State Policies Expanding Access to Behavioral Health Care in Medicaid
Issue Brief
Key Takeaways
Behavioral health conditions—including mental illnesses and substance use disorder (SUD)—are especially common among Medicaid enrollees and have worsened during the COVID-19 pandemic. Efforts to address these issues have been a focus in Medicaid at the federal level, including in the 2018 SUPPORT Act and more recently in the 2021 American Rescue Plan Act (ARPA), which provided enhanced Medicaid funding for certain behavioral health providers and mobile crisis services. The proposed Build Back Better Act (BBBA) passed by the House of Representatives on November 19, 2021 would build on both ARPA provisions and also expand funding for community mental health services. Also, CMS under the Biden Administration has identified behavioral health policy and investments as a key federal Medicaid priority.
States are taking advantage of new federal policy options to address behavioral health issues in Medicaid and are also developing other initiatives to improve mental health and substance use outcomes. Outside of Medicaid, other state agencies may also take steps to address behavioral health outcomes, sometimes including Medicaid populations but often broader. On KFF’s 21st annual Medicaid budget survey, all responding states reported at least one initiative to expand behavioral health care in Medicaid in state fiscal year (FY) 2021 and/or 2022,1 including crisis service and other benefit expansions, initiatives to expand telehealth and address equity, and managed care changes. This brief summarizes data from this survey, with key findings including:
- More than half of states reported plans to take up the new ARPA community-based mobile crisis intervention service option and about two-thirds reported another crisis service initiative. States are also expanding a wide range of other Medicaid behavioral health services such as screening.
- Many states expanded telehealth to increase access to care during the COVID-19 pandemic, and as of July 1, 2021, nearly all states covered telehealth delivery of behavioral health services. Many states plan to continue this coverage post-pandemic. States also reported other access-related behavioral health initiatives including to address disparities and to promote co-location.
- Most states continue to rely on managed care organizations (MCOs) to deliver behavioral health services. Most allow MCOs to use “in lieu” of authority to cover certain behavioral health services, particularly to allow coverage of services provided in institutions for mental disease (IMDs).2
Some states reported behavioral health initiatives across many areas, often as part of wide-ranging statewide initiatives identified as top priorities for their Medicaid programs—examples include California, Colorado, Massachusetts, Montana, and Washington. Looking ahead, more than one-third of responding states mentioned behavioral health initiatives as a future priority, and several identified behavioral health services as an upward spending pressure in FY 2022. Continued efforts at the federal level may affect the level of enhanced Medicaid funding available to states for expanded behavioral health services. Additionally, it is unclear how behavioral health service patterns may change in the aftermath of the COVID-19 pandemic and whether or how states may modify or adopt new initiatives in this area.
Introduction
Medicaid plays a key role in covering and financing behavioral health care: in 2020, Medicaid covered 23% of nonelderly adults with mental illness, 26% of nonelderly adults with serious mental illness (SMI), and 22% of nonelderly adults with SUD; in comparison, Medicaid covered 18% of the general nonelderly adult population (see Appendix A).3 The COVID-19 pandemic and resulting economic recession have negatively affected mental health and substance use outcomes and exacerbated barriers to care.
Efforts to address the opioid epidemic and broader behavioral health issues have been a focus in Medicaid in recent years, including through federal legislation such as the 2018 SUPPORT Act. More recently, ARPA provided enhanced Medicaid funding that could be used to support behavioral health home and community-based services (HCBS) providers and to provide community-based mobile crisis intervention services; the proposed BBBA (passed by the House of Representatives on November 19, 2021) would build on both of these options. The BBBA would also expand funding for a community mental health services Medicaid demonstration program for states to implement Certified Community Behavioral Health Clinics.
This brief draws on data from KFF’s 21st annual Medicaid budget survey4 to assess how states are using new federal policy options and implementing other innovative behavioral health initiatives. We focus on efforts to expand behavioral health benefits, improve access to behavioral health care and equity, and leverage MCOs to deliver behavioral health benefits.
How are states expanding behavioral health benefits?
Federal law mandates Medicaid coverage of many behavioral health benefits, and states may also cover additional optional behavioral health benefits. Behavioral health services for children are particularly comprehensive due to Medicaid’s Early, Periodic Screening, Diagnosis, and Treatment (EPSDT) benefit for children (see Appendix A). In the years prior to the COVID-19 pandemic, states were increasingly expanding optional behavioral health benefits and taking advantage of federal options in the SUPPORT Act. Adverse effects of the COVID-19 pandemic on mental health and substance use outcomes have brought further focus to behavioral health issues and prompted the Substance Abuse and Mental Health Services Administration (SAMHSA) to issue multiple COVID-19 grants, available to state agencies to address mental health and SUD outcomes. Other recent federal policy options more directly target Medicaid, such as ARPA’s expansion of mobile crisis response services, which aim to connect Medicaid enrollees experiencing mental health crises to appropriate community-based care (an option which the proposed BBBA would make permanent).
At the time of survey completion, more than half of states indicated they will or probably will take up the new option under ARPA to provide community-based mobile crisis intervention services. ARPA provides 85% federal matching funds for these crisis intervention services for the first three years, with these additional funds to supplement, not supplant, the level of state spending for these services. The ARPA model dispatches multidisciplinary mobile crisis teams to provide Medicaid-covered services to enrollees experiencing a mental health or SUD crisis outside a hospital or other facility setting. These mobile crisis services generally do not have to be offered statewide and can be targeted to specific groups of enrollees (rather than be available to all Medicaid enrollees). States may limit enrollees’ choice of provider for these services. Under ARPA, this new option is available to states for five years, beginning April 1, 2022; however, a provision in the proposed BBBA would make this option available permanently. ARPA also authorized $15 million for state planning grants; these were awarded to 20 states in September 2021 (however, under ARPA, all states are eligible to take up this option beginning April 1, 2022, including those that did not receive planning grants).
About two-thirds of responding states indicated they have other, non-ARPA-related crisis service initiatives in place in or planned for FY 2022. Some of these initiatives are limited to Medicaid enrollees and funding, but others have a broader focus. Commonly reported initiatives include mobile crisis response and service initiatives (separate from the ARPA option); crisis hotlines; and crisis diversion, stabilization, and/or receiving centers. Crisis hotlines include 988 hotlines, which were designated by the Federal Communication Commission as the new phone number to connect individuals with suicide prevention and mental health crisis counselors. One state (New Hampshire) is planning implementation of a Critical Time Intervention model to provide support to individuals with SMI during vulnerable periods of transition (e.g., discharge from a psychiatric hospital).
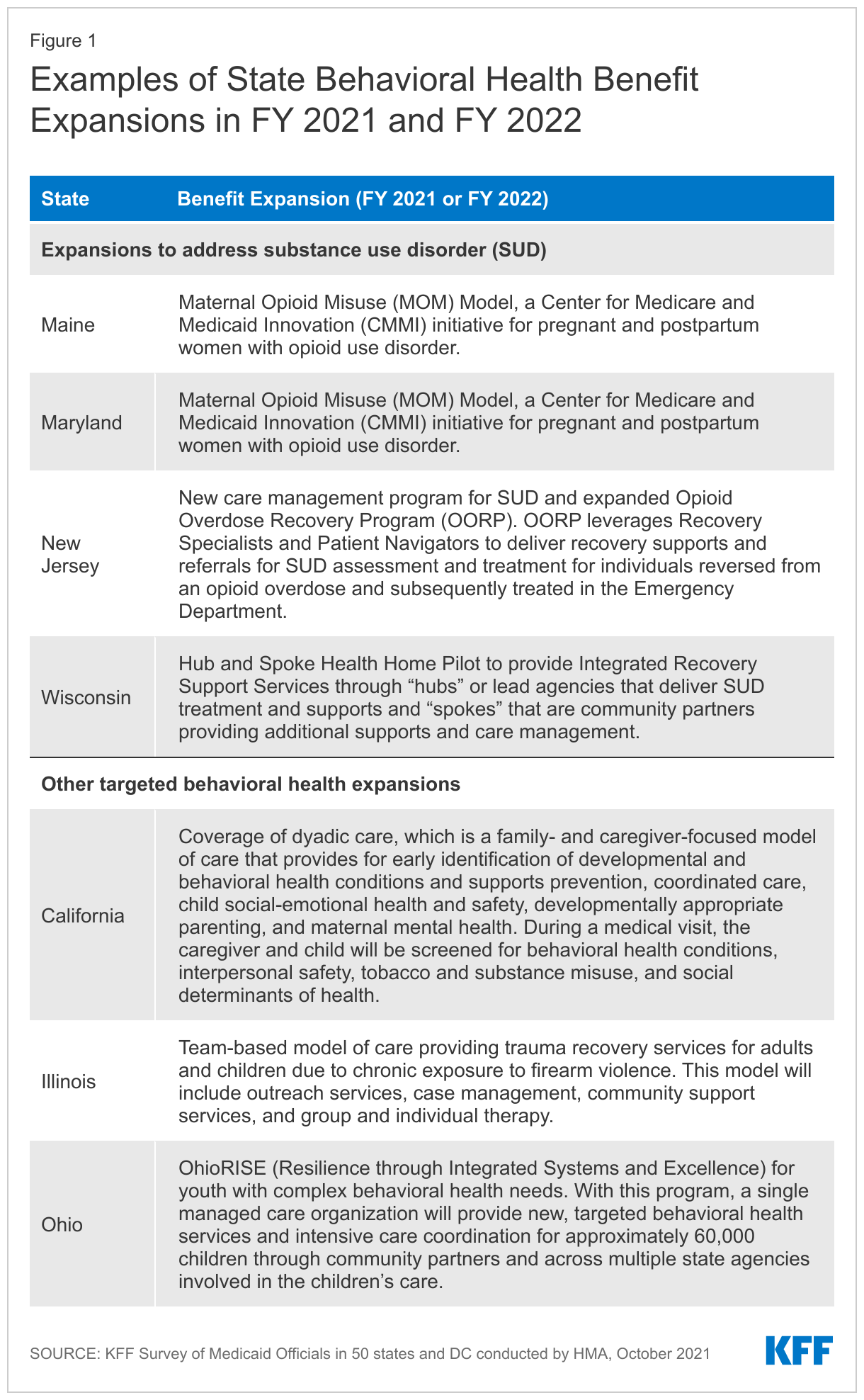
States are also expanding a wide range of Medicaid behavioral health services, some targeted to specific populations or needs (Figure 1). States reported service expansions across the care continuum, including institutional, intensive, outpatient, and home and community-based behavioral health services. Continued state focus on SUD benefit expansions is consistent with past years and aims to target the substance use crisis that has worsened during the COVID-19 pandemic. States reported approaches to targeting SUD including new or expanded residential/inpatient SUD benefits, coverage of opioid treatment programs, and enhanced care management.5 States are also implementing other targeted benefit expansions to address mental health and other needs that have been adversely affected by the COVID-19 pandemic, such as exposure to gun violence (addressed by a benefit expansion in Illinois). Overall, on the 2021 budget survey, 10 states reported new or expanded mental health and/or SUD benefits in FY 2021 and 14 states reported such expansions planned for FY 2022 (see Figure 1 for examples). These include expanded coverage of intensive outpatient services, clinic services, school-based services, and supportive employment services. Some behavioral health benefit expansions are targeted to specific populations such as children or pregnant/postpartum women.
More than four-fifths of states reported initiatives in place related to screening enrollees for behavioral health needs, in fee-for-service (FFS) and/or through MCO contract requirements. Behavioral health screenings are one strategy for Medicaid to connect individuals with behavioral health needs to the appropriate services. Most responding states that contract with MCOs (31 of 37) reported FY 2021 contract requirements related to behavioral health screening, and two MCO states reported plans to implement such requirements in FY 2022. About half of all responding states reported non-MCO initiatives related to behavioral health screening in FY 2021 and FY 2022.
What initiatives are states adopting to improve access to behavioral health care and equity?
The COVID-19 pandemic has created new barriers to care for people already experiencing behavioral health conditions and had disproportionate negative impacts on behavioral health outcomes for people of color. Telehealth—which was becoming more common in Medicaid programs prior to the pandemic—may be an important component of facilitating access to behavioral health services for children and adults, especially during the pandemic, and ARPA included funding accordingly to support behavioral health professionals’ utilization of telehealth. States have broad flexibility to determine whether and how to cover services (including behavioral health) delivered via telehealth in their Medicaid programs.
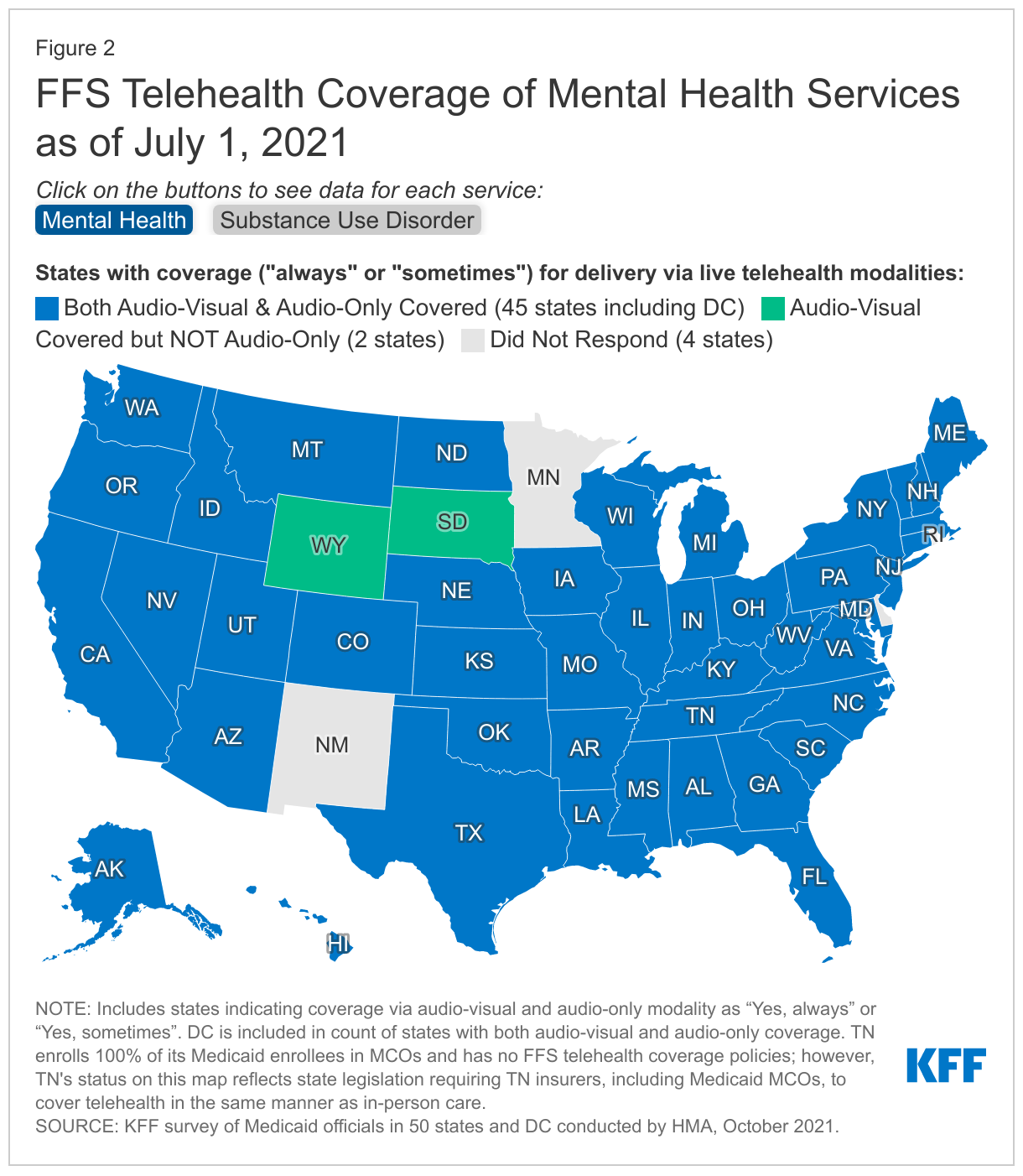
As of July 1, 2021, all responding states cover audio-visual telehealth delivery of behavioral health services, and almost all also cover audio-only delivery of these services (Figure 2). All responding states (47) reported that they sometimes or always covered audio-visual delivery of FFS mental health and SUD services. Almost all reported covering audio-only delivery of FFS mental health (45 states) and SUD services (44 states). Nearly all MCO states reported requiring MCOs to cover the same services via telehealth as covered in FFS. Across service categories, most states are considering post-pandemic telehealth policies, with many weighing expanded access against quality concerns especially for audio-only telehealth. States were more likely to report plans to maintain audio-only coverage for mental health and SUD services compared to other, non-behavioral health services.
States report that telehealth helped maintain and expand access to behavioral health care during the pandemic. Thirty-one states (out of 45 responding) reported that telehealth, especially expanded audio-only coverage, had particular value in maintaining or improving access to behavioral health services. The survey also asked states to identify the top two or three categories of behavioral health services that had the highest telehealth utilization during FY 2021; states most frequently identified psychotherapy, counseling (for mental health conditions and/or SUD), and patient evaluations.
Eight states reported current or planned initiatives to address racial/ethnic disparities in behavioral health in Medicaid.6 Prior to the pandemic, Black and Hispanic people were less likely to receive needed behavioral health services compared to the general population, and during the pandemic, Black and Hispanic adults have been more likely to report symptoms of anxiety and/or depressive disorder. The recent uptick in substance use issues is also disproportionately affecting many people of color. Of the states that identified any initiatives addressing racial/ethnic health disparities, eight reported initiatives to specifically address disparities in behavioral health care and outcomes. These include managed care requirements and/or initiatives, efforts to improve data collection and stratification, and eligibility or benefit expansions that would address behavioral health disparities. For example:
- California’s value-based payment program directs MCOs to address health disparities by making enhanced payments that target SMI, SUD, and homelessness.
- Connecticut’s recent procurement for behavioral health Administrative Services Organization (ASO) services requires bidders to identify specific, actionable strategies to improve equity, with an emphasis on race and ethnicity.
- Since FY 2020, Michigan has used capitation withholds to incentivize reductions in racial disparities in behavioral health metrics.
Many states reported a need to improve data collection to enable identification of racial/ethnic health disparities, and future initiatives to address behavioral health disparities may emerge as data becomes better known.
Nearly half of states reported initiatives to promote physical and behavioral health co-location in place in or planned for FY 2022. Some of these initiatives are limited to Medicaid enrollees and funding, but others have a broader focus. Many individuals receiving care for behavioral health conditions also have physical health conditions that require medical attention, and the inverse is also true. One approach to address care fragmentation and better integrate physical and behavioral health care is co-location of both types of care at the same site. Reported initiatives were most frequently at Certified Community Behavioral Health Clinics (CCBHCs),7 community mental health centers (CMHCs), federally qualified health centers (FQHCs), and health homes. For example, state legislation in Kansas directs the state to establish a certified CCBHC model in FY 2022, which will encourage CMHCs to begin offering physical health services. Several states reported plans to cover new integrated care services, while others reported allowing for payment of a behavioral health encounter on the same day as a medical encounter and/or other administrative changes. A few states mentioned incentive payments for providers or MCOs who promote integrated care.
Other notable co-location initiatives in place or planned include:
- California is proposing to implement its CalAIM initiative in January 2022, which will integrate the administration and financing of specialty mental health and SUD services under a single state/county contract. The goal is to improve outcomes for enrollees through more coordinated treatment and to allow providers to respond in a more patient-centered way. Distinct from this behavioral health integration effort, CalAIM also includes a plan to test the full integration of physical health, behavioral health, and oral health under one contracted managed care entity.
- Missouri aims to increase co-location by expanding its care integration program—which currently involves collaboration between FQHCs and CMHCs—to include collaboration between FQHCs and SUD providers.
- New Hampshire is continuing to implement ProHealth Grants to work with three CMHCs and three FQHCs to develop integrated health homes for people ages 16 to 35. The goal of this program is to integrate FQHC services (such as screening, detection, and treatment of physical health conditions) within the CMHCs to improve and prevent future health conditions.
How are states using MCOs to deliver behavioral health services?
States use a combination of FFS and managed care arrangements to deliver behavioral health care to Medicaid beneficiaries, with these services increasingly being provided by MCOs in recent years (see Appendix A). Under federal Medicaid regulations, states may allow MCOs to offer services or settings that substitute for those that are covered under the state plan. These in lieu of services (ILOS) must be identified in the MCO contract and enrollees may not be required to use them.8 In recent years, states have increasingly used MCO “in lieu of” authority to cover services provided to nonelderly adults in “institutions for mental disease” (IMDs) that otherwise would be ineligible for federal Medicaid funding. The 2018 SUPPORT Act codified the existing Medicaid managed care regulation allowing capitation payments to include IMD services up to 15 days per month using “in lieu of” authority.
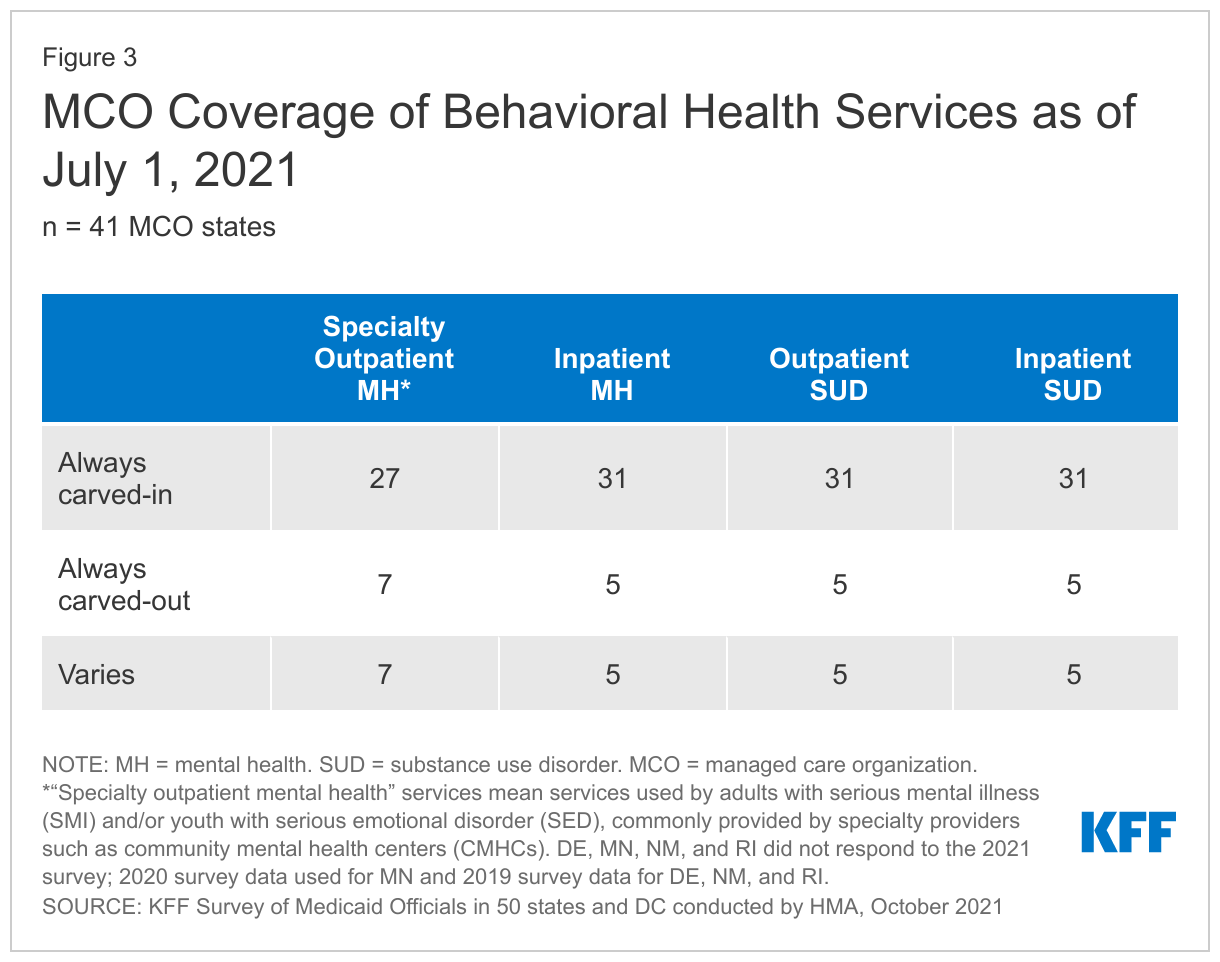
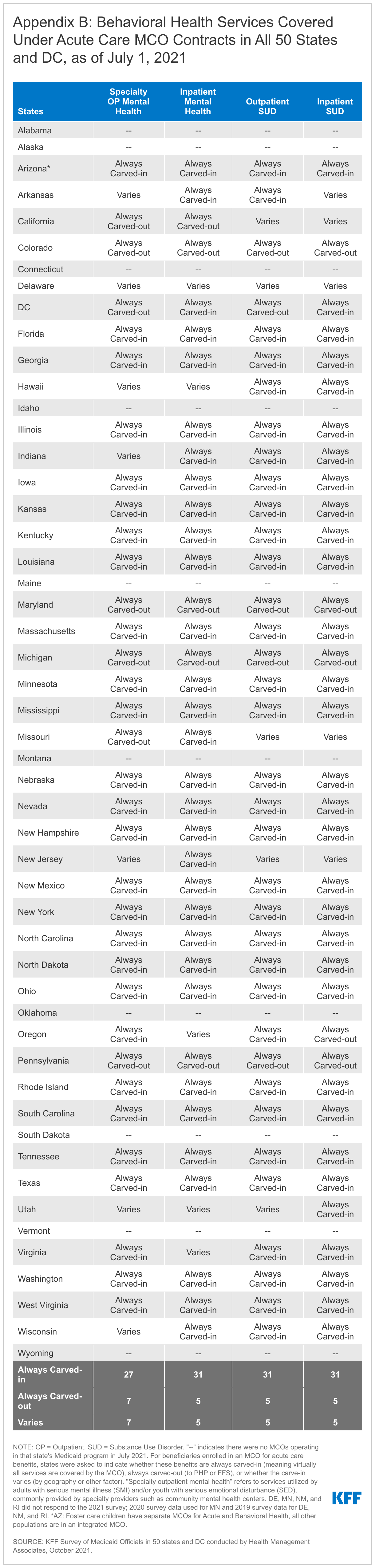
Most states continue to rely on MCOs to deliver inpatient and outpatient behavioral health services (Figure 3 and Appendix B). Although MCOs provide comprehensive services, states may carve specific services out of MCO contracts to FFS or limited benefit prepaid health plans (PHPs). Services frequently carved out include behavioral health, pharmacy, dental, and long-term services and supports (LTSS). However, there has been significant movement across states to carve these services in to MCO contracts. Consistent with results from past years, the majority of MCO states reported that specific behavioral health service types were always carved into their MCO contracts (i.e., virtually all services covered by the MCO); fewer states reported that services were always carved out (to PHP or FFS) or that carve-in status varies by geographic or other factors.9 Also, five states reported targeted carve-outs of behavioral health drugs, such as psychotropic medications, from MCO capitation payments (data not shown).
Eleven states reported making recent changes to how behavioral health benefits are delivered under MCO contracts: three states in FY 2021 only, four states in FY 2022 only, and four states in both FY 2021 and 2022. For example:
- California, through its CalAIM Section 1115 waiver initiative, reported a set of changes to streamline service delivery in both FY 2021 and FY 2022 to improve coordination of mental health care between Medi-Cal MCOs managing non-specialty mental health services and county-operated mental health PHPs managing specialty mental health services and SUD treatment.
- Ohio is implementing a specialized managed care entity—a prepaid inpatient health plan—responsible for providing behavioral health services, with limited exceptions, to youth with complex needs enrolled in both MCOs and FFS in FY 2022.
- West Virginia removed an MCO network requirement in FY 2021 that required MCOs to contract with all SUD providers; MCOs may now make contracting decisions based upon provider quality.
Most states allow MCOs to use “in lieu of” authority to cover certain behavioral health services, particularly to allow coverage of services provided in IMDs. Thirty10 of 37 responding MCO states indicated permitting at least one ILOS as of July 1, 2021; of these, more than three-quarters reported that the permitted ILOS included certain behavioral health services. By far, the most commonly cited ILOS was services provided to nonelderly adults in IMDs, which are otherwise ineligible for Medicaid funding except through in lieu of or waiver authority.11 Some states also mentioned other approved behavioral health services (including mental health and SUD services). Finally, at least two states plan to add behavioral health ILOS in FY 2022.12
Looking Ahead
Across the 2021 budget survey questions discussed in this brief, all responding states reported at least one initiative to expand access to behavioral health care in Medicaid. Some states reported initiatives across many areas, often as part of wide-ranging statewide initiatives identified as top priorities for their Medicaid program—examples include California’s CalAIM initiative, Colorado’s behavioral health care coordination efforts, Massachusetts’ Roadmap for Behavioral Health Reform, Montana’s pending HEART Section 1115 demonstration and parallel service additions, and Washington’s efforts to build an effective community behavioral health system. Further information is needed to understand in more detail how these reported behavioral health initiatives operate and the extent to which states are promoting referrals and treatment or receipt of other benefits following screenings.
Overall, more than one-third of responding states mentioned behavioral health initiatives as a priority for FY 2022 and beyond, and several identified behavioral health services as an upward spending pressure in FY 2022. This trend tracks with the Biden Administration’s identification of behavioral health policy and investments as a key federal Medicaid priority. Continued efforts at the federal level—including the proposed BBBA—may affect the level of enhanced Medicaid funding available to states and their take-up of expanded behavioral health services. For example, additional states may take up the ARPA mobile crisis services option if it becomes permanent under BBBA. The impact of the ARPA enhanced federal Medicaid funding for HCBS (beginning April 2022) on behavioral health HCBS providers also remains to be seen. Additionally, it is unclear how behavioral health service patterns—such as utilization of telehealth—may continue to evolve in the aftermath of the COVID-19 pandemic and whether or how states may modify or adopt new behavioral health initiatives. States also may pursue and CMS under the Biden administration may promote Section 1115 demonstration waivers to expand access to behavioral health care across the care continuum.
This brief draws on work done under contract with Health Management Associates (HMA) consultants Kathleen Gifford, Aimee Lashbrook, Sarah Barth, and Mike Nardone.
Kendal Orgera, Senior Data Analyst at KFF, provided analysis of 2020 National Survey on Drug Use and Health.
Appendices
Appendix A
Background on Behavioral Health Services in Medicaid
Medicaid plays a key role in covering and financing care for people with behavioral health needs. Behavioral health conditions include mental illnesses, such as anxiety disorders, major depression, bipolar disorder, schizophrenia, and post-traumatic stress disorder, as well as SUD, such as opioid use disorder. In 2020, Medicaid covered 23% of nonelderly adults with mental illness, 26% of nonelderly adults with SMI, and 22% of nonelderly adults with SUD. In comparison, Medicaid covered 18% of the general nonelderly adult population. In total, approximately 10.3 million nonelderly adults with Medicaid had a mental illness and over 4.0 million had an SUD in 2020. More than 2.5 million of these adults had both a mental illness and an SUD.13 Medicaid expenditures for enrollees with behavioral health conditions are relatively high due to this group’s substantial health needs.
Most beneficiaries with behavioral health conditions qualify for Medicaid because of their low incomes. Alternatively, people with behavioral health needs, especially those with SMI, may also qualify for Medicaid based on having a disability. Generally, individuals who have a mental illness that makes them eligible for Supplemental Security Income (SSI), the federal cash assistance program for low-income aged, blind, or disabled individuals, are automatically eligible for Medicaid; states may also offer other disability-related Medicaid eligibility pathways to people whose incomes exceed the SSI limit. Finally, though most children with behavioral health diagnoses are eligible through the poverty pathway, some qualify through the child welfare assistance pathway because of their involvement with the foster care system, and others may qualify through a disability-related pathway.
Behavioral health services are not a specifically defined category of Medicaid benefits. Some behavioral health benefits fall under mandatory Medicaid benefit categories: for example, psychiatrist services may be covered under the “physician services” category. States also cover behavioral health benefits through optional benefit categories that they choose to include in their Medicaid programs, such as case management services, prescription drugs, and rehabilitative services. Medicaid MCOs and alternative benefit plans (ABPs)14 that cover behavioral health services must do so at parity, i.e. to the same extent and on the same terms that they cover physical health services. States are encouraged, but not required, to apply the parity rules to their traditional Medicaid FFS programs as well. Behavioral health services for children are particularly comprehensive due to Medicaid’s EPSDT benefit for children, which includes all medically necessary Medicaid services permitted under federal law and is required for children from birth to age 21. Children diagnosed with behavioral health conditions receive any service available under federal Medicaid law necessary to correct or ameliorate the condition, even if the state does not cover the service for adults.
Historically, Medicaid paid for services, including those for behavioral health conditions, on a FFS basis, through which providers are paid for each billable service they deliver. During the past several decades, Medicaid payment has shifted to managed care arrangements, through which providers are paid for some or all services at a prepaid rate. Behavioral health services are increasingly provided through managed care arrangements, but some states “carve out” behavioral health services from their MCO contracts.
Appendix B
Endnotes
- State fiscal years begin on July 1 except for these states: New York on April 1; Texas on September 1; Alabama, Michigan, and District of Columbia on October 1. ↩︎
- “Mental disease” is an antiquated term used in the statute. It comprises “diseases listed as mental disorders in the International Classification of Diseases with the exception of mental retardation [sic], senility, and organic brain syndrome,” including the Diagnostic and Statistical Manual of Mental Disorders, and encompasses alcoholism and other chemical dependency syndromes. CMS State Medicaid Manual § 4309 (D), (E), https://www.cms.gov/Regulations-and-Guidance/guidance/Manuals/Paper-Based-Manuals-Items/CMS021927.html. ↩︎
- KFF analysis of 2020 National Survey on Drug Use and Health (NSDUH). Estimates from the 2020 NSDUH should not be compared to prior years due to methodological changes. ↩︎
- KFF’s 21st annual budget survey surveyed Medicaid officials in all 50 states and DC about certain policies in place in state fiscal year (FY) 2021 and policy changes implemented or planned for FY 2022, which began on July 1, 2021 for most states. State fiscal years begin on July 1 except for these states: New York on April 1; Texas on September 1; Alabama, Michigan, and District of Columbia on October 1. Delaware, Minnesota, New Mexico, and Rhode Island did not respond to the 2021 survey. In some instances, we used publicly available data or prior years’ survey responses to obtain information for these states. ↩︎
- In addition to the SUD benefit expansions counted here, eight states (District of Columbia, Georgia, New Mexico, North Dakota, Oklahoma, Rhode Island, South Carolina, and Tennessee) reported new or expanded medication-assisted treatment (MAT) benefits in FY 2021. Federally required changes, such as coverage of MAT (including all FDA-approved drugs, counseling services, and behavioral therapy) as mandated by the SUPPORT Act, are not counted as positive or negative benefit changes for purposes of the budget survey. Future research may explore state experiences with these federally required MAT benefit expansions. ↩︎
- The eight states are: California, Connecticut, Iowa, Massachusetts, Michigan, Montana, Nevada, and West Virginia. ↩︎
- Section 223 of the Protecting Access to Medicare Act of 2014 established a demonstration program to improve community mental health services by funding planning grants for states to implement CCBHCs. The proposed BBBA would expand this program by providing additional planning grant funding. In addition to setting requirements for CCBHCs, the 2014 Act directed CMS to issue guidance on a prospective payment system for mental health services furnished by CCBHCs to account for the total cost of comprehensive services they provide. The CCBHC demonstration aims to improve the availability and quality of ambulatory behavioral health services and to provide coordinated care across behavioral and physical health. CCBHCs provide nine types of services: crisis mental health services; screening, assessment, and diagnosis; patient-centered treatment planning; outpatient mental health and substance use services; outpatient clinic primary care screening and monitoring; targeted case management; psychiatric rehabilitation; peer support and counselor services and family supports; and intensive, community-based mental health care for members of the armed forces and veterans. CCBHCs may partner with designated collaborating organizations to provide some of these services. ↩︎
- 42 CFR § 438.3 (e)(2)(iv). ↩︎
- There may be small population enrollment variations to the classifications of “always carved-in” and “always carved-out.” For example: North Carolina launched its “Standard” acute managed care program July 1, 2021 with most mental health services carved in, with an exception to mandatory enrollment for individuals with SMI or SED for specialty outpatient mental health services. Missouri carves out inpatient mental health services for the foster care population, while these services are carved in for all other managed care populations. ↩︎
- Three of the 30 states answering “yes” did not provide examples of approved in lieu of services (Arkansas, Utah, and Virginia) and Maryland answered “yes” but noted that no in lieu of services were currently defined. ↩︎
- The 2016 Medicaid Managed Care Final Rule allows states, under the authority for health plans to cover services “in lieu of” those available under the Medicaid state plan, to receive federal matching funds for capitation payments on behalf of nonelderly adults who receive inpatient psychiatric or SUD treatment or crisis residential services in an IMD for no more than 15 days during a given month. KFF’s 2019 budget survey explicitly asked states to indicate if using Medicaid managed care ILOS for enrollees receiving inpatient treatment in an IMD as detailed in the 2016 final rule; 35 of 41 MCO states reported using this authority in FY 2019 and/or FY 2020 (see Table 9). ↩︎
- For example, Texas reported working with CMS and stakeholders to institute several additional behavioral health ILOS. California reported that while it does not permit MCOs to cover ILOS as of July 1, 2021, starting January 1, 2022, it would authorize a new menu of ILOS as part of its CalAIM initiative, including sobering centers. ↩︎
- KFF analysis of 2020 National Survey on Drug Use and Health (NSDUH). Estimates from the 2020 NSDUH should not be compared to prior years due to methodological changes. ↩︎
- States must offer ABPs to individuals newly eligible under the Affordable Care Act (ACA) Medicaid expansion and may choose to offer ABPs to most other Medicaid adults as well. ↩︎