Medicaid Enrollment Patterns During the Postpartum Year
Executive Summary
The Medicaid program finances about 4 in 10 births in the U.S. each year and a majority of births in some states. Federal law requires states to provide pregnancy-related Medicaid coverage through 60 days postpartum. After the 60-day postpartum period, however, some enrollees lose coverage if their income is too high to continue qualifying for Medicaid through another eligibility pathway. Rising maternal mortality rates, along with the recent Supreme Court decision to overturn Roe v Wade, have increased attention on Medicaid coverage for pregnant people. A provision in the American Rescue Plan Act (ARPA) of 2021 gives states a new option to extend Medicaid postpartum coverage to 12 months via a state plan amendment (SPA). This new option took effect on April 1, 2022 and is available to states for five years. Using Medicaid claims data from 2018, this brief examines enrollment patterns in the year following childbirth. Key findings include:
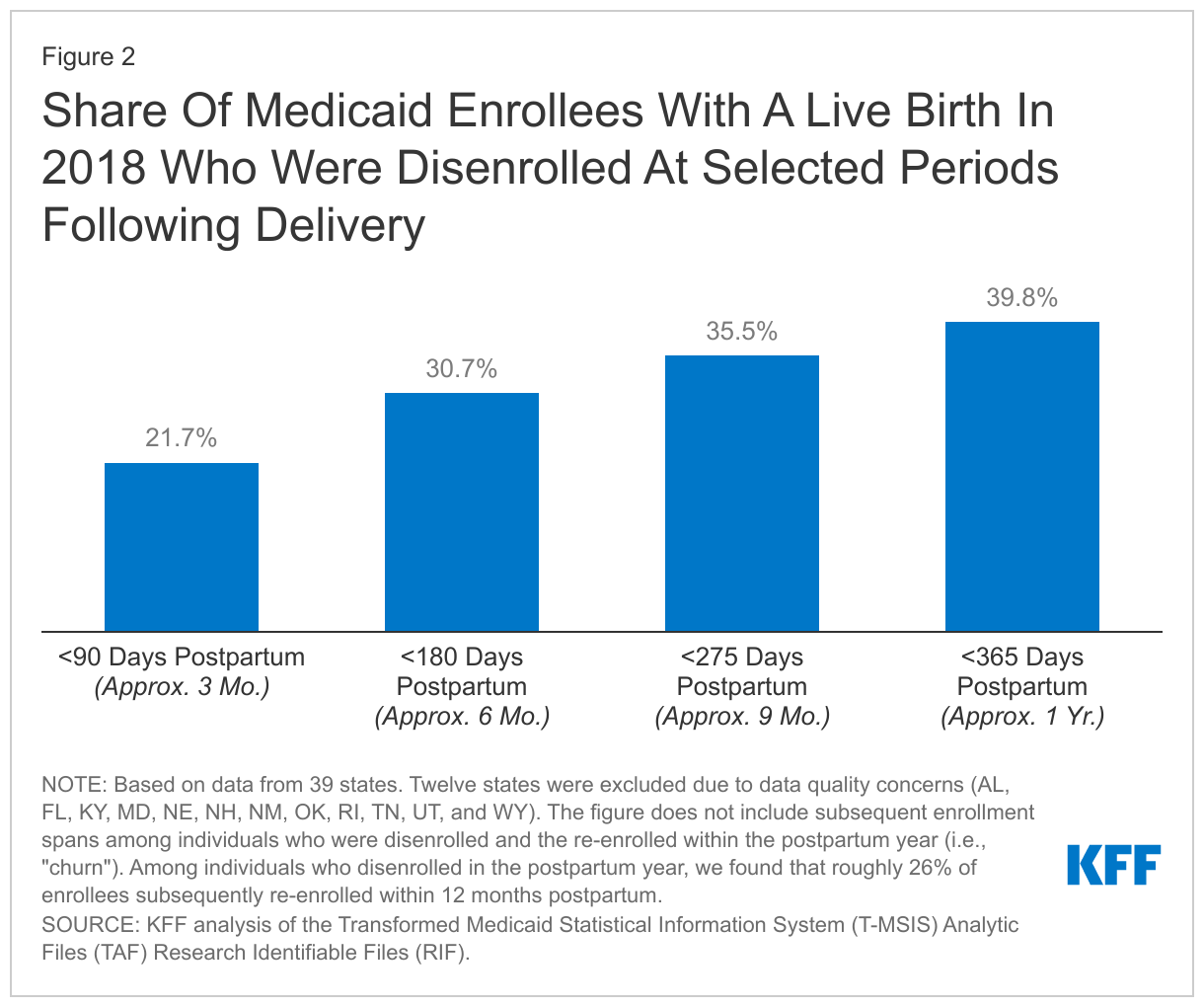
- Among Medicaid enrollees with a live birth in 2018, 31% were disenrolled from Medicaid coverage within six months and 40% disenrolled within a year after delivery.
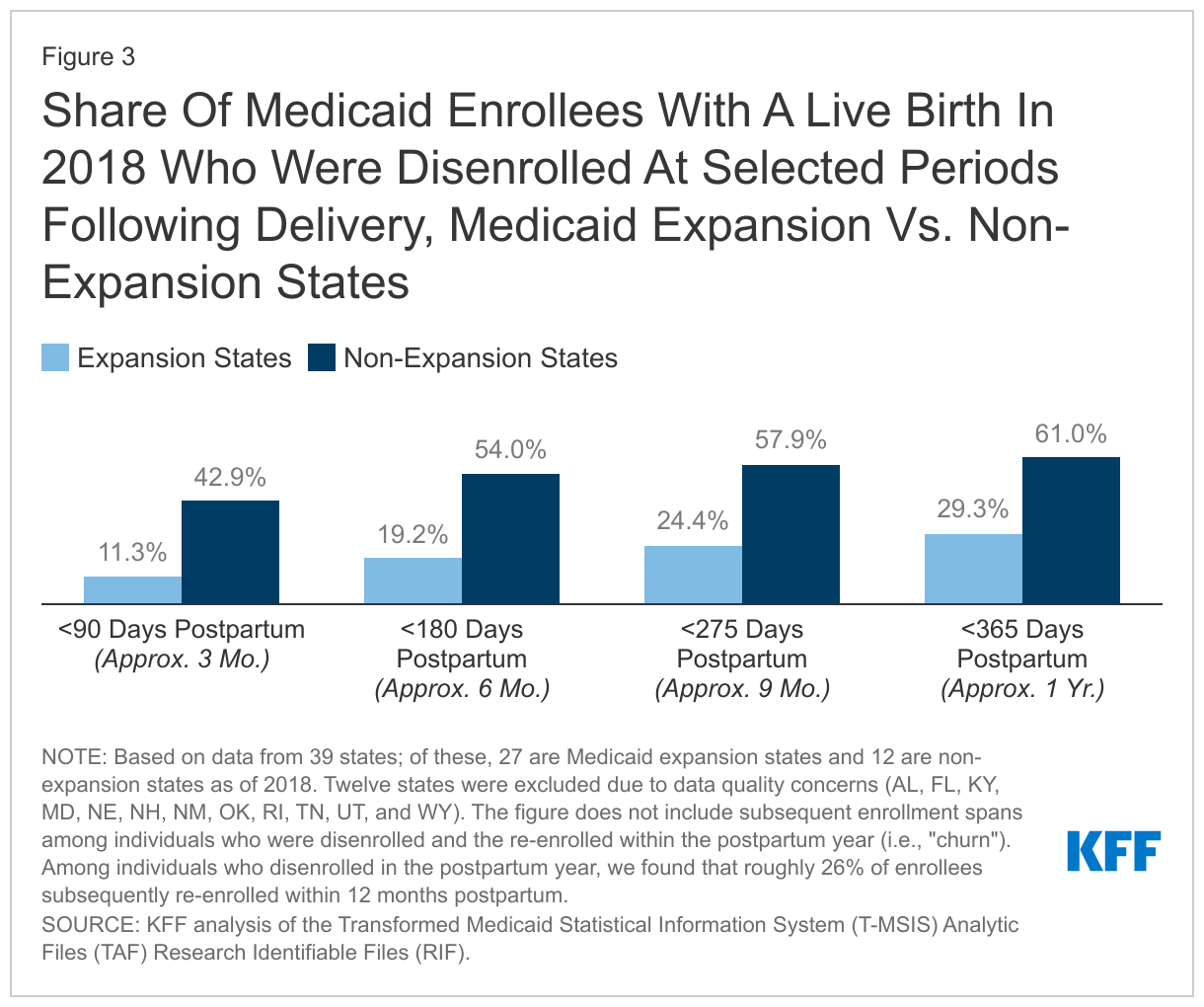
- In the states that had not implemented the Affordable Care Act’s (ACA) Medicaid expansion as of 2018, 61% of postpartum enrollees were disenrolled within a year after delivery – double the rate of 29% found in Medicaid expansion states.
- Among those who were disenrolled from Medicaid coverage in the postpartum year, roughly 1 in 4 (26%) experienced “churn,” meaning that they disenrolled and then subsequently re-enrolled within 12 months of delivery.
- In 2018, we estimate 610,000 enrollees with a live birth would have been able to retain continuous Medicaid coverage had a 12-month postpartum coverage extension been in place. These are among the roughly 1.5 million enrollees with a live birth who potentially could have benefited from a 12-month postpartum coverage extension by providing continuous eligibility for a full year after childbirth and reducing administrative hurdles for enrollees to maintain coverage.
Although a majority of states have extended postpartum Medicaid coverage under ARPA, the effects of the extension will not be felt until the end of the continuous enrollment requirement in Medicaid, which is in place until the end of the month in which the national public health emergency ends. However, state policy decisions about Medicaid postpartum coverage could be especially impactful in states set to restrict abortion access following the Supreme Court’s decision to overturn Roe v Wade, which could affect the number of births covered by Medicaid.
Introduction
The Medicaid program finances about 4 in 10 births in the U.S. each year and a majority of births in some states. Federal law requires states to provide pregnancy-related Medicaid coverage through 60 days postpartum. After the 60-day postpartum period, however, some enrollees lose coverage if their income is too high to qualify for Medicaid through another pathway, such as a low-income parent or through the Medicaid expansion. Maintaining consistent coverage during the postpartum period is important for monitoring individuals’ health following pregnancy, including pregnancy-related chronic and mental health conditions that often require attention far beyond 60 days postpartum. Rising maternal mortality rates, along with the recent Supreme Court decision to overturn Roe v Wade, have increased attention on Medicaid coverage for pregnant people.
To improve maternal health and coverage stability, a provision in the American Rescue Plan Act (ARPA) of 2021 gives states a new option to extend Medicaid postpartum coverage to 12 months via a state plan amendment (SPA). This new option took effect on April 1, 2022 and is available to states for five years. To date, 34 states (including DC) have implemented or plan to implement 12-month continuous eligibility for postpartum people. The Biden-Harris Administration recently included continuous Medicaid coverage for 12 months postpartum as a key element in its Blueprint for Addressing the Maternal Health Crisis. Notably, Congress included a 12-month postpartum coverage extension in Medicaid as a requirement for states in the Build Back Better Act that passed the House, and there are ongoing discussions in the Senate about the scope of a potential budget reconciliation package that could include a postpartum coverage extension in Medicaid.
Using Medicaid claims data for enrollees with a live birth in 2018, this brief examines enrollment patterns in the 12 months after delivery. We also estimate the number of enrollees who would benefit from the 12-month continuous eligibility policy for postpartum people if adopted by all states. See the methods section for more details about the data source and how we conducted the analysis.
Who Qualifies for Pregnancy and Postpartum Medicaid Coverage?
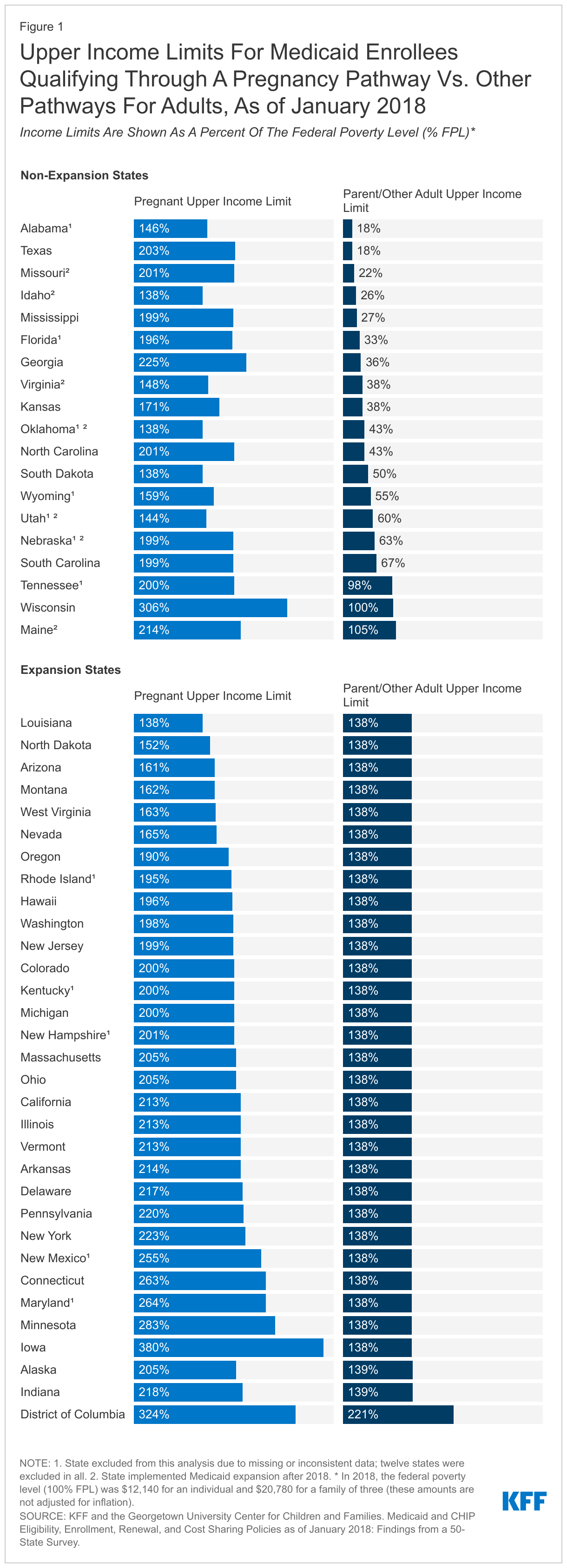
The federal government requires states to provide Medicaid coverage for pregnant individuals through 60 days postpartum and establishes a minimum income threshold of 138% of the federal poverty level (FPL).1 However, most states have set income eligibility for pregnant individuals above the federal minimum of 138% FPL, thus eligibility levels for pregnant people are higher than for low-income parents and expansion adults. The gap between states’ eligibility income limits for pregnancy and parents/other adults is generally larger in states that have not implemented the Medicaid expansion because these states have income limits for parents that are lower than 138% FPL (Figure 1). For example, income limits for parents in non-expansion states ranged from 18% FPL in Texas and Alabama to 105% FPL in Maine, although Maine would later implement the ACA expansion in 2019. In contrast, the median state income limit for pregnant individuals in 2018 was 200% FPL, ranging from 138% FPL in four states (ID, LA, OK, SD) to 380% FPL in Iowa. In that year, all but one state (LA) set eligibility limits for pregnant individuals that were higher than the limits for parents or expansion adults.
How Many Enrollees Lose Coverage During the Postpartum Year?
Among Medicaid enrollees with a live birth in 2018, 31% were disenrolled within six months and 40% disenrolled within a year after delivery (Figure 2). Many Medicaid enrollees are disenrolled after their 60-day postpartum coverage ends because their income is too high to qualify through another eligibility pathway, such as low-income parents or the Medicaid expansion. Additionally, some enrollees who continue to be eligible for Medicaid through another pathway may be disenrolled because of administrative barriers during eligibility redeterminations at the end of the postpartum coverage period. Due to wide variation in states’ income eligibility limits and administrative requirements for renewing coverage, there is considerable variation in disenrollment rates across states. The share of enrollees disenrolled within the postpartum year ranged from 9% in DC to 89% in Texas.
In the states that had not implemented the Affordable Care Act’s (ACA) Medicaid expansion in 2018, 61% of postpartum enrollees were disenrolled within a year after delivery, which is double the rate of 29% found in Medicaid expansion states (Figure 3). Notably, the five states (DC, CA, LA, WA, AZ) with the lowest 12-month disenrollment rates were all Medicaid expansion states, and all had disenrollment rates less than 20% (approximately half the national rate). Conversely, the five states (KS, MO, ID, SD, TX) with the highest 12-month disenrollment rates were all non-expansion states as of 2018, and all had rates exceeding 60% (roughly 1.5 times the national rate). Idaho and Missouri implemented the Medicaid expansion in in 2020 and 2021, respectively, and, as a result, their disenrollment rates are likely different today than what they were in 2018. The difference in disenrollment rates between Medicaid expansion and non-expansion states is expected, given higher income limits for adults in expansion states. In non-expansion states, postpartum people who are disenrolled may end up in the coverage gap if their income is above their state’s Medicaid eligibility limit for parents but below the poverty level, making them ineligible for premium subsidies in the ACA Marketplace. Without access to affordable Marketplace coverage, individuals in the coverage gap are more likely to end up uninsured. Expansion states cover adults up to 138% FPL, and postpartum enrollees in these states with incomes above this level who no longer qualify for Medicaid should be able to access premium subsidies in the Marketplace. Prior research suggests that those in non-expansion states are more likely than those in expansion states to become uninsured after the postpartum coverage ends.
Among postpartum enrollees who were disenrolled from Medicaid coverage in the postpartum year, roughly 1 in 4 (26%) experienced “churn,” meaning that they disenrolled and then subsequently re-enrolled within 12 months of delivery. For postpartum individuals, the most likely cause of churn is that they are unable to complete the renewal process when their postpartum coverage ends despite remaining eligible; however, short-term income fluctuations that cause enrollees to become temporarily ineligible can also cause churn. Churning on and off coverage can disrupt the continuity and quality of care for postpartum enrollees as well as causing additional administrative costs to state Medicaid agencies.2
How Many Medicaid Enrollees Would Benefit from Extending Postpartum Coverage to 12 Months?
We estimate that there were roughly 1.5 million enrollees with a live birth covered by Medicaid in 2018 who potentially could have benefited from a 12-month postpartum coverage extension and, of these, approximately 610,000 individuals who were disenrolled in the postpartum year and would have otherwise retained coverage throughout the year. Extending postpartum coverage to 12 months would push back coverage redeterminations for all postpartum individuals to a full year after the pregnancy ends, reducing administrative hurdles for enrollees to maintain coverage. However, the 12-month continuous eligibility policy would directly benefit those postpartum individuals who lost coverage during the postpartum year. A 12-month postpartum coverage extension would be particularly impactful in non-expansion states because these states have higher disenrollment rates during the postpartum year compared to expansion states. Our findings are based on estimates for the 50 states and DC and are similar to another national study using other data sources that found 720,000 enrollees would have otherwise stayed continuously eligible through postpartum year had all states implemented the coverage extension in 2021.
Thousands of people experiencing a pregnancy loss could also benefit from a 12-month postpartum coverage. We estimate that at least 50,000 enrollees with a pregnancy loss3 in 2018 were disenrolled in the postpartum year but would have otherwise stayed continuously enrolled if all states had implemented a 12-month coverage extension. Our estimate is likely an undercount because individuals who did not seek medical attention for a miscarriage would not be identifiable in the claims data used in this analysis and because we limited our estimate to individuals who had pregnancy as their primary eligibility pathway when their pregnancy loss occurred.4 Overall, if we include both enrollees with a live birth as well as those with a pregnancy loss, we estimate that roughly 660,000 individuals lost coverage during the postpartum year and would have otherwise remained continuously enrolled had all states implemented 12-month continuous eligibility for postpartum coverage.
Looking Ahead
The recent Supreme Court decision to overturn Roe v Wade and eliminate the constitutional right to abortion could increase the role Medicaid plays in covering pregnant and postpartum individuals. A number of states currently have laws in place that are intended to severely restrict or ban abortions. Most of the states that have not extended postpartum Medicaid coverage have laws in place to restrict or ban access to abortions. These laws restricting access to abortions will have a more significant impact on low-income individuals who do not have the money or means to travel to another state to obtain an abortion, which could affect the number of births covered by Medicaid and the need for postpartum coverage.
Although a majority of states have extended postpartum Medicaid coverage under ARPA, the effects of the extension will not be felt until the end of the continuous enrollment requirement in Medicaid. Provisions in the Families First Coronavirus Response Act (FFCRA) require states to provide continuous coverage for Medicaid enrollees until the end of the month in which the public health emergency (PHE) ends in order to receive enhanced federal funding. The PHE is in effect through mid-July 2022, although it is expected that the PHE will be extended for at least another three months (because the Biden administration did not provide a 60-day notice to states as of May 2022). The continuous enrollment requirement has helped prevent coverage loss and churn among enrollees, including postpartum enrollees, during the pandemic. However, in states that have not extended postpartum Medicaid coverage, we expect disenrollment and churn rates among enrollees in the postpartum year to return to levels that are comparable to those found in this analysis when the PHE ends.
Methods
Data Source
Our analysis uses the Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) Research Identifiable Files (RIF). We drew from the 2018 Inpatient and Other Services claims files (Release 1) linked with the 2018-2019 Demographic Eligibility (DE) Base File and DE Dates File (Release 1 for 2018, Preliminary for 2019). We used BENE_ID to link files when available and, when BENE_ID was missing, we used MSIS_ID to link files (see the TMSIS User Guide for information on linking variables). We identified Medicaid enrollees with a live birth or pregnancy loss (including miscarriage, still birth, or termination) from the claims and then used the eligibility files to estimate enrollment patterns and eligibility pathways at various periods postpartum.
State Exclusion Criteria
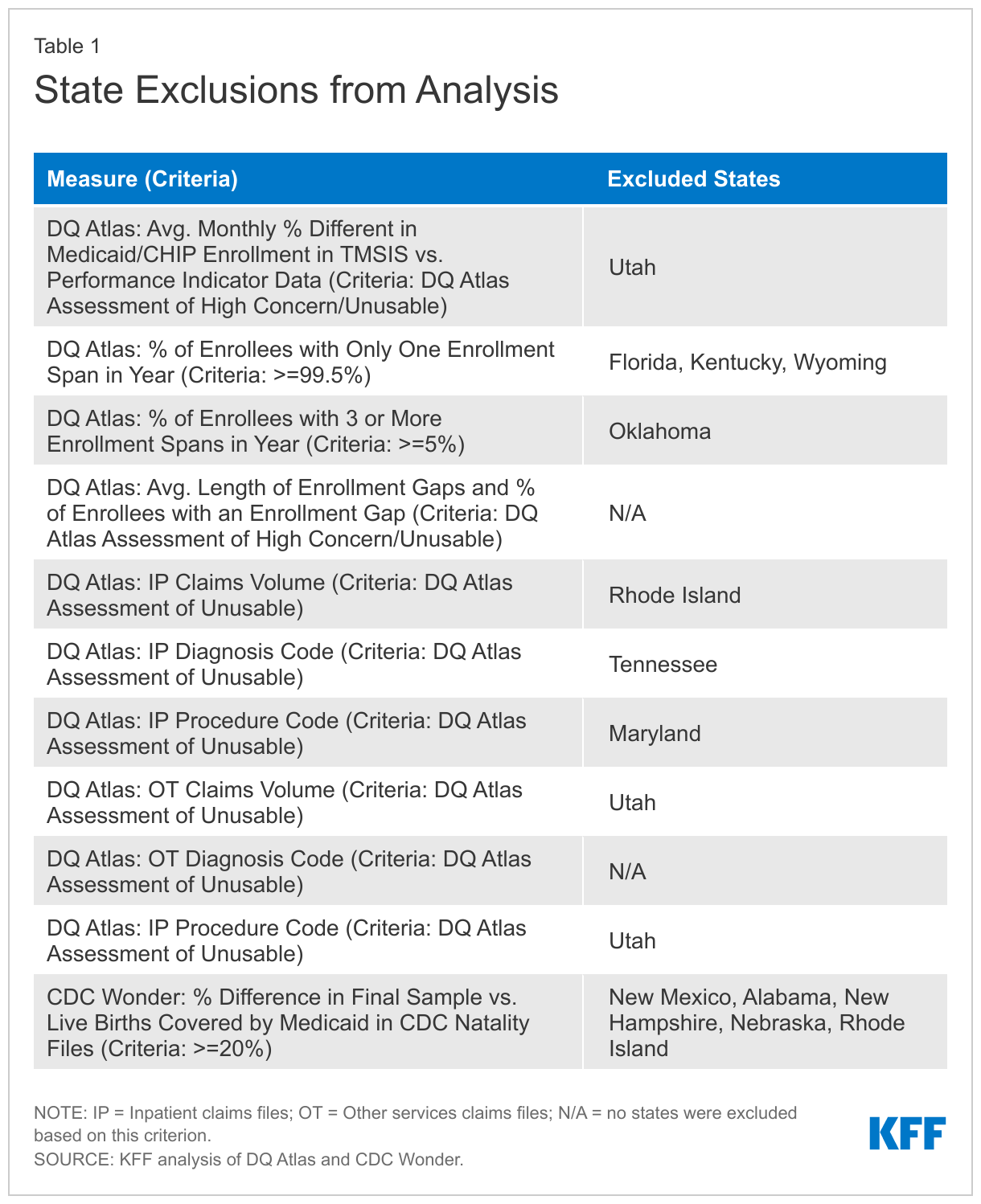
We use 39 states in our analysis. We exclude 12 states (AL, FL, KY, MD, NE, NH, NM, OK, RI, TN, UT, and WY) due to missing or inconsistent data based on state-level information available from the DQ Atlas as well as our own analysis of the CDC Wonder Natality Files. We used several measures from the DQ Atlas to assess states’ data quality, shown in Appendix Table 1. We further excluded states whose final sample in this analysis had a difference of 20% or more from the number of Medicaid-covered births in the CDC Wonder Natality Files. In total, our final sample included 1,286,000 deduplicated enrollees with a live birth, while CDC Wonder reported 1,301,000 newborns covered by Medicaid (a difference of -1.1% from CDC Wonder).
Enrollee Sample Selection
To identify Medicaid enrollees with a live birth or pregnancy loss in 2018, we followed the methods and all reference codes provided by Calkins et al. in their technical specifications for “Maternal and Infant Health (MIH): Identifying Pregnant and Postpartum Beneficiaries in Administrative Data,” available on the CMS website. We did not utilize “unknown” pregnancy outcomes in our analysis (an optional approach provided by Calkins et al.). In addition to flagging individuals with a live birth or pregnancy loss, we also captured the procedure or service start date for each claim that we flagged. Then, we rolled up the claim level data to the individual level, keeping the earliest date of service for live births and still births. About 2% of enrollees with a pregnancy loss had multiple claims that were more than 180 days apart and likely represented multiple pregnancy losses in the year. In a small number of cases where women had both a pregnancy loss and a live birth, we prioritized the live birth data and dropped all information on pregnancy loss to make the categories mutually exclusive. Our final sample included 1,616,000 unduplicated Medicaid enrollees with live birth or pregnancy loss. This included 1,286,000 unduplicated enrollees with a live birth and 329,000 unduplicated enrollees with a pregnancy loss.
Calculating Disenrollment and Churn During the Postpartum Period
To estimate postpartum disenrollment, we used the DE Dates File’s start and end dates on enrollment spans. In cases where people disenrolled and then re-enrolled the next day, we merged the two enrollment spells into one. Then, we calculated the disenrollment rates as the difference in days from the pregnancy end date to the next disenrollment date. To calculate “churn,” we counted the number of individuals who disenrolled and then re-enrolled within 365 days of their pregnancy end date.
Extrapolating Findings from 39 States to 50 and DC
We extrapolate our 39-state findings to a 50-state and DC estimate to provide a national number that illustrates the impact that a 12-month postpartum extension would have if all states implemented the policy in 2018. Our extrapolation simply applies a national level multiplier without any adjustments. Our analysis of 39 states’ data identified 1,286,000 individuals with a live birth; 511,000 enrollees with a live birth who disenrolled in the postpartum year; 329,000 enrollees with a pregnancy loss; 101,000 people with a pregnancy loss who disenrolled in the postpartum year; and 40,000 individuals with a pregnancy loss who disenrolled in the postpartum year and who had pregnancy as their primary eligibility pathway at the time of lost pregnancy. Based on annual Medicaid enrollment available on the CMS website, we found that the 39 states in our analysis represent approximately 84% of all Medicaid enrollees nationally. We assume that our findings also represent 84% of the enrollees who would benefit from a postpartum coverage extension, and so we divided our estimates by 0.84 to create a national estimate and rounded to the nearest 10,000.
These extrapolations may underestimate the impact of a 12-month postpartum extension because our sample of 39 states had a larger proportion of enrollees that lived in ACA expansion states (78%) compared to the national annual enrollment in 2018 reported by CMS (70% living in expansion states). Because expansion states have lower disenrollment rates, the higher representation of those states among our sample likely underestimates the number of individuals who would have stayed continuously enrolled under a postpartum coverage extension when we extrapolate our findings to the full 2018 Medicaid population.
- In 2018, the federal poverty level (100% FPL) was $12,140 for an individual and $20,780 for a family of three (these amounts are not adjusted for inflation). ↩︎
- While another KFF analysis on churn in the overall Medicaid/CHIP population also uses 2018 TMSIS data, the findings are not comparable due to important differences in the definition of “churn.” The previous KFF study defined churn as anyone with a coverage gap of 365 days or less, with the gap starting or ending at any point in the reference year (2018). However, this analysis on postpartum enrollees defines churn as a coverage gap that started and ended within the postpartum year (or within 365 days of childbirth). ↩︎
- As described in the methods section, we used reference codes from Calkins et al. (available on the CMS website) to identify enrollees with a live birth, miscarriage, still birth, or termination. As noted by Calkins et al., terminations are unlikely to appear in the TAF RIF claims data because, with limited exceptions, states are prohibited from using federal Medicaid funding to pay for abortions. ↩︎
- We limited the estimates for pregnancy to those that were disenrolled and had pregnancy as their primary eligibility pathway to be conservative in our approach. According to federal guidance, all pregnant individuals qualify for postpartum coverage if their pregnancy is known to the state Medicaid agency – e.g., because the pregnancy is reported by the enrollee or identified by the state through claims – regardless of their primary eligibility pathway. If we assume that having a Medicaid-covered medical visit for pregnancy loss would qualify the enrollee for postpartum coverage (because the visit would be identifiable in claims), then we would increase our original 51-state estimate from 50,000 to 120,000 enrollees with a pregnancy loss would have otherwise stayed continuously enrolled through the postpartum year. ↩︎