Contraceptive Implants: Access and Coverage in the U.S.
The contraceptive implant is the most effective reversible birth control method available. Implants, along with intrauterine devices (IUDs), are known as long-acting reversible contraception (LARCs) because they can be used to prevent pregnancy for several years and can be removed at any time. Implants have been available since the 1990s and have undergone substantial design modifications since their debut. The newest generation implant was introduced to the U.S. market in 2006 and remains the only contraceptive implant available in the U.S. Barriers to implant use include limited awareness and availability, high up-front costs for clinicians to stock the device, and required insertion and removal by a trained clinician. This fact sheet provides an overview of contraceptive implants including use, availability, and financing.
Background
In 1990, the Food and Drug Administration (FDA) approved Norplant, manufactured by Leiras Oy, the first subdermal contraceptive implant that was inserted under the skin of the upper arm by a trained clinician. Made of silicone, it had six capsules containing levonorgestrel, a synthetic hormone, and was effective for up to five years. Following concerns about its effectiveness and lawsuits on behalf of users who experienced complications, Norplant’s distributor, Wyeth-Ayerst, discontinued its U.S. distribution in 2002.
In 2006, the FDA approved Implanon, a single, thin, plastic, etonogestrel-releasing rod inserted under the skin of the arm. It is manufactured by Organon USA, a division of Merck. The improved design and composition made Implanon easier and faster to insert and remove than first generation implants. In 2010, the manufacturer replaced Implanon with Nexplanon, which is designed to be radiopaque (visible through x-ray) and has an improved insertion device. It is FDA-approved for use up to five years and prevents pregnancy by suppressing ovulation.
With a 0.05% failure rate, the contraceptive implant is the most effective FDA-approved reversible contraceptive. Additionally, the implant removes the potential for user error and non-use associated with self-administered contraception because it is inserted by a clinician and does not require any regular maintenance by the user.
Implants must be inserted and removed by a trained clinician who uses a special insertion device to place the implant just under the skin of the patient’s upper arm. Once inserted, the clinician ensures proper placement of the device by palpating the insertion site. The minor surgical procedure takes a few minutes and requires a local anesthetic and a small incision. After five years of use, the implant must be removed by a trained clinician, and if the patient desires, a new implant can be placed at that time. Implants may be removed by a clinician at any time before five years, and pregnancy can occur as soon as the first week following removal.
Contraceptive implants are safe for most people and can be inserted any time if the user is not pregnant. Implants are primarily used for pregnancy prevention, but they can also be used to reduce menstrual cramps and make menstrual periods lighter. While there has been some concern about hormonal contraception for individuals who are breastfeeding, findings from the U.S. Selected Practice Recommendations for Contraceptive Use show that progestin-only methods, such as the implant, do not appear to negatively affect breastfeeding outcomes. Some common side effects include irregular menstrual bleeding, headache, weight gain, and breast pain, which may lead to discontinuation among some users. Although rare, some users who smoke or have certain health conditions may have a higher risk of developing severe complications.
Implant Use, Availability, and Awareness
Use
Because of their efficacy, continuation, and satisfaction rates, leading medical groups including the American College of Obstetricians and Gynecologists (ACOG) and the American Academy of Pediatrics have recommended the use of implants for most individuals of reproductive age, including adolescents and nulliparous and postpartum women. However, research demonstrates persistent misperceptions and a lack of awareness about implants. Although implant use in the U.S. has increased since it was first introduced in 1995, it is still lower than other contraceptive methods such as the IUD, pill, and sterilization.
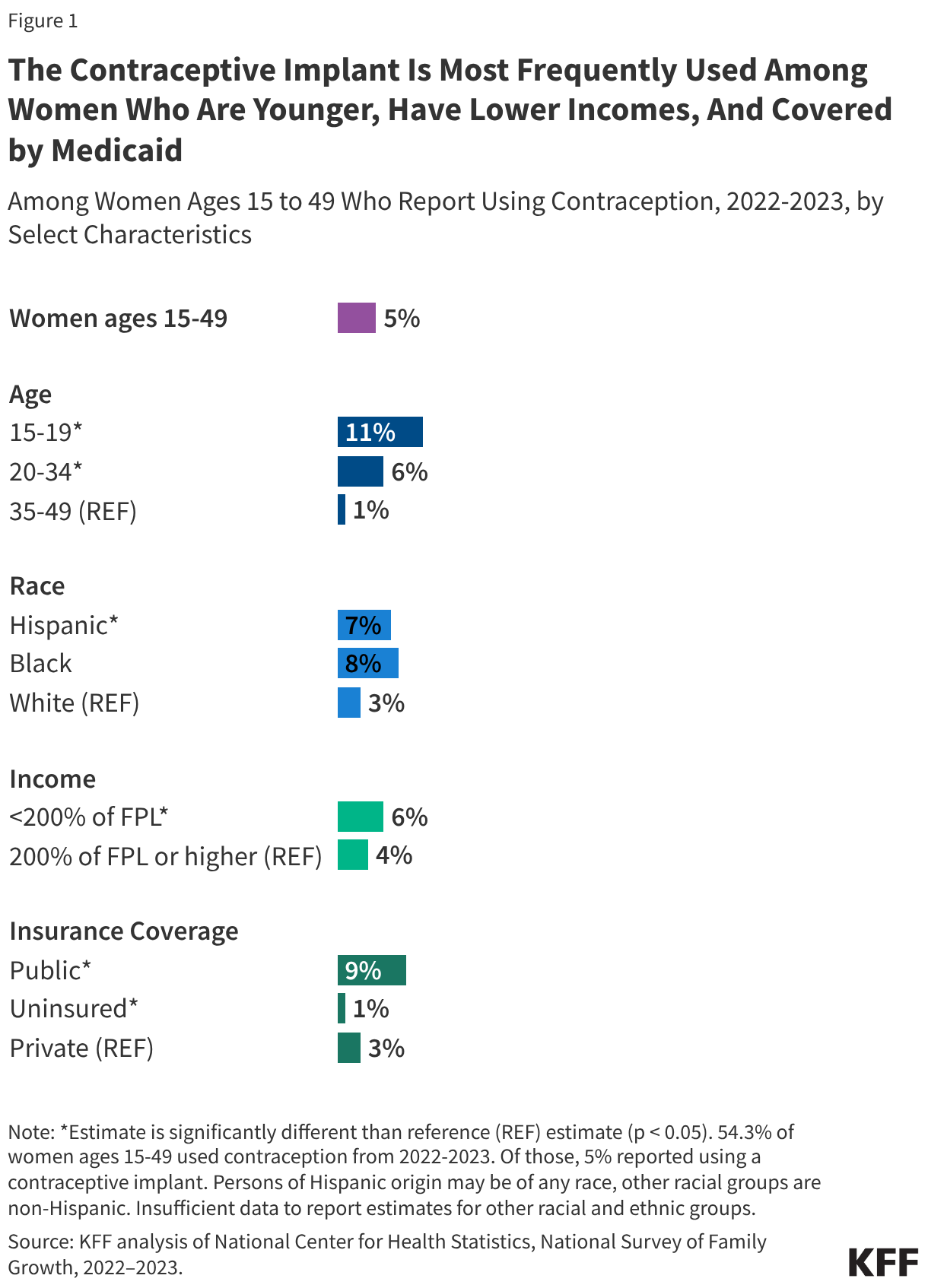
Between 2022 and 2023, the most recent years for which there are national data, 5% of women ages 15-49 who were currently using contraception used the implant (Figure 1). Implant users tended to be younger, lower-income, and covered by Medicaid. Notably, one in ten (11%) adolescent girls who use contraception report using the contraceptive implant compared to only 1% of women ages 35 to 49. Possible explanations for the association of higher implant use among younger women and lower-income women include the desire to avoid pregnancy for a longer period of time, lower maintenance and chance of user error, promotion of LARCs by medical organizations for adolescents, and availability at publicly funded clinics.
Availability and Awareness
Access to implants can depend, in part, on the clinician’s ability and willingness to offer them. A 2023 KFF survey of OBGYNs found that eight in ten (83%) OBGYNs provided contraceptive implants in their practice. Publicly funded family planning clinics are an important source of care for many low-income and uninsured people of reproductive age. Access to contraceptive implants has been challenging for some clinics due to high upfront costs, as well as limited training and staff capacity to insert the device. As a result, some sites may be unable to provide the full range of contraceptive services to their patients, including contraceptive implants. Overall, 75% clinics offered implants from 2022-2023 compared to 61% in 2015.
Physicians may require multiple visits for a contraceptive implant insertion, which can be inconvenient for patients with limited time and resources. ACOG recommends OBGYNs implement same-day insertion procedures to improve patient access and experiences with contraceptive care, but some clinicians report barriers such as high upfront costs and challenges with reimbursement for contraceptive implants. Nonetheless, the share of publicly funded family planning clinics that offer same-day contraceptive implant insertions has increased overall. Between 2022 and 2023, about two-thirds (69%) of clinics performed same-day insertions, compared to one in three (37%) in 2015.
In 2026, the FDA made some changes to the provision of implants. One change was the extension of the use of the implant from three to five years. Additionally, the FDA made the implant available only through the FDA’s Risk Evaluation and Mitigation Strategy program (REMS), a drug safety program with special requirements for clinicians, pharmacies, and other distributors who wish to provide the implant, due to the rare but serious health risks associated with improper insertion of the device. The Nexplanon REMS program requires clinicians to register with REMS, pass a specialized knowledge assessment, and complete an in-person 90-minute training from the manufacturer to become certified in Nexplanon insertion and removal. In addition to medical doctors, the training is open to advanced practice clinicians (such as nurses and physician assistants) who are authorized to perform implant insertions and removals in their practice jurisdiction. Additional clinical training for the implant is available from a variety of reproductive health organizations.
Insurance Coverage and Financing of Implants
The wholesale price for an implant is about $1275, in addition to potential costs associated with insertion and removal. The Affordable Care Act’s (ACA) contraceptive coverage requirement eliminated many women’s out-of-pocket costs for contraceptives, although some women still do not have access to full coverage.
There is currently no generic or therapeutically equivalent version of Nexplanon available in the U.S. Nexplanon’s manufacturer, Organon USA (a division of Merck), currently holds patents on the device and associated materials, though these patents are set to expire between 2027 and 2030.
Private Insurance
The ACA includes a requirement that most private insurance plans cover at least one type of all 18 FDA-approved contraceptive methods as prescribed without cost sharing. This means that most private plans must cover the implant at no cost to policy holders. Before the ACA was passed, individuals with private insurance were likely to face out-of-pocket expenses for the implant and associated visits. After the contraceptive coverage mandate went into effect in 2012, research found that about three in four (73%) women with private insurance paid $0 in out-of-pocket expenses for contraceptive implants in 2020, compared to about three in then (28%) in 2012. However, recent research suggests an increase in the number of women with out-of-pocket expenses for contraceptive implant insertion, despite the coverage requirement. While nearly two-thirds (64%) of women with private insurance continued to have no out-of-pocket expenses for contraceptive implant insertion, over one in three (36%) paid a median cost of $16.88 for implant-related services in 2023—including office visits, ultrasounds, medications, and STI and pregnancy testing. Nonetheless, studies have found an increase in LARC initiation overall among women with private insurance coverage since the ACA’s coverage requirement took effect.
Insurers can use medical management to help control costs and encourage beneficiaries to choose more affordable contraceptive methods, but federal guidance prohibits insurers from categorically restricting access to a particular contraceptive method. Insurers can choose to cover generic contraceptives while charging cost-sharing for the brand-name version. Since contraceptive implants do not have a generic equivalent, the brand-name version (Nexplanon) must be covered without cost-sharing.
Medicaid
Federal law requires Medicaid programs to cover family planning services and supplies without cost sharing, but there are variations in coverage between states and between different Medicaid populations. For enrollees of the traditional Medicaid programs that were in place prior to the passage of the ACA, coverage of implants is determined by each state program. Recognizing the high (cost) effectiveness of LARCs, many states are pursuing policies to reduce barriers to provision, like reimbursing for insertion and removal, returning unused devices for credit, and providing hospitals with separate payments for post-partum LARC insertion.
Those who qualify for Medicaid under the ACA’s expansion of the program must receive coverage for the implant because the ACA requires these expansion programs to cover all FDA-approved methods for women without cost sharing, which is the same as the requirement for private insurance plans. Furthermore, 30 states and D.C. extend Medicaid coverage for family planning services, including contraception, to some uninsured women who do not qualify for full scope Medicaid.
Uninsured
The federal Title X Family Planning Program funds a network of clinics to provide family planning care to millions of low-income and uninsured people at reduced or no cost. Federal guidelines such as the Office of Population Affairs’ and the CDC’s Providing Quality Family Planning Services (QFP) and the Health Resources and Services Administration’s (HRSA) recommendations for women's preventive services state that offering women the full range of FDA-approved contraceptive methods is a crucial aspect of quality family planning services.
Research shows that sites that received Title X funds were consistently more likely to offer contraceptive implants compared to sites that do not receive Title X funding. Community health centers (CHCs) and specialized family planning clinics such as Planned Parenthood centers play a critical role in providing reproductive health care to low-income people, medically underserved communities, and people who are uninsured. CHCs are required to provide “voluntary family planning” services but have significant leeway in determining the specific services they provide. For example, nearly all (98%) Planned Parenthood clinics offered same-day implant insertions from 2022 to 2023, compared to just over half (57%) of federally qualified health clinics.
As a result of the 2025 One Big Beautiful Bill Act and other federal policy changes, the uninsured rate is expected to rise substantially over the next decade. Uninsured women could decide to stop using contraception because they cannot afford it or switch to a less effective method, which could result in an increase of unwanted pregnancies and a loss of reproductive autonomy. KFF research has found that one in five uninsured women of reproductive age has had to stop using a birth control method in the past 12 months because they couldn’t afford it, a rate that is four times greater than those with Medicaid (5%) or private insurance (2%).