Recent Developments and Key Issues to Watch with Medicaid Section 1115 Waivers
Section 1115 demonstration waivers offer states an avenue to test new approaches in Medicaid that differ from what is required by federal statute, as long as the federal Centers for Medicare and Medicaid Services (CMS) determines that such proposals are “likely to assist in promoting the objectives of the [Medicaid] program.” While Section 1115 waivers have been used over time, recent activity from the Trump Administration and into the Biden Administration has tested how these waivers can be used to advance administrative priorities and has also tested the balance between states’ flexibility and discretion by the federal government. The Trump Administration’s Section 1115 waiver policy emphasized work requirements and other eligibility restrictions, payment for institutional behavioral health services, and capped financing. The Biden Administration has signaled a shift in policy to emphasize waivers that expand, rather than restrict, Medicaid coverage and access to care. The Biden Administration has withdrawn work requirements and started to phase out premium requirements, and has instead encouraged states to propose waivers that expand coverage, reduce health disparities, and/or advance “whole-person care” (including addressing health-related social needs). This policy watch describes the current landscape of Section 1115 waivers and highlights key issues to watch: the outcome of litigation related to Georgia’s waiver, as well as the Biden Administration’s decisions on pending requests from Tennessee and other states.
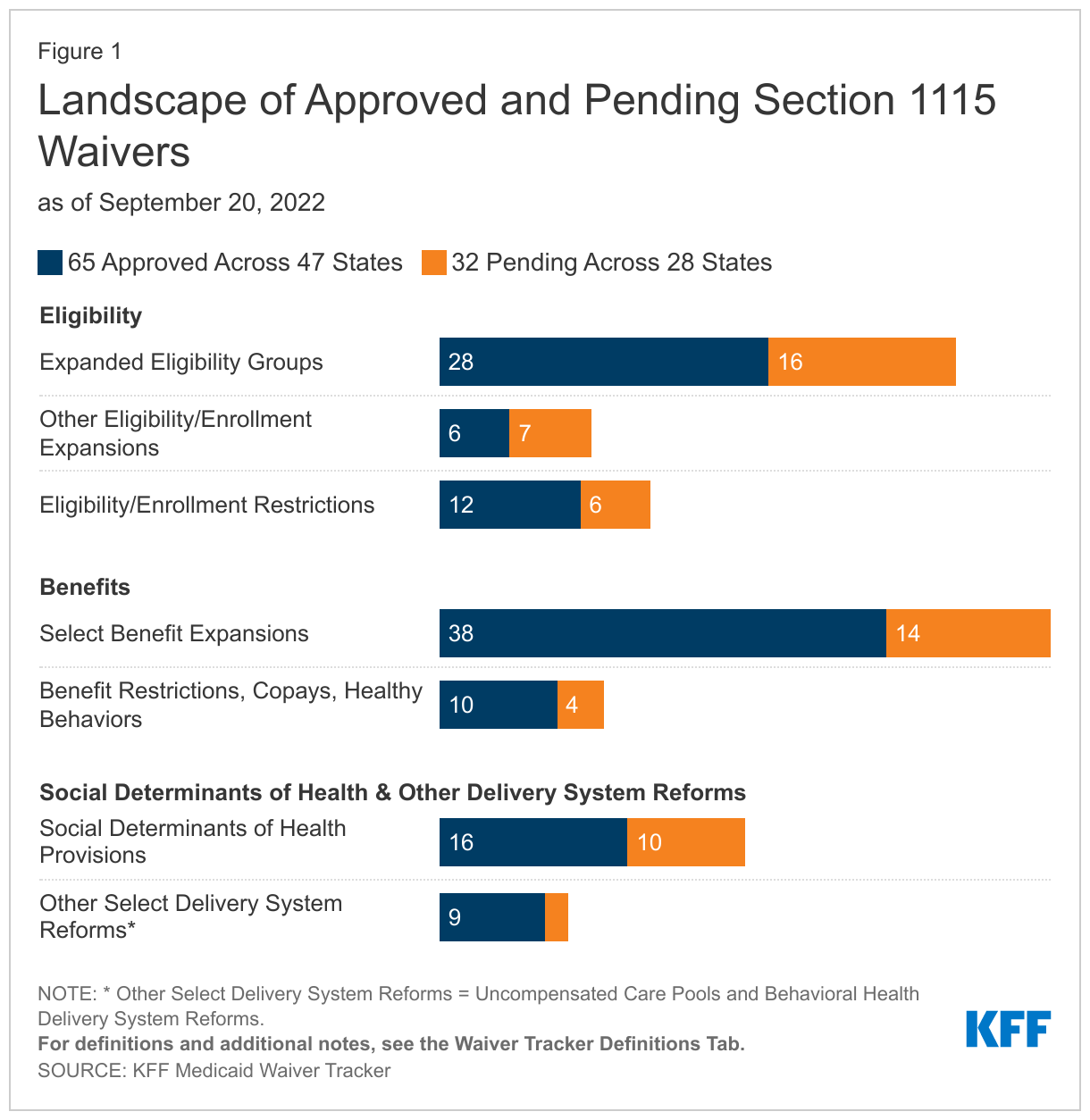
As of September 20, 47 states have a total of 65 approved Section 1115 Medicaid waivers, while 28 states have a total of 32 pending waivers (Figure 1). Pending waivers include new waiver requests and pending extensions or amendments to existing approved waivers. Key themes in current approved and pending waivers include targeted eligibility expansions, benefit expansions (particularly in the area of behavioral health, such as coverage of services provided in institutions for mental disease (IMDs)), and provisions related to social determinants of health (SDOH). More detail on these areas can be found on the updated KFF waiver tracker.
Key Issues to Watch
What will happen with Georgia’s Pathways waiver? The Trump Administration aimed to reshape the Medicaid program by newly approving Section 1115 waivers that imposed work and reporting requirements as a condition of Medicaid eligibility; however, courts struck down many of these requirements and the Biden Administration withdrew these provisions in all states that had approvals. One state affected by these administrative activities was Georgia: in December 2021, CMS rescinded work requirement and premium authorities that the Trump Administration had approved as part of a limited coverage expansion (at the state’s regular match rate for federal funding) in Georgia’s waiver—an action that the state subsequently challenged in court. In August 2022, a Federal District Court judge issued a decision in favor of the state, vacating CMS’s rescission of the work requirement and premium provisions and thus reinstating these provisions. Although CMS generally reserves the right to withdraw waiver authorities at any time, the judge found that its rescission of Georgia’s waiver provisions was arbitrary and capricious due to agency errors, including that it failed to weigh that the waiver would have increased Medicaid coverage. CMS has not yet indicated whether it will appeal this decision.
How will the Biden Administration respond to an amendment to Tennessee’s TennCare III waiver? In January 2021, CMS under the Trump Administration approved a waiver request from Tennessee that set an aggregate cap on federal spending and provided an opportunity for the state to keep a portion of any federal savings. Other controversial aspects of the approval included a closed prescription drug formulary and a 10-year approval period. In June 2022, CMS under the Biden Administration sent a letter to Tennessee asking the state to submit an amendment that would remove the aggregate cap and closed formulary provisions. Tennessee subsequently submitted an amendment that removed these provisions, instead transitioning to a per-capita budget neutrality cap that would allow the state to access the federal share of any savings if expenditures are lower than the cap to invest in Designated State Investment Programs (DSIPs). The amendment leaves the 10-year approval period (through 2030) in place. The waiver is open for federal comment through October 6, but it is unclear how the Biden Administration will respond to the revised financing request.
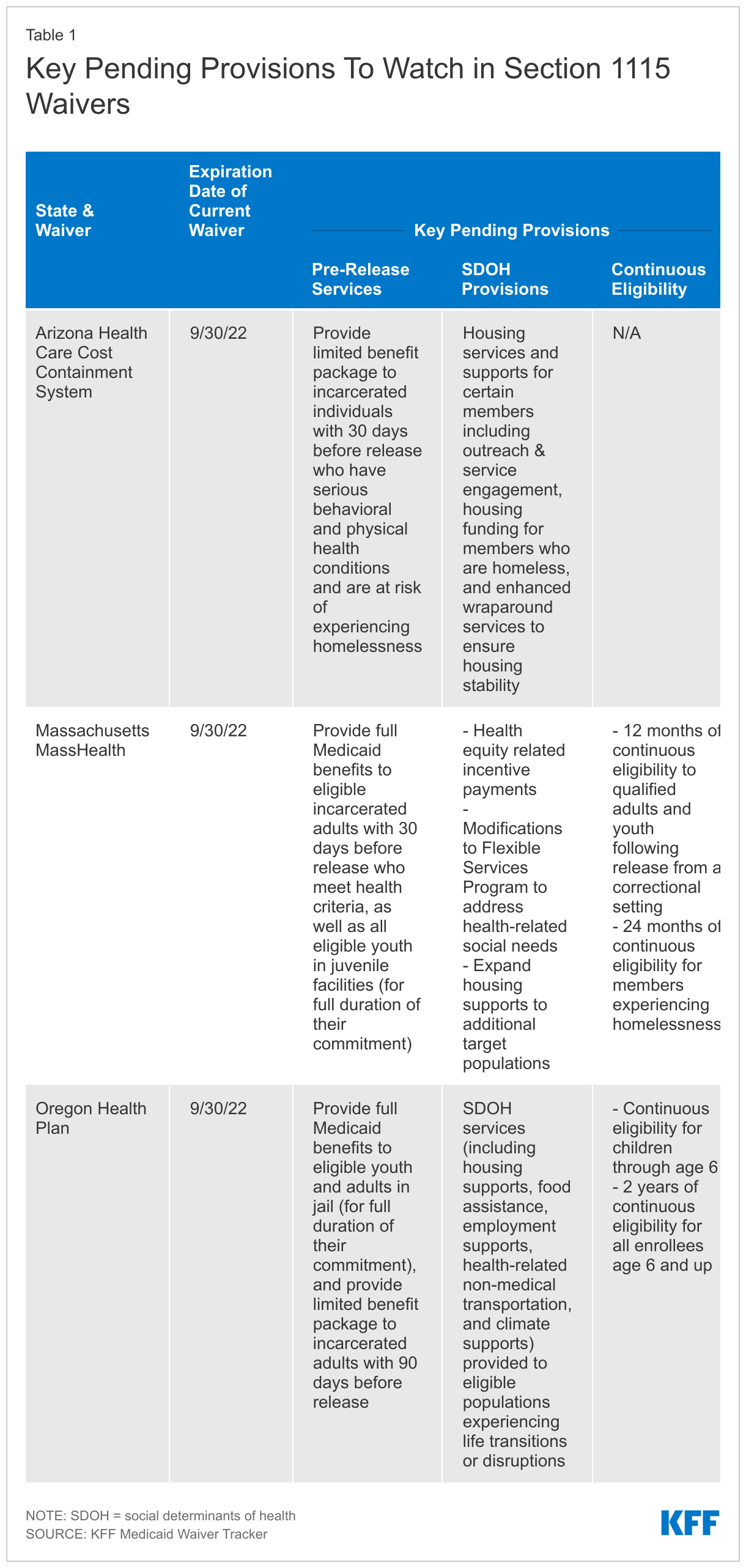
What provisions will be approved in several key waivers that expire at the end of September? Several states have Section 1115 demonstrations set to expire on September 30. Key provisions to watch in extension proposals from these states would: address enrollees’ SDOH and health equity; expand pre-release services available to incarcerated populations; and provide continuous eligibility for adults and children (Table 1). CMS has indicated an openness to approving some of these provisions, which may align with its strategic priorities under the Biden Administration. For example, in a June 2022 letter to Massachusetts, CMS wrote that it “strongly supports the goals set forth in the state’s extension proposal” and that “CMS and Massachusetts are jointly committed to finalizing the state’s demonstration extension by September 30, 2022, including approval of…authorities necessary to achieve our shared goals.”
The outcome of waiver proposals and litigation could have implications for other states. The court decision in favor of Georgia calls Section 1115 policy and process into question by limiting CMS’s authority to determine whether already-approved waivers advance Medicaid program objectives. Especially if CMS appeals the decision, the outcome of the case could have implications for other states that may similarly seek limited coverage expansions conditioned on other provisions (like work requirements and/or premiums). Upcoming CMS decisions on Tennessee’s amendment and waivers expiring at the end of September may indicate how the Biden Administration will respond to financing proposals and the extent to which the administration will allow states to use waivers for coverage for incarcerated individuals, to address social determinants of health, and for continuous coverage. In addition to Arizona, Massachusetts, and Oregon, other states are requesting similar provisions in waivers pending or in development at the state level. For example, 10 states in total have pending waivers to provide pre-release coverage to certain incarcerated individuals (Arizona, California, Kentucky, Massachusetts, Montana, New Jersey, Utah, Vermont, Washington, and West Virginia) and five states have pending waivers to provide continuous eligibility for certain populations (Kansas, Massachusetts, New Jersey, Oregon, and Washington). Similar to Oregon, Washington and New Mexico (whose waiver is currently undergoing state-level public comment) are both pursuing continuous enrollment for children through age six. Potential approval of these demonstrations could allow the Biden Administration to promote its strategic Medicaid priorities, which include expanded access to coverage.