KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
The U.S territories – American Samoa, the Commonwealth of the Northern Mariana Islands (CNMI), Guam, Puerto Rico, and the U.S. Virgin Islands (USVI) – have faced an array of longstanding fiscal and health challenges that were exacerbated by somewhat recent natural disasters and the COVID-19 pandemic. Over 1.7 million people residing in the territories were enrolled in Medicaid in fiscal year (FY) 2023. Medicaid financing in the territories differs from the states due to a statutorily set Federal Medical Assistance Percentage (FMAP) and an annual ceiling in federal funding that has historically resulted in lower levels of funding and often health care coverage and access.
Over time, Congress has provided temporary supplemental federal funding and increases to the FMAP rate in response to emergencies beyond the Medicaid allotments set in statute. Most recently, the Families First Coronavirus Response Act (FFCRA) significantly increased allotments for the territories and the 2023 Consolidated Appropriations Act (CAA) included a permanent statutory increase to 83% (from 55%) for most of the territories’ Medicaid allotments and FMAP rates, except Puerto Rico. In Puerto Rico, the allotments are set in statute through FY 2027, and the FMAP was increased to 76% and set to expire after FY 2027 and return to 55% without legislative action.
While neither candidate has announced detailed policy proposals in the campaign, the outcome of the 2024 election could have implications for the American territories. In a recently released policy fact sheet, Vice President Harris highlights several initiatives to support Puerto Rico, including calling for Congress “to pursue parity and equal access to key federal programs that support health care, nutrition, and other critical needs for low-income families, seniors, and people with disabilities.” In addition, the Biden-Harris administration proposed eliminating Medicaid funding caps for the American territories and bringing FMAP rates in parity with the states in their FY 2025 budget. In contrast, former President Trump previously proposed reducing Medicaid funding for Puerto Rico and has supported proposals to cap and reduce Medicaid financing and the FMAP, which could impact the territories as well. This issue brief provides background on how Medicaid financing differs between U.S. territories and states and the implications of these differences.
How does Medicaid in the territories differ from the states?
Unlike in the 50 states and D.C., annual federal funding for Medicaid in the U.S. territories is subject to a statutory cap and fixed matching rate. Both the capped federal allotment (known as the Section 1108(g) allotment) and the territories’ FMAP are fixed in statute. Annual federal Medicaid funding is set in statute for Puerto Rico for FY 2023 through FY 2027 and increases in the allotments are tied to the medical care component of the Consumer Price Index for All Urban Consumers (CPI-U) for the rest of the territories. This funding arrangement is unlike federal Medicaid funding for states, where federal dollars are uncapped and the FMAP is adjusted annually based on a state’s relative per capita income. In addition, the territories receive Section 1935(e) funding, also known as the Enhanced Allotment Program (EAP), which can be used to provide prescription drug coverage under Medicaid for low-income Medicare beneficiaries who would otherwise be eligible for subsidies under Medicare Part D. Most territories receive funding for Medicaid data systems, and Puerto Rico receives additional funds for physician payment rates and for program integrity through FY 2027.
Medicaid programs in the territories have programmatic differences in coverage and benefits compared to the states. Unlike the states, the territories develop their own measures rather than use federal poverty levels (FPL) to determine eligibility for Medicaid for the population. CNMI and American Samoa operate Medicaid programs under waivers so they are not subject to most program requirements, including flexibility that allows them to waive coverage of any benefits that are mandatory in the states when needed.
What are recent Medicaid financing changes for the Territories?
The 2023 CAA included a permanent statutory increase in territories’ Medicaid FMAP rate, except in Puerto Rico, where the increase will expire at the end of FY 2027. Congress has previously authorized both permanent and supplemental increases in the FMAP rate for the territories broadly and in response to specific emergency events (Table 1). Following the passage of the Affordable Care Act (ACA), the FMAP rate for territories was increased from 50% to 55% in 2011, and at the beginning of FY 2020, during the COVID-19 pandemic, the FMAP was temporarily increased to 100%. For the remainder of FY 2020 through the beginning of FY 2023, Congress increased FMAP rates from 55% to 83% for American Samoa, CNMI, Guam, and USVI and from 55% to 76% for Puerto Rico (with an additional increase of 6.2% if certain maintenance of eligibility requirements were met). With the 2023 CAA, Congress made the temporary FMAP increase to 83% permanent for American Samoa, CNMI, Guam, and the USVI, while authorizing a temporary increase to Puerto Rico’s FMAP to 76% through FY 2027. The law also provides 100% federal funding for qualifying data system improvements for American Samoa, CNMI, Guam, and USVI, up to $20 million for all four of the territories.
In addition to the change in the FMAP rates, annual federal capped funding for the territories increased substantially in FY 2020. The FFCRA increased allotments for each of the territories for FY 2020 and FY 2021 and then CMS used these levels as the new base for FY 2022 and beyond, except for Puerto Rico, where capped amounts are set in statute through FY 2027. The annual capped funding for Puerto Rico will be $3.475 billion for FY 2025, $3.645 billion for FY 2026, and $3.825 billion for FY 2027. After FY 2027, the allotments for Puerto Rico will be calculated from the much lower FY 2019 base without a legislative change.
What are the implications of the Medicaid financing structure in the territories?
The capped federal Medicaid funding structure in the territories contributes to cost shifts to the territories and/or coverage restrictions. Once a territory exhausts its capped federal funds, the territory must use local funds to cover costs of coverage or may suspend or limit services. Historically, all of the territories have reported depleting the capped federal funds before the fourth quarter of the year. Medicaid programs in American Samoa and CNMI have recently suspended or limited a wide range of services for parts of the fiscal year due to funding constraints, despite the recent increases in allotments and FMAP rates.
In the absence of additional statutory changes, annual federal allotments for Medicaid in Puerto Rico will drop and the FMAP rate will drop to 55% in FY 2028. Under the 2023 CAA, Puerto Rico’s annual federal allotment will drop in FY 2028 because it will be re-calculated based on the annual FY 2019 cap adjusted to the medical component of the CPI-U without regard for the additional funding received between FY 2020 and FY 2027, and the FMAP will return to 55% in FY 2028. Both of these changes would result in significant reductions in federal Medicaid funding for Puerto Rico. Beyond adjustments for Puerto Rico, proposals like the Territories Health Equity Act would treat the territories like states for Medicaid funding and eliminate federal funding caps if enacted by Congress.
Limits on federal Medicaid funding contribute to increasing challenges for the territories in addressing health care needs of their residents given growing poverty, infrastructure, and environmental challenges. Studies have found that the territories rank worse than the states on health care quality measures and health outcomes. The territories also have higher rates of poverty and unemployment, and all the territories, with the exception of Puerto Rico, also have higher rates of uninsured people than the U.S. population overall (Appendix Figure 1). Limitations in federal data on the American territories, including gaps in federal statistics and Medicaid claims reporting, and limited local public health workforce capacity may reduce government capabilities to understand and address these challenges. The territories have also become increasingly susceptible to natural disasters and environmental hazards due to climate change as well as U.S. colonial and military activity, which can exacerbate population loss due to outmigration and further negatively impact island economies. Recent disaster events in Puerto Rico have also shown how they negatively impact health outcomes and the mental health of residents in the long-term.
NOTE: This brief was updated on November 4, 2024 to incorporate additional information about the role of midwives in maternal and infant care.
Summary
Stark racial disparities in maternal and infant health in the U.S. have persisted for decades despite continued advancements in medical care. The disparate impact of the COVID-19 pandemic for people of color increased attention to health disparities, including the longstanding inequities in maternal and infant health. Additionally, the overturning of Roe v. Wade, increased barriers to abortion and may widen the existing disparities in maternal health. Given these factors, there recently has been increased attention to improving maternal and infant health and reducing disparities in these areas.
This brief provides an overview of racial disparities for selected measures of maternal and infant health, discusses the factors that drive these disparities, and provides an overview of recent efforts to address them. It is based on KFF analysis of publicly available data from CDC WONDER online database, the National Center for Health Statistics (NCHS) National Vital Statistics Reports, and the CDC Pregnancy Mortality Surveillance System. While this brief focuses on racial and ethnic disparities in maternal and infant health, wide disparities also exist across other dimensions, including income, education, age, and other characteristics. For example, there is significant variation in some of these measures across states and disparities between rural and urban communities. Data and research often assume cisgender identities and may not systematically account for people who are transgender and non-binary. In some cases, the data cited in this brief use cisgender labels to align with how measures have been defined in underlying data sources. Key takeaways include:
Large racial disparities in maternal and infant health outcomes persist. Pregnancy-related mortality rates among American Indian and Alaska Native (AIAN) and Black women are over three times higher than the rate for White women (63.4 and 55.9 vs. 18.1 per 100,000). Black, AIAN, and Native Hawaiian or Pacific Islander (NHPI) women also have higher shares of preterm births, low birthweight births, or births for which they received late or no prenatal care compared to White women. Infants born to Black, AIAN, and NHPI people have markedly higher mortality rates than those born to White people.
Maternal and infant health disparities reflect broader underlying social and economic inequities that are rooted in racism and discrimination. Differences in health insurance coverage and access to care play a role in driving worse maternal and infant health outcomes for people of color. However, inequities in broader social and economic factors, including income, are primary drivers for maternal and infant health disparities. Moreover, disparities in maternal and infant health persist even when controlling for certain underlying social and economic factors, such as education and income, pointing to the roles racism and discrimination play in driving disparities.
Increased attention to maternal and infant health has contributed to a rise in efforts and resources focused on improving health outcomes and reducing disparities in these areas. These include efforts to expand access to coverage and care, increase access to a broader array of services and providers that support maternal and infant health, diversify the health care workforce, and enhance data collection and reporting. However, addressing social and economic factors that contribute to poorer health outcomes and disparities will also be important. Moreover, the persistence of disparities in maternal health across income and education levels, points to the importance of addressing the roles of racism and discrimination as part of efforts to improve health and advance equity.
Moving forward, legislative and policy efforts and the outcome of the 2024 presidential election could all have important implications for efforts to address racial disparities in maternal and infant health. For example, state variation in access to abortion in the wake of the overturning of Roe v. Wade may exacerbate existing racial disparities in maternal health. Further, differences in records and proposed approaches by Vice President Harris and former President Trump on abortion, reproductive health, and maternal health will likely have different implications for disparities in maternal health going forward.
Racial Disparities in Maternal and Infant Health
Pregnancy-Related Mortality Rates
In 2020, approximately 900 women died in the U.S. from causes related to or worsened by pregnancy. Pregnancy-related deaths are deaths that occur within one year of pregnancy. Approximately one quarter (26%) occur during pregnancy, another quarter (27%) occur during labor or within the first week postpartum, and nearly half (47%) occur one week to one year postpartum, underscoring the importance of access to health care beyond the period of pregnancy. Recent data shows that more than eight out of ten (84%) pregnancy-related deaths are preventable. Although leading causes of pregnancy-related death vary by race and ethnicity, infection (including COVID-19) and cardiovascular conditions are the leading causes of pregnancy-related death among women overall, illustrating the importance of care for chronic conditions on pregnancy-related outcomes. Additional data from detailed maternal mortality reviews in 38 states found mental health conditions to be the overall leading cause of pregnancy-related deaths.
AIAN and Black people are more than three times as likely as White people to experience a pregnancy-related death (63.4 and 55.9 vs. 18.1 per 100,000 live births) in 2020 (Figure 1). Hispanic people also have a higher rate of pregnancy-related deaths compared to White people (22.6 vs. 18.1 per 100,000). The rate for Asian people is lower compared to that of White people (14.2 vs. 18.1 per 100,000). Data from one year were insufficient to identify mortality among NHPI women. However, earlier data showed that NHPI (62.8 per 100,000) people had the highest rates of pregnancy-related mortality across racial and ethnic groups.
Research shows that these disparities increase by age and persist across education and income levels. Data show higher pregnancy-related mortality rates among Black women who completed college education than among White women with the same educational attainment and White women with less than a high school diploma. Similarly, studies find that high income Black women have the same risk of dying in the first year following childbirth as the poorest White women. Other research also shows that Black women are at significantly higher risk for severe maternal morbidity, such as preeclampsia, which is significantly more common than maternal death. Further, AIAN, Black, NHPI, Asian, and Hispanic women have higher rates of admission to the intensive care unit during delivery compared to White women, which is considered a marker for severe maternal morbidity.
Maternal death rates declined across most racial and ethnic groups between 2021 and 2022 following the large increase in maternal deaths rates due to COVID-19. Maternal mortality and pregnancy-related mortality are similar concepts but maternal mortality is a narrower measure, limited to deaths that occur while pregnant or within 42 days or pregnancy and excluding those due to accidents or acts of violence. However, more recent maternal mortality data are available allowing for examination of trends since COVID-19. Black women had the highest maternal mortality rate across racial and ethnic groups between 2018 and 2022 and also experienced the largest increase during the pandemic (Figure 2). Maternal mortality rates decreased significantly across most racial and ethnic groups between 2021 and 2022. This decline may reflect a return to pre-pandemic levels following the large increase in maternal death rates due to COVID-19 related deaths. Despite this decline, the U.S. has the highest maternal mortality rate among high-income countries and the maternal mortality rate for Black women remained over two and a half times as high as the rate for White women.
Birth Risks and Outcomes
Black, AIAN, and NHPI women are more likely than White women to have certain birth risk factors that contribute to infant mortality and can have long-term consequences for the physical and cognitive health of children. Preterm birth (birth before 37 weeks gestation) and low birthweight (defined as a baby born less than 5.5 pounds) are some of the leading causes for infant mortality. Receiving pregnancy-related care late in a pregnancy (defined as starting in the third trimester) or not receiving any pregnancy-related care at all can also increase the risk of pregnancy complications. Black, AIAN, and NHPI women have higher shares of preterm births, low birthweight births, or births for which they received late or no prenatal care compared to White women (Figure 3). Notably, NHPI women are four times more likely than White women to begin receiving prenatal care in the third trimester or to receive no prenatal care at all (22% vs. 5%). Black women also are nearly twice as likely compared to White women to have a birth with late or no prenatal care compared to White women (10% vs. 5%).
While teen birth rates overall have declined over time, they are higher among Black, Hispanic, AIAN, and NHPI teens compared to their White counterparts (Figure 4). In contrast, the birth rate among Asian teens is lower than the rate for White teens. Many teen pregnancies are unplanned, and pregnant teens may be less likely to receive early and regular prenatal care. Teen pregnancy also is associated with increased risk of complications during pregnancy and delivery, including preterm birth. Teen pregnancy and childbirth can also have social and economic impacts on teen parents and their children, including disrupting educational completion for the parents and lower school achievement for the children. The drivers of teen pregnancy are multi-faceted and include poverty, history of adverse childhood events, and access to comprehensive education and health care services. Research studies have found that increased use of contraception as well as support for comprehensive sex education have helped lower the rate of teen births nationally.
Reflecting these increased risk factors, infants born to AIAN, Hispanic, Black, and NHPI women are at higher risk for mortality compared to those born to White women. Infant mortality is defined as the death of an infant within the first year of life, but most cases occur within the first month after birth. The primary causes of infant mortality are birth defects, preterm birth and low birthweight, sudden infant death syndrome, injuries, and maternal pregnancy complications. Infant mortality rates have declined over time although there was a slight increase between 2021 and 2022 (5.4 vs. 5.6 per 1,000 births, respectively). However, disparities in infant mortality have persisted and sometimes widened for over a century, particularly between Black and White infants. As of 2022, infants born to Black women are over twice as likely to die relative to those born to White women (10.9 vs. 4.5 per 1,000), and the mortality rate for infants born to AIAN and NHPI women (9.1 and 8.5 per 1,000) is nearly twice as high (Figure 5). The mortality rate for infants born to Hispanic mothers is similar to the rate for those born to White women (4.9 vs. 4.5 per 1,000), while infants born to Asian women have a lower mortality rate (3.5 per 1,000). Data also show that fetal death or stillbirths—that is, pregnancy loss after 20-week gestation—are more common among NHPI, Black and AIAN women compared to White and Hispanic women. Moreover, causes of stillbirth vary by race and ethnicity, with higher rates of stillbirth attributed to diabetes and maternal complications among Black women compared to White women.
About one in five AIAN, Asian or Pacific Islander, and Black women report symptoms of perinatal depression compared to about one in ten White women (Figure 6). Hispanic women (12%) have similar rates of perinatal depression compared to their White counterparts (11%). Other research shows that the prevalence of postpartum depression has grown dramatically over the course of the past decade increasing from 9.4% in 2010 to 19.3% in 2021, driven by increases among Black and Asian and Pacific Islander women. Women of color experience increased barriers to mental health care and resources, along with racism, trauma and cultural barriers. Research suggests that perinatal mental health conditions are a leading underlying cause of pregnancy-related deaths and that individuals with perinatal depression are also at increased risk of chronic health complications such as hypertension and diabetes. Infants of mothers with depression are more likely to be hospitalized and die within the first year of life.
Factors Driving Disparities in Maternal and Infant Health
The factors driving disparities in maternal and infant health are complex and multifactorial. They include differences in health insurance coverage and access to care. However, broader social and economic factors and structural and systemic racism and discrimination also play a major role (Figure 7). In maternal and infant health specifically, the intersection of race, gender, poverty, and other social factors shapes individuals’ experiences and outcomes. Recently there has been broader recognition of the principles of reproductive justice, which emphasize the role that the social determinants of health and other factors play in reproductive health for communities of color. Notably, Hispanic women and infants fare similarly to their White counterparts on many measures of maternal and infant health despite experiencing increased access barriers and social and economic challenges typically associated with poorer health outcomes. Research suggests that this finding, sometimes referred to as the Hispanic or Latino health paradox, in part, stems from variation in outcomes among subgroups of Hispanic people by origin, nativity, and race, with better outcomes for some groups, particularly recent immigrants to the U.S. However, the findings still are not fully understood.
Disparities in maternal and infant health, in part, reflect increased barriers to care for people of color. Research shows that coverage before, during, and after pregnancy facilitates access to care that supports healthy pregnancies, as well as positive maternal and infant outcomes after childbirth. Overall, people of color are more likely to be uninsured and face other barriers to care. Medicaid helps to fill these coverage gaps during pregnancy and for children, covering more than two-thirds of births to women who are Black or AIAN. However, AIAN, Hispanic, and Black people are at increased risk of being uninsured prior to their pregnancy, which can affect access to care before pregnancy and timely entry to prenatal care. Beyond health coverage, people of color face other increased barriers to care, including limited access to providers and hospitals and lack of access to culturally and linguistically appropriate care. Several areas of the country, particularly in the South have gaps in obstetrics providers. AIAN women also are more likely to live in communities with lower access to obstetric care. These challenges may be particularly pronounced in rural and medically underserved areas. For example, research suggests that closures of hospitals and obstetric units in rural areas has a disproportionate negative impact on Black infant health.
Research also highlights the role racism and discrimination play in driving racial disparities in maternal and infant health. Research has documented that social and economic factors, racism, and chronic stress contribute to poor maternal and infant health outcomes, including higher rates of perinatal depression and preterm birth among Black women and higher rates of mortality among Black infants. In recent years, research and news reports have raised attention to the effects of provider discrimination during pregnancy and delivery. News reporting and maternal mortality case reviews have called attention to a number of maternal and infant deaths and near misses among women of color where providers did not or were slow to listen to patients. A recent report determined that discrimination, defined as treating someone differently based on the class, group, or category they belong to due to biases, stereotypes, and prejudices, contributed to 30% of pregnancy-related deaths in 2020. In one study, Black and Hispanic women reported the highest rates of mistreatment (such as shouting and scolding, ignoring or refusing requests for help during the course of their pregnancy). Even controlling for insurance status, income, age, and severity of conditions, people of color are less likely to receive routine medical procedures and experience a lower quality of care. A 2023 KFF survey found that about one in five (21%) Black women say they have been treated unfairly by a health care provider or staff because of their racial or ethnic background. A similar share (22%) of Black women who have been pregnant or gave birth in the past ten years say they were refused pain medication they thought they needed.
Efforts to Address Maternal and Infant Health Disparities
Increased awareness and attention to maternal and infant health have contributed to a rise in efforts and resources focused on improving health outcomes and reducing disparities. These include efforts to expand access to coverage and care, increase access to a broader array of services and providers that support maternal and infant health, diversify the health care workforce, and enhance data collection and reporting.
Since the launch of the White House Blueprint for Addressing the Maternal Health Crisis in 2022, there has been a variety of actions and investments across federal agencies to improve maternal health. The Biden-Harris Administration’s Blueprint focuses on increasing coverage for perinatal services, improving data collection and analysis, expanding the maternity workforce, strengthening social supports, and improving patient-provider relations. Federal initiatives have included a pilot project with distribution of newborn supply kits, a $27.5 million program for specialized maternity care training to over 2,000 OB/GYNs, nurses, and other providers. In March 2024, the Biden Administration issued a new Executive Order to advance women’s health research and innovation, including support to fund research to identify warning signs of maternal morbidity and mortality among Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) recipients. The Office of Intergovernmental and External Affairs (IEA) and the March of Dimes have created a public-private partnership, Maternal Health Collaborative to Advance Racial Equity, to improve maternal health outcomes among Black mothers. Additionally, the Biden-Harris Administration recently launched the Expanding Access to Women’s Health grant program, which will provide funding to 14 states and the District of Columbia to address disparities in maternal health outcomes with an emphasis on improving access to reproductive and maternal health coverage and services.
Nearly all states have expanded access to Medicaid coverage during the postpartum period, helping to stabilize coverage. Medicaid covers four in ten births nationally. However, historically, many pregnant women lost coverage at the end of a 60-day postpartum coverage period because eligibility levels are lower for parents than pregnant women in many states, particularly those that have not implemented the ACA Medicaid expansion. The American Rescue Plan Act (ARPA) of 2021 initially provided states a new option to extend postpartum coverage to a full year beginning April 1, 2022. As of August 1, 2024, 47 states, including DC, had implemented a 12-month postpartum coverage extension, with additional states planning to implement the extension. KFF analysis suggests that the coverage extension could prevent hundreds of thousands of enrollees from losing coverage in the months after delivery. Additional actions to expand coverage may also help to reduce disparities, including adoption of the ACA Medicaid expansion in the ten remaining states that have not yet expanded, as nearly six in ten adults in the coverage gap in these states are adults of color, and Medicaid expansion promotes continuity of coverage in the prenatal and postpartum periods.
In addition, many state Medicaid programs have implemented policies, programs, and initiatives to improve maternity care and outcomes. This includes outreach and education to enrollees and providers about maternal health issues; expanding coverage for benefits such as doula care, home visits, and substance use disorder and mental health treatment; and using new payment, delivery, and performance measurement approaches. For example, Ohio’s Comprehensive Maternal Care program aims to develop community connections and culturally aligned supports for women with Medicaid as they and their families navigate pre- and post-natal care. Participating obstetrical practices are required to measure and engage with patients and families to hear firsthand accounts of how access to care, cultural competence, and communication methods affect patient outcomes. Some states also are leveraging managed care contracts to require Medicaid plans to develop an explicit focus on reducing disparities related to maternal and child health .
Implementation of evidence-based best practices may help to improve maternal and infant health outcomes. As part of its maternity care action plan, CMS has launched a “Birthing-Friendly” hospital designation to provide public information on hospitals that have implemented best practices in areas of health care quality, safety, and equity for pregnant and postpartum patients. Currently, more than 2,200 hospitals nationwide have received the “Birthing Friendly” designation, however, some argue that additional quality metrics and efforts are needed to improve the impact and utility of this designation. CMS is also proposing new baseline health and safety requirements for hospitals, including topics related to delivery of care in obstetric units, staffing, and annual training on evidence-based maternal health practice and cultural competencies. Moreover, in 2024, CMS has launched a new effort within its maternal and infant health initiative to focus on maternal mental health, substance use, and hypertension management.
Some states include a focus on equity as part of their Maternal Mortality Review Committee (MMRC). Nearly all states have an MMRC that reviews pregnancy associated deaths and offers recommendations to prevent future deaths. However, state MMRCs vary in how they examine racial disparities, with some specifying identifying and addressing disparities as a key focus. Beginning in 2020, discrimination was added to the list of circumstances surrounding a pregnancy-related death that can be reported by MMRCs. For example, in California, each death is examined through a health equity lens and considerations include how social determinants of health, discrimination, and racism may have contributed to the death. Similarly, Vermontamended the charge of its committee in 2020 to include considerations of disparities and social determinants of health, including race and ethnicity in perinatal death reviews. States also vary in the membership of their committees, with some having requirements related to Tribes and doulas or midwives. Washington, Montana and Arizona are examples of states that have a Native or Tribal Government representative, while Oregon and Louisiana have doula representation, and Vermont and Pennsylvania have midwife representation on their MMRCs.
A variety of efforts are underway to increase workforce diversity and expand access to doula services to improve maternal and infant health outcomes and reduce disparities. Studies have shown that a more diverse healthcare workforce and the use of midwives and doulas may improve birth outcomes. Midwives are an important component of the health care workforce, attending approximately one in ten births in 2021. Midwife-attended births are associated with fewer medical interventions, and there are efforts to grow and diversify the midwifery workforce to help improve maternal health outcomes and reduce mortality and morbidity.
The percent of maternal health physicians and registered nurses that are Hispanic or Black is lower than their share of the female population of childbearing age. The Biden Administration’s Blueprint includes efforts by HRSA to provide scholarships to students from underrepresented communities in health professions and nursing schools to grow and diversify the maternal care workforce.
Expanding access to doula services is another approach to increase diversity and expand the maternal health workforce. Doulas are trained non-clinicians who assist a pregnant person before, during and/or after childbirth by providing physical assistance, labor coaching, emotional support, and postpartum care. People who receive doula support have been found to have shorter labors and lower C-section rates, fewer birth complications, are more likely to initiate breastfeeding, and their infants are less likely to have low birth weights. The HHS FY2025 budget directs $5 million towards growing and diversifying the doula workforce and $5 million towards addressing emerging issues and social determinants of maternal health. Additionally, in recent years, there has been growing interest in expanding coverage of doula services through Medicaid. The MOMNIBUS is federal legislation that has been introduced to address maternal health disparities, and proposes to expand access to coverage of midwife and doula services. Some states are taking steps to include coverage through their state programs. As of early February 2024, 12 states reimburse services provided by doulas under Medicaid (CA, DC, FL, MD, MI, MN, NV, NJ, OK, OR, RI, VA), with two states, Louisiana and Rhode Island, also implementing private coverage of doula services. Some states also are seeking to increase access to these providers by providing patient education about these services, supporting training and credentialing of these providers, and raising reimbursement rates.
Some states are seeking to improve access to culturally responsive maternal and childcare through community engagement and collaboration with community stakeholders. For example, as part of its Birth Equity Project, Washington held listening sessions with Black, immigrant, and Indigenous families and birth workers to understand the challenges to birth equity in the state. In 2021 and 2022, Utah conducted the Embrace Project Study to reduce disparities among NHPI women by providing culturally responsive health services, with a focus on mental health and self-care practices rooted in ancestral NHPI cultural traditions. California has a Black Infant Health Program that includes empowerment-focused group support services and client-centered life planning to improve the health and social conditions for Black women and their families. Arizona hosts a maternal and infant mortality summit which brings together stakeholders to discuss how to improve equity and a Tribal maternal task force that develops a Tribal maternal health strategic plan and provides training about maternal health and family wellness from an Indigenous perspective.
A range of organizations are advocating for more interventions and support to address maternal mental health and substance use issues, major causes of pregnancy-related mortality and morbidity. Some studies have found higher rates of postpartum depression among some pregnant and postpartum women of color, but many mental health conditions are undiagnosed and untreated due to stigma and poor access to treatment. These issues also limit access to services for pregnant and postpartum people with substance use disorders. Additionally, some states have laws that take a punitive approach toward substance use during pregnancy, which may discourage some, particularly people of color, from seeking care. Community-based and provider organizations are calling for a number of policy and structural changes to address these challenges, including broader insurance coverage for behavioral health care, higher reimbursement for existing treatment services, greater education and awareness about screening for mental health and substance use conditions among health care providers and childbearing people. Federal initiatives in this area include the launch of the National Maternal Mental Health Hotline by HRSA to provide support, resources and referrals to new mothers and their families.
Looking Ahead
Improving maternal and infant health is key for preventing unnecessary illness and death and advancing overall population health. Healthy People 2030, which provides 10-year national health objectives, identifies the prevention of pregnancy complications and maternal deaths and improvement of women’s health before, during, and after pregnancy as a public health goal. Further, the National Institutes of Health (NIH) Pathways to Prevention panel recently recommended a “maternal mortality moonshot” with a goal of reducing preventable maternal mortality by 50% and eliminating racial disparities within the next 10 years.
While there are a range of efforts underway to reduce disparities in maternal and infant health, state abortion bans and restrictions may exacerbate poor maternal and infant health outcomes and access to care. Since the Dobbs ruling in June 2022, about half of states have banned abortion or restricted it to early in pregnancy. People of color are disproportionately affected by these bans and restrictions as they are at higher risk for pregnancy-related mortality and morbidity, are more likely to obtain abortions, and more likely to face structural barriers that make it more difficult to travel out of state for an abortion. There are many documented cases of people being forced to continue pregnancies that are endangering their lives because they could not obtain abortion care, and the recent deaths of two pregnant women in Georgia were attributed directly to delays in pregnancy termination. State-level bans and restrictions criminalize clinicians who provide abortion care which also has cascading effects on other aspects of maternity care, and as a result some clinicians are choosing not to practice in these states, potentially widening existing clinician shortages. Research also suggests that rates of infant mortality have increased since the Dobbs ruling.
The outcome of the presidential election also could have important implications for disparities in maternal and infant health. While both candidates have taken actions focused on improving maternal health, former President Trump and Vice President Harris have widely differing records and proposals related to health coverage and health. Vice President Harris has been an outspoken advocate for eliminating maternal health disparities and promoting access to abortion and contraception services in addition to maternity care for all. Trump expresses his support for letting states set their own abortion policy, which can limit the availability of other related services, including maternity care.
Health insurance is expensive and can be difficult to afford for people with lower or moderate incomes. In response, the Affordable Care Act (ACA) provides sliding-scale subsidies that lower premiums and insurers offer plans with reduced out-of-pocket (OOP) costs for eligible individuals.
This brief provides an overview of the financial assistance provided under the ACA for people purchasing coverage on their own through health insurance Marketplaces (also called exchanges).
Health Insurance Marketplace Subsidies
There are two types of financial assistance available to Marketplace enrollees. The first type, called the premium tax credit, reduces enrollees’ monthly payments for insurance coverage. The second type of financial assistance, the cost sharing reduction (CSR), reduces enrollees’ deductibles and other out-of-pocket costs when they go to the doctor or have a hospital stay. To receive either type of financial assistance, qualifying individuals and families must enroll in a plan offered through a health insurance Marketplace.
Premium Tax Credit
Premium tax credits can be applied to Marketplace plans in any of four “metal” levels of coverage: bronze, silver, gold, and platinum. Bronze plans tend to have the lowest premiums but have the highest deductibles and other cost sharing, leaving the enrollee to pay more out-of-pocket when they receive covered health care services, while platinum plans have the highest premiums but very low out-of-pocket costs.
Also offered on the Marketplace are catastrophic health plans with even lower premiums and higher cost sharing compared to bronze plans. Catastrophic plans are generally only available to individuals younger than 30, and premium tax credits cannot be applied to these plans.
Who is eligible for the premium tax credit?
To receive a premium tax credit for 2025 coverage, a Marketplace enrollee must meet the following criteria:
Have a household income at least equal to the Federal Poverty Level (FPL), which for the 2025 benefit year will be determined based on 2024 poverty guidelines (Table 1).
Not have access to an employer plan (including a family member’s employer) that both meets minimum value and is considered affordable. For 2025, the threshold that determines if an employer plan is affordable is if the premium is equal to or less than 9.02 percent of one’s household income.
Not be eligible for coverage through Medicare, Medicaid, or the Children’s Health Insurance Program (CHIP).
Have U.S. citizenship or proof of legal residency. (Lawfully present immigrants whose household income is below 100 percent FPL can also be eligible for tax subsidies through the Marketplace if they meet all other eligibility requirements.)
If married, must file taxes jointly.
Income: For the purposes of the premium tax credit, household income is defined as the Modified Adjusted Gross Income (MAGI) of the taxpayer, spouse, and dependents who are required to file a tax return. The MAGI calculation includes income sources such as wages, salary, foreign income, interest, dividends, and Social Security.
Employer coverage: Employer coverage is considered affordable if the required premium contribution is no more than 9.02 percent of household income in 2025. The Marketplace will look at both the required employee contribution for self-only and (if applicable) for family coverage. If the required employee contribution for self-only coverage is affordable, but the required employee contribution is more than 9.02 percent of household income for family coverage, the dependents can purchase subsidized exchange coverage while the employee stays on employer coverage.
The employer’s coverage must also meet a minimum value standard that requires the plan to provide substantial coverage for physician services and for inpatient hospital care with an actuarial value of at least 60 percent (meaning the plan pays for an average of at least 60 percent of all enrollees’ combined health spending, similar to a bronze plan). The plan must also have an annual OOP limit on cost sharing of no more than $9,200 for self-only coverage and $18,400 for family coverage in 2025.
People who are offered employer-sponsored coverage that fails to meet either the affordability threshold or minimum value requirements can qualify for Marketplace subsidies if they meet the other criteria listed above.
Eligibility for Medicaid: In states that have expanded Medicaid under the ACA, adults earning up to 138 percent FPL are generally eligible for Medicaid and not for Marketplace subsidies. In states that have not adopted Medicaid expansion, adults with income as low as 100 percent FPL can qualify for Marketplace subsidies. However, those with incomes lower than 100 percent FPL are generally not eligible for tax credits or Medicaid unless they meet other state eligibility criteria. KFF estimates that 1.5 million Americans living in non-expansion states fall into this coverage gap.
Certain lawfully present immigrants are exempt from the rule restricting tax credit eligibility for adults below the poverty level. Other federal rules restrict Medicaid eligibility for lawfully present immigrants, other than pregnant women, refugees, and asylees, until they have resided in the U.S. for at least five years. Immigrants who would otherwise be eligible for Medicaid but have not yet completed their five-year waiting period may instead qualify for tax credits through the Marketplace. If an individual in this circumstance has an income below 100 percent of poverty, for the purposes of tax credit eligibility, his or her income will be treated as though it is equal to the poverty level. Exceptions are also made for Deferred Action for Childhood Arrivals (DACA) recipients, who became newly eligible for Marketplace coverage after the Biden-Harris administration passed new regulations in May 2024 expanding the definition of lawfully present to include DACA recipients. Immigrants who are not lawfully present are ineligible to enroll in health insurance through the Marketplace, receive tax credits through the Marketplaces, or enroll in non-emergency Medicaid and CHIP.
What amount of premium tax credit is available?
The premium tax credit limits an individual’s contribution toward the premium of the “benchmark” plan, the second-lowest cost silver plan in their Marketplace. This “required individual contribution” is set on a sliding income scale. In 2025, for individuals with income up to 150 percent FPL, the required contribution is zero, while at an income of 400 percent FPL or above, the required contribution is 8.5 percent of household income (Table 2). Individuals making above 400 percent FPL whose required contribution for a benchmark silver premium is greater than the actual cost of a benchmark silver plan relative to their household income would be ineligible for subsidies.
These contribution amounts were set by the American Rescue Plan Act (ARPA) and later temporarily extended by the Inflation Reduction Act (IRA). Prior to the ARPA, the required contribution percentages ranged from about two percent of household income for people with poverty level income to nearly 10 percent of household income for people with income from 300 to 400 percent FPL. In addition, prior to the ARPA, people with incomes above 400 percent FPL were not eligible for premium tax credits.
The amount of tax credit is calculated by subtracting the individual’s required contribution from the actual cost of the “benchmark” plan. So, for example, if the benchmark plan costs $6,000 annually, the required contribution for someone with an income of 150 percent FPL ($22,590 in 2025) is zero, resulting in an annual premium tax credit of $6,000. If that same person’s income equals 250 percent FPL (or $37,650 in 2025), the individual contribution is four percent of $37,650, or $1,506 per year, resulting in an annual premium tax credit of $4,494.
The premium tax credit can then be applied toward any other plan sold through the Marketplace (except Catastrophic coverage). The amount of the tax credit remains the same, so a person who chooses to purchase a plan that is more expensive than the benchmark plan will have to pay the difference in cost. Conversely, if a person chooses a less expensive plan, such as the lowest-cost silver plan or a bronze plan, the tax credit will cover a greater share of that plan’s premium, and possibly even cover the entire cost, leaving the consumer with a zero-premium plan. When the tax credit exceeds the cost of a plan, it lowers the premium to zero and any remaining tax credit amount is unused.
For certain components of a Marketplace plan premium, the premium tax credit will not apply. First, the tax credit cannot be applied to the portion of a person’s premium attributable to covered benefits that are not essential health benefits (EHB). For example, a plan may offer adult dental benefits, which are not currently included in the definition of EHB. In that case, the person would have to pay the portion of the premium attributable to adult dental benefits without financial assistance. In addition, the ACA prohibits applying premium tax credits to the portion of premiums covering “non-Hyde” abortion benefits. Marketplace plans that cover abortion are required to charge a separate $1 monthly premium to cover the cost of this benefit; this means a consumer who is otherwise eligible for a fully subsidized, zero-premium policy would still need to pay $1 per month for a policy that covers abortion benefits. Finally, if the person smokes cigarettes and is charged a higher premium for smoking, the premium tax credit is not applied to the portion of the premium that is the tobacco surcharge.
How do people receive the premium tax credit?
To receive the premium tax credit, people must apply for coverage through the Marketplace and provide information about their age, address, household size, citizenship status, and estimated income for the coming year. After submitting the application, people will receive a determination letting them know the amount of premium tax credit for which they qualify. The consumer then has the option to have the tax credit paid in advance, claim it later when they file their tax return, or some combination of the two options.
The advanced premium tax credit (APTC) option allows consumers to have 1/12 of their tax credit paid directly to their Marketplace plan insurer each month, reducing the monthly amount the consumer owes. However, because the APTC eligibility determination is based on estimated income, the enrollee is required to reconcile their APTC at tax time the following year, once they know what their actual income was. For people receiving an advanced payment of the premium tax credit in 2025, the reconciliation would occur when they file their 2025 tax return in 2026. If the consumer overestimated their income when they applied, they can receive the unclaimed premium tax credit as a refundable tax credit when they file. If the consumer underestimated their income at the time of application and excess APTC was paid on their behalf during the year, they would have to repay some or all of the excess tax credit when they file. There are maximum repayment limits which vary depending on income, shown in Table 3.
Alternatively, people can opt to pay their entire premium costs each month and wait to receive their tax credit until they file their annual income tax return the following year, although most Marketplace participants cannot afford this option. The premium tax credit is refundable, meaning it is available to qualifying enrollees regardless of whether they otherwise owe any federal income tax. Everyone who receives an APTC in a tax year is required to file a tax return for that year in order to continue receiving financial assistance in the future. People who fail to file and reconcile for two consecutive years will be ineligible for premium tax credits the following year.
Cost Sharing Reduction
The second form of financial assistance available to Marketplace enrollees is a cost sharing reduction. Cost sharing reductions lower enrollees’ out-of-pocket cost due to deductibles, copayments, and coinsurance when they use covered health care services.
Who is eligible for the cost sharing reduction?
People eligible for premium tax credits and have household incomes between 100 to 250 percent of poverty are eligible for cost sharing reductions.
How are cost sharing reductions provided?
Unlike the premium tax credit (which can be applied toward any metal level of coverage), cost sharing reductions (CSR) are only offered through silver plans. For eligible individuals, cost sharing reductions are applied to a silver plan, essentially making deductibles and other cost sharing under that plan more similar to that under a gold or platinum plan. Individuals with income between 100 and 250 percent FPL can continue to apply their premium tax credit to any metal level plan, but they can only receive plans with reduced cost sharing if they pick a silver-level plan.
What amount of cost sharing reductions are available to people?
Cost sharing reductions are determined on a sliding scale based on income. The most generous cost sharing reductions are available for people with income between 100 and 150 percent FPL. For these enrollees, silver plans that otherwise typically have higher cost sharing are modified to be more similar to a platinum plan by substantially reducing the silver plan deductibles, copays, and other cost sharing. For example, in 2024, the average annual deductible under a silver plan was just over $5,000, while the average annual deductible under a platinum plan was $97. Silver plans with the most generous level of cost sharing reductions are sometimes called CSR 94 silver plans (with 94 percent actuarial value, which represents the average share of health spending paid by the health plan, compared to 70 percent actuarial value for a silver plan with no cost sharing reductions).
Somewhat less generous cost sharing reductions are available for people with incomes above 150 and up to 200 percent FPL. These reduce cost sharing under silver plans to 87 percent actuarial value (CSR 87 plans). In 2024, the average annual deductible under a CSR 87 silver plan was about $700.
For people with incomes above 200 and up to 250 percent FPL, cost sharing reductions are available to modestly reduce deductibles and copays to 73 percent actuarial value (sometimes called CSR 73 plans). In 2024, the average annual deductible under a CSR 73 silver plan was about $4,500.
Insurers have flexibility in how they set deductibles and copays to achieve actuarial value benchmarks set by the ACA for Marketplace plans, including CSR plans, so actual deductibles may vary from these averages.
The ACA also requires maximum annual out-of-pocket spending limits on cost sharing under Marketplace plans, with reduced limits for CSR plans. In 2025, the maximum OOP limit will be $9,200 ($18,400 family) for all QHPs with lower maximum OOP limits permitted under cost sharing reduction plans (Table 4).
This brief was updated on October 24, 2024 to incorporate updates to Medicare and Medicaid administrative data.
In 2021, 13 million people under age 65 received income from the Social Security disability programs, Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI), which provide monthly income to people who are unable to work on account of a disability. A less-commonly appreciated benefit of qualifying for Social Security disability programs is the connection to health insurance coverage through Medicare or Medicaid. In most states, SSI beneficiaries automatically qualify for and receive Medicaid coverage, while SSDI beneficiaries qualify for Medicare after receiving disability benefits for at least two years. Many who receive benefits from the SSDI and SSI programs also qualify for both Medicare and Medicaid, known as dual-eligible individuals.
This analysis examines enrollment in disability programs and characteristics of enrollees from 2002-2022 Social Security Administration data and related health coverage through the Medicare and Medicaid programs using data from the Centers for Medicare and Medicaid Services for 2021, the most recent year of data available. (See methods for details.) State-level data about the disability programs are also available on KFF’s State Health Facts.
Key Takeaways
In 2021, 12.9 million people were eligible for Medicare or Medicaid because they received disability benefits from either SSDI or SSI. Of that total, 4.6 million, or more than one-third (35%), qualified for health coverage under both Medicare and Medicaid (dual-eligible individuals). Another 4.8 million SSI beneficiaries had Medicaid coverage only and 3.5 million SSDI beneficiaries had Medicare coverage only.
A total of 13.0 million people under age 65, including working-age adults and children, received disability benefits in 2022, including 7.8 million people who received income from SSDI, 4.2 million who received income from SSI, and 1 million who received income from both programs.
Enrollment of working-age adults in both the SSDI and SSI programs has decreased since 2014, reflecting the changing demographics of the U.S. population, the economy, and other factors that have reduced the number of new beneficiaries, including in more recent years, the lasting effects of Social Security office closures during the COVID-19 pandemic. The decline in SSDI enrollment has also meant a decline in the number of Medicare beneficiaries under age 65 who qualify due to disability.
Mental disorders—which include intellectual and developmental disorders and other mental disorders—comprise the largest percentage of disabling conditions across both programs. In the SSDI program, musculoskeletal conditions are the most common disabling conditions among disabled beneficiaries (30%), followed by other mental disorders (16%) and intellectual/developmental disorders (14%). For SSI beneficiaries, intellectual and developmental disorders are the most common disabling conditions (33%), followed by other mental disorders (19%) and musculoskeletal disorders (12%).
The average monthly benefit in 2022 was more than twice as large for disabled workers in the SSDI program (nearly $1,500 per month) than disabled beneficiaries in the SSI program (nearly $650 per month).
How many people under age 65 qualify for Medicaid and Medicare through the Social Security disability programs?
In 2021, 12.9 million people who received benefits through the Social Security disability programs qualified to receive coverage from Medicare, Medicaid, or both programs on account of their eligibility for disability benefits (Figure 1). While 61% of working age adults and nearly half of children had health coverage through an employer in 2022, employment-based coverage is much less common among people with disabilities, who are less likely to work. As a result, the Social Security disability programs – Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI) (see Box 1) – play an important role in helping people with disabilities access health insurance coverage through the Medicaid or Medicare programs, with some people with disabilities qualifying for health coverage under both Medicare and Medicaid (known as dual-eligible individuals).
Of the 12.9 million people with disabilities who have coverage from Medicare, Medicaid, or both based on their eligibility for disability programs, a total of 4.6 million, or more than one-third (35%), are dual-eligible individuals. Overall, the overall group includes:
4.8 million SSI beneficiaries who have Medicaid only;
3.5 million SSDI beneficiaries who have Medicare only;
3.0 million SSDI beneficiaries who have both Medicare and Medicaid; and
1.6 million beneficiaries receiving both SSDI and SSI, who have both Medicare (through SSDI) and Medicaid (through SSI).
Although most people qualify for Medicare based on age when they turn 65, people under age 65 may become eligible for Medicare if they have received SSDI payments for 24 months. In 2021, 8.3 million people under the age of 65 were eligible for Medicare because of a disabling condition. Nearly all (8.1 million) were eligible through SSDI, and 0.2 million were eligible because they had End-Stage Renal Disease (ESRD) but did not receive SSDI. SSDI beneficiaries often must wait 5 months for SSDI payments after the onset of benefits, followed by a two-year waiting period between receipt of SSDI benefits and Medicare eligibility, referred to as the “Medicare waiting period.” It is unknown how many people are currently in the waiting period or what their health insurance coverage is during this period. Because of the length of the SSDI application process and the fact that SSDI eligibility is retroactive, applicants may complete some or all of the waiting period prior to receiving SSDI benefits, but many experience gaps in coverage during this time too. (Those under age 65 who qualify for Medicare based on having ESRD or Amyotrophic Lateral Sclerosis (ALS) do not have to wait 24 months for their Medicare benefits to start because they are not required to qualify for SSDI first.)
According to KFF analysis, although majorities of people with Medicare of all ages rate Medicare positively, people under age 65 with disabilities are less likely than older beneficiaries to give positive ratings to Medicare and some features of it, such as the quality and availability of providers. Medicare beneficiaries under age 65 with disabilities have also reported worse access to care, more cost concerns, and lower satisfaction with care than those age 65 or older. The lower ratings by people under 65 with disabilities may possibly be related to their different pathways to Medicare eligibility and because the program was originally designed to cover older adults, with coverage for younger people with disabilities added later. Also, because a larger share of people with Medicare under 65 with disabilities report that they are in fair or poor physical and mental health and have severe chronic conditions compared to people age 65 or older, those under 65 with disabilities may be more likely to have multiple encounters with the health care system during the year and encounter problems when they do.
States must generally provide Medicaid to people who receive SSI. In 2021, 6.5 million people were eligible for Medicaid through the SSI disability program. If states do not want to use the SSI eligibility criteria, they can use more restrictive rules so long as the rules are no more restrictive than what the state had in place in 1972 when the SSI program was established. There are currently 8 states using their own criteria, known as the 209(b) states: Connecticut, Hawaii, Illinois, Minnesota, Missouri, New Hampshire, North Dakota, and Virginia.
Box 1: What are the Differences Between SSDI and SSI?
Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI) are federal programs administered by the Social Security Administration (SSA), but they differ in terms of how people qualify, the benefits they receive, and how they are financed. Both programs require adults under age 65 to have a qualifying disability, but SSI also includes qualifying disability criteria for children.
How do people qualify for SSDI and SSI? To qualify for SSDI, enrollees must have a sufficient work history, which varies by age but generally requires ten years of employment at least five of which were within the past decade. Some individuals with a disability can qualify based on a relative’s work history including:
Spouses of disabled workers (and divorced spouses if the marriage lasted for at least 10 years) if they have a child in their care or if they are at least 63 years old; and
Children of disabled workers if they are under age 18, 18 years old but still in high school, or are adults who have disabilities that started under the age of 22.
SSI is a means-tested program in which eligibility is based on an assessment of income and resources. To qualify, SSI enrollees must have low incomes, limited assets, and either be over age 64 or have a qualifying disability. Unlike SSDI, SSI is available to people regardless of their work history. The SSA redetermines eligibility and benefit amounts for SSI beneficiaries every 1 to 6 years or when a change that affects eligibility or payment is reported.
What benefits do people receive and how are the programs financed? Under both programs, the federal government pays monthly benefits to people who meet the eligibility criteria, and 45 states add supplemental payments for some SSI recipients. Maximum monthly benefits for SSI are legislatively established and updated annually to reflect inflation. Monthly benefits for SSDI reflect the payments workers made into the program through payroll taxes and are updated annually based on the growth in average wages. There are no state supplemental payments for SSDI. People can receive both SSDI and SSI if the income from SSDI is less than the maximum SSI payment. In those cases, SSI can cover the difference between the SSDI income amount and the maximum SSI.
How many people under age 65 receive income from Social Security disability programs?
Among the 268 million people under age 65 in the U.S., 5% or 13 million people received income from SSDI, SSI, or both programs in 2022. More than half (60%, or 8 million) of Social Security disability program beneficiaries under 65 exclusively receive SSDI income, and nearly a third (32%, or 4 million) receive only SSI, while over 1 million people received benefits from both programs (Figure 2).
How has enrollment in the Social Security disability programs changed over time?
Enrollment of working-age adults in the Social Security disability programs increased from the early 2000s through 2014 but has been declining since (Figure 3). Enrollment of people under age 65 in SSDI and SSI has decreased from 14.9 million beneficiaries in 2014 to 13.0 million beneficiaries in 2022. Enrollment trends in the disability programs reflect the demographics of the U.S. population, the economy, and other factors. Program size depends in part on the size of the labor force, and some of the decreased participation in recent years reflects the baby boomers entering their retirement years. For the SSDI program, participation also requires people to meet past employment requirements and lower labor force participation means fewer people can meet those requirements. Research has also found lower application and award rates for “contingent workers,” which includes independent contractors, consultants, and those in temporary, on-call, and gig economy jobs, who make up an increasing share of the workforce. Lower SSDI enrollment over the past decade also likely reflects fewer applications stemming from the end of routinely-mailed social security statements in 2011.
More stringent disability determinations could also contribute to the lower enrollment. Between 1999 and 2019, the percentage of applicants who were approved to receive benefits (the “award rate”) declined for both disability programs: from 56% to 29% for SSDI and from 44% to 34% in 2021 for SSI. Lower award rates mean that even if a similar number of people apply, fewer people will enroll and receive benefits.
The decline in SSDI enrollment has meant fewer people under age 65 qualifying for Medicare due to having a long-term disability. The total number of Medicare beneficiaries under age 65 with disabilities (excluding those who qualify based on having end-stage renal disease) has declined since 2016, both in terms of the total number and the share of overall Medicare enrollment, based on Medicare enrollment data from the Centers for Medicare & Medicaid Services. In 2016, there were 8.6 million Medicare beneficiaries under age 65, or 16% of all beneficiaries, decreasing to 7.2 million in 2023, or 11% of the total.
The same trend is not observed in Medicaid because people have more options for qualifying for Medicaid than they do Medicare. Between 2014 and 2022, most states adopted Medicaid expansions under the Affordable Care Act, which provided another mechanism for adults under age 65 to qualify for Medicaid and spurred enrollment growth. Enrollment also grew between 2020 and 2023 because of the COVID-19 continuous enrollment period, a three-year period during which Medicaid eligibility disenrollments were paused.
Historically, economic downturns led to increases in SSDI and SSI enrollment, but notably, there was no enrollment surge during the economic downturn associated with the COVID-19 pandemic. In fact, the enrollment decline accelerated during the COVID-19 pandemic, when Social Security offices were closed for 2 years, likely further reducing the number of applicants. Office closures also contributed to a backlog of cases that is causing people to wait longer for eligibility decisions: Social Security data show that the average review time for initial applications increased from 4 months or less before the pandemic to nearly 8 months in 2023. Similar trends occurred for applications that were reconsidered after an initial denial.
The application for Social Security disability benefits can be a lengthy and complicated process, spanning months, if not years. A chart visualizing the steps to disability determinations in 2022 by the National Organization of Social Security Claimants’ Representatives shows that 62% of the 1.8 million applicants in 2022 were denied at the initial application, but that hundreds of thousands pursued reconsiderations and subsequent legal proceedings to establish eligibility. A 2022 study by the National Bureau of Economic Research found that legal representation did not affect the likelihood of a successful SSDI outcome but reduced the time it took for approval by nearly one year. The challenge with demonstrating eligibility is in proving that one has a disabling condition that makes substantive employment impossible.
The Biden-Harris Administration’s proposed FY 2025 budget includes a $1.3 billion (9%) increase to the Social Security Administration’s budget from FY 2023 to 2025 to improve customer service across field offices, disability determination, and teleservice, and reduce wait times. The Biden-Harris Administration also supports using the budget increase to advance equity and accessibility. The new funding would support simplifying the SSI application process, broadening access to Social Security programs especially for unserved populations, and preventing overpayments. The Social Security Administration would also use the funding to continue improving information technology systems to make accessing services and communication with staff easier both online and via phone.
What are the most common conditions that qualify people for Social Security disability benefits?
For both SSDI and SSI, musculoskeletal system diseases and mental disorders are the most common conditions that qualify people for disability benefits (Figure 4). Both Social Security disability programs use a strict definition of disability when assessing eligibility, which limits how many people with disabilities ultimately qualify for SSDI or SSI payments. The Social Security Administration defines disability for adults as the inability to engage in any “substantial gainful activity” because of one or more medically determinable physical or mental disabilities that are either expected to result in death or have lasted or are expected to last for a continuous period of at least 12 months. Substantial gainful activity describes a level of work that involves doing significant physical or mental activities or a combination of both. For children to qualify as disabled, they must be under 18 and have one or more physical or mental impairments which result in marked and severe functional limitations and the impairment must have lasted or be expected to last for at least 12 months or be expected to result in death.
Over the past two decades, musculoskeletal system diseases and mental disorders (including both intellectual and developmental disorders and other mental disorders) have accounted for the largest shares of disability determinations, and in 2022, these conditions combined account for 60% of disability determinations among SSDI beneficiaries and 64% among SSI beneficiaries. The most common conditions for SSDI beneficiaries are musculoskeletal system diseases, which include non-healing or complex fractures, abnormalities of major joints, and disorders of the spine. The most common conditions for SSI beneficiaries are intellectual/developmental disorders which include autism spectrum disorders and neurocognitive disorders. Other mental disorders include depressive, bipolar, and related conditions and schizophrenia spectrum and other psychotic disorders.
How much do Social Security disability program beneficiaries receive in monthly benefits?
SSDI beneficiaries receive average monthly benefits that are over twice as large as what SSI beneficiaries receive, with monthly SSDI payments for disabled workers averaging nearly $1,500 per month, compared with roughly $650 per month for people receiving SSI benefits (Figure 5). Family members of SSDI workers receive lower monthly benefits, on average: just under $900 for widowers and $1,000 for adult children. The monthly payment from SSDI is calculated using a statutory formula that accounts for people’s earnings and is designed to pay higher benefits to people with higher earnings but to replace a larger percentage of earnings for people with lower earnings. In 2022, SSDI benefits ranged from less than $600 to more than $3,000 each month. The maximum SSI benefit is set by Congress and in 2022 was $841 per month for an individual ($943 in 2024) and $1,261 for a couple ($1,415 in 2024). If people have non-SSI income, their SSI benefits are reduced by the amount of countable income.
Many beneficiaries are now facing benefit reductions on account of prior overpayments by the Social Security Administration, as reported by KFF Health News, but the Biden-Harris Administration is taking steps to limit the effects of benefit reductions. Each year, more than 2 million beneficiaries have been receiving notices that their disability benefits were overpaid and are being asked to repay the specific amounts within 30 days or have their monthly disability benefits reduced. In many cases, those payments had been made years earlier without the recipients’ knowledge. There have been overpayments in both programs, but they are more common in SSI because SSI eligibility and payment amounts change when recipients experience changes in income and assets.
From April through June 2024, new overpayment policies went into effect to address those benefit reductions, including:
Limiting the amount that can be withheld from a recipient’s monthly disability benefits (to adjust for overpayments) to no more than 10% of the recipient’s monthly benefits for SSI recipients and either 10% or $10 for SSDI recipients (whichever is greater), rather than withholding the entire amount,
Increasing the amount of time for recipients to repay the overpayment,
Making overpayment notices easier to understand,
Simplifying the waiver application for beneficiaries who meet repayment exemption criteria, and
Holding the Social Security Administration responsible for providing proof of overpayment rather than the beneficiary.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
Included Areas: The analysis includes data from the 50 states and Washington D.C. (excluding enrollees in the territories and foreign countries).
Included Beneficiaries: Beneficiaries of Social Security disability programs who are under age 65.
Disability Programs: Data on the Social Security disability programs come from the Annual Statistical Report on the Social Security Disability Insurance Program, 2002-2022; and the Supplemental Security Income Annual Statistical Report, 2002-2022. The numbers in the issue brief come from the online appendix tables.
Medicare and Medicaid Enrollment: Data are from a KFF analytic file that merged the Centers for Medicare & Medicaid Services Chronic Conditions Data Warehouse 2021 research-identifiable Master Beneficiary Summary File (MBSF) Base and the 2021 Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) Research Identifiable Files (RIF) file using a Chronic Conditions Warehouse (CCW) beneficiary identifier crosswalk. The numbers include all Medicare enrollees who were currently eligible for Medicare on the basis of disability using ENTLMT_RSN_ORIG with values of 1, 3 and under 65 using AGE_AT_END_REF_YR in 2021, and all Medicaid enrollees who were currently eligible for Medicaid on the basis of SSI enrollment using the monthly ELGBLTY_GRP_CD with values of 11-22, 37, 38, 40, 41 and under 65 using AGE in 2021. People with records in both the Medicare and Medicaid data were categorized as dual-eligible beneficiaries.
Limitations: The estimates for SSDI and SSI enrollment are not comparable to the estimates of SSI and SSDI enrollees with Medicare and Medicaid coverage in 2021 for several reasons:
The data come from different sources and years.
The SSDI and SSI numbers are in the month of December whereas the Medicare and Medicaid numbers are people who were ever enrolled during the year.
Some people who are eligible for Medicare or Medicaid in a given month because of SSDI or SSI may not be receiving benefits from those programs in that month, particularly, if they are enrolled in certain programs designed to help people with disabilities work. This may be especially true between the years of 2020 and 2023 because states did not disenroll people during that time period on account of a continuous enrollment provision.
Some people who are receiving SSDI or SSI in a given month may not be receiving Medicare or Medicaid. This occurs most frequently for people with SSDI who must receive two years of SSDI benefits before they become eligible for Medicare.
This brief was updated on October 24, 2024 to incorporate updates to Medicare and Medicaid administrative data.
Policymakers, researchers, and others have long called for reforms to improve the coordination of Medicare and Medicaid benefits for the people who receive health insurance coverage through both programs. People in this group, also known as dual-eligible individuals, have lower incomes, are more racially and ethnically diverse, and often face greater mental and physical health challenges than the general Medicare population. Dual-eligible individuals with full Medicaid benefits, who comprise most dual-eligible individuals, usually have Medicare benefits covered under traditional Medicare or Medicare Advantage and, separately, Medicaid benefits covered through Medicaid fee-for-service or Medicaid managed care (referred to here as Medicaid delivery systems). A small percentage of dual-eligible individuals have most of their Medicare and Medicaid benefits covered through a single plan or program.
Some have raised concerns that, for dual-eligible individuals, care is fragmented, and benefits are poorly coordinated across the Medicare and Medicaid programs, contributing to lower quality care and higher costs. There are concerns that separate coverage arrangements make it more difficult for dual-eligible individuals to navigate different coverage rules and provider networks. Over the years, there have been numerous efforts to increase the integration of benefits and financing for the dual-eligible population across the two programs, including the Financial Alignment Initiative authorized under the Affordable Care Act. A recent systematic review of arrangements that aim to integrate benefits and financing for the dual-eligible population found that evidence on care coordination and hospitalizations is inconclusive; health outcomes are mixed and vary by type of arrangement; and some arrangements are found to increase Medicare spending. These findings are consistent with a previous inventory of evaluations by the Medicaid and CHIP Payment and Access Commission (MACPAC), raising questions about how well this approach serves dual-eligible individuals or achieves savings.
There are several proposals in the current Congress to integrate coverage by enrolling all dual-eligible individuals in a single plan or program that provides both Medicare and Medicaid benefits, as well as additional funding and changes to financing for states that pursue integrated models of coverage. These proposals raise a number of questions for consideration, including how to establish integrated plans in places without health plans experienced in providing Medicare and Medicaid benefits; how to minimize potential disruptions to existing care relationships; how to establish fair Medicare and Medicaid payments to the entities responsible for services; whether to provide dual-eligible individuals the option to get benefits under traditional Medicare, which does not have a limited network of providers; and to the extent private insurers administer these arrangements, how best to hold them accountable for improving care and lowering costs.
This analysis uses merged beneficiary-level Medicare and Medicaid data from 2021 – based on the most current final version of Medicaid data at the time of this analysis — to document sources of coverage for dual-eligible individuals nationwide and by state, which provides data useful for assessing the implications of potential proposals to change coverage arrangements for this population. The analysis includes 7.9 million dual-eligible individuals living in 47 states and the District of Columbia, who had full Medicaid benefits in March 2021 (referred to simply as dual-eligible individuals hereafter; see methods for further details).
Key Takeaways
The vast majority (95%) of full-benefit dual-eligible individuals received their Medicare and Medicaid benefits through separate Medicare and Medicaid coverage arrangements in 2021.
28% of dual-eligible individuals were in traditional Medicare and Medicaid fee-for-service;
23% were in traditional Medicare and Medicaid managed care; and
19% in Medicare Advantage and Medicaid fee-for-service.
24% were in Medicare Advantage and Medicaid managed care;
Just 5% of dual-eligible individuals received their Medicare and Medicaid benefits through a single coverage arrangement, either the Program of All-Inclusive Care for the Elderly (PACE) or a Medicare-Medicaid Plan (MMP).
Medicare and Medicaid coverage combinations for dual-eligible individuals varied widely across states. For example, in 18 states and DC, more than half of all dual-eligible individuals were in traditional Medicare and Medicaid fee-for-service, while in 4 states, more than half of all dual-eligible individuals were in Medicare Advantage and Medicaid managed care. Rhode Island and Ohio were the only states that had more than 25% of their dual eligible population in PACE or a Medicare-Medicaid Plan, while in 38 states and DC, fewer than 5% of the dual-eligible individuals were in these plans, in many cases, because they were not available.
Within Medicaid coverage arrangements, 55% of dual-eligible individuals were enrolled in multiple Medicaid delivery systems, which refers to the way a state Medicaid program provides benefits to enrollees. This occurs because states may offer limited benefit plans covering only a subset of Medicaid benefits, such as behavioral health or dental care, and they may exclude a subset of benefits from a larger managed care contract.
Within Medicare coverage arrangements:
28% of dual-eligible individuals received their Medicare benefits through a Medicare Advantage dual eligible special needs plan (D-SNP), though relatively few were enrolled in fully-integrated dual eligible special needs plans (FIDE SNPs), which generally offer a greater degree of coordination between Medicare and Medicaid than other types of D-SNPs.
12% of dual-eligible individuals were in traditional Medicare and aligned with a Medicare Shared Savings Program Accountable Care Organization (ACO), in which groups of doctors, hospitals and other health care providers form partnerships to collaborate and share accountability for the quality, coordination, and cost of care delivered to their patients.
How Did Dual-Eligible Individuals Receive Their Medicare and Medicaid Benefits in 2021?
Most (95%) dual-eligible individuals received Medicare and Medicaid benefits through separate coverage arrangements.
Existing coverage arrangements for dual-eligible individuals vary in how benefits are coordinated, and how plans and providers are paid. In all cases, Medicare serves as the primary payer and source of coverage, covering acute and post-acute care, while Medicaid pays Medicare premiums, and in most cases, cost-sharing. Full-benefit dual-eligible individuals are also eligible for Medicaid benefits that are not covered by Medicare, such as long-term care, vision, and dental benefits.
The most common coverage combination was traditional Medicare and Medicaid fee-for-service, accounting for 28% of dual-eligible individuals (Figure 1). In traditional Medicare and Medicaid fee-for-service, a mix of fee-for-service, bundled and prospective payments, as well as value-based payment models, such as accountable care organizations (ACOs), are used. In traditional Medicare, dual-eligible individuals may seek care from any provider that accepts Medicare (only a small share of providers opt out), with minimal constraints on health care use (such as prior authorization). However, in most states, there are policies that limit Medicaid payment of Medicare cost sharing so that total payment does not exceed the Medicaid rate, which is typically lower than the Medicare rate. This means providers in these states may be paid less to treat dual-eligible individuals than to treat other Medicare beneficiaries. Research shows that in those states, dual-eligible individuals have fewer primary care visits, suggesting that Medicare providers may be less willing to see dual-eligible individuals when they are paid less. For Medicaid covered services, dual-eligible individuals with Medicaid fee-for-service can see all providers that accept Medicaid in the state.
About one-quarter (24%) of dual-eligible individuals were in Medicare Advantage and Medicaid managed care. With this coverage combination, Medicare benefits are provided by Medicare Advantage plans and Medicaid benefits are provided by health plans that contract with state Medicaid programs. These entities receive set payments per enrollee, adjusted for health status, to incentivize care coordination. Plans can establish provider networks and use other tools to manage service utilization, including prior authorization.
About one-quarter (23%) of dual-eligible individuals were in traditional Medicare and Medicaid managed care. With this coverage combination, Medicare benefits are provided under traditional Medicare and Medicaid benefits are provided by health plans. Dual-eligible individuals can go to any provider that accepts dual-eligible individuals but may have to see a provider that is in network for Medicaid-covered services.
Just under one in five (19%) dual-eligible individuals were in Medicare Advantage and Medicaid fee-for-service. With this coverage combination, Medicare benefits are provided by Medicare Advantage plans and state Medicaid programs administer Medicaid benefits.
A small share (5%) of dual-eligible individuals were enrolled in a single plan or program that covered their Medicare and Medicaid benefits.
Medicare-Medicaid Plans and PACE are two models of coverage for dual-eligible individuals that provide Medicare and Medicaid benefits, including long-term services and supports, behavioral health services, and prescription drug coverage, under a single plan or program with integrated financing. Medicare-Medicaid Plans and PACE are not available in all areas, which helps to explain the relatively low enrollment in these coverage arrangements. Medicare-Medicaid Plans are a single plan that provide most Medicare and Medicaid benefits and were established as a demonstration under the Financial Alignment Initiative. They were offered in 9 states in 2021. PACE, a program that provides comprehensive medical and social services, was offered in a subset of counties across 31 states in 2021 (Appendix Table 1).
Evaluations of Medicare-Medicaid Plans and PACE have shown varied outcomes. Most evaluations of Medicare-Medicaid Plans found few measurable differences in health outcomes or spending. Many evaluations of PACE found improved outcomes, such as lower mortality and depression, but there is limited evidence on how the program affects Medicare and Medicaid spending.
Medicare and Medicaid coverage combinations for dual-eligible individuals varied widely across states.
In all states included in this analysis, most dual-eligible individuals received their Medicare and Medicaid benefits from separate coverage arrangements, though the distribution of the coverage combinations varied widely (Figure 2). (Note, Alabama, Arkansas, and Idaho were excluded from the below analysis due to missing or inconsistent data.)
The share of dual-eligible individuals in traditional Medicare and Medicaid fee-for-service (28% nationally) ranged from less than 1% in Tennessee, Nebraska, and Hawaii to over 50% in 18 states and DC.
The share of dual-eligible individuals in Medicare Advantage and Medicaid managed care (24% nationally) ranged from less than 1% in 18 states and DC to over 50% in Arizona, Hawaii, Pennsylvania, and Tennessee.
The share of dual-eligible individuals in traditional Medicare and Medicaid managed care (23% nationally) ranged from less than 1% in 19 states to over 50% in 6 states (Delaware, Iowa, Kansas, Nebraska, New Hampshire, and New Jersey).
The share of dual-eligible individuals in Medicare Advantage and Medicaid fee-for-service (19% nationally) ranged from less than 1% in Alaska, Hawaii, Iowa, Nebraska, and Tennessee to 52% in South Carolina and 54% in Georgia.
The share of dual-eligible individuals enrolled in a single coverage arrangement – Medicare-Medicaid Plans or PACE – (5% nationally) ranged from less than 1% in 32 states and DC to 28% in Ohio and 34% in Rhode Island. In 18 (including DC) of the 32 states and DC with low Medicare-Medicaid Plan and PACE enrollment, neither Medicare-Medicaid Plans nor PACE were available in any county.
Some states have worked to expand access to PACE in different areas and legislation has been proposed requiring all states to offer this program. The challenges in expanding PACE include high start-up costs, administrative barriers in reviewing applications for new programs and service area expansions, and limitations on federal and state resources.
In 20 states and DC, at least 80% of dual-eligible individuals were enrolled in Medicaid fee-for-service and in 14 states, at least 80% were enrolled in Medicaid managed care (Appendix Table 2). In the remaining 13 states, enrollment in Medicaid fee-for-service and managed care was more mixed. The tendency for most enrollees to be in either Medicaid managed care or fee-for-service within a given state reflects state decisions about whether to provide Medicaid benefits through managed care for dual-eligible individuals, and if so, whether enrollment is mandatory or voluntary. Among the states included in this analysis, 8 states did not enroll dual-eligible individuals in Medicaid managed care in 2021.
In 7 states, at least 80% of dual-eligible individuals were in traditional Medicare, and there were no states where at least 80% of dual-eligible individuals were enrolled in Medicare Advantage (Appendix Table 3). (Medicare Advantage enrollment is higher in Puerto Rico, which is not included in this analysis). The pattern of Medicare coverage for dual-eligible individuals is in part due to differences within states with respect to Medicare Advantage penetration. While some, mostly rural, states have low Medicare Advantage enrollment across the state, in most other states, Medicare Advantage penetration varies substantially across counties within the state. Counties with higher Medicare Advantage penetration and larger numbers of beneficiaries have the effect of boosting the state’s overall Medicare Advantage enrollment rate.
More than half of dual-eligible individuals were enrolled in multiple Medicaid delivery systems.
Within Medicaid, the way a state Medicaid program provides benefits to enrollees is sometimes referred to as a delivery system. State Medicaid programs may provide benefits on a fee-for-service basis, in which states reimburse health care providers a payment for each service, or through managed care, in which Medicaid pays a predetermined fee to another entity to deliver a specified set of benefits. Sometimes the set of benefits includes all Medicaid-covered services, but other times it is limited to a subset of benefits such as behavioral health, dental care, or long-term services and supports. As a result, enrollees in managed care may receive some services through the fee-for-service system or through limited benefit plans or carve-out plans that cover a small number of Medicaid benefits. Similarly, enrollees in Medicaid fee-for-service may receive a subset of their benefits through a limited benefit plan. To better understand how many delivery systems dual-eligible individuals enrolled in, this analysis counted the number of managed care plans each person was enrolled in and, for enrollees in managed care, used the claims data to determine whether they also received services through fee-for-service Medicaid (see methods).
More than half (55%) of dual-eligible individuals were enrolled in multiple Medicaid delivery systems (Figure 3). Nearly half of dual-eligible individuals (46%) were enrolled in two Medicaid delivery systems, 9% were enrolled in three or more, and 45% were enrolled in one. The extent to which dual-eligible individuals were enrolled in multiple Medicaid delivery systems varied substantially across states from less than 1% in 9 states to over 97% in Iowa, New Jersey, and Nebraska (Appendix Table 4). Variation across states reflects differences in the extent to which states use limited benefit plans and the extent to which states that use managed care exclude some services from the managed care contracts, instead providing them through fee-for-service or limited benefit plans.
Dual-eligible individuals in Medicaid managed care or single coverage arrangements were enrolled in multiple Medicaid delivery systems more often than those in Medicaid fee-for-service. Most dual-eligible individuals enrolled in Medicaid managed care (71%) were enrolled in more than one delivery system, as were most dual-eligible individuals in a Medicare-Medicaid Plan or PACE (60%). Fewer than half (39%) of dual-eligible individuals in Medicaid fee-for-service were enrolled in multiple service delivery systems. The large share of dual-eligible individuals in single coverage arrangements with multiple Medicaid delivery systems is primarily because Medicare-Medicaid plans may excludesome services from their contracts, such as hospice and certain behavioral health services (though the plan is still responsible for coordinating these services for enrollees). In contrast, PACE always provide long-term care benefits and are intended to be the sole source of all other Medicaid and Medicare benefits. As a result, two thirds (65%) of Medicare-Medicaid plan enrollees were enrolled in multiple Medicaid delivery systems compared with only 15% of those in PACE (data not shown).
States’ use of limited benefit plans and exclusions from managed care contracts may allow for management of specialized Medicaid benefits but means that single coverage arrangements may still not be fully integrated. One of the primary reasons states may exclude some benefits from a primary delivery system is when the primary delivery system lacks experience in delivering specialized Medicaid benefits such as long-term care, behavioral health, or non-emergency medical transportation. In some cases, the entities with the most experience providing such benefits are standalone limited benefit plans, which frequently include county departments of social or behavioral health services. In other cases, the state is the most experienced with providing such benefits, so they are excluded from the managed care contracts that cover other Medicaid benefits. There are tradeoffs between fully integrating Medicare and Medicaid benefits through a managed care plan and allowing the most experienced entities to provide specialized benefits.
More than half of all dual-eligible individuals enrolled in Medicare Advantage plans were enrolled in D-SNPs
Among the 43% of dual-eligible individuals in Medicare Advantage, more than half (28%) were covered through dual eligible special needs plans D-SNPs (including 24% in coordination-only D-SNPs or highly integrated dual eligible special needs plans (HIDE SNPs)), and 3% in fully integrated dual eligible special needs plans (FIDE SNPs) (Appendix Table 1). D-SNPs are required to coordinate Medicare and Medicaid benefits to different degrees depending on the state in which they operated and the type of D-SNP, but those with the highest degree of coordination, FIDE SNPs, have the lowest enrollment.
There are efforts underway intended to improve how dual-eligible individuals in Medicare Advantage SNPs receive their Medicare and Medicaid benefits. In 2021, FIDE SNPs were required to provide all Medicare and some Medicaid benefits, including LTSS or behavioral health (but not required to provide both), under the same parent organization (from the D-SNP or an aligned Medicaid managed care plan owned by the D-SNP’s parent company). Additionally, states determined whether to require exclusively aligned enrollment, meaning the plans could only enroll dual-eligible individuals who received their Medicare and Medicaid benefits from the same parent organization (an option that four states – Idaho, Massachusetts, Minnesota, and New Jersey exercised).
Starting in 2025, the Centers for Medicare and Medicaid (CMS) will require FIDE SNPs to have exclusively aligned enrollment. Consequently, FIDE SNPs will not be able to enroll dual-eligible individuals unless they are enrolled in the aligned Medicaid plan (further details in Table 1). Additionally, the FIDE SNP or its aligned Medicaid plan will be required to cover a more comprehensive set of services, including LTSS, behavioral health, and home health. Although Medicare and nearly all Medicaid benefits will be provided by a single parent organization, financing will remain separate (see Table 1 for further details).
About one in eight (14%) dual-eligible individuals were in individual Medicare Advantage plans and the remaining 2% were in chronic condition or institutional SNPs. Individual Medicare Advantage plans are open to all Medicare beneficiaries. Chronic condition SNPs (C-SNPs) serve individuals with specific chronic conditions, while institutional SNPs (I-SNPs) serve individuals who are in institutions or receiving long term services and support in the community. While C-SNPs and I-SNPs enroll dual-eligible individuals, they are not required to coordinate Medicare and Medicaid benefits.
Just over half (52%) of dual-eligible individuals were in traditional Medicare and most were not aligned to an accountable care organization.
The Affordable Care Act created the Medicare Shared Savings Program, which permanently established accountable care organizations (MSSP ACOs) as part of the Medicare program. ACOs are a group of doctors, hospitals, and other health care providers that form partnerships to coordinate care for their patients. CMS attributes traditional Medicare beneficiaries to an ACO if they received most of their primary care services from a provider affiliated with the ACO. Beneficiaries also have the option of voluntarily aligning with an ACO. Providers that participate in a Medicare ACO are required to inform their patients of their participation. In addition to the MSSP ACOs, the Center for Medicare and Medicaid Innovation has tested various other ACO models over the years. This analysis focused on MSSP ACOs and thus may undercount the number of dual-eligible individuals aligned to any Medicare ACO in 2021.
Most dual-eligible individuals in traditional Medicare were not aligned to MSSP ACOs. Overall, just 12% of dual-eligible individuals were in traditional Medicare and aligned to an MSSP ACO (Figure 4). Across all states, at least some dual-eligible individuals were aligned with a MSSP ACO (Appendix Table 1). The share of dual-eligible individuals in traditional Medicare aligned to a MSSP ACO ranged from just under 1% in Vermont to 30% in Delaware.
CMS aims to have all traditional Medicare beneficiaries, including dual-eligible individuals, in alternative payment models, which to date are predominately ACOs, by 2030. Given the higher share of dual-eligible individuals in traditional Medicare and the relatively low number aligned to MSSP ACOs, this move could have broad implications for dual-eligible individuals who remain in traditional Medicare and raises questions about how ACOs will help dual-eligible individuals access and coordinate their Medicare and Medicaid benefits. In the 2023 final rule, CMS made changes to the Medicare Shared Savings Program, including rewarding ACOs that provide quality care to dual-eligible individuals and other underserved populations. In addition, new ACO models are being tested, in particular the ACO REACH Model, which aims to align underserved communities, including dual-eligible individuals, with accountable care arrangements that are specifically designed to meet their needs. More evaluation will be useful in understanding how well these goals are achieved.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
Data: Data are from a KFF analytic file that merged the Centers for Medicare & Medicaid Services Chronic Conditions Data Warehouse 2021 research-identifiable Master Beneficiary Summary File (MBSF) Base and the 2021 Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) Research Identifiable Files (RIF) file using a Chronic Conditions Warehouse (CCW) beneficiary identifier crosswalk.
Dual-eligible individual inclusion criteria: Full dual-eligible individuals were included if (1) they were in both the MBSF and T-MSIS files using the CCW crosswalk (2) and if individuals were a full dual-eligible individual in March (03) 2021 using the Medicare monthly DUAL_STUS_CD_03 with values of 02,04,08 or the Medicaid monthly code (March=03) DUAL_ELGBL_CD_03 with values of 02,04,08 or the monthly code (March=03) RSTRCTD_BNFTS_CD_03 values of 1,A,D,4,5,7. Dual-eligible individuals also had to have both Part A and B in March 2021 to be included in this analysis.
State inclusion criteria: To assess the usability of states’ data, the analysis examined quality assessments from the DQ Atlas for enrollment in managed care and compared enrollment in comprehensive managed care with the Medicaid Managed care enrollment report for dual-eligible individuals in 2021. The analysis excluded any states that had both a “Unclassified/ Unusable” DQ Atlas assessment and more than 50% difference between the number of dual-eligible individuals in managed care in T-MSIS and the number reported in the Medicaid managed care enrollment report. Three states (Alabama, Arkansas, and Idaho) were excluded based on these criteria in 2021, leaving 47 states and DC in the main analysis. Enrollees were assigned a state based on their T-MSIS STATE_CD.
Assignment to Medicare coverage arrangements
Traditional Medicare: Beneficiaries without a valid Medicare Advantage contract ID in March 2021 were defined as enrolled in traditional Medicare. This analysis identifies individuals who are in traditional Medicare and aligned to an Accountable Care Organization using the Medicare Shared Savings Program Accountable Care Organizations (ACO) Beneficiary-level RIF. Dual-eligible individuals were identified as being aligned to an ACO if they were assigned to an ACO in quarter 1 (Q1_Assign).
Medicare Advantage plans: Beneficiaries with a valid contract ID in March 2021 were identified as enrolled in Medicare Advantage. To determine the type of plan in which the beneficiary was enrolled, the contract ID and plan ID were matched to the March 2021 Monthly Enrollment by Plan, or the Special Needs Plan Report data published by CMS. This includes enrollment in all private plans which are predominately Medicare Advantage plans.
Program Of All-Inclusive Care for The Elderly (PACE) or Medicare-Medicaid Plan. Enrollment in PACE and Medicare-Medicaid Plan was determined using the approach defined in the “Medicare Advantage” section.
Assignment to Medicaid delivery systems
PACE or Medicare-Medicaid Plan. Enrollment in PACE and Medicare-Medicaid Plan for the Medicaid delivery systems was determined using Medicare data and the approach is defined in the “Medicare Advantage” section.
Medicaid managed care. For enrollees who were not enrolled in PACE or a Medicare-Medicaid Plan, enrollment in comprehensive managed care plans was identified by the MC_PLAN_TYPE_CD_03 variable with values of 01 (Comprehensive managed care), 04 (Health Insuring Organization), 07 (Long-term Care Prepaid Inpatient Health Plan (PIHP)), 17 (PACE), 19 (Long term care services and supports and mental health Prepaid Inpatient Health Plan(PIHP)), 80 (Integrated care for dual-eligible individuals). Enrollment data among dual-eligible individuals using the values of PACE (17) and Integrated care for dual-eligible individuals (80) were not always consistent with the MBSF (which was used to assign PACE and Medicare-Medicaid Plan status). As a result, dual-eligible individuals with a value or 17 or 80 who did not have a corresponding assignment in the MBSF were assigned to Medicaid managed care.
Medicaid fee-for-service. Enrollment in Medicaid fee-for-service includes anyone not in PACE, a Medicare-Medicaid Plan, or Medicaid managed care, as defined above. This analysis does not identify individuals who receive their Medicaid benefits through a Financial Alignment Initiative managed FFS program.
Number of Medicaid delivery systems. The analysis counted the number of Medicaid delivery systems by adding the number of plan types identified in MC_PLAN_TYPE_CD_03. All plan types were included except for 02 (Traditional Primary Care Case Management provider arrangement), 03 (Enhanced Primary Care Case Management provider arrangement), 60 (ACO), 70 (Health/Medical Home). For individuals enrolled in managed care, the analysis counted fee-for-service Medicaid as an additional delivery system if individuals incurred any fee-for-service spending in 2021.
Americans spend on average more than $1,000 per person per year on prescription drugs, far surpassing prescription drug spending in other peer nations. According to a 2023 KFF poll, 3 in 10 adults taking prescription drugs report that they have not taken their medication as prescribed due to costs. In a 2023 KFF consumer survey, nearly one-quarter (23%) of insured adults reported that their health insurance did not cover a prescription drug or required a very high copay for a drug that a doctor prescribed, increasing to more than one-third (35%) of insured adults in fair or poor physical health. People who need specialty or brand-name medications to treat chronic health conditions such as diabetes, cancer, arthritis, and HIV are especially vulnerable to high costs, particularly considering rising deductibles over the years. In addition, plans are more likely to apply coinsurance (a percentage of the cost paid by the enrollee after meeting their deductible) than copayments (a flat dollar amount) for specialty or higher cost prescription drugs than they are for lower cost drugs, which could result in enrollees having to pay more out of pocket for these drugs.
As biologics and other specialty drugs have become increasingly available, many people who take these high-cost medications receive financial assistance from drug manufacturers to offset these high out-of-pocket costs. For people with private insurance, when applied to patient deductibles and out-of-pocket costs, this assistance can provide considerable help, but increasingly plans have applied “copay adjustment programs” that do not count these amounts toward enrollees’ out-of-pocket obligations. This issue brief provides an overview of copay adjustment programs, arguments made for and against their use, their prevalence, and federal and state efforts to address them.
Key Takeaways
Many drug manufacturers provide copay coupons for their high-cost (often specialty) medications to encourage the use of their drugs and help offset out-of-pocket costs for consumers who use their medications. Concerned about the potential for these coupons to undermine their benefit designs and increase costs, some health plans have changed the way coupons apply to enrollee out-of-pocket obligations. The separate incentives of these two industry players can wind up putting the patient in the middle.
With copay accumulators, the value of the manufacturer copay coupon is applied each time the prescription is filled but that value does not count toward the enrollee’s deductible or out-of-pocket maximum. Once the coupon is exhausted the enrollee is suddenly subject to their deductible and then a copayment and/or coinsurance, which can be substantial for these medications.
The 2024 KFF Employer Health Benefits Survey found that nearly one in five (17%) large employer-sponsored health plans have a copay accumulator program in their largest plan, increasing to one-third (34%) of firms with 5,000 or more workers. Another analysis found that two-thirds (66%) of individual Marketplace plans sold in states that do not prohibit copay accumulator programs have such a program in 2024.
With copay maximizers, insurers seek to capture the savings from coupons provided by drug manufacturers. Plans re-classify certain high-cost specialty medications such that they are no longer subject to the Affordable Care Act’s patient cost sharing limitations. Copay coupons do not count toward the enrollee’s deductible or out-of-pocket maximum. Enrollee cost sharing requirements are set to match the maximum coupon value, which is applied evenly throughout the year. Enrollees who choose to participate in the program do not typically face immediate out-of-pocket costs for that medication, but if they choose not to participate, they face substantial out-of-pocket obligations that do not count toward their out-of-pocket obligations.
Definitive data on the prevalence of copay maximizers is limited, but one study found that their use has increased dramatically in recent years, with roughly half of commercially-insured individuals exposed to one.
Federal regulations have not yet fully addressed the use of copay adjustment programs, but federal legislation has been introduced, and 20 states and Washington, DC, have taken action to fill these gaps for state-regulated health plans.
Overview of Manufacturer Copay Coupons
Many prescription drug manufacturers have established copay assistance programs in the form of copay cards and coupons to help offset immediate out-of-pocket costs (deductibles, copays, and coinsurance) for brand name, often specialty, prescription drugs for people with health insurance. Some branded drugs with coupons have a generic equivalent. The structure of copay coupons varies by manufacturer and by drug. Some coupons are valid for a certain number of prescription fills or for the duration that the patient is prescribed the medication. Some have a maximum annual dollar value while others have a monthly maximum, or a combination of both. Some manufacturer copay coupon programs require a relatively nominal monthly contribution (e.g., $10) from the patient toward the cost of the drug. Copay coupons can also be applied toward patient deductibles and coinsurance payments.
Eligibility may vary depending on whether the insured patient’s health insurance plan has a copay adjustment program (discussed in the next section). Copay assistance programs are different from patient assistance programs (PAPs), which typically provide financial assistance to those without insurance (or who are underinsured) who meet certain maximum income thresholds. Co-pay assistance programs are also different from drug discount cards that are available to any consumer that may provide them with a discount on a medication at a pharmacy.
Copay assistance is available for the vast majority of brand name drugs and that share has increased over time. In 2023, copay assistance was used for an estimated 19% of prescriptions for patients with private insurance (though much higher for some therapy areas), with a total value of $23 billion. Nearly one-third of brand commercial prescriptions used manufacturer copay assistance in the top 10 therapy areas that year.
The federal anti-kickback statute prohibits manufacturers from offering copay coupons for beneficiaries of federal health care programs, including Medicare and Medicaid, because coupons can act as a financial incentive for beneficiaries to choose more expensive drugs over lower-cost equivalents, which can also lead to higher federal spending. Manufacturers typically have safeguards in place to help ensure compliance with the law, such as notices printed on coupons and sent to pharmacies or verification during the claims transaction system. However, a 2014 study by the Office of the Inspector General of the Department of Health and Human Services found that these safeguards may not prevent all copay coupons from being used to pay for Medicare Part D drugs, in part because coupons are not always transparent in the pharmacy claims transaction system to entities other than manufacturers and manufacturers could be relying on unreliable patient information.
By contrast, federal laws that apply to private insurance, such as the Affordable Care Act (ACA), do not specifically address copay coupons. The ACA does, however, place annual limits on out-of-pocket cost sharing for covered essential health benefits (EHBs), including prescription drugs, for consumers with private insurance (see callout box). At least two states (MA (until 2026) and CA) prohibit the use of copay coupons in their state-regulated private insurance markets if the drug has a generic equivalent, with some specific exceptions.
Essential Health Benefits (EHBs)
What are they? A set of 10 categories of services that certain health insurance plans must cover under the Affordable Care Act (ACA), including prescription drug coverage, doctors’ services, hospital care, pregnancy and childbirth, mental health services, and more. Plans subject to EHB requirements must cover of at least as many prescription drugs in every category and class in the U.S. Pharmacopeia Medicare Model Guidelines as covered by the state’s EHB-benchmark plan, or one drug in every category and class, whichever is greater.
What types of health plans must cover the EHBs? Non-grandfathered, ACA-compliant plans sold in the individual and small group markets.
What types of health plans do not have to cover the EHBs? Large group plans (whether fully-insured or self-funded) and self-funded small group plans. However, if these plans opt to cover any EHBs, and most do, they must count cost-sharing amounts toward the plan’s annual out-of-pocket maximum. Agency regulations require plans to choose a state benchmark plan to determine what services count.
How do manufacturer copay coupons work?
To explain how manufacturer copay coupons work in practice, consider the following hypothetical scenarios in which a patient, who takes a brand-name, specialty medication to treat her cystic fibrosis that costs $2,000/month, does and does not receive a copay coupon (Table 1). Assume the patient, whose plan year begins in January, has a:
$2,000 deductible which she has not yet met,
25% coinsurance (which equates to $500),
$5,000 out-of-pocket (OOP) maximum, and
A $6,000/year manufacturer coupon, when applied.
Without a copay coupon: The patient pays the full cost of the medication in January after which point her deductible has been met. The insurance plan begins to cover the drug in February and the patient pays her required coinsurance. In July, she reaches her OOP maximum ($5,000) and the plan covers in full her cystic fibrosis medication (and all other covered health care services and medications received in-network) for the remainder of the plan year.
With a copay coupon: The patient’s copay coupon is applied to her deductible and coinsurance each month. In this scenario, her $5,000 OOP maximum is met in July, meaning that even though the coupon was for $6,000, the manufacturer ends up paying $1,000 less. Her health plan will now cover the drug in full for the remainder of the year. The patient pays $0 for this medication over the course of the plan year. The health plan receives no benefit from the copay coupon.
In both scenarios, the patient reaches her deductible and OOP maximum in the same month. The total cost sharing amounts paid are the same in both scenarios; however, in the scenario without a coupon, that amount is shifted from the patient to the drug manufacturer.
Issue Brief
Overview of Copay Adjustment Programs
A ‘copay adjustment program’ is an umbrella term that includes various pharmacy benefit designs that allow enrollees to use manufacturer copay coupons at the point-of-sale but ensure that only amounts paid by the enrollee count toward their deductible and out-of-pocket maximum. Two common types of copay adjustment programs are copay accumulators and copay maximizers, though plans may refer to them in different terms, such as patient assurance programs out-of-pocket protection programs, and variable copay programs. While some copay adjustment program features may vary slightly from plan to plan, and some hybrid models do exist, these programs commonly include the following characteristics (Table 2):
As mentioned above, the use of copay coupons is not always evident in pharmacy claims transaction systems to entities other than manufacturers. Many plans require specialty medications to be filled through the PBM’s specialty pharmacy in an effort to reduce costs. (The three largest PBMs are vertically integrated with health insurers and specialty pharmacies.) This requirement may also provide a better opportunity for plans/PBMs to detect when a coupon is being used to pay for a medication. In addition, because large and self-insured employer plans that are not required to cover the EHBs are still required to have out-of-pocket maximums, and to select a state benchmark plan on which to base those amounts, copay maximizer vendors often encourageplan sponsors to select a state EHB benchmark plan that requires the fewest number/classifications of drugs to be covered.
How Copay Adjustment Programs Work: Example Scenarios
To explain how copay adjustment programs work in practice, consider the following hypothetical scenarios (Table 3) using the same assumptions as above:
With a copay coupon and a copay accumulator program: The patient still receives the copay coupon for her medication, but that assistance no longer counts toward her deductible or OOP maximum. The coupon pays the full cost of the medication until it has been exhausted in March. The patient then begins paying toward their deductible, which she reaches in April, and then her coinsurance until she reaches her OOP maximum, in October.
With a copay coupon and a copay maximizer program: The patient’s cost-sharing requirements are set to the full annual value of a copay coupon, which is applied evenly throughout the year such that she is not subject to a sudden deductible payment after the coupon has been exhausted (as is the case in the copay accumulator example). The manufacturer coupon covers all her cost sharing for this medication for the plan year; however, the patient does not satisfy any of her deductible or reach her OOP maximum unless she is paying for other covered benefits that count toward these cost-sharing requirements.
As demonstrated in these hypothetical scenarios, the patient receives the greatest direct benefit from the coupon without a copay adjustment program (Table 4). She meets her deductible and OOP maximum in the same months as she would have without having a copay coupon (January and July, respectively), but she pays less. In the copay accumulator scenario, the patient pays the same OOP costs as she would have without a manufacturer coupon ($5,000) but her deductible and OOP maximum are not met until later in the year (April and October, respectively). Under the copay maximizer scenario, she pays $0 out-of-pocket for her medication, like she would without a copay adjustment program, but she does not reach her deductible or OOP maximum during the plan year from this medication alone.
With a copay accumulator, the health plan reaps the vast majority of the benefit of the drug manufacturer coupon, shifting costs back to the consumer. With a copay maximizer, the health plan recaptures some of the benefit of the coupon.
Outside of these hypothetical scenarios, it should be noted that generally:
Patients, especially those with chronic conditions requiring expensive medications, may use other covered medical services or prescription medications during the plan year, which may affect their out-of-pocket costs and when during the plan year they reach their OOP maximum.
Some plans begin covering certain prescription medications before the deductible has been met.
In the case of a copay maximizer program, the third-party program a patient is enrolled in to administer the maximizer program may be able to secure a higher value copay coupon and set the patient’s cost sharing obligation to that amount, which could result in higher cost sharing than otherwise would have been required.
Sometimes, though not always, a medically appropriate, generic equivalent is available that costs less than the branded drug, which could result in lower out-of-pocket costs even without a manufacturer coupon.
Arguments For and Against Copay Adjustment Programs
The advantages and disadvantages of copay adjustment programs vary by stakeholder, with drug manufacturers, patients, and patient advocacy groups generally opposing such programs, and health plans/sponsors defending their use. The following discussion summarizes many of these arguments and industry incentives.
Drug Manufacturers
There are several business reasons manufacturers may choose to offer coupons, including to enhance brand loyalty and promote the use of their drug over others, and to compete for market share when generic drugs enter the market. (As previously mentioned though, these coupons are not permitted in public programs such as Medicare.) Manufacturers argue that this assistance helps patients afford needed medications. They contend that copay adjustment programs undermine that assistance and threaten the availability of patient assistance for those it is intended to help. Manufacturers and patients/patient advocacy groups are often aligned in their criticism of copay adjustment programs. Some manufacturers have taken action to address plans’ use of these programs (discussed in more detail later).
Health Plans/Sponsors
As health plan sponsors explore options to address increasing prescription drug prices, they (and sometimes their third-party vendors) argue that copay adjustment programs are a valuable tool to help reign in health care costs and that copay coupons circumvent formulary designs intended to steer enrollees to higher value, lower-cost medications. They state that manufacturer discount programs incentivize patients to choose brand-name, higher-cost drugs instead of generic, lower-cost drugs, which could, in turn, increase premiums, and that manufacturers benefit from coupons by taking advantage of federal tax deductions for charitable donations for the cost of the coupons. One study of one state’s commercial insurance market found that drug coupons for certain branded drugs with a generic equivalent increase utilization and spending, which could increase premiums.
Third-party vendors that administer copay adjustment programs report that their programs result in reduced specialty drug claims and significant savings for employers. Insurers also contend that the manufacturer assistance programs encourage manufacturers to keep drug prices high, pointing to studiesthathaveconfirmed some of these claims. There are concerns that plans may simply be capturing these assistance dollars intended for patients. Insurers have disputed claims that copay adjustment programs allow health plans/PBMs to “double dip,” which refers to plans essentially collecting two deductibles (one from the manufacturer and one from the patient), and capturing both manufacturer drug rebates and assistance dollars, asserting that manufacturer coupons do not get directed to the plans and that the plan still pays the pharmacy the negotiated rate. (The typical flow of money for prescription drugs is complex and many factors, including manufacturer rebates paid to PBMs and the potential passthrough of savings from PBMs to plan sponsors, play a role in determining health plan profitability, though these market dynamics are beyond the scope of this brief.)
Patients/Patient Advocacy Groups
Patient advocacy groups have challenged the use of copay accumulator programs and advocate for policies that require health insurers to apply manufacturer cost sharing assistance to the enrollee’s out-of-pocket maximum. Opponents of copay adjustment programs contend that many patients with chronic illnesses rely on copay coupons to afford expensive specialty medications such as those used to treat HIV and hepatitis. The exclusion of this financial assistance from patients’ deductibles and out-of-pocket maximums, they argue, places an unfair cost burden on these patients and can lead to reducedmedication adherence particularly with copay accumulator programs. (It should be noted that many of the patient advocacy groups speaking out against these programs are funded at least in part by pharmaceutical companies.)
Additionally, opponents of copay adjustment programs state that many of the brand name drugs that chronically ill people use do not have a generic version and that, when available, generics are not always substantially cheaper than the brand name or therapeutically equivalent or appropriate for the specific patient. Furthermore, one study found that although White and “non-White” patients utilize copay coupons at similar rates, non-White patients are more likely than White patients to face copay adjustment programs (though the reasons for this are not clear), which could exacerbate racial and ethnic disparities in access to medications. Copay maximizers have also been accused of artificially inflating cost sharing amounts to match the amount of assistance, and criticized as coercive to patients and lacking in transparency.
Prevalence of Copay Adjustment Programs
While definitive data on the prevalence of programs designed to blunt the financial impacts of manufacturer assistance are limited, there has been some research that can help quantify the extent to which commercial health plans employ and enrollees are exposed to these programs.
According to the nationally-representative 2024 KFF Employer Health Benefits Survey, among firms with 500 or more workers offering health benefits, nearly one-fifth (17%) have a copay accumulator program (including programs administered through the PBM) in their plan with the largest enrollment (Figure 1). This share increases to 34% for firms with 5,000 or more workers, compared to 13% for firms with 500-999 workers. About one-quarter (27%) of firms are unsure if their largest plan has a copay accumulator program. Firms with self-funded plans are more likely than those with fully-insured plans to offer a plan with a copay accumulator program (22% vs. 6%). (On average, larger firms are more likely to be self-funded than smaller firms.)
Although not a copay adjustment program per se, some health plans exclude cost sharing for certain medications from counting toward the enrollee’s out-of-pocket maximum which, as discussed below, new federal regulations aim to prevent. To better understand the extent to which this practice is occurring, the Employer Health Benefits Survey also asked large firms whether their largest health plan excludes cost sharing on any specialty drugs toward enrollees’ out-of-pocket maximum obligation. Overall, 10% of firms with 500 or more workers that offer health benefits report having this plan feature, increasing to 20% of the largest firms (Figure 1). Twelve percent of firms with self-funded plans have this feature, compared to 5% of firms with fully-insured plans. One-quarter (25%) of firms do not know if their plan has this feature.
With so many survey respondents, who are generally human resources or benefits managers, not knowing whether their plan has one of these plan features, plan enrollees also may not be aware of their plan’s coverage policy for certain medications. This lack of awareness presents an opportunity for increased health plan transparency and firm and enrollee education about their pharmacy benefit designs.
The KFF survey did not ask about copay maximizer programs specifically, but according to another organization’s2023 survey of a convenience sample of 35 PBMs and payers representing nearly 118 million enrollees with private coverage, half (49%) of those enrollees covered by these respondents were in a plan that had implemented a copay maximizer program for at least some covered drugs, an approximately eight-fold increase since 2018 (Figure 2). This sharp increase could reflect plan sponsors’ desire to cut their costs further than copay accumulator typically can, while still allowing enrollees to benefit from manufacturer assistance. However, respondents to this survey reported that their enrollees are now just as likely to be in a plan with copay maximizer program as they as with an accumulator. Health plans may use one or both of these copay adjustment programs.
A review of ACA Marketplace plans conducted by a patient advocacy group found that among states that do not prohibit copay accumulator programs, two-thirds (66%) of plans sold on those Marketplaces in 2024 have a copay adjustment program (not including the 16 plans that have a copay accumulator adjustment policy that only applies to brand name drugs that do not have a generic alternative) (data not shown).
The share of enrollees with private coverage exposed to copay adjustment programs varies by certain therapeutic areas, ranging from 11% for autoimmune medications to 18% for multiple sclerosis and oncology medications in 2023, as another study of 23 specialty brands and biosimilars in commercial claims data found (data not shown).
Manufacturer Response
As plan sponsors’ use of copay adjustment programs continues to proliferate, drug manufacturers have taken notice, and at least one has responded by filing a lawsuit against vendors of copay maximizer programs.
For example, in 2022, manufacturer Johnson & Johnson filed a lawsuit against SaveOnSP (a vendor that administers a copay maximizer program for Cigna’s PBM, Express Scripts), accusing SaveOnSP of deceptive trade practices and exploiting its copay assistance program in violation of its terms and conditions. The lawsuit states that because of SaveOnSP, Johnson & Johnson has paid millions more in copay assistance than it otherwise would have and for a purpose it did not intend. The case is ongoing.
Some drug manufacturers have responded by changing their copay assistance programs, which could inadvertently put patients in the crosshairs of the battle between health plans and manufacturer assistance programs. For example, Pfizer updated the terms and conditions of its copay assistance program to state that the program is not available to patients in plans with a copay accumulator or adjustment program. Other manufacturers, such as Vertex, which manufactures a cystic fibrosis medication, have reduced the value of their copay coupons when a plan/PBM is using a copay adjustment program.
Federal and State Actions
As health plans’ use of copay adjustment programs have increased in recent years, so too, have federal regulations, lawsuits, and state laws.
Federal
The HHS Notice of Benefit and Payment Parameters (NBPP) for 2020 could be read to permit private plans to use copay accumulators only when the drug has a “medically appropriate,” generic equivalent, as permitted by state law. The NBPP for 2021 reversed that provision, providing that, when consistent with state law, health plans/PBMs could opt to decline to credit copay coupons towards enrollee cost sharing obligations, regardless of whether a generic equivalent was available, citing potentially conflicting regulations regarding the tax treatment of high-deductible health plans paired with a health savings account.
However, in 2022, patient advocacy groups filed a lawsuit challenging that portion of the 2021 rule. In 2023, a U.S. District Court ruled in favor of the plaintiffs and vacated the 2021 copay accumulator rule in part because it conflicted with the ACA’s definition of “cost sharing,” concluding “that the regulatory definition unambiguously requires manufacturer assistance to be counted as “cost sharing,” which is “any expenditure required by or on behalf of an enrollee.” A later decision clarified that because the 2021 copay accumulator rule was vacated,” plans have to adhere to the 2020 rule. However, in its 2023 motion to clarify, HHS stated that it would not take enforcement action against issuers or plans that do not count manufacturer assistance for drugs that have generic equivalents toward out-of-pocket obligations and that it intended to issue a new final rule. HHS has withdrawn its appeal of the decision. A new rule specifically addressing the definition of cost sharing or the treatment of copay adjustment programs has not yet been issued.
In response to concerns about plan sponsors reclassifying certain drugs as “non-EHB” and not counting enrollee cost sharing for these drugs to count toward out-of-pocket maximums, the 2025 NBPP explicitly requires non-grandfathered individual and fully-insured small group plans that cover prescription drugs in excess of the state’s benchmark plan (with limited exceptions) to consider those drugs part of its essential health benefits (EHB) package and clarifies that plans are required to count these amounts toward the required annual limitation on cost sharing. The final rule states that the Departments intend to propose rulemaking that would also make these standards applicable to large group plans and self-funded plans.
In 2023, a bipartisan group of federal lawmakers introduced the Help Ensure Lower Patient (HELP) Copays Act, which would require plans/PBMs to apply copay coupons to enrollees’ out-of-pocket obligations. It also stipulates that health plans that cover drugs must consider all covered drugs part of its essential health benefits package, which are required by the Affordable Care Act to count toward an enrollee’s out-of-pocket maximum for individual and small group market plans. If passed, the law would apply to all private health plans including those that are self-funded, thereby filling a substantial gap in state copay accumulator laws. The legislation has not yet been brought to a vote.
Also of note, the Federal Employees Health Benefits (FEHB) Program, which covers millions of federal workers and their dependents, does not permit the plans it contracts with to use copay maximizers or other similar programs, asserting that these types of benefit designs are not in the best interest of enrollees or the federal government.
State
There has been increasing interest at the state level in recent years to address the use of copay accumulator programs, with 20 states and the District of Columbia restricting them in their state-regulated health plans/PBMs. Eleven of those states prohibit accumulator programs only if a generic equivalent is available and the others ban them in all cases (Figure 3). Beginning in 2025, Nevada and Oregon will also require their state-regulated health plans to count drug manufacturer financial assistance toward the enrollee’s cost sharing limits if there is no generic available.
State insurance laws, including prohibitions on copay accumulator programs, only apply to state-regulated health plans and not to self-funded plans sponsored by private employers, which cover 63% of covered workers at private firms nationally. There is some variation by state, ranging from 35% of covered workers in Hawaii to 73% in Nebraska (Figure 3). Among the 25 states where a higher than average share of adults has multiple chronic health conditions, 13 restrict the use of copay accumulators in their state-regulated health plans (Figure 3), perhaps reflecting an interest among state legislators and patient advocates to shield these populations, who may rely on more expensive medications, from high out-of-pocket costs. No state laws have yet directly addressed copay maximizer programs.
Federal policies could affect state policies on copay adjustment programs. If the state laws conflict with federal laws and regulations, there are arguments that the state law is preempted.
Looking Forward
State and federal efforts to address the use of manufacturer financial assistance are part of broader efforts to limit patient drug costs. These efforts coincide with changes to Medicare drug pricing, state laws limiting cost sharing for insulin, as well as litigation related to these efforts, all amid increasing concerns about medical debt. In a 2024 KFF public opinion poll, just over half (55%) of U.S. adults reported worrying about being able to afford prescription drug costs; and according to a 2023 KFF poll, nearly three in ten (28%) said they have difficulty affording their prescriptions.
Studies show that reducing copayments results in better adherence to needed medications and better health outcomes and that manufacturer financial assistance can help promote this. However, counting this assistance toward patient out-of-pocket obligations could limit the ability of plans to steer patients to lower cost drugs and drive up costs for plan sponsors and, in turn, premiums paid by all consumers.
Entering this landscape is a relatively new approach to funding high-cost specialty medications called “alternative funding programs” (AFPs). These programs are being increasingly marketed to employers as a way to lower their costs by shifting the financial responsibility for these drugs to alternative funding sources such as patient assistance programs (PAPs) established by pharmaceutical companies and charitable organizations. To do this, some or all specialty medications are removed from the plan’s formulary, and patients, who now appear to be uninsured or underinsured, are enrolled in a PAP that pays for the drug. Data on the prevalence of these programs is limited, but their practices are alreadyunderscrutiny.
Although federal regulations in recent years have sought to address the use of copay accumulator programs, there still is no definitive policy, and they have not yet addressed newer models such as copay maximizers and alternative funding programs. Many states have taken action to fill gaps in federal policies related to copay accumulators, but most have also not caught up with the use of these newer models and their reach is limited to state-regulated health plans.
The outcome of a lawsuit decided by the U.S. Supreme Court in 2024, Loper Bright, could have new, far-reaching implications for federal regulations. Regulations related to any number of policy areas, including those that address the use of copay adjustment programs and alternative funding programs, could be subject to increased legal scrutiny as courts are no longer required to defer to agency decisions where federal law is silent or unclear.
While laws and regulations address prescription drug costs to some extent in Medicare (e.g., out-of-pocket caps on insulin) and Medicaid (e.g., drug rebates to states and the federal government), prescription drug costs in the private insurance market are largely unregulated. Drug manufacturers have the ability to set high prices, particularly for drugs still under patent protection, and then provide financial assistance directly to privately-insured patients, which can increase their market share. Health plans, in an effort to control costs, then try to recapture that financial assistance. In the meantime, patients are caught in the middle of these market dynamics shouldering the consequences.
This work was supported in part by a grant from the Robert Wood Johnson Foundation. The views and analysis contained here do not necessarily reflect the views of the Foundation. KFF maintains full editorial control over all of its policy analysis, polling, and journalism.
How Abortion Misinformation Gives Rise to Restrictive Abortion Laws
This is Irving Washington and Hagere Yilma. We direct KFF’s Health Misinformation and Trust Initiative and on behalf of all of our colleagues across KFF who work on misinformation and trust we are pleased to bring you this edition of our bi-weekly Monitor.
Trump claims abortion is infanticide at election events
SDI Productions/Getty Images
False claims about abortions later in pregnancy are often spread to distort perceptions of when and how often pregnant people have abortions. Some have exaggerated these claims even further, falsely stating that individuals seek abortions after birth. During the presidential debate on September 10, former President Trump falsely claimed that Democrats support “abortion after birth,” equating it to execution. Despite the fact that killing a child after birth is infanticide and illegal in all states, Trump’s statement sparked outrage among anti-abortion advocates who accepted his words as fact.
Some posts after the debate debunked claims comparing abortion access to infanticide, but other public figures, such as former Arkansas Governor Mike Huckabee, repeated similar misleading statements. Huckabee’s Facebook post expressed dismay at the fact-checking during the debate, saying, “I assume [Harris] knows that most Americans find late-term abortion to be infanticide.” An X user received approximately 2 million views and 21,000 shares on their post in support of Trump’s false claim, stating “This is the level of depravity, incompetence, and casual evil that we are dealing with in government.” Most commenters agreed with the post, with many calling Trump a “truther.”
False claims equating abortion to infanticide and misleading claims about the prevalence of abortions later in pregnancy have circulated intermittently for decades, with Trump repeating this narrative several times this year. Each time he made the claim, there was a spike in mentions of terms like “late-term,” “nine month,” and “post-birth” abortions—non-medical terms that refer to abortions later in pregnancy or describe infanticide. On the evening of the debate, there were approximately 105,000 mentions of these terms on social media and in news articles. The frequent use of “late-term abortion” in social media posts suggests that the public has accepted it as a medical term, despite it having no medical meaning.
Politicians and anti-abortion advocates often claim that a significant number of abortions occur late in pregnancy, suggesting that people carry pregnancies for eight or nine months and then suddenly decide to seek an abortion. In reality, abortions later in pregnancy typically occur because individuals receive new information about their pregnancies, such as the discovery of serious fetal or maternal health issues, or because they were unable to access abortion services sooner. A KFF Issue Brief explains how rare abortions later in pregnancy actually are.
Polling Insights:
Abortions at or after 21 weeks are uncommon and represent 1% of all abortions in the U.S. However, KFF’s March Health Tracking Poll found that there is widespread misunderstanding among the public about when most abortions occur. Most adults (67%), including similar shares of women and men, are unaware that less than five percent of abortions occur more than 20 weeks into a pregnancy, while one-third of adults (32%) correctly say that fewer than five percent of abortions occur before this point (Figure 1).
Misleading Claims Push the False Narrative That Abortion Pills Harm Health
MementoJpeg/Getty Images
Last month, ProPublica reported that the 2022 deaths of Amber Thurman and Candi Miller in Georgia were preventable and linked to the state’s six-week abortion ban. The report explains that both women developed rare complications after taking abortion pills and ultimately died because they were unable to access timely medical care under Georgia’s abortion ban. Medical experts affirm that such complications are rare and that the primary risk comes from delayed medical intervention, but these cases have been misrepresented to stoke fear and push for further restrictions on access to abortion pills.
Online conversations following the reports reflect widespread misunderstanding about abortion pill safety. Some commenters on an X post from Vice President Kamala Harris’s presidential campaign, which included a clip of her mentioning a death in Georgia, claimed it was due to a “botched abortion” and argued that abortion pills are unsafe. Another comment read, “If she just wouldn’t have taken that poison abortion pill with the intention of ending the life of her own twins, she would be alive today.”
False claims that abortion pills are unsafe have existed in the U.S. since the FDA approved medication abortion in 2000. These claims picked up after Roe v. Wade was overturned in 2022, as abortion pills became a more common method for ending a pregnancy. The false claims that abortion pills are unsafe undermine trust and contribute to laws restricting access. This sort of misinformation was central to a Supreme Court case reviewing a challenge to the FDA’s approval of mifepristone. The Court decided to uphold the FDA’s approval, but only because the defendants lacked standing to bring this challenge. A KFF Policy Watch explains how the Court’s decision leaves room for states to impose restrictions, like in Louisiana, where a law reclassifying abortion pills as a controlled substance recently went into effect.
Recent Developments
Misinformation Campaigns Undermine Abortion Rights Ballot Measures in Upcoming Elections
SDI Productions/Getty Images
Misinformation about the safety of abortions threatens ballot measures in the upcoming elections, as voters in 10 states will have the opportunity to vote on protecting or expanding abortion rights. In Florida, a proposed constitutional amendment aims to protect abortion rights for state residents, but some worry that the government is using false information to dissuade voters from supporting this amendment. A website produced by the Florida Agency for Health Care Administration (AHCA) claims the amendment “threatens women’s safety” and will “expose women and children to health risks.” A lawsuit accused the AHCA of spreading false information on a government-sponsored website. However, a Leon County circuit judge denied the temporary injunction to block the AHCA from sharing the information, ruling that it is a political issue for voters to decide.
Misleading Claims Suggest That Exceptions to Abortion Bans Provide Sufficient Protection
ericsphotography/Getty Images
A federal judge temporarily blocked the DeSantis administration from threatening broadcasters with criminal charges for airing a television ad supporting a proposed state amendment to protect abortion access. The ad features a woman who had a life-saving abortion but said she would be unable to do so under Florida’s current abortion ban. The Florida Department of Health claimed the ad contained false information, stating that women in life-threatening situations can still obtain abortions. Broadcasters defended the ad’s accuracy, citing the law’s vague language, which permits abortions after six weeks only when there is an “immediate” threat—a condition that did not apply in the woman’s case. The judge ultimately decided that the actions of the Florida DOH threatened First Amendment Rights, but the accuracy of the ad’s content was not central to the decision.
Anti-abortion advocates made similar claims following ProPublica’s reports that attributed two deaths to Georgia’s abortion ban, arguing that misinformation about exceptions to bans, rather than the bans themselves, causes harm. The tactic of misrepresenting harm caused by restricting abortion access is not new, but it remains misleading. A KFF Issue Brief explains that while many states with restrictive abortion laws have exceptions, the vague and inconsistent language of these laws creates confusion, leaving patients and physicians uncertain about when an abortion is legally permitted.
Polling Insights:
The 2024 KFF Women’s Health Survey found that 45% of women of reproductive age were aware of the status of abortion policy in their state, while 23% incorrectly described the status of abortion in their state, and 1 in 3 were unsure (Figure 2). Even in states where abortion is generally available, majorities were not aware of the policies around abortion.
Research Insights
Belief in Alternative Medicine Is Linked to Greater Acceptance of Health Misinformation
Oleksandra Yagello/Getty Images
A study in the Journal of Experimental Psychology examined the relationship between beliefs in complementary and alternative medicine (CAM), which includes non-traditional treatments like herbal remedies, and susceptibility to health-related misinformation. The researchers found that people who believe in CAM are more likely to accept false health information and resist changing their views, often ignoring standard credibility cues like scientific qualifications. There was also a strong link between vaccine hesitancy and initial belief in misinformation, demonstrating that personal beliefs shape how individuals process information. Therefore, a tailored approach to pointing out the lack of expertise of unreliable health sources may help reduce belief in misinformation.
Source: Swire-Thompson, B., Kilgallen, K., Dobbs, M., Bodenger, J., Wihbey, J., & Johnson, S. (2024). Discrediting health disinformation sources: Advantages of highlighting low expertise. Journal of Experimental Psychology: General, 153(9), 2299.
AI and Emerging Technology
Generative AI Fuels Growth of Fake Local News Sites
Hallfpoint Images/Getty Images
AI technology, particularly generative AI, has contributed to the proliferation of “pink slime” sites, which are deceptive websites appearing as legitimate local news sources. These sites use AI to rapidly generate large volumes of content, often blending factual information with partisan or misleading narratives for political or financial gain. As of June, these pink slime sites began to outnumber real local news sites, undermining the integrity of information. Recently, Metric Media, a major operator of these sites, faced criticism for its role in spreading misleading content ahead of the November elections. Critics argue that Metric Media’s network of over 1,200 websites pushes a political agenda instead of providing unbiased news. Last year, the company was also criticized for sharing fake print local news which contained biased articles supporting an Ohio ballot initiative. The initiative sought to make it more challenging to amend the state’s constitution, thereby restricting residents’ ability to codify abortion rights.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.
The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The Public Good Projects (PGP) provides media monitoring data KFF uses in producing the Monitor.
Access to Pregnancy and Parenting Support Services: Women’s Views and Experiences from the 2024 KFF Women’s Health Survey
Following the overturning of Roe v. Wade on June 24, 2022, there has been an increased focus and recognition of the importance of pregnancy and parenting support services for people across the country, especially for those living in states where abortion is banned or severely restricted. Prior research has found that overall states with restrictive abortion laws have fewer policies and programs that provide medical and social support for families and children. The 2024 KFF Women’s Health Survey asked reproductive age (18 to 49) women in the U.S. to rate how easy or difficult they feel it is to access a range of services that are important to the health of women and families. This analysis focuses on women with children ages 5 and under because they likely have more recent firsthand experience with many of these services important to pregnant people and parents, including maternity care, Medicaid coverage, food stamps, contraceptive services, and affordable childcare. A consistent pattern throughout this analysis is that a higher share of women with young children report difficulties in getting access to pregnancy-related services and parenting supports in states that ban or restrict abortion.
KEY FINDINGS:
Maternity Care: Even before the Dobbs decision, there were concerns about closures of hospitals and maternity wards as well as workforce shortages, with current estimates finding that over 5 million reproductive age women live in counties with no or few obstetric providers. Since the fall of Roe, some initial studies have showed that fewer medical students are applying for residency positions in states where abortion is banned and there have been anecdotal reports of OBGYN providers leaving states where abortion is banned, potentially exacerbating longstanding workforce shortages. Nationally, the KFF survey finds that over a quarter (28%) of women of reproductive age with young children say it is very or somewhat difficult to get maternity care in their state (Figure 1). In states where abortion is banned or restricted to the first 6 weeks of pregnancy, one in three (34%) women with young children say it is difficult for women in their states to get maternity services, higher than those who live in states that allow abortions up to 24 weeks or later (23%).
Medicaid: For women with low incomes, Medicaid is an important source of coverage and covers 4 in 10 births in the country. A third of women with young children (32%) say that it is very or somewhat difficult for women in their state to get Medicaid coverage (Figure 2).
Four in 10 women living in states where abortion is banned or restricted to early in pregnancy (41%) say it is difficult for women in their state to get Medicaid compared to less than one in four women (23%) in states where abortion is generally available. Of the ten states that have not adopted the ACA Medicaid expansion, seven also ban abortion or have 6-week gestational limits.
Food Stamps: Nationally, four in 10 women with young children say it is difficult for women in their state to get food stamps (Figure 3). Food stamps, also known as the Supplemental Nutrition Assistance Program (SNAP), provide financial support for groceries to individuals with low incomes who meet their states’ income and resource requirements. Average monthly SNAP household benefits ranged from $183 to $457 in 2019, varying by state. Yet, half (48%) of women with young children living in states where abortion is banned or with early gestational limits say it is difficult to get food stamps compared to three in ten women living in states where abortion is generally available.
Contraceptive Services: One in eight (13%) women with young children say it is difficult for women in their state to obtain contraceptive services (Figure 4). In states where abortion is banned or restricted to early in pregnancy, one in five (19%) women with young children say it is difficult to obtain contraceptive services, double the share (9%) of women who live in states where abortion is generally available. Research conducted following the Dobbs decision reveals a decline in the number of oral contraceptive and emergency contraceptive pills dispensed in pharmacies in states with abortion bans.
Child Care: Nationally, a large majority (72%) of women with young children say that affordable child care is difficult to obtain in their state, standing out as a big challenge for families irrespective of state abortion policy (Figure 5). Median yearly child care costs for one child range from $5,357 to $17,171, and costs are even higher for infant care and vary by state. The issue has gained traction during this year’s Presidential campaign and remains a challenge for most parents of young children regardless of where they live.
Methodology
The 2024 KFF Women’s Health Survey was designed and analyzed by women’s health researchers at KFF. The survey was conducted from May 13 – June 18, 2024, online and by telephone among a nationally representative sample of 6,246 adults ages 18 to 64, including 3,901 women ages 18 to 49. Findings from this brief are based on 1,053 women ages 18 to 49 who said that at least one child ages 5 and under currently lived in their household. Women include anyone who selected woman as their gender or who said they were non-binary transgender, or another gender and chose to answer the female set of questions about sexual and reproductive health. Download: Topline & Methodology.
This page provides access to the reports stemming from the 50-state Medicaid budget surveys published annually since 2000 by KFF. It includes the annual surveys as well as shorter mid-year updates that were conducted in select years. The report based on the annual survey is traditionally released each Fall and tracks trends in Medicaid spending and enrollment, as well as Medicaid policy actions around eligibility and enrollment, provider rates, provider taxes/fees, premiums and cost-sharing, benefits and pharmacy, long-term care and delivery system and payment reform.
Data are captured from Medicaid directors and staff through the completion of written surveys as well as structured follow-up telephone interviews. Each survey focuses on spending and enrollment trends as well as policy actions taken for the in the state fiscal year that just ended as well as definitive plans for the coming year. The survey does not attempt to catalog all Medicaid policies. Experience has shown that adopted policies are sometimes delayed or not implemented, for reasons related to legal, fiscal, administrative, systems or political considerations, or due to delays in approval from CMS. Policy changes under consideration are not included in the survey.
The annual survey is conducted by KFF and Health Management Associates. Beginning in 2014, the survey was completed through a partnership with the National Association of Medicaid Directors (NAMD).
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2024 and 2025. Findings are based on data provided by state Medicaid directors as part of the 24th annual survey of Medicaid directors in all states and the District of Columbia conducted by KFF and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth.
As Pandemic-Era Policies End, Medicaid Programs Focus on Enrollee Access and Reducing Health Disparities Amid Future Uncertainties: Results from an Annual Medicaid Budget Survey for State Fiscal Years 2024 and 2025
This report provides an in-depth examination of the changes taking place in Medicaid programs across the country, as states were wrapping up the unwinding of the pandemic-related continuous enrollment provision and focusing on an array of other policy priorities. The findings are drawn from the 24th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by KFF and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD). This report highlights policies in place in state Medicaid programs in FY 2024 and policy changes implemented or planned for FY 2025. Key areas of focus include delivery systems, provider rates and taxes, benefits, and pharmacy.
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2023 and 2024. Findings are based on data provided by state Medicaid directors as part of the 23rd annual survey of Medicaid directors in states and the District of Columbia conducted by KFF and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth.
Amid Unwinding of Pandemic-Era Policies, Medicaid Programs Continue to Focus on Delivery Systems, Benefits, and Reimbursement Rates: Results from an Annual Medicaid Budget Survey for State Fiscal Years 2023 and 2024
This report provides an in-depth examination of the changes taking place in Medicaid programs across the country, as states focused on unwinding of the pandemic-related continuous enrollment provision as well as an array of other policy priorities. The findings are drawn from the 23rd annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by KFF and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD). This report highlights policies in place in state Medicaid programs in FY 2023 and policy changes implemented or planned for FY 2024. Key areas of focus include delivery systems, provider rates and taxes, benefits, pharmacy, and telehealth.
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2022 and 2023. Findings are based on data provided by state Medicaid directors as part of the 22nd annual survey of Medicaid directors in states and the District of Columbia conducted by KFF and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth.
How the Pandemic Continues to Shape Medicaid Priorities: Results from an Annual Medicaid Budget Survey for State Fiscal Years 2022 and 2023
This report provides an in-depth examination of the changes taking place in Medicaid programs across the country, as states are preparing for the unwinding of the COVID-19 federal public health emergency and also are focusing on longstanding issues and new priorities. The findings are drawn from the 22nd annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by KFF and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD). This report highlights policies in place in state Medicaid programs in FY 2022 and policy changes implemented or planned for FY 2023. Key areas of focus include delivery systems, health equity, benefits, telehealth, provider rates and taxes, and pharmacy.
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2021 and 2022. Findings are based on data provided by state Medicaid directors as part of the 21st annual survey of Medicaid directors in states and the District of Columbia conducted by KFF and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth.
States Respond to COVID-19 Challenges but Also Take Advantage of New Opportunities to Address Long-Standing Issues: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2021 and 2022
This report provides an in-depth examination of the changes taking place in Medicaid programs across the country, reflecting states’ continued focus on COVID-19 pandemic response as they also look ahead to the unwinding of the public health emergency and other non-emergency priorities. The findings are drawn from the 21st annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by KFF and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD). This report highlights policies in place in state Medicaid programs in FY 2021 and policy changes implemented or planned for FY 2022; it also highlights state experiences with policies adopted in response to the COVID-19 pandemic. Key areas of focus include delivery systems, benefits and telehealth, social determinants of health (also including information on health equity and COVID-19 vaccine uptake), provider rates and taxes, and pharmacy cost containment.
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2020 and 2021. Findings are based on data provided by state Medicaid directors as part of the 20th annual survey of Medicaid directors in all 50 states and the District of Columbia conducted by KFF and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth.
State Medicaid Programs Respond to Meet COVID-19 Challenges: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2020 and 2021
Findings from this year’s budget survey policy report primarily focus on Medicaid policy changes planned for FY 2021, particularly those related to the COVID-19 pandemic. The findings are drawn from the 20th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by KFF and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD). Key areas of focus include eligibility and enrollment, provider rates and taxes, delivery systems, long-term services and supports, benefits and telehealth, and pharmacy cost containment.
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2019 and 2020. Findings are based on interviews and data provided by state Medicaid directors as part of the 19th annual survey of Medicaid directors in all 50 states and the District of Columbia conducted by the Kaiser Family Foundation (KFF) survey and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth.
A View from the States: Key Medicaid Policy Changes: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2019 and 2020
This report provides an in-depth examination of the changes taking place in Medicaid programs across the country. The findings are drawn from the 19th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Family Foundation (KFF) and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD). This report highlights certain policies in place in state Medicaid programs in FY 2019 and policy changes implemented or planned for FY 2020. Key areas of focus highlighted in the report include Medicaid initiatives to address social determinants of health, control prescription drug spending, improve birth outcomes and reduce infant mortality, and address the opioid epidemic.
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2018 and 2019. Findings are based on interviews and data provided by state Medicaid directors as part of the 18th annual survey of Medicaid directors in all 50 states and the District of Columbia conducted by the Kaiser Family Foundation (KFF) survey and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth.
States Focus on Quality and Outcomes Amid Waiver Changes: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2018 and 2019
This report provides an in-depth examination of the changes taking place in Medicaid programs across the country. Report findings are drawn from the annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Family Foundation (KFF) and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD). This report examines the reforms, policy changes, and initiatives that occurred in FY 2018 and those adopted for implementation for FY 2019 (which began for most states on July 1, 2018). Key areas covered include changes in eligibility, managed care and delivery system reforms, long-term services and supports, provider payment rates and taxes, covered benefits, and pharmacy and opioid strategies.
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2017 and 2018. Findings are based on interviews and data provided by state Medicaid directors as part of the 17th annual survey of Medicaid directors in all 50 states and the District of Columbia conducted by the Kaiser Family Foundation (KFF) survey and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth.
Medicaid Moving Ahead in Uncertain Times: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2017 and 2018
This report provides an in depth examination of the changes taking place in state Medicaid programs across the country. The findings in this report are drawn from the 17th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Family Foundation and Health Management Associates (HMA), with the support of the National Association of Medicaid Directors. This report highlights policy changes implemented in state Medicaid programs in FY 2017 and those planned for implementation in FY 2018 based on information provided by the nation’s state Medicaid Directors. Key areas covered include changes in eligibility and enrollment, delivery and payment system reforms, provider payment rates, and covered benefits (including prescription drug policies).
Putting Medicaid in the Larger Budget Context: An In-Depth Look at Three States in FY 2017 and 2018
This report provides an in-depth examination of Medicaid program changes in the larger context of state budgets in three states: Nevada, North Carolina, and West Virginia. These case studies build on findings from the 17th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Family Foundation and Health Management Associates (HMA).
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2016 and 2017. Findings are based on interviews and data provided by state Medicaid directors as part of the 16th annual survey of Medicaid directors in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured (KCMU) survey and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth and also look at expansion versus non-expansion states.
Implementing Coverage and Payment Initiatives: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2016 and 2017
This report provides an in depth examination of the changes taking place in state Medicaid programs across the country. The findings in this report are drawn from the 16th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured and Health Management Associates (HMA), with the support of the National Association of Medicaid Directors. This report highlights policy changes implemented in state Medicaid programs in FY 2016 and those planned for implementation in FY 2017 based on information provided by the nation’s state Medicaid Directors. Key areas covered include changes in eligibility and enrollment, delivery and payment system reforms, provider payment rates, and covered benefits (including prescription drug policies).
Putting Medicaid in the Larger Budget Context: An In-Depth Look at Four States in FY 2016 and 2017
This report provides an in-depth examination of Medicaid program changes in the larger context of state budgets in four states: Maryland, Montana, New York, and Oklahoma. These case studies build on findings from the 16th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured and Health Management Associates (HMA).
This issue brief provides an overview of Medicaid spending and enrollment growth with a focus on state fiscal years 2015 and 2016. Findings are based on interviews and data provided by state Medicaid directors as part of the 15th annual survey of Medicaid directors in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured (KCMU) survey and Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth and also look at expansion versus non-expansion states.
Medicaid Reforms to Expand Coverage, Control Costs and Improve Care: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2015 and 2016
This report provides an in depth examination of the changes taking place in state Medicaid programs across the country. The findings in this report are drawn from the 15th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured and Health Management Associates (HMA), with the support of the National Association of Medicaid Directors. This report highlights policy changes implemented in state Medicaid programs in FY 2015 and those planned for implementation in FY 2016 based on information provided by the nation¹s state Medicaid Directors. Key areas covered include changes in eligibility and enrollment, delivery and payment system reforms, provider payment rates, and covered benefits (including prescription drug policies).
Putting Medicaid in the Larger Budget Context: An In-Depth Look at Three States in FY 2015 and 2016
This report provides an in-depth examination of Medicaid program changes in the larger context of state budgets in three states: Alaska, California, and Tennessee. These case studies build on findings from the 15th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured and Health Management Associates (HMA).
Medicaid in an Era of Health & Delivery System Reform: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2014 and 2015
This report provides an in depth examination of the changes taking place in state Medicaid programs across the country. The findings in this report are drawn from the 14th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured and Health Management Associates (HMA), with the support of the National Association of Medicaid Directors. This report highlights policy changes implemented in state Medicaid programs in FY 2014 and those planned for implementation in FY 2015 based on information provided by the nation’s state Medicaid Directors. Key areas covered include changes in eligibility and enrollment, delivery systems, provider payments and taxes, benefits, pharmacy programs, program integrity and program administration.
Implementing the ACA: Medicaid Spending & Enrollment Growth for FY 2014 and FY 2015
This report provides an overview of Medicaid financing and Medicaid spending and enrollment growth with a focus on state fiscal years 2014 and 2015 (FY 2014 and FY 2015.) Findings are based on interviews and data provided by state Medicaid directors as part of the 14th annual survey of Medicaid directors in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured (KCMU) survey with Health Management Associates (HMA). Findings examine changes in overall enrollment and spending growth and also look at expansion versus non-expansion states.
Putting Medicaid in the Larger Budget Context: An In-Depth Look at Four States in FY 2014 and 2015
This report provides an in-depth examination of Medicaid program changes in the larger context of state budgets in four states: Michigan, Utah, Virginia, and West Virginia. These case studies build on findings from the 14th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured and Health Management Associates (HMA.)
Medicaid in a Historic Time of Transformation: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2013 and 2014
The report findings are drawn from the 13th annual budget survey of Medicaid officials in all 50 states and the District of Columbia. The report highlights trends in Medicaid spending, enrollment and policy initiatives for FY 2013 and FY 2014 with an intense focus on eligibility and enrollment changes tied to the implementation of the ACA as well as payment and delivery system changes. The report provides detailed appendices with state-by-state information and a more in-depth look at four case study states: Arizona, Florida, Kentucky and Washington.
Medicaid Today; Preparing for Tomorrow: A Look at State Medicaid Program Spending, Enrollment and Policy Trends Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2012 and 2013
After the worst economic downturn since the Great Depression, state policy makers were finally beginning to see signs of economic recovery at the end of state fiscal year (FY) 2012 and heading into FY 2013. Growth in total Medicaid spending and enrollment slowed substantially in FY 2012 as the economy began to improve. Relatively slow spending and enrollment growth are expected to continue in FY 2013.
Moving Ahead Amid Fiscal Challenges: A Look at Medicaid Spending, Coverage and Policy Trends Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2011 and 2012
The 11th annual 50-State Medicaid budget survey from the Kaiser Family Foundation’s Commission on Medicaid and the Uninsured finds that Medicaid officials in virtually every state are enacting a variety of cost cutting measures as states’ spending for Medicaid is projected to increase 28.7 percent in fiscal year 2012 to make up for the loss of federal stimulus money.
Hoping for Economic Recovery, Preparing for Health Reform: A Look at Medicaid Spending, Coverage and Policy Trends — Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2010 and 2011
This annual 50-state survey finds that number of states experienced rapid growth in their Medicaid enrollment and spending last year and expect additional growth, though at a slower pace, in fiscal year 2011.
The Crunch Continues: Medicaid Spending, Coverage and Policy in the Midst of a Recession
This annual 50-state survey finds that number of people on Medicaid and state spending on the program are climbing sharply as a result of the recession, straining state budgets and pressuring officials to curb costs despite increased financial help from the federal government through the American Recovery and Reinvestment Act (ARRA).
Headed for a Crunch: An Update on Medicaid Spending, Coverage and Policy Heading into an Economic Downturn, Results from a 50-State Medicaid Budget Survey for State Fiscal Year 2008 and 2009
As states finalized Medicaid policy decisions for fiscal year 2009, they faced a dramatically different situation than the prior year. At the start of state fiscal year 2008, the economy was generally strong and many states were restoring cuts from the last economic downturn and moving forward with Medicaid improvements and expansions to cover more low-income uninsured individuals. A year later, over half of all states faced significant budget shortfalls and slower than anticipated state revenue growth. For some states, plans to expand Medicaid were put on hold as states struggled to allocate funding and balance their budgets. Despite the budget crunch, few states took significant actions to cut Medicaid. During the last economic downturn from 2001 to 2004, most of the major Medicaid restrictions came later in the downturn cycle, not at the very beginning.
As Tough Times Wane, States Act to Improve Medicaid Coverage and Quality: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2007 and 2008
The annual 50-state survey of state officials on Medicaid and state budget actions reports enrollment in Medicaid declined for the first time in nearly a decade. The 0.5 percent enrollment decline in fiscal year 2007 was driven primarily by two factors. States reported that the new citizenship documentation requirements were causing significant delays in processing applications, affecting mostly individuals already eligible for the program. State officials also cited the good economy and lower unemployment for reducing enrollment. Faced with an improving economy, 42 states expect to expand coverage to the uninsured in the next year.
Low Medicaid Spending Growth Amid Rebounding State Revenues: Results From a 50-State Medicaid Budget Survey State Fiscal Years 2006 and 2007
The 50-state annual survey about budget conditions and Medicaid cost containment actions in FY2006-07 finds an improved economy combined with the implementation of the new Medicare prescription drug benefit has contributed to the lowest rate of Medicaid spending growth in a decade and the fourth consecutive year in which Medicaid spending growth has slowed.
Medicaid Budgets, Spending and Policy Initiatives in State Fiscal Years 2005 and 2006
The 50-state annual survey of about budget conditions and Medicaid cost containment actions in FY2005-06 shows that all states implemented and planned more Medicaid cost-containment actions, but are also implementing expansions as the gap between Medicaid spending growth and state tax revenue narrowed.
The Continuing Medicaid Budget Challenge: State Medicaid Spending Growth and Cost Containment in Fiscal Years 2004 and 2005
The 50-state annual survey of about budget conditions and Medicaid cost containment actions in FY2004-05 shows that all states plan more Medicaid cost-containment actions in FY2005.
States Respond to Fiscal Pressure: State Medicaid Spending Growth and Cost Containment
The third annual survey of the 50 states and the District of Columbia reveals that all 50 states and DC implemented Medicaid cost control strategies in FY2003 and they all planned additional action for FY2004 as they cope with fiscal crisis.
Medicaid Spending Growth: Results from a 2002 Survey
The report presents the findings of a 50 state survey of Medicaid directors, identifying state Medicaid spending trends and how states are responding to them for FY 2003 budgets.
For a three-year period following the onset of the COVID-19 pandemic, states provided continuous Medicaid enrollment in exchange for an increase in the federal share of Medicaid spending (known as the Federal Medical Assistance Percentage or “FMAP”). This policy resulted in the largest ever number of enrollees in Medicaid, which, along with enhanced subsidies in the Affordable Care Act (ACA) Marketplaces, contributed to the lowest ever uninsured rate. The 2023 Consolidated Appropriations Act (CAA) ended the continuous enrollment provision on March 31, 2023, requiring states to begin the process of “unwinding”, and millions of individuals have been disenrolled from Medicaid since the unwinding began. Most states began unwinding related disenrollments in late state fiscal year (FY) 2023 (which ends June 30 in most states) and completed disenrollments in late FY 2024, though state unwinding timelines vary. The CAA also phased down the enhanced federal matching funds through the end of 2023 (partway through FY 2024 for most states).
Heading into FY 2025, states are expected to wrap up unwinding-related eligibility redeterminations; however, uncertainty remains regarding post-unwinding Medicaid spending and enrollment trends and what the new “normal” will look like. Adding to this uncertainty are the loss of pandemic-related enhanced federal funding, shifts in state fiscal conditions, and the upcoming election, all which can have implications for Medicaid spending trends.
This brief analyzes Medicaid enrollment and spending trends for FY 2024 and FY 2025, based on data provided by state Medicaid directors as part of the 24th annual survey of Medicaid directors. 50 states (including the District of Columbia) responded to the 2024 survey, although response rates for specific questions varied. More information on response rates and methodology can be found at the end of the brief. Nearly all officials indicated that their spending projections reflect what is assumed in their states’ adopted budgets. Key survey findings include the following:
Following years of significant growth, Medicaid enrollment declined by -7.5% in FY 2024 and state Medicaid officials expect enrollment to continue to decline by -4.4% in FY 2025. These growth rates reflect the net Medicaid enrollment change from year to year including new enrollments, coverage losses due to unwinding, and some “churn” when those who lose coverage re-enroll within a short period of time. The unwinding of the continuous enrollment provision was the largest driver of enrollment declines.
Total Medicaid spending growth slowed to 5.5% in FY 2024 and is expected to slow further to 3.9% in FY 2025. While state Medicaid officials identified unwinding-related enrollment declines as the most significant factor driving changes in total Medicaid spending, they also noted a number of upward pressures on total spending. This included enrollment increases from eligibility changes such as 12-month continuous eligibility for children or overall state or Medicaid eligible population growth, the higher health care needs of enrollees that retained coverage during unwinding, and rate increases.
As anticipated, state Medicaid spending growth increased sharply in FY 2024 (19.2%) as the enhanced FMAP phased down and expired (after declining earlier in the pandemic despite high enrollment growth). State Medicaid spending growth is projected to slow to 7.0% in FY 2025, only slightly higher than total spending growth as the shifts caused by the enhanced FMAP expiration end.
Context
Medicaid provides comprehensive health care coverage and long-term services and supports (LTSS) to over one in five people living in the US. Medicaid also represents nearly one in five dollars spent on health care in the U.S. and half of LTSS spending. Medicaid is administered by states within broad federal rules and jointly funded by states and the federal government through a federal matching program with no cap. Medicaid is often central to state fiscal decisions as it is simultaneously a significant spending item as well as the largest source of federal revenues for states. Medicaid is a counter-cyclical program, meaning that more people become eligible and enroll during economic downturns. At the same time, states typically may face declines in revenues that make it difficult to finance the state share of funding for the program. After peaking after the implementation of the ACA in 2014, Medicaid enrollment and total spending growth slowed or declined in the years leading up to the COVID-19 pandemic, due in part to improving economic conditions and restrictions permitted under the Trump Administration.
The economic fall-out from the COVID-19 pandemic, and the ensuing federal and state response, lead to significant increases in Medicaid enrollment and spending. As in past economic downturns, Congress enacted legislation that temporarily increased the federal share of Medicaid spending to help states maintain their Medicaid programs. States received a 6.2 percentage point FMAP increase that generally applied to Medicaid spending that would have otherwise been reimbursed at the state’s regular FMAP. In exchange, states were prohibited from disenrolling people, and as a result Medicaid and Children’s Health Insurance Program (CHIP) enrollment grew from 71 million to 94 million, an increase of 23 million or 32% between February 2020 and April 2023. Total Medicaid spending reached $804 billion in federal fiscal year 2022, with 29% financed by states and 71% paid by the federal government – a somewhat higher federal share than in prior years due to the pandemic-related enhanced FMAP. The CAA ended the continuous enrollment provision on March 31, 2023 and required states to begin the process of “unwinding” (i.e., resume historically typical eligibility redeterminations and disenroll individuals found to be no longer eligible for Medicaid). The CAA also phased down the enhanced federal matching funds from April 2023 through December 2023. Since the unwinding period began, millions of individuals have been disenrolled from Medicaid, but total net Medicaid and CHIP enrollment as of June 2024 remained over 8 million more than enrollment in February 2020, before the pandemic began. Though state unwinding timelines varied, all states except four completed unwinding renewals by August 2024.
State economic conditions worsened rapidly when the pandemic hit but recovered quickly, leading to a period of significant revenue and expenditure growth for states. Early in the pandemic, initial unemployment claims and the unemployment rate spiked and state revenue collections declined but all quickly rebounded. By FY 2021 and FY 2022, most states were seeing record-breaking revenue growth as well as budget surpluses. Favorable state fiscal conditions combined with federal fiscal relief mitigated the need for widespread state spending cuts and allowed states to make investments and expansions, including to Medicaid programs. Given strong revenue growth and budget surpluses, states also adopted some of the largest tax cuts on record. In FY 2023 and FY 2024, however, these tax cuts combined with a weaker stock market performance and changes in inflation and consumer consumption patterns led to flat state revenue growth. Despite slower growth in revenue collections, state general fund spending continued to grow in FY 2024 (due to one-time spending of surplus funds), and some states ended FY 2024 with modest budget surpluses and continued to build rainy day funds.
State fiscal conditions remained stable at the beginning of FY 2025, but the longer term fiscal outlook is less certain. Heading into FY 2025, revenue collections have begun to stabilize and states are returning to more “normal” state budget environments, following multiple years of high revenue and spending growth as well as pandemic-related volatility and unpredictability. States appear to be in a stable fiscal position, though there is variation across states. According to FY 2025 enacted budgets, most states anticipate revenue growth will continue to flatten and expect state general fund spending growth to slow. Reduced revenue collections due in part to earlier tax cuts, the expiration of pandemic-era federal funding, and macroeconomic uncertainties may dampen enthusiasm for further investments in Medicaid seen over the past few years and could even prompt spending reductions. The upcoming election also contributes to a more uncertain state fiscal outlook.
Trends in Enrollment Growth FY 2024 and FY 2025
Following years of significant growth, Medicaid enrollment declined by -7.5% in FY 2024 and is expected to continue to decline by -4.4% in FY 2025, primarily due to the unwinding of the continuous enrollment requirement (Figure 2). Following the onset of the COVID-19 pandemic and start of the Medicaid continuous enrollment provision, enrollment rose sharply in FY 2021 and continued to grow, though more slowly, through FY 2023, reaching record highs for the program. When the continuous enrollment provision ended, most states began Medicaid disenrollments in late FY 2023 and finished in FY 2024 (though some states will continue to process renewals in FY 2025). As a result, Medicaid enrollment declined in FY 2024 and is projected to decline again in FY 2025. These growth rates reflect the net Medicaid enrollment change from year to year including new enrollments, coverage losses due to unwinding, and some churn. Additional KFF analysis of data through June 2024 found that net Medicaid enrollment remained above pre-pandemic levels; however, with a few states continuing unwinding renewals into FY 2025, estimates of both enrollment and spending for FY 2025 and beyond remain uncertain and continue to evolve.
As anticipated, the unwinding of the continuous enrollment provision was the largest driver of enrollment declines. Almost all responding states in FY 2024 and over half in FY 2025 reported unwinding and returning to normal renewal operations was the most significant downward pressure on total Medicaid enrollment. A number of state Medicaid agencies also mentioned a strong economy as a downward pressure on Medicaid enrollment in FY 2025 (though a few states noted potential worsening economic conditions in their state as an upward pressure). While Medicaid enrollment is expected to decline in both FY 2024 and FY 2025, about half of responding states in FY 2024 and FY 2025 mentioned eligibility expansions or overall state and Medicaid eligible population growth were putting an upward pressure on enrollment. The most frequently reported change was the new federal requirement that began January 2024 for all states to adopt 12-month continuous eligibility for all Medicaid and CHIP children under age 19. A few states also noted adopting multi-year continuous eligibility for children from birth to age six, an option to extend Medicaid postpartum coverage to 12 months, and changes in eligibility policy for justice-involved populations. A number of states also mentioned eligibility system and operational changes, such as increasing ex parte (or automated) renewal rates and unwinding waiver flexibilities offered by CMS, have mitigated some churn and coverage loss among eligible individuals, resulting in increased enrollment.
Trends in Spending Growth FY 2024 and FY 2025
Total Medicaid spending growth slowed to 5.5% in FY 2024 and is expected to slow further to 3.9% in FY 2025 (Figure 2). Total spending growth increased when the pandemic and continuous enrollment period began before peaking in FY 2022 and starting to slow slightly in FY 2023 as the continuous enrollment period ended. For FY 2024 and FY 2025, the total spending growth rate is projected to slow further as states wrap up the unwinding process. Nearly all responding states noted that Medicaid projections (for FY 2025) reflect the assumptions used in the state’s adopted budget.
Almost all states in FY 2024 and half in FY 2025 pointed to declines in enrollment during unwinding as the most significant factor driving changes in total Medicaid spending. Despite the downward pressure of enrollment declines due to unwinding, states are simultaneously experiencing a number of upward expenditure pressures, causing total spending to continue to increase but at a slower rate. Almost half of states noted upward pressure from enrollment increases due to eligibility expansions, overall state or Medicaid eligible population growth, or more generally, post-unwinding enrollment remaining above projected levels. States also noted that the enrollees that retained coverage during unwinding have higher health care needs and utilize more services than those disenrolled, resulting in increased per enrollee costs. A majority of responding states cited MCO or provider rate increases as an upward pressure on spending in FY 2024 and FY 2025. States noted that inflation and workforce shortages were driving higher labor costs, resulting in pressure to increase provider rates. Almost a quarter of states also mentioned expanding services available to members, directed or supplemental payments, and increasing LTSS costs as upward pressures on total spending in either FY 2024 or FY 2025 or both. A few states also reported increasing pharmacy costs as an upward budget pressure, though a few states noted pharmacy rebates or pharmacy cost containment initiatives were a downward pressure. A few states also mentioned a strong economy and its impact on enrollment as a downward pressure.
As anticipated, state Medicaid spending growth increased sharply in FY 2024 (19.2%) but is projected to slow to 7.0% in FY 2025, only slightly higher than total spending growth as the shifts caused by the enhanced FMAP expiration end (Figure 3). The state share of Medicaid spending typically grows at a similar rate as total Medicaid spending growth unless there is a change in the FMAP. During the Great Recession, state spending for Medicaid declined due to fiscal relief from a temporary FMAP increase provided in the American Recovery and Reinvestment Act (ARRA) but increased sharply when that fiscal relief ended. This pattern also occurred during the pandemic, with state Medicaid spending declining in FY 2020 and FY 2021 then increasing but at a slower rate than total spending in FY 2022 due to the pandemic-era enhanced FMAP. The rate of state spending growth increased in FY 2023 and FY 2024, surpassing the rate of total spending growth due to the phasing out of the enhanced FMAP. A few states also reported additional pressure on state spending from changes in their regular FMAP formula and/or the end of the enhanced FMAP for HCBS implemented as part of the American Rescue Plan Act (ARPA). Following the expiration of the enhanced FMAP, state Medicaid officials project state Medicaid spending in FY 2025 (7.0%) will fall back closer to total Medicaid spending growth projections (3.9%).
Despite overall stable budget conditions, over half of responding states at the time of the survey thought the chance of a Medicaid budget shortfall was “50-50”, “likely”, or “almost certain.” This is a significant change from the 2022and 2021 surveys where most states did not anticipate state revenue shortfalls and signals that some states will have to contend with Medicaid budget gaps in FY 2025. A number of state officials commented on how challenging budgeting was at this time due to the downward expenditure pressure of declining enrollment coupled with the upward pressure of increasing per enrollee costs during unwinding as well as overall changes in the share of enrollees in each eligibility group and the implementation of recently enacted federal rules. States also noted uncertainty in their longer-term fiscal outlook due to emerging high-cost prescription drugs and economic factors such as costs of medical care and workforce challenges.
Methods
KFF commissioned Health Management Associates (HMA) to survey Medicaid directors in all 50 states and DC to identify and track trends in Medicaid spending, enrollment, and policymaking. Given differences in the financing structure of their programs, the U.S. territories were not included in this analysis. This is the 24th annual survey, conducted at the beginning of each state fiscal year from FY 2002 through FY 2025. State fiscal years begin on July 1 in most states except for: New York on April 1; Texas on September 1; Alabama, Michigan, and District of Columbia on October 1. The KFF/HMA Medicaid survey for this report was sent to each Medicaid director in June 2024. 50 states provided survey responses by October 2024; Florida did not respond to this year’s survey.
Medicaid Enrollment Growth: The average annual Medicaid enrollment growth rate for FY 2025 was calculated using weights based on Medicaid and CHIP preliminary monthly enrollment data for June 2024 published by CMS. For FY 2025, 48 states reported Medicaid enrollment growth rates. The data reported for FY 2024 and FY 2025 for Medicaid spending and FY 2025 for Medicaid enrollment are weighted averages, and therefore, data reported for states with larger enrollment and spending have a greater effect on the national average.
Historical enrollment trend data for FY 1998 to FY 2013 reflects the annual percentage change from June to June of monthly enrollment data for Medicaid beneficiaries collected from all states and DC. Enrollment trend data for FY 2014 to FY 2024 reflects growth in average monthly enrollment based on KFF analysis of the Medicaid & CHIP Monthly Applications, Eligibility Determinations, and Enrollment Reports from CMS for all 50 states and DC. Note that several states have revised monthly enrollment data as far back as June 2017 to better align with reporting criteria for the CMS, Medicaid & CHIP Monthly Applications, Eligibility Determinations, and Enrollment Reports. Data for months prior to June 2017 have not been revised and may use slightly different criteria for reporting monthly enrollment and generally result in larger enrollment totals.
Medicaid Spending Growth: For FY 2024 and FY 2025, annual rates of growth for Medicaid spending were calculated as weighted averages across all states. 50 states reported Medicaid expenditure growth rates for FY 2024 and FY 2025. Weights for spending were derived from net Medicaid expenditure data (including collections and adjustments) for FY 2023 from the CMS-64 Financial Management Reports and adjusted for state fiscal years.
FY 2023 spending growth rate is also derived from net Medicaid expenditure data (including collections and adjustments) for FY 2023 from the CMS-64 Financial Management Reports, adjusted for state fiscal years. We estimate state fiscal year spending by summing 75% of spending from the same federal fiscal year with 25% of spending from the previous federal fiscal year. Historic Medicaid spending for FY 2022 and earlier are based on estimates prepared for KFF by the Urban Institute using CMS Form 64 reports.
Definition of Medicaid Spending. Total Medicaid spending includes all payments to Medicaid providers for Medicaid-covered services provided to enrolled Medicaid beneficiaries. Medicaid spending also includes special disproportionate share hospital (DSH) payments that subsidize uncompensated hospital care for persons who are uninsured and unreimbursed costs of care for persons on Medicaid. Total Medicaid spending does not include Medicaid administrative costs and federally mandated state “Clawback” payments to help finance the Medicare Part D prescription drug benefit for Medicaid beneficiaries who are also enrolled in Medicare. States are also asked to exclude costs for the Children’s Health Insurance Program (CHIP). Total Medicaid spending includes payments financed from all sources, including state funds, local contributions, and federal matching funds. Historical state Medicaid spending refers to all non-federal spending, which may include local funds and provider taxes and fees as well as state general fund dollars.
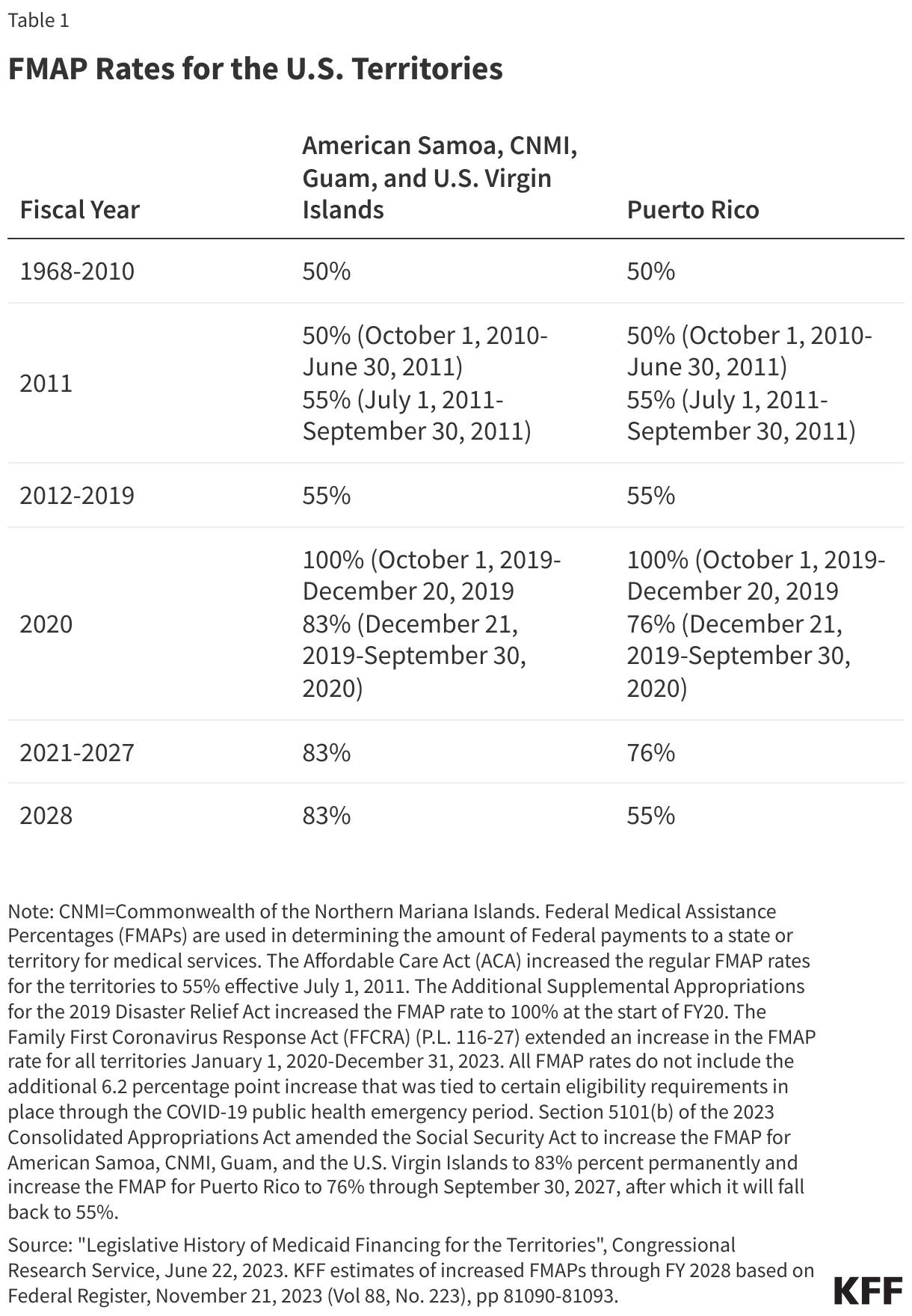
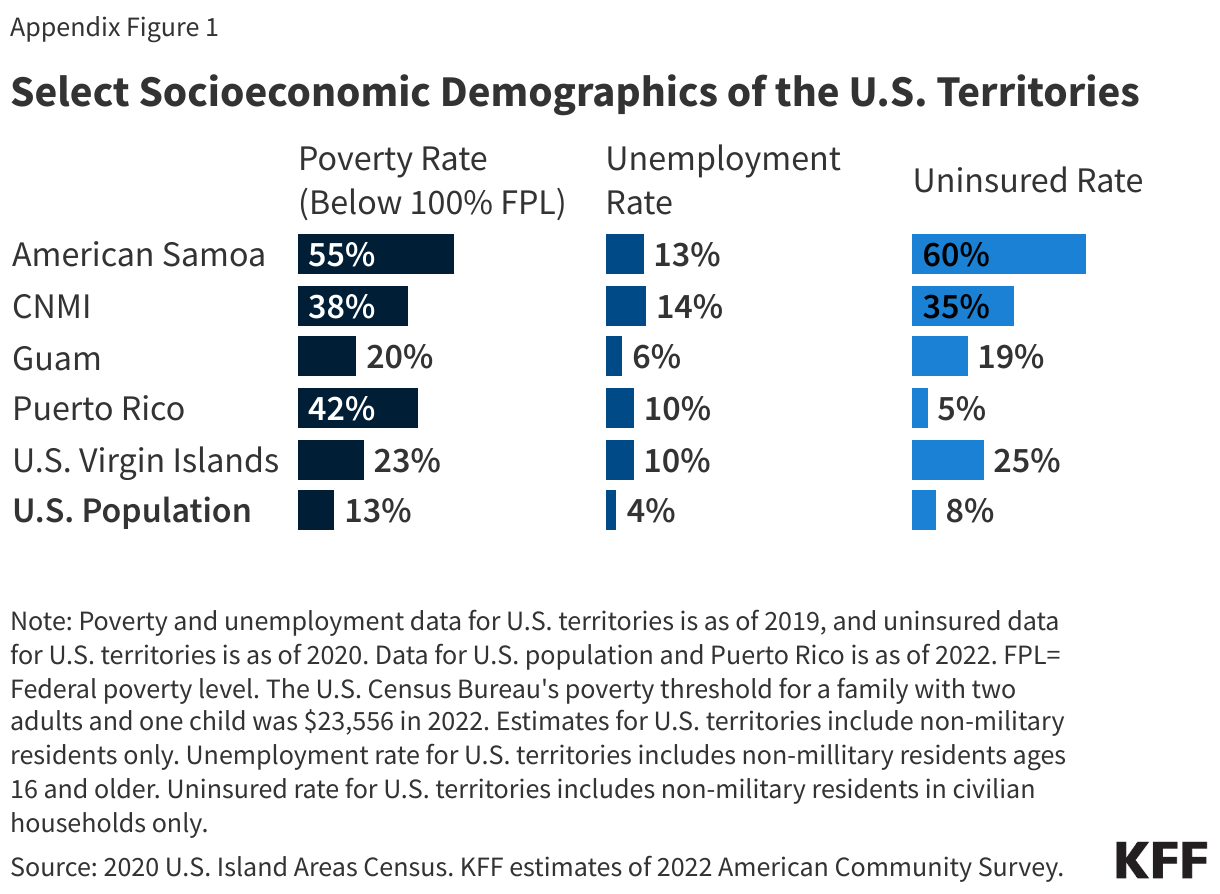
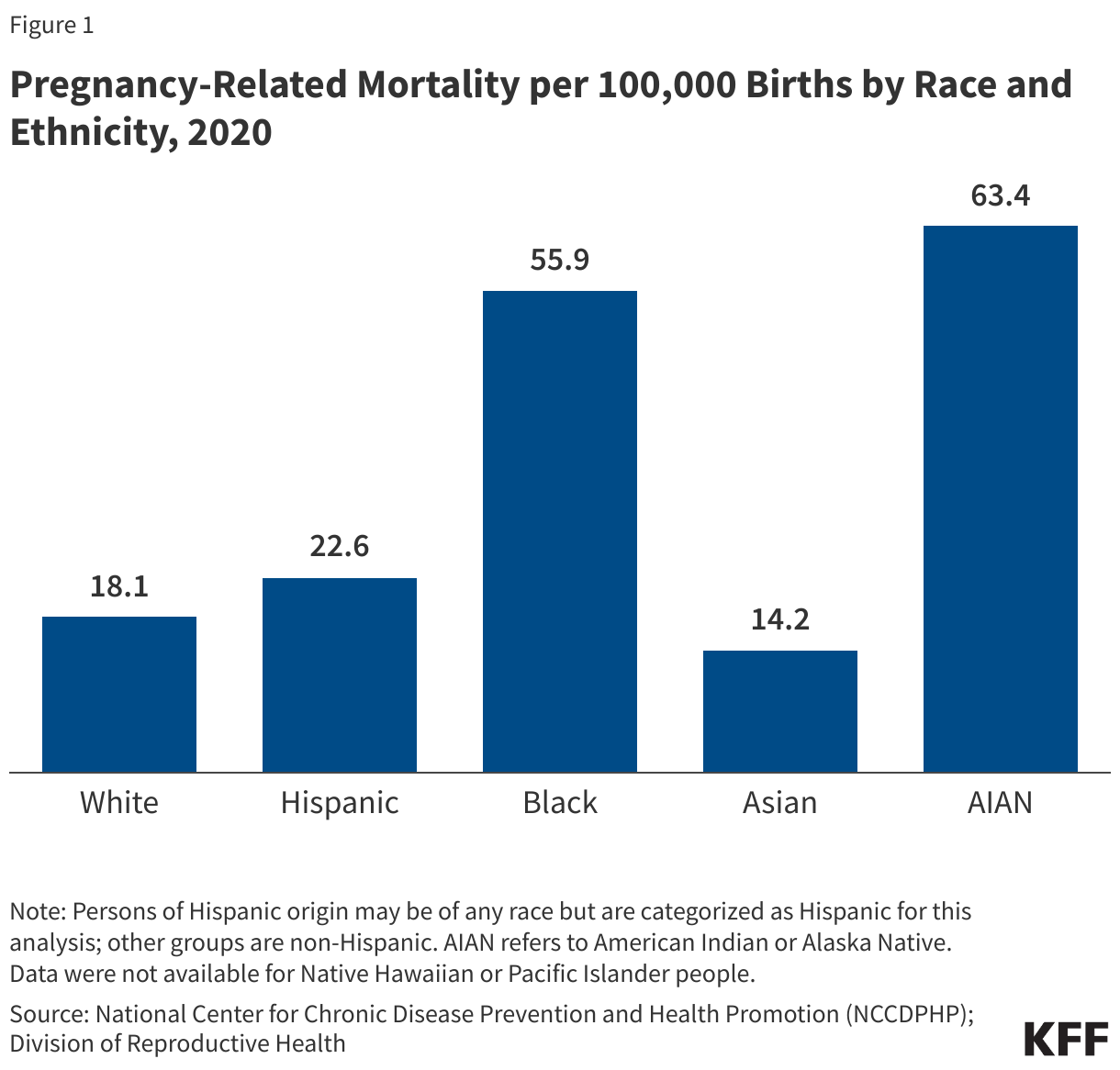
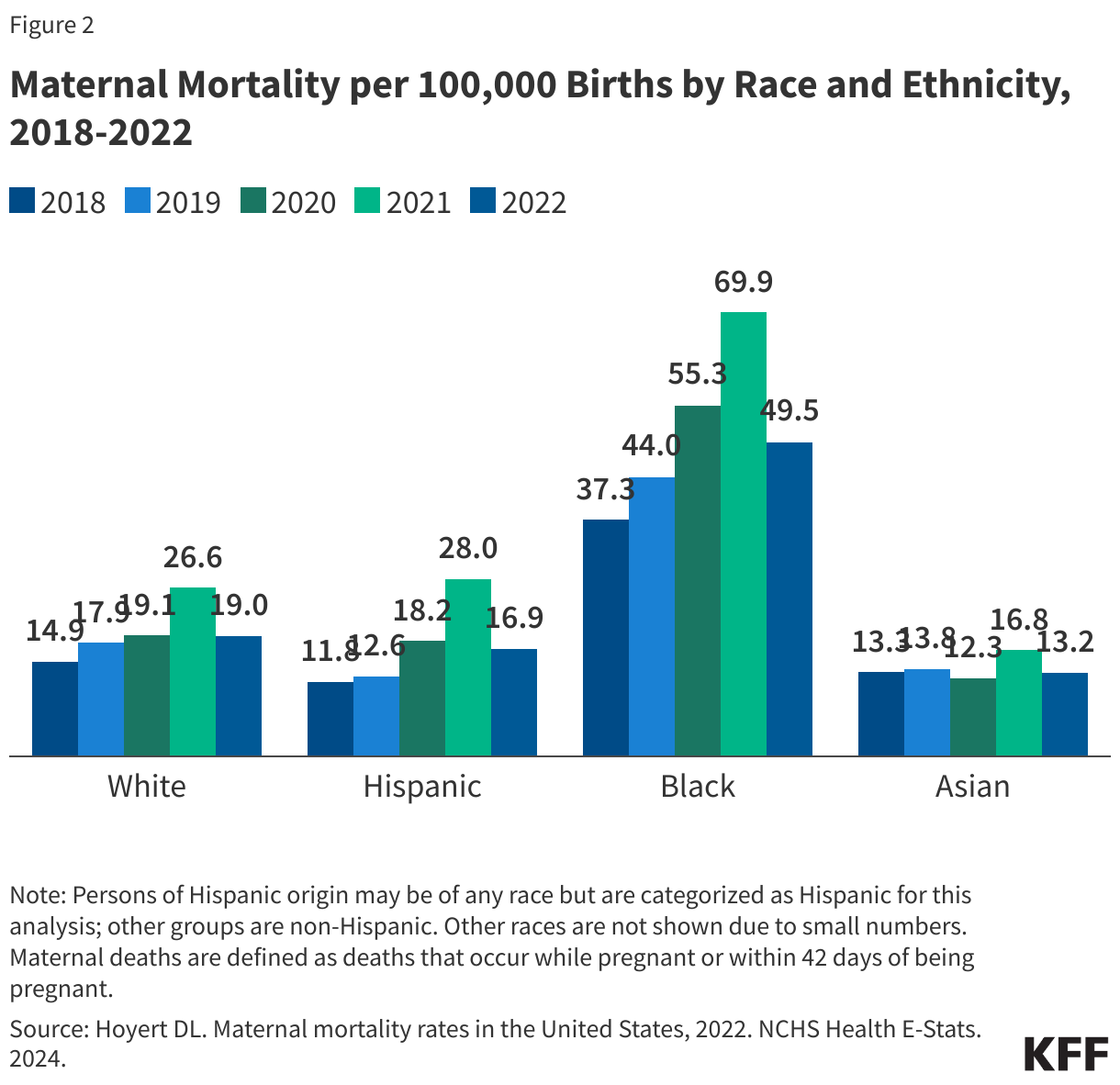
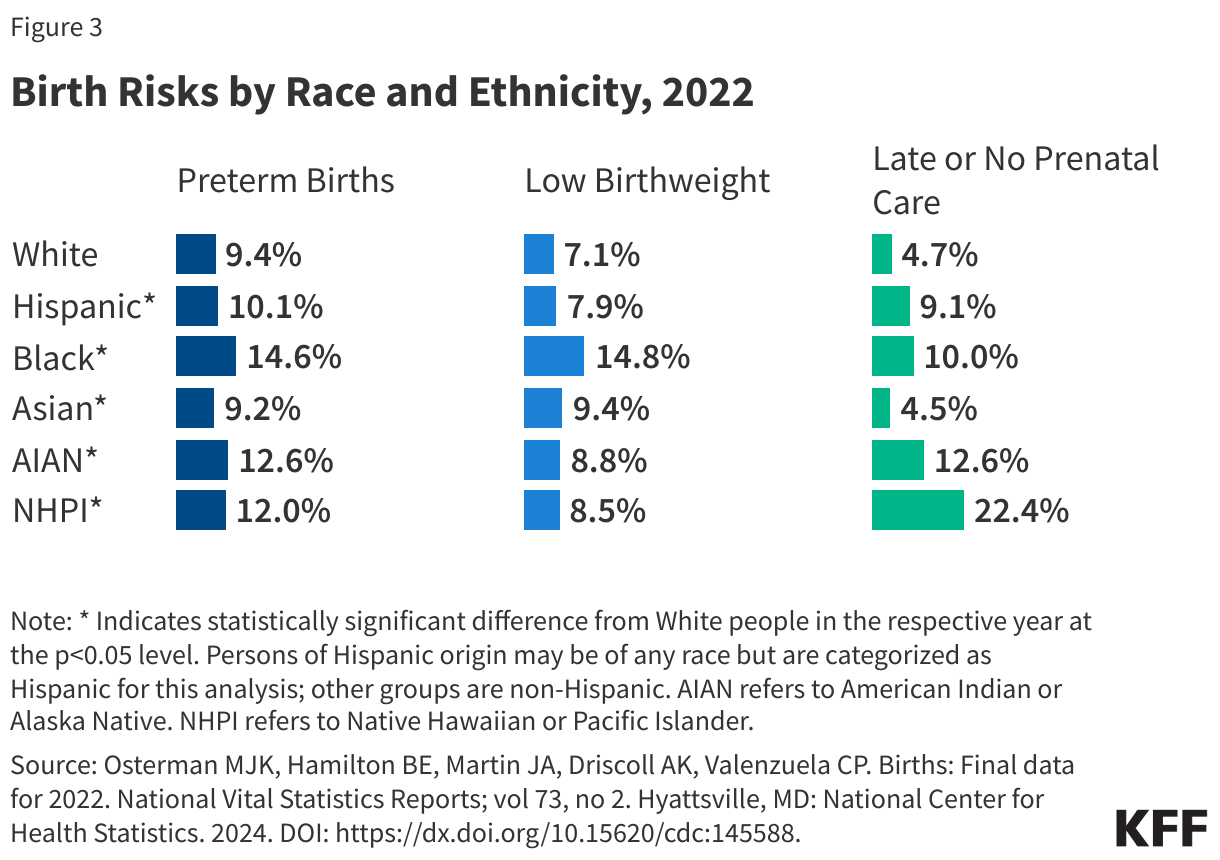
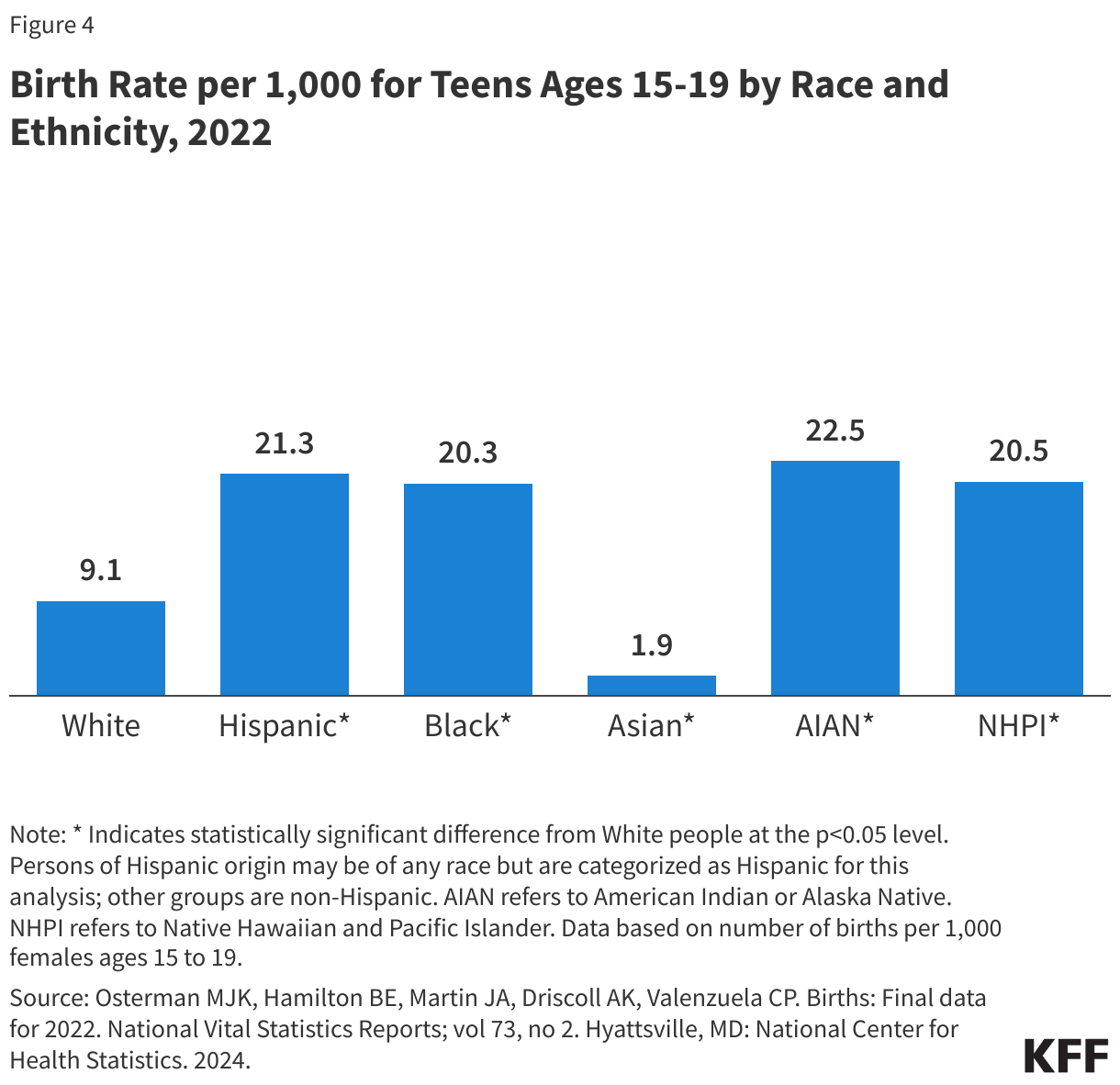
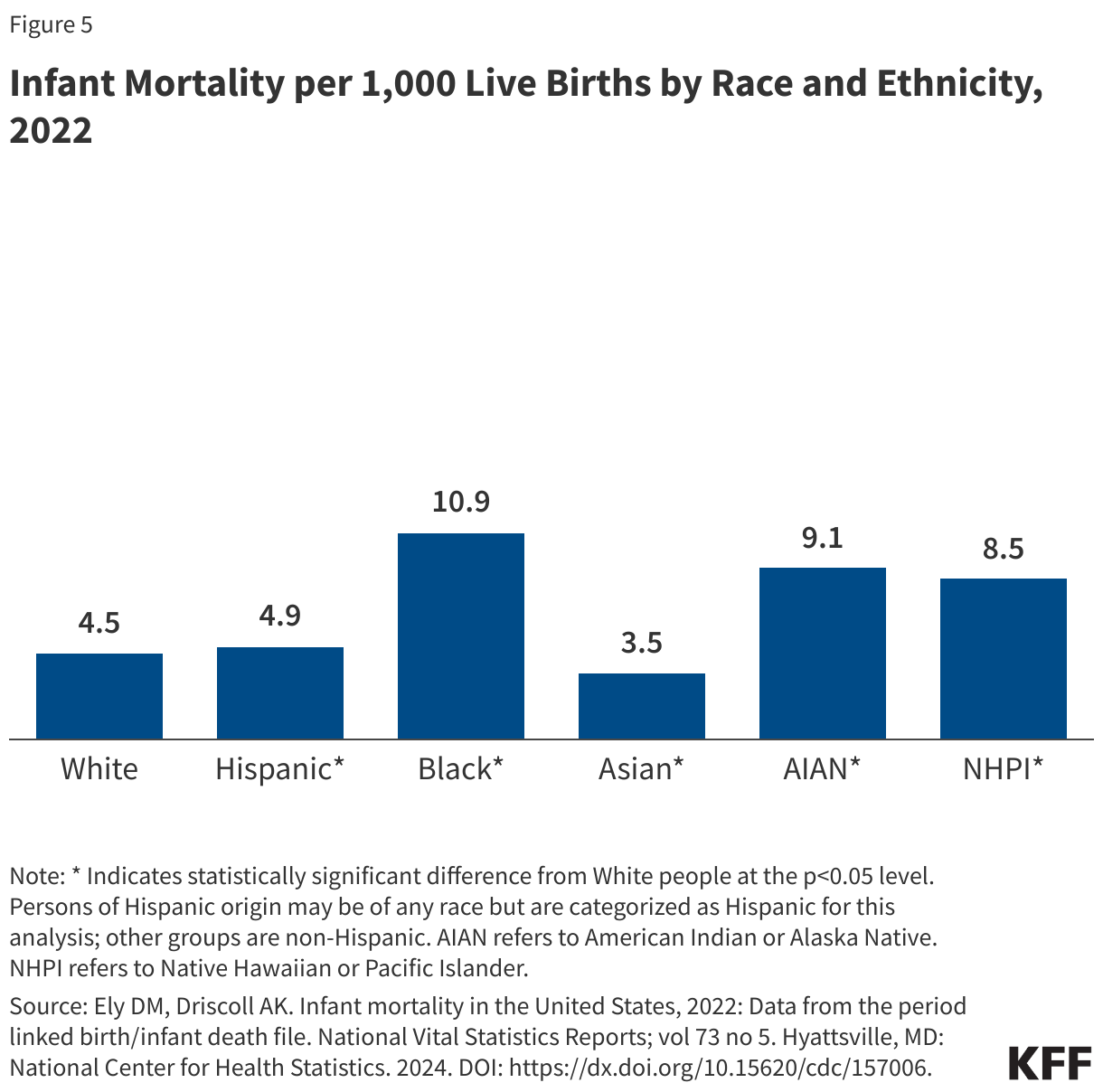
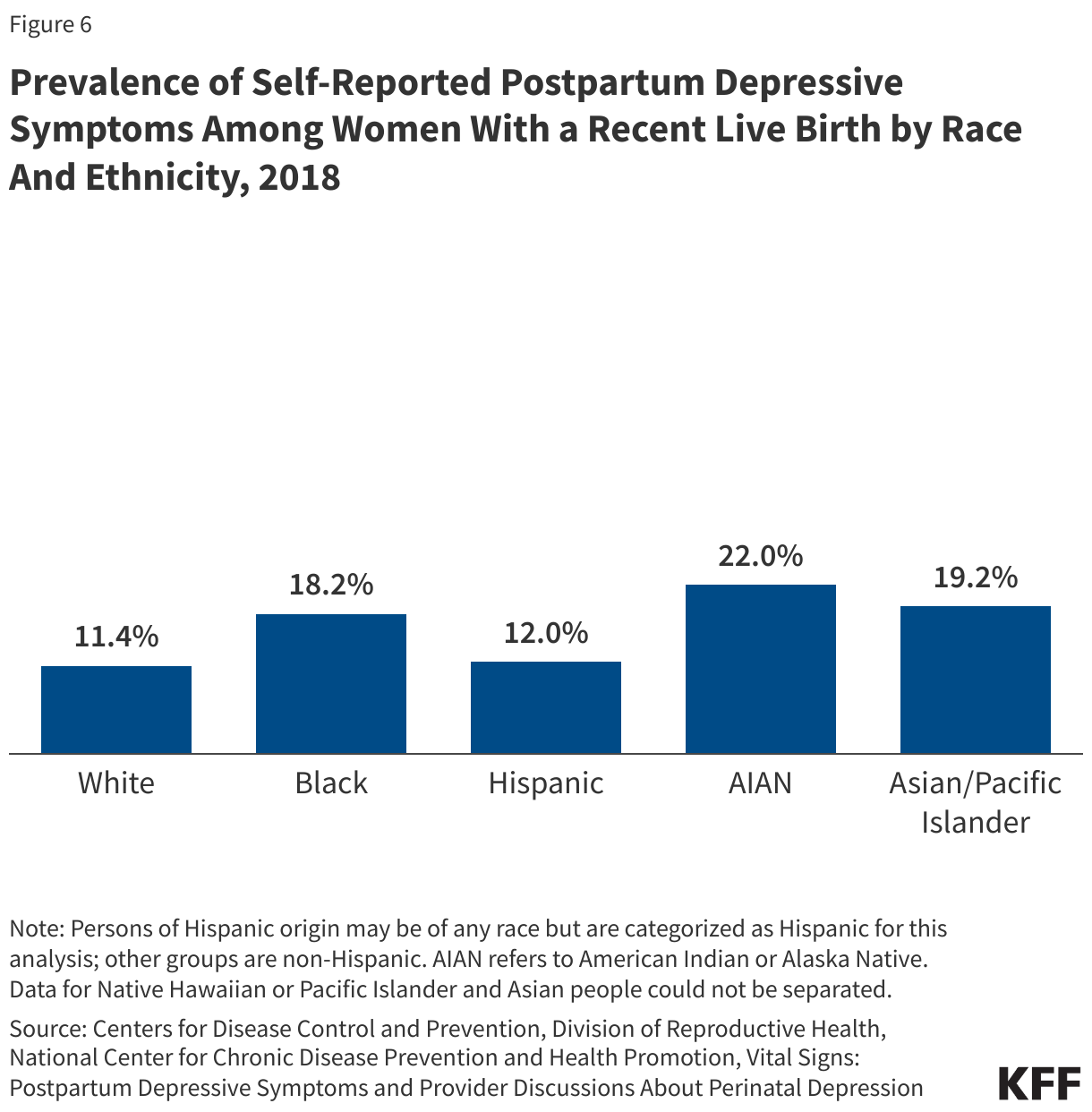
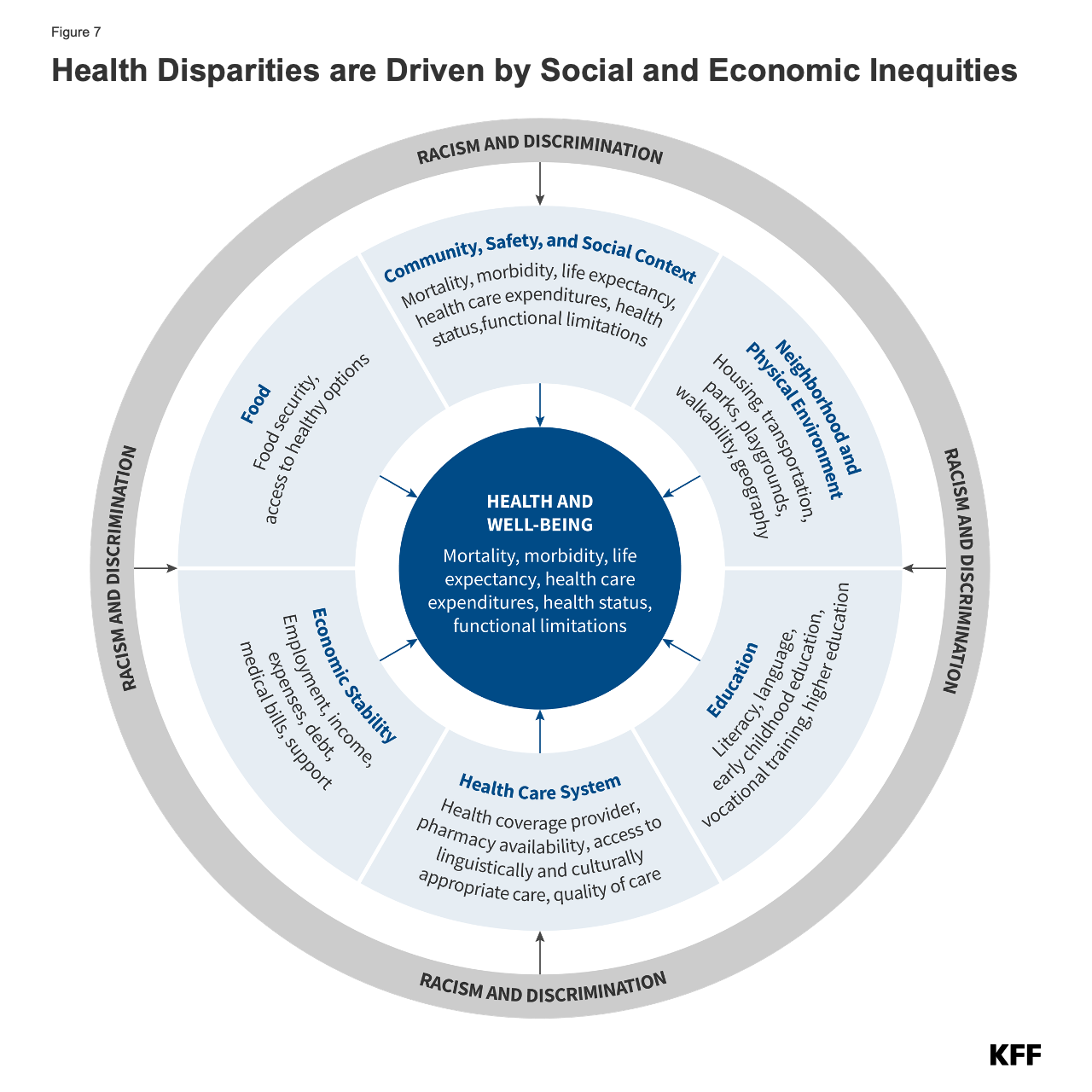
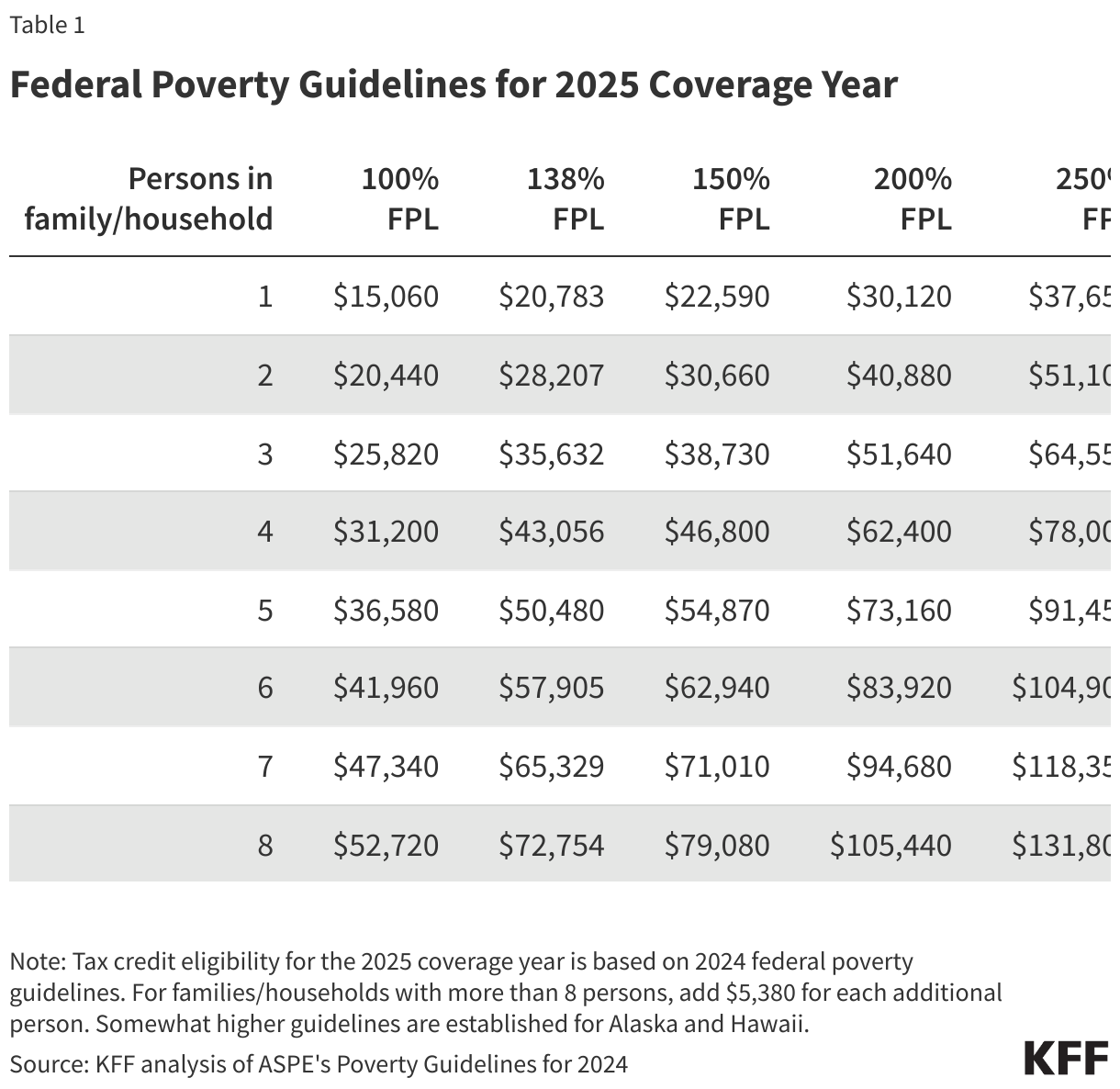
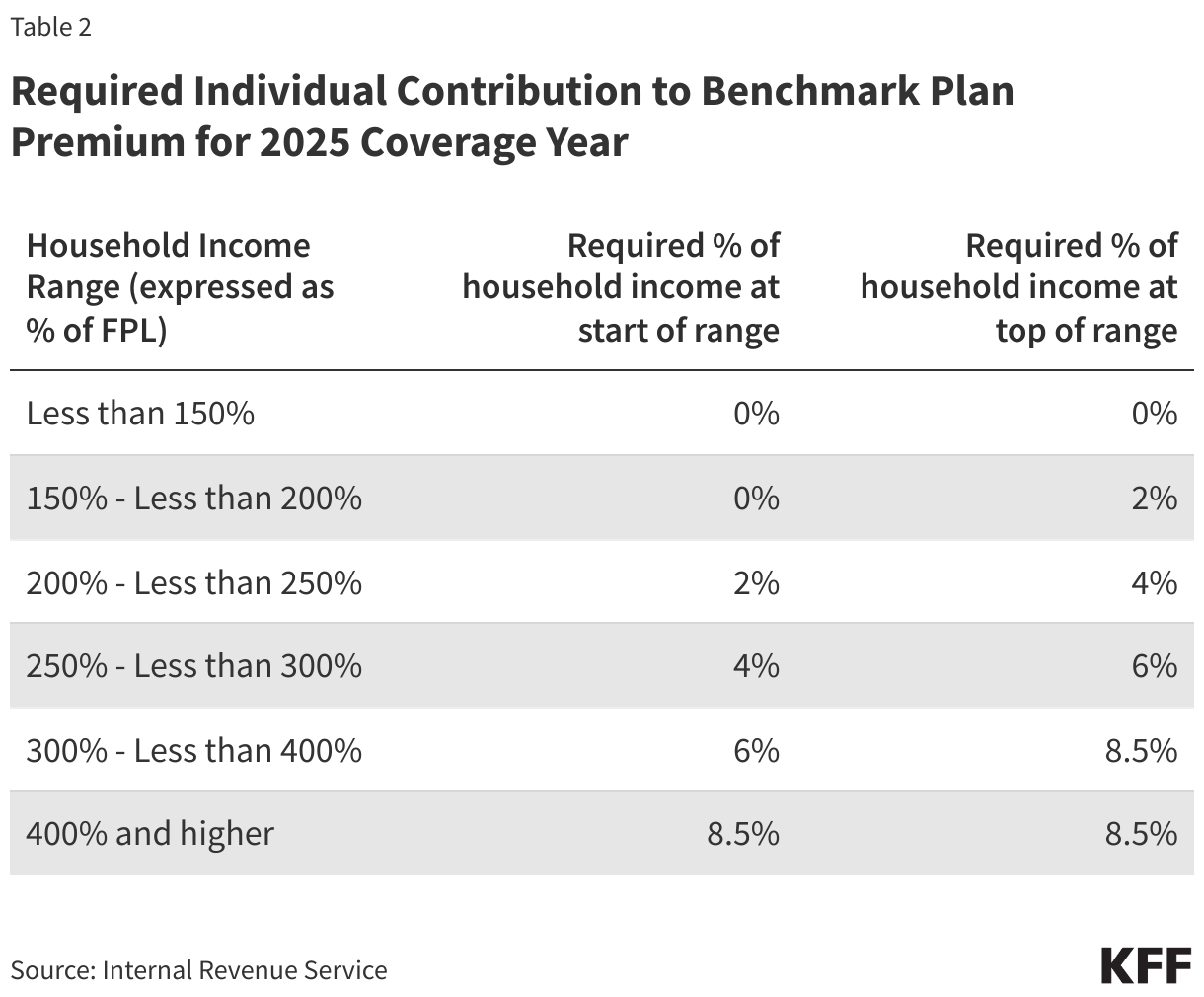
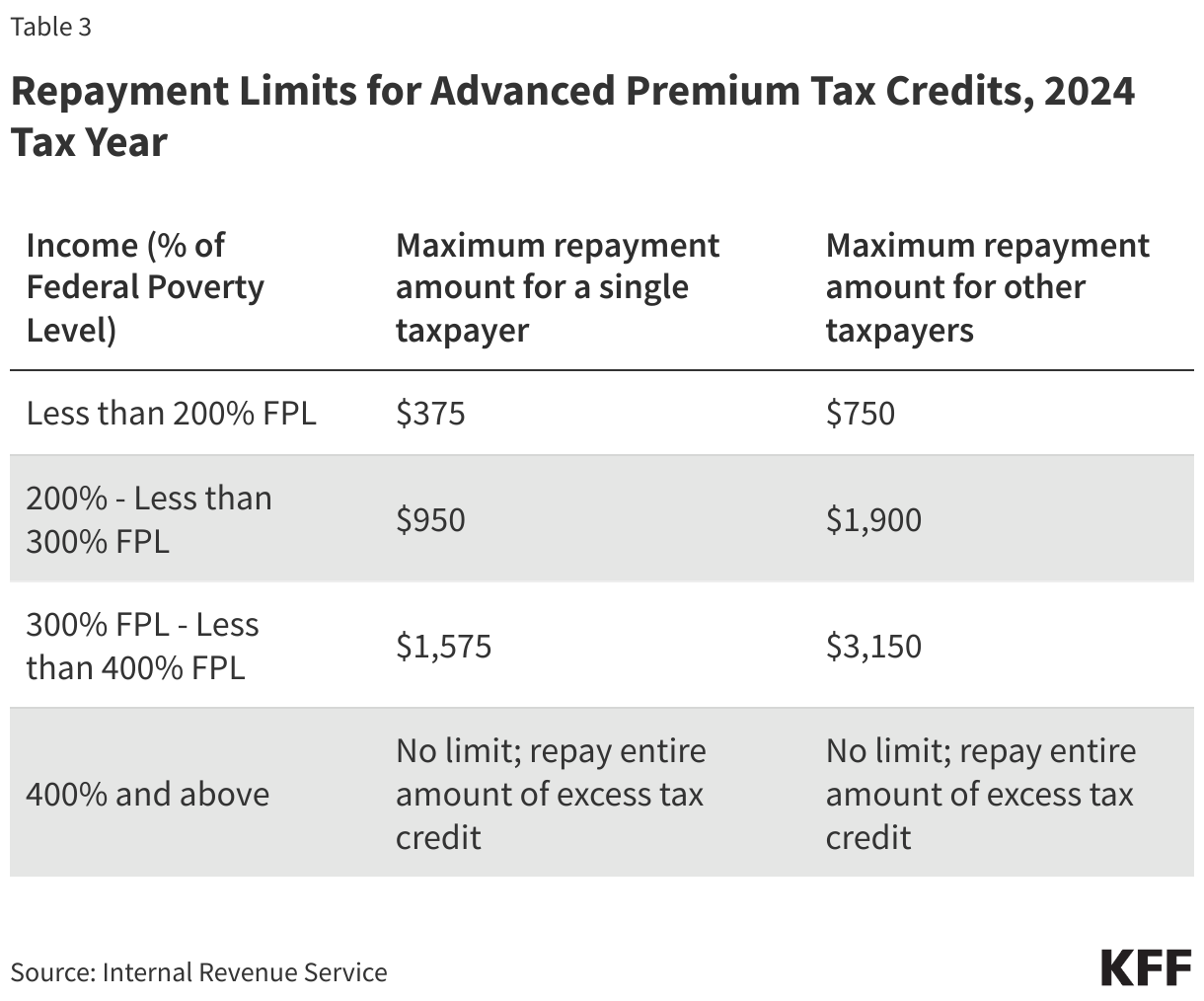
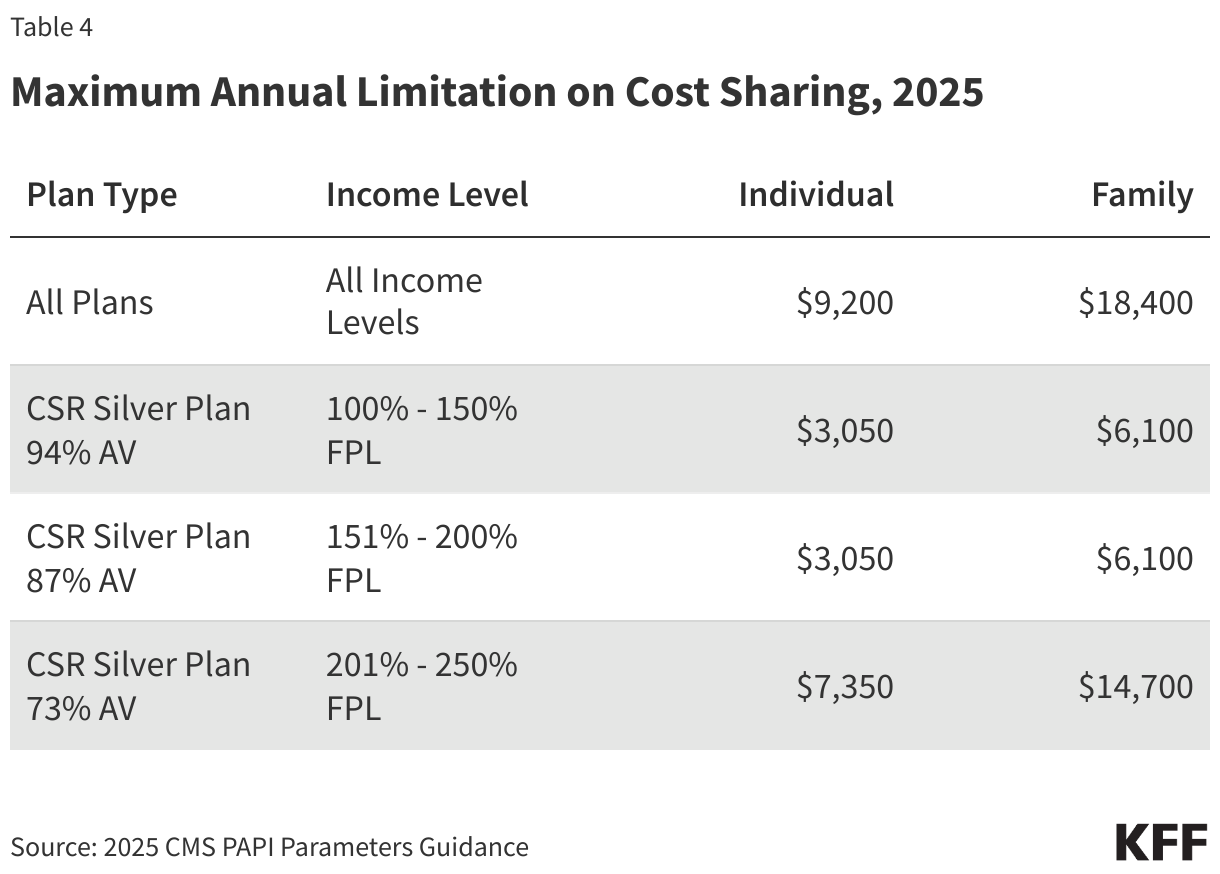
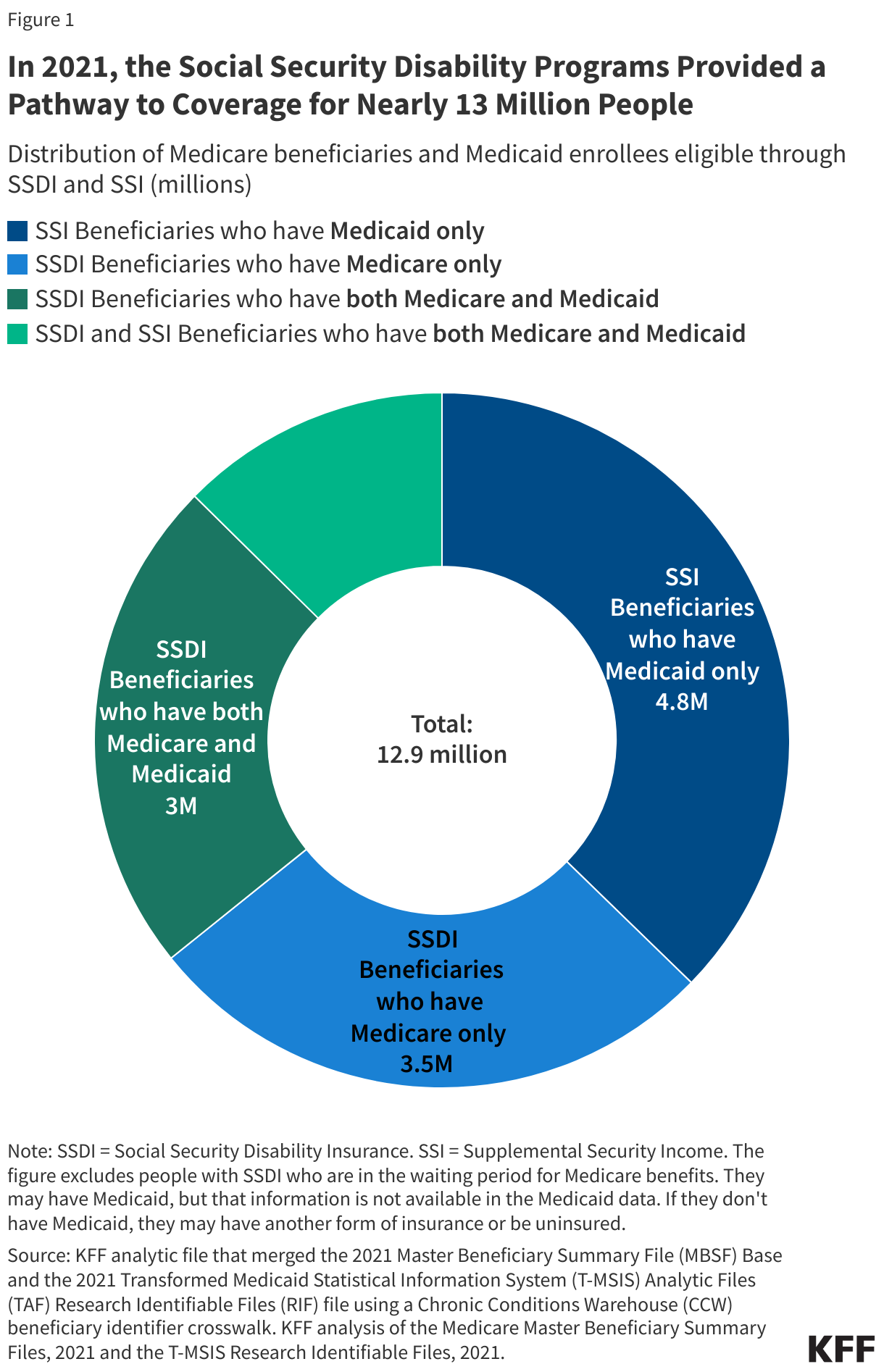
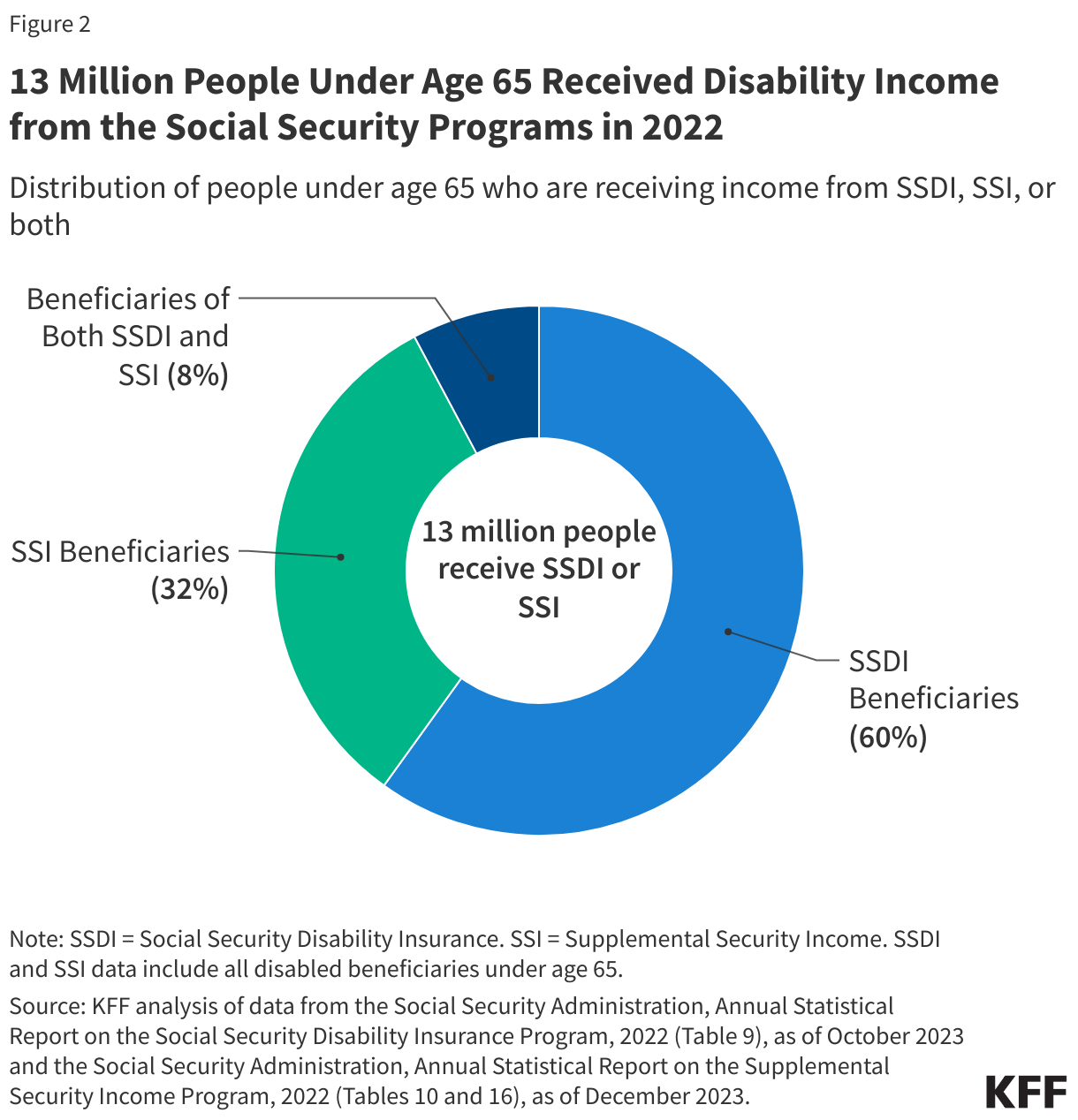
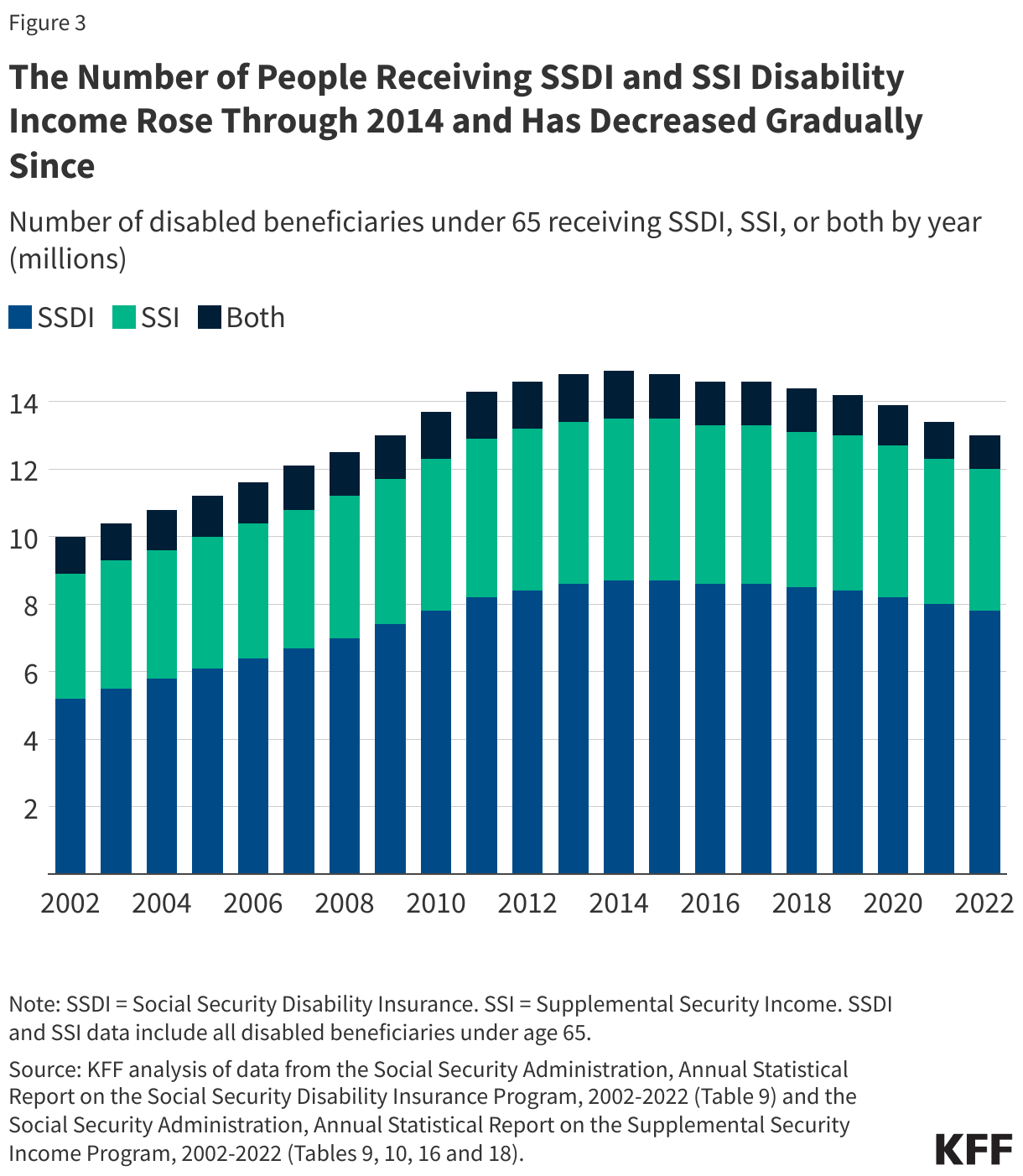
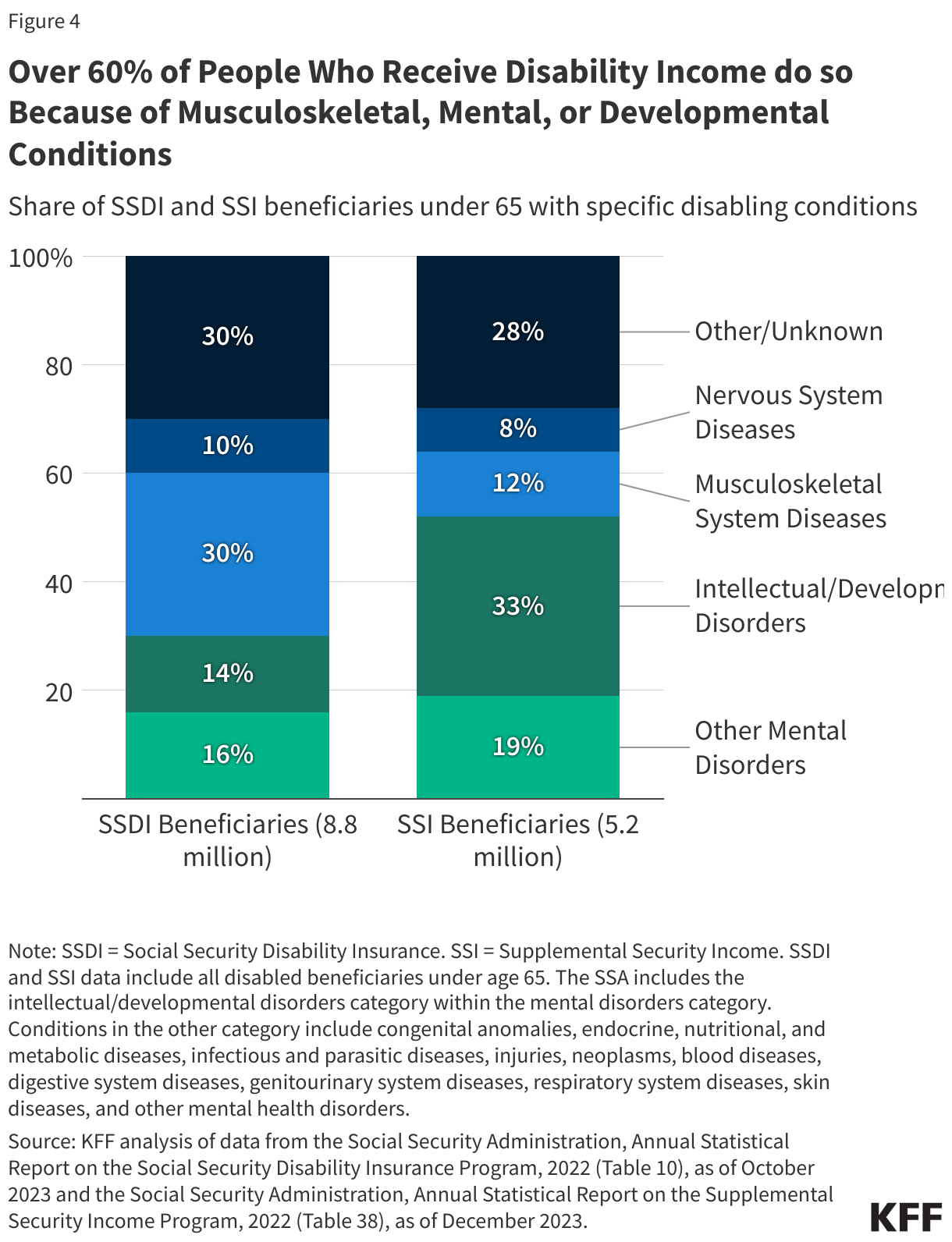
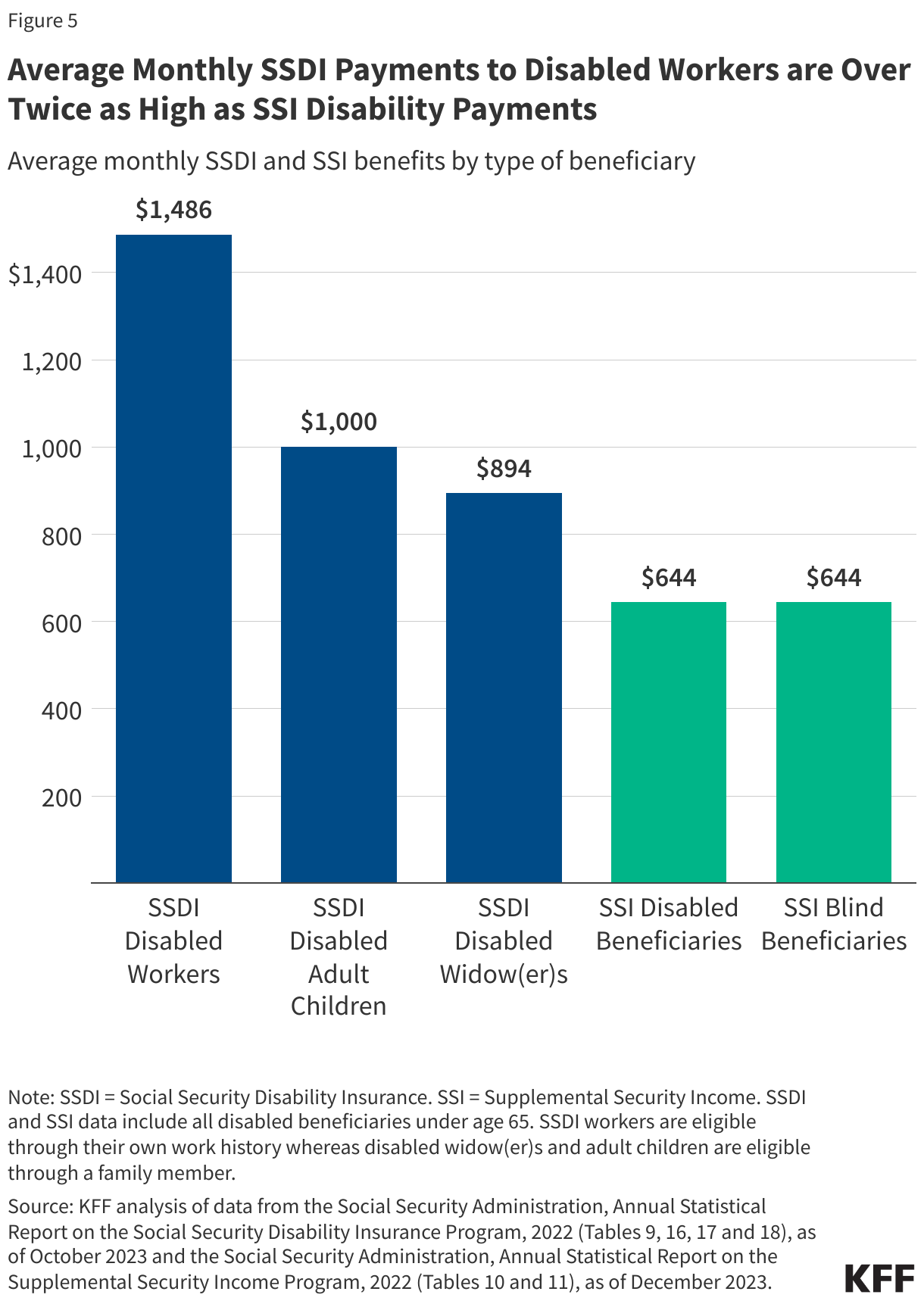
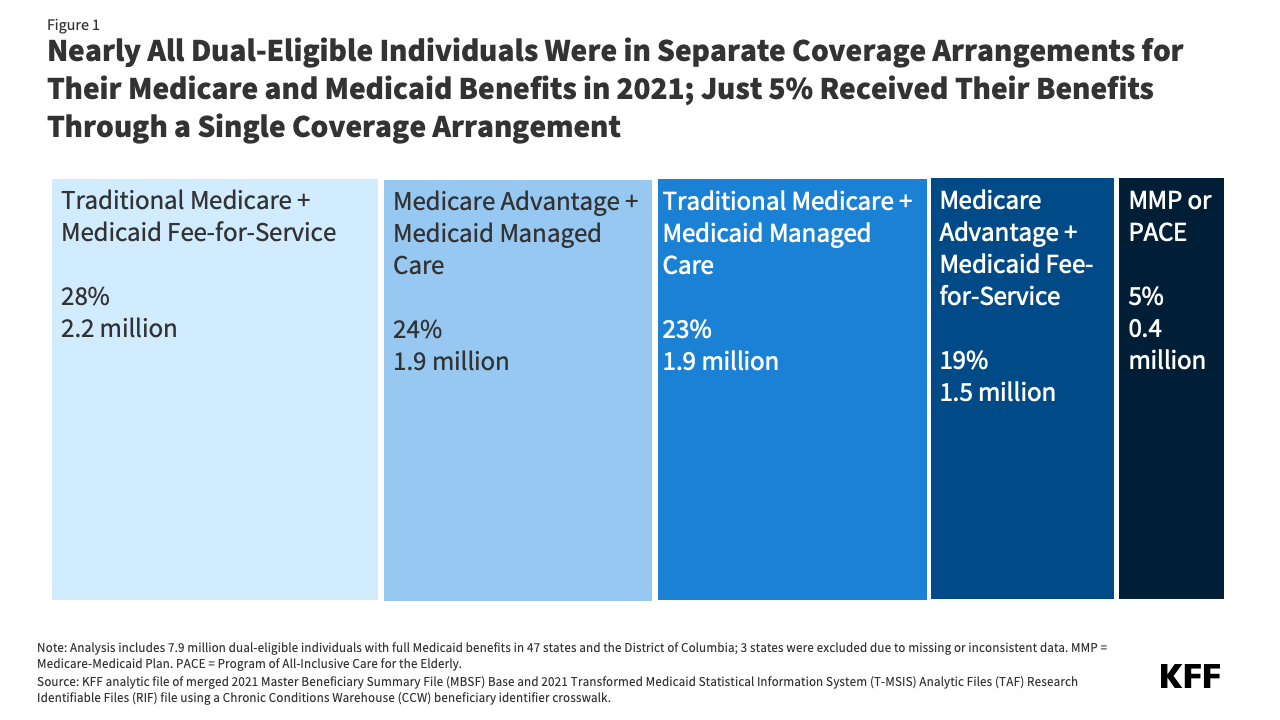
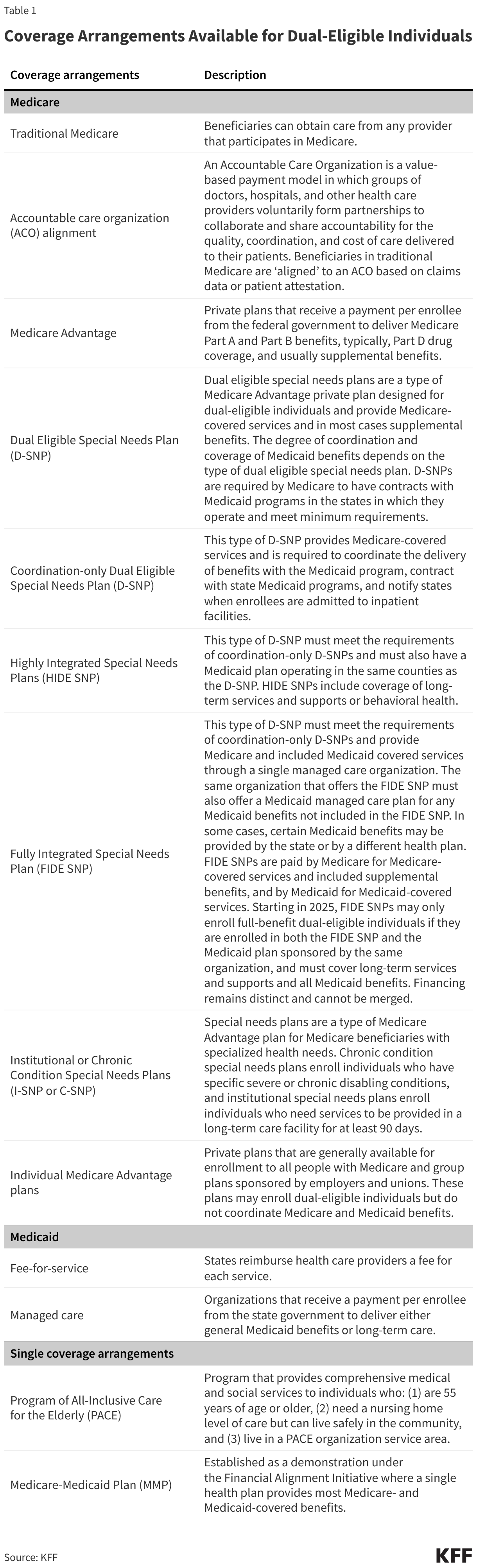
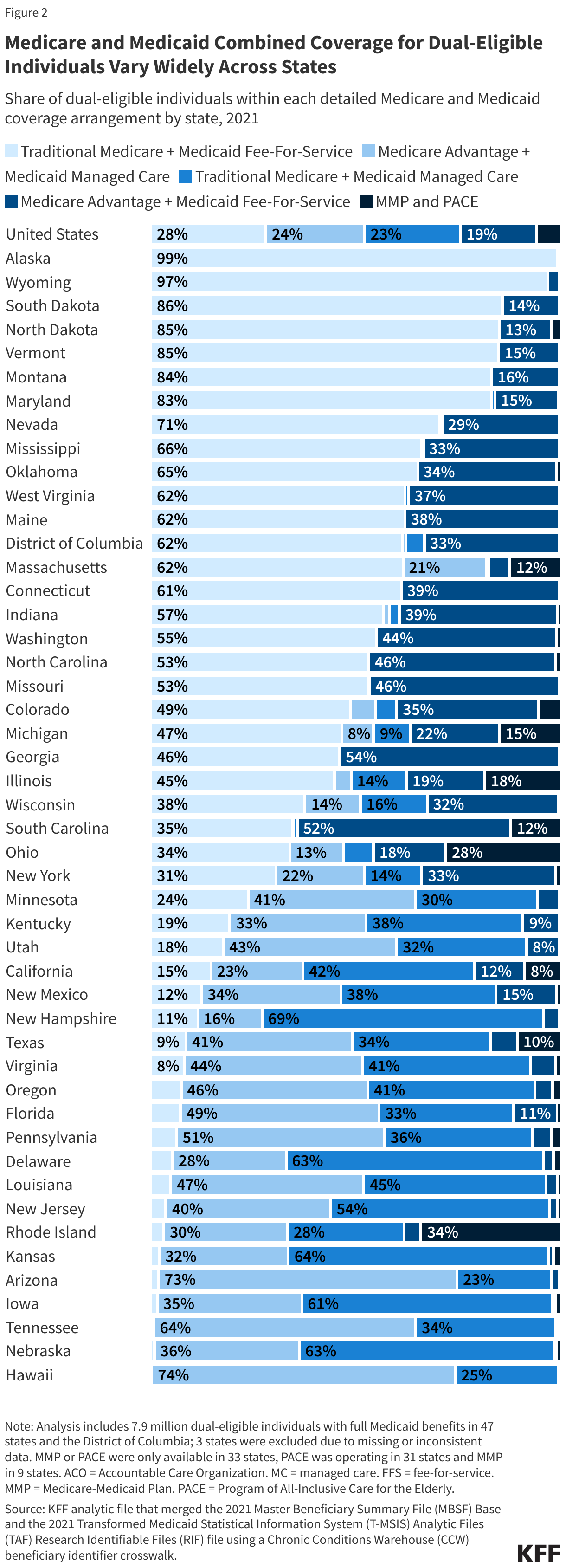
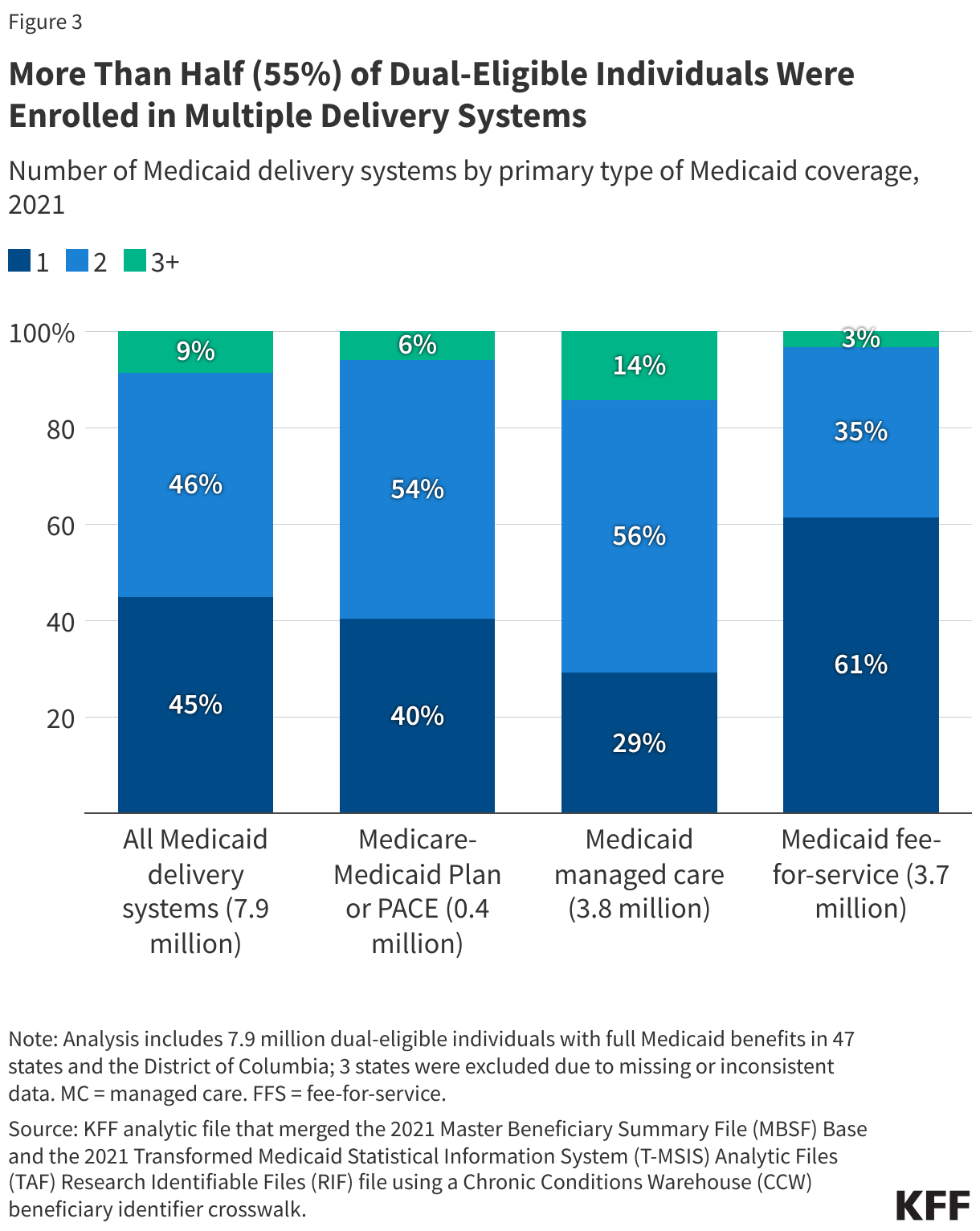
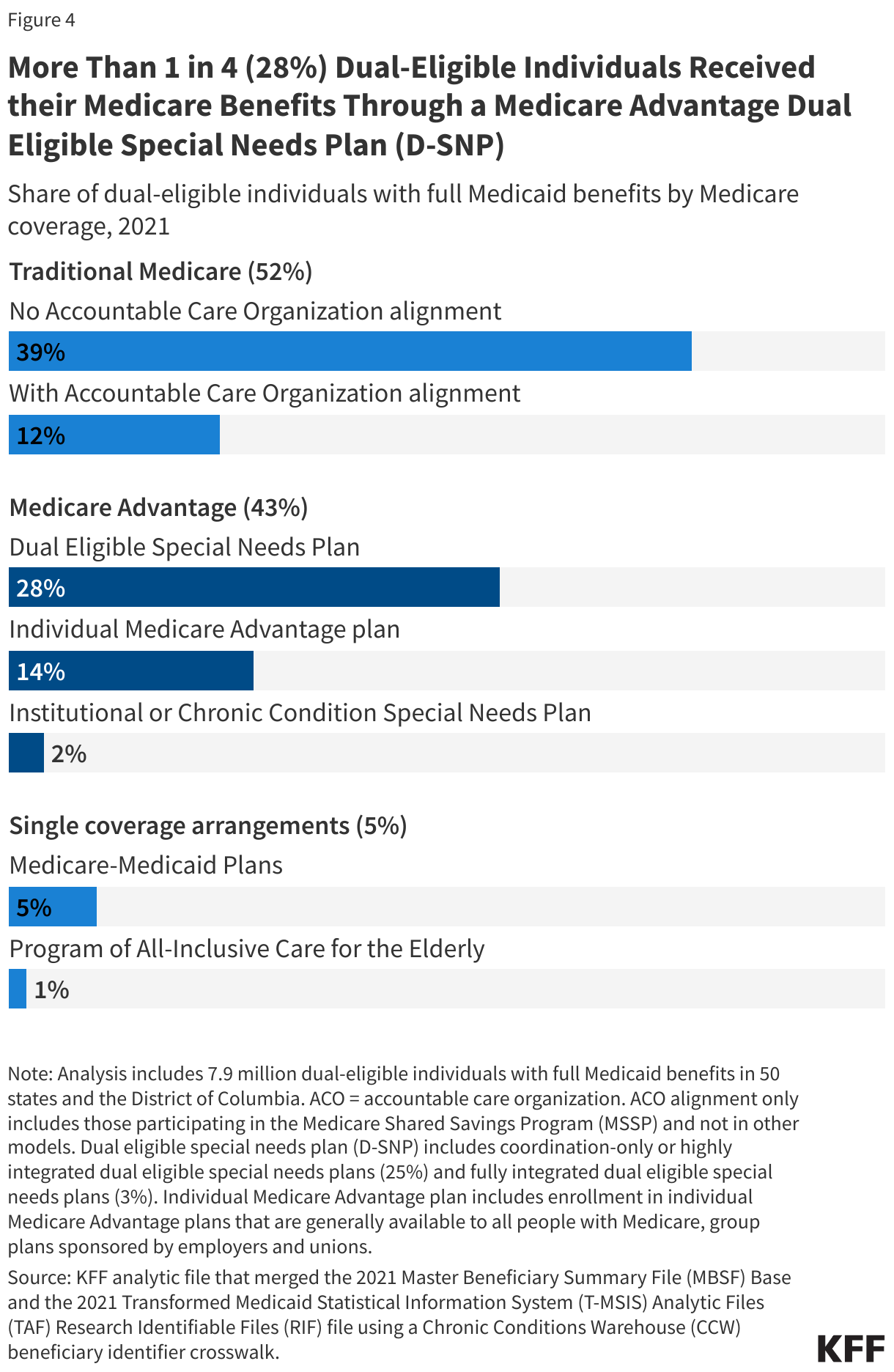
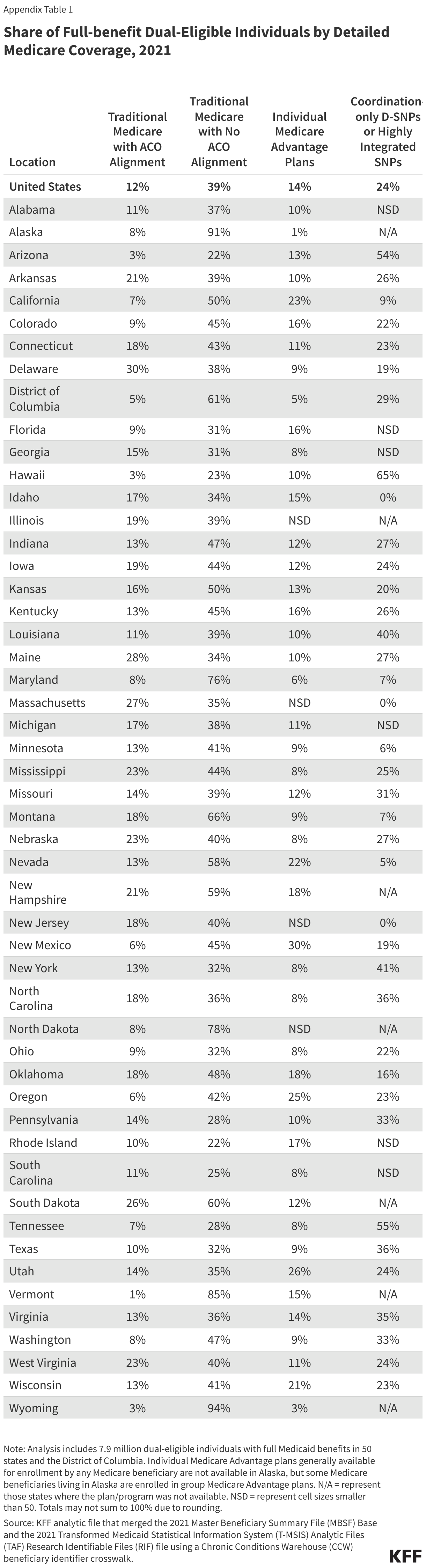
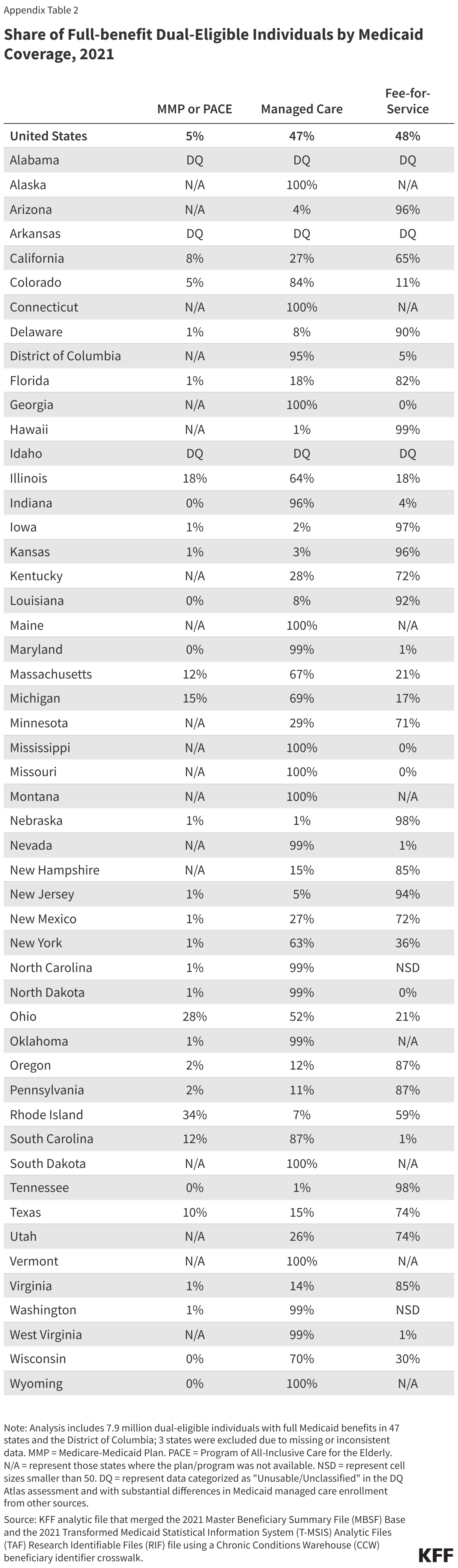
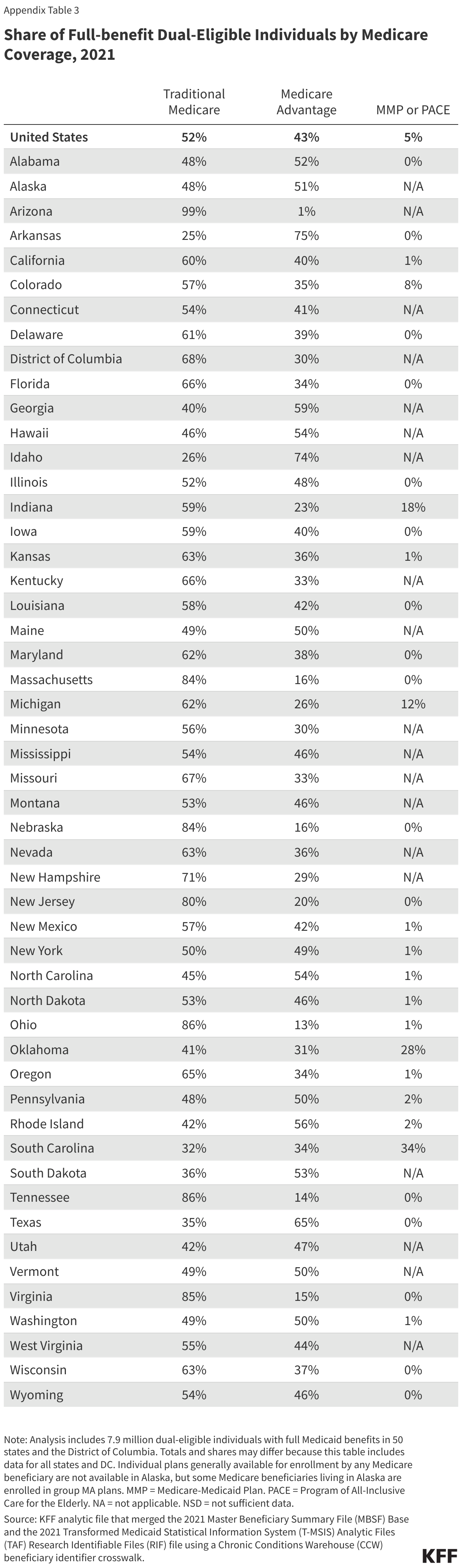
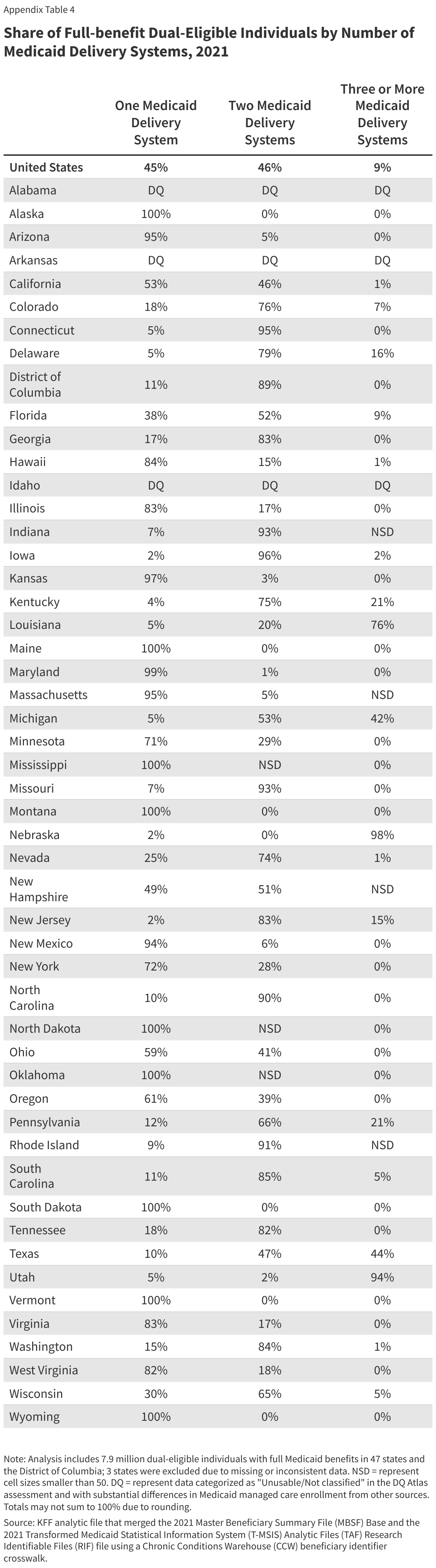
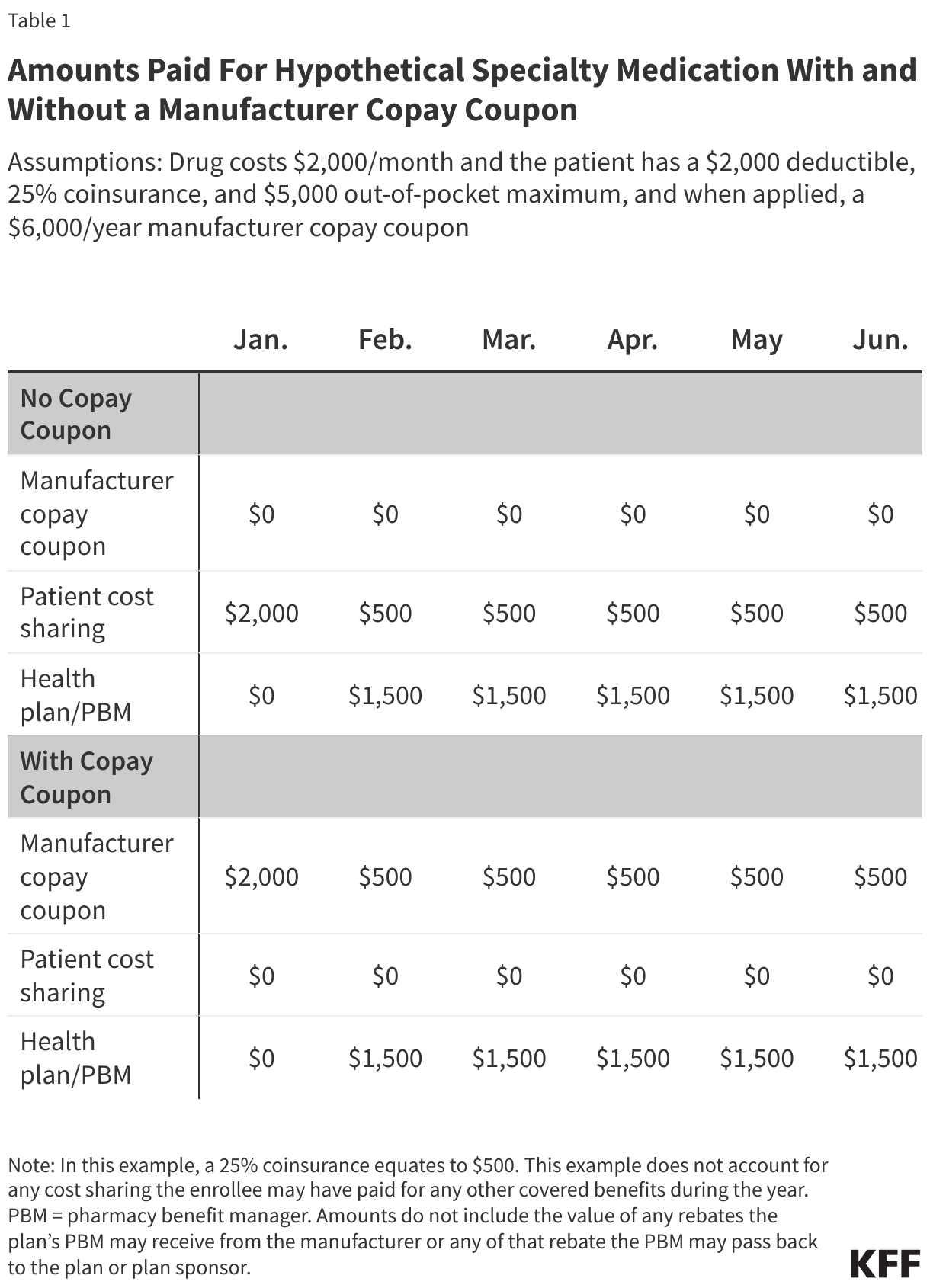
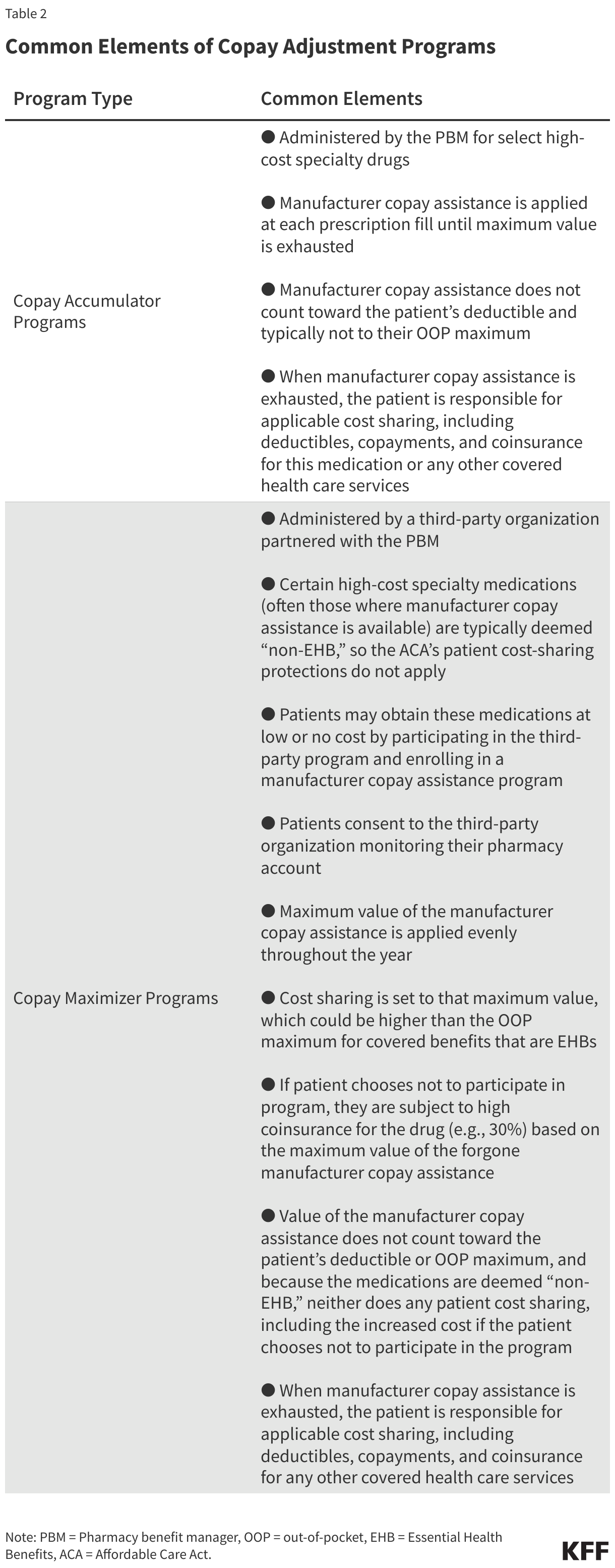
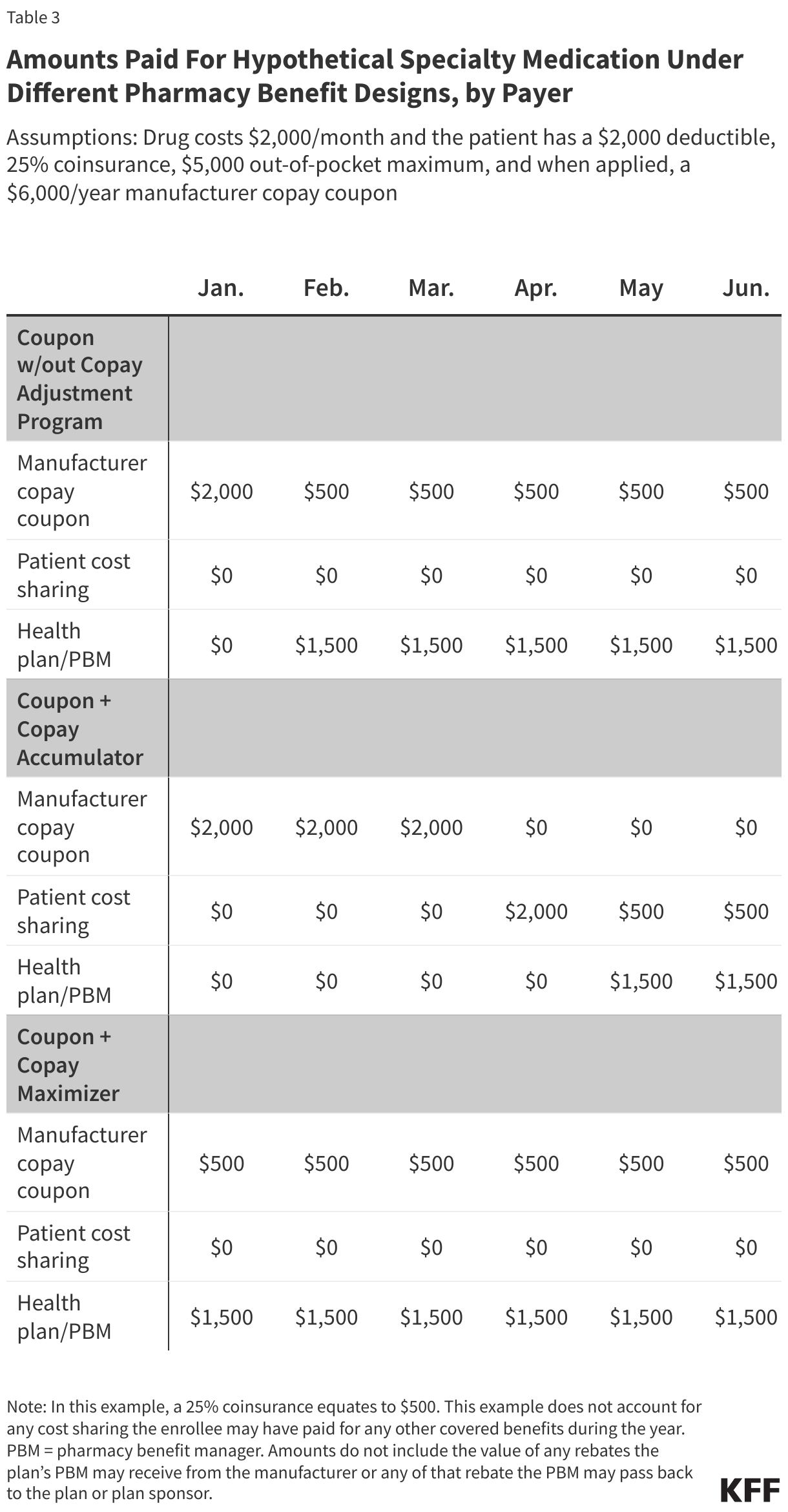
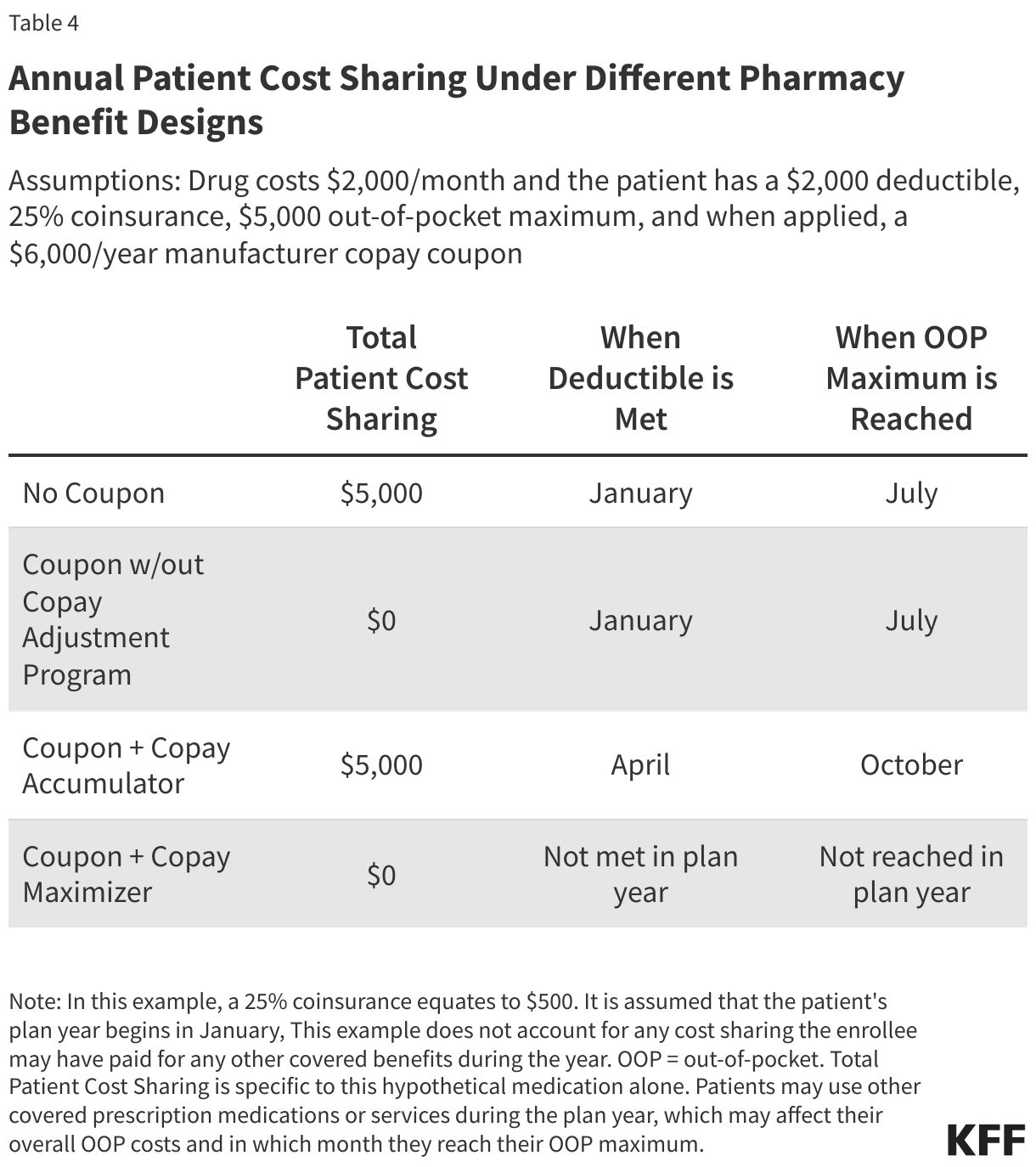
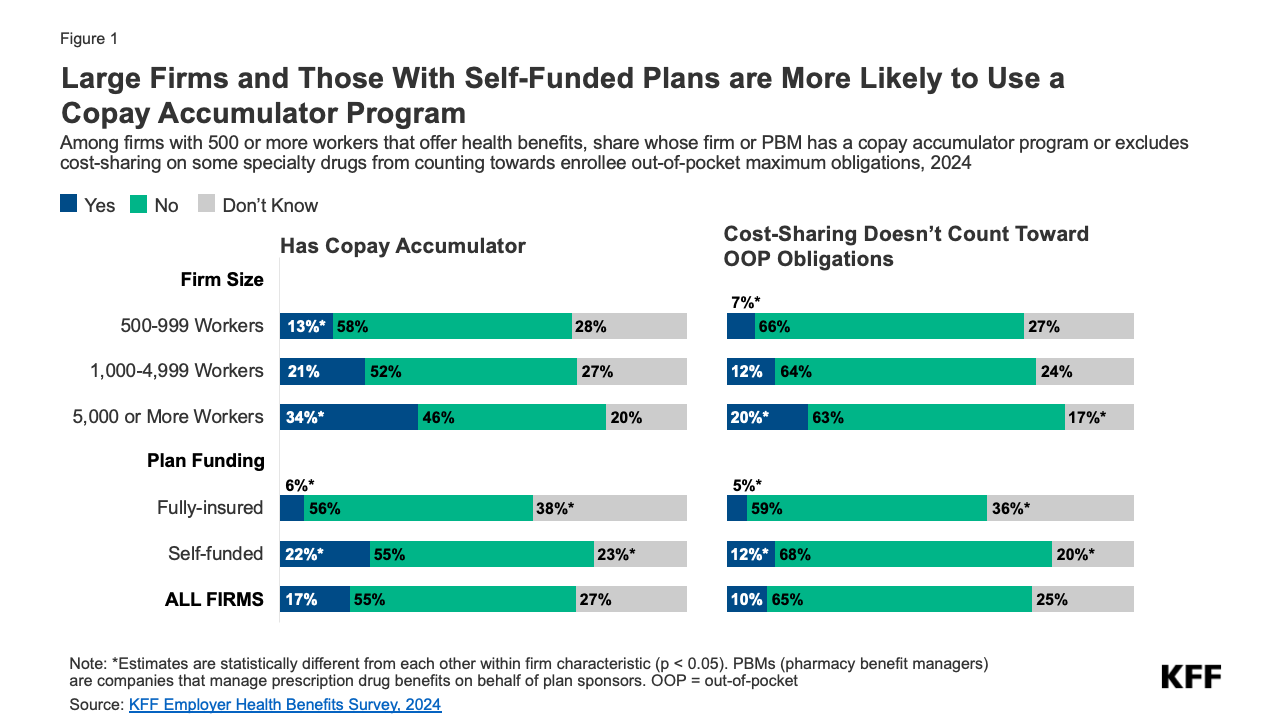
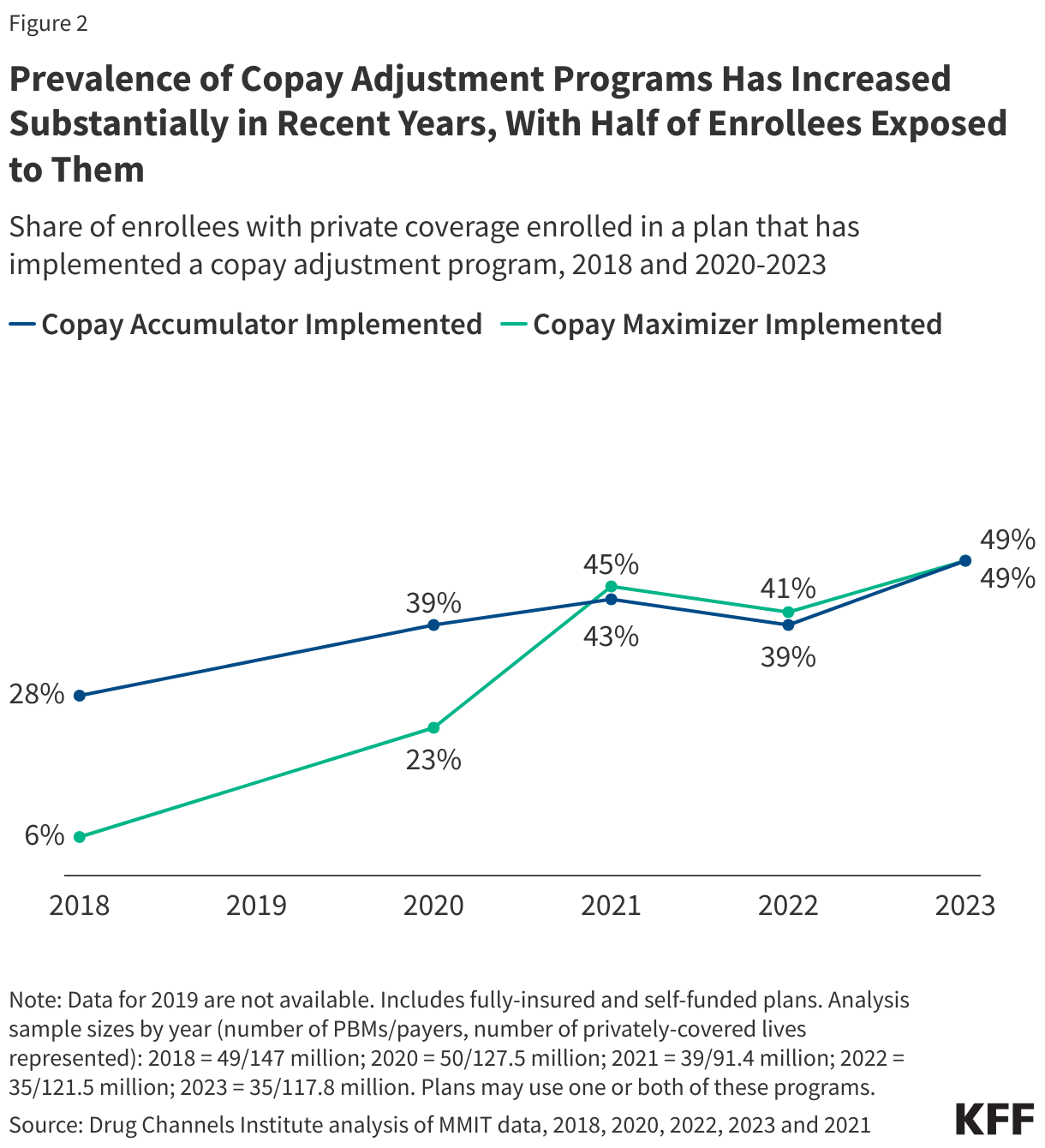
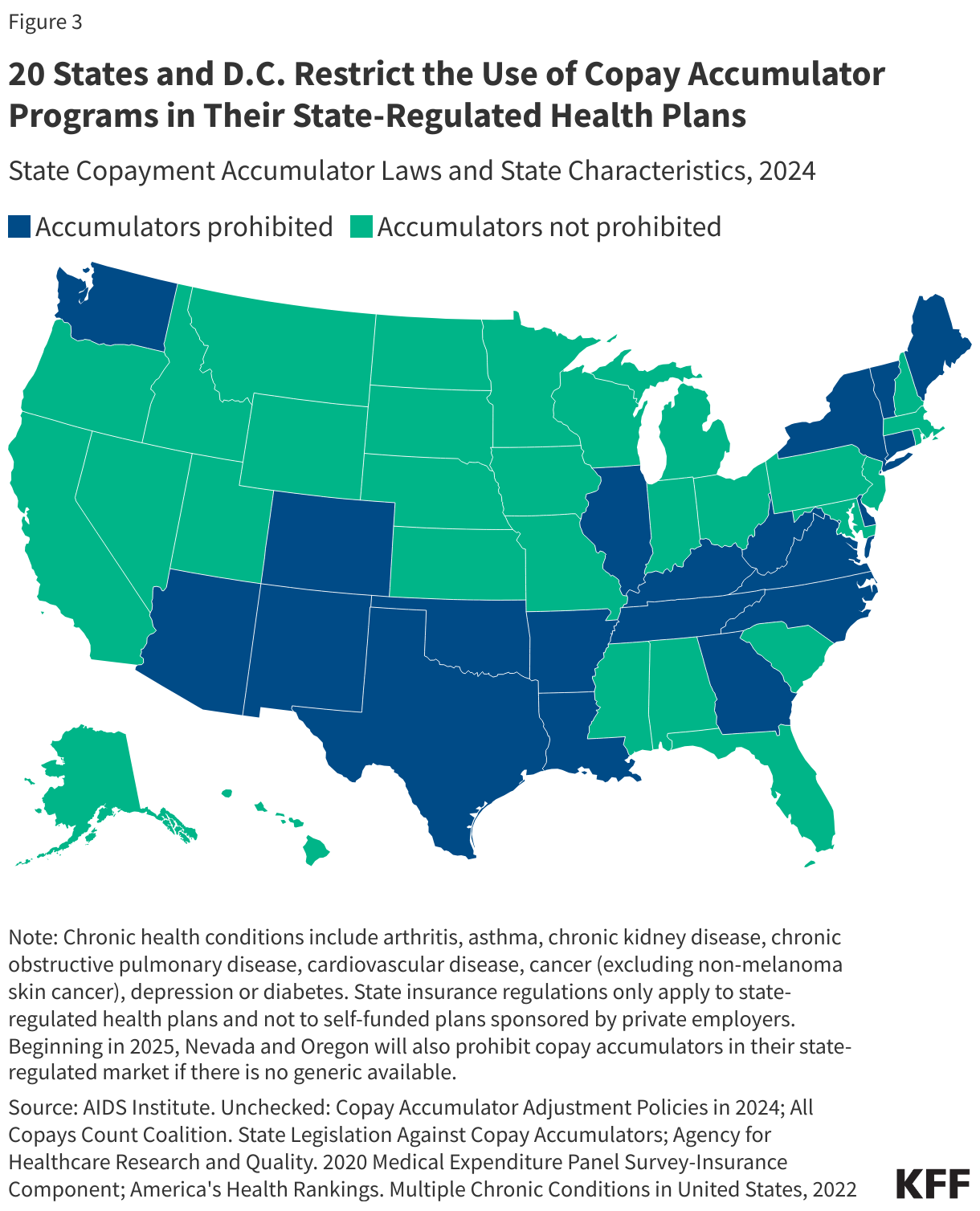


 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma