTQ persons in fertility policy and coverage.
Appendices: Appendix 1: Private Insurance
Appendix 1: States That Require Private Insurance Coverage of Infertility Services
Infertility coverage required:(As of May 2020)
State (Statute year)
By which insurers?
For which indications?
For which treatments?
AR
(1987, 2011)
Included: all individual and group insurers*
Excluded: HMOs; self-insurers
Eligible: Infertility due to male factor, endometriosis, blocked fallopian tube (or unexplained for 2 years)
Ineligible: if egg/sperm not from spouse
Covered: IVF (lifetime max $15,000)
Not covered: Fertility preservation for iatrogenic infertility
CA
(1990)
Mandate to offer, not cover: group insurers must let employers know coverage for diagnostic tests and some treatment is available (excludes IVF and fertility preservation), but employers do not need to provide coverage to employees
CO
(Effective 2022)
Passed House Bill 20-1148 in April 2020 to mandate coverage for infertility diagnosis and treatment, and fertility preservation for iatrogenic infertility. Applies to all individual and group health benefit plans renewed or issued after January 1, 2022, but religious employer may request exemption.
CT
(1989, 2005)
Included: Health insurance organizations
Excluded: Persons on plan for <12 months; religious employers; self-insurers
Eligible: Infertility for 1 year or iatrogenic infertility
Not Covered: Lifetime max of 4 cycles of ovulation induction, 3 cycles of IUI
DE
(2018)
Included: Individual and group insurers, HMOs **
Excluded: <50 employees; religious employers; self-insurers
Eligible: Infertility or iatrogenic infertility
Covered: consultation, diagnostics, medications, IUI, IVF and other treatments; fertility preservation for iatrogenic infertility
Not Covered: Egg retrieval after age 45, >6 egg retrievals, surrogacy compensation, reversal of voluntary sterilization
HI
(1989, 2003)
Included: Individual and group insurers
Excluded: self-insurers
Eligible: 5 years of unexplained infertility, OR infertility due to male factors, endometriosis, blocked/ removed fallopian tubes
Ineligible: if egg/sperm not from spouse
Covered: 1 cycle of IVF, all outpatient expenses arising from IVF
IL
(1991, 1996)
Included: Group insurers and HMOs*; individual insurers for iatrogenic infertility
Excluded: <25 employees; religious employers; self-insurers
Eligible: 1 year of infertility or iatrogenic infertility
Covered: Diagnostics, IUI, IVF, and other treatments; fertility preservation for iatrogenic infertility
Not Covered: More than 6 egg retrievals
MD
(2000)
Included: Individual and group insurers*
Excluded: <50 employees; religious employers; self-insurers
Eligible: Infertility due to male factor, endometriosis, blocked/removed fallopian tubes (or if unexplained for 2 years)
Covered: 3 cycles of IVF per life birth (lifetime max $100,000); fertility preservation for iatrogenic infertility
Not Covered: Storage of sperm/eggs
MA
(1987, 2010)
Included: All insurers and HMOs*
Excluded: self-insurers
Eligible: Infertility for 1 year if age <35, 6 months if 35+
Covered: IUI, IVF, cryopreservation and others (no lifetime limit on cost or cycles)
Not Covered: Surrogacy, reversal of sterilization
MT
(1987)
Included: HMOs
Excluded: all other insurers
Eligible: No definition of infertility
Covered: must cover “infertility services,” does not define which
NH
(2020)
Included: Group insurers***
Excluded: Small business health options program; extended transition to ACA- programs; self-insurers
Eligible: Ability to become/cause pregnancy is impaired
Covered: Diagnostics, treatment including medications, egg/sperm procurement; fertility preservation for iatrogenic infertility
Not Covered: reversal of voluntary sterilization; some aspects of care if surrogate involved
NJ
(2001)
Included: Group insurers; HMOs; State Health Benefits Program; School Employees Health Benefits Program*
Excluded: <50 employees; religious employers; self-insurers
Eligible: Infertility for 1 year if age <35, 6 months if 35+; single female unable to conceive with 12 IUIs if <35, 6 IUIs if >35; persons involuntarily sterilized
Ineligible: >46 years old
Covered: diagnostics, medications, surgery, IUI, IVF, and other treatments (max 4 egg retrievals per lifetime)
Not Covered: reversal of voluntary sterilization; cryopreservation
NY
(1990, 2002, 2020)
Included: Large group insurance market for IVF (>100 employees); all commercial markets for cryopreservation
Excluded: Individual and small group markets for IVF; self-insurers
Eligible: Infertility for 1 year if age <35, 6 months if 35+
Ineligible:
Covered: diagnostic procedures, medications, 3 cycles of IVF; fertility preservation if iatrogenic infertility
Not Covered: surrogacy, reversal of elective sterilization
OH
(1991)
Included: HMOs
Excluded: all other insurers
Eligible: No definition of infertility
Covered: diagnostic and exploratory procedures to correct cause for infertility (endometriosis, blocked fallopian tube, testicular failure)
Not Covered: IVF and other treatments
RI
(1989, 2007)
Included: Insurers and HMOs*
Excluded: Self-insurers
Eligible: Infertility for 1 year; iatrogenic infertility
Ineligible: women aged <25 of >42 (unless for fertility preservation)
Covered: diagnostics and treatment, including IVF; fertility preservation for iatrogenic infertility (up to 20% copay allowed)
Not Covered: >$100,000 on treatment
TX
(1987, 2003)
Mandate to offer, not cover: Group insurers must offer IVF as a benefit, employers can choose whether or not to include it. If choose to include, must be egg/sperm from spouse.
UT
(2014)
Included: Insurers*
Excluded: Self-insurers
Eligible: no definition of infertility; persons wishing to adopt
Covered: $4000 adoption indemnity, can also be used for infertility treatment
WV
(1995)
Included: HMOs
Excluded: all other insurers
Eligible: no definition of infertility
Covered: must cover “infertility services,” does not define which
NOTES: *Insurers must cover if they also provide pregnancy-related benefits. ** Must cover infertility services to same extent as other pregnancy-related services. ***Must cover if also provide medical/hospital expenses.AL, AK, AZ, CO, DC, FL, GA, ID, IN, IA, KS, KY, LA, ME, MI, MN, MS, MO, NE, NV, NM, NC, ND, OK, OR, PA, SC, SD, TN, VT, VA, WA, WI, and WY do not require private insurers to cover infertility treatments.SOURCES: NCSL. State Laws Related to Insurance Coverage for Infertility Treatment. 6/12/2019; American Society for Reproductive Medicine (ASRM). State Infertility Insurance Laws; Resolve. Infertility Coverage by State; Colorado House Bill 20-1158
Appendices: Appendix 2: Medicaid
Appendix 2: State Medicaid Coverage of Infertility Services
Covered and Non-Covered Services by State(As of January 2020)
Not Covered: Infertility studies/procedures for diagnosing/treating infertility (Family Planning Manual)
CO
Covered: Basic fertility and reproductive health counseling is provided (Family Planning Services Benefits)
Not Covered: Sterilization reversal. Infertility treatment, counseling and testing. Tests normally associated with infertility management (e.g., HSG and semen analysis) covered only to confirm success of a sterilization
CT
Covered: Lab tests to detect the presence of conditions affecting reproductive health (Member Handbook)
Covered: infertility diagnosis/treatment when infertility is a symptom of a suspected medical problem (e.g., thyroid disease). No coverage if the sole purpose is achieving pregnancy (Physician services)
Covered: infertility office visits, diagnosis (HSG, pelvic ultrasounds, lab tests), fertility drugs (bromocriptine, clomiphene citrate, letrozole, tamoxifen). Limited to 3 cycles of treatment per lifetime (Infertility Benefit)
Not Covered: Infertility treatments beyond those described above.
NC
Not Covered: Infertility services and related procedures. Services to manage/treat complications of women’s health problems, including heavy bleeding or infertility (Family Planning Services)
ND
Not Covered: Diagnostic, medical, surgical or pharmaceutical services related to infertility. Removal of long acting reversible contraceptive devices to regain fertility (Provider manual)
Not Covered: Will not pay for medical procedures if goal is fertility (semen analysis, fallopian tube repair, laparoscopy). Covered if reproductive system disease requires treatment to maintain overall health, and is medically necessary (Provider Manual). No fertility drugs (Pharmacy manual)
NOTES: * Benefits vary between Medicaid managed care plans. Information collected on individual Medicaid managed care plans when information on fertility benefits not found in member benefits or provider manuals pertaining to all Medicaid plans.ⱡ OR covers basic infertility counseling as part of The Oregon Reproductive Health Program for low income women, but not a Medicaid benefitSOURCES: Information compiled from member handbooks and provider manuals as linked above, available online as of January 2020 (see links above).
Endnotes
The evaluation of fertility can start after six months if the woman is over the age of 35. ↩︎
Data and research often assume cisgender identities and may not systematically account for people who are transgender and non-binary. The language used in this brief attempts to be as inclusive as possible while acknowledging that the data we are citing uses gender labels that we cannot change without misrepresenting the data. ↩︎
The CDC reports the percentage of women (ages 15-49) who have ever received “infertility services” (12.7%) which also includes medical help to prevent miscarriage. We report on the percentage of adult women (ages 18-49) who have ever received medical help to become pregnant, excluding medical help once women are already pregnant. ↩︎
The CDC does not track the number of births as a result of other fertility assistance, like fertility medications or IUI. However, in the 2012 CDC National Public Health Action Plan for the Detection, Prevention and Management of Infertility, they recommended the development of surveillance systems which would monitor the utilization and health outcomes of non-IVF treatment for infertility. ↩︎
IL has a mandate to cover that applies only to group plans; however, the state’s benchmark plan includes coverage for infertility treatment, so individual plans in IL also cover these services. ↩︎
The TX benchmark plan includes coverage for diagnosis of infertility, so individual plans in TX also cover this service. ↩︎
“Comprehensive coverage” for ART defined by CDC as covering at least four oocyte (egg) retrievals. ↩︎
Availability was judged by the number of physicians performing IVF per 1,000 reproductive age women, and utilization was calculated by number of IVF cycles per 100,000 reproductive age women. ↩︎
Definitions of preconception care, basic infertility services and infertility treatment were left up to the interpretation of the respondent. ↩︎
With planning beginning for an eventual COVID-19 vaccine, one important consideration is making sure that distribution processes and outreach and communication strategies reach people of color. COVID-19 vaccination among people of color will be particularly important because they are bearing a heavy, disproportionate burden of the disease, and population immunity is not likely to be reached without high vaccination rates across all communities. However, doing so will require public health officials and providers to overcome a range of barriers to vaccination among people of color, many of which are rooted in a historic legacy of abuse and mistreatment by the medical system and ongoing racism and discrimination today.
Analysis of seasonal flu vaccination rates provides some insight into the potential barriers and issues to be addressed as part of COVID-19 vaccination efforts. Experts recommend an annual flu vaccination for all people age 6 months and older as the primary way to prevent sickness and death caused by the flu, and Healthy People 2030 national health objectives set a goal of vaccinating at least 70% of this population. Despite being widely recommended and fully covered as a preventive service under the Affordable Care Act (ACA), data show that overall flu vaccination rate remains low and that there are persistent racial disparities in uptake of the vaccine.
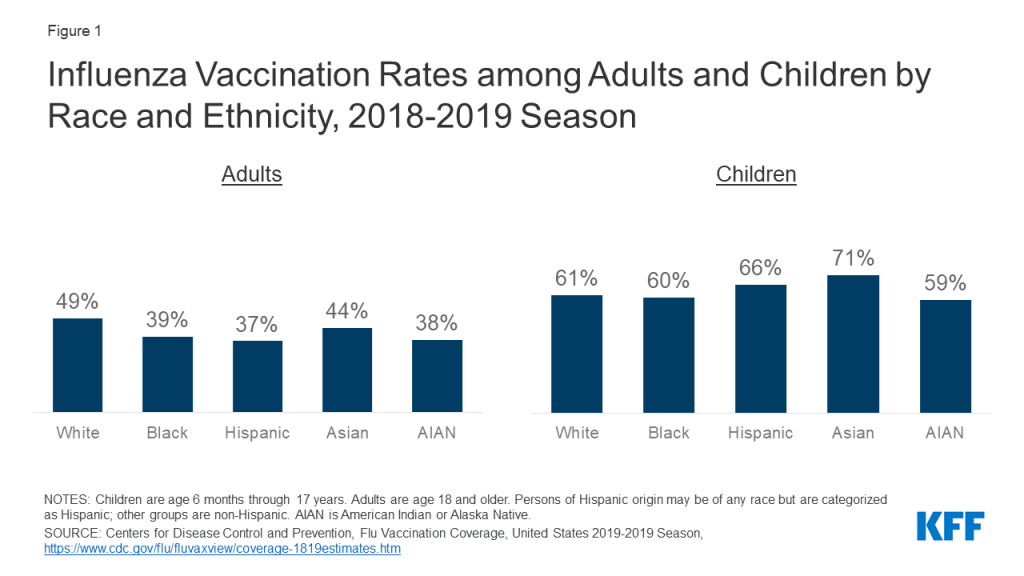
Analysis of flu vaccination rates shows persistent gaps and racial disparities in flu vaccination among adults. Data from the Centers for Disease Control and Prevention (CDC) show that the flu vaccination rate generally has been increasing over time but remains below the target level, with lower rates of vaccination among Black and Hispanic individuals compared to White individuals. These gaps and racial disparities in vaccination are concentrated among adults. During the 2018-2019 flu season, less than four in ten Black (39%), Hispanic (37%), and AIAN (38%) adults were vaccinated compared to nearly half of White adults (49%) (Figure 1). Vaccination rates were higher among children compared to adults and the rates for children of color were generally equal to or higher than those for White children.
Figure 1: Influenza Vaccination Rates among Adults and Children by Race and Ethnicity, 2018-2019 Season
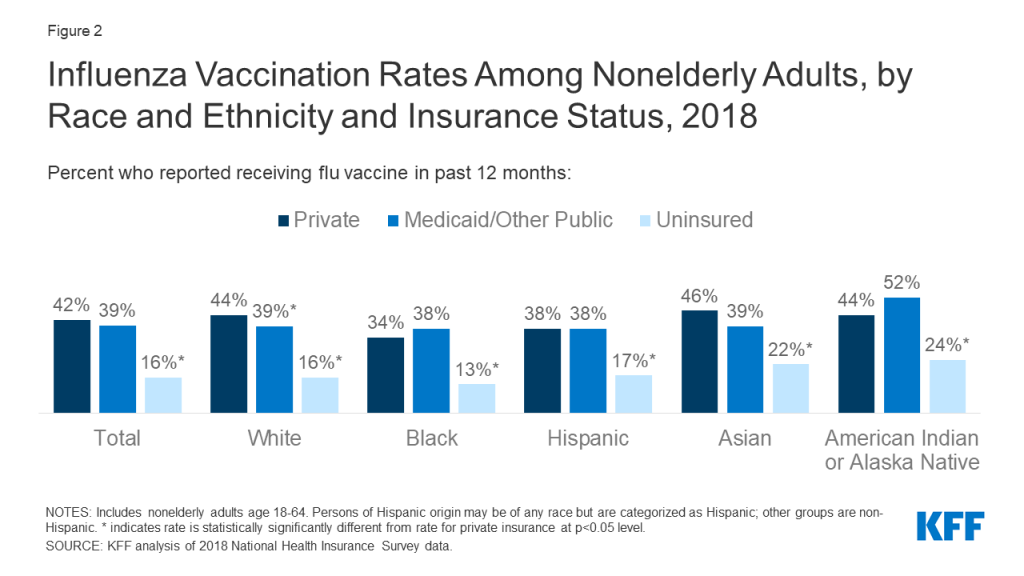
The lower vaccination rates among adults of color, in part, reflect their higher uninsured rates.Data show that people of color are more likely be uninsured and less likely to have a usual source of care. Seasonal flu vaccines, especially for adults, are delivered and administered primarily through a system of private distributors and providers. As a preventive service under the ACA, the vaccine is available at no charge for individuals with insurance. However, uninsured individuals either need to pay out-of-pocket for the vaccine or identify sites, such as clinics or health centers, that are offering it for free. Evidence suggests that the federally-funded Vaccines for Children (VFC) program, which provides vaccines at no cost to children who might not otherwise be vaccinated because of inability to pay, has contributed to the higher vaccination rates among children across racial and ethnic groups. However, analysis of National Health Interview Survey data illustrates the barriers to vaccination facing uninsured adults. Across racial and ethnic groups, uninsured adults were less likely to be vaccinated compared to those with private coverage (Figure 2). Vaccination rates among adults with Medicaid coverage were similar to those with private coverage across most groups.
Figure 2: Influenza Vaccination Rates Among Nonelderly Adults, by Race and Ethnicity and Insurance Status, 2018
Research also shows that distrust, safety concerns, and experiences with discrimination and other factors contribute to disparities in vaccination rates. For example, research shows that, compared to White adults, African American adults perceive a higher risk of side effects from the seasonal flu vaccine, have less knowledge about the vaccine, and have less trust in the vaccine. Another study found that African Americans were more likely than any other group to cite concern over the vaccine causing influenza or serious side effects as the main reason for non-vaccination. Other research shows that African American and AIAN individuals were less likely than White individuals to say they believed the 2009 H1N1 influenza vaccine was “very safe.” Another study found that the majority of people would not accept a new but not yet fully approved vaccine, with Black individuals expressing the highest level of worry. Research also points to variation among Black individuals in willingness to obtain a vaccination, for example, finding that older adults were more likely to have attitudes that increase vaccine acceptance. Additional research finds that perceptions of racial fairness and the influence of race in health care settings as well as experiences with discrimination are associated with attitudes and beliefs about the flu vaccine that may influence willingness to obtain it. Beyond differences in beliefs and attitudes, other work suggests people of color may have more “missed opportunities” for flu vaccination, finding that adults of color were more likely to remain unvaccinated compared to White adults even when they had at least one health care visit during the flu season and indicated that they would be willing to get vaccinated if a healthcare provider strongly recommended it.
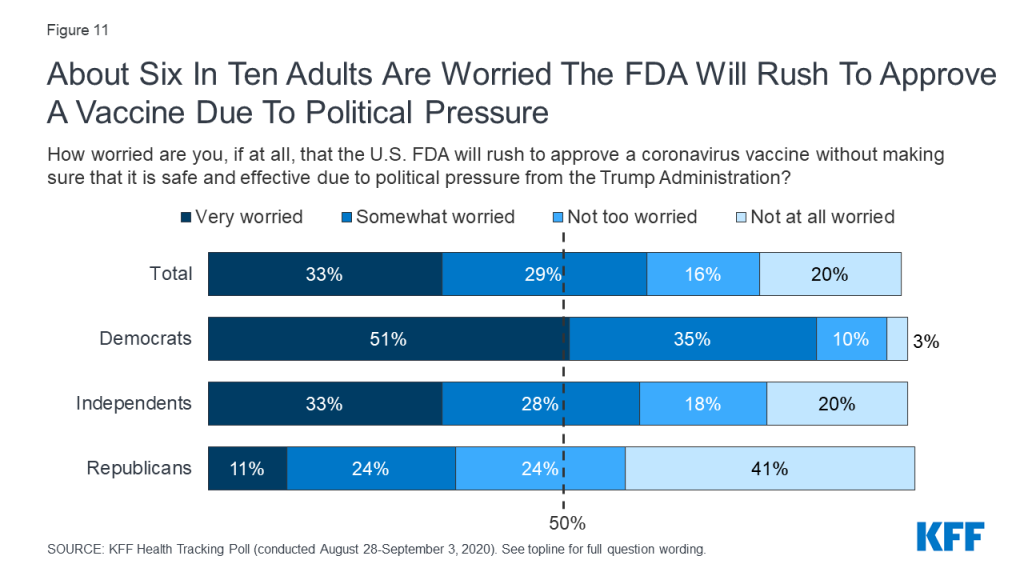
Together these findings show that once a COVID-19 vaccine becomes available, accomplishing a high vaccination rate will require addressing multiple barriers to vaccination among people of color, including access-related challenges and distrust and safety concerns. Under federal law, insurers must make the COVID-19 vaccine available at no cost. The Trump administration has also indicated it will make the vaccine available to uninsured individuals at no cost, but questions remain about whether there is sufficient funding to cover these costs. Beyond addressing cost barriers, it also will be important to make the vaccine easily accessible at convenient locations and to ensure people know where and how to access it free of charge. Moreover, effective outreach and media strategies will be important to build public trust and willingness to get the vaccine. People of color’s distrust of the health care system, particularly among Black individuals, reflects the historical legacy of the system’s abuse and mistreatment of people of color and ongoing racism and discrimination today. Distrust and safety concerns are likely to be further compounded in the context of COVID-19 vaccination efforts since the majority of the public is concerned that political pressure from the Trump administration will lead the Food and Drug Administration to rush to approve a vaccine without making sure that it is safe and effective. Research suggests that health care providers and public health agencies can increase education about vaccine recommendations and that health care providers can increase vaccine acceptance by recommending and offering a vaccine at the same time. Previous public health and health coverage enrollment experience further points to the importance of providing information in linguistically and culturally appropriate ways, proactively addressing people’s concerns, and using trusted individuals from the community as messengers. Even with targeted strategies, it likely will be difficult to overcome distrust and safety concerns, further amplifying the importance of using trusted messengers to share information and conduct outreach to the community.
From the Federal Response to COVID-19 to Ongoing Efforts to Repeal the ACA and Proposals for Lowering Drug Prices, President Trump Has an Extensive Record on Health Care
Since taking office in 2017, President Trump has laid down an extensive record on health care, including his response to the COVID-19 pandemic, his early and ongoing efforts to repeal and replace the Affordable Care Act, his annual budget proposals to curb spending on Medicare and Medicaid, his executive orders and other proposals to lower prescription drug prices, and his initiative on hospital price transparency.
President Trump’s record on health care provides a window into his policy priorities in an area that represents one-fifth of the U.S. economy and affects the lives of every American. A new issue brief from KFF describes the Trump Administration’s record on health care, including major proposals and actions relating to the COVID-19 pandemic, the ACA and private insurance markets, Medicaid, Medicare, prescription drugs and other health costs, sexual and reproductive health, mental health and substance use, immigration and health, long-term care, HIV/AIDS policy, and LGBTQ health.
The new resource is part of KFF’s ongoing efforts to provide timely and useful information about health policy issues relevant to the 2020 elections, including policy analysis, polling, and journalism. Find more on our Election 2020 resource page, including a side-by-side comparison of President Trump’s record and Democratic presidential nominee Joe Biden’s positions on key health issues.
Since taking office, President Trump has laid down an extensive record on health care, beginning on day one with his clearly-stated intention to repeal and replace the Affordable Care Act, and continuing through his most recent response to the COVID-19 pandemic. In addition, the Trump Administration has made or proposed many changes to health policies and programs that could have a significant impact on health coverage and health care.
President Trump’s record on health care illustrates his priorities. An incumbent president’s record is always relevant, but especially so for President Trump, who has not released more conventional campaign policy proposals. Moreover, the President’s response to the COVID-19 crisis, and its economic consequences could influence how voters view the president in terms of his character, his leadership and his ability to protect the nation – particularly given widespread and ongoing transmission of the virus in the U.S. and evidence that the U.S. has fared relatively poorly compared to peer nations.
The Trump Administration has moved forward on many other health care fronts. The Administration has proposed spending reductions for both Medicaid and Medicare, along with proposals that would promote flexibility for states but limit eligibility for coverage under Medicaid (e.g., work requirements). The President has made prescription drug prices a top health policy priority and has issued several executive orders and other proposals that aim to lower drug prices; most of these proposals, however, have not been implemented, other than one change that would lower the cost of insulin for some Medicare beneficiaries with diabetes, and another that allows pharmacists to tell consumers if they could save money on their prescriptions. The Trump Administration has also moved forward with an initiative to improve price transparency in an effort to lower costs, though it is held up in the courts. President Trump has made other policy changes that have had a direct impact on reproductive rights, immigration, and on other health care issues that convey his priorities for the future.
This issue brief provides a detailed overview of the Trump Administration’s record on health care issues, including major proposals and actions on health care during his tenure in office relating to: the Administration’s response to the COVID-19 pandemic, the ACA and private insurance markets, Medicaid, Medicare, reducing prescription drug and other health care costs, sexual and reproductive health, mental health and substance use, immigration and health, long-term care, HIV/AIDS policy, and LGBTQ health. A separate resource compares President Trump’s record and proposals to those of former Vice President Biden.
The COVID-19 pandemic, the worst health crisis facing the global community in more than a century, has taken a particular toll on the United States. Although the U.S. only represents 4% of the global population, it accounts for 23% of all COVID-19 cases and 21% of all deaths as of early September and ranks number one among high income countries as measured by cases per capita. The Trump administration has not established a coordinated, national plan to scale-up and implement public health measures to control the spread of coronavirus, instead choosing to have states assume primary responsibility for the COVID-19 response, with the federal government acting as back-up and “supplier of last resort.” The President has downplayed the threat of COVID-19, given conflicting messages and misinformation, and often been at odds with public health officials and scientific evidence. Despite this, the Administration has taken a number of actions to address the pandemic, including declaring federal emergencies to free up resources and flexibilities, signing emergency spending bills passed by Congress, providing emergency use authorization for hundreds of tests and other devices, issuing guidance documents, and announced “Operation Warp Speed”, to produce and deliver coronavirus vaccines. On the global front, the Administration has reduced U.S. engagement in addressing the pandemic, including ended funding for the World Health Organization (WHO) and announcing withdrawal from WHO membership.
COVID-19 Response Policy Actions
Policy
Implications
Declared federal emergencies
Three federal emergencies have been declared, enabling the authorization of funds and allowing the mobilization of resources and enhanced flexibilities to respond to the pandemic: HHS declared a public health emergency on January 31 (renewed on April 21 and July 23) and, on March 13, the President declared national emergencies under the Stafford Act and under the National Emergencies Act.
Instituted travel bans and other immigration restrictions
President’s initial response to the new outbreak was focused on sealing U.S. borders and preventing entry of the virus, beginning with China on January 31, 2020. Other actions include: establishing screening and quarantine requirements for all persons arriving in the U.S. within 14 days after having been in mainland China, and suspended entry of those traveling from Canada or Mexico to the U.S. who would otherwise be held in a congregate setting (e.g., those seeking asylum).
Issued federal social distancing and re-opening guidance
The White House issued federal social distancing guidelines on March 16 for a 15-day period, extended through the end of April. Reopening guidelines were issued on April 16.
Signed legislation and increased resources to address the costs of prevention, testing, and contact tracing
The President signed into law emergency relief legislation that was passed by Congress to eliminate cost-sharing for testing and prevention and provide funds that can be used to enhance testing capacity and/or support clinical provision of tests, and require public and private health coverage of COVID-19 diagnostic testing with no cost-sharing.
The Trump administration modified a $175 billion grant program for hospitals and other health care entities, making available a portion of funds to reimburse claims for COVID-19 testing and treatment for uninsured patients.
The Administration designated a “Testing Czar” to coordinate COVID-19 diagnostic testing across federal public health agencies, state and local authorities, and private sector.
While there is no national testing or contact tracing plan, the White House has issued a Testing Blueprint and HHS has issued a federal COVID-19 Strategic Testing Plan, as required by Congress. These documents place primary responsibility for testing and contact tracing with the states.
Despite these efforts, there have been ongoing challenges with COVID-19 testing including shortages of critical testing supplies; significant delays in turn-around times for results; and shifting and sometimes confusing federal guidelines.
Signed legislation and issued waivers related to health insurance coverage
The Administration issued an emergency regulation extending the COBRA election period.
The Administration declined to reopen ACA enrollment during the emergency period but increased the time available to sign up for marketplace plans following loss of other coverage during the pandemic.
Congress passed legislation increasing the federal Medicaid funding match rate by 6.2 percentage points from January 1 through the end of the quarter in which the public health emergency ends.
Congress passed legislation that includes several measures to address mental health and substance use disorder need (See more in Mental Health and Substance Use Section).
Signed legislation and guidance related to reopening schools
The President has pushed schools to re-open in person and suggested emergency funding would be tied to in-person schooling.
CDC issued school re-opening guidance on July 23, emphasizing the importance of in-person schooling. It has since updated and modified that recommendation.
The CARES Act includes $13 billion for elementary and secondary schools and the President has called for Congress to pass $105 billion, including $70 billion for K-12 schools.
The President has put forward eight recommendations to guide schools on reopening safely.
Signed legislation that includes protections for workers
Families First and the CARES Act provide emergency short-term paid sick leave benefits and longer-term paid family leave through the end of 2020, although at least 69 million workers are not guaranteed access to this benefit due to the law’s exclusions and the Department of Labor’s subsequent guidelines offering additional exemptions.
Families First and the CARES Act created new unemployment compensation programs for those affected by the pandemic, including a “Federal Pandemic Unemployment Compensation benefit,” which has since expired. By executive order, the President temporarily extended a portion of the federal unemployment supplement in states that could share in the cost.
The President has activated the Defense Production Act to direct domestic industry to expedite and expand supply of medical countermeasures, which can be used to help frontline health care workers.
Signed legislation and issued guidance to help hospitals/ health care facilities & providers
The Army Corps of Engineers and National Guard constructed temporary hospitals and medical centers to treat patients with COVID-19, and the Navy’s two hospital ships, the USNS Mercy and USNS Comfort, were deployed.
The CARES Act and the Paycheck Protection Act together provide $175 billion in grants to health care providers. The administration allocated a portion of the funds to reimburse providers for COVID-19 care provided to uninsured patients.
The CARES Act accelerated and increased payments to hospitals for the treatment of Medicare inpatients diagnosed with COVID-19 by 20%.
The Administration temporarily broadened access to telehealth benefits under Medicare during the emergency period.
The Administration has issued numerous guidance to and recommendations for nursing home and long-term care facilities to address COVID-19 outbreaks, including requiring nursing facilities to report COVID-19 cases and deaths and establishing an independent commission to assess their COVID-19 response. However, significant problems remain. The number of cumulative deaths in long-term care facilities has increased 7-fold from 10,000 deaths in mid-April to more than 70,000 deaths in August.
The Administration launched “Project Airbridge” to procure and transport critical supplies and equipment from overseas to the U.S.; it has since ended.
The President announced restructuring of the federal Strategic National Stockpile (SNS).
HHS announced a new partnership between Biomedical Advanced Research and Development Authority (BARDA) and private sector companies, to ensure the supply of critical medicines and pharmaceutical ingredients.
Signed legislation and announced efforts relating to research and development, treatment, and distribution for potential vaccines
Two of the four emergency spending bills passed by Congress provide funding for COVID-19 vaccines, therapies and diagnostics. As of September 2, an estimated $10.7 billion had been spent on vaccine research and development.
In June, the White House announced “Operation Warp Speed,” with the goal of delivering “300 million doses of a safe, effective vaccine for COVID-19 by January 2021.”
HHS and DoD have announced efforts to advance domestic manufacturing capabilities for vaccines and therapeutics, syringes for future vaccines, and vials that may be used for vaccines and treatments.
None of these emergency measures addresses vaccine pricing. Administration officials have said they would ensure access to vaccines without imposing price controls.
The White House decided not to participate in the WHO-led international R&D collaborative that was launched in April.
Initiated changes to international cooperation and global health security efforts
The Administration has scaled back the U.S. international engagement on global health, including related to COVID-19 as follows:
Dissolved the National Security Council’s Directorate for Global Health Security and Biodefense.
Announced it would not participate in the WHO-led global research and development initiative for drugs and vaccines.
Two of the four emergency spending bills passed by Congress and signed by the President provide funding for the global COVID-19 response, totaling $3.2 billion.
Affordable Care Act – Private Health Insurance
President Trump’s record on the Affordable Care Act (ACA) marketplaces and private insurance began on his first day in office, when he issued an executive order stating, “It is the policy of my Administration to seek the prompt repeal of the Patient Protection and Affordable Care Act.” Pending such repeal, he ordered executive branch agencies to exercise all authority and discretion available to waive, defer, grant exemptions from or delay implementation of any provision that would impose a fiscal or regulatory burden on any state, individuals, families, health care providers or health insurers. A few days later, the Administration cancelled advertising and outreach activities already scheduled and paid for to promote signups during the final week of Open Enrollment in 2017; enrollment during that week declined compared to the same period in 2016. In addition to supporting Congressional repeal of the ACA and a federal lawsuit to overturn it, the Trump Administration has taken other steps to modify how it operates.
ACA Marketplace and Private Insurance Policy Actions
The House-passed measure would replace income-related premium subsidies with a more limited, flat tax credit. It also would allow states to waive coverage of essential health benefits, allow insurers to charge higher premiums to people based on their health, and to permit pre-existing condition exclusion periods for people who experience a gap in coverage.
Congressional Budget Office estimated this would increase the number of uninsured individuals by 23 million by 2026 and reduce the federal deficit by $119 billion over 10 years.
Later in 2017, the President signed a new tax cut law that reduced the individual mandate penalty to $0.
In 2018, a group of Republican-led states filed suit in federal court (California v. Texas, formerly Texas v. US.) arguing the entire ACA is invalid.
The Trump Administration is not defending the ACA and agrees the entire law should be invalidated. However, it has asked the Supreme Court to prohibit it from enforcing only those provisions (unspecified) that are found to harm the individual plaintiffs. Oral argument is scheduled for November 10, 2020, one week after the election.
The ACA affects nearly everyone in some way; if the entire law were to be invalidated, this would have complex and far-reaching impacts throughout the health care system.
Open Enrollment in the federal marketplace was reduced to 45 days in 2017 (previously had been 90 days or longer).
Mid-year enrollments in federal marketplace were limited as of June 2017. Consumers must now document eligibility for a Special Enrollment Periods (SEP) before they can enroll. The number of SEPs in the federal marketplace fell from 1.6 million during 2015 to 800,000 over two years, 2018-2019.
Funding for navigators in federal marketplace states was cut from $63 million in 2016 to $10 million in 2019 and outreach was reduced by 90%. The Administration also changed navigator standards including ending the requirement that navigators maintain a physical presence in a state.
Nearly 5 million consumers tried unsuccessfully to find enrollment assistance during the last open enrollment. Roughly one in four marketplace enrollees who were helped by a broker or who enrolled through a commercial website say they were offered non-ACA compliant plans instead of or in addition to a marketplace plan.
Ended payments to insurers for cost sharing reduction (CSR) expenses in 2017
The Administration ended CSR payments to insurers weeks before Open Enrollment for 2018 coverage began.
Uncertainty about the future of CSR payments and the repeal/replace effort prompted many insurers to exit the marketplace for 2018, while those remaining increased silver plan premiums by 32% on average. So-called “silver loading” of premiums increased the dollar value of premium tax credits for marketplace participants, which helped to stabilize enrollment in 2018.
Short-term policies have lower premiums than ACA-compliant coverage because they can exclude pre-existing conditions and they don’t cover essential health benefits or meet other ACA standards.
A Congressional report documented enrollment of more than 3 million people in 2019 under short term policies offered by 9 insurers.
Changed marketplace plan standards and oversight in 2017, 2018 and reduced federal marketplace user fees
The federal government suspended oversight of network adequacy standards, relying instead on states or private organizations, and reduced the number of essential community providers marketplace plans must cover.
The Administration gave insurers flexibility to substitute covered benefits within and between categories of essential health benefits.
The Administration raised the threshold of annual premium increases that trigger rate review from 10% to 15%.
The Administration reduced insurer user fees that support healthcare.gov and other implementation activities from 3.5% of premium to 3%.
Relaxed standards for state waivers under Section 1332 of ACA
In evaluating whether a state ACA waiver would result in at least the same level of health coverage and affordability, the Administration will permit states to count coverage under short-term plans that exclude pre-existing conditions. It also eliminated a requirement to measure coverage access and affordability specifically for individuals with low-income or pre-existing conditions. Through waivers, states could also apply marketplace subsidies to non-ACA compliant plans and make other changes.
This 2018 regulation changed standards for coverage offered through association health plans (AHPs). Under certain circumstances, the regulation defined the AHP to be a large “employer” under federal law and not required to cover essential health benefits.
In 2019 a federal court found major provisions of this regulation to be unlawful and “clearly an end-run around the [ACA.]” The Administration is appealing this decision.
Expand employer ability to offer HRAs that can fund (pre-tax) premiums and out-of-pocket costs associated with individual coverage.
Also create a new “excepted benefit HRA” option that employees can use to pay (pre-tax) premiums for non-ACA compliant policies such as short-term policies or dread-disease policies.
A new proposed rule, issued in June 2020 (not yet final), would allow employers to reimburse employees through an HRA for fees for health care sharing ministries and direct primary care arrangements.
Other Proposals
For ACA-related changes pertaining to abortion, contraceptive coverage, non-discrimination policies and other changes pertaining to women’s health, see section below on Sexual and Reproductive Health.
Medicaid
Overall, the Trump Administration has made efforts to reduce federal spending for Medicaid and limit eligibility through proposed legislation and budget proposals, new state demonstration waivers and its support of litigation to overturn the ACA.
Released policyproposals to allow closed formularies in Medicaid (May 2018 and January 2020).
Signed into law the Continuing Appropriations Act, 2020, and Health Extenders Act of 2019, which included a provision to change calculation of prices used for Medicaid rebates (September 2019).
Released guidance on PBM rebates/price concessions and MLR claims calculations for Medicaid MCOs (May 2019) (See more in Reducing Prescription Drug and Other Health Care Costs Section).
Implemented legislation and provided guidance related to Medicaid and COVID-19
In his most recent State of the Union address, President Trump said his Administration will “protect” Medicare just as he has vowed to protect Social Security. President Trump signed into law multiple pieces of legislation that had the effect of accelerating the insolvency of the Medicare Hospital Insurance Trust Fund. The Trump Administration has proposed changes to the Medicare program, including reductions in Medicare spending through changes (or proposed changes) to provider payments, and regulatory requirements for providers and Medicare private plans (Medicare Advantage and Part D). The Administration has issued many proposals relating to Medicare prescription drug costs, most of which have not been implemented (See more in Reducing Prescription Drug and Other Health Care Costs Section).
Medicare Policy Actions
Policy
Implications
Supported repeal of the Affordable Care Act (ACA) and supporting lawsuit to overturn entire law
ACA repeal would eliminate provisions that closed the Medicare prescription drug “donut hole”; provided free coverage of preventive services; reduced Medicare payments to hospitals and other health care providers and Medicare Advantage plans, which improved the solvency of the Medicare Hospital Insurance Trust Fund; and established the CMS Innovation Center.
Signed legislation that directly affected Medicare spending and the solvency of the Medicare Hospital Insurance (HI) Trust Fund
Signed the Tax Cuts and Jobs Act of 2017, reducing federal income tax rates, which lowered payroll tax revenues, and repealed the ACA individual mandate penalty, which increased Medicare spending, both of which adversely affected the solvency of the Medicare Hospital Insurance Trust Fund.
Signed the Further Consolidated Appropriations Act of 2020, repealing the “Cadillac Tax” (the excise tax on employer-sponsored group health insurance premiums above a specified level), which lowered payroll tax revenue and adversely affected the solvency of the Medicare Hospital Insurance Trust Fund.
Signed legislation and made other changes pertaining to Medicare and COVID-19
Introduced initiatives related to Medicare provider regulatory requirements and health care data
Signed executive order in July 2017 and introduced the “Patients Over Paperwork Initiative” to revise and remove regulations.
Signed executive order in October 2017 and introduced the “MyHealthEData Initiative” in March 2018 that allows Medicare beneficiaries to view and download current and past claims and share these healthcare data in a universal digital format.
Implemented regulatory changes related to certain Medicare Accountable Care Organizations (ACOs)
Issued final rule in December 2018 that makes changes to the Medicare Shared Savings Program and requires participating ACOs to ultimately take on risk.
Introduced and implemented initiatives related to rural health
Signed executive order in August 2020 on “Improving Rural Health and Telehealth Access” that would test payment models for rural health care (CHART model below) and review telehealth policies that were expanded during the public health emergency.
Introduced the Community Health Access and Rural Transformation (CHART) Innovation Center Model in August 2020 to provide funding to rural organizations and provide advanced payments to rural-focused ACOs that join the Medicare Shared Savings Program.
Introduced and implemented initiatives related to kidney care
Signed executive order in July 2019 on “Advancing American Kidney Health,” and announced Innovation Center models to change kidney care
Issued final rule in September 2020 for the End-Stage Renal Disease Treatment Choices (ETC) Model, which will take effect in January 2021.
Reducing Prescription Drug and Other Health Care Costs
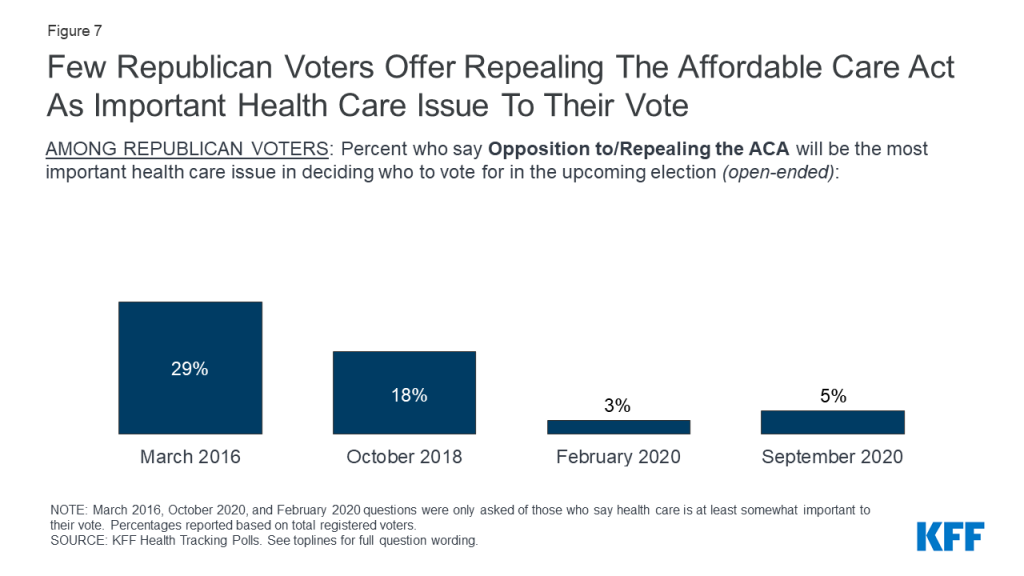
The Trump Administration has issued many proposals to lower prescription drug prices and spending, although most have not been adopted by the Congress or implemented by the Administration through the regulatory process, and pending proposals are unlikely to be adopted prior to the November election. President Trump signed into law legislation passed by Congress that banned “pharmacy gag” clauses and accelerated the phase out of the Medicare Part D “donut hole” and is moving forward with an Innovation Center model that will lower insulin costs for some Medicare beneficiaries (to take effect in 2021). In addition, the Trump Administration has moved forward on a hospital price transparency initiative that aims to give consumers better information to help lower costs.
Reducing Prescription Drug and Other Health Care Costs Policy Actions
Signed legislation that prohibits “gag clauses” in pharmacy contracts, meaning pharmacists can tell customers when they can save money on their prescriptions by paying the pharmacy’s lower cash price instead of the price negotiated by their insurance plan.
Implemented and proposed changes to Part D benefit design
Implemented legislation and released rules and proposals to change the Medicaid Drug Rebate Program
Released policy proposals to allow closed formularies in Medicaid. The drug pricing blueprint included a demonstration for five states to negotiate their own formularies. The Healthy Adult Opportunity 1115 demonstration also includes an option for closed formularies for waiver populations (May 2018 and January 2020).
Signed into law the Continuing Appropriations Act, 2020, and Health Extenders Act of 2019, which included a provision to eliminate the use of authorized generics in the price used to calculate Medicaid rebates. (September 2019).
Issued proposed rule in February 2019 (withdrawn in July 2019) and signed executive order in July 2020 requiring the HHS Secretary to promulgate regulations to ban prescription drug rebates, which is projected to reduce copays for some drugs, but increase total Medicare spending and Part D premiums; not yet implemented.
Issued final rule in May 2019 to require drug companies to disclose prices in TV ads to give consumers have more knowledge about their potential drug costs (U.S. District Court struck down proposal in July 2019; U.S. Appeals Court upheld ruling in June 2020).
Signed executive order in July 2020, and issued proposed rule in September 2020 that requires Federally Qualified Health Centers (FQHCs) that participate in the 340B program to make available insulin and injectable epinephrine at 340B price; not yet implemented.
Implemented legislation and provided guidance related to prescription drugs and COVID-19
Signed legislation requiring Part D plans (both stand-alone drug plans and Medicare Advantage drug plans) to provide up to a 90-day (3 month) supply of covered Part D drugs to enrollees who request it during the COVID-19 public health emergency.
Issued final regulations related to price transparency for hospitals
Issued an executive order and final rule that requires hospitals to disclose “standard charges” (negotiated prices) so consumers can shop for lower prices, expected to take effect in 2021 (currently being challenged in federal court)
Sexual and Reproductive Health
The Trump Administration has made efforts to reduce access to contraception by issuing regulations that allow employers to opt out of the ACA’s requirement to offer no-cost contraception in its health plans and that exclude family planning clinics that provide or refer for abortion from the Title X family planning program for low-income people. The Administration has also sought to limit access to abortion coverage and care by appointing judges opposed to abortion rights and issuing restrictive rules and regulations.
Sexual and Reproductive Health Policy Actions
Policy
Implications
Appointed federal judges opposed to abortion rights
Nearly 200 federal judges have been appointed since Trump took office. Many states have enacted abortion bans and restrictions, hoping these new judges will rule in their favor or that they are on a trajectory to the new conservative majority at the Supreme Court to reconsider the abortion precedents of Roe v. Wade and Planned Parenthood v. Casey.
Prohibited federal Title X family planning funds for clinics that provide or refer for abortion
Some federal Title X family planning funding has been redirected to faith-based organizations (“crisis pregnancy centers”) that do not provide contraception, including condoms for STI patients, and may only provide counseling on abstinence and natural family planning methods.
Issued regulations that allow employers with religious or moral objections to be exempt from the ACA’s requirement to include no-cost contraceptive coverage
Workers with health insurance provided by employers with a religious or moral objection to contraception are no longer entitled to that coverage. Female workers and dependents will have to pay for contraception out of pocket.
Issued regulations (not currently in effect) which add new billing and payment requirements for ACA Marketplace plans that include coverage for abortion
Insurers who offer plans that cover non-Hyde abortion services would have to send enrollees two separate bills, one for the portion of the premium attributable to abortion coverage and another for all other health care coverage. Policyholders would be required to make two separate payments.
Issuers in states that do not require private plans to include abortion coverage may choose to no longer cover it due to administrative burden, resulting in reduced access to abortion coverage for people buying or enrolled in a Marketplace plan.
It is unclear how these regulations would impact issuers in the 6 states that require most private plans to include coverage for abortion. Litigation brought by these states is pending.
Eliminated anti-discrimination regulatory protections in health care for patients who have terminated a pregnancy and permits providers with a religious objection to refuse to provide abortion care
Providers may discriminate against patients on the basis of termination of pregnancy.
Patients in need of abortion or other health care services that violate a provider’s religious beliefs could be denied, delayed, or discouraged from seeking care, placing them at risk of serious or life-threatening results in emergencies and other circumstances where the individual’s choice of health care provider is limited.
Litigation is ongoing.
See LGTBQ Health section below for details on anti-discrimination regulatory provisions related to protections for LGBTQ patients.
Rescinded 2016 guidance that had barred state Medicaid programs from excluding abortion providers without evidence of wrongdoing
The Trump administration approved a waiver from Texas’s Medicaid program to block Medicaid payments to Planned Parenthood and other providers affiliated with an abortion provider for non-abortion family planning services.
Disregarding Medicaid’s ‘free choice of provider’ provision limits low-income people’s access to affordable, comprehensive reproductive health care.
Promoted and expanded access to loosely-regulated short-term plans
Short-term plans allowed by the Administration typically do not cover maternity care, mental health, or prescription drugs, meaning enrollees may have to pay out-of-pocket for these services or forgo them. See ACA section for more details.
Sought to terminate the Teen Pregnancy Prevention Program (TPPP) and redirect funding to abstinence-until-marriage educational programs
In 2017, the Trump administration notified TPPP grantees nationwide that their funding would end two years early. In 2018, a district court blocked the administration from cutting the grants.
Federal funding supports abstinence-until-marriage programming that has already been demonstrated to be ineffective in preventing teen pregnancy and STIs and potentially harmful.
Supports legislative efforts to ‘repeal and replace’ the ACA and is supporting a lawsuit to overturn it
If the ACA is found to be unconstitutional, women could lose access to coverage for no-cost preventive care including mammography screenings, contraception, well woman visits, Pap smears, and other services.
Insurance reforms that ban gender rating (charging women more than men for the same coverage) and require plans to include services such as contraception and pregnancy care would be eliminated.
Signed the Preventing Maternal Deaths Act of 2018 that supports state and local surveillance of maternal mortality
Approximately 700 women die each year in U.S. as a result of pregnancy or delivery complications. The Preventing Maternal Deaths Act of 2018 authorized the CDC to increase support for state and tribal maternal mortality review committees to collect, analyze, and report data related to pregnancy-associated deaths.
Reinstated and expanded the Mexico City Policy
In January 2017, the President reinstated and expanded the Mexico City Policy, now called “Protecting Life in Global Health Assistance.” The policy requires foreign non-governmental organizations to certify that they will not “perform or actively promote abortion as a method of family planning,” even with their own funds, as a condition of receiving most U.S. global health assistance. This marks a significant expansion of the policy from prior Republican administrations.
Mental Health and Substance Use
The Trump Administration has taken steps to address the opioid epidemic and high suicide rates among veterans. The Administration also supports overturning the ACA and increased the duration of short-term health plans, steps that would ultimately reduce coverage of mental health and substance use disorder services and limit the scope of mental health parity rules. President Trump also proposed budget reductions to the Substance Abuse and Mental Health Services Administration (SAMHSA) and Medicaid, key funders for substance use disorder services. Most recently, during the COVID-19 pandemic, President Trump signed legislation providing some additional funding to SAMHSA and to support mental health services for isolated veterans.
The ACA extended mental health parity requirements to the small group, individual, and Medicaid managed care markets; and required coverage of mental health services as an “essential health benefit” in many private health plans (except large employer plans). Overturning the ACA would reduce coverage for mental health services and substantially limit the scope of mental health parity rules.
Insurers can now sell short-term health plans that provide coverage for twelve months, as opposed to three months.
Short-term health plans do not have to comply with ACA requirements, typically do not cover mental health services or substance use treatment, and generally exclude people with pre-existing conditions such as serious mental illnesses.
Released a five-point opioid strategy to address prevention and treatment, access to Naloxone, improve data collection and research.
Signed legislation approving additional grant funds to combat the opioid epidemic, including the SUPPORT for Patients and Community Act in 2018. However, President Trump’s proposed 2021 budget decreased overall funding to SAMHSA and Medicaid, key funders for substance use disorder services. The proposed budget for opioid response programs in rural areas under HRSA shows a decrease from 2019 funds.
Through the executive order, the PREVENTS task force was created to focus on suicide prevention among veterans.
Proposed 2021 budget for the Department of Veterans Affairs allocates roughly 30% more in funding for suicide prevention among veterans than the 2020 enacted budget.
Proposed 2021 budget for SAMHSA includes a small increase in funding for specific grant-based suicide prevention programs.
Proposed changes in HHS Fiscal Year Budget for behavioral health workforce development programs
The 2021 budget proposal for Health Resources and Services Administration (HRSA) includes an increase in funding (by over 20%) for behavioral health workforce development programs from 2019 to 2020. However, funding would remain flat for 2021.
Signed the CARES Act, legislation in response to the COVID-19 pandemic
The CARES Act includes several measures to address mental health and substance use disorder needs:
Allocated a $425 million appropriation for use by SAMHSA
Created provisions aimed at expanding coverage for, and availability of, telehealth and other remote care for those covered by Medicare, private insurance, and other federally-funded programs
Allowed for the Department of Veterans Affairs to arrange expansion of mental health services to isolated veterans via telehealth or other remote care services
Extended duration of, and expanded, Certified Community Behavioral Health Clinics, which are currently underway as part of efforts to increase care access and quality at community behavioral health clinics.
Immigration and Health
Since taking office, the Trump Administration has taken numerous actions to reshape immigration policy. These efforts have included limiting entry into the country, including restrictions for humanitarian immigrants such as refugees and asylees; enhancing interior enforcement efforts and expanding the scope of individuals targeted for removal; and discouraging legal immigrants from using public programs for which they are eligible, including Medicaid. A number of these actions have particularly significant implications for the health and well-being of immigrant families, including their children, who are primarily U.S.-born citizens.
Immigration and Health Policy Actions
Policy
Implications
Limited admission into the U.S.
Implemented a zero-tolerance policy in 2018 that resulted in the separation of thousands of children from their parents when they were taken into criminal custody for entering the country without authorization. Family separations were largely halted in June 2018 following an executive order and a preliminary injunction, although some separations are ongoing due to broader criteria for separating children from parents deemed to be unfit or a danger to the child.
Implemented Migrant Protection Protocols, under which families with children are sent to Mexico to await their U.S. asylum cases, and other policies that limit avenues to claim asylum in the U.S.
Also sought to withhold federal funding from jurisdictions that limit cooperation with federal enforcement agencies (i.e., sanctuary cities); this action has been blocked by the courts.
Rescinded the DACA program
In September 2017, rescinded the DACA program, which had granted permission to certain undocumented youth who came to the U.S. as children to stay in the U.S. and work for temporary renewable periods.
On June 18, 2020, the Supreme Court ruled that the termination of DACA violated federal law. However, in July 2020, the administration issued a memorandum to limit the program, including eliminating eligibility for new applicants and reducing the renewal period from two years to one.
Made changes to public charge test applied when determining whether to grant individuals entry into the U.S. or adjustment to legal permanent resident (LPR or “green card”) status
In August 2019, issued regulatory changes to public charge inadmissibility policies. (In addition, the State Department made parallel changes for individuals seeking visas or adjustment to LPR status from outside the U.S.).
Under the changes, the federal government will newly consider potential future use of certain health, nutrition, and housing programs, including non-emergency Medicaid for non-pregnant adults, when determining whether someone is likely to become a public charge and denied entry or LPR status. It also will consider age, income, health insurance coverage, and health status, among other factors. Implementation remains subject to ongoing litigation.
The changes to public charge policy will make it more difficult for individuals with lower incomes and health needs to obtain LPR status or immigrate to the U.S. Further, prior to implementation, it was already contributing to decreased enrollment in public programs and decreased use of health care among immigrant families beyond those directly affected by the rule.
Required proof of health insurance coverage or sufficient resources to pay for anticipated health care needs to enter country
On October 4, 2019, issued a proclamation suspending entry of immigrants into the United States unless they provide proof of health insurance within 30 days of entry or have financial resources to pay for reasonably foreseeable health insurance costs. Court action has blocked implementation of this requirement.
Collect data on citizenship status as part of 2020 Census and exclude undocumented immigrants from the Census count
After abandoning efforts to add a question on citizenship status to the 2020 Census, in July 2019, issued an executive order directing every federal agency to share records on citizenship status in connection with the Census data collection. In July 2020, issued a memorandum ordering the exclusion of undocumented immigrants from the Census count. Key questions remain about the legality and feasibility of this action.
Continued broad enforcement actions, curtailing of the Census period for follow-up response, and the emphasis on excluding undocumented immigrants from the Census count may result in lower response rates among immigrant households. Lower responses would affect the apportionment of Congressional representation and may also result in resources being shifted away from areas with higher shares of immigrants because the data are used to determine distribution of federal funds to the states.
Long-term Care
The Trump Administration has proposed changes to Medicaid financing that would have affected the program’s ability to pay for long-term services and supports. In addition, the Administration supported repeal of the ACA which would eliminate some options for states to expand access to Medicaid home and community-based services. Prior the onset of COVID-19, the Administration proposed changes to relax certain requirements for nursing homes, and subsequently relaxed additional requirements at the onset of the pandemic while imposing new ones to prevent the spread of the virus. Since March, as the number of COVID-19 deaths in long-term care facilities increased substantially, the Trump Administration issued new guidance and waivers, established a new commission to make recommendations, required nursing facilities to report cases, deaths and shortages, distributed tests to facilities and made additional funds available to nursing facilities and assisted living facilities.
In April 2020, CMS issued guidance directing facilities to screen all staff, residents, and visitors for symptoms, ensure staff use PPE “to the extent available,” and designate separate staff and facilities or units for COVID-19 patients. CMS also announced the formation of an independent commission to conduct a comprehensive assessment of facility response to COVID-19.
New interim final regulations require nursing homes to report COVID-19 cases and deaths weekly to the CDC, beginning in May 2020. CMS also issued nursing home reopening recommendations and an informational toolkit with best practices for states to mitigate COVID-19 in nursing homes.
In June 2020, CMS issued additional guidance to states on COVID-19 survey activities and enhanced enforcement for infection control deficiencies.
In late July 2020, CMS began requiring, rather than recommending, that all staff be tested weekly in nursing homes in states with a 5% or greater positivity rate. HHS distributed rapid diagnostic tests to nursing homes in COVID-19 hotspots through a one-time procurement to facilitate on-site testing of residents and staff.
In August 2020, CMS issued an interim final rule requiring long-term care facilities to test residents and staff for COVID-19.
The Administration also issued an emergency Section 1135 blanket waiver to allow nursing homes to employ nurse aides who do not meet federal training and certification requirements longer than four months to address potential staffing shortages due to COVID-19.
President Trump has taken steps to address the domestic HIV epidemic. In 2019, he launched a new effort, the Ending the HIV Epidemic (EHE): A Plan for America, which aims to drive down new HIV infections, especially in hard hit areas, and includes new funding for domestic HIV programs. It has helped to focus new attention and resources on HIV in the United States. At the same time, other actions of the Administration, such as ongoing attempts to overturn the ACA, which has helped to expand insurance coverage for people with HIV, and the removal of protections for LGBTQ people in health care, threaten to undermine the reach of the EHE. On the global front, the President has publicly supported PEPFAR, but called for significant budget cuts to PEPFAR and the Global Fund to Fight AIDS, Tuberculosis and Malaria each year.
HIV/AIDS Policy Actions
Policy
Implications
Left vacant the White House Office of AIDS Policy
The Administration did not appoint a director of the White House Office of National AIDS Policy, an executive office role that has been filed under both Democratic and Republican administrations since its inception in the early 1990s. HHS leads the EHE.
Launched the “Ending the HIV Epidemic” (EHE): A Plan for America
The Ending the HIV Epidemic (EHE): A Plan for America was announced during the 2019 State of the Union address and is a targeted federal approach to address HIV in the U.S., aiming to reduce new HIV infections by 75% in five years and by 90% in ten years by focusing first on the hardest hit areas of the country.
The initiative was funded at $270 million in FY20 and the Administration nearly tripled that figure with their FY21 request. It marks the first significant funding increases for CDC HIV prevention and the Ryan White HIV/AIDS Program in over a decade.
A cornerstone of the initiative expands access to pre-exposure prophylaxis (PrEP) to prevent HIV acquisition among those at higher risk.
Promoted and expanded access to short-term limited duration (STLD) plans
STLDs plans are exempt from ACA requirements prohibiting medical underwriting, pre-existing condition exclusions, and other protections and generally will not cover individuals with HIV.
Eliminated anti-discrimination regulatory protections in health care for LGBTQ patients.
Requires service members who have been “non-deployable” for 12 months to be processed for separation from military, allegedly used to discharge members with HIV. A suit challenging these discharges is pending and discharges are currently blocked.
CARES Act funding for the Ryan White and Housing Opportunities for People with AIDS (HOPWA) Programs.
The CARES Act, the third major legislative initiative to address COVID-19, included $90 million for the Ryan White HIV/AIDS Program to prevent, prepare for and respond to coronavirus and $65 million for HOPWA to maintain operations and for rental assistance, supportive services, and other necessary actions, in order to prevent, prepare for, and respond to coronavirus.
Global HIV/PEPFAR
The President has publicly supported PEPFAR and signed bipartisan reauthorization legislation for the program in 2018. However, he has requested significant budget cuts to PEPFAR and the Global Fund each year (which have been rejected by Congress).
LGBTQ Health
The Trump Administration has implemented or supported several policies that remove or reduce protections for LGBTQ people in in health care. Many of these actions have occurred against the backdrop of protections for “provider conscience.” In some cases, these policies have been halted or are still being considered by the courts.
LGBTQ Health Policy Actions
Policy
Implications
Eliminated anti-discrimination regulatory protections in health care for LGBTQ individuals.
The Trump Administration issued final regulations regarding Section 1557 of the ACA removing health care protections based on gender identity and, through conforming amendments to ten other regulations, sexual orientation. Without these protections, providers could, for example, potentially refuse to serve individuals who are transgender or who do not conform to traditional sex stereotypes or could deny services to transgender people based on their gender identity. A recent Supreme Court decision and subsequent federal district court ruling calls these actions into question and other litigation is pending.
Issued executive order directing federal agencies to expand religious protections.
Issued executive order directing federal agencies to expand religious protections, potentially laying groundwork for denying care to LGBTQ individuals, couples, and families.
Created new Division of Conscience and Religious Freedom in the Office of Civil Rights (OCR) at U.S. Department of Health and Human Services (HHS) and issued final regulation on “Conscience Rights in Health Care”
Created the Division of Conscience and Religious Freedom in the OCR at HHS and issued final regulation on “Conscience Rights in Health Care” which aims to protect health care entities from discrimination on the basis of conscience, potentially allowing for discrimination based on LGBTQ status.
Here’s our recap of the past week in the coronavirus pandemic from our tracking, policy analysis, polling, and journalism.
With U.S. coronavirus cases totaling 6.4 million and confirmed deaths edging toward the 200,000 mark, new polling indicates that 20% of registered voters say the coronavirus outbreak is the most important issue in deciding their vote for president, ranking second to the economy (32%).
The poll also reports that if there is an approved vaccine before Election Day made available free of charge, about 54% of adults say they would not want to get vaccinated. 62% of Americans worry that political pressure from the Trump administration will lead the Food and Drug Administration to rush vaccine approval without making sure it is safe and effective.
With the coronavirus outbreak an important voting issue for many Americans, a new brief presents a side-by-side comparison of President Trump and Democratic nominee Joe Biden on their records, actions and proposals related to the pandemic and its consequences.
Here are the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: Total cases worldwide surpassed 28 million this week – with an increase of approximately 1.9 million new confirmed cases in the past seven days. There were approximately 40,800 new confirmed deaths worldwide, bringing the total to more than 909,500 confirmed deaths.
U.S. Cases and Deaths: Total confirmed cases in the U.S. neared 6.4 million this week. There was an approximate increase of 246,000 confirmed cases between September 3 and September 10. Approximately 5,000 confirmed deaths in the past week brought the total in the United States to nearly 192,000.
State Reports of Long-Term Care Facility Cases and Deaths Related to COVID-19 (Includes Washington D.C.) as of 9/4
Data Reporting Status: 47 states are reporting COVID-19 data in long-term care facilities, 4 states are not reporting
Long-term care facilities with known cases: 18,147 (across 46 states)
Cases in long-term care facilities: 468,607 (across 46 states)
Deaths in long-term care facilities: 76,270 (in 47 states)
Long-term care facility cases as a share of total state cases: 8% (across 46 states)
Long-term care facility deaths as a share of total state deaths: 41% (across 47 states)
KFF Health Tracking Poll – September 2020: Top Issues in 2020 Election, The Role of Misinformation, and Views on A Potential Coronavirus Vaccine (News Release, Poll Findings)
Few issues are likely to matter as much to voters in November’s presidential election as President Trump’s response to the COVID-19 pandemic and resulting economic crisis, which have left almost 200,000 Americans dead and prompted job layoffs and furloughs affecting tens of millions of Americans.
A new election brief compares President Trump and Democratic nominee Joe Biden on their records, actions and proposals related to the pandemic and its health and economic consequences, including a detailed side-by-side table summarizing different aspects of their approaches. These matters have been generally viewed through a partisan lens by the electorate, a phenomenon well documented in KFF polling.
It is part of KFF’s ongoing efforts to provide timely and useful information related to the health policy issues relevant for the 2020 elections, including policy analysis, polling, and journalism. Find more on our Election 2020 resource page.
The coronavirus pandemic has caused a sharp increase in unemployment across the country. The unemployment rate peaked at 14.7% in April and remained above 10% until very recently. In the United States, health insurance and employment often go hand-in-hand: With the majority of working age adults receiving coverage through an employer-sponsored plan, people who lose work due to the pandemic also risk losing their health coverage when they might need it most. An earlier KFF brief, based on unemployment figures through the start of May, estimated that roughly 27 million people were at risk of losing their job-based coverage when they or family members lost their jobs. However, at the time, it was unclear what decisions employers were making about whether to keep their workers covered (e.g. by keeping furloughed workers on health plans or by helping employees pay for COBRA continuation coverage).
Data has now become available that provide a glimpse into what has happened to enrollment among employer plans since the start of the pandemic. Surprisingly, in comparison to the nearly 9% drop in employment from March to June, early data suggests that employers had kept coverage rates remarkably steady, at least through mid-summer. We examined data that insurance companies submit to the National Association of Insurance Commissioners, compiled by Mark Farrah Associates, finding that enrollment in the fully-insured group market dropped by just 1.3% from the end of March through the end of June (Figure 1).
Figure 1: Change in Overall Employment and Fully-Insured Group Market Enrollment, March to June 2020
Part of the explanation for this apparent discrepancy could be that many of the people who lost employment were never enrolled in employer-based coverage in the first place, as lower-wage workers are less likely to be covered by their employer’s plan. Even so, there are some reasons this 1.3% drop may even overstate employer coverage losses during the early months of the pandemic. For years, the fully-insured group market has gradually shrunk: While the 1.3% is the largest drop in recent years and is likely largely driven by job losses, over the last several years we have seen enrollment drops from the first to second quarter of the year ranging from 0.3% to 0.7% in the fully-insured market. Also, though we do not have data on self-funded plan enrollment rates, there are reasons to suspect the types of companies that self-insure (which tend to be larger companies) were better able to weather the early financial hits and might have had fewer job losses or might have been in a better position to let their employees retain their health benefits.
The relatively low coverage losses through the end of June are consistent with data showing growth in Medicaid enrollment through May and relatively flat Marketplace enrollment, not yet indicative of big losses in employer coverage. If there were large coverage losses in the employer market, we previously estimated that 85% would have been eligible to move to Medicaid or the ACA Marketplaces.
From discussions with employers and benefit consultants, we have heard that some employers elected to keep furloughed workers enrolled in health coverage. As the pandemic continues it’s unclear how long this can continue. Data from BLS show that temporarily laid-off workers made up the vast majority of the unemployed in the spring and early summer. However, temporary lay-offs have decreased, while the number of permanent job losses has increased through the summer. If this trend continues, we could see larger coverage losses later this year.
The first cases of a novel coronavirus were reported by the World Health Organization (WHO) in early January. Since then, the COVID-19 pandemic has become the worst health crisis facing the global community in more than a century. It has also taken a particular toll on the United States. Although the U.S. only represents 4% of the global population, as of early September, it accounts for 23% of all COVID-19 cases and 21% of all deaths, and ranks number one among high-income countries as measured by cases per capita. In addition, most states in the U.S. are considered “hotspots”, with ongoing, widespread community transmission; shortages of testing and other needed supplies also continue. COVID-19 has significantly affected daily life in America, including the economy and school closures, and has emerged as an important factor in the 2020 Presidential election. Polling data indicate that a majority of voters disapprove of President Trump’s handling of the outbreak and prefer Democratic candidate Joe Biden when it comes to tackling the pandemic. To gain a better understanding of how the candidates differ on their approach to addressing COVID-19, this document compares Trump’s record with Biden’s proposals. It starts with a broad overview of each candidate’s approach, followed by a detailed, side-by-side comparison.
Donald Trump
To date, in place of a coordinated, national plan to scale-up and implement public health measures to control the spread of coronavirus, the Trump Administration has chosen to rest the main responsibility for the COVID-19 response with the states, with the federal government serving as “back-up” and “supplier of last resort.” While this in part reflects federalism and the decentralized nature of U.S. public health, the lack of a national plan and strong federal guidelines have significantly contributed to a patchwork of policies, supplies, and outbreak trajectories across the country, and worsening community spread.
Early on, the President’s initial response to the new outbreak was focused on sealing U.S. borders and preventing entry of the virus. President Trump moved to suspend entry from China on January 31, followed by others since. However, with community transmission already underway in the U.S., and challenges with screening arriving passengers, travel restrictions were not effective in curtailing spread in the U.S. Meanwhile, the federal government was slow in bolstering public health capacities, such as testing and contact tracing, at the time the virus began to circulate domestically. As cases and deaths escalated, the gulf between what was needed and what was available grew quickly.
By mid-March, facing growing case numbers and seeing what had happened in other countries, several U.S. state and local jurisdictions began implementing stay-at-home orders and other social distancing policies. After conflicting messages from the President, who minimized the threat of the virus, the White House issued federal social distancing guidelines on March 16 for a 15-day period. Soon after, the President began pushing toward reopening, tweeting on March 22, for example, that “We cannot let the cure be worse than the problem itself. At the end of the 15 day period, we will make a decision as to which way we want to go!” and saying he hoped the country would reopen by Easter, with “packed churches.” The White House extended the social distancing period through the end of April, and issued reopening guidelines for states on April 16. Still, even before the end of April, the President began encouraging Governors to reopen, although key reopening metrics were not yet met in most places. The President has also pushed for schools to re-open in-person even though community transmission has remained high in many places, and is much higher than it was in other countries that moved to re-open in-person schooling.
There have been ongoing challenges with COVID-19 testing in particular. These started with an early, faulty test developed by the Centers for Disease Control and Prevention (CDC) that resulted in a significant delay in scaling-up testing as coronavirus spread quickly in the U.S. They have continued through to the present with ongoing shortages of critical testing supplies; significant delays in turn-around times for results; and shifting and sometimes confusing federal guidelines that have been reported to be subject to political pressure. Yet the President said in March that “Anybody that wants a test can get a test,” and in May, “As far as Americans getting a test, they should all be able to get a test right now.” More recently, while Administration officials have continued to say that anyone who needs a test could get one, they have acknowledged the need to reduce turn-around times and continue to work to increase testing capacity.
Throughout the pandemic, and even as cases and deaths increased, the President has downplayed the threat of COVID-19. For example:
On January 22, in response to a question about whether he was worried given the first report of known U.S. case, he said, “No. Not at all. And– we’re– we have it totally under control. It’s one person coming in from China, and we have it under control. It’s—going to be just fine.”
On February 2, “We pretty much shut it down coming in from China.”
On February 25, “We have very few people with it.”
On April 28, “But I think what happens is it’s going to go away. This is going to go away.”
On July 19, “I think we’re gonna be very good with the coronavirus. I think that at some point that’s going to sort of just disappear. I hope.”
On August 5, “It’s going away. Like things go away. No question in my mind that it will go away, hopefully sooner rather than later.”
The President has also given conflicting messages and conveyed misinformation about coronavirus and has sometimes been at odds with public health officials (including those in the government) and scientific evidence. For example:
He has touted the use of the drug, hydroxychloroquine to treat COVID-19, despite the lack of evidence of its effectiveness, warnings of potential harms, and even after federal COVID-19 treatment guidelines recommended against its use.
He suggested that applying ultraviolet light to or inside the body, or injecting disinfectant, could combat coronavirus.
He has questioned the use of face masks, and given inconsistent messages about their use, even after CDC guidelines recommended them. It was only in July that he began to wear one in public at times and talk about their importance.
In pushing schools to re-open in person, he has said that children are “almost immune” and “don’t have a problem,” despite evidence to the contrary.
He called the FDA’s issuance of an emergency use authorization for convalescent plasma, a potential treatment for COVID-19, “historic” and a “breakthrough,” even though the FDA itself said it “may be effective” and the National Institutes of Health COVID-19 treatment guidelines panel concluded that there were insufficient data to recommend either for or against it and at this time, it “should not be considered standard of care for the treatment of patients with COVID-19.”
President Trump and White House officials often publicly disagreed with the recommendations being made by federal officials and public health scientists. The CDC, which in previous national public health emergencies was very much in the public eye, did not give press conferences. The President has also publicly criticized Dr. Anthony Fauci, who has been the Director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health since 1984, and generally not appeared in public with him recently, unlike earlier in the pandemic.
Even as the administration’s primary strategy was to rely on states, it has taken a number of actions to address the pandemic. The President established a White House COVID-19 Task Force on January 27, even before the WHO had declared COVID-19 to be a Public Health Emergency of International Concern (PHEIC) (although leadership of the Task Force has shifted and its public-facing and internal activities have diminished). Three federal emergencies have been declared, enabling the authorization of funds and allowing the mobilization of resources and enhanced flexibilities to respond, as follows: HHS declared a public health emergency (PHE) on January 31 (renewed since then) and the President declared national emergencies under the Stafford Act and the National Emergencies Act, on March 13.
The President has also signed four emergency spending bills passed by Congress, which provide trillions to address COVID-19 and offer new flexibilities and relief for individuals, businesses, states, and localities. He has activated the use of the Defense Production Act (DPA) to expand production, prioritize, and allocate supplies in the U.S., if needed, and this authority has been used in select cases. The Food and Drug Administration (FDA) has provided emergency use authorization for hundreds of tests and other devices and the CDC has issued more than 170 guidance documents on COVID-19. In addition, the U.S. has launched “Operation Warp Speed”, a significant initiative to expedite research, development, and distribution of coronavirus vaccines. Finally, numerous other federal agencies have acted to help ease the burden of COVID-19, such as granting state Medicaid programs additional flexibilities, accelerating Medicare payments to hospitals and other health care providers, instituting new protections for nursing home residents, and issuing a strategy for “Accelerating Progress Towards Reducing COVID-19 Disparities and Achieving Health Equity.”
These measures are taking place against the backdrop of other non-COVID-19 specific Administration actions that could significantly affect the response, such as a continued push before the Supreme Court to overturn the Affordable Care Act (ACA), which has provided millions of Americans with insurance coverage and expanded access to health care.
On the global front, two of the emergency spending bills included funding for other countries, and the Administration had already begun sending international assistance to countries in need before the bills were passed. Following a more general foreign policy approach of “America First”, the Administration has chosen not to participate in several high-level international efforts to address COVID-19, has ended funding for the WHO, and has announced its intent to withdraw from WHO membership, actions that mark a significant departure from the role the U.S. has historically played, including its major role in combating the 2014 Ebola outbreak.
As part of his second term agenda, the President recently released the following goals for his proposal to “eradicate COVID-19”:
“Develop a Vaccine by The End Of 2020.”
“Return to Normal in 2021.”
“Make All Critical Medicines and Supplies for Healthcare Workers in The United States.”
“Refill Stockpiles and Prepare for Future Pandemics.”
Joe Biden
Former VP Biden has outlined a number of proposals for how he would address the coronavirus pandemic as President. VP Biden was also part of the Obama Administration’s response to the 2009 H1N1 outbreak, the 2014 Ebola outbreak, and 2016 Zika outbreak. During his tenure, the Obama Administration played a lead role in creating the “Global Health Security Agenda,” a multilateral initiative that aims to serve as “a catalyst for progress toward the vision of attaining a world safe and secure from global health threats posed by infectious diseases.” In addition, as follow-up to the 2014 Ebola outbreak, the Obama Administration established the Directorate for Global Health Security and Biodefense at the National Security Council (NSC) to lead the federal government’s pandemic response (the Directorate was disbanded by the Trump Administration in 2018).
VP Biden has put forth the following principles for his proposed response to COVID-19:
“Restoring trust, credibility, and common purpose”.
“Mounting an effective national emergency response that saves lives, protects frontline workers, and minimizes the spread of COVID-19”.
“Eliminating cost barriers for prevention of and care for COVID-19”.
“Pursuing decisive economic measures to help hard-hit workers, families, and small businesses and to stabilize the American economy”.
“Rallying the world to confront this crisis while laying the foundation for the future”.
VP Biden’s plan states that “The federal government must act swiftly and aggressively” and that “Public health emergencies require disciplined, trustworthy leadership grounded in science.” His approach calls for the federal government, not the states, to assume primary responsibility for many aspects of the COVID-19 response, including for scaling up testing and contact tracing, providing and managing the distribution of critical supplies, and setting strong national standards. For example, VP Biden has said he would call on all Americans to wear masks and work with governors and mayors to mandate mask wearing. He would appoint a “Supply Commander” to oversee national supply chain of essential equipment, medications, protective gear, directing distribution of critical equipment as cases peak at different times in different states or territories, and make more aggressive use of the DPA to direct companies to produce needed supplies. Additionally, in recognition of the disproportionate toll COVID-19 has taken on racial and ethnic minorities in the U.S., VP Biden would establish a “COVID-19 Racial and Ethnic Disparities Task Force”.
VP Biden has also called for adopting measures that go beyond what have been passed by Congress or supported by the Administration to further extend fiscal relief to individuals, schools, and businesses, provide enhanced insurance coverage, support states in providing COVID-19 related services, and eliminate cost-sharing for COVID-19 treatment. For example, VP Biden would reopen enrollment for marketplace plans and cover COBRA at 100% for those who lose their jobs and health insurance due to COVID-19. In addition, VP Biden would further expand paid leave for sick workers and those caring for family members, among others, due to COVID-19, and provide additional pay for frontline/essential workers. On vaccine pricing, he would authorize the federal government to approve the price of any COVID-19 vaccine developed with federal resources, in contrast to the Trump Administration, which has said it does not want to pursue price controls. On schools, a key difference between Biden and Trump is Biden’s emphasis on the need to get the virus under control before reopening in-person education. More broadly, VP Biden proposes to expand and protect the ACA.
On the global front, VP Biden would “re-embrace international engagement,” leadership, and cooperation. His platform states that “Even as we take urgent steps to minimize the spread of COVID-19 at home, we must also help lead the response to this crisis globally. In doing so, we will lay the groundwork for sustained global health security leadership into the future.” He would act to restore the Directorate for Global Health Security and Biodefense at the NSC and work to help create a Global Health Emergency Board to harmonize crisis response for vulnerable communities around the world. Finally, he would restore funding to and fully resource the WHO and reverse the Trump Administration’s decision to withdraw from WHO membership.
Sources
Unless otherwise noted, the following are the primary sources for this side-by-side:
The Trump Administration has declared three federal emergencies:
HHS declared a public health emergency (PHE), under Section 319 of the Public Health Service Act, on January 31 (renewed on April 21and July 23)
The President declared a national emergency under Section 501(b) of the Stafford Act, on March 13, and hasapproved major disaster declarations for all 50 states and 4 territories.
The President declared a national emergency under the National Emergencies Act, on March 13.
Travel Restrictions
Trump
Biden
Travel restrictions and limitations put in place include the following:
Suspended entry of foreign nationals from:
China on January 31
Iran on February 29
The European Schengen Area on March 11
The UK and Ireland on March 14
Brazil on May 24
Suspended entry of those on immigrant visas on April 22 (extended on June 22), designed to protect the U.S. labor market
Suspended entry of individuals traveling from Canada or Mexico to the U.S. (regardless of country of origin) who would otherwise be held in a congregate setting (e.g., those seeking asylum); this has included unaccompanied minors, some of whom have been held in hotels vs authorized holding facilities.
Established screening and quarantine requirements for all persons—including U.S. nationals, lawful permanent residents, and their immediate family members—arriving in the U.S. within 14 days after having been in mainland China.
Biden has said that, as President, “the first step I will take will be to get control of the virus that’s ruined so many lives….We will never get our economy back on track, we will never get our kids safely back to school, we will never have our lives back, until we deal with this virus.” He would implement a national strategy on day one of his Presidency.
Federal Social Distancing and Reopening Guidelines
Trump
Biden
The White House:
Issued federal social distancing guidelines on March 16 for a 15-day period, extended through the end of April.
Has said that “Social distancing is not a lightswitch. It is a dial” and that he would direct CDC to provide specific evidence-based guidance for “how to turn the dial up or down relative to the level of risk and degree of viral spread in a community, including when to open or close certain businesses, bars, restaurants, and other spaces; when to open or close schools, and what steps they need to take to make classrooms and facilities safe; appropriate restrictions on size of gatherings; when to issue stay-at-home restrictions.”
On April 12, issued a plan to re-open America safely, focused on controlling the virus.
On May 11, criticized the White House for presenting a “false choice” between health and the economy.
President Trump began encouraging schools to re-open in person in July and has suggested he would tie emergency funding for schools to in-person schooling. As recently as mid-August, the President has focused on the importance of reopening schools.
CDC issued school re-opening guidance on July 23, emphasizing the importance of in-person schooling. It has since updated and modified that recommendation.
The CARES Act includes $13 billion for elementary and secondary schools.
The President has called for Congress to pass $105 billion – $70 billion of which is for K-12 schools – to provide financial assistance and incentives to help schools implement safety measures in their resumption of in-person classes.
The President has put forward eight recommendations to guide schools on reopening safely:
Ensure all students, teachers, and staff understand the symptoms of COVID-19 and its risk factors.
Require all students, teachers, and staff to self-assess their health every morning before coming to school; if they are symptomatic, they should consult their physician.
Encourage frequent handwashing or hand sanitizing during the school day
Minimize large indoor group gatherings; hold large gatherings outdoors whenever possible.
Maintain high standards of hygiene and ventilation within all classrooms
Require students, teachers, and staff to socially distance around high-risk individuals.
Encourage the use of masks when social distancing is not possible.
Liberally post instructions regarding hygiene and social distancing around the school.
On re-opening schools, Biden has said that “Creating the conditions to make it happen should be a top national priority” and that “the decision about when to reopen safely should be made by state, tribal, and local officials, based on science and in consultation with communities and tribal governments. It should be made with the safety of students and educators in mind. And, it should be made recognizing that if we do this wrong, we will put lives at risk and set our economy and our country back.”
Setting National Safety Guidelines with objective criteria for local decision-making. Decisions on re-opening should be tied to level of risk and spread and when schools have sufficient PPE, masks and other supplies.
Providing emergency funding for public schools and child care providers, including through passage of the HEROES Act, which includes approximately $58 billion for local school districts; through renewable fund for state, tribal, and local governments; through a separate emergency package to provide $30 billion for child care providers and public schools and $4 billion to upgrade technology and broadband.
Mobilizing a Department of Education effort to develop, adopt, and share the latest tools and best practices to ensure high-equality learning
Close the COVID-19 Educational Equity Gap through a White House-led initiative to identify evidence-based policy solutions; launching a COVID-19 Educational Equity Gap Challenge Grant and other measures.
Congress has passed and the President signed emergency relief measures requiring free COVID-19 diagnostic testing and providing funding to states and localities for testing and contact tracing.
The Administration designated a “Testing Czar” to coordinate COVID-19 diagnostic testing across federal public health agencies, state and local authorities, and private sector.
While there is no national testing or contact tracing plan, the White House has issued a Testing Blueprint and HHS has issued a federal COVID-19 Strategic Testing Plan, as required by Congress.
Biden proposes to:
Ensure all who need a test can get one.
Provide daily public White House report on number of tests conducted.
Establish Pandemic Testing Board to scale up and oversee provision of diagnostic and antibody tests, including surge production of test kits and lab supplies; coordinate distribution to every state, tribe, and territory; identify testing sites and personnel; ensure adequate lab capacity and swift reporting of results; and provide clear guidance on who needs a test.
Double the number of drive-through facilities per state.
Build a National Contact Tracing Workforce by creating a U.S. Public Health Jobs Corps which would mobilize at least 100,000 people.
Addressing the Costs of COVID-19 Testing, Prevention, Treatment and an Eventual Vaccine
Trump
Biden
Congress has passed and the President has signed emergency relief measures eliminating costs for testing, preventive services, and an eventual vaccine (but in most cases, not for treatment) as follows:
The Families First Coronavirus Response Act (Families First) requires free COVID-19 diagnostic testing, provides $1 billion for the National Disaster Medical System to reimburse providers for COVID-19 testing and testing-related visits for the uninsured, and creates a new optional Medicaid eligibility pathway for states to cover COVID-19 testing and testing-related services for uninsured individuals with 100% federal matching funds (although immigrants still face restrictions on eligibility for Medicaid). As a condition of receiving Medicaid enhanced federal matching funds during the public health emergency, states must cover COVID-19 testing and treatment, including vaccines, specialized equipment, and therapies, without cost-sharing.
The Coronavirus Aid, Relief, and Economic Security Act (CARES) expands no-cost provisions for testing, prevention, and an eventual vaccine to all payers. The Trump administration is reimbursing providers for treating uninsured patients with a primary diagnosis of COVID-19 by tapping $175 billion in grant funding for hospitals and other health care entities. The administration has said it would also use this fund to pay providers to administer a COVID-19 vaccine to uninsured patients. While the CARES Act requires insurers to cover the costs of an eventual COVID-19 vaccine, it does not address vaccine pricing (nor does other federal legislation). Administration officials have said they would ensure access but do not want to impose price controls.
The Paycheck Protection Program and Healthcare Enhancement Act (Paycheck Protection) provides $11 billion in funding to states and localities for testing and contact tracing and up to $1 billion to cover the cost of testing for the uninsured.
Biden would work to eliminate cost-barriers (co-payments, deductibles, surprise billing) for all COVID-19 services and commodities, including testing, preventive services, treatment, and an eventual vaccine, for both those who are insured and uninsured, by:
Requiring all private plans (employer plans and individually purchased) to immediately cover all testing, treatment, and preventive services related to COVID-19, and for an eventual vaccine, and ensure that testing is free to everyone regardless of immigration status. On vaccine pricing, Biden would provide explicit authority for HHS Secretary to approve the commercial price of vaccines that are developed in conjunction with federally funded research.
Applying the same requirement to public plans including Medicare, Medicaid, the Children’s Health Insurance Program, Indian Health Service, Veterans Affairs, DoD’s TriCare program and the Federal Employees Health Benefits (FEHB) Program.
Fully funding and expanding authority for the National Disaster Medical System (NDMS) to reimburse health care providers for COVID-19-related treatment costs not directly covered by health insurance for the insured as well as uncompensated care incurred by uninsured and underinsured populations.
Health Insurance Coverage During the Emergency Period
Trump
Biden
In response to COVID-19, the Administration has:
Issued an emergency regulation extending COBRA election period (but has not provided subsidies).
Extended the time people have to sign up for marketplace coverage if they lose other coverage during the emergency period. However, declined to reopen ACA enrollment to all individuals during the emergency period.
Signed legislation increasing Medicaid FMAP by 6.2 percentage points from January 1 through the end of the quarter in which the public health emergency ends.
Immigrants remain subject to restrictions on eligibility for federal health and financial relief provided in response to COVID-19, as well as to health coverage more generally, that could leave them facing barriers to testing and treatment.
In response to COVID-19 specifically, Biden proposes to:
Cover COBRA at 100% for those who lose their job due to COVID-19.
Reopen ACA enrollment during the emergency period.
Increase Medicaid FMAP by at least 10 percent for all states during the crisis, with upward adjustments for states that are facing particularly high unemployment rates.
Ensure that immigrants also have access to free testing and work to reverse the Trump Administration’s public charge rule, which has made immigrant families more fearful of accessing health programs and services.
Helping Workers/Workplaces
Trump
Biden
Under President Trump:
Congress passed and the President signed legislation establishing emergency paid sick and family leave due to COVID-19, through the end of the year as follows:
Employers with fewer than 500 employees and all public employers are required to provide up to two weeks of fully-paid sick leave for eligible employees unable to work due to quarantine or isolation, or symptoms of coronavirus, and up to two-thirds pay for employees unable to work in order to care for someone in quarantine or whose child’s school or day care is closed.
Employers with fewer than 500 employees and all public employers are required to provide two-thirds pay for up to an additional 10 weeks for employees unable to work because their child’s school or day care is closed.
Employers receive refundable tax credits to cover costs of providing emergency paid leave.
Employees of private businesses with 500 or more employees are not eligible for emergency paid sick leave, totaling at least 69 million workers, including 8 million health care workers subsequently exempted by Department of Labor guidelines.
Employees of private businesses with 500 or more employees and most federal employees are not eligible for emergency paid family leave. Additionally, employers with fewer than 50 employees may be exempt from providing this benefit.
Congress passed and the President signed legislation creating new unemployment compensation programs for those affected by the pandemic, including a federally-financed $600/week supplement to state unemployment benefits that expired in late July. By executive order, the President temporarily extended a portion of the federal unemployment supplement in states that could share in the cost. No additional pay for frontline/essential workers, specifically, has been provided.
The CARES Act also provides a “recovery rebate” (a refundable tax credit) of up to $1,200 for eligible individuals ($2,400 for joint filers), and an additional $500 for each qualifying child. This benefit is limited to people filing taxes, leaving out some immigrant workers and their spouses.
The President has activated the DPA to direct domestic industry to expedite and expand supply of medical countermeasures, in the context of a national emergency. The DPA has been used to expand access to PPE, ventilators, and testing.
Expand emergency paid sick and family leave to include all workers regardless of industry, sector, or employer size.
Reimburse employers when employees use emergency paid leave benefits.
Include a refundable tax credit for employers’ extra costs of providing full health benefits to all workers during periods of work hour reductions due to COVID-19.
Ensure all essential workers have priority access to PPE, testing, childcare assistance, and other emergency COVID-19 support.
Ensure additional pay for frontline/essential workers.
Expand emergency unemployment compensation and ensure that workers receive payments quickly by issuing funds electronically or by prepaid debit cards.
Expand the use of the DPA to increase production of masks, face shields, and other PPE, and ensure equitable distribution in at-risk communities, particularly those with vulnerable populations.
Establish and enforce health and safety standards in workplaces including:
An Emergency Temporary Standard to give employers and frontline employees enforceable guidance.
Finalize permanent infectious disease standard to require health facilities and certain other high exposure workplaces to permanently. implement infection control programs to protect workers.
Double number of OSHA investigators.
Helping Hospitals/Health Care Facilities & Providers
Trump
Biden
Under President Trump:
The Army Corps of Engineers and National Guard constructed temporary hospitals and medical centers, and the Navy’s two hospital ships, the USNS Mercy and USNS Comfort, were deployed.
Congress passed and the President signed the CARES Act and the Paycheck Protection Act which together provide $175 billion in grants to health care providers.
CMS accelerated $100 billion in Medicare payments to hospitals, physicians, and other entities that participate in Medicare to minimize the effects of revenue shortfalls due to COVID-19, and the CARES Act significantly expanded this authority. The CARES Act also increased Medicare payments to hospitals for the treatment of Medicare inpatients diagnosed with COVID-19 by 20%.
Based on new waiver authority included in the Coronavirus Preparedness and Response Supplemental Appropriations Act (and amended by the CARES Act), the Administration has temporarily broadened access to telehealth benefits under Medicare during the emergency period.
The Administration has waived or modified requirements under Section 1135 of the Social Security Act to allow, for example, out-of-state providers with equivalent licensing to practice in other states.
The Administration has issued numerous guidance to and recommendations for Medicare and Medicaid certified nursing facilities to address COVID-19 outbreaks, including: restricting visitors, except for compassionate care circumstances; guidance on screening all staff, residents, and visitors for symptoms and other risk factors; requiring nursing homes to report COVID-19 cases weekly; forming an independent commission to conduct a comprehensive assessment of facility response to COVID-19; providing a one-time procurement of rapid diagnostic tests to nursing homes in COVID-19 hotspots; and requiring LTC facilities to test all residents and staff.
Prepare to stand up multi-hundred-bed temporary hospitals in any city on short notice by deploying existing Federal Medical Stations in the strategic national stockpile and preemptively defining potential locations for their use as needed.
Direct DoD to prepare for potential deployment of military resources, both the active and reserve components, and work with governors to prepare for potential deployment of National Guard resources, to provide medical facility capacity, logistical support, and additional medical personnel if necessary, including by activating the Medical Reserve Corps and deploying additional surge capacity, including U.S. Department of Veterans Affairs/DOD medical equipment and HHS Disaster Assistance Medical Teams.
Direct and assist hospitals to surge care for 20% more patients than current capacity through flexible staffing, use of telemedicine support, and delaying elective procedures.
Instruct CDC to establish real-time dashboards tracking (1) hospital admissions related to COVID-19 (2) supply chain information for essential equipment and PPE.
Expand CDC sentinel and other surveillance programs to offer tests broadly, especially to vulnerable populations like nursing home patients and people with underlying medical conditions.
Establish testing capacity so that long-term care residents could safely see at least one visitor every week.
Create “State and Local Emergency Fund” with resources to be allocated according to a formula: 45% to state governments; 45% to local governments; and 10% reserved for special assistance for “hot-spots” of community spread. Can use for medical supplies, critical health infrastructure, hiring of health care and other workers, and other services and supplies.
Building the Strategic National Stockpile & Critical Supplies
The White House launched “Project Airbridge,” an effort to procure and transport critical supplies and equipment from overseas to the U.S. Millions of supplies, including N95 respirators, surgical masks, and gowns, arrived in the US through this effort, which was shut down at the end of June.
The White House announced a restructuring of the federal Strategic National Stockpile (SNS) to improve predictive analytics of supply and demand, ensuring a 90-day supply of critical items, and fostering more domestic production and less reliance on foreign suppliers. According to the Administration, the role of the SNS is to supplement state supplies during public health emergencies, a revision from how it had previously been described.
HHS has announced new partnerships, for example between the Biomedical Advanced Research and Development Authority (BARDA) and private sector companies, to ensure the supply of critical medicines and pharmaceutical ingredients.
Biden proposes to:
Undertake a 100-day review upon taking office to identify critical national security risks across America’s international supply chains and ask Congress to enact a mandatory quadrennial Critical Supply Chain Review to institute this process permanently.
Sign an Executive Order to inventory U.S. supply chain vulnerabilities.
Appoint Supply Commander to oversee national supply chain of essential. equipment, medications, protective gear.
Increase federal stockpiles of medical supplies and other critical goods through regulation and other measures.
Direct distribution of critical equipment as cases peak at different times in different states or territories.
Use the DPA to manufacture critical products, including those immediately needed to respond to the COVID-19 pandemic in near term and create process to determine the best way forward over the mid- and long-term.
Work with businesses to expand production of critical supplies and incentivize greater supplier production, including committing, if necessary, to large scale volume purchasing and removing all relevant trade barriers to their acquisition.
Task the Department of Justice with combating price gouging for critical supplies.
Use BARDA to spur medical production to ensure adequate production of vaccines and other medical countermeasures to address COVID-19.
Leverage federal purchasing power to encourage pharmaceutical companies to make key drugs, drug inputs, and medical devices in the U.S. while ensuring fair and transparent pricing.
Ensure the U.S. tax code encourages on-shoring of pharmaceutical supply chains.
Research & Development/ Treatment and Vaccine Distribution
Trump
Biden
Under President Trump:
Congress passed and the President signed emergency legislation providing additional funding for vaccines, therapies and diagnostics totaling an estimated $9 billion.
In June, the White House announced “Operation Warp Speed” with the goal of delivering “300 million doses of a safe, effective vaccine for COVID-19 by January 2021” through “investing in and coordinating countermeasure development.”
HHS announceda task order to advance domestic manufacturing capabilities for vaccines and therapeutics.
DoD and HHS announceda $138 million contract for more than 100 million syringes for future vaccines.
HHS and DoD announced a joint effort to increase domestic manufacturing capacity for vials.
As part of Operation Warp Speed, US agencies, including CDC and DoD, developing portfolio of distribution options for eventual COVID vaccines.
The White House decided not to participate in the WHO-led international R&D collaborative that was launched in April.
Biden proposes to:
Establish a New Emerging Infectious Disease Clinical Trial Network.
Scale-up National Institutes of Health-funded COVID-19 pediatric research partnerships to help address gaps in understanding of how the virus affects children and generate evidence-based guidance.
Invest $25 billion in a vaccine manufacturing and distribution plan, and plan for the effective, equitable distribution of treatments and vaccines.
Be part of coordinated global approach to develop a safe, effective vaccine and the manufacturing capacity for the doses and related materials like syringes that we will need at home and around the world.
The following 3 principles should guide vaccine development:
Put scientists in charge of all decisions on safety and efficacy.
Publicly release clinical data for any vaccine the FDA approves.
Authorize career staff to write a written report for public review and permit them to appear before Congress.
International Cooperation and Global Health Security
Trump
Biden
Under President Trump:
An “America First” approach has guided foreign policy.
The National Security Council’s Directorate for Global Health Security and Biodefense (charged with overseeing pandemic response) was dissolved in 2018.
Supported the extension of The Global Health Security Agenda (GHSA) for another five-year period (2019-2024).
The President signed legislation providing $3.2 billion for global COVID-19 response efforts, to assist governments, international efforts and non-governmental organizations.
The U.S. announced it would not participate in the WHO-led global research and development initiative for drugs and vaccines.
The White House suspended funding for the World Health Organization (WHO) and announced its intention to withdraw the U.S. from WHO membership.
Biden proposes to:
Re-embrace international engagement and alliances.
Restore the National Security Council’s Directorate for Global Health Security and Biodefense, created under the Obama Administration.
Empower the State Department to ensure the U.S. plays a major role in all global decisions about COVID-19.
Direct USAID, in coordination with State, DOD, HHS, and CDC, to mobilize an international response to assist vulnerable nations.
Help create a Global Health Emergency Board to harmonize crisis response for vulnerable communities, including to offset the cost of an eventual vaccine, with leadership from the U.S., G7 partners, and other countries in support of WHO.
Bolster CDC and DOD’s disease detection and protection programs overseas.
Re-launch and strengthen USAID’s “PREDICT” program.
Revitalize, elevate, expand Global Health Security Agenda GHSA including by fully staffing all federal agencies and advisory groups focused on global health security, establishing an Assistant Secretary at the State Department to oversee an office of Global Health Security and Diplomacy, and prioritizing sustained funding for global health security.
Call for creation of a Permanent Facilitator within the Office of the United Nations Secretary-General for Response to High Consequence Biological Events.
Fully resource WHO and reverse Trump Administration decision to withdraw from WHO membership.
The economy has now secured a spot as the top issue in the 2020 election with one-third of registered voters (32%) saying it will be the most important issue in deciding their vote for president, followed by the coronavirus outbreak (20%), criminal justice and policing (16%), and race relations (14%). There is a strong partisan divide, with Republican voters prioritizing the economy followed by criminal justice and policing, and Democratic voters prioritizing coronavirus followed by race relations. The share of voters who say health care will be the most important issue in deciding their vote has dropped 16 percentage points since February (from 26% to 10%), and outside of coronavirus, health care now ranks 5th as an issue for voters (and ranks 3rd for Democrats).
In light of recent protests following the police shooting of Jacob Blake in Kenosha, Wisconsin and President Trump’s focus on violence in cities as a campaign issue, the share of voters who now say violence caused by protestors is a “big problem” in the U.S. has increased 15 percentage points since June (52% compared to 37%). The increase in the share who say violence caused by protesters is a big problem is particularly large among Republican and independent voters as well as among white voters (which is mostly driven by white Republicans rather than Democrats).
Recently, the Centers for Disease Control and Prevention (CDC) issued a notice to states to start preparing to distribute a coronavirus vaccine by November 1st, 2 days before the 2020 election. Most adults (81%), including majorities across partisans, do not think a vaccine for coronavirus will be widely available in the U.S. before the presidential election in November.
Many (62%) are worried that the political pressure from the Trump administration will lead the FDA to rush to approve a coronavirus vaccine without making sure that it is safe and effective – including 85% of Democrats and 61% of independents. Fewer Republicans (35%) express this level of concern. About four in ten adults overall say both the FDA (39%) and the CDC (42%) are paying “too much attention” to politics when it comes to reviewing and approving treatments for coronavirus or issuing guidelines and recommendations.
The latest KFF Health Tracking Poll finds a shift in the public’s attitudes on the coronavirus outbreak. More than six months into the pandemic, about four in ten (38%) now say “the worst is yet to come” (down nearly half from 74% in early April), while an equal 38% say “the worst is behind us” (up from 13% in April).
Nearly half of adults hold at least one misconception about coronavirus prevention and treatment, including one in five who say wearing a face mask is harmful to your health and one in four who say hydroxychloroquine is an effective treatment for coronavirus. Three in four Republicans have at least one misconception, compared to 46% of independents and one in four Democrats. At the same time, trust in some official sources of information on coronavirus has declined since April, including a particularly steep drop in Republicans’ trust of Dr. Anthony Fauci and the CDC.
One-Third Of Voters Say Economy Is Most Important Issue For 2020 Election; Health Care Ranks Lower
With less than two months before the 2020 November election, one-third of registered voters (32%) say the economy is going to be the most important issue in deciding their vote for president. About one-fifth of voters say the coronavirus outbreak (20%) is the top issue, while about one in seven say criminal justice and policing (16%) or race relations (14%) are the top issues. Fewer voters choose health care (10%) or immigration (4%) as the most important issue in deciding their vote for president.
Figure 1: Voters Say The Economy Is Top Issue For The 2020 Presidential Election
The economy is overwhelmingly the top issue for Republican voters with more than half (53%) choosing it as the most important issue in making their decision about who to vote for president, and it is also the top issue for independent voters (29%). Nearly four in ten Democratic voters (36%) say the coronavirus outbreak is the top issue in deciding their vote, followed by race relations (27%). Few Republican voters say the coronavirus outbreak (4%) or race relations (2%) is their top issue in the election.
Figure 2: Democratic Voters Prioritize Coronavirus In Presidential Voting Decision, Republicans Prioritize The Economy
The latest KFF Health Tracking Poll was conducted soon after the police shooting of Jacob Blake in Kenosha, Wisconsin (fielded August 28-September 3) and amidst the nation struggling with the health and economic effects of the coronavirus pandemic. Besides coronavirus, which ranks second as a voting issue, the issue of health care in general (which dominated the presidential campaign in early 2020), has fallen as a priority for voters and now ranks behind the economy, coronavirus, criminal justice and policing, and race relations. Democrats continue to prioritize the issue of health care more highly than independents or Republicans, ranking it third (tied with the economy, and ranking behind the coronavirus pandemic and race relations).
Figure 3: Besides Coronavirus, Health Care Is No Longer A Top Issue For Voters In Deciding The 2020 Presidential Election
Swing voters
The economy is also now the top issue for swing voters, the crucial group of voters who say they are “probably” going to vote for either President Trump or former Vice President Biden but haven’t made up their minds yet or say they are still “undecided” about who they are going to vote for (24% of voters are “swing voters”).
Swing Voters
A majority of voters have already decided who they plan on voting for in the 2020 presidential election with more than one-third of voters (35%) saying they are “definitely going to vote for President Trump” and four in ten (38%) saying they are “definitely going to vote for Joe Biden.” Yet, there is a crucial group of voters, “swing voters,” who have not made up their minds yet. When asked how they plan to vote in 2020, about one-fourth (24%) of registered voters either say they are either “undecided” or don’t know who they are going to vote for (6%), “probably going to vote for President Trump” (8%), or “probably going to vote for Joe Biden” (10%), but haven’t made up their minds yet.
About one-third (35%) of swing voters say the economy is their top issue, followed by criminal justice and policing (17%), the coronavirus outbreak (15%), and race relations (14%). About one in ten swing voters (11%) say health care is their top issue while few swing voters (2%) choose immigration is their top issue.
Figure 4: Swing Voters Say The Economy Is The Most Important Issue In Deciding Their Vote For President
Recent events May Be shifting Voters’ priorities
The recent police shootings of unarmed black Americans and subsequent protests have resonated with voters with both criminal justice and policing and race relations ranking among the top election issues, depending on party identification. About one-fourth of Democratic voters (27%) say race relations is going to be the most important issue in deciding their vote for president while a similar share of Republicans (23%) say criminal justice and policing will be the top issue in to their vote.
In addition, large majorities of voters view racism, police violence, and violence caused by protestors as at least “somewhat of a problem” in the U.S. About six in ten (58%) say racism is a “big problem” while about four in ten say the same about police violence against the public (43%). Over the past three months, there has been a 15 percentage point increase in the share of voters who say violence caused by protestors is a “big problem,” 52% compared to 37% in June. This comes as national attention has focused on protests and acts of violence in cities like Kenosha, Wisconsin and Portland, Oregon, and as President Trump has made tamping down violence in cities a central issue in his campaign.
Figure 5: Majorities Say Racism, Violent Protests, And Police Violence Are Problems In The U.S. Today
The partisan divisions in perceptions of these problems, especially views about the violence caused by protestors, have also shifted since June. While a large majority of Democratic voters and six in ten independent voters continue to say racism is “big problem” in the U.S. today, compared to 33% of Republican voters; now eight in ten Republican voters (81%) and half of independent voters (52%) say violence caused by protestors is “big problem,” compared to 62% of Republican voters and 35% of independent voters back in June. One-fourth of Democratic voters say this is a “big problem” – relatively unchanged since June (21%).
Table 1: Increasing Partisan Divide On How Big Of A Problem Racism, Protestor Violence Is In U.S.
Percent of voters who say each of the following is a “big problem” in the U.S. today:
Party ID
Democratic voters
Independent voters
Republican voters
KFF Health Tracking Poll – September 2020
Racism
84%
58%
33%
Police violence against the public
67
39
20
Violence caused by protesters
25
52
81
KFF Health Tracking Poll – June 2020
Racism
82
57
25
Police violence against the public
63
38
13
Violence caused by protesters
21
35
62
Percentage point change (June-September)
Racism
+2
+1
+8
Police violence against the public
+4
+1
+7
Violence caused by protesters
+4
+17
+19
This shift is notable among all white voters with now similar shares of white voters saying that violence caused by protestors (56%) and racism (53%) are each a “big problem” in the U.S. today. The share of white voters who say violence caused by protestors is a “big problem” is up 17 percentage points since June, mostly driven by the views of white Republicans and independents and less of a change among white Democratic voters. About four in ten (37%) white voters say police violence against the public is a big problem.
Health Care As A Voting Issue
In the early months of 2020 and during the height of the Democratic primary contest, health care was consistently rated as one of the top issues for voters and was the top issue for Democratic primary voters in all of the seventeen Democratic contests analyzed by KFF researchers. But the latest KFF poll finds voters’ priorities have shifted during the last six months with the coronavirus outbreak, the closing of businesses due to the spread of the virus and subsequent recession, the police shootings of unarmed Black Americans, and violence occurring around protests. When asked what about health care is important to their vote, voters offer responses related to increasing access to health insurance coverage (18%) such as universal coverage, the cost of health care (15%) including issues around affordability and the cost of prescription drugs, the coronavirus outbreak (8%), and Medicare or senior concerns (7%).
Figure 6: Costs And Access Are Still Top Health Care Concerns
A health care issue that no longer seems to be resonating with voters, especially Republican voters, is the 2010 Affordable Care Act (ACA). The latest KFF Health Tracking Poll finds 5% of Republican voters offering responses related to opposing or getting rid of the ACA as a top health care issue (compared to 29% of Republican voters who said the same prior to the 2016 presidential election).
Figure 7: Few Republican Voters Offer Repealing The Affordable Care Act As Important Health Care Issue To Their Vote
A recent analysis of the Republican National Convention found only one mention of the ACA during the 2020 convention, compared to 13 mentions in 2016 and 23 mentions in 2012. The future of the ACA is still in question as the U.S. Supreme Court case will hear arguments for Texas v. California, the court case challenging the law’s constitutionality, one week following the November election.
Overall views towards the 2010 health reform law remain similar to July, with half of the public (49%) continuing to hold favorable views of the ACA while 42% view the law unfavorably (up slightly from 36%). The increase in the share with an unfavorable view was mostly driven by independents (41% now view it unfavorably compared to 35% in July) while a majority of Democrats continue to favor the law and most Republicans continue to hold unfavorable views with 79% saying they have an unfavorable opinion, showing that it is still unpopular among Republicans even if it is no longer a top issue in the 2020 election. KFF has been tracking views of the ACA since April 2010.
Figure 8: Public Views Of The Affordable Care Act Are Mostly Stable With Half Viewing The Law Favorably
Half Of Voters Say Biden Has Better Approach On Most Health Care Issues
At least half of voters think former Vice President Biden has a better approach than President Trump to handle a variety of different health care issues including making decisions about women’s reproductive health choices and services (55%), determining the future of the ACA (54%), maintaining protections for people with pre-existing health conditions (52%), and ensuring access to health care and insurance (52%). On all of these health care issues, a larger share of voters say Biden has the better approach than say the same about President Trump. Voters are more divided on which candidate has the best approach lowering the cost of health care for individuals and protecting people from surprise medical bills with nearly half of voters saying they think Biden has the better approach compared to four in ten who say President Trump does.
When it comes to overseeing the development and distribution of a COVID-19 vaccine, voters are more closely divided with Biden having a slight, but not statistically significant, advantage. About half (49%) of voters say Biden has the better approach for the COVID-19 vaccine while 44% say President Trump does. Voters are also divided on who has the better approach to lowering prescription drug costs, an issue that President Trump has been focusing on throughout his presidency.
Figure 9: Half Of Voters Say Biden Has Better Approach To Handle Most Health Care Issues
As expected, views on which candidate has the better approach largely fall down party lines with vast majorities of Democratic voters saying Biden has the better approach (93%) and nine in ten Republican voters (91%) saying President Trump has the better approach. Independent voters are equally divided with about four in ten saying each candidate has the better approach to the development and distribution of a vaccine.
Table 2: Partisan Voters Give Their Party’s Candidate The Advantage On The Development Of COVID-19 Vaccine
Percent who say each has the better approach to overseeing the development and distribution of a COVID-19 vaccine:
Democratic voters
Independent voters
Republican voters
Donald Trump
5%
43%
91%
Joe Biden
93
44
4
Don’t know (vol.)
2
10
3
Few Expect A Coronavirus Vaccine Before The November Election
On September 2nd, the Centers for Disease Control and Prevention alerted states that they should be ready to distribute a coronavirus vaccine by November 1st, two days before the 2020 election. The latest KFF Tracking Poll finds most adults (81%) – including majorities of Democrats (90%), independents (84%), and Republicans (75%) – do not think a vaccine for coronavirus will be widely available in the U.S. before the presidential election in November. Moreover, if a coronavirus vaccine was indeed approved by the FDA before the election and was made available and free to everyone who wanted it, just four in ten adults (42%) say they would want to get vaccinated while a slight majority (54%) say they would not want to get vaccinated under those circumstances. Notably half of Democrats (50%) say they would get vaccinated if a vaccine were available before the election while majorities of independents (56%) and Republicans (60%) say they would not get the vaccine.
Figure 10: Most Do Not Expect A Vaccine Before The November Election, Just Four In Ten Would Get A Vaccine If It Was Available Before Then
A majority of the public (62%) is worried that the political pressure from the Trump Administration will lead the FDA to rush to approve a coronavirus vaccine without making sure that it is safe and effective. A third of adults (33%) say they are “very worried” the FDA will rush to approve a vaccine while a further 29% say they are “somewhat worried.” Across partisans, 85% of Democrats and six in ten independents (61%) say they are worried the FDA will rush to approve a vaccine, while fewer Republicans (35%) express this level of concern. Notably, women are more likely than men to say they are worried the FDA will rush to approve a vaccine (70% vs. 55%).
Figure 11: About Six In Ten Adults Are Worried The FDA Will Rush To Approve A Vaccine Due To Political Pressure
Public’s Views On Coronavirus Outbreak May Be Shifting
More than six months into a pandemic that has killed more than 180,000 Americans, the public is divided on whether the worst is behind us or yet to come. This comes on the heels of a Republican National Convention in which President Trump was lauded for his handling of COVID-19 and with conflicting information about the availability of a vaccine this fall. About four in ten (38% each) say “the worst is behind us” or “the worst is yet to come.” The share of adults who think the worst is yet to come has decreased by 22 percentage points since July.
Figure 12: Fewer Adults Now Say The Worst Of The Coronavirus Outbreak Is Yet To Come
Across partisans, a majority of Republicans (56%) say the worst of the coronavirus outbreak is behind us (up from 31% in July). While a majority of Democrats (58%) say the worst is yet to come, the share who expect the worst still lays ahead has decreased by 21 percentage points since July.
Figure 13: Six In Ten Democrats Say The Worst Of Coronavirus Is Yet To Come; Similar Share Of Republicans Say The Worst Is Behind Us
In addition, President Trump is now receiving slightly better marks on his handling of the coronavirus, with the share of the public who approve of his handling of the outbreak in the U.S. up 9 percentage points since July 2020. A slight majority (55%) still disapprove of his handling of the current coronavirus outbreak (down from 62% in July).
Figure 14: President Trump Receives More Positive Marks On Handling Of Coronavirus In U.S., Majority Still Disapprove
The Public Is Divided In Who They Trust For Coronavirus Information, Some Misconceptions Exist
CDC and Fauci Are Most Trusted Information Sources, But Trust In Both Has Become Increasingly Partisan
About two in three adults say they have at least a fair amount of trust in Dr. Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases (68%), and in the U.S. Centers for Disease Control and Prevention (CDC) (67%) to provide reliable information on coronavirus. About half say they trust Dr. Deborah Birx, the Coronavirus Response Coordinator for the White House Coronavirus Task Force (53%) as a reliable source of information. Half of the public say they trust Joe Biden to provide reliable information on coronavirus while about four in ten say the same about President Trump (52% vs. 40%).
Figure 15: Most Adults Have At Least A Fair Amount Of Trust In Dr. Fauci, The CDC, And Dr. Birx To Provide Reliable Information On Coronavirus
While majorities across partisans continue to trust the CDC, there are large partisan differences on trust in other sources, with Democrats more likely to trust Joe Biden and Dr. Anthony Fauci, and Republicans more likely to trust President Trump and Dr. Deborah Birx.
Table 3: Trust In Sources of Coronavirus Information By Party Identification
Percent who say they trust each of the following a great deal or a fair amount to provide reliable information on coronavirus:
Total
Party ID
Democrats
Independents
Republicans
Dr. Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases
68%
86%
71%
48%
The U.S. Centers for Disease Control and Prevention, or CDC
67
74
70
60
Dr. Deborah Birx, the Coronavirus Response Coordinator for the White House Coronavirus Task Force
53
44
54
70
Joe Biden
52
91
48
16
President Trump
40
8
37
86
Notably, the share of adults who trust the CDC to provide reliable information has decreased by 16 percentage points since April. Similarly, the share of adults who say they trust Dr. Anthony Fauci has declined by 10 percentage points since April. Trust in the CDC has decreased from April across partisans, though the decrease has been among Republicans in particularly steep, with 60% now saying they trust the CDC, down 30 percentage points from April when 90% said they trusted the CDC to provide reliable information. Likewise, there has been a steep decline in trust of Dr. Anthony Fauci among Republicans. While the share of Democrats who say they trust Dr. Fauci has increased slightly since April (86%, up from 80%), among Republicans, the share who trust Dr. Fauci has decreased by 29 percentage points (48%, down from 77%).
Figure 16: Trust In The CDC And Dr. Anthony Fauci Has Declined Since April
Public mostly knows key facts about coronavirus, though some MISCONCEPTIONS remain
A large majority of the public (87%) is aware that there is no FDA-approved vaccine to prevent coronavirus and that it is possible for children under 18 to transmit coronavirus to other people (88%). Similarly, eight in ten (80%) know that there is no cure for coronavirus and that wearing a face mask helps to limit the spread of coronavirus (81%). Three in four adults (77%) know that wearing a face mask is not harmful to your health, though notably, one in five adults say wearing a face mask is harmful. While 55% of adults say hydroxychloroquine is not an effective treatment for COVID-19, one in four (24%) say it is an effective treatment. Nearly half of adults (48%) hold at least one misconception about coronavirus prevention and treatment, giving an incorrect answer to at least one of these questions.
Figure 17: Most Adults Know Key Facts About Coronavirus, Though Some Misconceptions Remain
There are some notable partisan differences on some key coronavirus facts. While majorities across partisans say wearing a facemask is not harmful to your health, Republicans (36%) are more likely than Democrats (7%) and independents (17%) to say wearing a face mask is harmful. Similarly, while majorities across partisans say wearing a face mask helps to limit the spread of coronavirus, Republicans (32%) are more likely than Democrats (3%) and independents (17%) to say masks do not help to limit the spread. Perhaps reflecting the difference among partisans in who they trust for reliable information, the largest partisan gap is on hydroxychloroquine, which President Trump has touted as a treatment for coronavirus. Most Democrats (78%) and independents (57%) say it is not an effective treatment for COVID-19. However, half of Republicans (51%) say it is an effective treatment.
Table 4: Misconceptions of Coronavirus Facts By Party Identification
Total
Party ID
Democrats
Independents
Republicans
Percent who believe in at least one misconception:
48%
25%
46%
73%
Percent who say:
…Hydroxychloroquine is an effective treatment for COVID-19
24
8
20
51
…wearing a face mask is harmful to your health
20
7
17
36
…there is a cure for coronavirus
14
12
15
13
…there is a vaccine to prevent coronavirus that has been approved by the U.S. FDA
7
8
6
6
…wearing a face mask does not help limit the spread of coronavirus
16
3
17
32
…it is not possible for children under age 18 to transmit coronavirus to other people
8
3
9
13
In August, the U.S. Food and Drug Administration (FDA) issued an emergency use authorization for convalescent plasma in the treatment of COVID-19. In a press conference with President Trump, FDA commissioner Stephen Hahn misstated the benefits of convalescent plasma and has since clarified his remarks. A slight majority of the public (55%) has heard about convalescent plasma receiving emergency authorization from the FDA. Among those who have heard about this new treatment for COVID-19, about three in four (74%) say more studies are needed to determine how effective it is. Majorities across partisans say more studies are needed to determine the effectiveness of convalescent plasma for treating people who are sick from coronavirus.
Figure 18: Over Half Of Adults Have Heard Of Convalescent Plasma Treatment, Most Say More Studies Are Needed To Determine Effectiveness
Commissioner Hahn’s misstatement in his press conference with President Trump and his subsequent clarification has highlighted the issue of potential political pressure impacting the work of organizations such as the FDA and the CDC. The public is divided on whether the FDA pays enough attention to science when approving treatments for coronavirus with 43% saying it pays about the right amount of attention to science while 46% say it does not pay enough attention. The public is similarly divided on whether the CDC pays enough attention to science when issuing guidelines and recommendations related to coronavirus with 43% saying it pays about the right amount of attention and 46% saying it does not pay enough attention to science.
However, when asked about the amount of attention these two organizations pay to politics, pluralities say they pay too much attention. About four in ten (39%) say the FDA pays too much attention to politics when reviewing and approving treatments for coronavirus, while a similar share say the CDC pays too much attention to politics when issuing guidelines and recommendations related to coronavirus.
Figure 19: About Four In Ten Say The FDA And The CDC Pay Too Much Attention To Politics
Majorities of Democrats say that under the Trump Administration, the FDA and the CDC pay too much attention to politics. About four in ten independents say these organizations pay too much attention to politics. Among Republicans, about one in five (19%) say that under the Trump Administration, the FDA pays too much attention to politics when approving treatments for coronavirus while about a third (35%) say the CDC pays too much attention to politics when issuing guidelines and recommendations related to coronavirus.
Figure 20: Over Half Of Democrats And Four In Ten Independents Say The FDA And The CDC Pay Too Much Attention To Politics
These additional findings were released October 1.
In previous KFF surveys, large shares of public have reported putting off or postponing different types of care due to cost. Since the outbreak of the coronavirus pandemic in the U.S., many hospitals and medical offices have had to close for periods of time, limited capacity, and many elective procedures have been postponed. Moreover, with adults across the nation urged to social distance, the coronavirus pandemic and its related safety concerns have kept many adults from seeking medical and dental care. The September KFF Health Tracking Poll asks people whether they have put off medical care for any reason in the past six months, and then drills down to find out the reasons why people may have skipped or postponed care, the type of care that was skipped, and whether they anticipate getting the delayed care in the coming months. Compared to June, fewer people now report skipping care due coronavirus-related office closures and safety concerns, suggesting that as medical offices have reopened, some people are now getting care they postponed earlier this year. However, the ongoing outbreak – along with concerns over the cost and affordability of care – continue to keep some adults from seeking the medical and dental care they may need.
Four In Ten Adults Say Someone In Their Household Skipped Or Postponed Care
As the country continues to deal with the ongoing coronavirus pandemic and its public health and economic impacts, four in ten adults (42%) say that they or a family member living in their household skipped or postponed some type of medical or dental care in the past six months (including 18% who say they personally skipped or postponed care, 7% who say it was only a family member, and 17% who say both they and a family member).
When asked what type of care they or a family member skipped or postponed, 13% say it was dental care only, 8% say it was only medical care, and one in five (21%) say they or family member skipped both dental and medical care. Notably, about one-third of those who say they or a family member skipped or postponed care (14% of all adults) report a worsening condition as a result.
Figure 1: Four In Ten Say They Or A Family Member Have Skipped Or Postponed Medical Or Dental Care In The Past Six Months
People report different reasons for skipping or postponing care. Most commonly, 28% say they or a family member skipped or postponed care because the medical facility was closed or offering limited appointments, followed by 21% who say it was because they felt unsafe visiting a medical facility during the coronavirus outbreak. Amidst a coronavirus related economic recession and with unemployment currently at 8.4 percent, 17% of adults say they or a family member skipped or delayed care because they couldn’t afford it or were concerned about the cost. Previous KFF research indicates that this may be an underestimation of the true share of adults who are delaying care or relying on over-the-counter or home remedies to treat conditions instead of seeking care.
Fewer Say They Have Skipped Care Due To Coronavirus-related Closures or fears
While the coronavirus pandemic continues to have an impact on people seeking medical and dental care, survey trends indicate that as many medical facilities re-open with safety precautions in place, fewer people are now skipping care for coronavirus-related reasons compared to earlier this summer. The share of adults who say they or a family member skipped or postponed care due to office closures has decreased by 15 percentage points since June (28%, down from 43%). Similarly, the share who say they or a family member skipped or postponed medical or dental care because they felt unsafe seeking care during the coronavirus outbreak is also down from June (21%, down from 27%).
Figure 2: Fewer Adults Now Report Postponing Care Due To Coronavirus-Related Medical Office And Facility Closures, Safety Concerns
Groups that tend to go to the doctor more routinely are also the groups that have higher shares saying they put off care for coronavirus-related reasons. Women are more likely than men to put off care either because of office closures or because they felt unsafe going to an appointment during the pandemic, and the same is true for people living in households with chronic medical conditions and those with health insurance, compared to those without. On the other hand, younger adults, who typically go to the doctor less often, report lower levels of putting off care for coronavirus-related reasons.
Figure 3: Women, Insured Adults, Households With Chronic Condition More Likely To Report Skipped Care Due Office Closures, Feeling Unsafe
Cost Concerns Keep About One In Five Women, Younger Adults, from Getting Medical or Dental Care
While coronavirus-related medical office closures and fear about the safety of visiting medical office is contributing to number of people delaying getting care, cost also continues to be a factor, and affects a different segment of the population than those skipping care for coronavirus-related reasons. Overall, 17% of adults say the inability to afford the care or concern about the cost was a reason they skipped or postponed getting medical or dental care in the last six months. Notably, adults under age 65 and those with lower household incomes are more likely than their counterparts to say they or a family member have delayed getting care due to cost concerns. Women are more likely than men to say they or family member have skipped or postponed care due to cost.
Figure 4: Younger Adults, Women, And Those With Lower Incomes Are More Likely To Say They Or A Family Member Skipped Care Due To Cost
Though coronavirus and cost concerns are contributing to some delays in people getting the medical or dental care they need, most of those who say they or a family member skipped or postponed care say they expect to get the care within the next year. Indeed, 10% say they or a family member have already gotten the care that was postponed while nearly half (46%) say they expect to get the care within the next 3 months. Just 6% of those who said they or someone in their household delayed getting medical or dental care say they do not expect to get the care that was skipped or postponed.
Figure 5: Nearly Half Of Those Who Skipped Or Postponed Care Say They Expect To Get Needed Care In The Next Three Months
Methodology
This KFF Health Tracking Poll was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted August 28-September 3, 2020, among a nationally representative random digit dial telephone sample of 1,199 adults ages 18 and older, living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). The sample included 290 respondents reached by calling back respondents that had previously completed an interview on the KFF Tracking poll at least nine months ago. Computer-assisted telephone interviews conducted by landline (295) and cell phone (904, including 652 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. To efficiently obtain a sample of lower-income and non-White respondents, the sample also included an oversample of prepaid (pay-as-you-go) telephone numbers (25% of the cell phone sample consisted of prepaid numbers) as well as a subsample of respondents who had previously completed Spanish language interviews on the SSRS Omnibus poll (n=6). Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s March 2019 Supplement of the U.S. Census Population Survey (CPS) on sex, age, education, race, Hispanic origin, and region along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the January- June 2019 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of prepaid cell phones and likelihood of non-response for the re-contacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.