Usha Ranji
Usha Ranji  Karen Diep
Karen Diep  Ivette Gomez
Ivette Gomez  Laurie Sobel
Laurie Sobel  Alina Salganicoff
Alina Salganicoff Health care is a central element of women’s lives, shaping their ability to care for themselves and their families, to be productive members of their communities, to contribute to the workforce, and to build a base of economic security. Women’s reproductive health care needs, their central roles managing family health as parents and as family caregivers, and their longer lifespans, albeit with greater rates of chronic health problems and functional limitations than men, all shape their relationships with the health care system. While women are major consumers of health care services and play a central role as health navigators and caregivers for their families, structural factors can challenge their ability to get the health care they need. Factors, including national and state policies that shape the health care delivery system to research priorities and discriminatory economic and societal forces, can deprioritize women’s health concerns. Access challenges are greater for women who are in low-income households, who face structural and societal racism and discrimination, who struggle with complex or understudied medical conditions, or who live in states or communities that have enacted or invested in policies and programs that do not support their health needs.
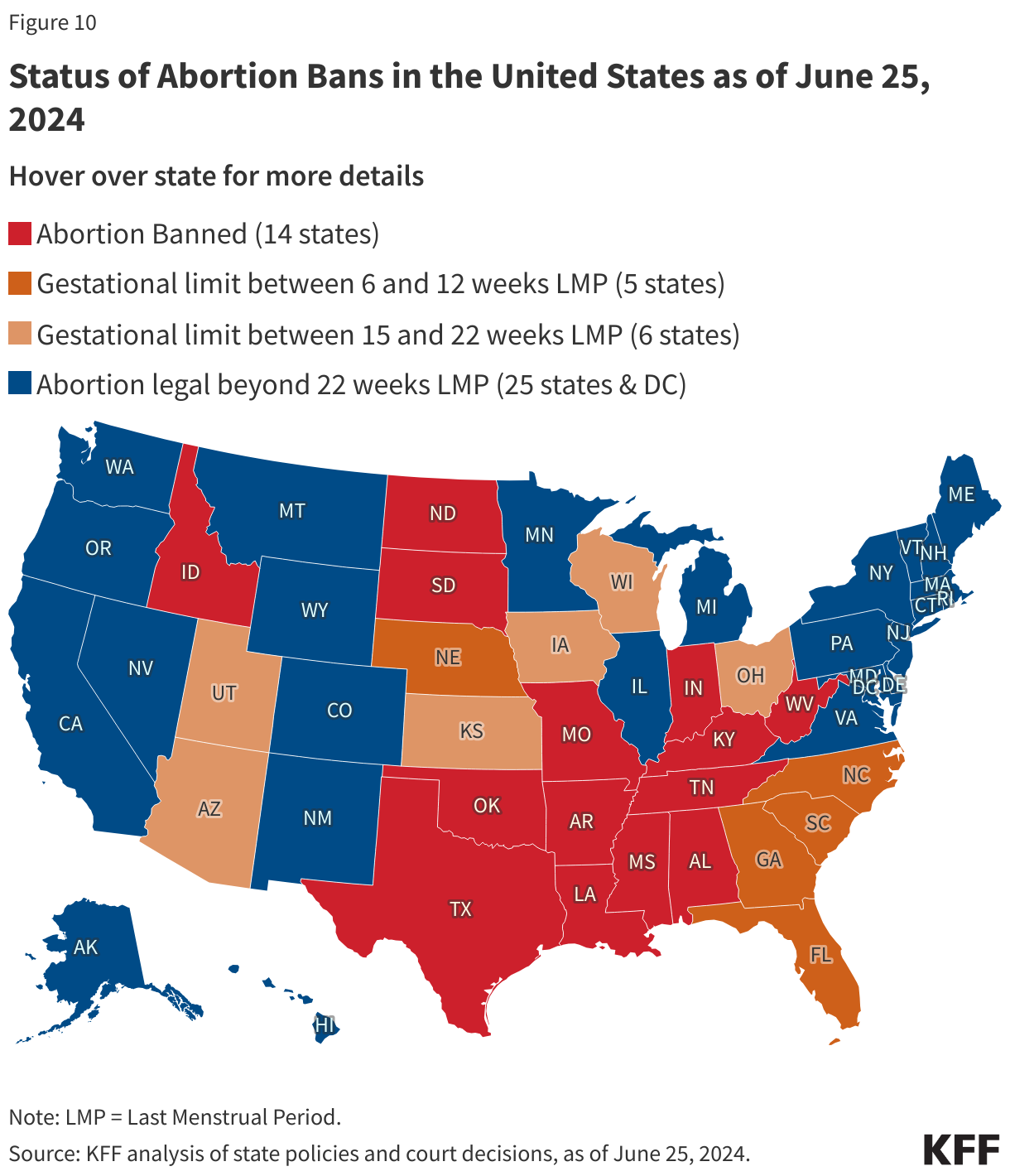
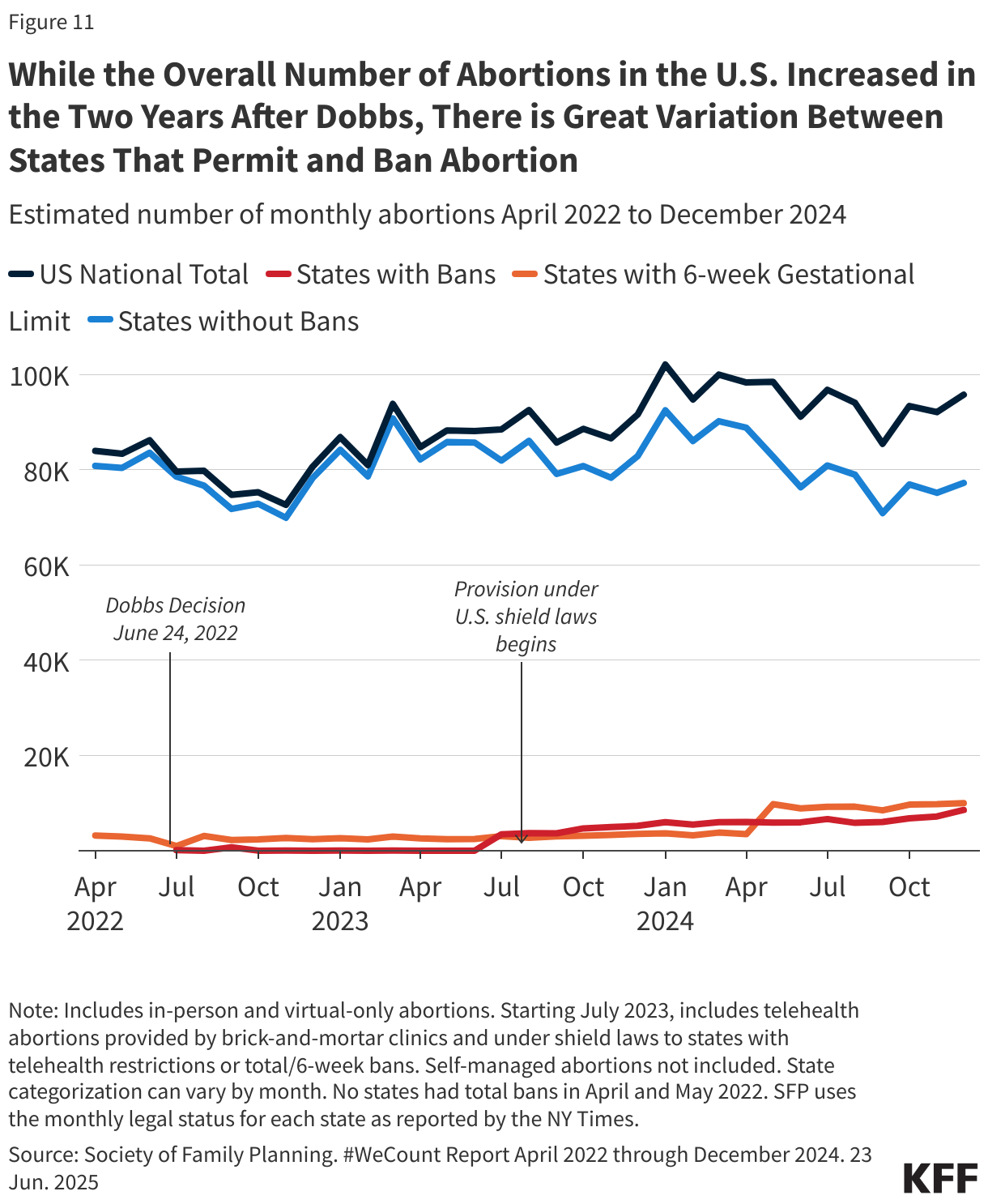
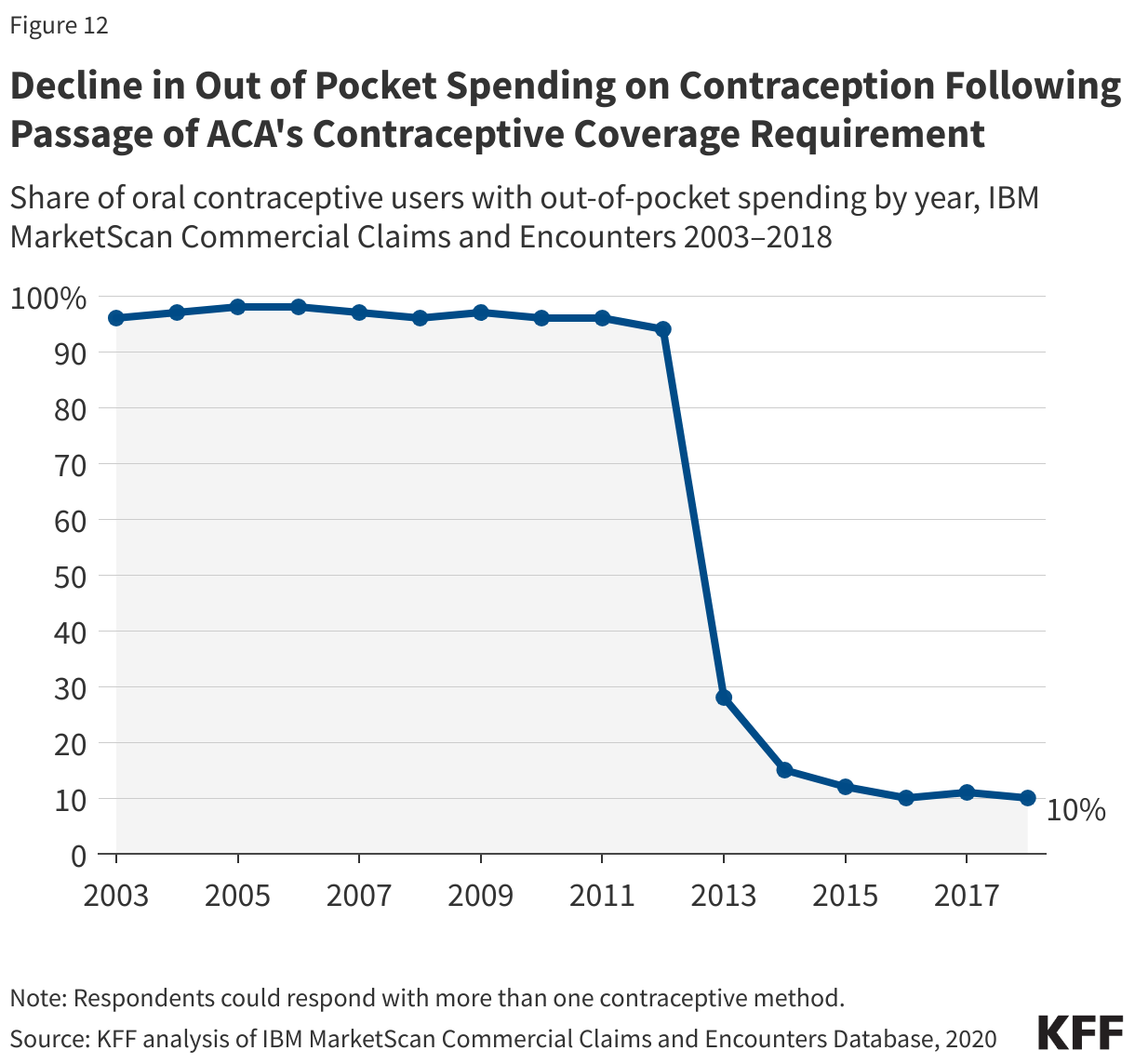
In the United States, the women’s health movement gained significant traction in the 1960s and 1970s as part of a larger grassroots women’s rights movement that challenged long-standing inequities and discrimination that limited women’s economic and social opportunities. The book, “Our Bodies, Ourselves,” brought a wide range of women’s health concerns, ranging from abortion and sexuality to menopause and cancer, into the mainstream. Over time, federal action also began to address many of the long-standing discriminatory sex and gender-based policies that were baked into our employment, health, and research policies. The 1973 U.S. Supreme Court ruling in Roe v. Wade decriminalized and protected the right to abortion care for nearly 50 years; the Pregnancy Discrimination Act of 1978 offered workplace and insurance protections to pregnant workers; the National Institutes of Health (NIH) Revitalization Act of 1993 mandated the inclusion of women in clinical research and formally established the NIH Office of Women’s Health; and in 2010, the Affordable Care Act (ACA) banned many of the discriminatory practices that had shaped women’s coverage of and access to care. While many of these policy changes have resulted in improvements and advances in women’s health, including access and coverage, the advances have not been linear. In 2022, the Supreme Court, with a conservative supermajority, struck down the right to abortion in Dobbs v Jackson Women’s Health, resulting in the outright banning of abortion in many states. Despite advances in women’s health research, many gaps remain and the Trump Administration has targeted and blocked federal funding that focuses on gender, a pillar of women’s health research.
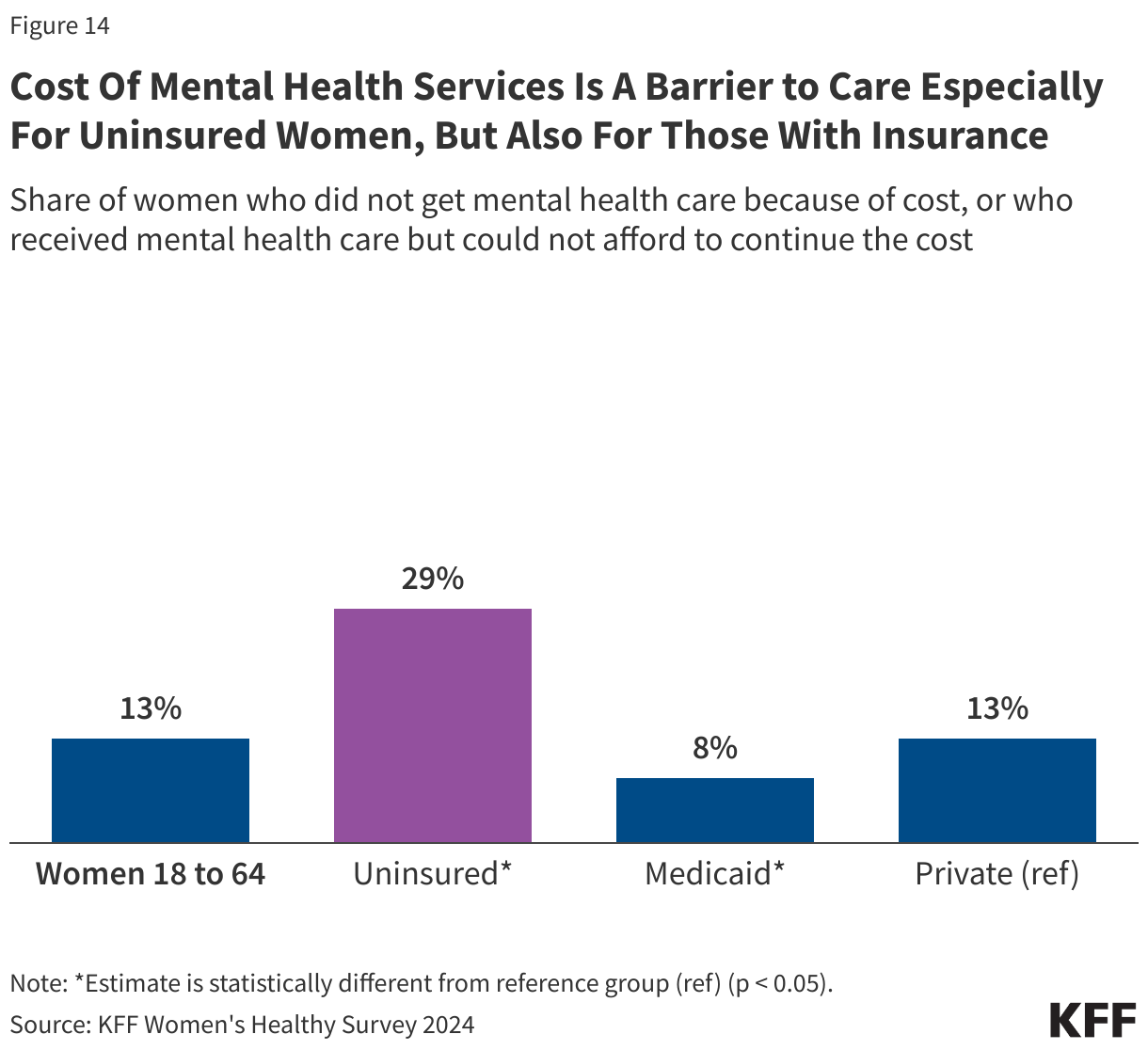
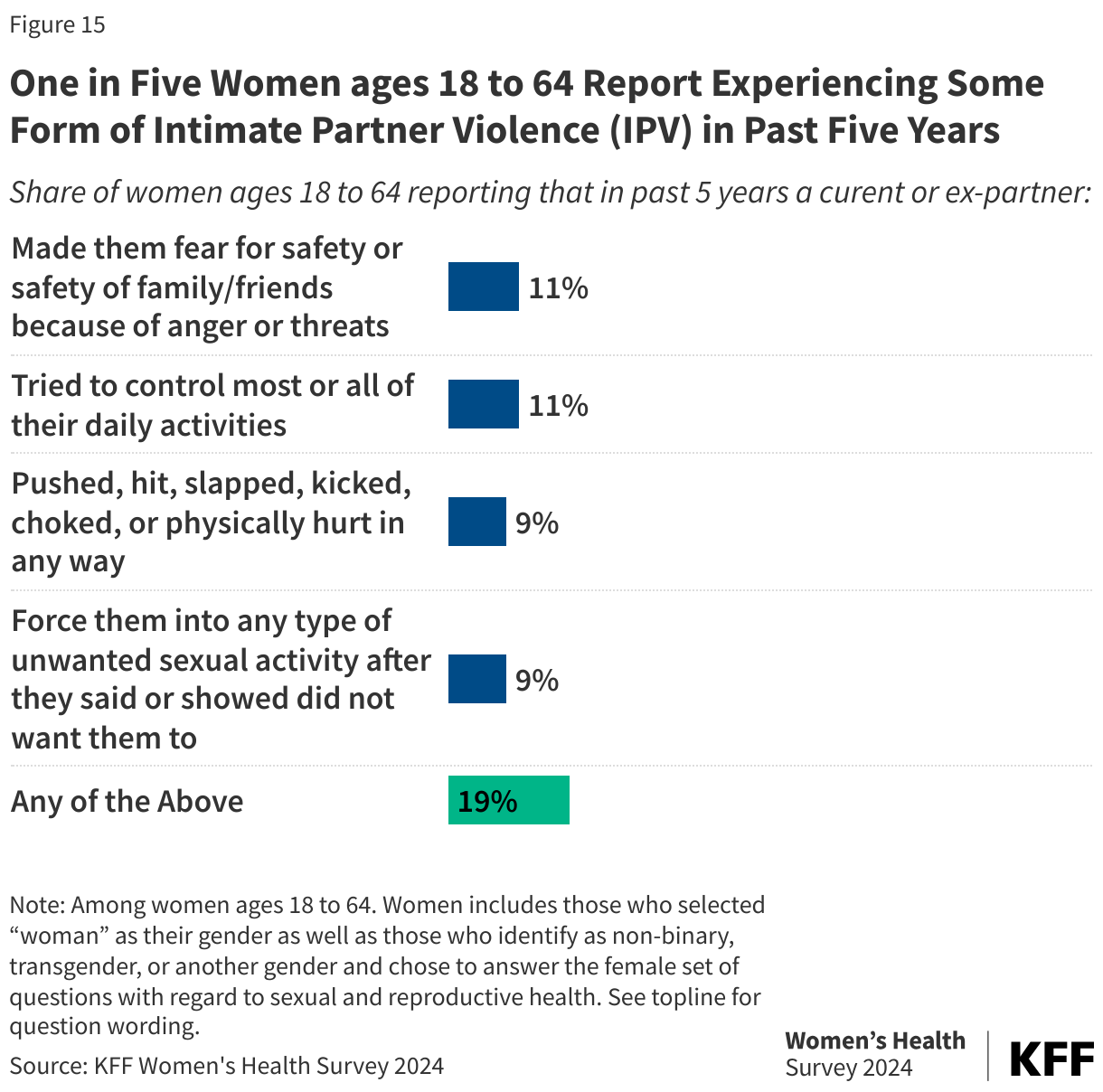
This primer focuses on some of the key areas disproportionately affecting women today that are shaped by national and state health policies. This includes health coverage and costs, reproductive health services, maternal health, mental health, and intimate partner violence. In addition, it highlights some of the structural factors and inequities that still impact women’s health, particularly women of color and gender-expansive individuals such as those who are transgender or non-binary or otherwise gender fluid or non-conforming who are at risk of being marginalized or discriminated against by their health coverage or providers. We note that while we refer to “women” and “women’s health” throughout this chapter, some persons assigned female sex at birth do not identify as women, such as transgender men, non-binary individuals, and otherwise gender-expansive individuals. Still, many of the issues discussed in this chapter also apply to them.