Note: This fact sheet largely reflects activities prior to the second Trump administration, which has issued numerous executive actions that directly affect global health efforts, and has been updated to highlight key recent actions that may affect PMI and other U.S. global malaria efforts. See also the KFF fact sheet on the Trump administration’s foreign aid review and the status of PMI.
Key Facts
- About half of the world’s population is at risk of being infected with malaria. In 2023, there were an estimated 263 million cases of malaria and 597,000 deaths from malaria worldwide. Sub-Saharan Africa is the hardest hit region in the world.
- While gains have been made over the past two decades in increasing access to malaria prevention and treatment, many challenges (including drug and insecticide resistance and climate change impacts) continue to complicate malaria control efforts in hard-hit areas. Recently, in promising developments, the first malaria vaccine was recommended in 2021 by the World Health Organization (WHO) for widespread use in children, and its broader rollout began in 2023. Additionally, in late 2023, WHO recommended a second malaria vaccine. These vaccines are now being rolled-out across Africa in routine childhood immunization programs.
- The U.S. government (U.S.) has been involved in global malaria activities since the 1950s and, today, is the largest donor government to global malaria efforts.
- U.S. malaria efforts include activities primarily through the U.S. President’s Malaria Initiative (PMI) that is overseen by the U.S. Global Malaria Coordinator, as well as through other U.S. activities; collectively, the U.S. reaches approximately 30 countries.
- U.S. funding for malaria control efforts and research activities was approximately $1 billion in FY 2025, up from $873 million in FY 2016. Additionally, the U.S. is the largest donor to the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), which in turn is the largest overall funder of malaria efforts in the world.
- As the Trump administration reorganizes foreign assistance (and Congress considers whether to approve these changes), including dissolving the U.S. Agency for International Development (USAID) – the lead implementer of PMI, its impact on the future of U.S. global malaria efforts remains to be seen.
Global Situation1
Malaria is one of the world’s most common and serious tropical diseases, with about half the world’s population at risk of being infected with malaria. Although preventable and treatable, malaria causes significant morbidity and mortality, with the greatest numbers of cases and deaths in resource-poor regions and among young children.2
Malaria: an infectious disease caused by certain Plasmodium parasites, which are transmitted to humans by Anopheles mosquitoes. This mosquito thrives in warm, tropical, and subtropical climates. Infection with malaria parasites can cause common symptoms like fever, chills, and flu-like illness and lead to anemia, causing severe malaria disease and sometimes death. When the infected parasites clog small blood vessels in the brain, causing cerebral malaria, it can also be fatal.3
Strategies and efforts to address malaria have evolved over time, with global eradication efforts waning in the 1970s, resulting in rising rates.4 In the late 1990s, malaria began to receive renewed attention, particularly after the 1998 creation of the Roll Back Malaria Partnership (RBM), now referred to as the RBM Partnership to End Malaria.5 In 2000, all nations agreed to global malaria targets as part of Millennium Development Goal 6 (combat HIV/AIDS, malaria, and other diseases). Since then, expanded efforts by the U.S. government, other donor governments, multilateral institutions, and affected countries have helped to increase access to malaria prevention and treatment and reduce cases and deaths, and there has been, at times, discussion of the possibility of finally eradicating the disease.6
Today global malaria activities are focused on sustaining, improving, and expanding efforts to control the disease. Still, the rate of progress has stalled in some countries recently, and many challenges continue to complicate malaria control efforts in countries with ongoing malaria transmission, including poverty, poor sanitation, weak health systems, limited disease surveillance capabilities, natural disasters, armed conflict, migration, climate change, and the presence of counterfeit and/or sub-standard antimalarial drugs.7
Morbidity and Mortality8
- WHO estimates that there were approximately 263 million cases of malaria and 597,000 deaths, mostly among children under the age of five, in 2023. Overall, substantial scale-up of malaria interventions helped reduce the malaria case incidence and death rates over the past two decades, though case incident rates were slightly higher in 2023 than in 2022 due to increased rates in some countries.
- Multidrug-resistant malaria is a widespread and recurring problem, and while highly-effective artemisinin-based combination therapies (ACTs) have been introduced to treat drug-resistant strains, evidence suggests ACT resistance is occurring in parts of Asia and Africa.9 Resistance to insecticides has emerged as a problem in Africa, the Americas, Eastern Mediterranean, South-East Asia, and the Western Pacific.10
- Certain groups, particularly pregnant women and children, are more vulnerable. Making up 76% of all malaria deaths in the Africa region, children under five are especially at-risk of malaria infection, because they lack developed immune systems to protect against the disease. Other high-risk groups include people living with HIV/AIDS, travelers, refugees, displaced persons, and migrant workers entering endemic areas.
Interventions
Malaria control efforts involve a combination of prevention and treatment strategies and tools, such as:
- insecticide-treated bed nets (ITNs),11
- indoor residual spraying (IRS) with insecticides,
- diagnosis and treatment with antimalarial drugs, particularly artemisinin-based combination therapies (ACTs),12
- intermittent preventive treatment in pregnancy (IPTp, a drug treatment for pregnant women that prevents complications from malaria for a woman and her unborn child),
- perennial malaria chemoprevention (PMC, formerly called intermittent preventive treatment in infants (IPTi), a drug treatment aimed at reducing adverse effects of malaria in children belonging to age groups at high risk of severe malaria), and
- seasonal malaria chemoprevention (SMC, a treatment course administered at monthly intervals to children belonging to age groups at high risk of severe malaria during the high malaria transmission season).
More recently, in 2021, WHO recommended, and in 2022 prequalified, the first malaria vaccine (RTS,S/AS01 or RTS,S) and in 2023 recommended and prequalified a second malaria vaccine (R21/Matrix-M or R21), both of which have been shown to be safe and effective in preventing malaria in children during clinical trials.13 As of December 2024, 17 countries that represent approximately 70% of the global malaria burden offered these vaccines through routine childhood immunization programs, and more are planning to introduce or scale them up.14 Roll-out of these vaccines will depend on financing and country decisions about whether to adopt the vaccines as part of their national malaria control strategies, among other things.
Access to prevention and treatment services has grown over time, as ITN coverage has increased and the number of ACT treatments procured by the public and private sectors has expanded substantially.15
Global Goals
Since the late 1990s, new initiatives and financing mechanisms have helped increase attention to malaria and contributed to efforts to achieve global goals; these include the RBM Partnership to End Malaria, a global framework established in 1998 for coordinating malaria efforts among donor governments, major UN agencies, international organizations, and affected countries, among others; and the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), an independent, international financing institution established in 2001 that provides grants to countries to address TB, HIV, and malaria (see the KFF fact sheet on the U.S. and the Global Fund).16
These and other efforts work toward achieving major global malaria goals that have been set through:
- Sustainable Development Goals (SDGs). Adopted in 2015, the SDGs aim to end the malaria epidemic by 2030 under SDG Goal 3, which is to “ensure healthy lives and promote well-being for all at all ages.”17
- Global Technical Strategy for Malaria (GTS). Developed in close alignment with the RBM Partnership and adopted by the World Health Assembly in 2015, the GTS includes the goals of reducing malaria incidence and mortality rates by at least 90% by 2030, eliminating the disease in at least 35 new countries, and preventing the disease’s re-establishment in countries that are malaria free.
With these goals, the GTS sets out a vision for countries to accelerate progress towards malaria elimination, and globally, more countries are moving towards elimination. Since 2000, 26 countries (Algeria, Argentina, Armenia, Azerbaijan, Belize, Cabo Verde, China, Egypt, El Salvador, Georgia, Iran, Iraq, Kazakhstan, Kyrgyzstan, Malaysia, Maldives, Morocco, Oman, Paraguay, Sri Lanka, Syrian Arab Republic, Tajikistan, Turkey, Turkmenistan, United Arab Emirates, and Uzbekistan) have attained three consecutive years of zero indigenous malaria cases and are therefore recognized as having eliminated the disease.18 In 2023, of 83 malaria-endemic countries, 47 countries worldwide were reported to have been nearing elimination.19 Most recently, in March 2024, WHO along with Ministers of Health in Africa and other partners convened a Malaria Ministerial Conference and signed a declaration committing to accelerating action to end deaths from malaria.20
The U.S. Government
Involved in global malaria activities since the 1950s, the U.S. government (U.S.) is the largest government donor to malaria efforts.21 It is also the largest donor to the Global Fund, which in turn is the largest overall funder of malaria efforts in the world.22
History
The U.S. government’s international response to malaria began in the 1950s through activities at the U.S. Centers for Disease Control and Prevention (CDC) and U.S. Agency for International Development (USAID); early efforts focused on technical assistance but also included some direct financial support for programs overseas.
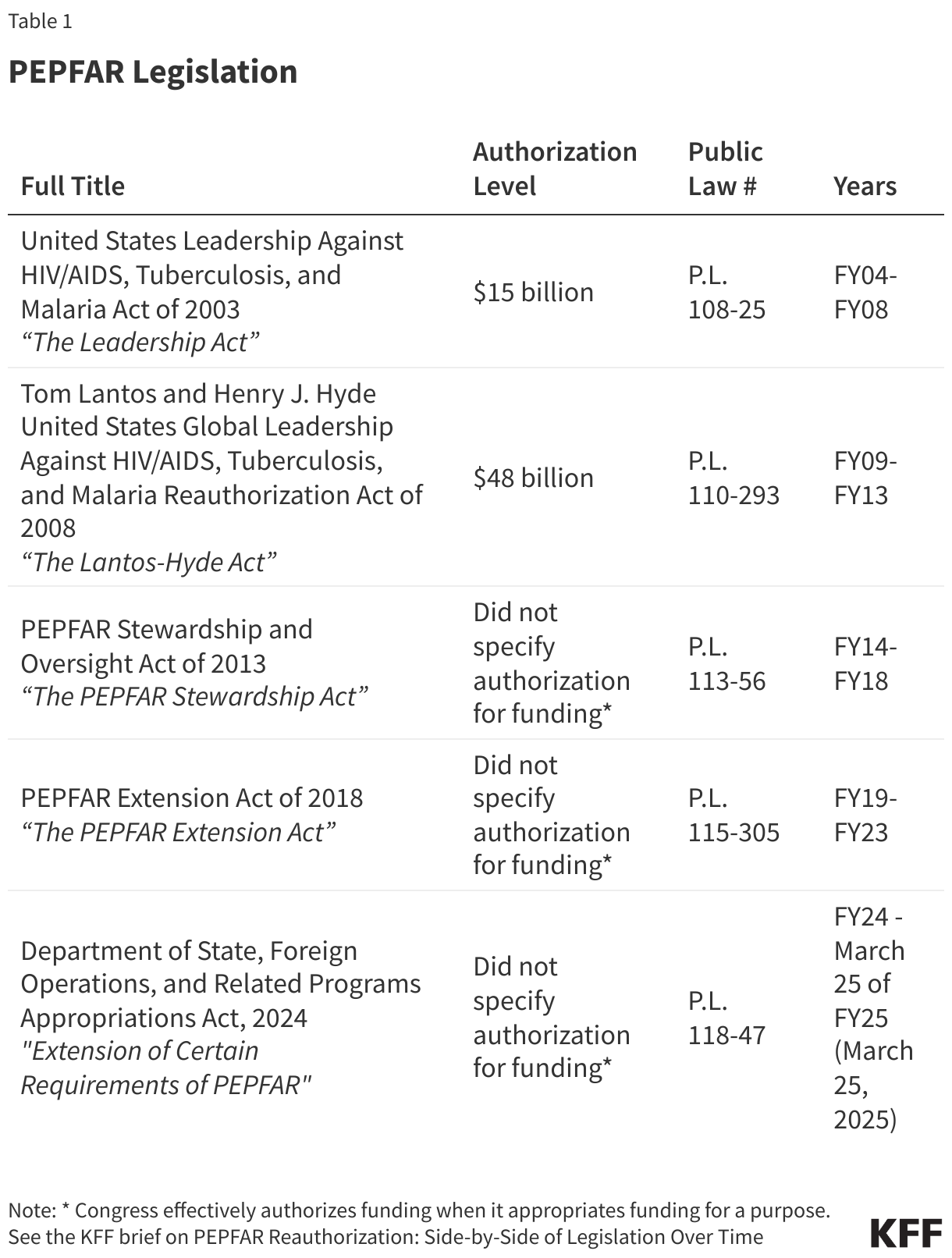
Since the early 2000s, the U.S. has assigned a heightened priority to and provided greater funding for bilateral and multilateral malaria efforts. In 2003, the U.S. Leadership Against HIV/AIDS, Tuberculosis, and Malaria Act of 2003 (the legislation that created PEPFAR, the expanded U.S. government response to global AIDS) authorized five years of funding for bilateral malaria efforts and the Global Fund. In 2005, the U.S. launched the President’s Malaria Initiative (PMI), a five-year effort to address malaria in 15 hard-hit African countries, which has since been extended and expanded. In 2008, the Lantos-Hyde U.S. Global Leadership Against HIV/AIDS, Tuberculosis, and Malaria Reauthorization Act of 2008 (which reauthorized PEPFAR) authorized another five years of funding and codified the position of the U.S. Global Malaria Coordinator.23 More recently, in 2021, the U.S. released its PMI strategy for 2021-2026, which outlines its goals as well as its approach to achieving them by 2026.24 (See the KFF fact sheet on PEPFAR, the KFF fact sheet on the Global Fund, the KFF brief on PEPFAR reauthorization legislation, and the KFF dashboard monitoring progress toward global malaria targets in PMI countries.)
Organization and Goals
President’s Malaria Initiative (PMI)25
Launched in 2005, the President’s Malaria Initiative (PMI) is an interagency initiative to address global malaria that was, until its recent dissolution, led by USAID and implemented in partnership with CDC. It is overseen by the U.S. Global Malaria Coordinator, who is appointed by the President and reports to the USAID Administrator, and an Interagency Advisory Group made up of representatives from USAID, CDC, the National Institutes of Health (NIH), the Department of Defense (DoD), the State Department, the Peace Corps, the National Security Council, and other U.S. government agencies.26 USAID has served as the lead implementing agency for U.S. global malaria efforts, primarily through PMI, with other agencies also carrying out malaria activities. Collectively, prior to the second Trump administration, U.S. bilateral activities reached approximately 30 countries.27 Now, as the Trump administration reorganizes foreign assistance (and Congress considers whether to approve these changes), having dissolved USAID, it is unclear whether it will integrate any remaining USAID global health activities, including PMI, into the State Department, and what the future holds for PMI. See the KFF fact sheet on the status of malaria efforts.
Goals
In 2021, the U.S. released the President’s Malaria Initiative Strategy 2021-2026; its goals include:
- reducing malaria mortality by one-third from 2015 levels in high-burden PMI-supported countries, 28
- achieving a greater than 80% reduction from PMI’s original 2000 baseline levels,
- reducing malaria morbidity in PMI-supported countries with high and moderate malaria burden by 40% from 2015 levels,29 and
- assisting at least ten PMI-supported countries to meet the WHO criteria for national or sub-national elimination and at least one country in the Greater Mekong subregion to reach national elimination.
The strategy also states that these efforts contribute to longer term goals, such as elimination of malaria in a growing number of countries, and aligns with global priorities.30
Key Activities31
Prior to the current administration, PMI activities focused on expanding access to and the use of six key malaria control interventions: insecticide-treated bed nets (ITNs), indoor residual spraying (IRS) with insecticides, entomological monitoring, intermittent preventive treatment in pregnancy (IPTp),32 diagnosis of malaria and treatment with artemisinin-based combination therapies (ACTs), and seasonal malaria chemoprevention (SMC).33
They also included a range of malaria control activities, including technical assistance to affected countries, monitoring and evaluation, supply chain management, and commodity procurement (since the start of PMI, U.S. support for commodities, such as ITNs, insecticides, and antimalarial drugs, like ACTs, has increased significantly34 ). Additionally, PMI supported activities in the following areas: behavior change communication, health systems strengthening, monitoring and evaluation, operational research, elimination, and community health.35
USAID had also supported regional efforts in Latin America and the Caribbean, including providing technical assistance to support countries in tailoring their approaches for malaria control through its Amazon Malaria Initiative.36 CDC provided technical assistance to these regional efforts and was also designated as the WHO Collaborating Center for Prevention and Control of Malaria,37 though with the Trump administration’s announcement that the U.S. would withdraw from WHO, the future of this partnership remains an open question. It also remains to be seen how recent announcements of global health reductions at CDC could further affect malaria efforts.
Additionally, NIH and DoD have been involved in malaria research and development (R&D). NIH is the lead agency for U.S. malaria R&D efforts (including its International Centers of Excellence for Malaria Research program, which established a global network of malaria research centers in 2010 to support research activities in malaria-endemic countries).38 DoD also supports extensive R&D efforts as well as worldwide malaria disease surveillance, and technical assistance and capacity building with local partners.39 The future of U.S. support for these efforts is uncertain as the Trump administration reduces and eliminates foreign research grants.
Countries Reached
Prior to the current administration, PMI spanned 27 sub-Saharan African “focus countries” (gradually scaled up from three countries in FY 2006), as well as three countries in Southeast Asia under the PMI Greater Mekong Subregion regional initiative.40 Focus countries were selected based on the following criteria:41
- high malaria burden,
- alignment of National Malaria Control Plan (NMCP) with WHO standards,
- country capacity to implement national control policies,
- willingness to partner with the US in fighting malaria, and
- involvement of other international donors (e.g., Global Fund; World Bank).
Both USAID and CDC stationed staff in each PMI focus country, though USAID staff are or have been recalled to the U.S. due to the Trump administration’s dissolution of USAID and reorganization of foreign assistance.
Beyond PMI, the Amazon Malaria Initiative spanned several countries in Latin America and the Caribbean, and other U.S. activities may reach more countries. For example, CDC and USAID have carried out activities in additional countries in sub-Saharan Africa, the Caribbean, and Asia.42
Multilateral Efforts
The U.S. partners with international institutions and supports global malaria funding mechanisms. Key partners include the World Health Organization (although the second Trump administration immediately announced the U.S. would withdraw as a member of and halt funding to WHO), the RBM Partnership, and the World Bank. Additionally, the U.S. government is the largest donor to the Global Fund, which has approved over $22 billion in funding for malaria programs worldwide and is the largest overall funder of global malaria efforts.43
Funding44
U.S. funding for malaria, which is specified by Congress in annual appropriations bills and includes support for PMI as well as other malaria control efforts and research activities, has increased over the past decade from $873 million in FY 2016 to approximately $1 billion in FY 2025; while funding increased over the period, it has been relatively flat in recent years (see figure for the latest information). Additional U.S. support for malaria activities is provided through its contribution to the Global Fund. (See the KFF fact sheet on the U.S. Global Health Budget: Malaria/PMI and the KFF budget tracker for more details on historical appropriations for U.S. global malaria efforts.)
Most U.S. bilateral funding for malaria has been provided through the Global Health Programs account at USAID with additional funding provided through NIH, CDC, and DoD. The majority of U.S. malaria funding has been directed to PMI focus countries, with additional funding directed to other bilateral and regional malaria efforts as well as malaria research activities.