The Landscape of School-Based Mental Health Services
Editorial Note
This analysis, originally published on September 6, 2022, was updated on September 11, 2025 to incorporate the latest developments and data.
Nearly one in five students attending public schools in the United States utilize school-based mental health services, underscoring how schools can serve as an access point for mental health treatment among youth. Federal policy measures, including the Bipartisan Safer Communities Act, the American Rescue Plan Act, and changes to Medicaid guidance, provided pathways to expanding and improving access to school-based services. However, recent actions – such as cuts to the Department of Education, the freezing of $1 billion allocated for school-based mental health services, and major reductions to Medicaid – may cause disruptions. Some school programs have already reported concerns with providing mental health services in the wake of these recent actions, including programs in New York, North Carolina, and Texas. These disruptions come at a time when approximately 1 in 5 teens are experiencing symptoms of anxiety or depression and many youth have reported bullying and exposure to violence, which can have adverse effects on their mental health. Additionally, a 2024 KFF survey found differences in receipt of mental health care services by race and ethnicity, with a larger share of White parents compared to Black, Hispanic, and Asian parents reporting that their children received these services in the past three years.
This issue brief explores the landscape of mental health services, including services offered, utilization, barriers, and funding, and how recent federal actions may affect school-based mental health care. This analysis draws upon survey data collected directly from public school administrators via the School Pulse Panel,1 a study by the National Center for Education Statistics and the U.S. Census Bureau that surveys schools monthly on a variety of topics, including school mental health services. Key Findings include:
- In the 2024-2025 school year, 18% of students utilized school-based mental health services.
- About one-third of schools reported they strongly (11%) or moderately disagreed (25%) that they could effectively provide mental health services. Barriers to providing mental health care services to students include funding and mental health provider shortages.
- Ninety-seven percent of schools provide at least one mental health service to students. In recent years, larger shares of these schools provide services via telehealth, and provide group-based and family interventions.
- Seventy percent of public schools that provide mental health services had a school or district-employed licensed mental health professional on staff and 57% employed an external mental health provider.
- Thirteen percent of schools did not have mental health services available for staff in the 2024-2025 school year.
Background
School-based mental health services can improve access to care, allow for early identification and treatment of mental health issues, and may be linked to reduced absenteeism and better mental health and substance use outcomes. School-based services can also reduce access barriers for underserved populations, including children from low-income households and children of color.
The delivery of mental health services in schools has evolved over time and continues to vary across schools. Some students access in-person mental health services at schools or near campus while others access services through telehealth. Service delivery can range from a single provider (who is not necessarily a licensed mental health professional) to a team of providers, including psychologists, social workers, and academic or guidance counselors. A growing number of schools have also integrated social and emotional learning and other mental health literacy programs into their curriculum.
Schools receive support for providing mental health services in several ways. This includes support at the federal level through the Department of Education and the Department of Health and Human Services. A recent federal measure, the Bipartisan Safer Communities Act (BSCA) of 2022, included provisions to support and expand school-based mental health services, such as $1 billion to increase the number of mental health providers in schools and provide training. However, in April 2025, under the Trump Administration, the Department of Education announced the cancellation of these funds. Additionally, President Trump signed an executive order in March 2025 to dismantle the Department of Education, an entity which has developed guidance regarding school-based health services in partnership with Medicaid and provides resources and grants to support mental health, anti-bullying, and trauma-prevention interventions in schools.
Schools can also receive support through Medicaid, including reimbursement for medically necessary services that are part of a student’s Individualized Education Plan (IEP), reimbursement for eligible health services for students with Medicaid coverage and for some administrative services. In 2022 and 2023, CMS issued guidance to increase the accessibility of these services by eliminating some of the practical barriers that schools faced when delivering services through Medicaid. However, significant changes to Medicaid, including budget cuts, in the reconciliation bill passed in July 2025 may impact how Medicaid can support school services in the future. In 2023, nearly four in ten children in the U.S. had Medicaid coverage.
What Share of Students Utilize School-Based Mental Health Services?
In the 2024-2025 school year, public schools reported that on average 18% of students utilized school-based mental health services. Additionally, 58% of schools reported that the number of students who sought school-based mental health services increased since the prior school year. Similarly, there was a 61% increase from the 2023-2024 school year to the 2024-2025 school year in concerns expressed by staff about students exhibiting depression, anxiety, trauma, or emotional dysregulation/disturbance.
What Have Schools Said About Their Ability To Provide Mental Health Services To Students?
In the 2024-2025 school year, approximately half of public schools reported they could effectively provide mental health services to all students in need. This includes 10% of schools that say they strongly agree they could effectively provide mental health service and 42% that moderately agreed. Meanwhile, about one-third of schools reported they strongly (11%) or moderately disagreed (25%) that they could effectively provide mental health services and 11% neither agreed or disagreed. These shares have remained mostly similar since survey data collection began in the 2021-2022 school year.
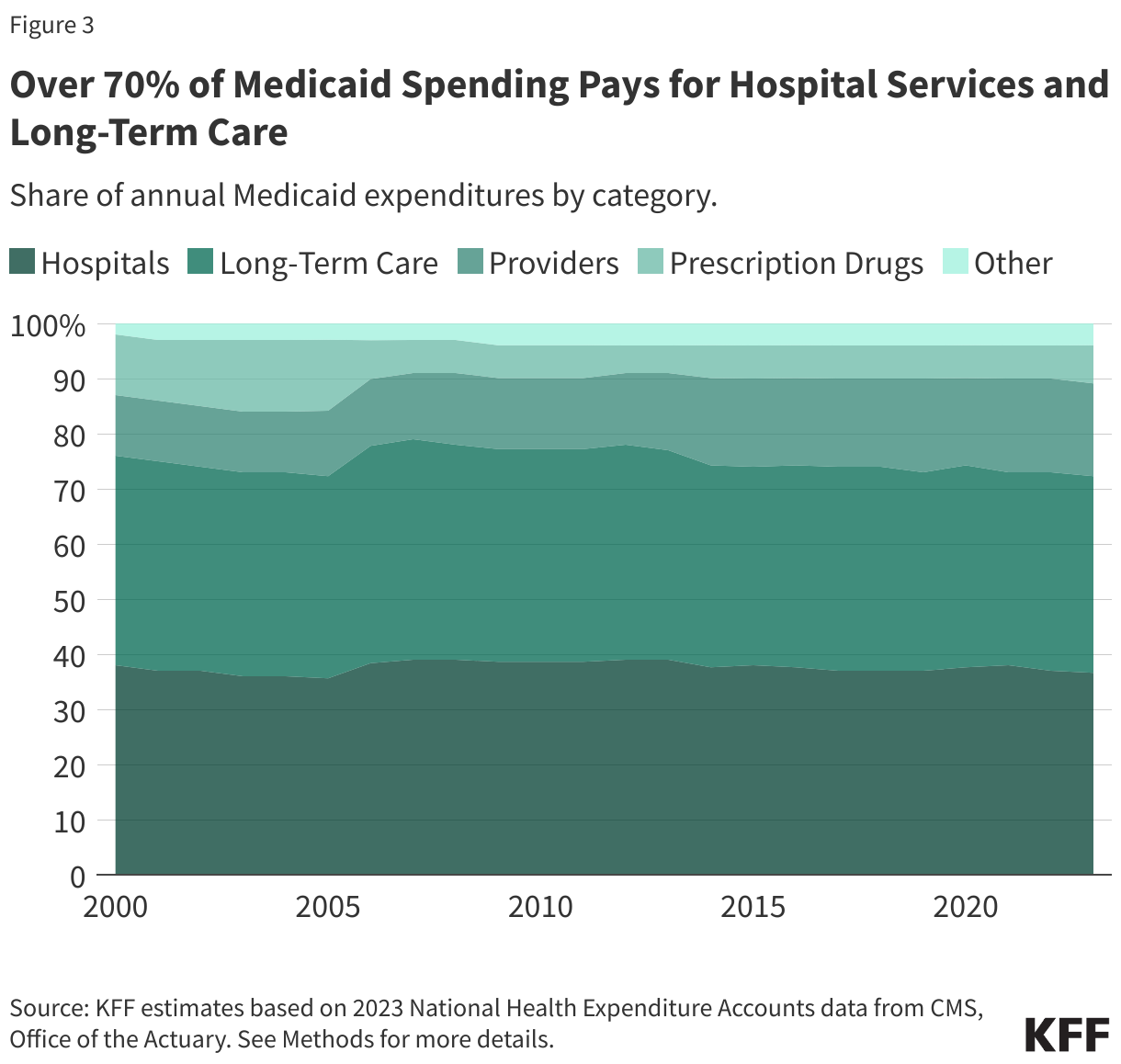
Among the schools that did not strongly believe they could effectively provide mental health services to students in need, inadequate funding and mental health provider shortages have remained the most frequently reported limitations since the 2021-2022 school year (Figure 1).
However, the share reporting inadequate funding has increased over time (from 47% in 2021-2022 to 56% in 2024-2025), while the share reporting insufficient mental health staff coverage and access to licensed professionals has slightly decreased over the same period (from 61% to 55% and from 57% to 51%, respectively). These changes may reflect recent federal efforts to increase the number of school mental health professionals but also the end of federal pandemic-era funds. Further, many schools continue to not meet recommended ratios for psychologists to students (500:1) or counselors to students (250:1). Among schools with staffing vacancies in the 2024-2025 school year, 28% of public school administrators feel they are understaffed with mental health providers.
What Mental Health Services Are Offered to Students?
In the 2024-2025 school year, 97% of public schools reported offering at least one type of mental health service to their students. As shown in Figure 2, the most frequently offered services are:
- Individual-based intervention like one-on-one counseling or therapy (83% of public schools)
- Case management or coordinating mental health services (70%), and
- Referrals for care outside of the school (67%).
The use of telehealth to deliver mental health treatment has increased from 17% to 22% between the 2021-2022 and 2024-2025 school years. While telehealth became a more widely used pathway to delivering health care since the pandemic, a growing number of schools were already providing care through telehealth prior to the pandemic.
Group-based interventions increased between the 2021-2022 and 2024-2025 school year (from 56% to 65%), as well as family interventions (from 38% to 43%).
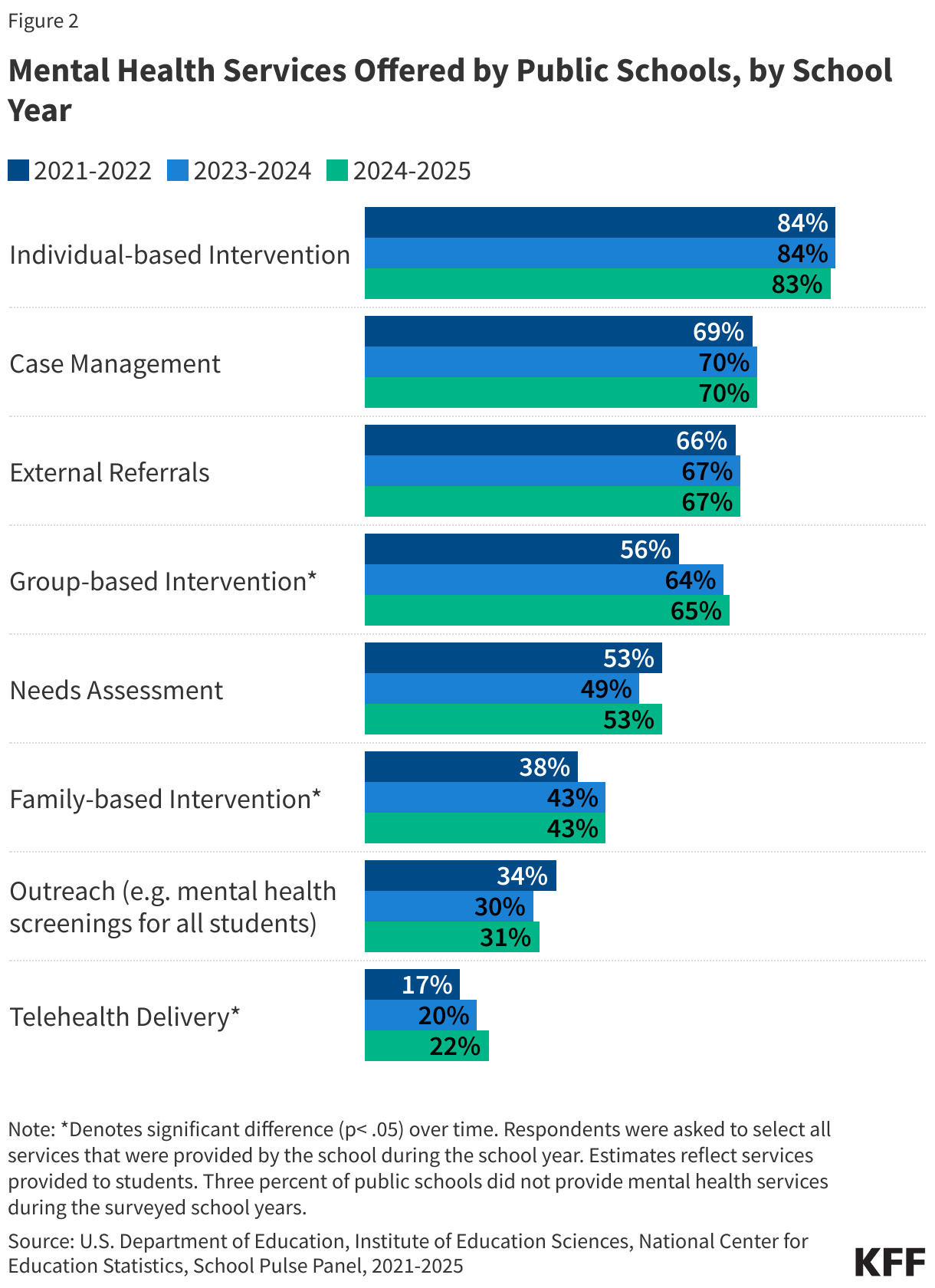
Only about one-third of schools provide outreach services, which includes mental health screenings for all students. These universal behavioral health screenings are considered a best practice and allow for schools to better identify all students with needs and tailor services to their specific student population. However, many schools do not offer these screenings often due to a lack of resources or difficulty accessing providers to conduct screenings, burden of collecting and maintaining data, and/or a lack of buy-in from school administrators.
Who Provides Mental Health Services in Schools?
Staffing models for school-based mental health care can vary across schools. In the 2024-2025 academic year, 76% of public schools that provide mental health services had two or more types of mental health providers while 24% have one type of provider. In the same year, 70% of these public schools had a school or district-employed licensed mental health professional on staff and 57% had an external mental health provider (Figure 3).
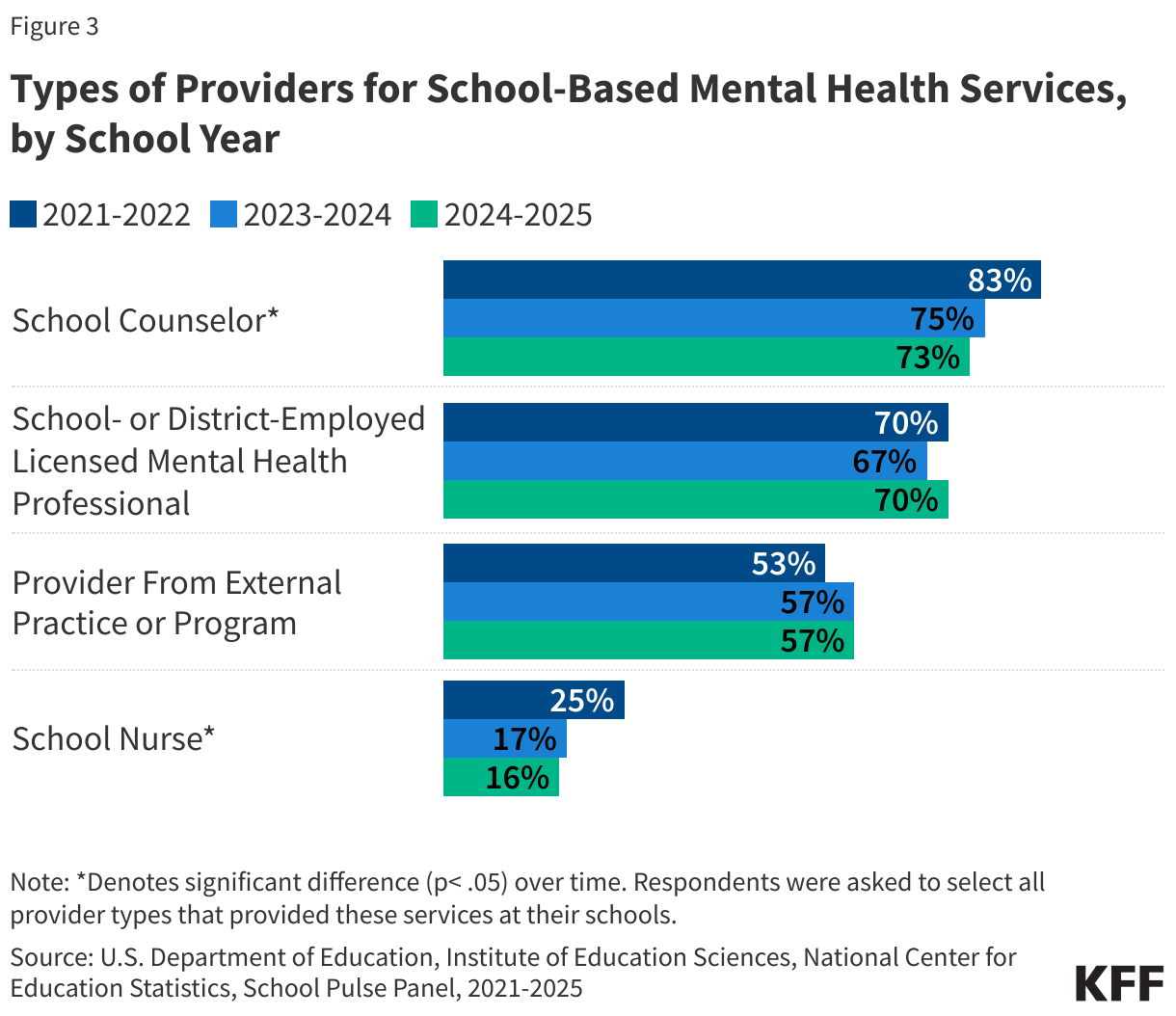
Between the 2021-2022 and 2024-2025 school years, there was a decrease in the share of public schools reporting that school counselors (from 83% to 73%) or school nurses (from 25% to 16%) provided mental health services to students (Figure 3). These decreases may be reflective of schools expanding their mental health teams in recent years so that they are less reliant on general counselors and medical staff. While general or academic school counselors can provide mental health services to students, they are not equipped to offer long-term care.
Teachers often play a role in identifying students with mental health needs and linking them to care, although prior research suggests that many teachers may not be adequately trained to do so. In the 2024-2025 school year, 61% of schools reported providing trainings and professional development to staff in order to help them support the emotional and mental health of school students. Data on the impact of these trainings is unavailable and it is unclear what share of schools provided trainings in the years prior.
How Do Schools Receive Funding For The Mental Health Services They Provide?
School mental health services are supported through multiple sources of funding at the national, state, and local level. In recent years, a growing share of public schools reported receiving funding for mental health services from district or school funds (from 58% in 2021-2022 to 65% in 2024-2025) or partnerships with organizations (from 38% in 2021-2022 to 44% in 2024-2025) (Figure 4). Note that the School Pulse Panel survey questionnaire does not specify which funds are from Medicaid.
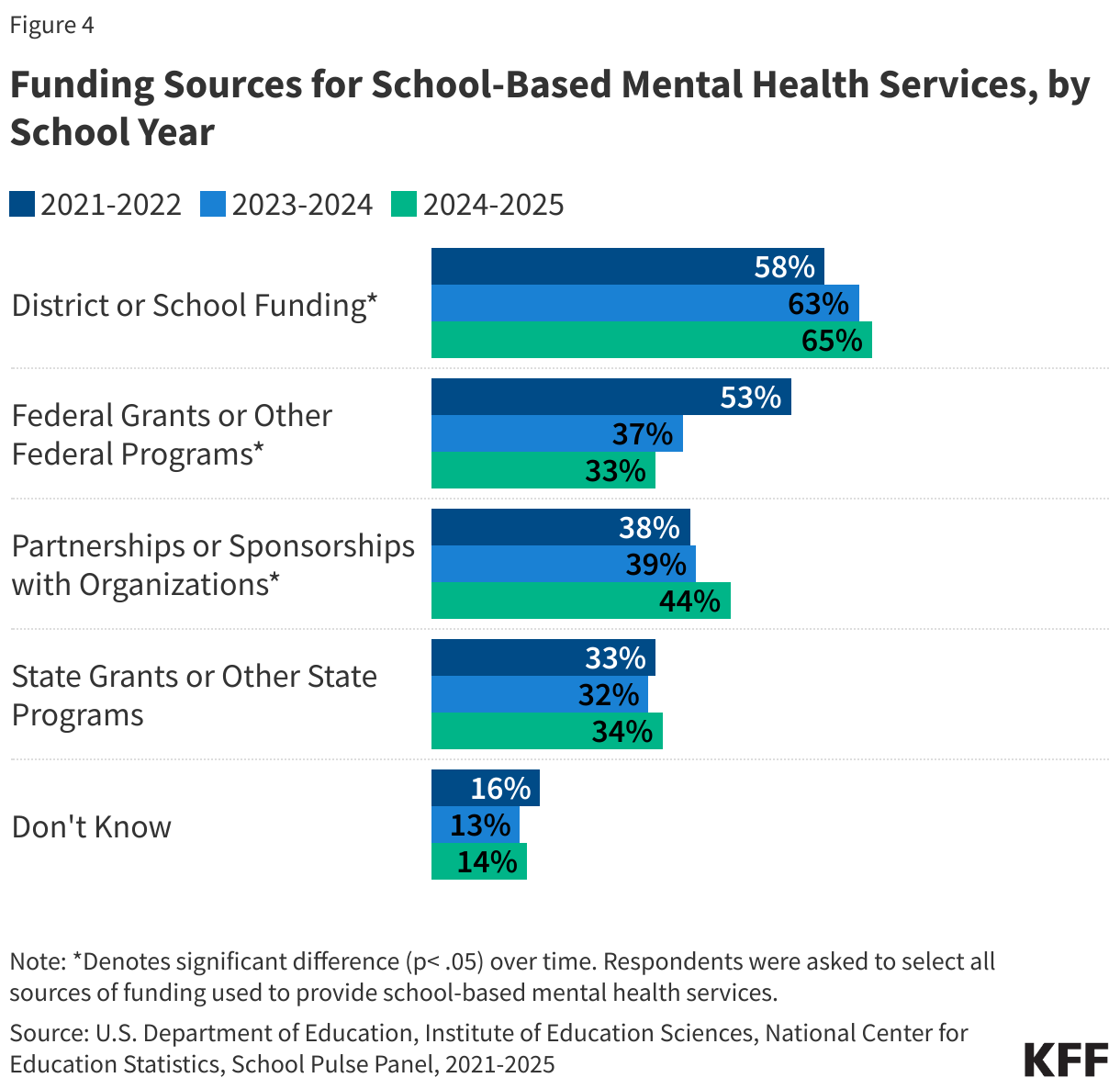
The share of public schools receiving funding from federal grants or programs has decreased from 53% in 2021-2022 to 33% in 2024-2025. This change may be due to the cessation of pandemic-era relief funds, like the Elementary and Secondary School Emergency Relief (ESSER) funds, which provided schools with the financial resources to address increasing concerns about student mental health. In 2022, the Bipartisan Safer Communities Act allowed for new funding sources to support school-based mental health services, however the Trump Administration froze $1 billion in funding in 2025.
What Mental Health Services Are Available For Staff?
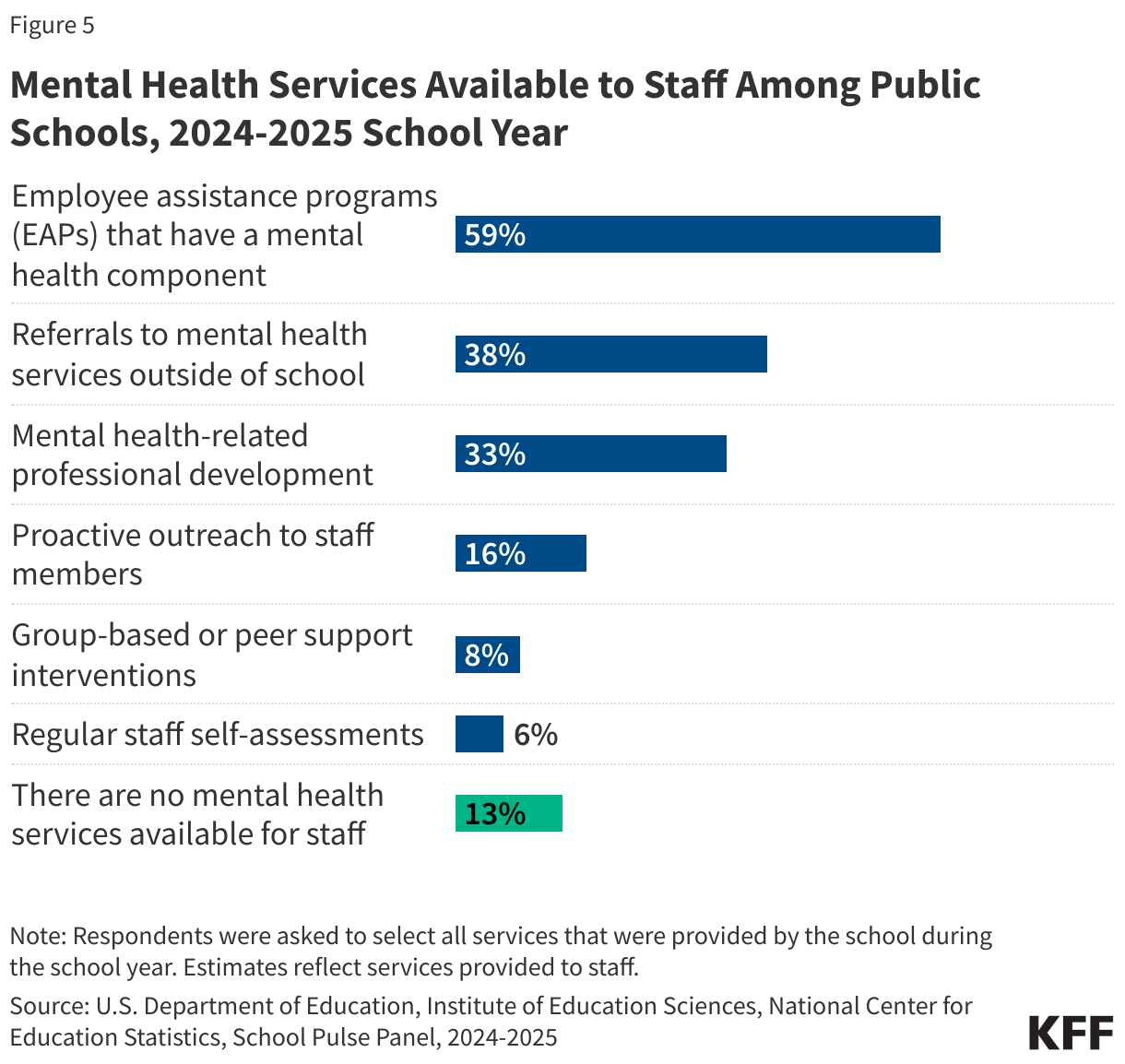
Teachers and other school staff play a multitude of roles, including monitoring students’ mental health and providing support as needed. Burnout, driven by anxiety, depression, and low job satisfaction is prevalent among teachers. In the 2024-2025 academic year, 36% of staff reported that they have seen an increase in staff expressing concerns about themselves or their colleagues showing signs of depression, anxiety, emotional dysregulation or trauma since the prior school year. While many schools offer mental health services for staff, 13% of schools do not (Figure 5).
Sasha Zitter, formerly with KFF, contributed to this analysis.
- The School Pulse Panel utilizes a random stratified sample of the Common Core of Data, a universe of public schools. This stratified sample includes public and public charter schools, schools with magnet programs, alternative schools, special education schools, and vocational schools. Approximately 4,000 schools were included in the sample for the 2024-2025 school year. Approximately 1,600 schools responded to the March survey – findings from this survey are included in this brief. There has been some variation in the number of schools that respond each month. While school principals are the initial point of contact to complete the survey, they may invite other school and district staff to assist with completion. Published data is weighted and adjusted to account for non-response. ↩︎