KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
The 2025 reconciliation law will—for the first time—require adults who are enrolled in Medicaid though the Affordable Care Act (ACA) expansion, along with those in partial expansion waiver programs in Georgia and Wisconsin, to meet work requirements or qualify for an exemption as a condition of eligibility starting in January 2027 in most states.
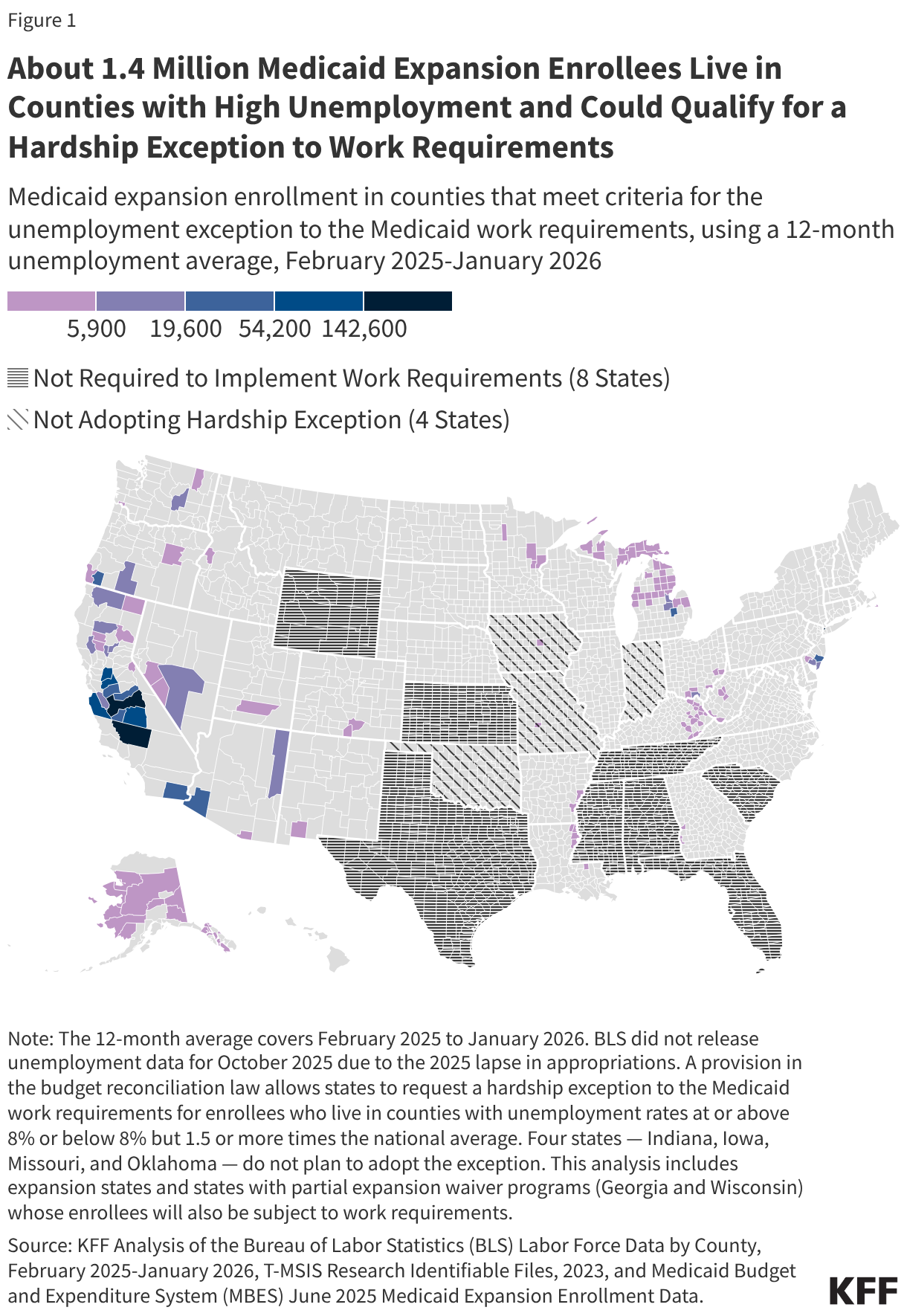
States may adopt an optional hardship exception to Medicaid work requirements for individuals living in counties with unemployment rates at or above 8%, or at least 1.5 times the national average unemployment rate. A recent KFF survey found that most states plan to adopt this exception, which will exempt both Medicaid applicants and enrollees in counties with unemployment rates that meet the specified thresholds. However, four states, Indiana, Iowa, Missouri, and Oklahoma, do not plan to adopt the exception.
An update to a previous KFF analysis of county unemployment rates, using 12-month average unemployment rates from February 2025 through January 2026, and county-level Medicaid expansion enrollment estimates that:
1.4 million expansion enrollees, or 7.5% of expansion enrollees, live in counties that meet the high unemployment threshold and may qualify for the hardship exception in the 27 states that plan to adopt the exception and in the 12 states that had not made a decision on adoption at the time of the KFF survey.
Among the states that are planning to adopt or may adopt the exception, 133 counties in 22 states meet the high unemployment thresholds, representing 7% of counties in expansion states and states with partial expansion waiver programs. No counties meet the thresholds in 16 states, and DC does not meet the thresholds.
Nine in ten expansion enrollees who are in counties that meet the high unemployment criteria and could be exempt from the work requirements live in five states—California, New York, Michigan, New Jersey, and Oregon.
Among the states that do not plan to adopt the hardship exception, two counties in Iowa and Missouri meet the high unemployment thresholds, and approximately 3,300 expansion enrollees in those counties may have qualified for the high unemployment hardship exception if the states had decided to adopt the exception. In Indiana and Oklahoma, there are no counties that meet the thresholds.
Nebraska began enforcing work requirements on May 1, 2026, the first state to implement the new requirements. Although the state indicated it would adopt the high unemployment hardship exception, no counties in the state currently meet the thresholds.
States are waiting for federal guidance on how to implement this hardship exception, including what data will be used to identify counties that meet the thresholds and what additional information states must submit. This analysis uses the most recent available county-level unemployment data from Bureau of Labor Statistics (BLS) and is consistent with the methods used to determine whether any counties qualify for the high unemployment exemption waiver from SNAP work requirements. However, the guidance, which CMS is expected to release in early June, may require a different method.
KFF’s interactive Medicaid work requirements tracker includes new county-level unemployment data by state, showing which counties meet the high unemployment thresholds and how many expansion enrollees in those counties may be exempt from work requirements.
The President’s Emergency Plan for AIDS Relief (PEPFAR) has been and continues to be subject to a range of Congressional reporting requirements. These include enduring (ongoing) requirements as well as time-bound requirements, through both PEPFAR’s authorizations as well as appropriations legislation in some years.
This document provides a list of reporting requirements identified in PEPFAR’s authorizing legislation over time as well as other key legislation. Table 1 includes current requirements and requests. Table 2 includes past requirements and requests that are no longer in effect. While this document lists most such requirements, it may not be exhaustive.1
There are other requirements [such as those that are not specific to PEPFAR established under the Foreign Aid Transparency and Accountability Act (FATAA) of 2016, for example, which includes more general reporting requirements; and some in appropriations legislation, along with accompanying congressional reports and explanatory statements, over the more than 20 years of PEPFAR] that are not included in this analysis. ↩︎
Note: The map in this brief will be updated regularly to include new federal actions about potential Medicaid fraud and new state responses. The brief was last updated on May 15, 2026.
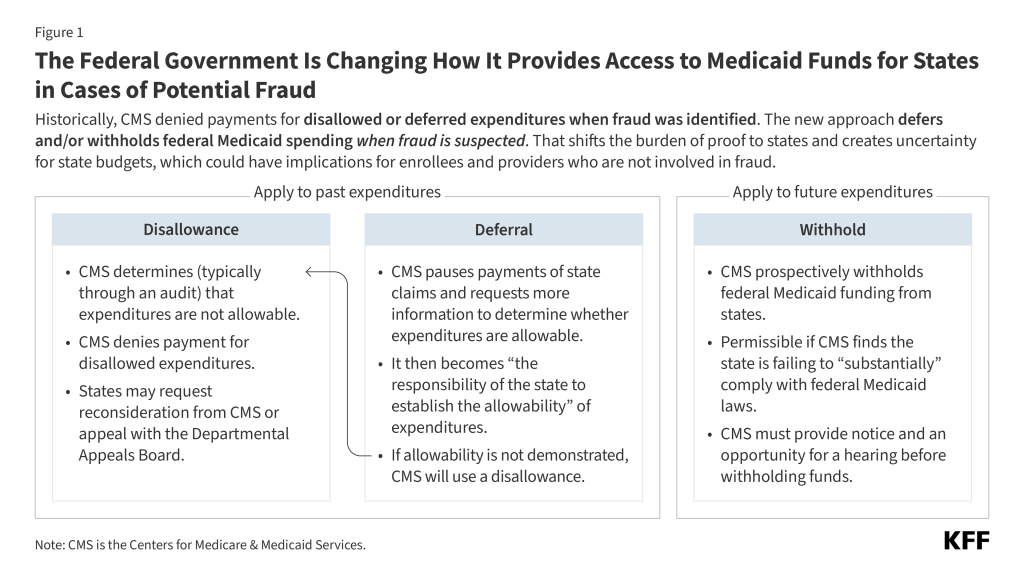
The current administration is placing a new emphasis on potential fraud in Medicaid with its Comprehensive Regulations to Uncover Suspicious Healthcare (CRUSH) initiative. The Centers for Medicare and Medicaid Services (CMS’) started the new initiative in Medicaid focusing on Minnesota and three other states with Democratic governors (California, Maine, and New York) while the House Committee on Energy and Commerce sent requests for information to 11 states. CMS has historically partnered with states to identify and resolve issues of fraud, waste, and abuse, and denied the federal share of Medicaid spending when fraud has been identified by an audit, investigation, or reported by the state. However, CMS has recently announced a new approach to fraud that will rely more heavily on options to prevent spending federal funds in cases of potential fraud, which could have broad implications for states and enrollees. This issue brief explains the new approach. Key findings include:
CMS’ historic practice has relied on disallowing federal Medicaid payments when fraud is identified (typically through an audit), a process that may take several years to implement.
CMS’ new approach to potential fraud involves potentially pausing or withholding federal Medicaid payments when fraud is suspected (Figure 1). This approach differs from prior approaches because, if implemented, it could have more immediate consequences, place a much larger share of federal spending at risk (including spending that pays for services uninvolved in fraud), and proactively shift the burden of proof to states to obtain federal funds.
While all approaches aim to limit future fraudulent payments using tools such as corrective action plans, the new approach to federal Medicaid spending when fraud is suspected creates uncertainty for state budgets and could have implications for Medicaid enrollees and providers who are not involved in fraud.
What is a disallowance?
The federal and state governments share responsibility for financing Medicaid, and states draw on federal funds to pay health care providers and health plans for providing health care to enrollees. The federal government makes quarterly grant awards to states to cover the federal share of Medicaid spending. Awards reflect states’ estimated expenditures for the upcoming quarter and adjustments from prior quarters’ expenses. Adjustments reflect various considerations such as:
Instances where states’ estimated expenditures are higher or lower than actual expenditures
Changes to accounting practices or federal matching rates
Reductions in payment resulting from claims where fraud has been identified
Publicly-available data on Medicaid expenditures show the total amount of adjustments each year, reflecting the net impact of all various factors, and do not specifically identify adjustments due to disallowances and deferrals.
Historically, CMS has used disallowances to deny federal matching funds for state Medicaid expenditures that have already occurred and are later determined to be not allowable. There is limited information available about the frequency and scope of Medicaid disallowances, but an older report by the Government Accountability Office (GAO) suggests that they were not infrequent between 2014 and 2017.Upon receiving a disallowance notice, states may request that CMS reconsider the decision and provide additional information to CMS to demonstrate that the expenditures were allowable or accept the disallowance and resolve it directly with CMS. In all cases, once CMS has issued a disallowance, “the state has the burden of documenting the allowability” of the expenditures to overturn the disallowance. When states request a reconsideration, CMS has 60 days to decide, although this timeline may take longer if CMS requests additional information from the state.
States may appeal the disallowance decisions to a Departmental Appeals Board, but the state still has the burden of proof for documenting the allowability of expenditures and the process may take years to resolve. States are not required to request a reconsideration before appealing the disallowance. More information is publicly available for cases where states do appeal the decisions than for cases where they settle or request a reconsideration. In such cases, data about the decisions of the Department Appeals Board are available online through the Department’s website. Between 2020 and 2025, the Departmental Appeals Board has issued 12 Medicaid disallowance rulings (with 6 rulings being an appeal of a prior case). In all 6 new rulings, there were on average 15 years between the oldest year of disputed expenditures and the final ruling, highlighting how long it takes to resolve these cases (see Figure 2 for an example from Texas). All cases were decided in favor of CMS, but that may reflect the fact that CMS has historically used disallowances only in cases where fraud is well-established.
The amount of disputed disallowances where the Departmental Appeals Board issued a ruling between 2020 and 2025 ranged from less than $500,000 to almost $200 million, but these amounts reflect differences in the number of years and scope of services within the disallowed claims. Some of the largest disallowances to be upheld involve disproportionate share hospital (DSH) payments.
The largest disallowance ruling between 2020 and 2025 was $195.7 million in a case involving Michigan’s DSH payments between 2001-2009. In that instance, CMS in 2018 determined that the state had made DSH payments to a small number of hospitals that were ineligible to receive them. The Departmental Appeals Board ruling was in 2024.
The second largest disallowance ruling between 2020 and 2025 was for more than $97 million in a case where Florida made DSH payments between 2006-2013 in excess of the limits established for specific hospitals (CMS first issued this disallowance in 2016 and the Departmental Appeals Board ruling was in 2021).
Figure 2
What is a deferral?
With deferrals, CMS pauses payment for state Medicaid expenditures that have already ocurred and requires the state to provide additional information demonstrating that expenditures are “allowable.” Deferrals are usually initiated by the federal government and may be used to pause federal funding while the state and federal governments work out the details of a disallowance, and in cases where fraud, waste, or abuse has been identified and the state and federal governments are gauging the extent of the issue. In the past, deferrals were used as temporary measures that pause funding until CMS either reimburses the expenditures or issues a disallowance. Deferral notices must specify the reason for the deferral and include a request for all documents and materials that CMS believes are necessary to determine whether the expenses are allowable. After the notice is sent, the loss of federal funds occurs immediately.
After receiving a deferral notice from CMS, states have 60 days to provide all requested documents and materials unless they request an additional 60-day extension. CMS usually begins document review within 30 days but may request different formats or additional materials from the state. States have 15 days to submit additional materials and if they do not meet that deadline, CMS disallows the expenses. Once all documents are available, CMS has 90 days to review and determine whether expenditures are allowable. If CMS determines expenditures are not allowable, the disallowance process begins, offering the state the opportunity to request a reconsideration and appeal to the Departmental Appeals Board.
Deferrals are receiving new attention after the administration announced that it would temporarily defer $259 million in federal Medicaid payments to Minnesota for expenditures incurred in quarter 4 of in fiscal year (FY) 2025, an unprecedentedly large amount. In the announcement, CMS noted that it may continue to defer federal payments for either additional quarters in 2025 or future quarters in 2026, and that similar announcements for other states would likely be coming soon. As of March 25, 2026, 4 additional states have received formal letters from CMS requesting information about program integrity, and 11 states have received formal letters from the House Committee on Energy and Commerce (Figure 3).
What is a withhold?
In January 2026, CMS notified Minnesota that pending the outcome of a hearing, it would begin withholding $515 million in quarterly federal Medicaid payments moving forward, a process that has seldom been used in prior years. Withholding funds has been referred to as the “compliance process” because it is only permissible in cases where the state is failing to comply with Medicaid law. Prior use of withholding has been limited. When CMS has considered withholding as a compliance tool in the past, it announced withholdings that were at most between 1 and 10 percent of the federal share of Medicaid spending for specific services (in most cases, the administrative costs states incurred to implement their Medicaid programs). Prior CMS communication notifying states of possible withholdings appear to have been used when states incorrectly restrictedeligibility or benefits, thus failing to comply with minimum requirements regarding access to coverage or eligibility. Minnesota’s case is different because of the scope of the proposed withholding and because the proposed withholding would be to address potential future fraud, rather than state policies that restrict Medicaid eligibility or benefits. The announced level of withholding would have represented nearly 20% of the federal share of Minnesota’s spending on an annual basis.
To withhold federal Medicaid funds, CMS must first provide states with the opportunity for an administrative hearing, and withholding generally ends when CMS is satisfied with states’ resolution of the issue. Withholdings may reflect issues with states’ Medicaid approved plans or with states’ implementation of the plans. Because CMS has authority to approve states’ plans, most issues arise regarding implementation of the plan and are resolved using a corrective action plan. Corrective action plans may also be used to address other types of issues in Medicaid (such as payment error rates or eligibility re-determinations). In general, the plans include a narrative of steps states are planning to take to address issues related to proper implementation of the Medicaid program. On January 13, 2026, Minnesota requested a hearing about the withholding and on January 30, 2026, Minnesota submitted a revised corrective action plan to CMS. On March 20, 2026, CMS accepted Minnesota's revised corrective action plan. Successful completion of the corrective actions outlined in the plan will resolve the threat of withholding.
What are the implications of new reliance on deferrals and withholds?
The new approach to federal Medicaid spending when fraud is suspected creates uncertainty for state budgets, particularly given the magnitude of federal funding at stake and the time it takes to resolve administrative disputes. Unlike the federal government, states must generally operate balanced budgets, which is one reason states are able to draw down matching funds to finance ongoing expenditures. If withholding is implemented, the loss of federal funds could make it difficult for states to maintain current programs while details of the cases are being sorted out. More extensive use of deferrals could have similar, but more immediate, destabilizing effects on states’ budgets because they reduce the amount of federal funds available to states for several months, and the state has no option to request reconsideration or appeal until a disallowance is issued. Increasing the use of deferrals so that it applies to entire categories of services where fraud is suspected but not established would also place a new administrative burden on states to demonstrate the allowability of expenditures. Other approaches to addressing suspected fraud, waste, and abuse remain available to CMS. The National Association of Medicaid Directors (NAMD) has suggested the following actions to help states to address fraud waste, and abuse in Medicaid:
Help states identify federal materials about best practices such as recommendations and provider enrollment self-assessments;
Create rapid methods to share information about provider disqualifications between Medicare, the Veterans' Health Administration, and Medicaid;
Respond more quickly to fraud reports from state attorneys general and the Medicaid Fraud Control Units;
Strengthen procedural pathways for states and CMS to work collaboratively on Corrective Action Plans to enhance adherence to provider requirements while maintaining access to Medicaid benefits;
Conducting additional analysis of Medicaid data through the Center for Program Integrity;
Strengthening federal data sources and their interoperability; and
Providing technical assistance to state officials and staff.
New uncertainty about the availability of federal funding could have implications for Medicaid enrollees and providers who are not involved in fraud. If states have inadequate funding to maintain existing Medicaid services, they may face difficult decisions regarding how to limit Medicaid spending. In general, states can reduce Medicaid spending by decreasing payment rates for providers, covering fewer services, or enrolling fewer people. Such actions could affect enrollees and providers who are not using or providing services in which fraud is suspected. There will also be additional disruptions for providers who lawfully provide Medicaid services where fraud is suspected because of new administrative burdens associated with increased audits, delayed payments, and other administrative practices.
CMS’ new approach to addressing cases of suspected fraud may exacerbate administrative and financial challenges states face as they implement the 2025 reconciliation law. The 2025 reconciliation law made historic reductions in federal funding for Medicaid and created new administrative requirements for states, particularly those that must implement work requirements for enrollees eligible for Medicaid through the Affordable Care Act Medicaid expansion. As states work to implement those changes and adjust to changes in federal financing, the new approach to fraud creates additional administrative requirements and potential new reductions in federal funding. Combined, these changes may have more significant implications for states’ ability to maintain existing levels of Medicaid payment rates, coverage, and eligibility.
The American Association of Public Opinion Research (AAPOR) last night recognized KFF’s Mollyann Brodie, Ph.D., with the AAPOR Award for Distinguished Achievement for her outstanding leadership and contributions to the field of public opinion research over three decades.
The award honors Dr. Brodie, a KFF executive vice president and executive director of KFF’s Public Opinion and Survey Research, for leading KFF’s polling team as it has built a body of work “that has become the nation’s definitive source for public opinion on health — earning the confidence of policymakers, journalists, and the public alike.”
The association notes Dr. Brodie’s role in developing the KFF Health Tracking Poll, which has documented the arc of the public’s opinions on and experiences with the Affordable Care Act and provided a record of how sweeping legislation affects ordinary Americans, and the KFF COVID-19 Vaccine Monitor, which became a critical resource for understanding the public’s views, access, uptake, and concerns about emerging vaccines. “In each case, her vision produced research that went beyond poll numbers to tell the broader story of how Americans experienced major changes in health and health care,” AAPOR noted in its award citation.
AAPOR also praised Dr. Brodie’s commitment to inclusion for women and other underrepresented groups, both in her work at KFF and as a leader within the association. The association notes her role in developing methodologically innovative surveys of working-class Americans, transgender adults, Hurricane Katrina evacuees, and rural communities — populations whose voices too rarely get elevated in other nationally representative polls.
In addition, KFF’s Surveys of Immigrants received the 2026 AAPOR Inclusive Voices Award, which recognizes work examining complex challenges related to underrepresented populations.
The multi-year initiative, including surveys conducted in partnership with The New York Times and The Los Angeles Times, is the only large-scale, nationally representative probability-based survey of immigrants in the United States in decades. Through innovative multi-frame, multilingual, and multi-mode methods, the surveys succeeded in amplifying the voices of groups often excluded from survey research, such as undocumented immigrants and those with limited English proficiency.
“We started our polling program when we started KFF in the early 1990s, but it made the jump to light speed after Molly arrived. These awards recognize her expertise and vision, and how effective we’ve been in coordinating our polling under Molly’s leadership with our equally tremendous capacity in policy research and journalism,” said Dr. Drew Altman, Founding President and CEO, KFF.
At KFF, Dr. Brodie works closely with Senior Vice President and Director of Public Opinion and Survey Research Liz Hamel, Director of Survey Methodology Dr. Ashley Kirzinger, and Dr. Altman, in addition to the policy research team led by Executive Vice President Larry Levitt, and journalists at KFF Health News. She also helped develop KFF’s polling partnerships with major news organizations, including The New York Times and The Washington Post. Dr. Brodie and Mr. Levitt are the executive team who work with Dr. Altman to oversee all of KFF’s program directions, finances, and operations.
The awards were presented last night at AAPOR’s 81st annual conference in Los Angeles.
For decades, the federal government has overseen two key vaccine injury compensation programs: the National Vaccine Injury Compensation Program (VICP) and the Countermeasures Injury Compensation Program (CICP). The VICP and CICP are designed to help maintain vaccine access while also recognizing that vaccine injuries can occur and those affected by such injuries should be compensated. However, over time, the demands on, and challenges faced by, these programs have grown. Recently, they have become targets of criticism from members of the Trump administration, including the Secretary of Health and Human Services (HHS) Robert F. Kennedy Jr. ,who said (without evidence) in 2025 that VICP had “devolved into a morass of inefficiency, favoritism, and outright corruption” and that he would lead an effort to overhaul it. Some lawmakers and external groups have called to replace or end these programs while others have suggested keeping them intact but adopting policy changes that could help modernize them and make them more effective. Some have raised concerns that making drastic changes to vaccine injury compensation programs could undermine the U.S. vaccine market and, more generally, confidence in vaccines.
To provide background and context on this topic, this brief summarizes the history and rationale for these programs and their key elements, analyzes publicly available information on claims and compensation under the programs, and discusses key policy issues they currently face. The programs, while both having been created as alternatives to civil courts, vary significantly in their structures, processed, vaccines covered, and compensation rates and amounts, among other factors.
Origins and Rationales for VICP and CICP
VICP and CICP were both created as alternative pathways to civil courts to allow individuals to seek compensation for vaccine-related injuries and address vaccine safety while also addressing concerns about vaccine supply in the U.S. Prior to the existence of these programs, there were times when vaccine manufacturers faced a large volume of lawsuits linked to rising public concerns about vaccine safety, which threatened to drive vaccine makers from the market and led them to raise their prices, affecting access to vaccines.
VICP, created by Congress in 1986, was designed as a legal pathway separate from traditional civil courts through which individuals can seek compensation for potential vaccine injuries directly from the federal government. VICP was created by Congress following a wave of public concern regarding vaccine safety in the late 1970s and 1980s that was fueled, in part, by sensationalizedtelevision programs on the topic of vaccine injuries in children. There had been a surge in lawsuits in the civil court system filed against health care practitioners and vaccine makers. Facing rising legal costs, some vaccine manufacturers chose to exit the vaccine market and those that remained raised their prices, which threatened the market for childhood vaccines in the U.S. In response, Congress passed the 1986 National Childhood Vaccine Injury Act (NCVIA) that, among other things, established the VICP. It was intended to help stabilize the vaccine market, preserve public confidence in immunization, while also providing a less adversarial and more streamlined pathway for families to submit claims and receive compensation payments for vaccine injuries compared to civil litigation. The act created the process by which vaccines could be added to VICP coverage and created the VICP trust fund, which funded the program using excise taxes placed by Congress on each of the vaccines covered under VICP. Congress has made several statutory changes and additions to VICP since 1988, including the 1993 Omnibus Budget Reconciliation Act that allowed for rapid inclusion of new U.S. Centers for Disease Control and Prevention or CDC-recommended vaccines into VICP once Congress enacted the excise tax on that vaccine, and the 21st Century Cures Act from 2016 that added vaccines recommended for pregnant women to VICP and explicitly included injuries to children in utero as eligible for VICP compensation.
CICP was created by Congress in 2005 to allow individuals to seek compensation for injuries that may have occurred from use of medical countermeasures (such as vaccines) during a public health emergency (as distinct from routine use addressed under VICP). It was established as part of the Public Readiness and Emergency Preparedness (PREP) Act, at a time of heightened national security concerns following the September 11, 2001 attacks, anthrax mailings, and the threat of an influenza pandemic. The PREP Act was meant to address concerns that in a public health emergency, such as a bioterrorist attack or a naturally occurring outbreak, private companies might be reluctant to develop and manufacture vaccines, drugs, and other medical countermeasures because of liability risks they could face from use of those products during an emergency. As part of a broader strategy incentivizing rapid development and deployment of countermeasures, the PREP Act offered immunity from liability to manufacturers and distributors of these products, and created the CICP as the federal compensation mechanism for injuries that may occur through use of these products.
Vaccines and Injuries Covered, and Processes for Review and Compensation
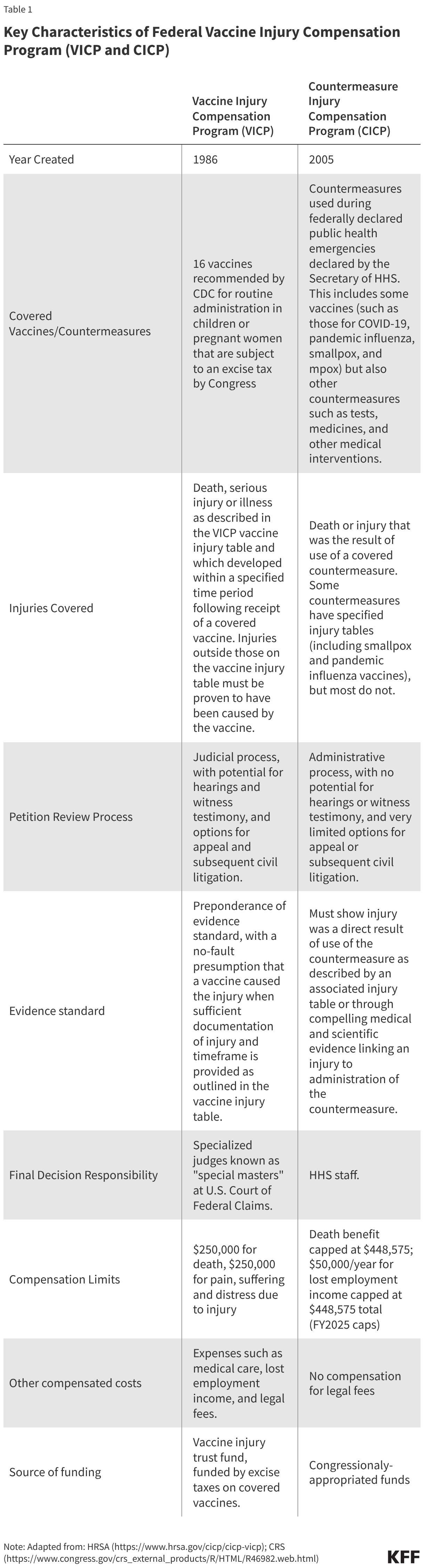
While both VICP and CICP are designed to be more efficient and streamlined mechanisms compared to civil courts for vaccine injury compensation cases, they are distinct in terms of which vaccines are covered and how claims are submitted, reviewed, and adjudicated (see Table 1 for a comparison of key characteristics of these programs).
VICP
There are currently 16 vaccine types covered under the VICP program. By statute, VICP covers FDA approved vaccines used in the U.S. that are 1) recommended by the CDC for “routine administration” to children or pregnant women, 2) subject by Congress to the VICP excise tax, and, 3) added to the official VICP vaccine injury table by the Secretary of HHS. When first passed in 1986, VICP covered 6 vaccines, a number that has grown to 16 existing vaccines, including the components of common childhood vaccines such as DPT, MMR, and polio as well as child and adult vaccines such as seasonal influenza. The VICP also covers “any new vaccine” recommended by CDC, subject to an excise tax and issued a notice of coverage by the Secretary of HHS.
The vaccine injury table is a key VICP document listing vaccine types and injuries compensable by VICP. The table lists and explains injuries presumed to be caused by vaccines and the time periods in which the first symptom of these injuries must occur after receiving the vaccine. The current table lists 14 compensable injuries across the 16 vaccine types, with most injuries associated with one or a few vaccine types only. For example, “chronic arthritis” is listed as a potential injury associated only with rubella-containing vaccines, and “vaccine-strain polio infection” is only associated with oral polio vaccine. Others are associated with multiple vaccine types, such as “shoulder injury” and “vasovagal syncope” (i.e. a drop in blood pressure and heart rate), which are each listed for 15 vaccine types.
VICP claims are submitted to HHS and the U.S. Court of Federal Claims and reviewed through a judicial process overseen by the Office of Special Masters. An individual (or legal representative) must first file a petition with the U.S. Court of Federal Claims “Office of Special Masters” which handles VICP cases. “Special Masters” are specialized officers of the court who function similarly to a judge. Upon receipt, each claim is assigned to one of eight Special Masters and initially reviewed by specialized HHS staff for compliance with VICP submission requirements. Documentation to support an injury claim must be provided, and typically only injuries listed on the vaccine injury table are eligible for compensation. For injuries not on the table, a petitioner must prove, through medical documentation and/or expert opinion, that the vaccine in fact caused the alleged injury. VICP typically pays petitioners’ legal fees, even if the claim is eventually unsuccessful.
Special Masters issue a ruling on compensation based on a “preponderance of evidence” standard. VICP is designed as a no-fault system, meaning petitioners do not need to prove negligence on the part of vaccine makers or health care practitioners. With sufficient documentation of an injury matching a condition and fitting the timetable listed on the vaccine injury table, it is usually presumed that the vaccine caused the injury. In some cases, additional information is needed such as expert testimony or medical research findings to support injury claims, and evaluating evidence may require hearings with witnesses.
Petitioners can accept or reject a compensation decision, with the option for appeal. If a ruling is made in favor of a petitioner, the Special Master determines the level of compensation, which a petitioner can accept or reject. If the claim is denied, the petitioner can seek review by a judge of the Court of Federal Claims and potentially appeal further to the U.S. Court of Appeals. If the claimant moves through all appeals and is still denied compensation, then they may have the right to subsequently file a suit in civil court (with some limitations).
The Secretary of HHS can modify the VICP vaccine injury table, though changes must abide by a statutory process including external expert review and a public comment period. The Secretary of HHS has the explicit authority to modify the vaccine table, though any changes are subject to a process outlined in statute (42 U.S.C. § 300aa-14) and federal regulations (Code of Federal Regulations (CFR) Part 100), including referred to an external expert advisory body known as the Advisory Commission on Childhood Vaccines (ACCV), which has at least 90 days to review suggested changes. In addition, HHS must follow Administrative Procedures Act (APA) guidelines, including publishing a Notice of Proposed Rulemaking (NPRM) in the Federal Register and a 180-day public comment period. Adding a new vaccine to the vaccine injury table requires that new vaccine to be recommended for routine use by CDC, and for Congress to apply an excise tax on that vaccine, before HHS can publish a notice of coverage and submit related changes to the vaccine injury table.
The VICP vaccine injury table has rarely been updated; its last major revision was in 2017. At that time, “Shoulder Injury Related to Vaccine Administration, or SIRVA was added. HHS proposed adding this to the Table, submitted it to ACCV for input, and in 2015 published the related NPRM. In 2017 HHS issued the final ruling after reviewing and responding to public comments, as required under APA.
CICP
CICP covers countermeasures used in federally declared public health emergencies, which has included COVID-19 vaccines, as well as vaccines for pandemic influenza, smallpox, and mpox. By statute, covered countermeasures are those that the Secretary of HHS specifically lists in the declarations issued under the PREP Act for each health emergency. Currently, there are 10 such declarations in effect covering countermeasures against health emergencies, including Anthrax, Ebola, Marburg, pandemic influenza, mpox, and COVID-19.
CICP claims are reviewed through an administrative process by HHS staff, rather than a judicial process. Individuals submit a request to the Health Resources and Services Administration (HRSA) within HHS, which administers CICP. Filings must include sufficient medical records and other documentation linking the countermeasure and the individual’s claimed injury. In contrast to VICP, there no judges or hearings under CICP. Instead, claims are reviewed internally by HHS medical and legal staff. CICP does not pay petitioners’ legal fees.
CICP does not have a single “injury table” reference for covered countermeasures, with claims typically requiring individualized, case-by case review. Some declared health emergencies – including smallpox and pandemic influenza – have a specified countermeasure injury table, but most do not (COVID-19 countermeasures, for example, do not have an injury table). Therefore, most claims require individualized scientific review and case-by-case considerations. To receive compensation, a petitioner must show “serious physical injury was sustained as the result of the use of a covered countermeasure,” which is a higher evidentiary standard compared to VICP.
CICP decisions leave little room for appeal. HRSA issues a written determination on whether the injury is eligible for compensation under CICP and, if found eligible, how much compensation is awarded. If found ineligible, a petitioner can request reconsideration, but further review is still handled internally, with no process for formal legal appeal. In most cases, individuals who have pursued compensation through CICP cannot go on to pursue lawsuits in civil court against manufacturers or providers for covered countermeasures.
The HHS Secretary has broad authority to make changes to countermeasures and injuries covered under CICP. The PREP Act provides the HHS Secretary more discretion and imposes fewer regulatory requirements on the process to make changes to injuries covered by CICP, compared to VICP. The Secretary can determine which countermeasures are covered and which injuries are presumed to be compensable under the CICP, and there is no statutory requirements for advisory committees or public comment periods for changes to these policies.
Historical Data on Petitions and Compensation Decisions
The number of petitions submitted to VICP and CICP has varied over time, and both programs have seen large increases in petitions in certain years driven by different factors, such as a surge in CICP claims related to COVID-9 vaccines starting in 2021 (COVID-19 claims comprise most CICP petitions at this point). Overall, VICP provides compensation for a much greater share of its petitions compared to CICP (48% compared to less than 1% for COVID-19 vaccine petitions), largely reflecting the differences between the programs. Still, given the large number of vaccines administered in the U.S., very few petitions or claims in either program are found to be compensable relative to vaccines received (1.89 VICP compensable petitions per million vaccine doses and 0.14 compensable CICP claims per million COVID-19 vaccine doses).
VICP
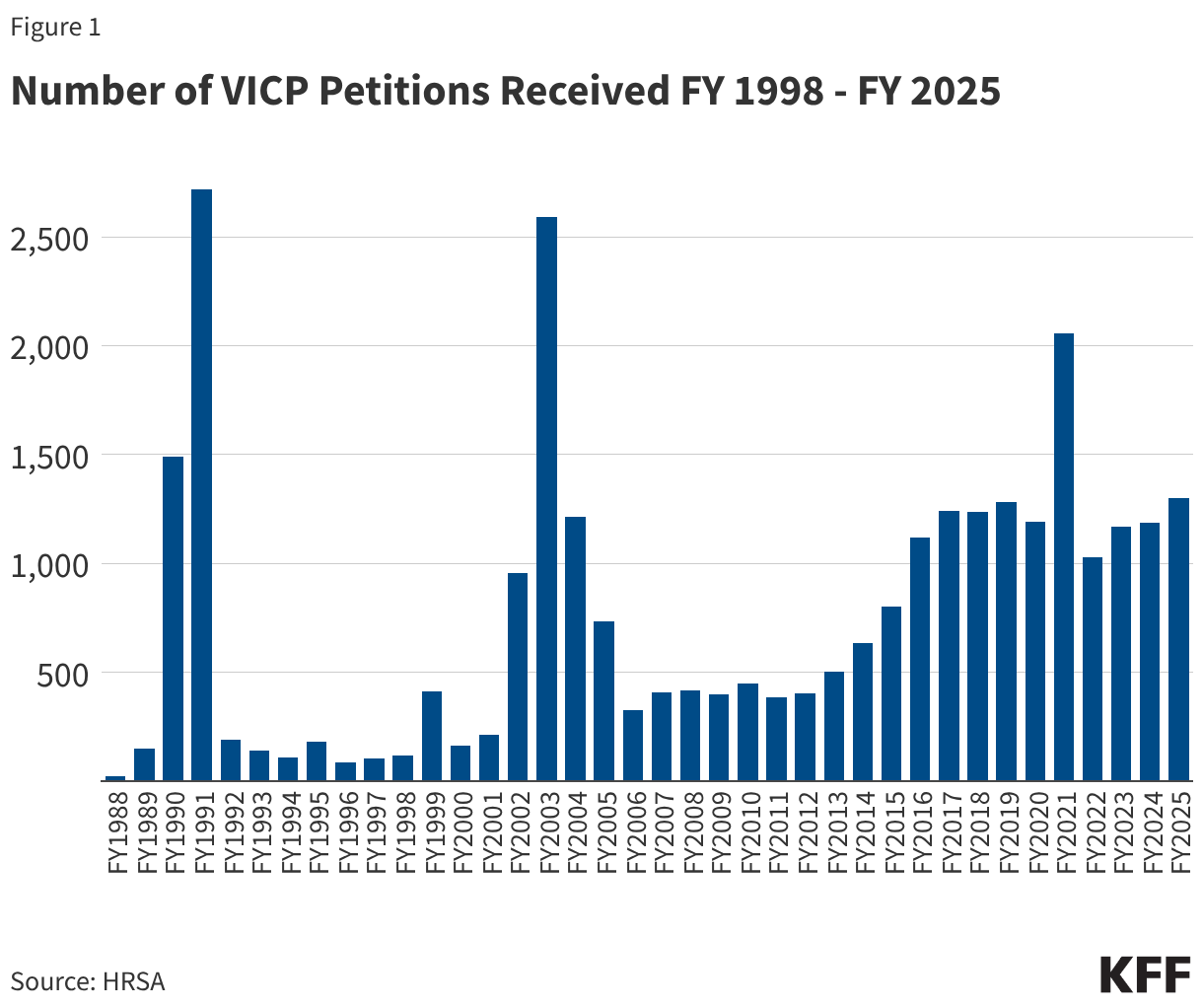
From FY 1988 through FY 2025, VICP received a total of 28,673 petitions. The annual number of petitions has varied over time, including notable surges in some years (see Figure 1). Surges occurred in FY 1990 and FY 1991 (1,492 and 2,718 VICP petitions were filed, respectively) due to a large increase in claims stemming from parental concerns about injuries caused by DPT vaccines. There was also a surge a decade later, primarily reflecting a wave of public concern about MMR vaccine after reports (later found to be false) that the vaccine could be linked to autism.1 Since FY 2014, there has been a general increase in the number of petitions filed, with the average number growing from 466/year during the FY 2005-FY 2014 period to 1,238/year during FY 2015-FY 2025. This increase may be linked to policy changes that expanded the scope of the vaccine injury table, such as the inclusion of “Shoulder Injury Related to Vaccine Injury (SIRVA),” which was formally added in 2017.
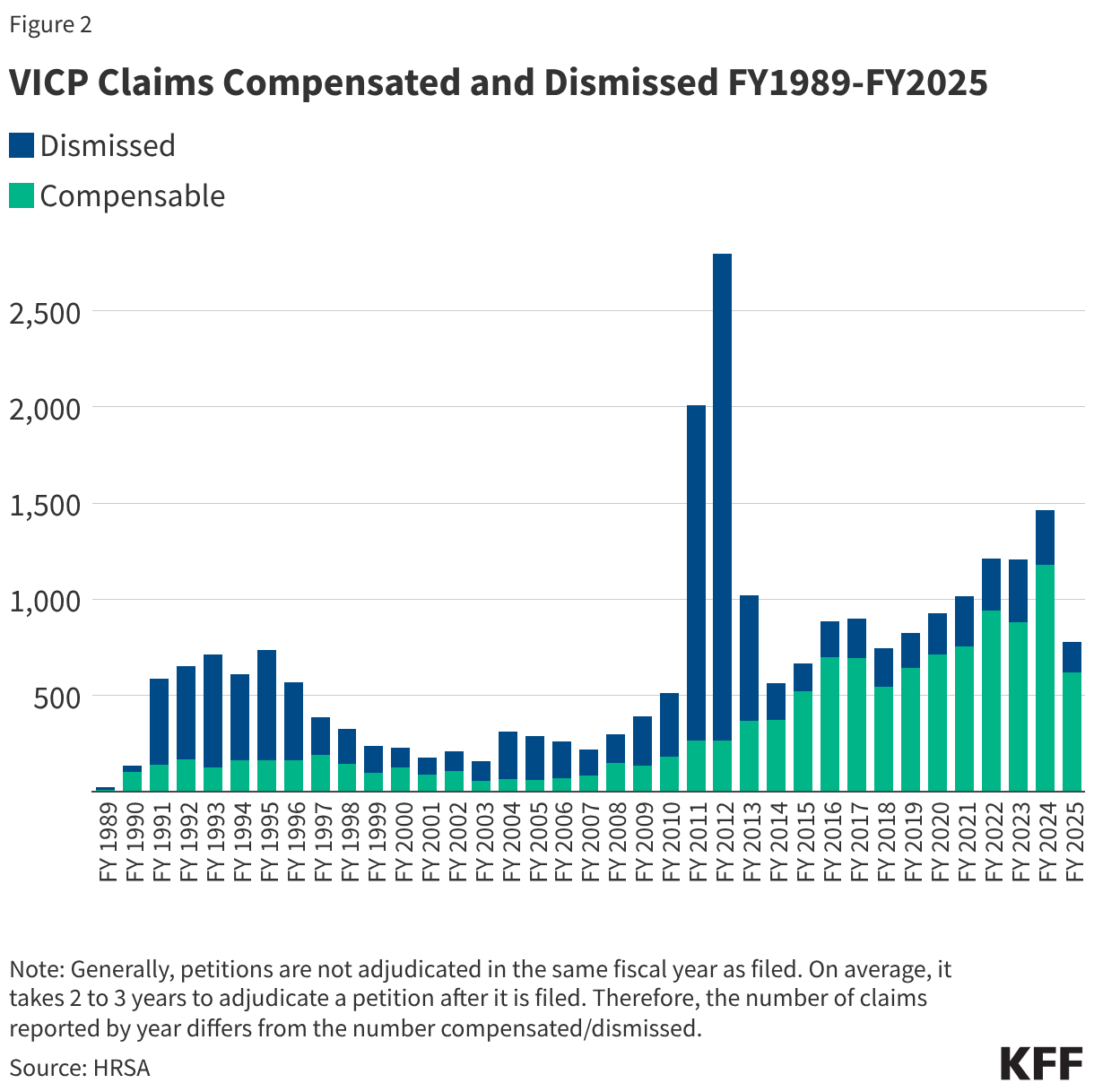
25,026 VICP petitions (87% of all 28,673 petitions received) have been adjudicated through FY2025, with 12,019 (48%) found to be compensable and 13,007 (52%) dismissed. As shown in Figure 2, the share of compensable injuries has generally increased in recent years compared to earlier periods of the program, with 77% of petitions found compensable between FY 2016-FY 2025 compared to 28% of petitions in the prior 10-year period (FY2006-FY2015). This again may be partially attributed to increasing scope of the vaccine injury table. The notable spike in claims dismissed in FY 2011-FY 2012 was a result of the resolution of the Omnibus Autism Proceedings allowing a backlog of claims related to autism as a vaccine injury to be processed and dismissed when the program found no credible evidence that vaccines were the cause of autism.2
The number of VICP claims and compensation adjudications represents a tiny fraction of the number of vaccines distributed in the U.S. According to HRSA and CDC data, from January 1, 2006 to December 31, 2024 there were 5.65 billion doses of VICP-covered vaccines distributed in the U.S.. During this same period, there were 14,409 VICP petitions filed, or 2.6 VICP petitions per million doses distributed. Of these, 10,633, or 1.89 petitions per million doses, were found to be compensable.
CICP
Between FY 2010 and FY 2026 (through March 1, 2026) CICP received a total of 14,733 claimsfor covered countermeasures. CICP reports it has reached a decision on 7,423 (50%) of those claims, finding 135 (1.8%) were eligible for compensation. The remainder are still being processed.
The majority of CICP petitions received were related to COVID-19 vaccines (10,981 or 75% of all petitions filed). CICP has reached a decision on 6,827 (62%) of these. Overall, 95 (0.9%) of COVID-19 vaccine claims been found eligible for compensation through CICP. With over 670 million doses COVID-19 vaccines administered in the U.S. between December 2020 and May 2023, that translates into approximately 16 petitions filed per million doses administered, and 0.14 compensation-eligible claims per million doses.
Relatively few non-COVID-19 vaccine countermeasure claims have been filed through CICP. For example, CICP reports 29 compensation payments were made related to the 2009 H1N1 vaccine (after approximately 90 million doses were administered in the U.S., translating to about 0.3 compensation payments per million doses administered). One CICP compensation payment was reported related to the smallpox vaccine, though CICP reports that 8 petitions related to the mpox vaccine and 2 additional claims related to the smallpox vaccine have been filed and are still being processed.
Publicly available information about CICP claims and compensation is limited compared to VICP. In contrast to VICP, CICP does not report petitions received or claims processed by year and does not publicly release details on the rationale for compensation decisions.
Funding and Expenditures
These two programs have different funding sources, with VICP funded through a trust fund holding revenues collected from the excise taxes and CICP funded through the annually-appropriated funds provided to HHS/HRSA. Compensation award amounts through VICP, while variable, have averaged between $500,000 and $1 million for most of the program with some recent declines.. In contrast, most awards (75%) through CICP are for amounts under $10,000, though there have been a few very large individual payments exceeding $1 million.
VICP
VICP is funded through revenues collected from an excise tax placed by Congress on every dose of each vaccine covered under VICP produced in the U.S.. The excise tax is paid into a Vaccine Injury Compensation Trust Fund overseen by the U.S. Treasury. The Trust Fund also generates revenue from investing its assets. Treasury uses Trust Fund resources to make payments and transfers to government agencies responsible for administering VICP including the Department of Justice, the U.S. Court of Appeals, and HHS/HRSA.
Over time, the VICP trust fund has grown as its annual revenues typically exceed expenses. The U.S. Treasury reports that as of September 30, 2025 the VICP trust fund held $4.66 billion. In FY 2025, $363 million was added to the trust fund (including $131 million from excise taxes, $169 million from interest on investments, and $63 million in refunds from current and prior year authority). VICP expenses totaled $314 million in FY 2025, which were primarily for compensation payments but also administrative and other costs.
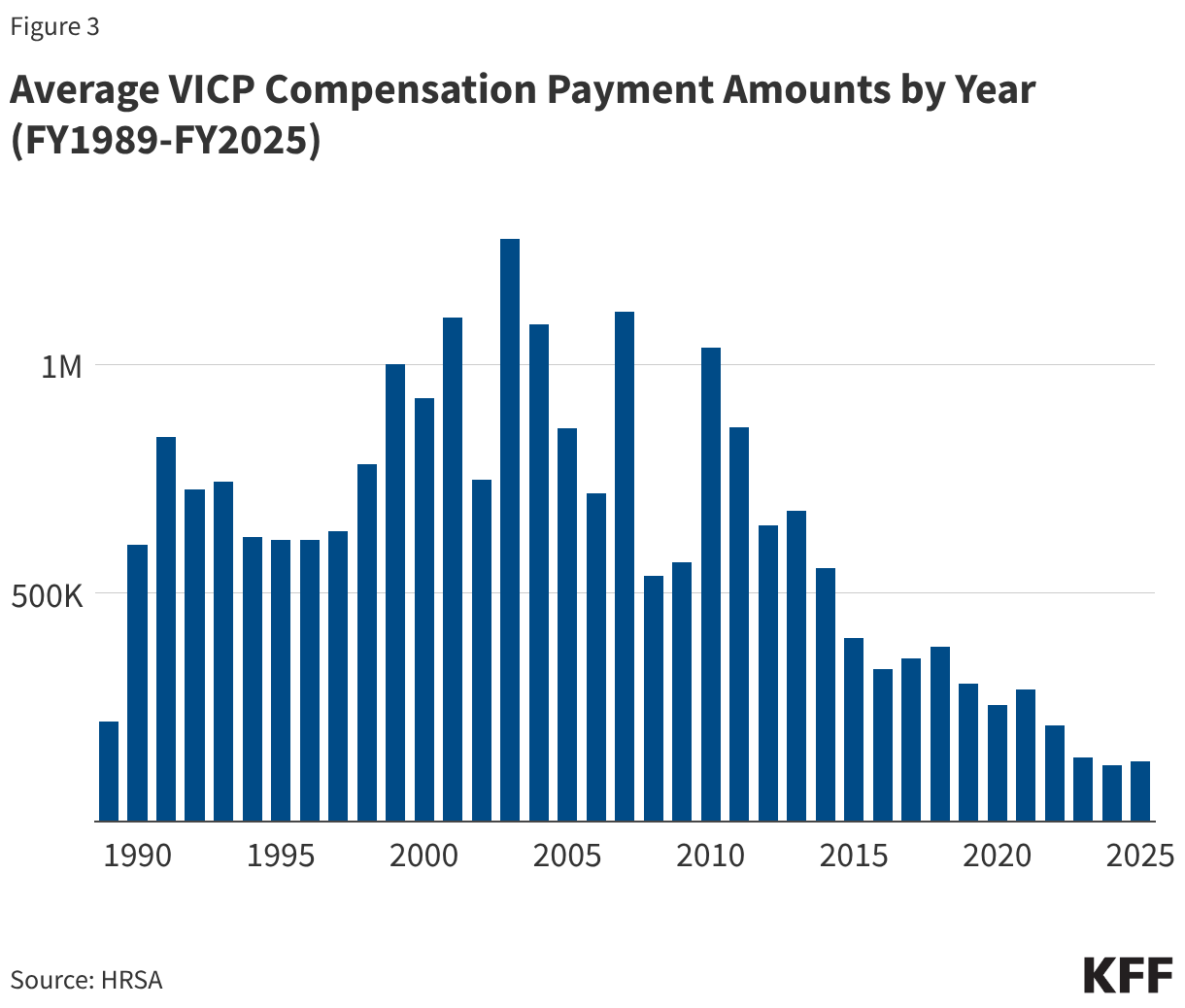
12,409 VICP compensation payments have been awarded between FY1989 and FY2025 totaling $4.89 billion (see Figure 3). Since the early 2010s, the average amount of compensation has generally declined, and has remained below $500,000 since FY 2015, likely a reflection of the expansion of the vaccine injury table to include milder injuries such as SIRVA (which entail comparatively lower payments relaive to other injuries).
CICP
There is no specific tax or dedicated funding source for CICP compensation payments, as there is for VICP. CICP funding comes from annual Congressional appropriations to HRSA rather than an excise tax. Through the PREP Act Congress created a “Covered Countermeasures Process Fund (CCPF)” to be administered by HRSA for CICP purposes, though little information is available on how much funding – if any – is currently held in the CCPF. At times Congress has provided emergency appropriations (such as the CARES Act during the COVID-19 response) that allowed, but did not require, HHS to direct funds to the CCPF.
Several large single payments comprise the majority of all compensation provided by CICP since 2010. There is only limited information about CICP expenditures, which includes the number and amounts of CICP compensation payments that have been made since FY2010. According to this data, CICP has paid compensation for 81 claims totaling more than $13 million. Most of the this total comes from a few very large single compensation payment amounts – for example there are reported payments of $5.9 million (related to thrombotic thrombocytopenia syndrome injury linked to COVID-19 vaccination), $2.3 million, and $1.8 million (the latter two related to Guillain-Barre Syndrome injury linked to 2009 H1N1 pandemic influenza vaccines). Of the 81 claims that received compensation, 11 (14%) were for amounts over $100,000, 10 (12%) were for amounts between $10,000 and $100,000, and 60 (74%) were for amounts under $10,000.
There are significant caseload, backlog, and capacity constraints in both programs. As noted above, there has been a growing number of petitions filed for each these programs over the last few years. However, the staffing and resources allocated to the programs have not matched this growth. For example, the VICP is limited by statute to eight special masters, with each now facing a larger caseload. The CICP has faced a surge of claims related to COVID-19 vaccines since 2021. The growing burden of claims and limited set of resources has contributed to long case review times and delays in issuing decisions and settlements.
The question of how best to address COVID-19 vaccine injuries has been an ongoing issue, particularly now that the COVID-19 public health emergency has ended. Under current law, COVID-19 vaccines are still covered under the CICP through the end of 2029. However, because CICP was created to address smaller scale deployments of medical countermeasures during a health emergency, rather than national-level responses to pandemics that extend over years, it has faced limitations in taking on COVID-19 vaccine injuries. Available compensation is generally lower compared to VICP, and the standard of proof for non-table injuries is higher. Even though the deployment of COVID-19 vaccines began as an emergency countermeasure during a national health emergency, these vaccines have become integrated into routine vaccinations and are recommended by CDC for broad segments of the U.S. population. For that reason, some health policy experts, lawyers, and politicians have advocated for including COVID-19 vaccines under VICP rather than CICP.
Politicization of vaccines and strains on scientific credibility threaten confidence in and stability of these programs. As views about vaccines have become more politicized, vaccine injury compensation programs have become a frequent target of partisan criticism. There is a striking partisan divide on the benefits and risks of COVID-19 vaccines, for example, with Republicans seeing those vaccines as causing more harm and arguing for more injury compensation as a result, compared to Democrats. This has also played out in actions taken by the Trump administration, such as seeking to narrow recommendations for several childhood vaccines and calling into question vaccine safety. On VICP, the Secretary of HHS Kennedy has argued that the program is too restrictive and the number and scope of vaccine injuries covered should be expanded to include conditions such as autism, though there is no credible evidence that vaccination causes autism, and the VICP itself reviewed available evidence on autism and vaccines during the Omnibus Autism Proceedings in the early 2000s and found no scientific evidence to support the link. Secretary Kennedy has also said that VICP has become a “morass of inefficiency, favoritism, and outright corruption.” Advocates linked to Secretary Kennedy have argued for expanding the VICP injury table to cover as many as 300 additional conditions they claim are injuries linked to vaccines. Others have raised concerns that adding injuries without sufficient scientific evidence to do so threatens the credibility of these programs and could even lead to insolvency if the scope of covered “injuries” expands to highly prevalent conditions like autism.
Updating legislation and regulations on compensation payment rules and related policies is politically challenging. A frequent criticism of these programs is that compensation payments were set when the programs were first created and have not been updated over time to reflect new developments and are not indexed to inflation. VICP, for example, has the same $250,000 cap on compensation for injuries or death that was in place when the program was established in 1988. However, making changes to these rules would require that Congress amend the underlying legislation, and doing so has proven politically challenging (changes were last made in 2016 through the “21st Century Cures Act”). There have been multiple legislative proposals introduced to update and modernize the vaccine injury compensation systems legislation but none has advanced. For example, the Vaccine Injury Compensation Modernization Act (H.R. 5142), which was last introduced in 2022-2023, proposed changes such as: increasing the number and tenure of special masters, requiring a formal plan to eliminate backlog, moving COVID-19 vaccines from CICP to VICP, increasing compensation caps and indexing payments to inflation, and increasing transparency and reporting requirements. Another proposal, recognizing that CICP has been inundated with claims for COVID-19 vaccines even though the program was designed with a smaller scale in mind, would replace that program with a “pandemic injury compensation system” that would be pre-funded, scalable, and automatically activated during a public health emergency. However, these bills have not advanced.
Endnotes
Due to the increased public concern about a potential vaccination-autism link and the large number of related claims filed, VICP established a special program in 2002 called the Omnibus Autism Proceeding, which evaluated several hypotheses for vaccine-autism links, ultimately finding that there was no causal relationship. No scientific evidence has shown autism to be linked to childhood vaccines, therefore autism is not included as an injury in the VICP vaccine injury table. ↩︎
Due to the increased public concern about a potential vaccination-autism link and the large number of related claims filed, VICP established a special program in 2002 called the Omnibus Autism Proceeding, which evaluated several hypotheses for vaccine-autism links, ultimately finding that there was no causal relationship. No scientific evidence has shown autism to be linked to childhood vaccines, therefore autism is not included as an injury in the VICP vaccine injury table. ↩︎
This analysis, originally published on June 17, 2025, was updated to note that changes to the final legislation that became law reduced the number of low-income Medicare beneficiaries who would be affected. CBO did not provide a detailed analysis of the impact, but based on available information the number is likely somewhat lower.
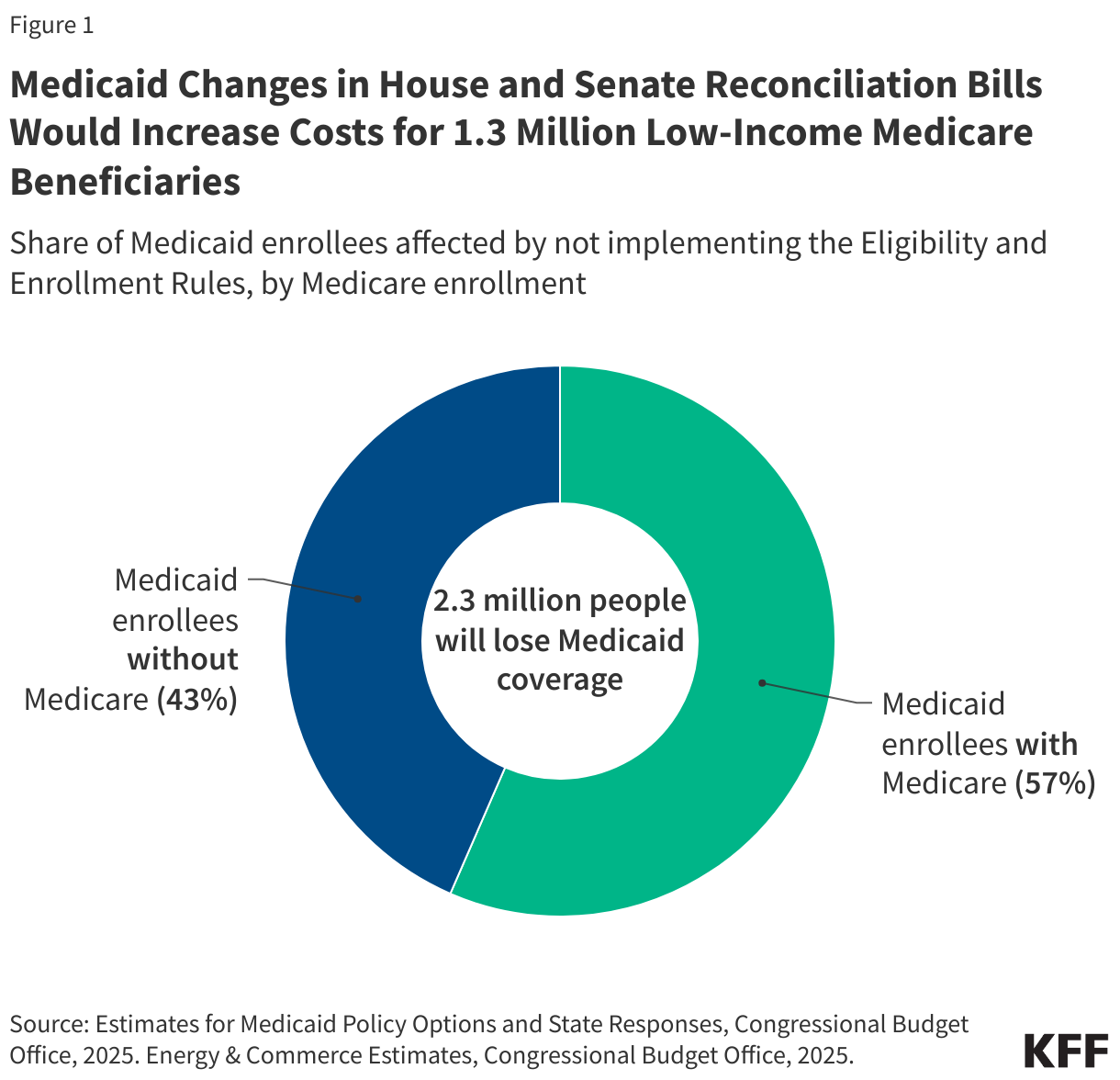
On May 22, the House passed a reconciliation bill, the One Big Beautiful Bill Act, which would partially pay to extend expiring tax cuts by cutting Medicaid. The Congressional Budget Office (CBO) estimates that the bill would reduce federal Medicaid spending by $793 billion over ten years and 10.3 million fewer people would be enrolled in Medicaid in 2034, including 1.3 million people with Medicare, otherwise known as “dual-eligible individuals”. The loss of Medicaid coverage for Medicare beneficiaries stems from delaying implementation of two rules that aimed to streamline the enrollment process and make it easier for people to maintain Medicaid coverage by reducing administrative barriers. Dual-eligible individuals would be disproportionately impacted by these provisions, comprising nearly 60% of the 2.3 million Medicaid enrollees who are estimated to lose coverage as a result of delaying these rules under the House reconciliation bill (Figure 1). Instead of placing a moratorium on implementation of the rules, the recently released Senate reconciliation language would prohibit nearly all of the provisions in the rules from ever being implemented.
Dual-eligible individuals have low incomes and modest savings. The 1.3 million people that would no longer have Medicaid if the eligibility and enrollment rules were not implemented would retain their primary health insurance coverage under Medicare, but lose Medicaid coverage of Medicare premiums, and in most cases, cost sharing, which are provided through Medicare Savings Programs (MSPs) administered by state Medicaid programs. Many would also lose coverage of Medicaid benefits that supplement their Medicare coverage, such as long-term care, dental services, and non-emergency medical transportation.
The loss of Medicaid coverage for Medicare beneficiaries stems from provisions in the House bill that would delay implementation of two Biden administration rules until 2035. The two rules that would be delayed under the House reconciliation bill were intended to make it easier for people to enroll in and maintain Medicaid coverage by minimizing administrative burden in the following ways.
One rule aimed to reduce barriers to enrollment in the Medicare Savings Programs (MSPs), under which Medicaid pays Medicare premiums, and in most cases, cost sharing for low-income Medicare beneficiaries. Among other changes, the rule would automatically enroll Medicare beneficiaries with Supplemental Security Income (SSI) into the MSPs and would more closely align the MSP application to the application for Medicare’s Part D prescription drug Low-Income Subsidy (LIS).
The second rule would more broadly streamline application, enrollment, and renewal processes in Medicaid. Among the changes most relevant for dual-eligible individuals are new requirements for states to assist applicants with procuring appropriate documentation to validate income and assets, a requirement to renew Medicaid coverage only once per year, and a prohibition on requiring in-person interviews as part of the application process
CBO estimates that delaying these two rules would reduce federal spending by $167 billion over 10 years, making this the second largest source of cuts to federal Medicaid spending in the bill. Illustrating why administrative burdens may make it hard for dual-eligible individuals to maintain Medicaid, prior KFF research finds that among people who newly become eligible for both Medicare and Medicaid, 28% lose Medicaid coverage within the first year despite living on fixed incomes.
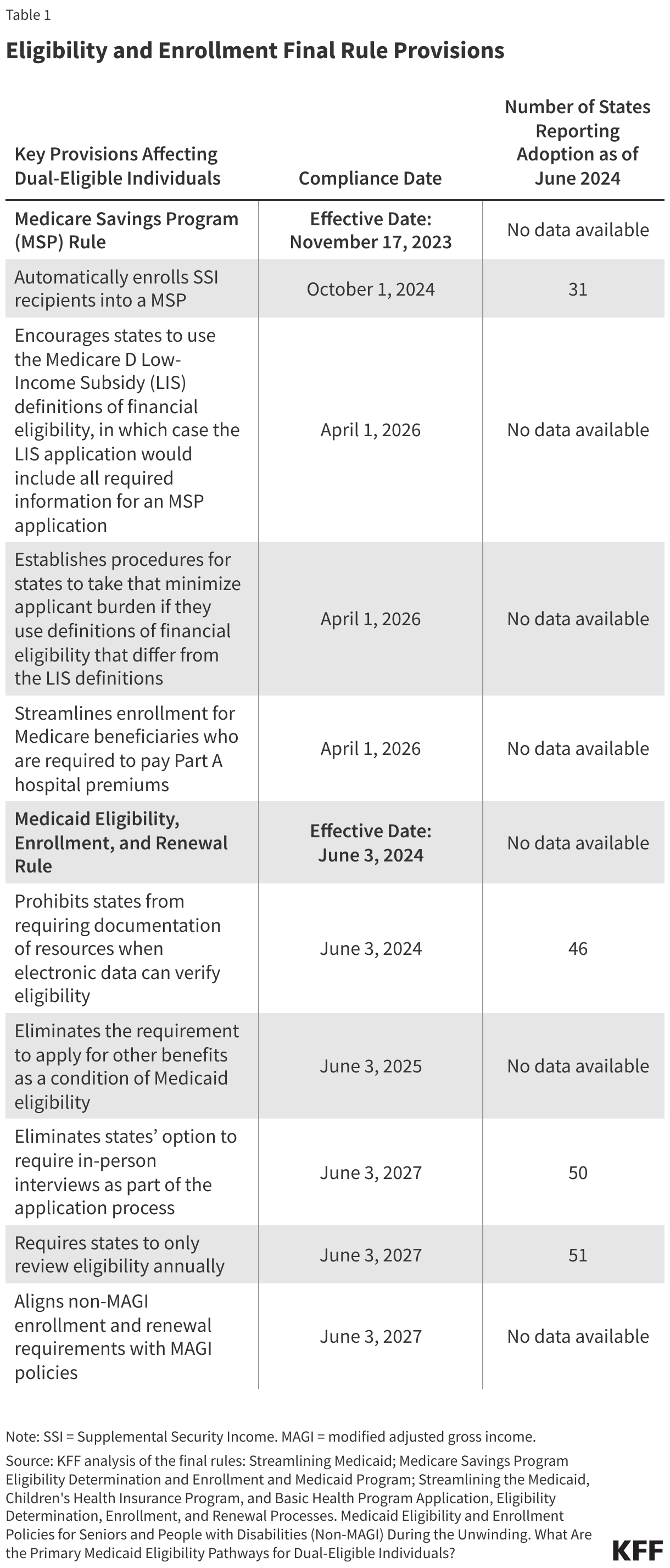
Although states have already implemented some of the rules’ provisions (Table 1), if the rules are delayed, it is expected that further implementation will cease and states may resume some practices that were prohibited under the rules. For example, 38 states report sending pre-populated renewal forms to Medicaid enrollees who qualify because they are ages 65 and older or have a disability, a practice they may discontinue if the rules are delayed. Alternatively, it’s possible that some states will reinstate requirements for applicants to submit paper documentation or report for in-person interviews. In a few cases, states will be required to reinstate application requirements or be prohibited from using more streamlined application processes.
Losing Medicaid coverage would substantially increase out-of-pocket costs for low-income Medicare beneficiaries. Because Medicare beneficiaries who qualify for Medicaid typically have very low incomes and little to no savings, the loss of Medicaid payment for the costs of Medicare’s premiums and cost sharing could make their Medicare coverage unaffordable. For example, the first rule would automatically enroll low-income Medicare beneficiaries who receive Supplemental Security Income (SSI) into a MSP. Without the MSP, such people must pay 20% of the $967 SSI monthly benefits for the $185 Medicare Part B monthly premium in 2025. (In order to qualify for SSI, individuals must have low incomes, limited assets, and either be over age 64 or have a qualifying disability.) This same individual would have additional out-of-pocket costs if they went to the doctor or were admitted to the hospital. Those additional out-of-pocket costs could discourage low-income beneficiaries from using health care and is the reason for CBO’s estimate that delaying implementation of the rules would reduce Medicare spending by $11 billion over 10 years.
Additionally, some of the 1.3 million Medicare beneficiaries expected to lose Medicaid under the House reconciliation bill may also lose subsidies that help pay for prescription drug premiums and cost sharing. Medicare beneficiaries with Medicaid are automatically enrolled in the Medicare Part D Low-Income Subsidy (LIS), which provides assistance with Part D prescription drug premiums and cost sharing. Illustrating the connection between Medicaid enrollment and LIS coverage, between December 2024 and January 2025, the number of LIS recipients decreased by 1 million, following Medicaid disenrollments that stemmed from the unwinding of the Medicaid continuous enrollment provision. Before the decline, LIS enrollment had been slowly but steadily growing over time.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Medicaid is the primary program providing comprehensive coverage of health care to about 80 million low-income people in the U.S. Medicaid is an insurance program, not a population health system. It can only fund services for eligible individuals. The public health system in the U.S. is decentralized, with most authorities and programs delegated to the state and local levels. State and local public health agencies are responsible for protecting community health through surveillance, disease prevention, and policy development and enforcement. Local health departments frequently focus on service delivery (immunizations, screenings, maternal health, environmental health) and community outreach to address local health needs. Public health serves entire communities, not just insured individuals.
Medicaid agencies and state/local public health agencies work to advance the health of their communities, often with similar priorities serving common populations. However, there is often a lack of strong and sustained partnerships between Medicaid and public health agencies. Strengthening collaboration between Medicaid and public health could improve safety net services, help coordinate and leverage resources and financing, improve intervention targeting and outreach, and reduce system fragmentation.
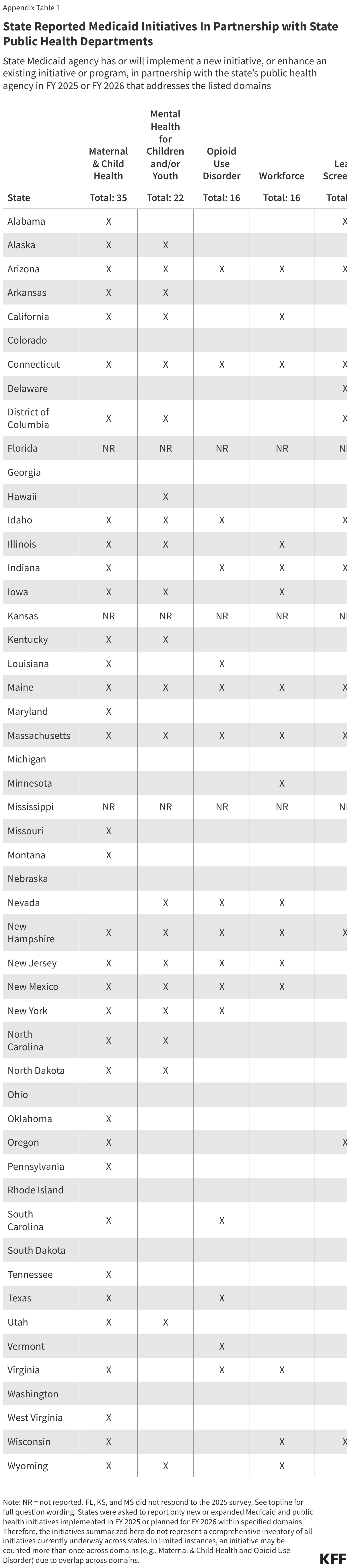
To improve understanding of Medicaid and Public Health agency partnerships, the 25th annual Medicaid budget survey, conducted by KFF and Health Management Associates (HMA) in collaboration with the National Association of Medicaid Directors (NAMD), asked state Medicaid directors about new or enhanced initiatives involving public health implemented in FY 2025 or planned for FY 2026 across the following domains. (The survey did not capture the full scope of established Medicaid and Public Health agency partnerships across states, including initiatives implemented or expanded before FY 2025 – FY 2026, nor all activity within these domains as states select which efforts to report.)
More than three quarters of responding states1 reported at least one new or expanded initiative implemented in FY 2025 or planned for FY 2026 (see Appendix), with maternal and child health and behavioral health emerging as areas of focus for newly implemented or expanded Medicaid and Public Health initiatives. Initiatives frequently fell into common areas, including data sharing, rural-focused initiatives, initiatives to improve access, and workforce initiatives.
Findings
States were asked to report only new or expanded Medicaid and Public Health initiatives implemented in FY 2025 or planned for FY 2026 under specific domains. Therefore, initiatives summarized and reported here do not represent a comprehensive look at all initiatives currently in place across states. State counts are not identified in the sections below, as open-ended questions often lead to underreporting. See Appendix for additional (high-level) state-by-state detail.
To track common themes across domains, state responses have been summarized (at a high-level) under the following subheadings, as applicable: “data sharing,” “rural,” “workforce,” “access,” and “other.” State examples are included in text boxes under each domain. While the survey asked about workforce initiatives separately, “workforce” also emerged as a theme applicable to other domains. These initiatives are only summarized once (e.g., do not appear under the separate “workforce” domain if they also fell under another domain).
Maternal & Child Health
Conception through early childhood represents an important period for intervention to promote long-term health and other outcomes. More than one in four Medicaid/CHIP enrollees is a female in their reproductive years. Medicaid is the primary payer for about 41% of all births and provides coverage for 37% of all children in the U.S. Public health agencies often oversee maternal and child health surveillance, prevention, and early childhood initiatives to improve outcomes and reduce gaps in health outcomes and access.
States reported new or expanded maternal and child health initiatives in the following areas:
Data sharing. States reported cross-agency data sharing initiatives to strengthen maternal and child health surveillance.
Rural. States reported collaborative efforts to address rural maternal health needs, as individuals in rural areas face access challenges (lack of local obstetric services) and geographic barriers.
Workforce. Statesmentioned collaborating with public health agencies to certify and support community health workers (CHW), including doulas and other perinatal providers.
Access.
Transforming Maternal Health Model. States reported collaborating with public health agencies on implementing CMS’s Transforming Maternal Health Model (TMaH), identifying collaboration as important to developing strategies to direct resources / interventions to high-need communities. CMS’s TMaH model supports state Medicaid agencies in implementing evidence-based strategies to expand access to maternal care, integrate behavioral health and social determinants of health, and ensure care continuity in the postpartum period.2
Coverage expansions. States pointed to expansion of Medicaid coverage of maternal and child health services, such as doula and lactation services. Some described partnering with public health agencies to inform coverage expansions through shared data and collaborative program design.
MH/SUD expansions. States highlighted initiatives to integrate and/or expand mental health (MH) and/or substance use disorder (SUD) services for pregnant and parenting populations, including home visiting services for pregnant and postpartum individuals.
Other.
Interagency workgroups. States described leveraging interagency workgroups and committees to facilitate coordination and to advance maternal and child health priorities, including improving outcomes and addressing complex factors (e.g., social needs) that a single agency can’t solve alone.
Box 1: State Examples of Maternal and Infant Health Initiatives
Data Sharing:
The OklahomaMedicaid Birth Certificate Linkage Project is supported by an interagency agreement between the Oklahoma Health Care Authority (the state agency that administers the Medicaid program) and the Oklahoma State Department of Health. The project links vital records (birth certificate) data to Medicaid data to provide a more complete picture of pregnancy and birth outcomes of Medicaid enrollees.
Rural:
As part of a two-year HRSA-funded Maternity Care Deserts Policy Academy run by the National Academy for State Health Policy (NASHP), Kentucky Medicaid is working with the state’s Department of Public Health to identify maternity care deserts in the state and to develop solutions to connect pregnant individuals to care. (Maternity care deserts are places with no hospitals or birth centers offering obstetric care and no obstetric providers.) The Kentucky Perinatal Quality Collaborative and other state organizations are also involved.
Workforce:
Massachusetts reported providing training and technical assistance to MassHealth (Medicaid) providers to support maternal health initiatives, including efforts to strengthen care coordination and outreach and to support implementation of state maternal health legislation (enacted in 2024) that aims to expand access to midwifery, birth centers, doulas, and postpartum home visiting services.
Access:
California’s Department of Health Care Services was awarded $17 million in federal funding to implement CMS’s Transforming Maternal Health Model in five counties in the Central Valley. The model will provide funding to transform three key areas: access to care, infrastructure, and workforce; quality improvement and safety; and whole person care delivery (i.e., customized care to meet an individual’s unique needs). The Department of Health Care Services will work with managed care plans, providers, community-based organizations, and other partners to implement the model and to ensure alignment with the state’s Birthing Care Pathway initiative, a broader statewide effort to improve maternity care and outcomes.
To improve maternal health outcomes, Illinoisadded doula and lactation support services (without requiring physician referral) to its Medicaid coverage. The Department of Public Health supported the coverage expansion, highlighting differences in maternal health outcomes by race and ethnicity in the state.
Louisiana reported the state Department of Health launched Project M.O.M. (Maternal Overdose Mortality) in May 2025. Project M.O.M. aims to reduce pregnancy-associated opioid overdose deaths through early identification and treatment of substance use disorder during pregnancy. The project will convene hospital and community partners and aims to align managed care plans and health care providers to improve access to care and treatment coordination.
Montana Medicaid is partnering with state public health to implement targeted case management and evidence-based home visiting for pregnant and postpartum individuals and parents of children ages 0-5 who meet high-risk criteria, including mental health/SUD criteria.
Other:
Arizona reported that its Medicaid agency will continue to strengthen its relationship with the state Department of Health Services through ongoing participation in health-focused workgroups and committees, including the Maternal Mortality Review Committee, Congenital Syphilis Collaborative, Perinatal and Infant Health Committee, Home Visiting Workgroup, among other groups and committees.
Children/Youth Mental Health
Early childhood and adolescence are important developmental periods that can influence long-term health. In recent years, there have been growing concerns about children’s mental health and well-being. Medicaid provides health coverage for 37% of children in the U.S. and plays a significant role in funding school-based behavioral health services. Nearly one in five students attending public schools in the U.S. use school-based mental health services, underscoring how schools serve as an important access point for youth mental health treatment. Public health agencies may be involved in assessing the status of statewide and community early childhood mental health, developing policy and programming for youth and caregivers, encouraging participation in mental health programs, and partnering to maintain school-based behavioral health services.
States reported new or expanded children/youth mental health initiatives in the following areas:
Workforce. States reported working with public health agencies to connect PCPs to psychiatrist consultations, including initiatives specifically targeting rural areas.
Access. Statesreported collaborating with public health agencies on maintaining and increasing access to school-based services, which offer a convenient setting for delivering health services to students (overcoming transportation and other barriers), including mental health services.
Box 2: State Examples of Children/Youth Health Initiatives
Workforce:
Kentucky’s Medicaid agency reported working with the Kentucky Department of Public Health on “KY MARK,” an initiative that helps PCPs better manage children’s mental health issues by partnering with University systems to connect primary care providers to child psychiatrists. The program aims to help PCPs develop the skills to treat/manage mental and behavioral health needs.
Access:
Massachusetts’ Medicaid agency reported working with the state Department of Health on implementing school-based services and on conducting outreach. The Department of Health operates school-based health centers that provide comprehensive primary care and behavioral health services. The state’s Medicaid program covers these services for Medicaid eligible youth.
New Hampshire reported cross-agency work to strengthen the system of care for children with behavioral health needs, aiming to create a comprehensive, coordinated network of behavioral health services and supports for children and families.
Opioid Use Disorder (OUD)
Opioids were involved in over 79,000 deaths in 2023. The opioid epidemic’s impact remains widespread, with nearly three in ten adults (29%) reporting in a 2023 KFF poll that they or a family member experienced an opioid addiction. Medicaid is the primary source of coverage for adults with opioid use disorder (OUD), covering nearly half of all adults with OUD, over two-thirds of those receiving outpatient OUD treatment, and more than half of those receiving medication-based treatment. Public health departments have worked to reduce opioid overdoses through harm reduction strategies (e.g., naloxone distribution, fentanyl test strip distribution, syringe services) and data surveillance. The Centers for Disease Control (CDC) funds state and local health departments for drug overdose surveillance through its Overdose Data to Action (OD2A) program.
States reported new or expanded OUD initiatives in the following areas:
Data sharing. States reported engaging public health partners in strategic planning and data sharing initiatives (e.g., matching Medicaid records with OUD data) to understand state and local OUD impacts and prevent future OUD deaths.
Access. States reported initiatives focused on addressing opioid use disorder among pregnant and parenting populations. These initiatives have been captured and discussed under the “Maternal & Child Health” domain above.
Box 3: State Examples of Opioid Use Disorder Initiatives
Data Sharing:
Arizona reported data sharing with the public health agency’s drug overdose fatality review committee that works across state agencies to determine how system changes may help prevent overdose deaths.
DC reported matching and sharing Medicaid records with OUD death data to engage public health partners in strategic planning.
Lead Screening
Exposure to lead can seriously harm a child’s health, including damage to the brain and nervous system, which may lead to slow growth and development, learning and behavior problems, and hearing and speech problems. The federal government has estimated that more than half of children with elevated blood lead levels are eligible for Medicaid. Federal law requires that all children enrolled in Medicaid receive blood lead screening tests at age 12 months and 24 months. In addition, children between 36 and 72 months with no record of a previous blood lead screening test must receive one. While Medicaid cannot be used to abate or for remediation of environmental damage, states are required to provide medically necessary diagnostic and treatment services for children identified with elevated blood lead levels. Medicaid programs can leverage public health expertise in outreach, education, surveillance, and data analysis, strengthening identification of populations at risk of lead exposure and expanding the reach and effectiveness of Medicaid services.
States reported new or expanded lead screening initiatives in the following areas:
Data sharing. States described maintaining data-sharing agreements with public health agencies to monitor lead screening rates, close care gaps, and better coordinate interventions.
Other. States reported working with public health agencies to develop lead screening guidance for providers and/or managed care plans.
Box 4: State Examples of Lead Screening Initiatives
Data Sharing:
Maine‘s Medicaid and public health agencies share blood lead level testing data and coordinate technical assistance and communications to PCPs to increase blood lead testing rates. The Medicaid agency incorporated blood lead testing into an alternative payment model for primary care services (called Primary Care Plus) that emphasizes primary care quality and incentivizes providers to improve testing, screenings, and immunizations, including blood lead testing for children enrolled in Medicaid.
Other:
Arizona reported that its Medicaid agency works closely with the state Department of Health’s elevated blood lead level program to increase screening rates, identify children with elevated blood lead levels, and provide information to managed care plans for follow-up testing and treatment.
DC reported its Healthy Homes Program and Childhood Lead Poisoning Prevention Program moved from its Department of Energy & Environment to the DC Department of Health, streamlining efforts in risk mitigation from lead poisoning, asthma, and pest infestation, providing comprehensive home assessments and case management in one place, ensuring a closer link between environmental housing factors and direct public health intervention.
Wisconsin reported that public health staff are routinely included in Medicaid agency meetings with managed care plans to help identify potential quality improvement activities, including activities related to lead screening and environmental intervention.
Infectious Disease
Infectious diseases threaten public health, causing morbidity, mortality, and economic disruption. Recent outbreaks of vaccine-preventable and emerging diseases highlight the need for coordinated prevention, surveillance, and response efforts. States are required to provide comprehensive preventive care to children through the EPSDT benefit. States are required by (federal) law to cover certain preventive services for adults eligible under the ACA’s Medicaid expansion. Medicaid plays a key role in disease prevention by facilitating access to vaccines for children, adolescents, and adults. CMS and the Centers for Disease Control and Prevention (CDC) jointly run the Vaccines for Children program, which provides vaccines to Medicaid and CHIP-enrolled youth. State and local public health agencies lead disease surveillance, outbreak response, and vaccine administration. They provide guidance, education, and outreach to high-risk populations, coordinating with Medicaid to ensure prevention efforts reach eligible individuals
States reported new or expanded infectious disease initiatives in the following areas:
Data sharing. States reported collaborating with state public health agencies on disease-specific efforts (e.g., sharing and analyzing HIV data to guide outbreak response and enhance access to care) as well as broader data sharing initiatives with public health agencies to improve coordination and population health monitoring.
Workforce. States reported collaborative initiatives, including training and service coordination, to strengthen the local response capacity of public health teams and clinical providers.
Access. States highlighted cross-agency efforts aimed at maintaining vaccine access and aligning coverage policy with public health recommendations.
Box 5: State Examples of Infectious Disease Initiatives
Data Sharing:
DC’s Medicaid agency shared data with DC Health to support continuity of care for individuals with HIV following implementation of Medicaid eligibility policy changes effective January 1, 2026 that resulted in coverage changes for certain adults.
The North Carolina Division of Public Health’s Immunization Registry is collaborating with the state’s Health Information Exchange (HealthConnex) to draw patient immunization data into the registry. This integration allows providers to access a consolidated record of immunizations administered across the state, regardless of where the vaccines were given.
Workforce:
Maine’s Medicaid agency reported working closely with the Public Health agency on HIV outbreak response to coordinate services and training for local response teams and providers.
Workforce
Health care provider shortages can reduce access to care and lead to poor health outcomes. Provider shortages are a particular challenge in low-income and rural communities. Community health workers (CHWs), doulas, and other community-linked providers, often play a role in bridging gaps in care, connecting individuals to services, and addressing health related social needs. Medicaid provides coverage for eligible enrollees by reimbursing providers directly for services or paying managed care plans to deliver services. Public health agencies provide significant safety net clinical care, operating at the state and local level and often bridging gaps in care for underserved populations, including the uninsured.
States reported new or expanded workforce initiatives in the following areas:
Rural. States reported collaboration on workforce initiatives spurred by the introduction of the Rural Health Transformation Program, introduced by the 2025 reconciliation law. This program (also referred to as the “Rural Health Fund”) provides $50 billion in funding for state grants that can be used to support rural areas in a variety of ways, including to pay for health care services, expand the rural health workforce, promote care interventions, and provide technical assistance with system transformation. However, over time reductions in funding to Medicaid (due to reconciliation law) are likely to exceed funding from the Rural Health Fund.
Other.
Provider certification or initiatives to attract and retain providers. States reported working with public health agencies on initiatives to attract and retain (e.g., through loan repayment, training, and certification programs) providers and on provider certification initiatives.
Multi-agency committees. States reported participating in multi-agency workforce committees that include public health agency staff.
Box 6: State Examples of Workforce Initiatives
Rural:
Illinois specifically mentioned cross-agency collaboration at the Rural Health Fund application stage, while other states (including New Hampshire and Wyoming) described future and anticipated collaboration on workforce recruitment funded by the Rural Health Fund.
Other:
Indiana mentioned its state Health Workforce Council which brings together state agencies (including the Department of Health and Medicaid agency), legislators, health care experts, and industry leaders to coordinate health workforce-related policies, programs, and initiatives.
Massachusetts’ Medicaid agency reported partnering with the state Department of Public Health on the implementation and monitoring of the HRSA-funded Massachusetts Loan Repayment Program for health care professionals.
Nevada’s Medicaid agency reported continued collaboration with the state’s Division of Public and Behavioral Health to support the development of training and certification for enrolled Medicaid providers delivering behavioral health services.
The findings from this brief are drawn from the 25th annual budget survey of Medicaid officials conducted by KFF and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors (NAMD). Cory Caldwell is a Senior Policy Analyst at NAMD.
Appendix
Endnotes
Florida, Kansas, and Mississippi did not respond to the 2025 survey. ↩︎
Fifteen states have been selected to participate and are eligible to receive up to $17 million in funding to support implementation and technical assistance activities. ↩︎
KFF’s latest Health Tracking Poll finds that confidence in the independence of key government health agencies overseeing food and drug safety and public health is low among the public and across partisans. Most of the public also share a distrust of agriculture, food, and pharmaceutical companies to act in the public’s best interest, compared with doctors and health care providers who are much more trusted among the public.
Featured
KFF Poll Finds Low Levels of Confidence in Federal Health Agencies to Act Independently, Along with Low Trust in Food, Agriculture, and Pharmaceutical Industries to Act in the Public’s Interest
KFF’s latest April Health Tracking Poll finds that fewer than half the public express confidence in the independence of the CDC, FDA, or EPA – government agencies that hold key responsibilities over food and drug safety and public health. Overall, four in ten or fewer adults say they have “a lot” or “some” confidence in the U.S. Centers for Disease Control and Prevention (CDC) (40%), the U.S. Food and Drug Administration (FDA) (36%), or the U.S. Environmental Protection Agency (EPA) (36%) to act independently without interference from outside interests.
While Democrats are somewhat more likely than Republicans or independents to express confidence in the CDC (47% vs. 37% and 38%, respectively), four in ten or fewer across partisanship say they are confident in the FDA or EPA to act independently.
Coupled with concerns about the independence of government agencies, most of the public lacks trust in agriculture, food, and pharmaceutical companies to act in the public’s best interest. One in four or fewer adults say they trust food and beverage companies (25%) or pharmaceutical companies (21%) “a great deal” or “a fair amount” to act in the public’s best interest, while a somewhat larger share (40%) trust agriculture companies. These findings hold across partisanship, with fewer than half of Democrats, independents, and Republicans expressing trust in these industries to act in the public’s interest.
On the other hand, most of the public say they trust doctors and health care providers to act in the public’s best interest– a sentiment that is shared across partisanship. These findings are in line with past KFF polling showing that doctors and health care providers are consistently the public’s most trusted source of health information.
What We’re Watching
Differences in News Consumption Correlate with Trust in MMR Vaccine
A peer-reviewed study published in Vaccine found that among study participants, the type of media people consumed was associated with their attitudes toward the MMR vaccine, even after accounting for political identity and other demographic factors. Researchers assigned 22 media outlets to five categories, using data on media usage from Pew Research Center and AllSides Media, and selected one representative outlet from each category. Those who frequently engaged with “new” or primarily digital right-leaning media, like Breitbart, were about twice as likely to say that the risks of the MMR vaccine outweighed the benefits, compared to those who never did. Even infrequent engagement with such outlets was associated with elevated odds. At the same time, engagement with “legacy” right-leaning media, like Fox News, was not significantly associated with MMR vaccine hesitancy among participants.
What To Watch Out For: The information environment in which people consume news may shape vaccine attitudes, even within political identity. As health communicators work to increase vaccine confidence, understanding how differences in media consumption shape attitudes may help predict what populations are more likely to encounter and be influenced by misleading claims about vaccine safety.
Some Pregnant People Are Choosing to Deliver Without Medical Support, and Online Communities May Be Playing a Role
Online interest in "free births,” a movement that embraces delivering a baby without any medical professional present and was recently featured in the Season 2 finale of The Pitt, has trended upward over the last year, according to reporting from The New York Times. Research on women who choose free births points to a range of motivations, including previous negative or traumatic experiences with providers, concerns about unnecessary medical interventions and wanting a more natural birth, a desire for autonomy and control during birth, and cost and access barriers. These concerns are not without basis: research and polling have documented patterns of disrespectful and nonconsensual care in maternity settings, and women of color in particular face documented disparities in how they are treated and in maternal health outcomes. At the same time, a “free birth” can put both pregnant women and their infants at greater risk for adverse outcomes and death.
Misleading online narratives have entered this space, exploiting these real grievances to promote practices that can carry serious medical risks including infant deaths. Some online communities promoting free birth frequently invoke women’s autonomy and bodily sovereignty in ways that may resonate with some women given documented patterns of disrespectful maternal care. Some also promote narratives of women being empowered or “badass” by so-called free birth. But these communities and individuals promoting free birth also spread misguided approaches to manage birth emergencies that can cause women to delay seeking care and encourage unsafe practices. Even in low-risk pregnancies, up to 29% of births involve unexpected complications that can quickly escalate. According to the CDC, nearly one in 10 births in 2023 resulted in an admission to a neonatal intensive care unit. Without trained professionals present during childbirth, life-threatening emergencies like hemorrhage or shoulder dystocia cannot be quickly identified or treated.
An investigation by The Guardian, though, has documented cases in which organizations promoting free birth have characterized life-threatening emergencies as normal and actively discouraged members from seeking emergency care. Proponents sell access to “classes” and private online forums, some of which shame or prohibit participants who mention medical care. According to The Guardian’s reporting, one of the more prominent groups promoting free birth has earned more than $13 million in revenue since 2018 and charged $6,000 for a three-month Zoom course for so-called “authentic midwives.”
AI & Emerging Technology
World Health Organization Launches AI Tool Designed to Ground Responses in Evidence
The World Health Organization (WHO) has launched a beta version of a new health AI chatbot designed to help health workers, policymakers, and researchers find sexual and reproductive health information that is grounded in WHO and Human Reproduction Programme (HRP) evidence. The tool, called ChatHRP, uses retrieval-augmented generation (RAG), a technique that grounds AI responses in a curated external database rather than in broad training data, reducing the risk of inaccurate outputs and allowing users to trace answers back to specific vetted sources.
Misinformation in Sexual and Reproductive Health
A December 2025 review published in JMIR Infodemiology found that false sexual and reproductive health and rights information in digital spaces undermined informed decision-making and health-seeking behavior across multiple levels, from individuals to health systems. The review found that at the individual level, misinformation shaped beliefs and deterred seeking care; at the community level, it reinforced harmful norms and stigma; and at the policy level, it has been used as a tool to erode legal protections for reproductive rights. WHO has positioned its new AI tool as a response to this problem, saying it would steer users “away from algorithms, opinions, or misinformation.”
Why It Matters
While ChatHRP targets health workers and policymakers rather than the general public, its use of RAG to ground responses in vetted, traceable sources may offer a model for improving the reliability of the general-purpose AI tools that many consumers are already turning to for health information. About a third of U.S. adults now turn to AI for health information, according to KFF’s March 2026 Tracking Poll on Health Information and Trust, and while most users express trust in AI chatbots to provide reliable health information, only a third of adults overall say they have a “great deal” or “fair amount” of trust in these tools for health information. As more health institutions turn to AI to deliver information, how they design for accuracy and reliability will shape both the quality of information people receive and how willing people are to trust these tools.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.
The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The data shared in the Monitor is sourced through media monitoring research conducted by KFF.
Medicaid Mental Health and Substance Use: Expansion Trends and the Fiscal Pressure Ahead
Medicaid is a major source of financing for mental health and substance use disorder care. It covers nearly one-third of all adults with mental illness and nearly one-quarter of adults with substance use disorders (SUD), including many people with more intensive behavioral health needs. This includes adults with serious mental illness (SMI) and nearly half of all adults with opioid use disorder (OUD). Because Medicaid covers a large share of people with behavioral health conditions and finances a substantial share of treatment services and medications, it plays a central role in access to behavioral health care.
In recent years, many states have used Medicaid to expand the behavioral health treatment continuum and improve access to care. While increasing spending, these changes have helped address longstanding gaps in access to community-based treatment as well as higher levels of care. Benefit expansions have also helped to support state efforts to respond to the opioid epidemic and to build out the behavioral health crisiscontinuum of care. However, recent federal policy changes, including financing and coverage changes in the 2025 reconciliationlaw and a more tenuous fiscal climate for states may make those gains harder to sustain. The reconciliation law requires states to implementwork requirements (at application and renewal) for Medicaid expansion adults, which is the primary coverage pathway for people with mental health or substance use disorders. These requirements are expected to result in coverage losses, which may interrupt treatment and medication access.
Against this backdrop, this brief examines recent state trends in Medicaid behavioral health coverage and payment and state coverage of select treatment models for people with serious mental illness—a population that has historically faced significant barriers to care. The brief draws on the annual Medicaid budget surveys, conducted by KFF and Health Management Associates (HMA). The 2025 survey included additional detail about coverage of Certified Community Behavioral Health Clinics (CCBHCs) (as a provider type), Assertive Community Treatment (ACT), and Coordinated Specialty Care for First Episode Psychosis (CSC-FEP).
How do recent Medicaid trends reflect state efforts to address mental health and substance use needs?
Behavioral health services are not a specifically defined category of Medicaid benefits. Some fall under mandatory Medicaid benefit categories, such as physician services, while others fall under optional benefit categories, such as rehabilitative services. The ability to cover optional benefits and place limits on items and services results in variation acrossstates. State Medicaid benefit design is also shaped by broader fiscal conditions and federal policy changes.
State efforts to expand Medicaid behavioral health benefits reflect both state priorities and federal opportunities. Since the pandemic and intensifying opioid crisis, behavioral health has become a top priority for many state Medicaid programs. States have focused on expanding access (including in schools), integrating care, and addressing socialdeterminants of health. Federal opportunities, including the SUPPORT Act and American Rescue Plan Act (ARPA), have driven expansions in SUD treatment and crisis services. States have also taken steps to promote more coordinated and integrated care, including adding coverage for services provided under the Collaborative Care Model (CoCM) and enrolling provider types such as CCBHCs that offer a broad continuum of behavioral health services in one setting. Some of these initiatives are part of broader behavioral health state transformation efforts.
Behavioral health has been the most frequently cited category of Medicaid benefit expansion in KFF’s annual budget survey over the past decade. Annually, KFF’s Medicaid budget survey asks state Medicaid officials about recently implemented or planned benefit changes (i.e., benefit enhancements or additions and restrictions or eliminations). In every survey over the past 10 years, behavioral health services were the most frequently reported area of benefit expansions. States reported expansions across the full care continuum of behavioral health services, including institutional, residential, outpatient, home and community-based, peer supports, and crisis services. These trends show how states have used Medicaid to help address longstanding gaps in care and respond to emerging mental health and substance use needs; however future trends are less clear. For example, California’s FY 2026-27 proposed budget would make mobile crisis services optional for counties, rather than statewide and counties that continue to offer the service would have to finance the full non-federal share of costs.
States have also raised fee-for-service (FFS) provider payment rates to help strengthen access to behavioral health services. Even when states add benefits, access may still be limited by provider shortages and narrow networks. Increasing provider rates is one way states have tried to address Medicaid workforce shortages, though rate increases also often face fiscal headwinds. KFF’s Medicaid budget survey asks state Medicaid officials to report annual FFS rate changes for certain provider types. Beginning in FY 2024, KFF’s Medicaid budget survey asked states to report FFS rate changes specifically for outpatient behavioral health clinicians (e.g., psychiatrists, psychologists, clinical social workers, mental health counselors, and marriage and family therapists). More than half of states reported implementing FFS rate increases for one or more outpatient behavioral health providers in FY 2024 and about half of states in FY 2025. The two previous surveys, which asked more broadly about FFS rate increases for any behavioral health provider, found similar numbers of states planning to increase behavioral health provider rates in FYs 2022 and 2023. The size and scope of the rate increases varied, with some states targeting specific provider types or services, while others implemented broader increases. Although most Medicaid enrollees are now in managed care plans, state-set FFS rates often serve as a benchmark or floor for managed care payments in many states. The FY 2025 KFF survey suggests that behavioral health rate increases may be slowing, consistent with reimbursement rate trends for other provider types. About one quarter of states reported plans to increase outpatient behavioral provider rates in FY 2026. This slowdown may reflect the end of pandemic-era federal funds and anticipated federal funding reductions under the 2025 reconciliation law.
What does the FY 2025 KFF budget survey show about selected behavioral health provider types and treatment models?
The FY 2025 annual budget survey asked about state coverage of select optional behavioral health services and provider types: CCBHCs, which provide a broad array of coordinated services in a single setting, and two specialized treatment models for people with SMI: Assertive Community Treatment (ACT) and Coordinated Specialty Care for First Episode Psychosis (CSC-FEP).
State Medicaid recognition of Certified Community Behavioral Health Clinics (CCBHCs) as a provider type continues to grow. CCBHCs are a federally defined model of comprehensive community-based behavioral health clinics that provide or coordinate a core set of mental health and substance use services and serve patients regardless of an ability to pay. In FY 2025, KFF’s Medicaid budget survey asked state officials whether they recognized CCBHCs as a specific enrolled provider type for Medicaid reimbursement in FY 2025 or planned to add the recognition in FY 2026. Nineteen states reported recognizing CCBHCs as an enrolled provider type (Figure 1), up from nine in FY 2022, and several other states reported plans to add CCBHCs as a provider type in FY 2026. This growth has occurred alongside expanded federal support for the Section 223 CCBHC Medicaid demonstration, which gives participating states a pathway to certify CCBHCs, use prospective payments, and receive enhanced federal match rates. States may also add CCBHCs as a provider type through other pathways, including Section 1115 demonstration waivers and Medicaid state plan authority, a state option made permanent through the 2024 Consolidated Appropriations Act. Recognizing CCBHCs as a distinct Medicaid provider type can support more flexible payment approaches, certification of CCBHCs against federal defined criteria, and make CCBHC services easier to identify in claims data. However, formal recognition can require additional state administrative capacity, coordination across state agencies, and operational and budgetary changes. Some states may instead cover behavioral health services provided by CCBHCs through existing provider categories, while others may already have community mental health systems with state-defined service arrays that serve a similar function. Research suggests that CCBHCs have improved access to outpatient behavioral health care, with some evidence of reductions in acute behavioral health care use, such as emergency departments or hospitalization. More than 500 CCBHCs now operate across 46 states, DC, and Puerto Rico.
In FY 2025, two-thirds of states reported FFS coverage for Assertive Community Treatment (ACT), an evidence-based model for people with serious mental illness who need intensive support to remain stable in the community.ACT uses small, multidisciplinary teams to provide 24-hour individualized support in the community and can intensify support when symptoms worsen. It is designed for people with the most serious needs, including those whose severe symptoms and lack of illness awareness can make it difficult to stay engaged in treatment and have higher risk of repeated hospitalization and other disruptions to stable community living. Research suggests that ACT can reduce hospitalizations and improve engagement in care, especially for people with the highest needs and when services are implemented with fidelity to the ACT model. The American Psychiatric Association (APA) guidelines recommend ACT for patients with schizophrenia who have a history of poor engagement with services leading to frequent relapse or social disruption. In KFF’s FY 2025 Medicaid budget survey, 34 states including D.C. reported that ACT is covered under FFS Medicaid for adults (Figure 2). Even in states that report Medicaid coverage for ACT, workforce and infrastructure constraints may limit access. For example, only about one-quarter (27%) of mental health facilities serving people with SMI reported offering ACT services in 2023. Budget pressures may also affect the availability of these services. In Idaho, 2025 budget cuts interrupted ACT services for people who relied on ACT to stay stable in the community, and media reporting documented that some Medicaid enrollees receiving ACT services died after the disruption. Idaho later restored funding, though rebuilding these services may be difficult and costly.
Far fewer states reported FFS coverage for Coordinated Specialty Care for First Episode Psychosis (CSC-FEP), an evidence-based early intervention model for people experiencing a first episode of psychosis. KFF’s FY 2025 Medicaid budget survey asked state officials whether they provide FFS reimbursement for CSC-FEP codes in FY 2025 or plan to do so in FY 2026. Seven states reported covering this service in FY 2025 (Figure 2) and several more states reported plans to add coverage in FY 2026. CSC-FEP emerged in the late 2000s as an early intervention model designed to connect people experiencing psychosis for the first time to coordinated treatment to reduce the serious and potentially lasting effects of untreated psychosis. This model includes coordinated medication management, therapy, family support and education, and other services. Research shows that people who receive this treatment experience fewer psychotic symptoms, fewer preventable hospitalizations, and better outcomes in work, school, and quality of life. The APA guidelines recommend CSC-FEP for patients with schizophrenia experiencing a first episode of psychosis. In addition to the seven states reporting coverage for this model in FY 2025, four more states reported plans to add coverage for CSC-FEP in FY2026, and Virginia reported that coverage approved by its General Assembly will begin in FY 2027. Some states reported that these services are funded outside of Medicaid through the federal Community Mental Health Services Block Grant, which requires states to set- aside 10% of funds for evidence-based programs for people with early serious mental illness.
This work was supported in part by the Philos Foundation. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Episode 3, AI Series: When minutes matter for a patient’s care, what is AI’s role in clinical practice? Elad Walach, co-founder and CEO of Aidoc — a company with a comprehensive AI health care platform that analyzes real-time images and flags time-sensitive findings — shares his perspective on AI’s transformative power in dodging diagnostic error, improving access to care, and ensuring care quality in busy clinical settings.
Charles N. Kahn III is a senior visiting fellow at KFF. He is also a visiting senior fellow at the American Enterprise Institute and a nonresident senior scholar at the University of Southern California’s Schaeffer Center for Health Policy & Economics. He serves as co-chair of the international Future of Health collaborative.
Elad Walach is a co-founder and CEO of Aidoc. He is an expert in AI with visionary business insights in the healthcare space. Since establishing Aidoc in early 2016, Elad led the company through four investment rounds bringing the total investment to $250M, drove the commercial availability of 20 product lines, created an install base of over 1,600 global hospitals while growing the company to over 450 employees.
Transcript
AI Usage Disclosure: This transcript was created with assistance from AI tools. It was reviewed and edited by KFF Staff.
Chip Kahn: In our earlier episodes, we covered the strategic landscape for AI in health care and drew the line between what AI can do in clinical settings and what it cannot do. This conversation goes to the front line, to a firm that has put FDA-cleared clinical AI into more hospitals than anyone else. For most of modern medicine, the great leaps forward have been physical things you could see and touch. A new drug, a surgical technique, a new machine. But what we are witnessing now is something different. The new medical miracles may come not from a molecule or a device, but from digits, from patterns detected in data, from algorithms operating in an abstract, informational space that no surgeon’s hands will ever reach. That is what makes this episode both exciting and maybe a bit unsettling. You will learn that Aidoc’s platform is running right now in more than 1,600 hospitals worldwide, analyzing over 70 million patient cases a year. It holds 32 FDA clearances, the most in its category. When a patient gets a CT scan in an emergency department that runs Aidoc, the AI analyzes the images as they complete and flags time-sensitive findings. Brain hemorrhages, pulmonary emboli, aortic dissections. So, the radiologist sees the most urgent cases first, rather than in the order they arrived at the ER. When minutes matter, that patient lineup can be the difference between a good outcome or a catastrophic one. Elad Walach co-founded Aidoc in 2016, years before the current AI hype cycle. He came from national security AI where the lesson was that cutting edge algorithms mean nothing if they are not actionable. He has built the most widely deployed clinical AI platform in health care. And the question today is what that deployment has actually taught us. How will it change clinical practice? And can FDA-cleared AI change patient outcomes at scale or will obstacles presented by payment structures, workflow constraints and liability concerns limit dissemination despite the clinical validation? Elad Walach, welcome to KFF’s Business of Health with Chip Kahn.
Elad Walach: Hey Chip. Great to be here.
Chip Kahn: It’s so wonderful to have you here because you really represent what we’re trying to get at in this series, which is the ultimate application of AI. And that’s what we’re going to talk about. But before we get into, Aidoc, your company, and talking about the specifics of what you do, I’d like to give our audience some background and ask you how did you get from national security, in Israel, where you were doing AI to health care? And in a sense, what did that transition teach you as you went?
Elad Walach: I do not come from health care originally as you’ve mentioned, I led an AI division for more national security purposes in Israel. But I always had this health care bug in me. A lot of it was through my father, who’s been a huge influence on me. So, when he was younger, years ago, his sister unfortunately passed away due to diagnostic error. And I always had this influence in the back of my mind. It also influenced him. He was actually working in IBM research at the time, and he was one of the people that actually pushed IBM to go into health care, back in the day. He would tell me all the stories on what they’re working on and kind of ingrain that passion into me. When I finished my service together, my two co-founders, we all finished our service at the same time. We said that’s what we’re really passionate about — helping improve quality of care, helping mitigate errors and improve access. And we just spent a lot of time in hospitals. Basically, because we didn’t know much about health care, we spent about a year to a year and a half until we’ve started seeing these recurring problems, recurring problems of lack of access, recurring problems of amazing people who are the clinicians barely holding on in to this crazy system. And that’s why we decided to start Aidoc, really with the mission of improving access to care, improving quality of care.
Chip Kahn: Before we get into Aidoc, and I want to take you back to 2016 and the genesis but what is it about, Israel, and technology and health care that come together? I mean, I’ve spent a lot of time in Israel and done work with Sheba’s ARC, their innovation center. What is the sauce there that’s produced so much innovation?
Elad Walach: First of all, we’ve been proud to be working with Sheba’s ARC from the early days. And I think there are two things that work well in that ecosystem. First of all, we’re all very pragmatic AI people. So especially in the early days of clinical AI, people could get really excited about the model building. And especially I did a lot of work with professors in academia and they could get super excited about this new model coming out or this new paper and always trying to test stuff. But I think you kind of learn about a lot of the practical application and there is a lot more into making an impact than there is to the model-building. You would find a lot of innovation in Israel because of the fact we have to make things work. We’re becoming very practical. And that was a big aspect, by the way, of how we built Aidoc. The second aspect it is, you, know Israel is very small, and that actually has an advantage because everybody knows everybody. If you want to get a clinician together with a technology guy and a business guy in a room brainstorming ideas, it’s much more possible. It’s very easy to kind of find the right cohort.
Chip Kahn: That’s interesting. And just for the audience that, probably don’t know, Sheba Medical Center is, the largest hospital in the Middle East, 1,600 beds and just a tremendous complex and really a university unto itself, in terms of the teaching and the research that’s done there. So, let’s go back to 2016. And you, got into AI before all the hype. And what did you see that others didn’t see?
Elad Walach: I sometimes say I got into AI before it was cool, but it was always cool. So I, wouldn’t say that. But look, I think we’ve realized that there are intractable problems in health care that are going to be very hard to change, manually, basically. And we got into AI in the 2016 world. That was just the first time where deep learning came into being. So those that don’t know, machine learning before that was much less accurate. And it’s about that time when deep learning was invented. And that was the first time we could build an AI that was good enough to provide results that are clinical grade or physician accuracy. Not with the aim of replacing physicians, but finally you have to be roughly as good as them to be actually be able to support them. And that was only possible for the first time. Then there was a tradeoff, by the way, which we can talk more about, but the tradeoff was always that you can be really accurate, but you have to be very specific. You could build an algorithm, for example, to find brain bleed. That was the first one we built. It was very accurate. It could do it like 95% accuracy, but it could only do brain bleeds. If you want to do spine fractures or stroke, that’s a whole different model. And that was the world back then when we got started.
Chip Kahn: So, the focus is on imaging, and the focus is on the emergency room and this indispensable technology, the CT scan. Talk a bit about when a patient gets a CT scan and what Aidoc does.
Elad Walach: Clinical AI, the category we’re in, I think, is the category where people are thinking about health care AI, that’s what they’re imagining. So, Chip, you’ve mentioned that’s a lot of the conversations we are building up to. To be clear, I think we need to tackle the administrative burden. The backend offices describing all of those are really important problems. Clinical AI is really touching care delivery and boy, is that an area where I think health care needs the help. We’re stretched so thin. We have amazing, amazing, passionate clinicians, but the system they’re surrounded with is so overwhelmed. I just read a study today that shows that in ‘22 and ‘23, in two years, we more than doubled the wait times for outpatient imaging diagnosis in two years. The shortage of physicians is becoming so profound. It’s literally impacting access and quality of care. Another study that’s really influenced me is a study by a group at [Johns] Hopkins with David Newman-Toker who did a study about the impact of diagnostic errors in the U.S. and every person probably listening to this will suffer diagnostic harm due to diagnostic error in their lifetime. And the group estimated we have, every year in the U.S., 400,000 deaths due to delays and diagnostic errors. That is such a big number, it’s hard to wrap our heads around. And that is where I don’t think there are any manual things we can do to solve this problem. We threw labor at the problem for years and we’ve made some impact. But the problem keeps growing and growing and growing. The only way out in my mind is technology. And what we need to build as a society is this ubiquitous layer that analyzes every diagnostic encounter and provides this kind of second set of eyes that would help both the patient get accurate and timely diagnosis, the physician do their work efficiently. To imagine what Aidoc does today, we do exactly that for imaging, either as an ED patient or as an outpatient. You go to a facility that has Aidoc, you would get kind of this clinical AI platform, also analyze your data, and then identify certain types of findings. So, let’s say you’re in an ED with an abdominal pain, and today you’re going to get a scan and you’re going to go on a list with, maybe, 100 other patients and you’re going to be waiting for your diagnosis. With Aidoc, basically, the AI look at your scan and find whatever diseases are there. Let’s say it would now scan you for 15 different diseases and we’d say, oh, you likely have appendicitis, or you could have maybe a liver lesion, and it would then prioritize you for a radiologist read almost immediately. Or a pulmonary embolism is an example. So instead of waiting tens of minutes or an hour, you could get the results almost instantly and then get your next step of care. So that’s an example today of how patients get an impact through this technology.
Chip Kahn: So, to get this into the hospitals in the United States and get it disseminated…was it used in Israel before it came here?
Elad Walach: Actually, in tandem with Israel and the United States…
Chip Kahn: The first sort of regulatory hurdle is FDA. You’re in 1,600 hospitals. I want to talk about that in a moment, but let’s start with the regulation part of it. How do you deal with FDA with this kind of technology? How receptive was the regulator to this really disruptive technology that changes things completely?
Elad Walach: When we first started this, I was imagining FDA as this, you know, bureaucratic wall, that is more process than anything else. But through the years, I’ve actually learned it’s people, and it’s actually really passionate people about changing health care. The interaction is not like you’re submitting this and then you forget about it. You actually have continuous interactions with the agency. We’ve submitted more than 30 submissions to the FDA, so we’ve seen that often through the years. And they’re very passionate. And I actually believe they’re providing a critical service to the adoption of clinical AI. The way FDA reacts to it, they’re saying, we understand this is going to be one of the most transformative changes in care delivery we’ve had in decades. But on the flip side, we see a responsibility to both keep patients safe and create a layer of trust. Trust is going to be a determining factor in what gets adopted, what’s not going to get adopted, and, also, what’s getting used and what’s not getting used. It’s how do I know that you work in a safe manner? And I think FDA is actually serving a really critical function in that way. And what they do is they basically ask us, look, tell us what you think your device does, what is your claim, and then let’s validate that. The issue is that our claims keep changing as the technology evolves. But, they’re with us on the journey to keep evolving how we test these. I would say our testing methods really changed over the years as the technology expanded in capabilities.
Chip Kahn: So, in terms of first adoption, you’ve got health systems and you’ve got physicians, you’ve got radiologists and emergency room doctors, who are going to be either aides or obstacles here. And you’re at 1,600 hospitals worldwide right now, which is a phenomenal number. But I assume getting that first one or two here in the United States was a real hurdle to talk them into testing this. And then you had to go through a process. Can you talk about that process? I know with others I’ve talked to who brought startups in the United States from Israel, the biggest issue is how do we show what we can do and get a place to demo this.
Elad Walach: It all comes back to two things that were critical. First of all, it’s the topic of trust and safety and quality. Hospitals and health systems are very concerned on partnerships, both for patient care reasons, for cyber reasons. You have to show them. Even when we were a way smaller startup, right, we had to show them that we’re going to handle this relationship with the utmost care and that breeds trust. And I think that’s going to be really key for adoption. The second thing is they were really compelled by the vision of what we offered, especially in the early days, by the way. I believe in AI. It still is true today. You don’t partner on product, you partner on vision and roadmap and belief in execution. I think AI is in such rapid innovation right now that if you’re actually just evaluating a product, you’re valuing the wrong thing. Because a year from now, the product is going to be different and the value you’re going to get is going to be different. And you always have to think not just what the product that I want can do, but who am I going to bed with because that is going to matter a lot more than anything else.
Chip Kahn: Well, that actually maybe is a good opening to talk aboutWellSpan expanding from radiology AI to 21 care pathways, across nine hospitals. What convinced them?
Elad Walach: With WellSpan specifically, we started with six products. And each product, when I say product, I mean a different disease. So, think about, I mentioned the example of an abdominal pain or a brain bleed. Each one of them was a different disease. During the early phase of the partnership, it was all about obsessing about showing value. And that is a really, really important lesson learned. A lot of people in AI world are focusing on the model or focusing on the product. Both are awesome. But what people really care about in health care is outcomes. So, the real question is, what are the outcomes we can achieve? And for them, the things that they really cared about was time to diagnosis. In their backlog was efficiency. They want to make, you know, to make the reading more productive. They want to ensure their care is coordinated better. And within about 12 months, we were able to show massive improvement across all of these metrics enough that they said, look, we want to go big. On their end, they realize that AI is going to be one of the most important aspects of their strategy to moving forward. I think we all probably believe that AI is going to be a transformational technology, but the implication of that is that we have to change how we operate to absorb it and adopt it in a much more rapid fashion. They’ve basically said, look, we understand we want to build the future, and we don’t just want the future be built on top of us. And that kind of bold leadership is what allowed them to say, hey, we’re going to look at the outcome we’ve generated and then we’re going to go big and we’re not going to do this one at a time. We want in a year’s time to get from the six use cases to over 20 use cases. Once they made a choice, because they had an amazing team, they were able to get there not in a year, but actually in three months from the day we’ve signed. They were like, okay, we’re going to go from 6 to 20 and basically, we’re able to quadruple all the outcomes they’ve seen before, which is only possible, I think, with bold leadership and strong change management practices that their team has.
Chip Kahn: Just because the audience may not be aware, can you sort of talk about where they are geographically and what the spread was geographically of the operation? You just described this dissemination.
Elad Walach: I think that the geographical dissemination was less important because it was always around their whole footprint. The big deal was growing across service lines. So how health care health systems work is typically you have one service line, let’s say radiology, or one service line, cardiology. And the way health care AI can be adopted, there are two different approaches. There is the approach of letting a thousand flowers bloom and there is the approach of let’s develop an enterprise strategy. The thousand flowers bloom, meaning I’m going to let every clinician, every service line, pick their own flavor of the day, and they’re going to build their own point solutions. And these point solutions are really valuable. I don’t want to use “point solution”—is not a bad term. There are incredible point solutions out in the world, but that is one worldview: I want to let everybody do their own thing. I personally have not seen that scale in health care. The reason why it’s not scaling is because change is too complicated for health systems, there’s too many dependencies, and we’re lacking a lot of the platform and governance infrastructure to actually scale these one-by-one use cases. The other approach is saying we’re going to determine as an enterprise what is our approach. And yes, it may be less democratic, and yes, it may be less consensus driven, but what we’re going to get in return is velocity. We will get to dozens, if not hundreds of use cases in a very rapid clip because we’re creating the guardrails for that adoption that I think was the key for the WellSpan growth. It’s not just the geography, it’s more about the fact that they said we’re not going to let every service line or every clinician have a go at their point solution. We’re going to define enterprise guardrails, but with that look at the outcomes. Dozens of use cases running in production in less than six months. It’s pretty remarkable. I mean, if you try and do this in a one-by-one fashion, it’s almost impossible.
Chip Kahn: It’s interesting you describe it like you do because one of the things that was really stressed by Eric Larsen, our first guest on AI, was this notion of at the end of the day it’s going to be top down, in terms of getting the kind of dissemination that’s going to work. This is difficult, this process for the frontline physicians, radiologists, the ER docs, the other docs. And there’s this thing called “alert fatigue” that comes in decision support. And this is really a type of decision support. How do you deal with that? What is it? And how do you make sure it doesn’t undermine all of the advantages you have from the very specific accurate readings that, in a sense, your machine is doing?
Elad Walach: You’re asking a really good question about both alert fatigue and I’ll connect it to the topic of safety and quality. And both are really, really difficult. People are trying to understand, well, why, why wouldn’t we just use ChatGPT, you know, or Claude, and just let it run on all of our scans to identify signals. And you’re right. I think people treat accuracy as a solved problem, the model is going to be good enough. And I will tell you it is not good enough. It is actually the determining factor of what gets adopted versus what’s not getting adopted. Because accuracy means both safety and quality. You’re not missing critical things. But also, it’s the opposite of alert fatigue. I think we’re all sensing it. Also, why are agents not proliferated in every aspect of our life yet? Because agents are proactive. They analyze every piece of data to trigger an action that is a very, very difficult thing because the accuracy requirements when you analyze every piece of data are way higher. So, accuracy is going to be a really, really important factor in all of this. And in my mind, to create accuracy you have to do two things really well. First of all, on the model side, you have to build really, really good models. And we tried to use a lot of different tier models to help speed our work. It was not very productive. In fact, a few years ago we made the very tough decision;I still remember my hand shaking the day I had to present it to the board. We’ve decided to build our own foundation model. Basically, a model that is like a ChatGPT that can take a scan in this instance and not just find one disease like we spoke about before, but actually every disease, altogether. I remember the day the team had the first breakthrough and the team told me, Elad, the model is working. It can find every disease in like 95% accuracy, which was the accuracy of our old production grade models that have been analyzing tens of millions of patients a year. I was like, that’s great. But then my team told me I was like the overly optimistic CEO. My team told me, Elad, you’re not getting it. 95% is no longer good enough when you’re running on 100 diseases all at once because you’re going to have compounded errors. So, the 5%, to give a simple math, if I have a 5% false positive on a scan and I’m running 20 models, I know I’m oversimplifying the math here. It’s roughly going to be false positive, every scan you’re going to like, we’re going to false alarm the hell out of the physicians. Basically we then realized we have to get our models from 95 to 99.5 to become production rate. People don’t understand the difficulty of getting that extra ounce of accuracy. But effectively the model we built and recently got FDA cleared could get up to 99.7% on the specificity. And that was really the key determining factor. So that was the one aspect of everything you’ve mentioned. There is another aspect to it, which is unrelated to the model at all, and that’s thinking about the governments and the monitoring. Data drift is very, very real. It is not an imaginary ghost. On average, we as the market leader, we have the most volume of clinical AI. Even for us, accuracy drifts about 10% every 18 months, we don’t track it 10% in the accuracies I spoke about is the day and night difference between usable and unusable. So you have to build a governance and monitoring infrastructure to track performance drift, to track data drift, and then fix it somehow. Both of these components, the governance, and the monitoring, as well as the model, are key to get this higher accuracy level, which I agree with you, is the only difference between what you can and can’t use in the real world.
Chip Kahn: I want to get a deeper dive into some specific examples, but before that, let’s define, when you say data drift, what’s causing that? Because you’ve got a tremendous amount of records that are feeding all the information you have, and you’ve got all these scans, why a drift?
Elad Walach: I love that question. And it’s very counterintuitive when you’re kind of outside in. I’ll give a simple example. How do you know that a scan, let’s say, is a head scan and contains or doesn’t contain contrast? I would imagine it’s somewhere there in the metadata. It’s written somewhere, somebody knows. Nobody knows. It is all manual. You know, it’s manual all the way down. You need to have a person typically saying, this is a head CT and this is without contrast. And typically you need a human in the loop to determine that. So that is the problem called model orchestration. You need somebody to say, this model, this AI, is relevant to this piece of data. And in theory, if you don’t have another solution, it will be a very manual process. And these protocols keep changing. For example, I added a new stroke protocol, or I had a new type of machine, or I changed this type of workflow, or I acquired a health system, or I had another scanner in the ED. Each one of those changes my data. And because the data is unstructured by nature, that’s what causes the data drift. And you add one plus one plus one, and effectively what you’re getting is a whole complete new data set after two to three years. That is some of the problem we have in health care. When you think about even units of medication, types of medication, types of procedures, all of it changes all the time. So that is why another layer is necessary to both mitigate and then monitor all of that drift.
Chip Kahn: In terms of this drift, is the machine smart enough to constantly calibrate, or does it take human eyes to make sure that calibration is there?
Elad Walach: Yeah, that’s a beautiful question. And the answer is both. On the one hand, the machine can do some of it. If you train the model orchestrator good enough, it can fix some of this. But at the end of the day there are a lot of these that are unknown. You don’t know what’s going to change. And it’s very hard to train an algorithm that can face the unknown. You almost always have to have some sort of human in the loop to monitor at least the high-level components of the data. And I think it’s here to stay. I think it’s a new profession. I remember when the first ChatGPT paper came out, they thanked all their team members and one of the roles was they thanked their AI babysitters. And I found that so interesting that we have this new generation of professions of people whose expertise is to really manage these new models and agents and workflows. And it’s necessary. I actually think you have to have a human in the back end holding up the AI to some extent.
Chip Kahn: And this isn’t just a health care issue. This would be in every data-based process you’re going to have the same thing happening as you get new data expansion and the feedback loop is going to be somewhat distorted, it sounds like, and you’re going to have to constantly keep calibrated.
Elad Walach: I agree, it’s not just a health care issue. I think it’s slightly worse in health care because of the pace of change combined with the needed accuracy. Again, we’re all going back to accuracy, that it’s not a solved problem. Because safety and quality are so paramount. We have to be much more hawkish on ensuring consistent accuracy and performance.
Chip Kahn: So, let’s take a deeper dive. Patient comes in, Aidoc flags a brain hemorrhage 30 minutes earlier. Where’s the value versus what would happen without Aidoc?
Elad Walach: There are multiple areas of value. One area is that you mentioned the emergency department that is truly time to diagnosis, time to treatment. A friend of mine called me to tell me a true story right now. They went into a Mayo institution, and they got pulmonary embolism results in minutes from coming in. So, they came in, they were scanned for something oncological related, and within minutes they got, hey, you have a pulmonary embolism. We need to treat you for that. Because of the increasing backlogs we have, the likelihood of a pulmonary embolism being identified within minutes is very low if you’re not using AI because the backlogs in the ED are increasing by a lot. The other area of value is proactive care, or precision medicine. And I’ll give the example from Mercy, which is a fantastic hospital in St. Louis, what they said is there is a test called calcium scoring. It’s one of the best predictors we have for heart disease. You know, you pay whatever, a hundred bucks, you do a dedicated study. Well, guess what? Most people are not going to take the time of day and pay 100 bucks and get their calcium score. Especially as you go to rural America, right, or more community-based care. The opportunity we have is immense. Today AI can look at the scan and say, hey, we have suspicion, you actually have calcium score. We should take a look at that and we actually can marry that with your clinical record to find the short list of patients that have heart disease risk and are currently unmanaged. The example of Mercy in St. Louis, they’ve decided to be proactive for their patients. And they found that about 6% of all patients doing a chest CT for whatever reason—think about you broke a rib or whatever—have this unmanaged intermediate to high-risk calcium score and are now reaching out to those patients to help them get care. So, think about this, us also moving with AI, the health system from reactive—I’m just doing what I’m told—to proactive. We’ve got your back because we have all this data. These are some examples of how clinical AI can be used to really change the care paradigm.
Chip Kahn: I understand that one of your customers flagged 10,000 incidental findings in a year and these are conditions that nobody was looking for. What does it mean to sort of treat the whole patient through imaging here, and what are the positives and negatives of that? Because in a sense you’ve got, you know, finding disease. On the other hand, you have issues of liability and payment, and it gets complicated because of the way our system works.
Elad Walach: It does get complicated. I will tell you, I’ve met a lot of health system executives, and I think they all share the passion for improving care. They’re generally doing this for the right reasons, which is amazing because I get all these warnings at the beginning. It’s all cynical. It really isn’t, like people want to do the right thing for their patients, but obviously we have to be realistic and build sustainable models. In my mind, the key is not just creating problem with “lets us find all these solutions,” but actually help with the management and the workflow of these patients. And I think for that, that’s where you really need to have an end-to-end understanding of the situation. Notice the example of calcium scoring I gave you. I could have ended with the image. I could have said we’re just scanning the patient, looking at the image for suspicion, but I actually added another component. We’re looking at the charts, we’re looking to understand are they managed, what is the clinical history. And then you actually can shortlist the patients that require that follow up care. And that I think is the key. Don’t stop in just the detection in an already overwhelmed system. Help with risk certification to make sure that the patients that we’re finding are those that you actually want to treat.
Chip Kahn: Let’s talk a bit. And we’re sort of heading in that direction about the business model. I mean, there’s no reimbursement, necessarily, for this extra service. There’s the cost that’s paid, I mean the charge, that’s paid for the scan. So, who’s paying for this? I mean at the margin. Is this costing more money? And then, you know, where does the money come from? And obviously you need to be paid.
Elad Walach: You have to find sustainable ways to create innovation. Right? I think the people that I know in health care are doing this because they want to help improve care. But we all live in an environment where, you know, building this foundation model I described earlier costs $300 million at least. You know, you’re not going to get $300 million for just doing good, right? So, you have to figure out a sustainable way. And you’re right, there is no reimbursement. The way these models work, you have to find an ROI that is directly good for the health system in a financially sustainable way. And typically, the way these work is you have to show, and obviously it highly varies per the AI solution and disease, but you have to show either you’re improving efficiency, maybe reducing time to diagnosis. So, improve efficiency, that influences things like ED length of stay or driving more revenue because you’re able to create more valuable patient encounters. But whatever which way you’re looking at this, you have to find a way to show that every dollar you’re spending on improving quality of care through clinical AI is also good for them, by improving their operations. Otherwise, it’s just not sustainable. And they’ll just do like maybe a few, but they can’t really sustain that.
Chip Kahn: And then also, I guess the other factor is that you’ve got the EHRs, you’ve got Epic, that dominates, but you also have Oracle and Meditech and a few others. How do you integrate with them? And then in looking into the future, how do you sort of stay parallel and maintain your business model when in a sense you could argue that something like this should just be part of the EHR, the electronic health record in the first place.
Elad Walach: I’ll actually start with the second question. You know you’re asking really, you know, really bold and tough questions, which is great. I think that’s what makes it interesting.
Chip Kahn: That’s why they pay you the big bucks.
Elad Walach: Yeah, exactly. I think so. Let me start with the second question. I actually think those are two somewhat distinct categories like diagnostic FDA-cleared complex signal AI. FDA actually has a different category for what they call complex signal analysis. Like an image versus what they call clinical decision support, more text based. And in my mind the line draws on the topic of commoditization, what is like very hard to do. And we talked about accuracy, we talked about workflow integration. There are all sorts of these aspects that require this distinct category. And we’re seeing that trend of differentiation between what I would categorize, AI enabled system of records to an AI specific category. If you look at the broader software market, the interesting thing I find is that you find a lot of the AI natives are actually gaining a lot of share for AI-specific non-commoditized use cases while the AI enabled system records are also monetizing AI, but for very different use cases. And again, we’re seeing that play out in the broader software market as a whole. I’m not going to get into an argument who’s going to win in the long run in the broader software market but I think in here it actually is parallel. Those are two different spaces where we’re talking about the uncommodified, incredibly complex diagnostic AI versus doing some of the things that are more native to the workflow kind of semi-tech solved problem that are still very difficult. I’m not going to reduce the magnitude of them, and I do think they’re going to maintain parallel. Should they be integrated? Absolutely. I think workflow is key. Anybody who ever touched health care applications will tell you the same thing. And luckily, I actually think that all the vendors, if it’s Oracle or Epic or Meditech, I think they’re actually all opening up. We found them incredibly collaborative in a way to integrate back into the workflow. I would say the key would be not to take people out of the workflow but actually feed more information in. But I think it’s actually very possible today.
Chip Kahn: Well, it sounds like from your description that there has to be in proper use of Aidoc integration with the EHR so that you’ve got that data that sets a context for the image, reading, right?
Elad Walach: Yes, but even more than that, I think that it’s, A, it’s a patient context, but B, it’s about being easy to use and being automatic. The more you’re going to ask people to go outside of their norm, the harder adoption is going to be. So, you have to find ways to not overwhelm your users. If the whole point is to increase efficiency, you cannot ask them to click a button, go to a different system, click three more buttons, go back into the system, copy paste. I just think it’s going to be way harder to drive adoption this way. So, I think the integration into the EHR is going to be key, yes, for patient context, which as mentioned, multimodal is going to be key, but also to be embedded in the way they work.
Chip Kahn: And so where is the physician, particularly the radiologist here? Who’s had the role historically, traditionally of reading the image? I mean, prior to this technology, you know, you had to wait til the radiologist read the image, right? So, you’re coming in on top. What’s the response of the profession and what are the implications for the future of that profession and the other maybe other, specialties also?
Elad Walach: So, let me state very plainly. I don’t believe in the “we’re going to replace radiologist” paradigm. I also don’t believe in the paradigm of bypassing. I do believe it will enable better collaboration between the specialties. Because imagine an ED physician that now has these AI flag that alerts both them and the radiologist for the existence of a patient. Maybe for normal findings, they can speed through the ED. I do believe we’re going to see more of these workflows. Generally, I think we have to be extremely careful in how we think about workflow in the context of safety and quality. I know I’m like banging that drum time and time again, but what we don’t want to do is to move too fast and then have this blow up in our faces and actually, taking a decade back, I think there are ways to progress. There are collaborative and are not going to be overly disruptive to any specialty, but actually shifting over time more tasks between the different specialties. I do believe we want to do something like that to allow everybody, basically, to diagnose—radiologist or not—top of their license. And I do think saying that means we will shift over time some tasks but called the bottom of the license work out of that. But I think we need to do it safely, carefully, and it’s going to take us time to think through all the governance, through all the guardrails and how do we do it in a way that really preserves the quality of care.
Chip Kahn: So, to sort of see what comes next. I think your January 2026 clearance points towards an AI managing whole clinical workflows. And you’re beginning to hit on that. Where is that headed?
Elad Walach: I mentioned foundation models before. I think it’s the most transformative technology for care delivery, honestly, that we’ve seen. So, what are foundation models? I’ll say it briefly. It’s basically as mentioned, instead of finding one disease at a time, it’s a model think about like a ChatGPT where you can upload a scan and find every disease all at once. And also, as mentioned, with way higher accuracy than 99.5. It’s quite incredible. It’s expensive to build, but once you build it, it’s incredibly powerful. Today, an average health system using clinical AI with a platform would adopt 12 use cases, 12 different diseases. I think we’re a year and a half away with foundation models that we can cover every disease on an image, at least in CT and X-ray. My belief that a health system will be running over 100 clinical AI or disease detectors, at least an average system. We’re not that far away from this. I know it sounds crazy right now, but that’s the nature of exponential growth. Things like we can’t imagine are growing very, very rapidly. What I’m imagining in the future is that clinical AI will be as ubiquitous as driving with a seat belt. Right? You can’t think of going into a car and not putting your seatbelt on. I think similarly we should imagine a world that no diagnostic encounter doesn’t have this AI layer supporting it. And with foundation models, I actually don’t think we’re that far away. It has been that transformative and as you mentioned, it’s very new. We’ve got, to the best of my knowledge, world’s first clearance for a foundation model-based application. This was like a couple months ago, so, it’s all very new, it’s all very rapidly evolving, but the exponent is coming and I think it will have an immense impact on care.
Chip Kahn: I mean, that sounds transformational, not just a game changer. And maybe we’ll close out with this question. What should a patient know about AI’s role in their care that they certainly don’t know today, I mean, clearly, what you just described is something I think the average patient couldn’t. I can’t visualize even, what should they know?
Elad Walach: So today, AI has been serving a very backend role, and to some extent, justifiably so. The heroes in this equation are the clinicians, and the AI is just augmenting them. And I still believe that is going to be true. However, I do think as AI Is becoming more proliferated, and now we’re at the pace of over 70 million scans a year, so it’s becoming quite proliferated, it will become the standard. And as you want to know that your health system is using the best tools out there, I think patients should be aware of, at least, what are the systems doing to ensure they’re using the best tools out there. And I do think patients should be aware of that. I’ll give an example. If you’re a patient going into an outpatient imaging center that has clinical or imaging AI, it would scan you for acute findings, even if you’re not being suspected for that. If you are a cancer patient, you have increased risk of pulmonary embolism. Today, because of the backlogs, we have some institutions, not everywhere, but some, where you would be waiting a week to get your diagnosis. Now, imagine you’re one of the two of those 2 to 4% that has an acute finding. And now imagine the world where you’re waiting a week to get this result. Maybe pick up the phone, maybe not, versus getting picked up by the head immediately to go to the ED. That is not science fiction. That is an existing capability today and I think we should all start becoming more and more aware of that.
Chip Kahn: Elad, thank you so much. This has just been so informative, and, I think I used the word unsettling at the beginning, to characterize it. But I don’t think it’s unsettling. I think it really is exciting. We all should look for a better future, I think, from what you’re doing.
This weekly podcast features insightful conversations between host Chip Kahn and his guests, who discuss the business of health care, connecting the dots between the health care business, policy, and patients.
The podcast’s first series on AI in health care illuminates how AI is changing health care, and features guests who are deploying this technology, managing its consequences, and designing policy around it.