State Policies Connecting Justice-Involved Populations to Medicaid Coverage and Care
Introduction
The COVID-19 pandemic has magnified pre-existing health disparities for justice-involved populations, with coronavirus infection rates among incarcerated populations higher than overall infection rates in nearly all states. Justice-involved individuals are disproportionately low-income and often have complex and/or chronic conditions, including behavioral health needs. Although the statutory inmate exclusion policy prohibits Medicaid from covering services provided during incarceration (except for inpatient services), states may take other steps to leverage Medicaid to improve continuity of care for justice-involved individuals.
In states that have adopted Medicaid expansion under the Affordable Care Act (ACA), many justice-involved individuals could be eligible for Medicaid coverage. One analysis of inmates incarcerated between 2009 and 2013 found that in the first full year after release from incarceration, only 55% of individuals had any reported earnings and among those with jobs, median earnings were only $10,090. In the 39 states (including DC) that have adopted Medicaid expansion under the Affordable Care Act, nearly all adults with incomes up to 138% of the federal poverty level (FPL) ($17,774 for an individual in 2021) are eligible for Medicaid; however, eligibility for adults remains very limited in the remaining 12 states.
The 2018 SUPPORT Act included provisions to promote continuity of care for justice-involved individuals, including prohibiting states from terminating Medicaid eligibility for incarcerated individuals under age 21 or former foster care youth up to age 26 and requiring eligibility redeterminations prior to release. The Biden Administration has also identified investments in justice-involved populations as a key Medicaid priority. Both the version of the proposed Build Back Better Act (BBBA) passed by the House of Representatives on November 19, 2021 and the version revised by the Senate Finance Committee on December 11, 2021 would partially lift the inmate exclusion policy by allowing federal Medicaid money to be used to pay for Medicaid-covered services 30 days prior to release for people who are incarcerated. This provision would be effective on the first day of the first fiscal year calendar quarter that begins two years after date of enactment (as soon as January 1, 2024). The BBBA would also temporarily close the coverage gap for individuals with incomes below poverty living in states that have not adopted Medicaid expansion by allowing these individuals to purchase federally subsidized coverage on the ACA Marketplace through 2025. This provision would impact coverage options for justice-involved individuals in non-expansion states, who may have new coverage options through the Marketplace upon release from incarceration.
At the state level, states may expand access to Medicaid coverage and care for justice-involved populations through a variety of mechanisms, including existing authorities as well as Section 1115 demonstration waivers. Using information from KFF’s 21st annual Medicaid budget survey and ongoing analysis of Section 1115 waivers and other initiatives, this brief answers three key questions about state efforts to connect individuals to care before, upon, and following release from incarceration:
- What are state proposals to provide pre-release Medicaid coverage to incarcerated individuals?
- How are states coordinating care for incarcerated individuals upon release?
- How are states expanding access to care for justice-involved populations post-release?
What are state proposals to provide pre-release Medicaid coverage for incarcerated individuals?
Although the inmate exclusion policy limits Medicaid coverage available to incarcerated individuals, most states facilitate Medicaid enrollment prior to release. Current rules allow individuals to be enrolled in Medicaid while incarcerated, but the Medicaid inmate exclusion policy limits Medicaid reimbursement for incarcerated individuals to inpatient care provided at facilities that meet certain requirements, including hospitals. However, the majority of states facilitate access to Medicaid coverage by suspending rather than terminating coverage for enrollees who become incarcerated. Suspending eligibility expedites access to federal Medicaid funds if an individual receives inpatient care while incarcerated and also allows coverage to be active immediately upon release, which facilitates access to health care services in the community.
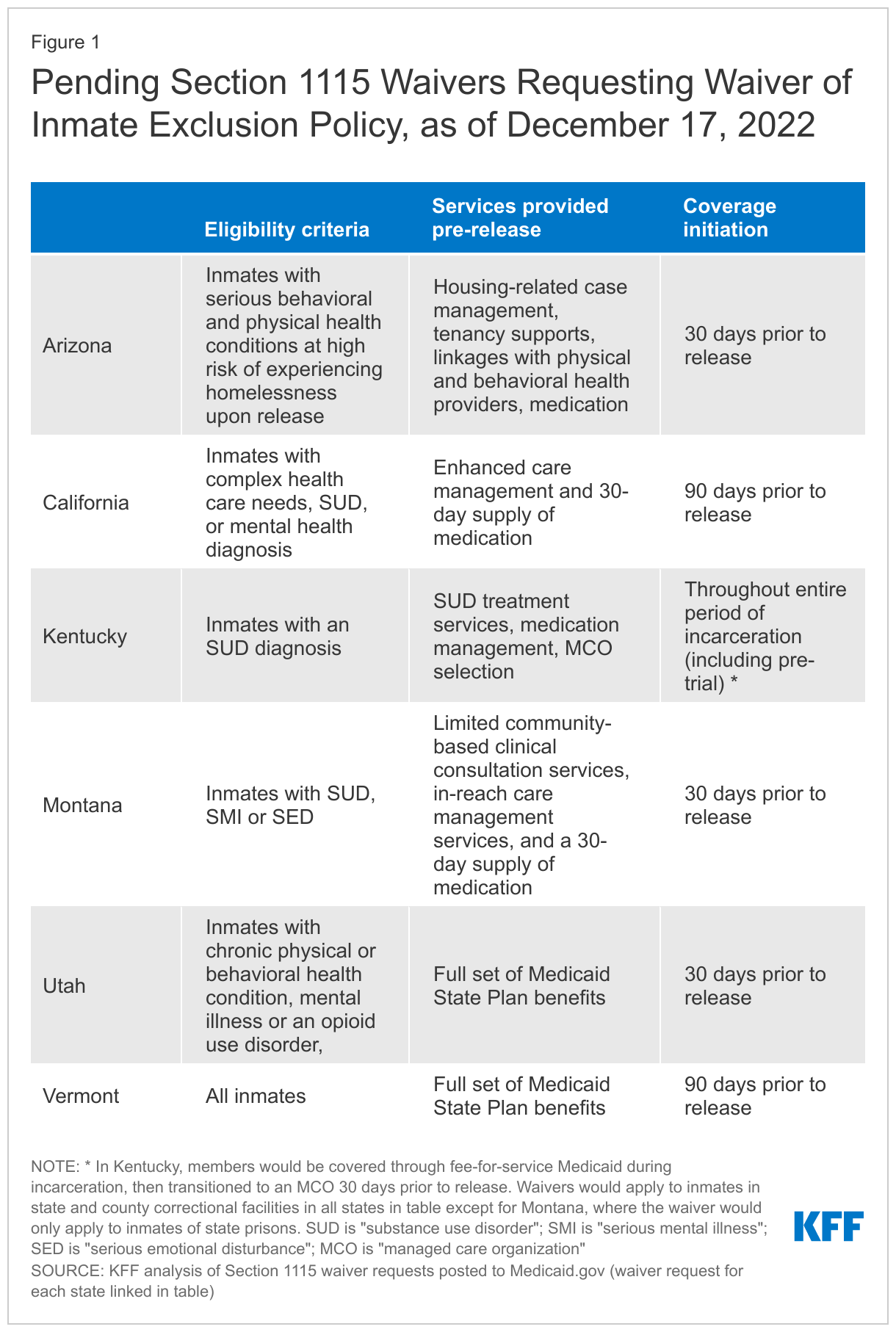
Some states are seeking Section 1115 waiver authority to partially waive the inmate exclusion and provide Medicaid coverage pre-release to certain groups of incarcerated individuals (Figure 1). Section 1115 waivers allow states to test new approaches in Medicaid that differ from federal rules if they promote the objectives of the Medicaid program. To date, no state has received a waiver of the inmate exclusion policy (requests from DC and Illinois were denied by CMS under the Trump Administration). Six states currently have Section 1115 requests (submitted in 2020 or 2021) pending CMS review that would waive the inmate exclusion to allow for coverage of certain Medicaid-eligible inmates prior to release (typically 30 or 90 days). These requests also vary in scope regarding eligible populations and benefit packages (see Figure 1 for details). Most states limit pre-release coverage to inmates with certain behavioral or physical health conditions and would also limit available benefits (typically to include services such as reentry support, enhanced case management, and behavioral health services). Vermont would not limit coverage to certain inmates and Utah and Vermont would provide a full State Plan benefit package for the Medicaid program for which the inmate is eligible.
How are states coordinating care for incarcerated individuals upon release?
An increasing number of states coordinate care for incarcerated Medicaid enrollees upon release through managed care organization (MCO) requirements and/or fee-for-service (FFS) initiatives.1 Although the inmate exclusion policy limits Medicaid coverage available to incarcerated individuals, pre-release care coordination can promote continuity of care for Medicaid enrollees upon release by facilitating connections to care in the community. In response to KFF’s 2021 Medicaid budget survey, more than one-third of states that contract with MCOs (13 of 36) reported requirements for MCOs to provide care coordination services to at least some enrollees prior to release from incarceration, either in FY 2021 (seven states) or planned for FY 2022 (six states).2 3 In comparison, just eight states reported current or planned MCO pre-release care coordination requirements in 2019. For example, states are requiring MCOs to:
- Target pre-release care coordination to incarcerated individuals with complex behavioral or other health needs. For example, Virginia plans to target pre-release care coordination services to high-need enrollees, including those with serious mental illness (SMI), substance use disorder (SUD), chronic conditions, HIV+, Hepatitis C, or who are pregnant. In Arizona, MCOs are contractually required to identify high-risk enrollees prior to release from incarceration and schedule post-release physical/behavioral health appointments for them. Pennsylvania requires MCOs to contract with the same provider used by the Department of Corrections to provide medication-assisted treatment (MAT) following release to ensure continuity of SUD care.
- Connect incarcerated enrollees to wraparound services in the community that target social needs. For example, Ohio requires MCOs to provide enrollees with complex needs with pre-release care coordination services, which may include assistance with social determinants of health (SDOH) (e.g., housing, transportation, food, or clothing.) In Louisiana, high-need MCO enrollees housed in state prison facilities are eligible for pre-release nurse case management. The MCOs are required to complete at least one pre-release case management session in the 60 days prior to release and to continue services post-release. The nurse case managers are responsible for linking members to any type of care they need as well as making referrals to wrap-around services (e.g., cell phones, Supplemental Nutrition Assistance Program benefits, Social Security benefits).
- Provide “in-reach” activities to connect incarcerated individuals with Medicaid prior to release. “In-reach” programs send MCO care managers into correctional facilities to enroll eligible individuals in Medicaid prior to release and connect them to care, such as by developing care plans or making connections to primary care providers. For example, Nevada reported an “in-reach” program to enroll incarcerated individuals in Medicaid prior to release, whereby MCOs go to prisons to explain their plans and value-added benefits.
Additionally, fourteen states (out of 45 responding) reported providing FFS care coordination to at least some individuals prior to release from incarceration, either in FY 2021 (eleven states) or planned for FY 2022 (three states).4 In comparison, eleven states reported current or planned FFS pre-release care coordination initiatives in 2019. Examples of FFS care coordination initiatives include:
- Connecticut facilitates access to medications post-release by providing pharmacy vouchers for up to a thirty-day supply of medication for individuals who applied for Medicaid prior to release, to be dispensed within five days of release.
- Oklahoma’s Office of Juvenile Affairs offers targeted case management to individuals under age 22, who are involuntarily in secure custody and meet Medicaid criteria for inpatient care.
How are state expanding access to care for justice-involved populations post-release?
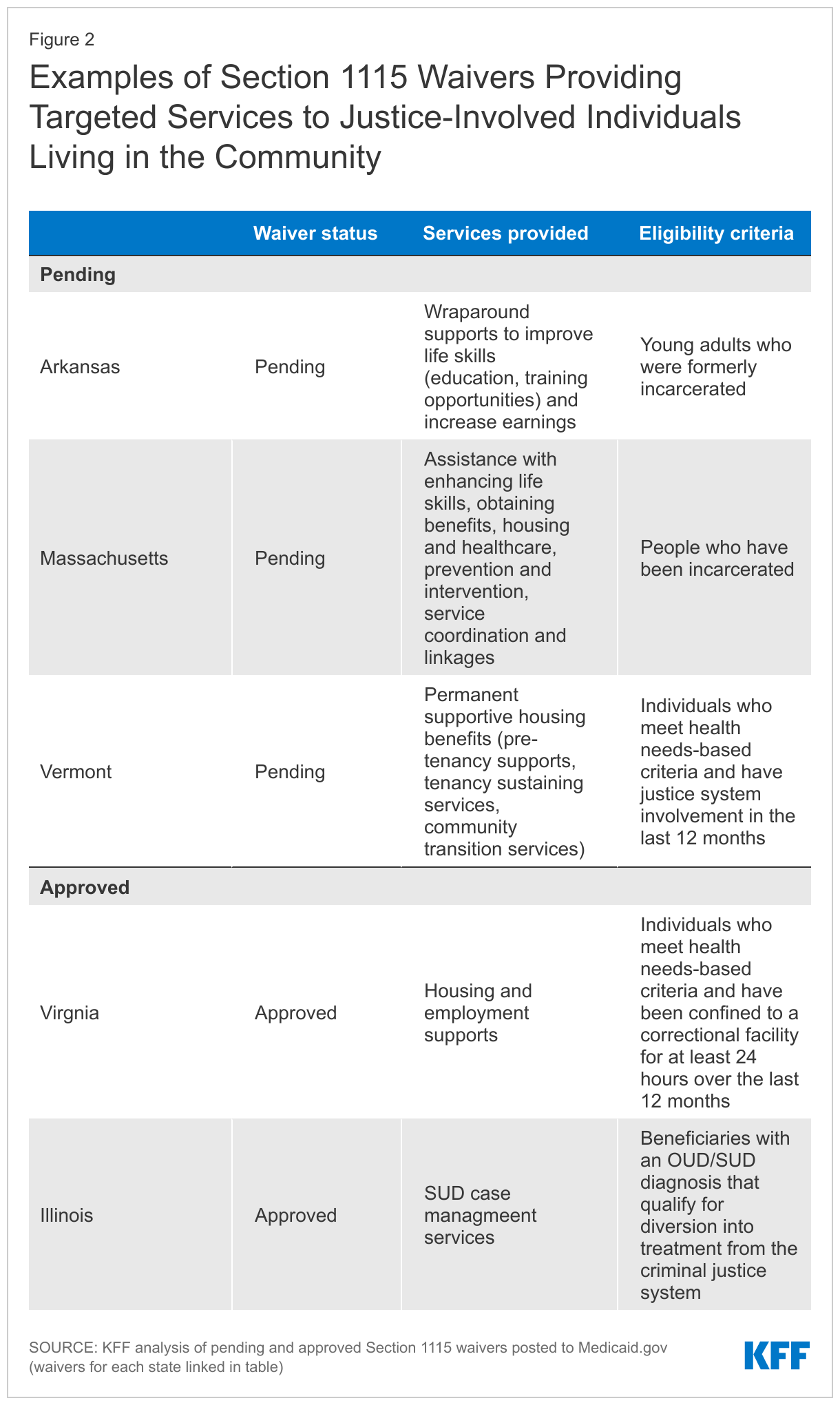
States are also using Section 1115 waivers to target justice-involved enrollees living in the community with social supports, enhanced case management and other care (Exhibit 2). In addition to requests to expand pre-release coverage and initiatives coordinating care upon release (discussed earlier in this brief), states also have approved and pending Section 1115 waivers targeting services and supports to no-longer-incarcerated enrollees with previous justice involvement. Some states limit these services to justice-involved individuals with behavioral health or other needs. Services provided often focus on addressing SDOH through housing, employment, and other social supports (pending in Arkansas, Massachusetts, and Vermont; approved in Virginia). In addition to examples in Exhibit 2, many other states also provide targeted Medicaid services addressing SDOH to high-risk populations, which may include justice-involved populations.
Some states have employed Medicaid State Plan Amendments (SPAs) to target services and supports to justice-involved populations. For example, New York and Rhode Island both have SPAs establishing Health Home pilots focused on care coordination for justice-involved populations with SUD or other behavioral health needs. Michigan is developing a targeted case management program via SPA for individuals recently released from prison or jail.
Looking Ahead
The Biden Administration has identified equity and investments in whole-person care for justice-involved populations as critical strategic priorities for the Medicaid program. Similarly, in response to KFF’s 2021 Medicaid budget survey, many responding state Medicaid officials reported that health equity was a top priority. As people of color are disproportionately represented in the criminal justice system, ensuring this population’s access to Medicaid coverage and care is likely to be a major focus for states and the federal government in the future. If passed, the BBBA’s partial repeal of the Medicaid inmate exclusion policy would allow states to claim Medicaid matching funds to promote continuity of care for Medicaid-eligible incarcerated individuals prior to reentry to the community. The BBBA provision temporarily closing the coverage gap for individuals with incomes below poverty living in non-expansion states would also provide additional coverage options for the justice-involved population. Separately, it is unclear whether and to what extent CMS under the Biden Administration may approve the six pending Section 1115 requests to partially waive the inmate exclusion for Medicaid-eligible inmates prior to release; additional states may also submit similar requests.5 States may also continue to take advantage of other existing authorities—such as SPAs or MCO requirements—to promote access to care for justice-involved individuals.
- Some initiatives reported by states require Section 1115 approval by CMS. Two states (Montana, New York) reported plans to seek waivers of the inmate exclusion policy. ↩︎
- The seven states in FY 2021 are: Arizona, Colorado, Louisiana, New Hampshire, Nevada, Ohio and Pennsylvania. The six states in FY 2022 are: California, Kentucky, Massachusetts, Virginia, Washington, and West Virginia. A total of 36 states with MCOs responded to this question. Delaware, Minnesota, New Mexico, Rhode Island, and Texas did not respond. ↩︎
- Some initiatives reported by states require Section 1115 approval by CMS. Two states (Montana, New York) reported plans to seek waivers of the inmate exclusion policy. ↩︎
- The eleven states in FY 2021 are: Arkansas, California, Colorado, Connecticut, Louisiana, Michigan, New Hampshire, Nevada, Oklahoma, Pennsylvania and Washington. The three states in FY 2022 are: Maine, Montana, and West Virginia. A total of 46 states responded to this question. Delaware, Kentucky, Minnesota, New Mexico, and Rhode Island did not respond. ↩︎
- For example, in response to the 2021 budget survey, New York indicated plans to seek a Section 1115 waiver requesting coverage for eligible inmates 30 days prior to release. ↩︎