Who Uses Telecontraception and Why? A Closer Look at Clients of Four Telecontraception Companies
Key Takeaways
- Based on the findings of a non-probability sample of 6,000 survey respondents from four telecontraception companies, the leading reason respondents cite for getting their most recent birth control via telecontraception is that it is delivered to their home (26%). Others cite privacy, difficulties getting appointments, and prior negative interactions with in-person care. Nearly one in five (18%) of respondents cited the COVID-19 pandemic as the reason they first accessed birth control online.
- The vast majority of respondents using telecontraception are women and two-thirds are 35 and younger, including larger shares who don’t have health insurance or who are LGBT+ compared to a nationally representative sample of contraceptive users in U.S. population.
- The most frequently received contraceptive method reported by telecontraception respondents is oral contraceptives (91%), followed by emergency contraceptive pills (9%). Nearly three in ten (29%) respondents overall say they purchased emergency contraception through an online company in the last 12 months.
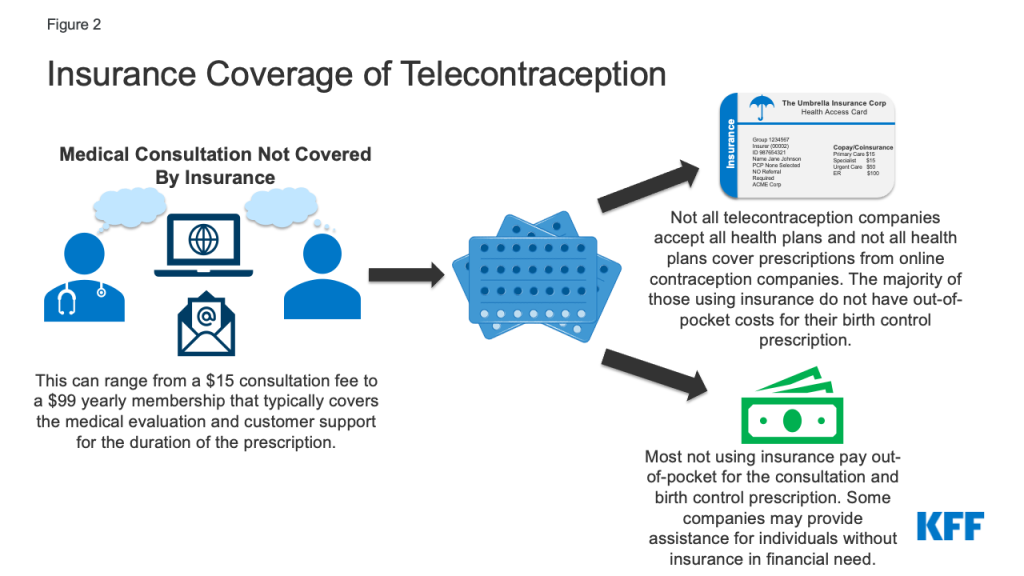
- About three in four respondents with private insurance or Medicaid who tried to use their insurance for telecontraception paid nothing out-of-pocket for their birth control method. Half (51%) of those who did not use insurance paid between $31 and $50 and about a quarter (24%) paid over $50 for their birth control. The companies do charge a consultation or membership fee for all of their users and this cost is not covered by insurance.
- Four in ten (43%) respondents say they do not have a regular doctor and one in five (20%) have never had an in-person birth control visit.
- Almost a quarter (24%) of respondents report they have gotten emergency contraception to have on hand and over a fifth (22%) have considered sterilization in response to the Supreme Court’s decision to overturn Roe v Wade. These findings were fairly consistent across states regardless of whether abortion was banned or not.
Introduction
In recent years there has been increased interest in making contraception more accessible, particularly outside of traditional clinical settings. These efforts have gained urgency in wake of the Supreme Court decision in Dobbs v Jackson Women’s Health, which overturned Roe v. Wade, and the COVID-19 pandemic. However, even prior to both of these events, online companies had started to offer consumers the option of having contraceptives delivered to their home without needing to go for an in-person healthcare visit. While only a small share of people say they have used these online platforms, companies have reported a rapid growth in clients during the COVID-19 pandemic and an increase in emergency contraception orders since the Dobbs decision. There has been very little research to date on who uses telecontraception and why they choose to get their birth control online aside from a recent study focused on one online platform. In order to learn more about who is using telecontraception in the Fall of 2022, KFF conducted a survey of current clients from four telecontraception companies. The responses from individuals who responded to the survey across the four companies have been combined to give a snapshot of who is using telecontraception.
Methods
The KFF Survey of Online Contraception Clients was designed and analyzed by researchers at KFF. The survey was conducted via SurveyMonkey using a unique survey link that was sent to four telecontraception companies who then sent the link to their active contraceptive clients over the age of 18 who had received contraception from their company in the past year (272,800 clients). The survey was fielded from October 13 to December 8, 2022. A total of 5,925 telecontraception clients participated in the survey. Clients had an opportunity to be entered into a drawing for twelve $100 Amazon gift cards (three for each company) by submitting their email after completing the survey.
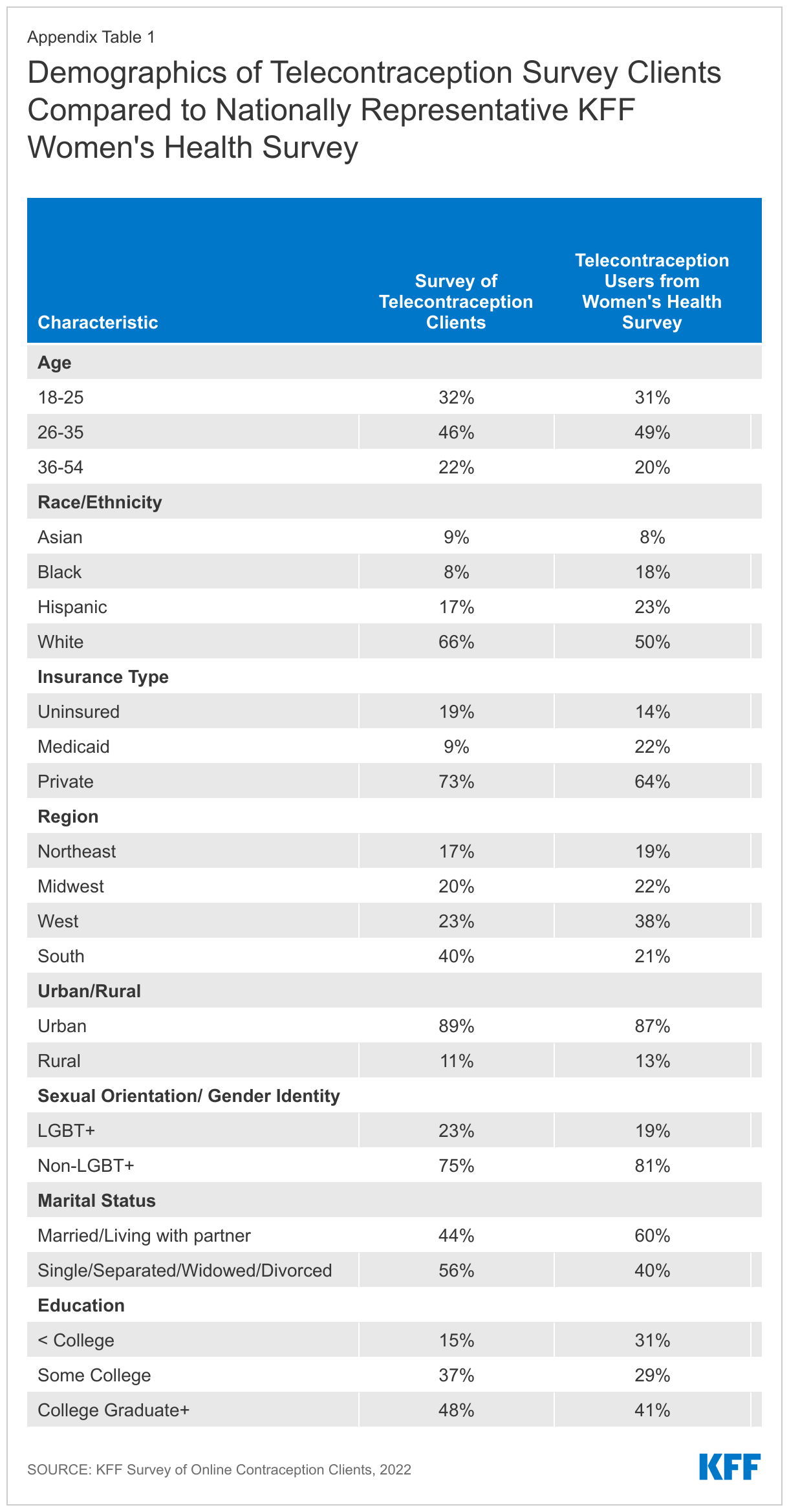
This survey is a non-probability sample based on telecontraception clients that responded to the survey from the four companies. There were not large differences in demographics and survey responses across the four companies surveyed, so the data for survey respondents from all four companies were combined to give an overall picture of telecontraception clients. These data were collected using a non-probability sampling frame, and the results are not necessarily representative of the broader population that receives online contraception. However, the overall demographics of telecontraception clients from this sample closely matched a similar sample of women who said they have received a prescription or obtained a health care service from an online company in the prior 12 months obtained from KFF’s 2022 Women’s Health Survey, a nationally representative sample of women (See Appendix Table 1). Therefore, no additional adjustments, such as weighting, were made to the sample.
Demographics of Telecontraception Survey Respondents
This report presents a snapshot of telecontraception clients of four companies who responded to the KFF survey. The vast majority (97%) of responding telecontraception clients identify as women, while 2% are non-binary, 1% prefer not to say, and less than 1% identify as men, transgender or another gender. The four companies surveyed for this project do not offer male condoms, which explains why there are so few male clients in the sample.
Telecontraception clients responding to this survey ranged in age from 18-54. The largest share of those using telecontraception are between the ages of 26-35 (46%), about a third are ages 18-25 (32%), and over one in five are ages 36-54 (22%). Compared to females using short acting reversible contraception (such as the pill, injectables, patches or condoms, (SARC)) from the nationally representative KFF Women’s Health Survey, larger shares of telecontraception respondents fell in the 26-35 age range (46% vs. 35%) and smaller shares fell in the 36-54 age range (22% vs. 35%).
The majority of telecontraception survey respondents are White (66%), 17% are Hispanic, less than one in ten are Asian (9%), Black (8%), and American Indian/Alaska Native (1%). Larger shares of telecontraception respondents were White compared to those using SARC nationally (66% vs. 55%). Nearly two-thirds (65%) of telecontraception survey respondents earn more than $25,000 a year, while over one in four (27%) earn less than $25,000 a year, and another 9% prefer not to say (Figure 1).
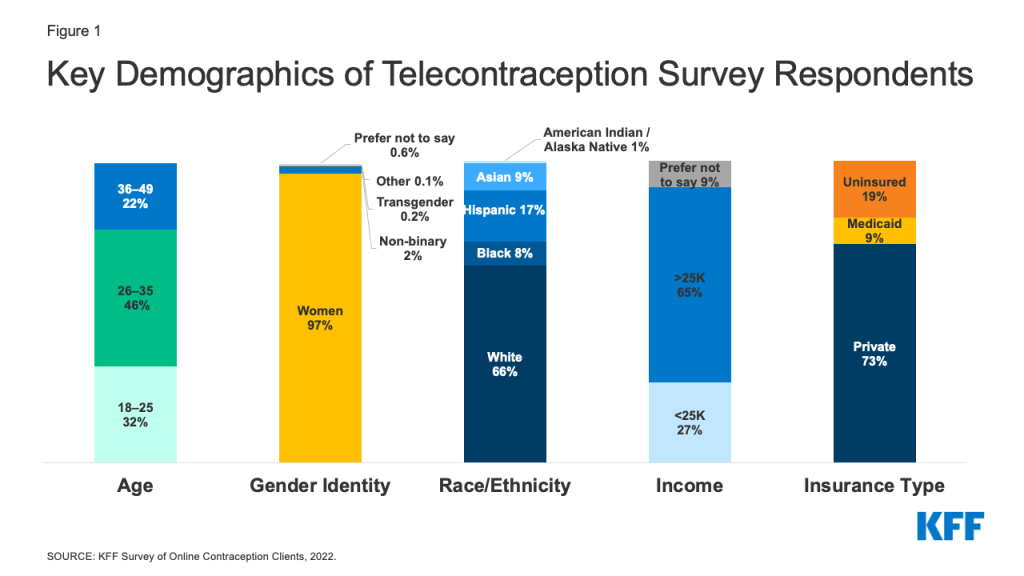
Seven in ten respondents have private insurance (73%), about one in ten (9%) have Medicaid coverage, and almost one in five (19%) are uninsured. Compared to our nationally representative sample of SARC users, the share of those in the survey who have Medicaid coverage is smaller (9% vs. 20% nationally) and those who are without insurance is larger (19% in this survey vs. 9% nationally).
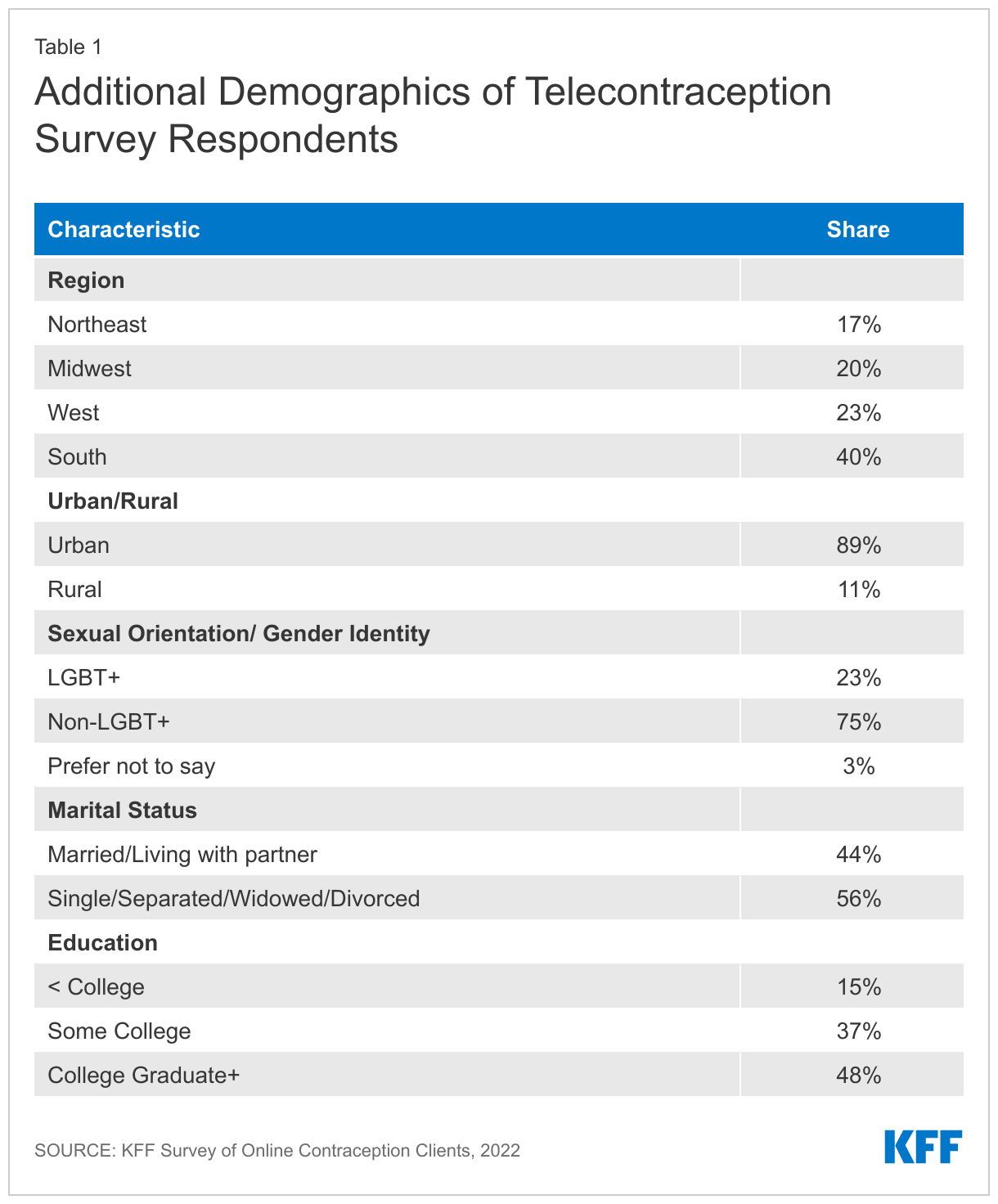
The largest share of respondents live in the South (40%), nearly a quarter are in the West (23%), one in five reside in the Midwest (20%), and 17% live in the Northeast United States, which is very similar to SARC users in our nationally representative sample (Appendix Table 1).
Nearly a quarter (23%) of respondents are LGBT+, three-quarters are non-LGBT+ (75%), and 3% prefer not to say. The share of respondents who are LGBT+ is slightly higher than the share of females who use SARC and identify as LGBT+ (23% vs. 17%).
Finally, a larger share of respondents are single, separated, widowed, or divorced compared to married or living with a partner (56% vs. 44%) and eight in ten have some college education compared to 15% with less than a college education (85% vs. 15%) (Table 1). Smaller shares of SARC users nationally are single, separated, widowed or divorced (42% vs. 56%) and larger shares of telecontraception respondents have some college education compared to SARC users nationally (85% vs. 75%).
Experiences with Telecontraception
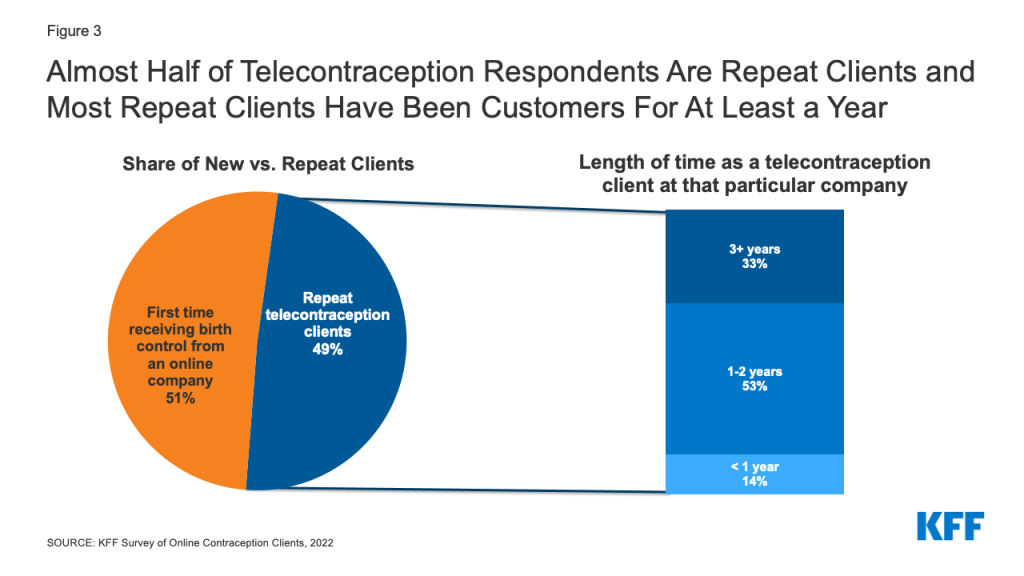
While telecontraception may be a new avenue for accessing contraception for many, nearly half (49%) of all telecontraception clients who responded to the survey say this is not the first time they have received their birth control from an online contraception company. Among those who have received birth control multiple times from an online contraception provider, the majority (86%) have been clients at the company for which they completed the survey for at least a year (Figure 3). The length of time people had been clients varied by company, with the majority of respondents at two of the companies saying they had been clients for at least a year (Company A = 85% and Company B = 95%), while about half of respondents at the other two companies say they have been clients for at least a year (Company C = 45% and Company D = 51%). All of the participating companies have been in business for a number of years.
One in five (20%) respondents say they have received birth control from at least one additional telecontraception company. This also differed by company, with Company A and Company B having smaller shares of respondents who have received birth control from a different online company (18% and 14%, respectively) compared to respondents at Company C and Company D (54% and 65%, respectively).
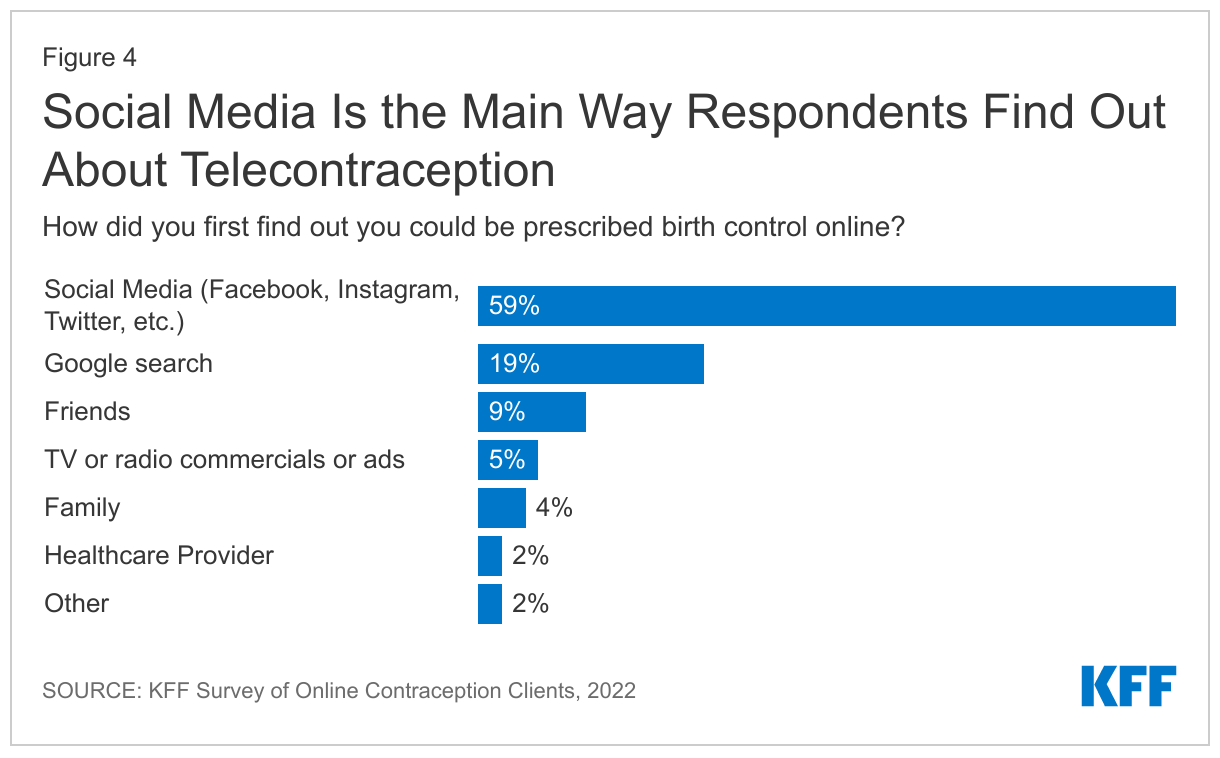
Many telecontraception companies utilize paid search engine marketing and social media to advertise and the majority of respondents say they first found out they could be prescribed birth control online through social media (59%), followed by Google search (19%), friends (9%), family (4%), and a healthcare provider (2%) (Figure 4).
Reasons for Accessing Birth Control Online
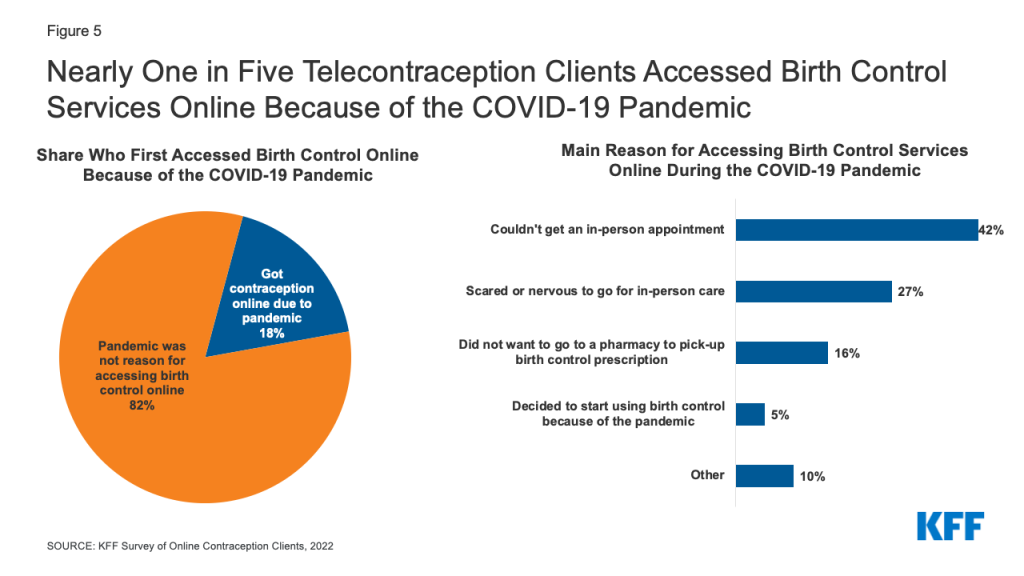
Although, telecontraception companies have reported they have seen a proliferation of clients due to the COVID-19 pandemic, most (82%) respondents say the pandemic was not the reason they accessed birth control online. Only one in five (18%) respondents say they first accessed birth control online because of the COVID-19 pandemic. Among those who first accessed birth control online because of the COVID-19 pandemic, the most widely cited reason was they could not get an in-person appointment (42%), followed by just over a quarter (27%) who were scared or nervous to go for in-person care, and 16% did not want to go to a pharmacy to pick-up their birth control prescription. A small share (5%) say they decided to start using birth control because of the pandemic and another one in ten cited another reason (Figure 5).
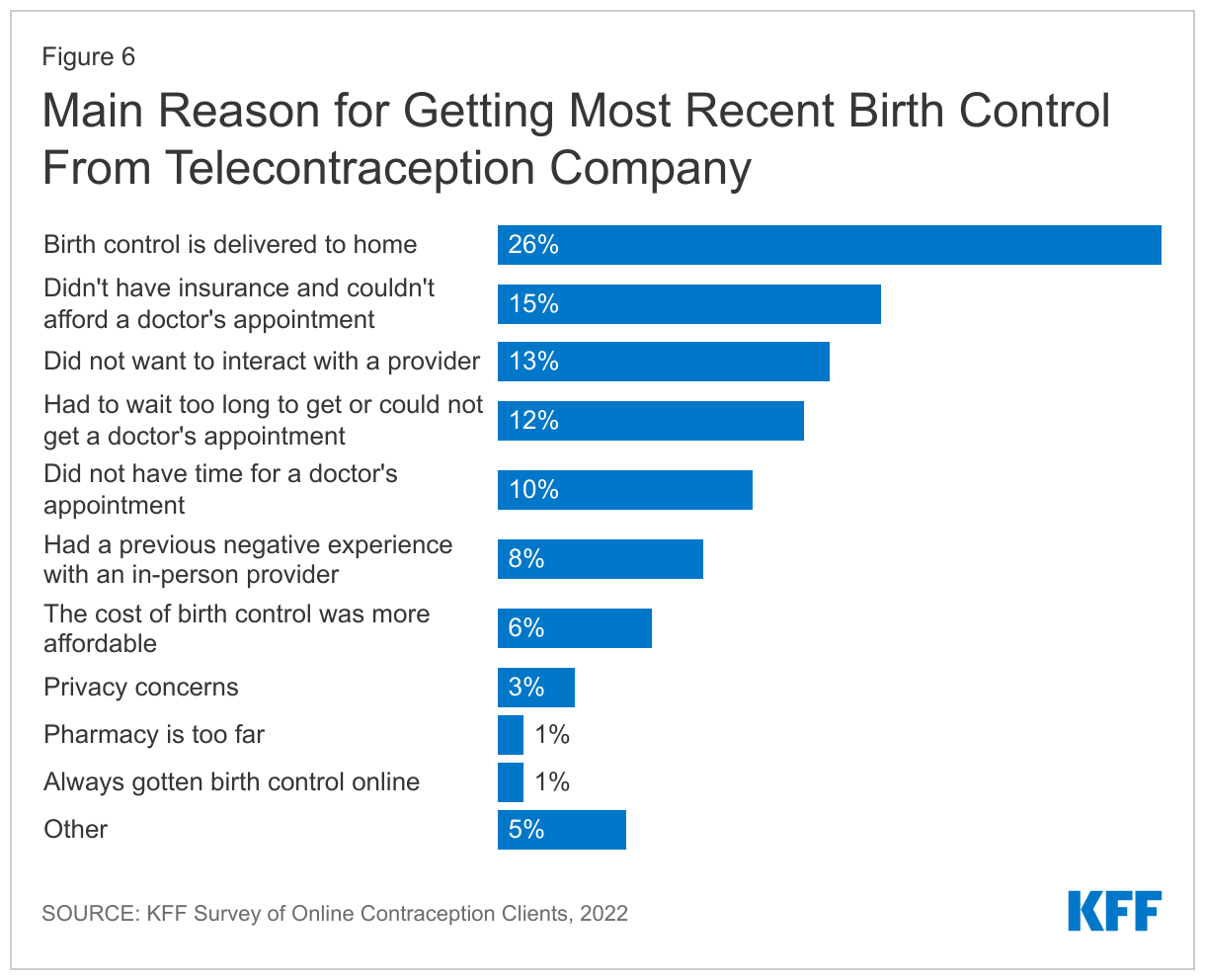
Among all respondents, the most frequent reason people cite for getting their most recent birth control via telecontraception is that the birth control is delivered to their home (26%). The second most frequent reason they say is they didn’t have insurance and couldn’t afford a doctor’s appointment (15%). Other reasons include not being able to get a doctor’s appointment (12%) or not having time for a doctor’s appointment (10%), as well as not wanting to interact with a provider (13%) or having a previous negative experience with an in-person provider (8%). Larger shares of LGBT+ individuals compared to non-LGBT+ cite a previous negative experience with an in-person provider as their main reason for getting their most recent birth control prescription via telecontraception (11% vs. 7%).
Among all respondents, smaller shares say the cost of birth control was more affordable (6%), they had privacy concerns (3%), a pharmacy is too far (1%), or they have always gotten birth control online (1%), and 5% cite some other reason (Figure 6).
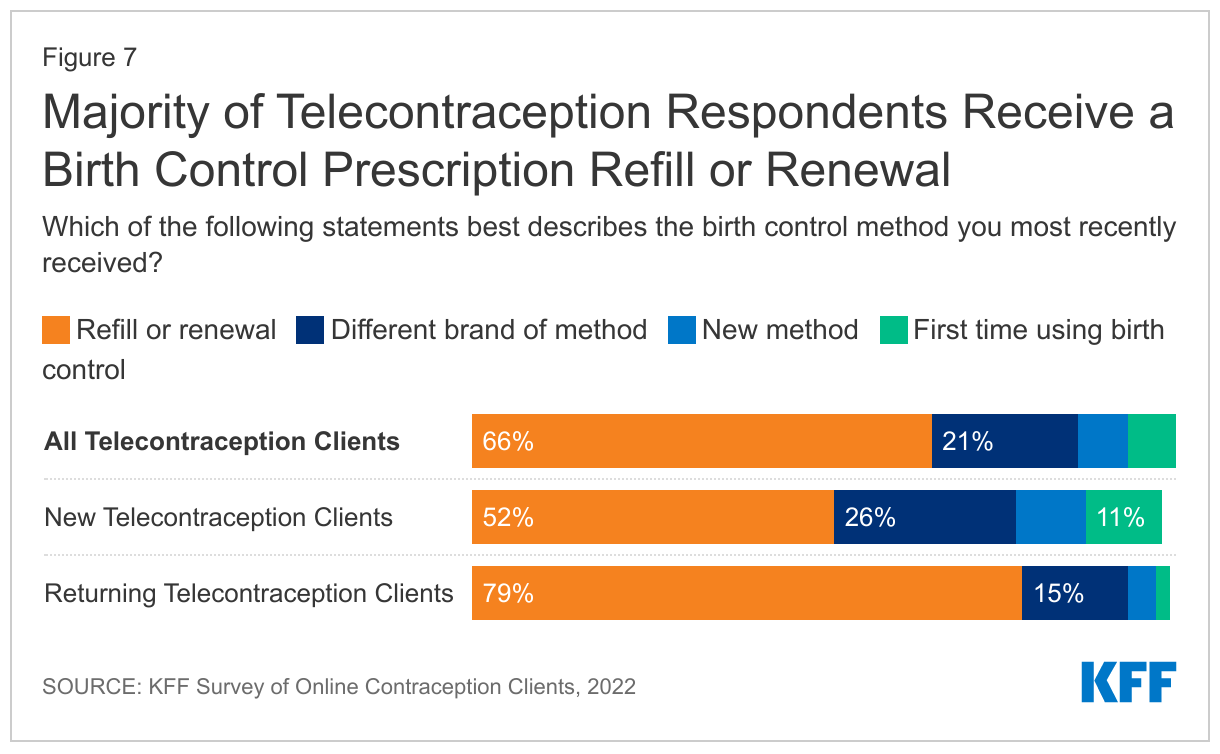
Individuals accessing telecontraception can get new prescriptions for contraception via a telehealth visit (typically asynchronous) with an online provider or refill an existing prescription. The majority of respondents (66%) say they most recently refilled or renewed a birth control prescription they were already using. Just over one in five (21%) say they obtained a different brand of their previous birth control method, like an oral contraceptive brand, or possibly a generic. Only 7% of respondents say they received a new birth control method and another 7% say the prescription they most recently received was their first time ever using birth control.
Compared to respondents who had previously received birth control online, smaller shares of respondents receiving birth control for the first time from a telecontraception company say their most recent birth control method was a refill or renewal (52% vs. 79%). Larger shares of new telecontraception clients compared to returning clients say they got a different brand of their previous method (26% vs. 15%) or got a new birth control method (10% vs. 4%). Just over one in ten (11%) new telecontraception clients say this was their first time ever using birth control (Figure 7).
Contraceptive Methods Prescribed
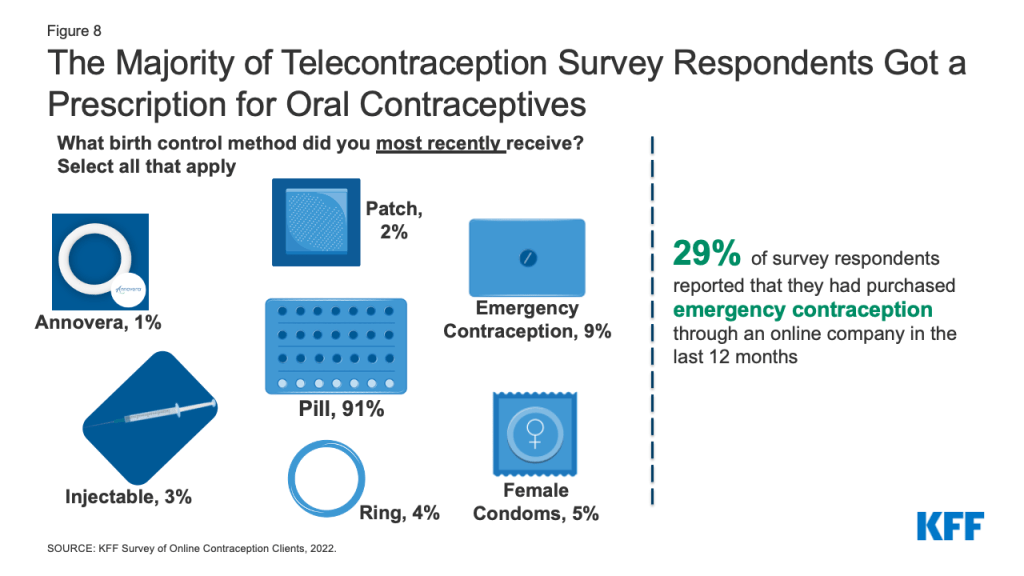
Among respondents, the most frequently obtained contraceptive method is oral contraceptives (91%), followed by emergency contraceptive pills (9%) (Figure 8). Five percent of respondents received female condoms, 4% monthly contraceptive rings, 3% injectable contraception, 2% contraceptive patch, and 1% received the one-year ring, Annovera. One in ten (10%) respondents most recently obtained more than one contraceptive method and 95% of those who got more than one contraceptive method received emergency contraception and almost one third (31%) got female condoms. Female condoms and emergency contraception are often included as add-ons at the end of an order. Nearly three in ten (29%) respondents overall say they purchased emergency contraception through an online company in the last 12 months.
Cost and Coverage
Since 2012, the ACA’s contraceptive coverage requirement has required all new private plans to cover FDA-approved contraceptive methods for women without cost-sharing from a participating provider. For individuals with Medicaid coverage, family planning services have been a mandatory benefit category that all state programs must cover without any cost-sharing, but services must be obtained from a Medicaid-participating provider. One of the companies that participated in this survey does not accept Medicaid and the other three do, but do not accept Medicaid in all states.
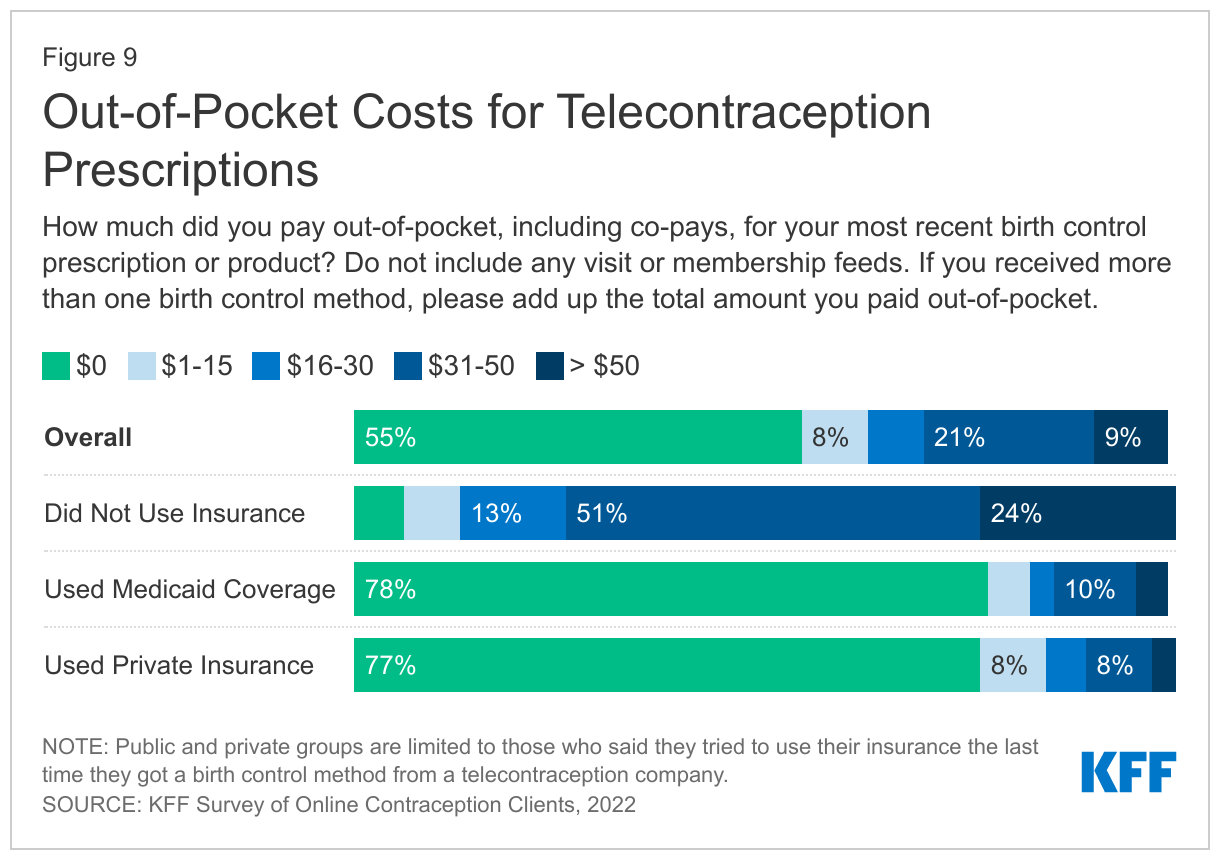
When asked how much they had to pay out-of-pocket, including co-pays, for their most recent birth control prescription or product, the majority of respondents say they did not have to pay anything (55%). For those with some out-of-pocket costs, just over one in five (21%) paid $31-50, 9% paid more than $50, 8% paid $1-15, and 7% paid $16-30 (Figure 9). However, this varied significantly among those with some type of health insurance coverage and those without insurance (See Insurance Coverage of Telecontraception above). About three in four individuals with private insurance or Medicaid who tried to use their coverage paid nothing out-of-pocket for their birth control compared to only 6% of individuals without insurance who had no out-of-pocket costs. Some companies provide free birth control for women without insurance who are in financial need. The largest share of those without insurance (51%) paid $31-50 and about a quarter (24%) paid over $50 for their birth control prescription or product. Individuals without insurance could get free or low-cost birth control from a federally funded Title X clinic or federally qualified health center, however, they may choose to pay for telecontraception for other reasons like convenience.
Despite the requirement that most private insurance plans cover contraceptive services and supplies free of cost-sharing, there may be multiple reasons individuals with private insurance may have out-of-pocket costs. The telecontraception company may not have had a contract with their insurance plan, the telecontraception company could have been considered out of network, or the client might be enrolled in a plan that is exempt from the contraceptive coverage requirements, such as those that are grandfathered, or those with coverage through an employer that is exempt on religious grounds.
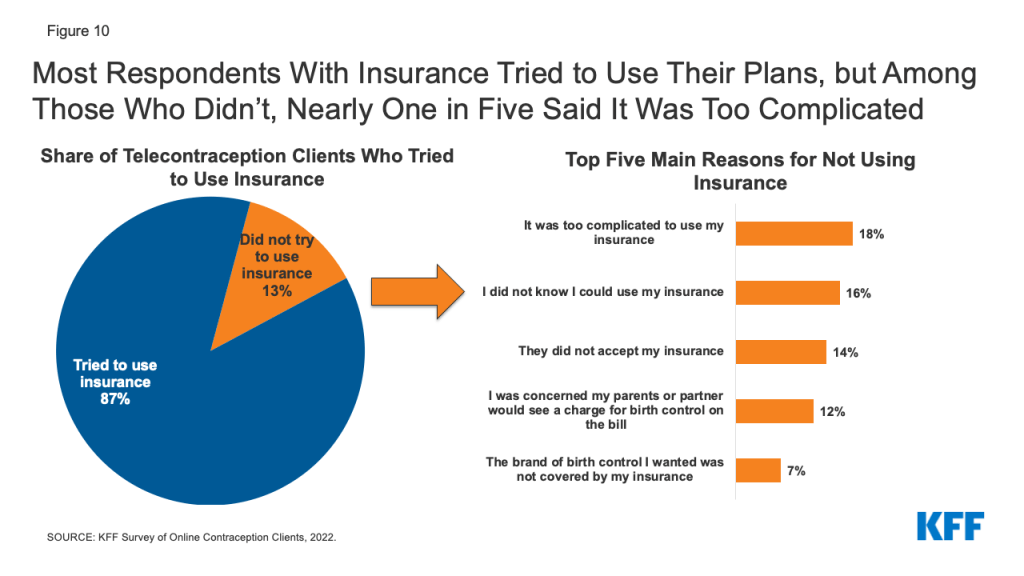
When asked about the last time they got a birth control method from a telecontraception company, the majority (87%) of insured respondents tried to use their insurance, while 13% did not (Figure 10). The top reason for not trying to use insurance was it was too complicated (18%). Another 16% of those who did not try to use their insurance say they did not know they could use their coverage. One in seven (14%) say the telecontraception company did not accept their insurance, while 12% did not try to use their insurance because they were concerned their parents or partner would see a charge for birth control. Seven percent say the brand of birth control they wanted was not covered by their insurance. Other reasons specified for not trying to use insurance included: the price was affordable without insurance, they hadn’t had a chance to update their insurance information, and they didn’t want their insurer to know about their birth control use.
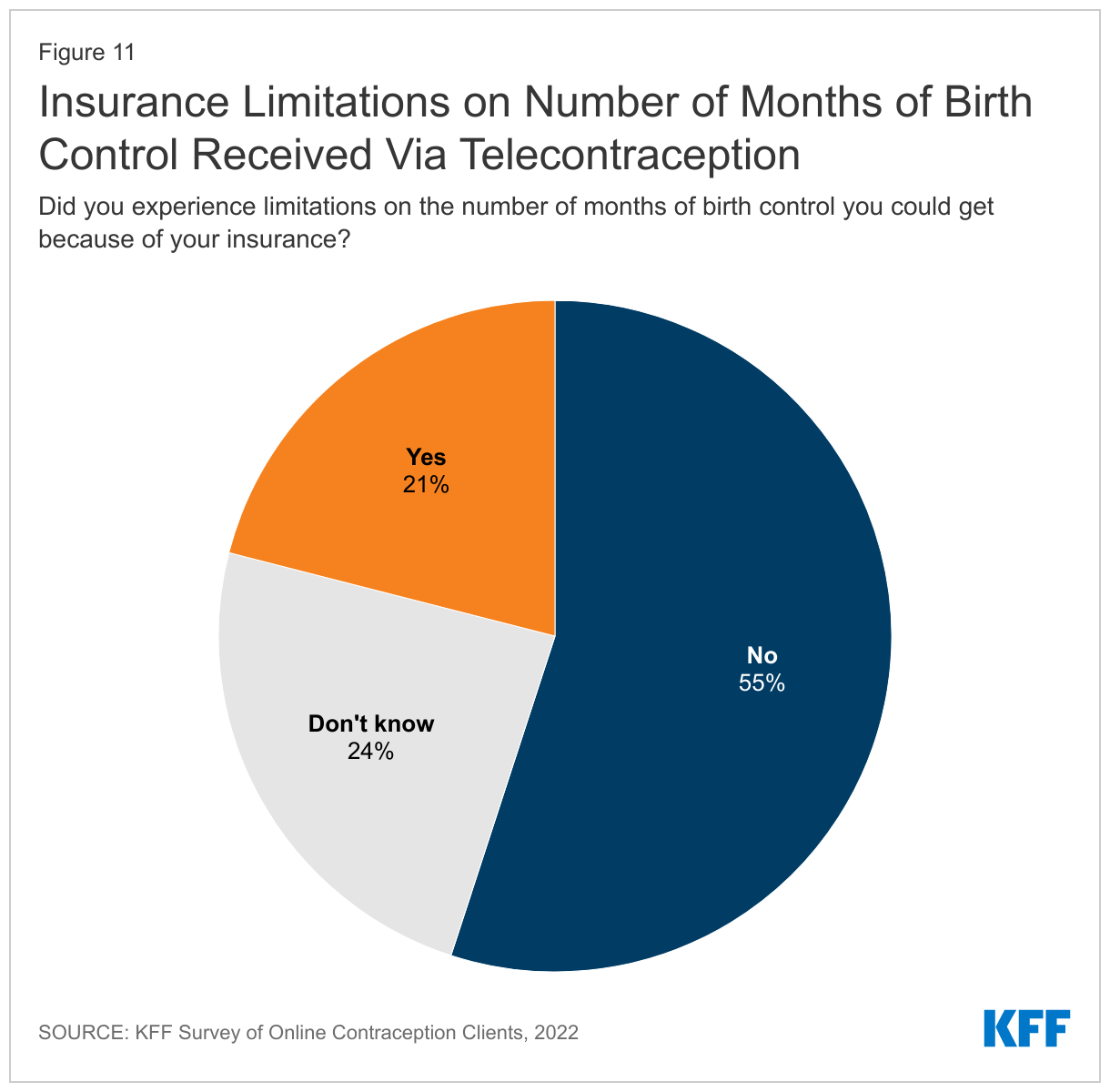
For individuals who tried to use their insurance for their telecontraception prescription, one in five (21%) say their insurance imposed limitations on the number of months of birth control they could get, while the majority (55%) did not experience limitations (Figure 11). About a quarter of respondents who tried to use their insurance did not know if they experienced limitations on the number of months of birth control they could get. The share reporting that they experiencing limitation did not differ between those with private insurance or Medicaid (data not shown).
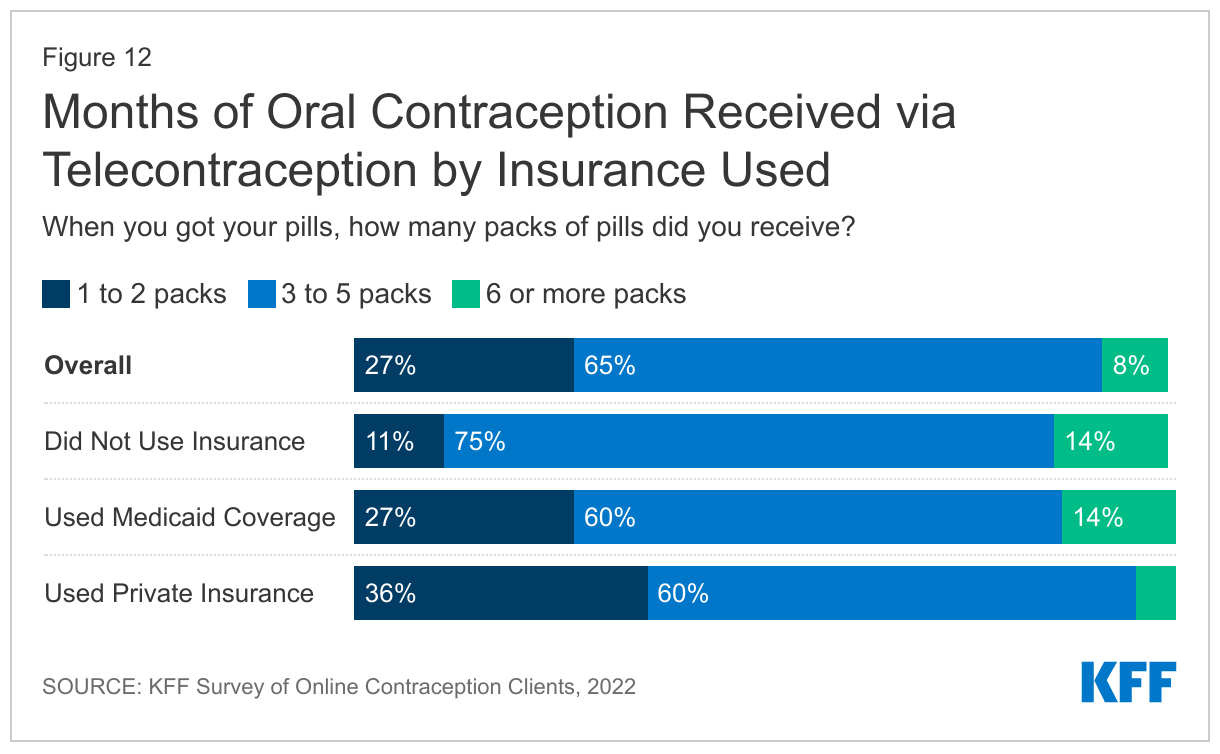
The largest share of respondents (65%) prescribed oral contraceptives say they receive three to five packs of pills at a time. While research has shown that best practice is to offer oral contraceptive users an extended supply of oral contraceptive pills such as a 12 month supply, few women receive a 12-month supply of contraceptives. Eight percent of respondents say they get 6 or more packs at a time, while 27% receive one to two packs at a time.
However, there are significant differences between those without insurance and those with Medicaid coverage compared to private insurance. Larger shares of respondents who used their Medicaid coverage (14%) or those that did not use insurance (13%) received six or more packs of pills compared to just 5% of those using private insurance (Figure 12). Currently, Medicaid programs in sixteen states and DC cover a 12-month supply of oral contraceptives at a time, which likely explains the larger share of individuals with Medicaid coverage receiving a 12-month supply. Some of the telecontraception companies also offer contraception at a discounted price if a larger number of packs at purchased at one time, which may be why a larger share of individuals without insurance received 6 or more packs. Twenty states and DC require state regulated insurers to cover an extended supply of contraceptives at one time, but this policy doesn’t include all plans (such as those that are self-funded) and there are still issues with implementation in getting insurance to cover more than 1 to 3 months of contraception at a time due to health plans’ concern over waste and increased costs.
Experiences Using Telecontraception
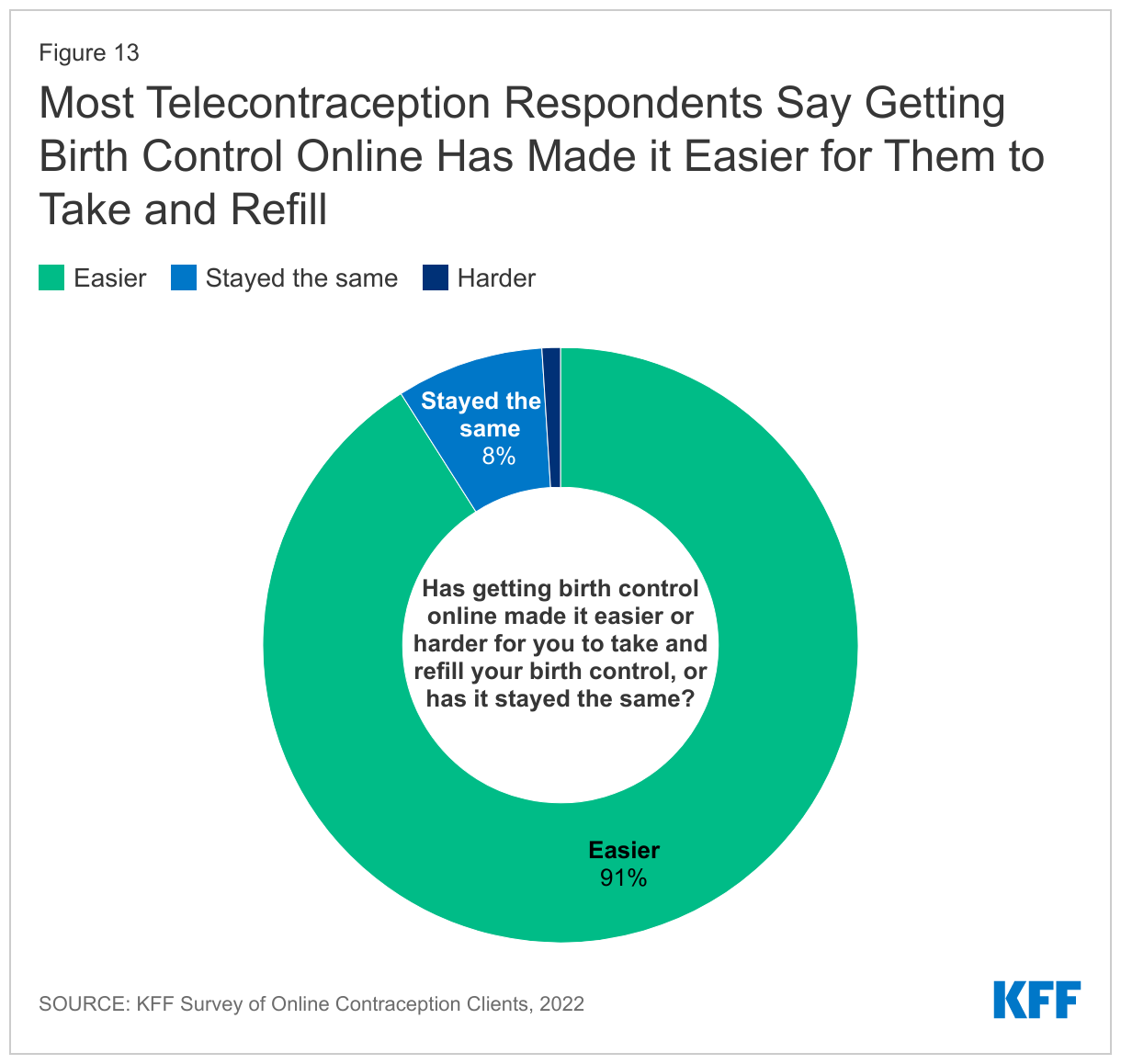
The telecontraception clients responding to this survey were largely satisfied with the services they received and felt that telecontraception made it easier for them to take and refill their birth control. Ninety-one percent of survey respondents report that getting their contraception through an online company has made it easier for them to take or get refills for their birth control, while only 1% report it has made it harder. Eight percent say there has been no change (Figure 13). Individuals that are able to continuously take and refill their birth control with little to no barriers are less likely to have an unwanted pregnancy.
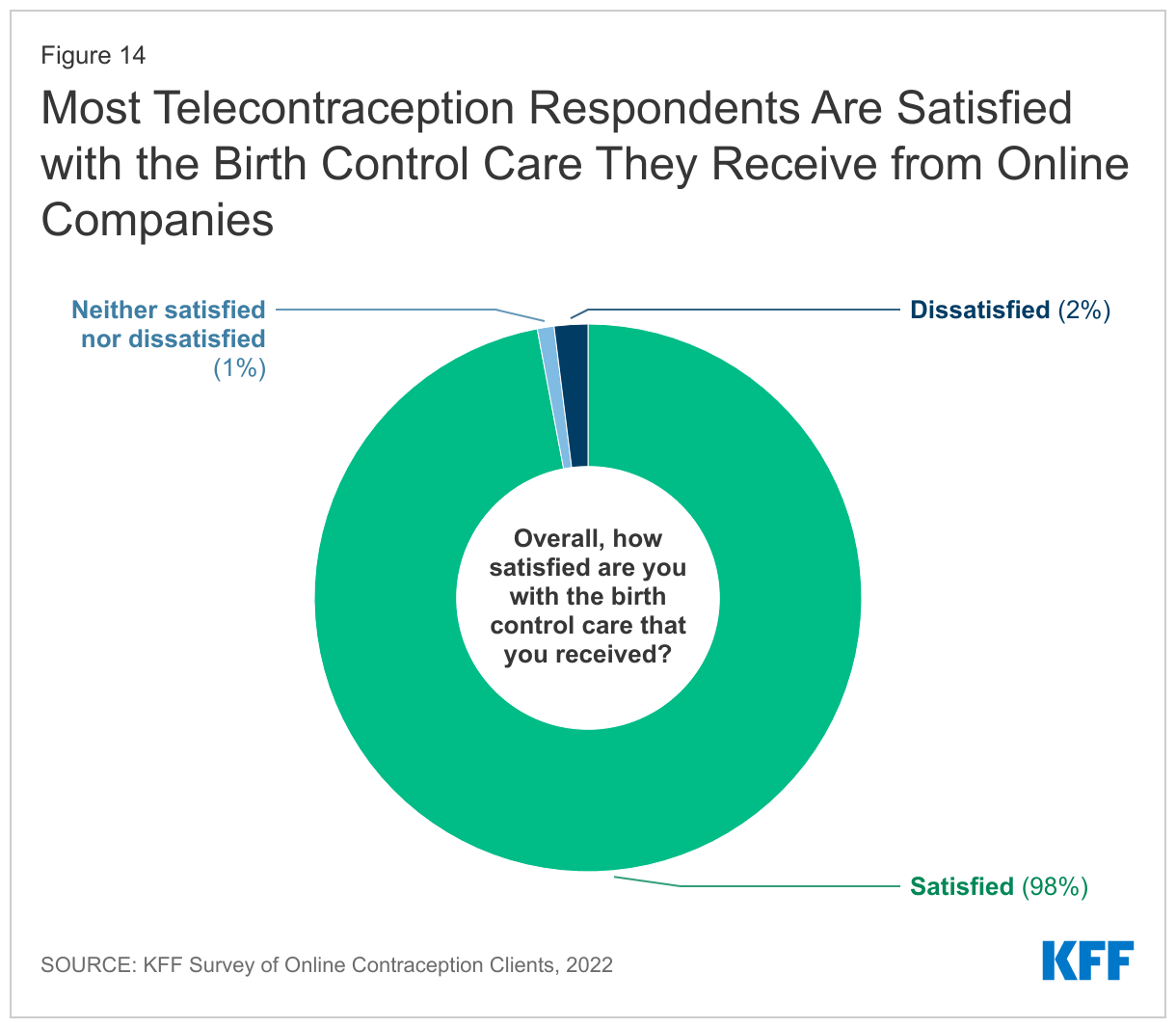
The majority (98%) of respondents report they are satisfied with the birth control care they received from the telecontraception companies (Figure 14). Across the four companies, between 93% to 98% say they were satisfied with their care. Two percent of respondents report they are dissatisfied with the care they received, and 1% report they are neither satisfied nor dissatisfied.
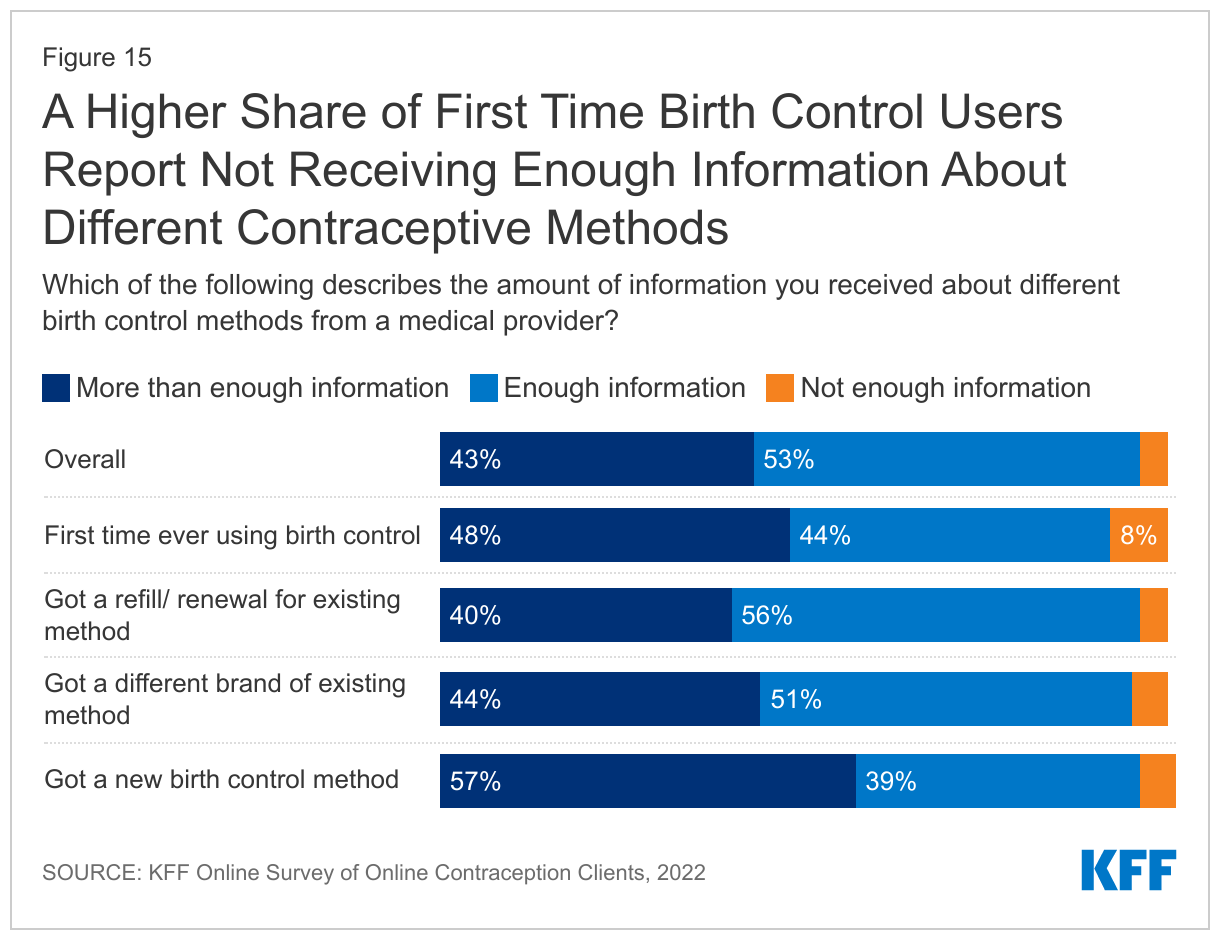
Most respondents say they received enough information about different birth control methods from a medical provider at the company of their choice. Half (53%) report they got enough information, and another 43% report they received more than enough information. Only 4% report they did not get enough information—across companies, this share ranged from 4% to 11%. However, a higher share of respondents who were using a birth control method for the first time report they did not get enough information (8%) compared to those getting a different brand (5%), a new method (5%), or a refill (4%) (Figure 15).
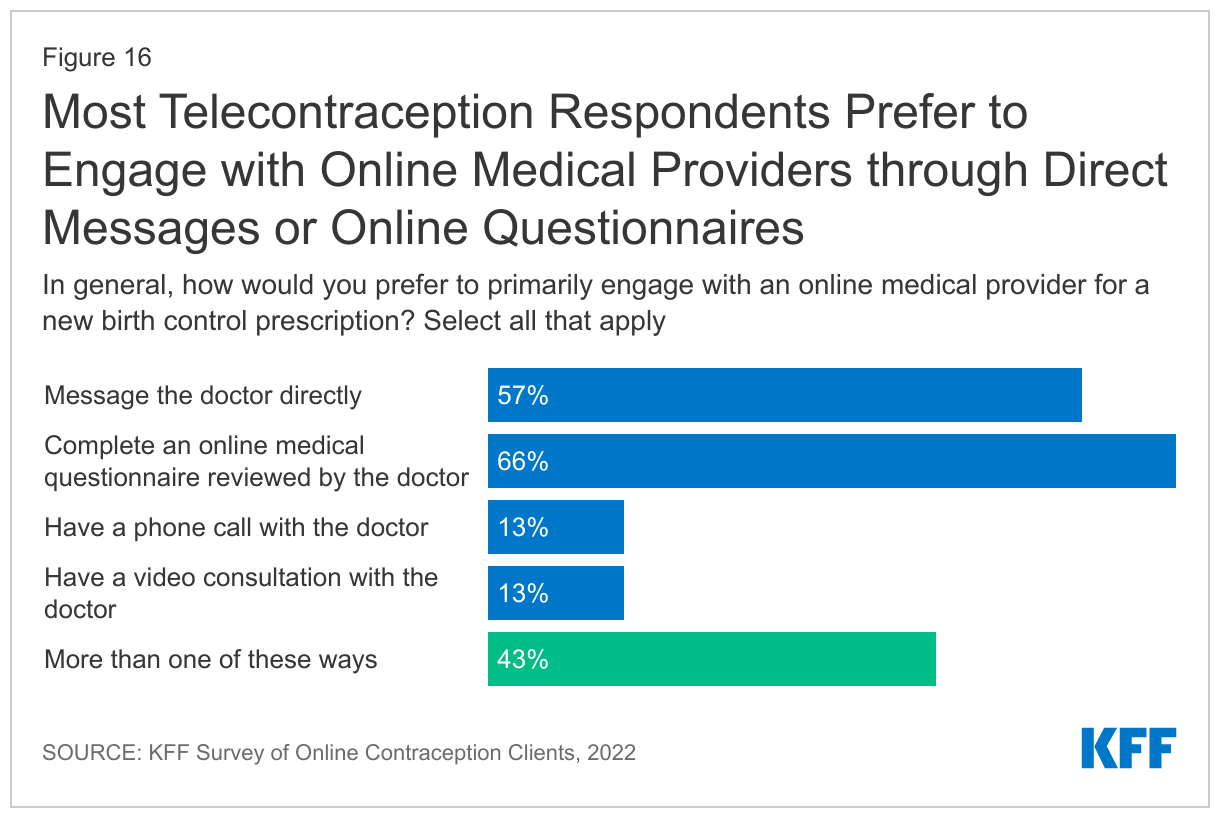
Telecontraception clients generally receive birth control prescriptions by filling out a health questionnaire meant to screen for birth control contraindications, such as high blood pressure, smoking status, or a history of strokes. These questionnaires are then reviewed by healthcare providers, and depending on the policies of the state they reside in, the provider will communicate with the patient via text or chat or will have a video call with the patient to determine whether they are a good candidate for birth control and what method or brand they should use. Survey respondents were asked how they would prefer to engage with online medical providers when obtaining a new birth control prescription, and 57% prefer to message the online medical provider directly. Thirteen percent prefer video calls and 13% prefer phone calls. Sixty-six percent report they prefer filling out an online questionnaire that was reviewed by the medical provider. Four in ten (43%) would prefer to be able to engage with an online medical provider in more than one of these ways (Figure 16).
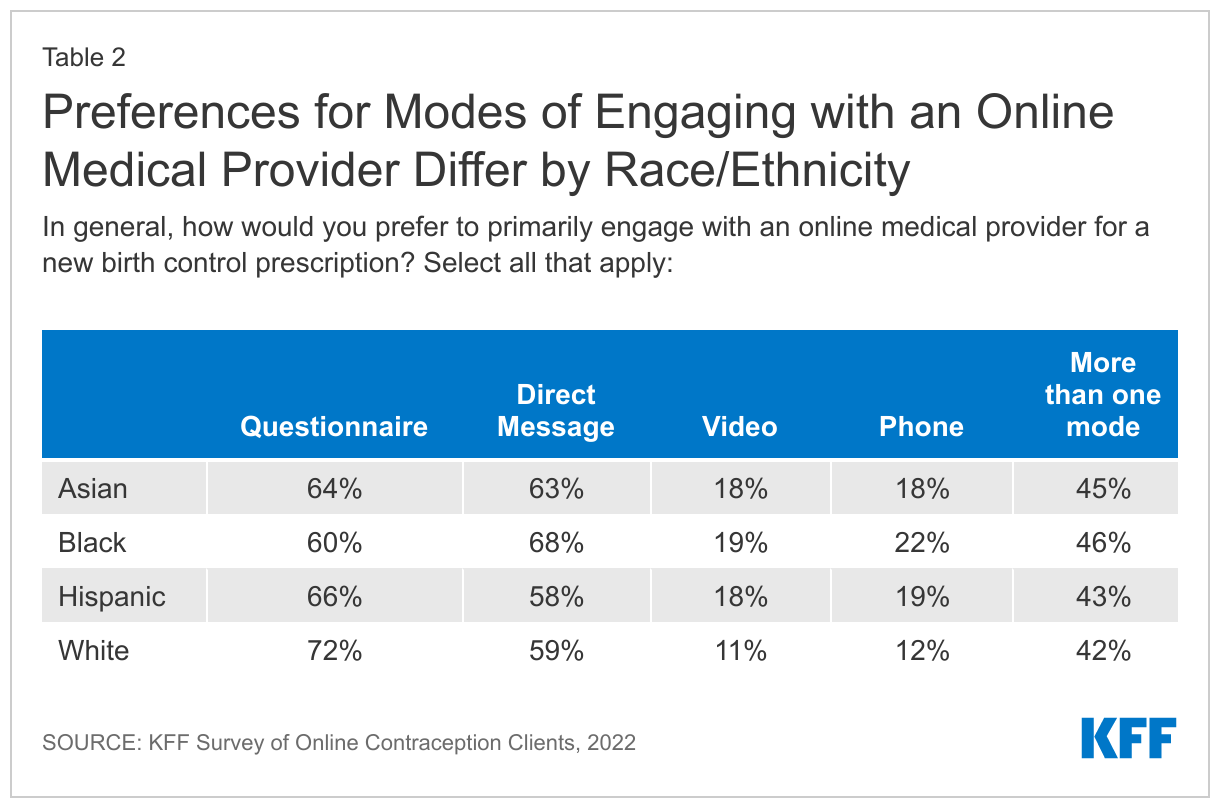
A somewhat higher share of Black respondents said they prefer to primarily engage with online medical providers via direct message compared to White respondents, and higher shares of Black, Hispanic and Asian respondents prefer to engage providers via video calls or phone calls. Somewhat higher shares of White respondents said they preferred to primarily engage with providers via a questionnaire (Table 2).
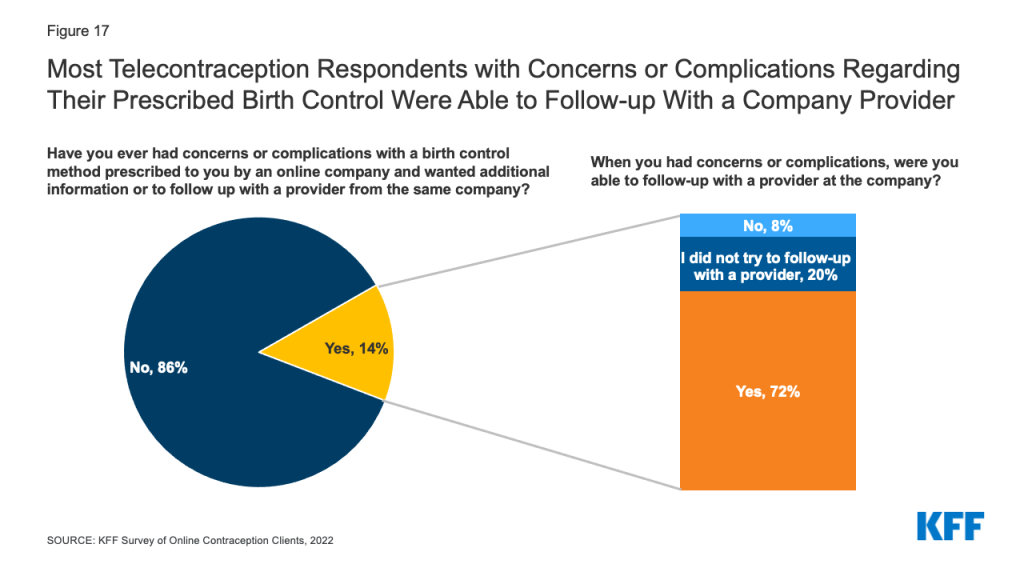
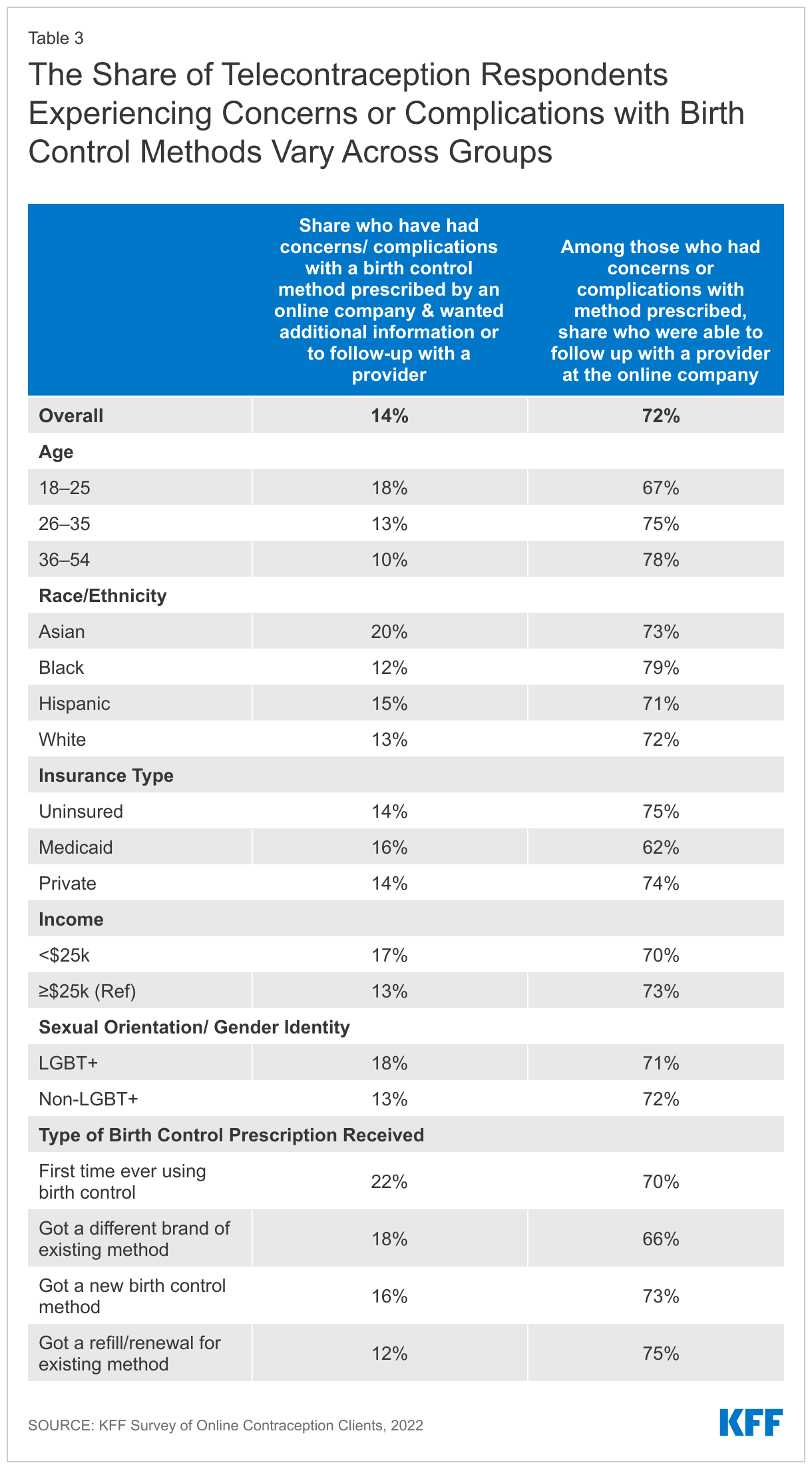
Overall, 14% of respondents report that they had had concerns or complications with a birth control method they had been prescribed through an online platform and wanted additional information or a follow with a medical provider (Figure 17). Among those who had concerns or complications, 72% report they were able to follow up with a provider at the company and another 20% say they never tried to follow up, and eight percent say they were not able to follow up. Larger shares of Asian respondents (20%) and respondents ages 18-25 (18%) report having a concern or complication with a birth control method prescribed through an online platform compared to White respondents (13%) and older respondents (10% of those over age 36) (Table 3). Additionally, larger shares of those getting birth control for the first time or getting a new method or different brand say they had concerns or complications with their method compared to those getting a refill or renewal.
Connections to the Health Care System
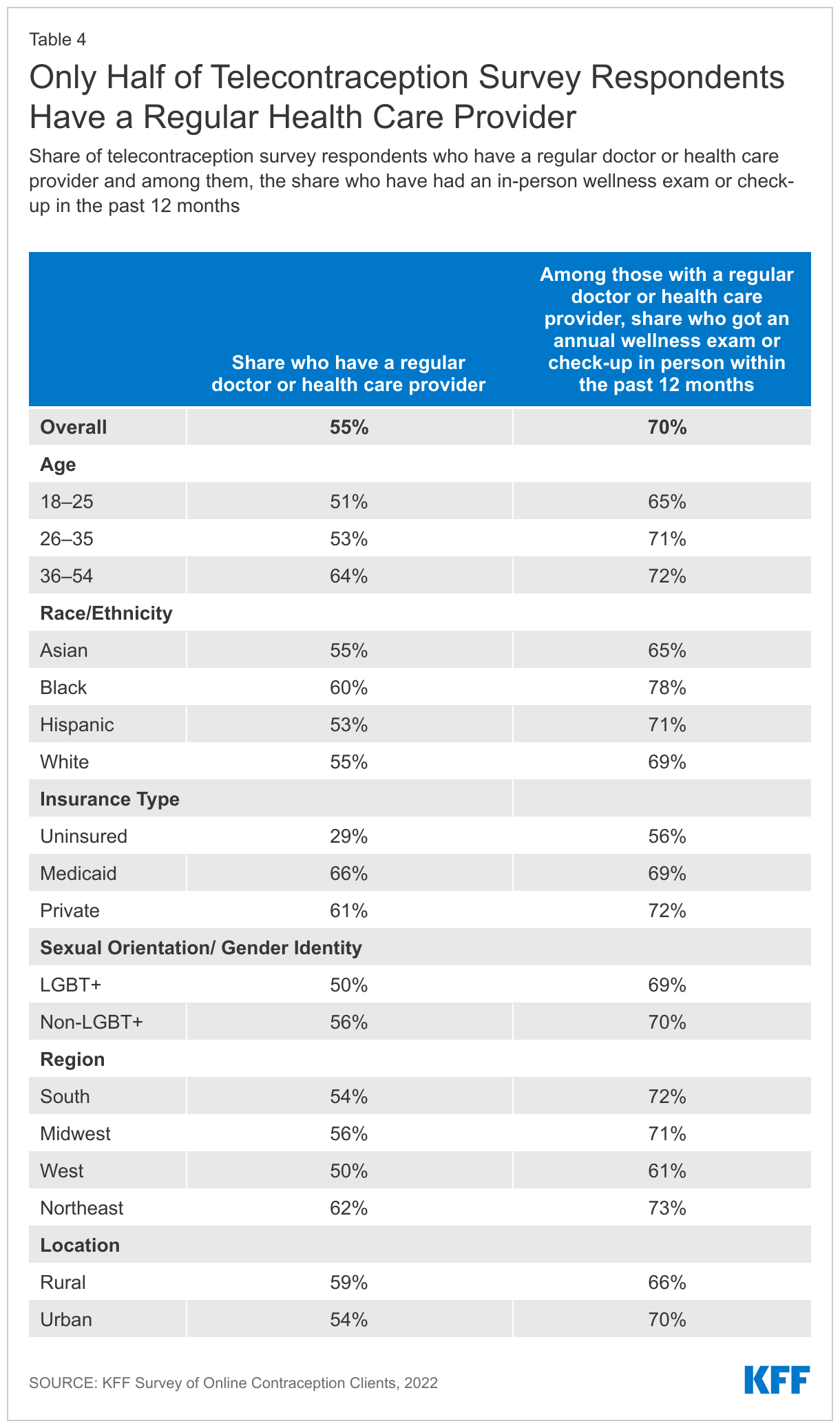
For some, interacting with a telecontraception provider may be their only interaction with a health care provider, while others may use telecontraception for a convenient way to get birth control, but have other connections to the health care system through a brick-and-mortar clinic. Over half (55%) of respondents report they have a regular doctor or health care provider they usually see when they are sick or need routine care. Four in ten (43%) say they do not have a regular doctor, and another 3% say they were not sure. The share without a regular doctor is much higher than women overall in the U.S. (43% vs. 18%). Larger shares of younger respondents compared to older and LGBT+ individuals compared to non-LGBT+ do not have a regular doctor or health care provider. Nearly seven in ten respondents without insurance say they do not have a regular health care provider. Larger shares of Black respondents compared to White respondents and respondents in the Northeastern part of the U.S. compared to all other regions of the country say they have a regular doctor.
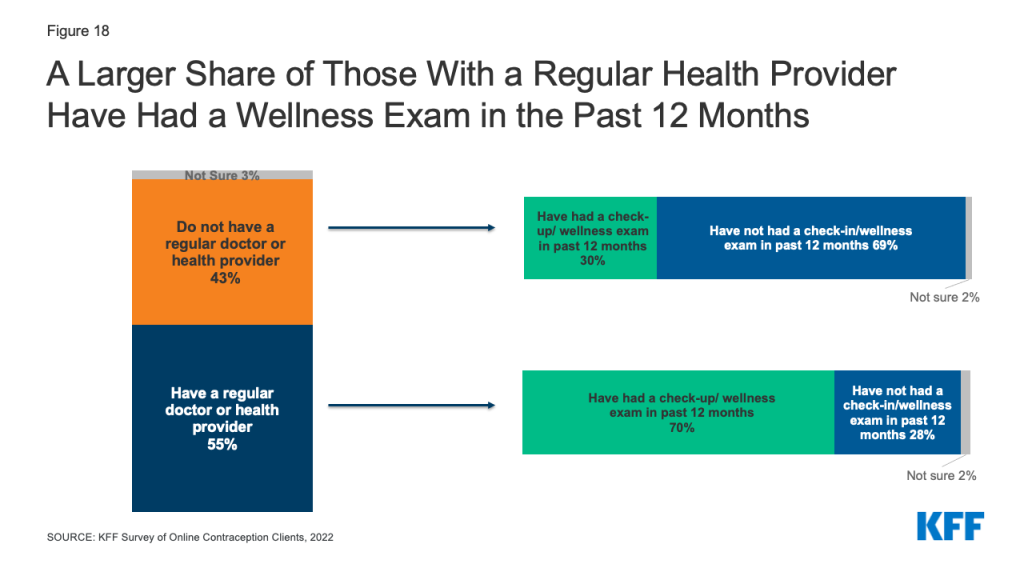
Regular check-ups give patients the opportunity to talk with their health care providers about a broad range of issues, such as preventive health services, role of lifestyle factors on health, and management of chronic health issues. Fifty-two percent of respondents say they have received an in-person annual wellness exam or check up in the past twelve months, while 46% have not. Among those who have a regular doctor or health care provider, 70% report they received an in-person annual exam or check-up in the past 12 months compared to just 30% of those without a regular doctor or health care provider (Figure 18 and Table 4).
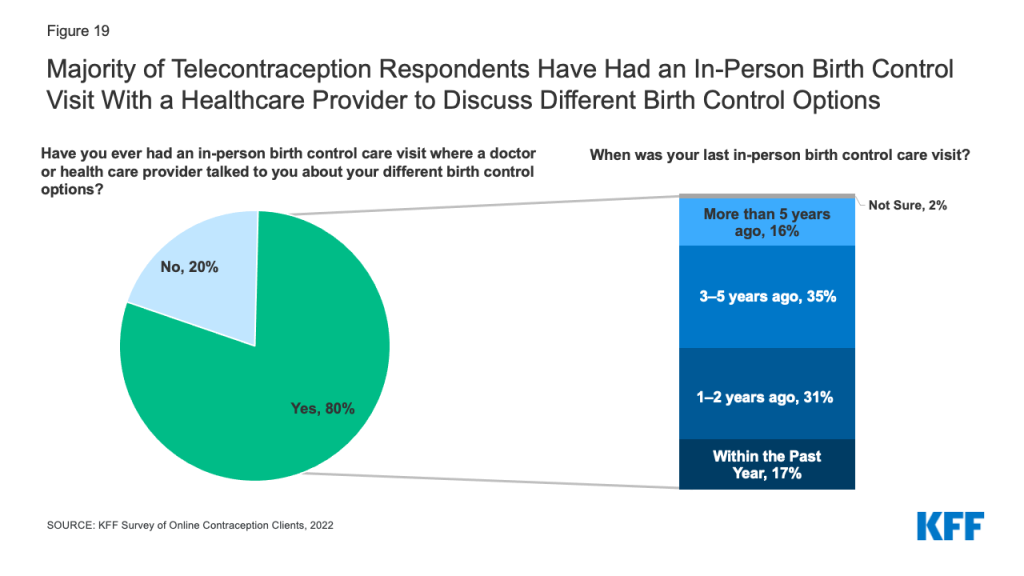
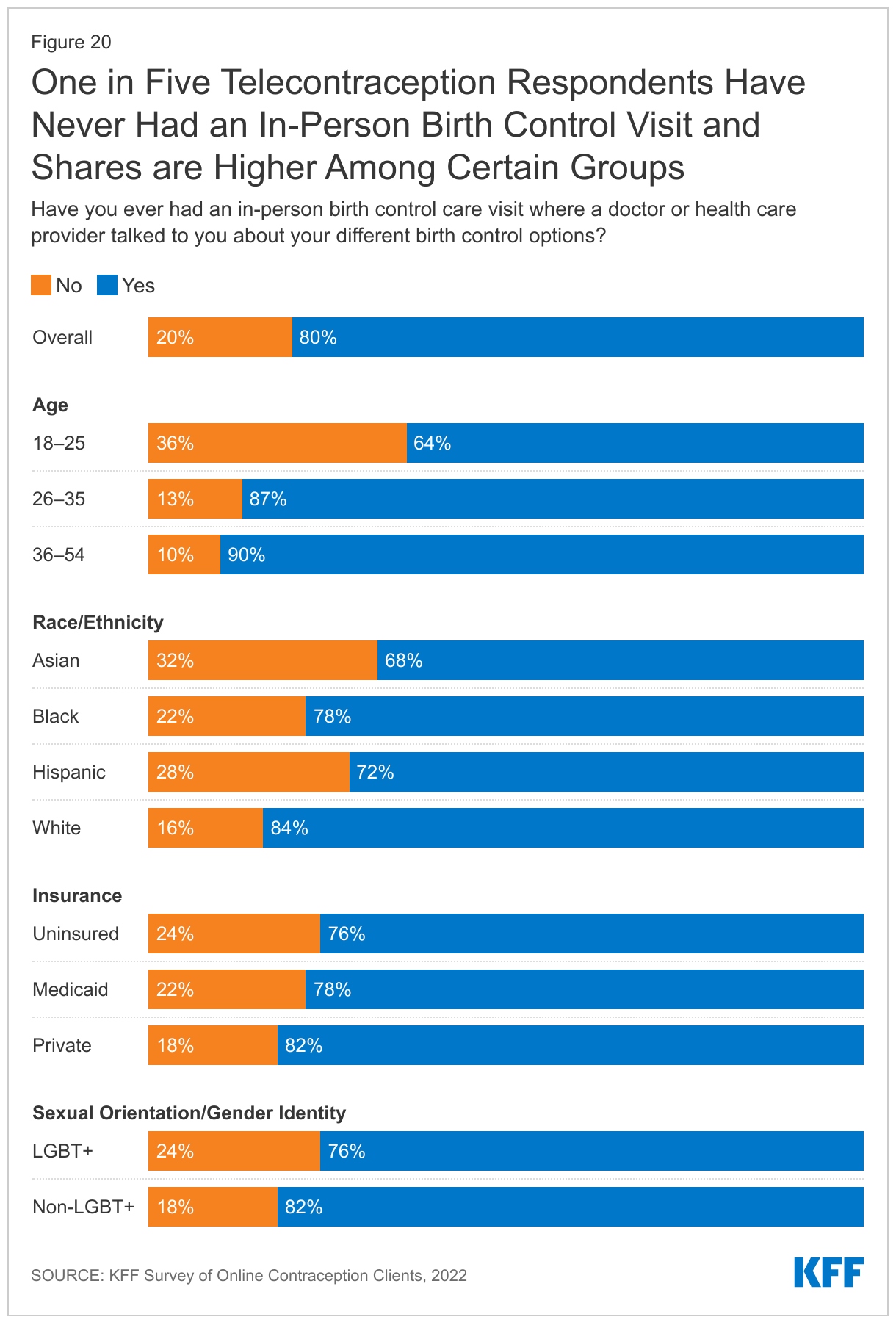
Eighty percent of respondents say they have had had an in-person birth control care visit where a doctor or health care provider had talked to them about their different birth control options at some point in their lives. Among this group, 17% say their last in-person visit was in the past year and 31% say it was one to two years ago. Another 35% report their last visit was in the last three to five years, and 16% say it was more than five years (Figure 19).
One in five (20%) telecontraception respondents report they have never had an in-person birth control visit (Figure 20). Higher shares of respondents ages 18-25 (36%), respondents who identify as LGBT+ (24%), those with Medicaid coverage (22%), and those who are uninsured (24%) report they had never had an in-person visit compared to respondents ages 26–35 and 36–49, those who identify as non-LGBT+, and those with private insurance. Over a third (32%) of Asian respondents and 28% of Hispanic respondents also say they have never had an in-person birth control visit, compared to 22% of Black respondents and 16% of White respondents.
Post-Roe Actions
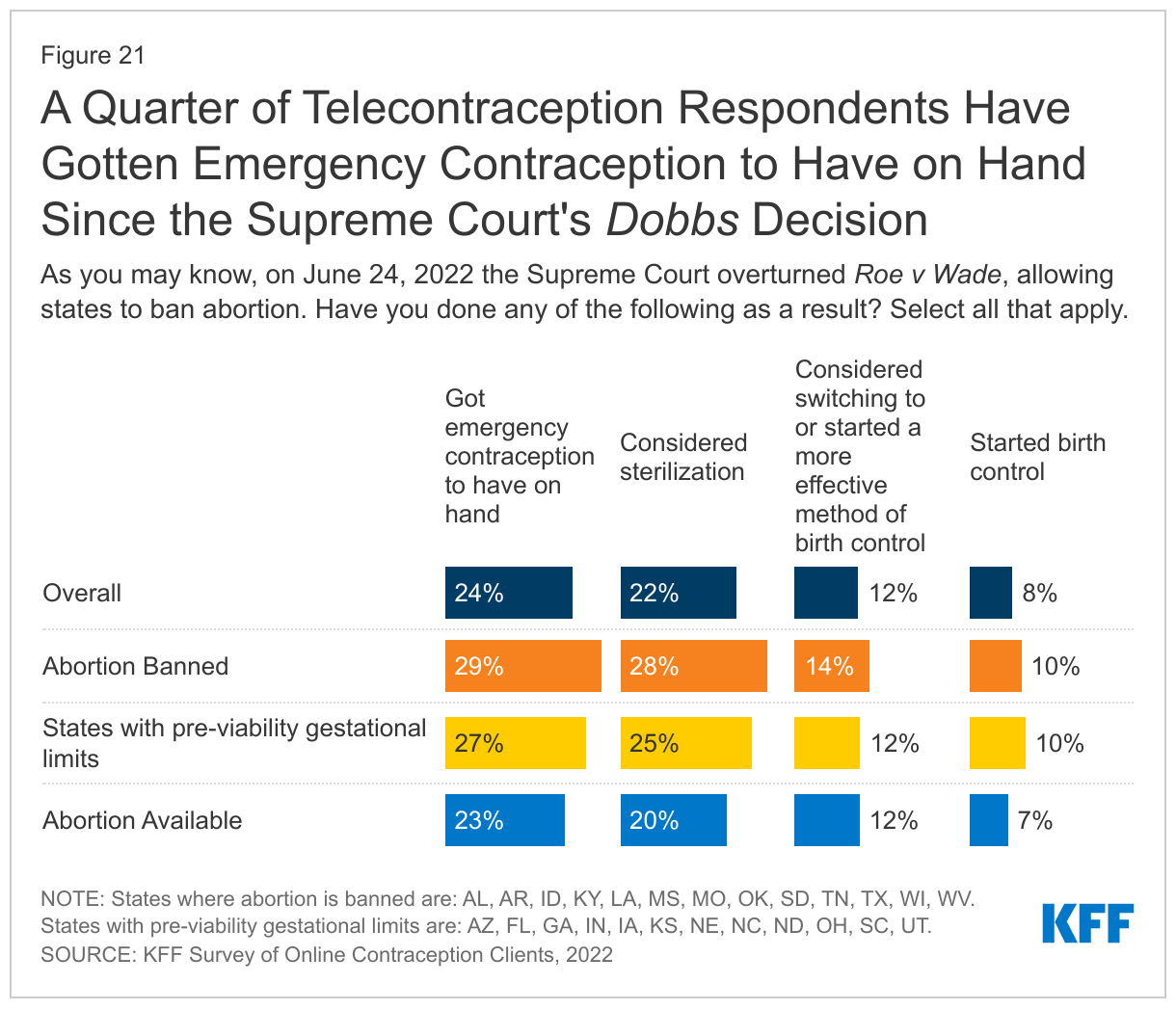
On June 24, 2022 the Supreme Court issued their decision in Dobbs vs Jackson Women’s Health, and overturned Roe v Wade, which eliminated the federal constitutional standard that had protected the right to abortion. Now states can set their own policies banning or protecting abortion rights. As of April 2023, 13 states have banned abortion. After the Dobbs decision, telecontraception companies reported an influx of emergency contraception orders.
In response to the ruling, almost a quarter (24%) of respondents report that they have gotten emergency contraception to have on hand and over a fifth (22%) have considered sterilization. Twelve percent report that they have considered switching to or have started a more effective method of birth control, and eight percent have started using birth control due to the Dobbs decision (Figure 21). These findings were fairly consistent across states regardless of whether abortion was banned or not.
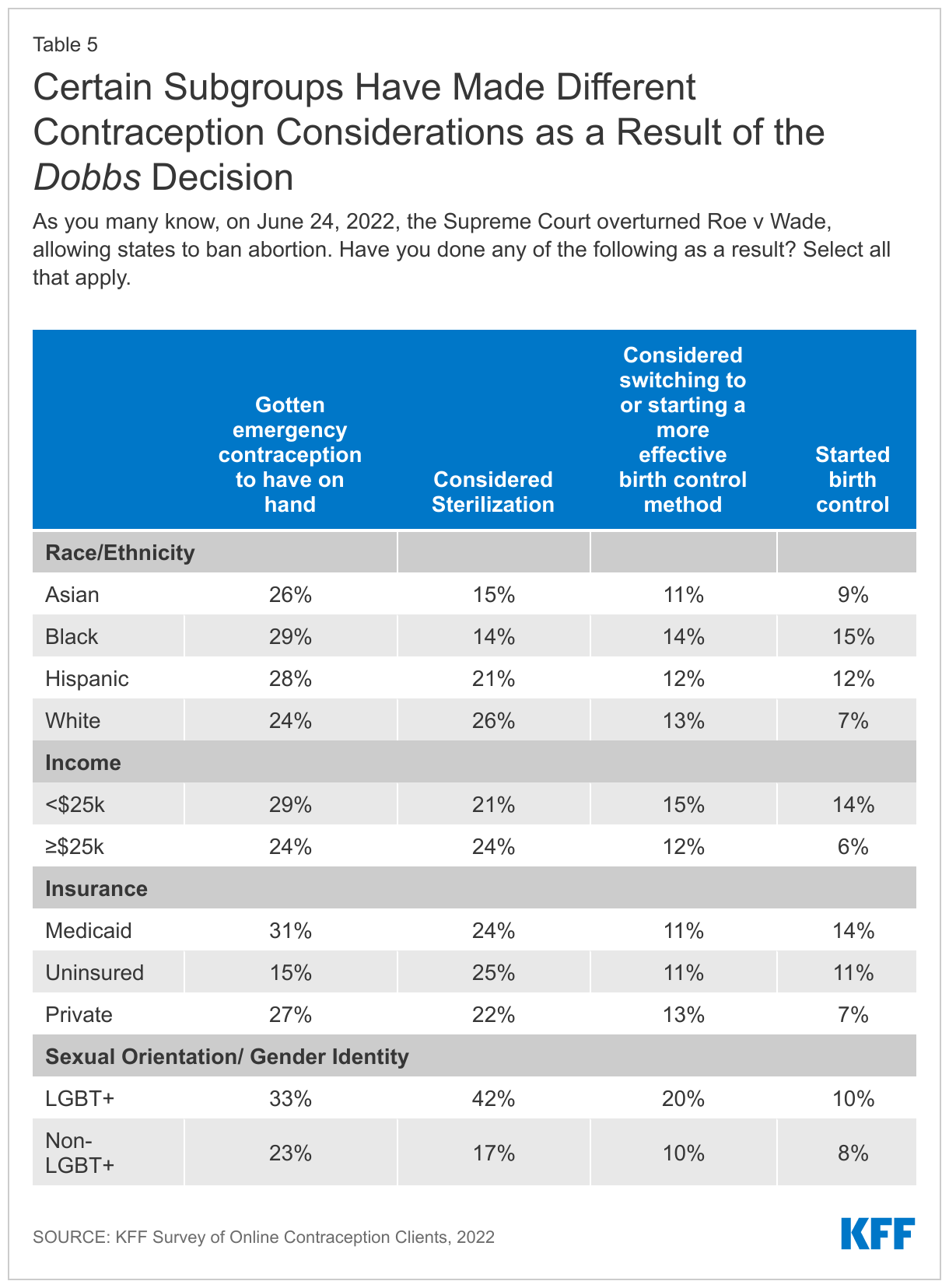
There were some differences in these contraceptive considerations or actions by certain subgroups like race/ethnicity, income, insurance type, and sexual orientation (Table 5). Smaller shares of Black and Hispanic respondents (14% and 21%) compared to White respondents (26%) say they had considered sterilization in the wake of the Dobbs decision, but larger shares of Black and Hispanic respondents say they started birth control (15% and 12%) compared to White respondents (7%). Larger shares of those with lower incomes compared to higher incomes (14% vs. 6%) and those with Medicaid coverage or those without insurance (14% and 11% vs. 7%) compared to those with private insurance say they started birth control. A larger share of LGBT+ individuals compared to non-LGBT+ individuals say they got emergency contraception to have on hand (33% vs. 23%), considered sterilization (43% vs. 17%), and considered switching to or starting a more effective birth control method (20% vs. 10%) after Roe v Wade was overturned.
Looking Forward
While telecontraception remains a relatively new avenue for accessing contraception and only a small share of people say they have accessed services through these platforms, it has been difficult to know the characteristics of telecontraception users and what their experience has been like. Those who responded to this survey are generally satisfied with their experience, say telecontraception has made it easier for them to get their birth control, and they appear to be getting enough information about different birth control methods. However, this is a limited convenience sample and may not be representative of the larger population of telecontraception clients. Telecontraception has provided a way for people to get their birth control without having to leave their home, which has been helpful for many during the COVID-19 pandemic. However, some are left paying out-of-pocket, especially those without insurance, for birth control methods that would otherwise be covered free of charge at a federally funded clinic or through their insurance. In addition, all users must pay a membership or consultation fee, even though their insurance or Medicaid would cover the full cost of a visit and supply if they went to an in-network provider. Many of those accessing contraception online do not have a regular doctor or have never had an in-person birth control visit, so this may be the only information they are getting about birth control methods. Because there are a limited number of birth control methods for them to choose from, telecontraception may not be a good fit for those wanting long-acting reversible contraceptive methods or more comprehensive contraceptive counseling. However, for those who use reversible hormonal methods or seek emergency contraceptive pills, telecontraception offers privacy and convenience, which is valued by the respondents of this survey.
As reproductive health policies and abortion access becomes more restrictive in some states, online companies may play a greater role in expanding access to sexual and reproductive health care.
This work was supported in part by Arnold Ventures. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
We would like to thank Nurx, The Pill Club, Twentyeight Health, and Pandia Health for working with us on this project.