VOLUME 23
New Vaccine Requirements, Anti-mRNA Narratives, and Disputed Gender-Affirming Care Report
Summary
This volume highlights how new vaccine requirements and the spread of anti-mRNA sentiments are fueling confusion and distrust. It also examines reactions to a federal report on gender-affirming care for minors and investigates how TikTok is being used to promote false health claims through deepfake personas targeting young women.
Recent Developments
HHS’ New Placebo Requirements for Vaccine Approval Prompt Confusion About Existing Procedures

The Department of Health and Human Services (HHS) announced that it will require all new vaccines to undergo placebo-controlled trials before approval, framing this as a shift from existing practices. A placebo-controlled trial is a study that compares participants who receive an experimental vaccine to a control group that receives a placebo—an inert substance—to help isolate the effects of the vaccine from other factors. While many vaccines, including COVID-19 vaccines, were tested this way, the American Medical Association (AMA) and the World Health Organization (WHO) do not consider placebos ethical when withholding a known effective vaccine could expose participants to unnecessary risk. In such cases, researchers use other rigorous methods, such as comparing a new vaccine to an approved one to evaluate differences in safety, immune response, and effectiveness. The HHS announcement has led to questions about the safety of existing vaccines among those unfamiliar with how clinical trials are designed and why placebo use is not always appropriate.
Online discussion about placebo-controlled trials spiked on May 1 and May 4, following news reports of HHS’ new policy. Some posts with large engagement argued that placebo-controlled trials should not be used when a vaccine is known to be protective, aligning with the AMA and WHO. Others misleadingly presented the policy change as evidence that past vaccine trials lacked proper oversight or were “corrupt.” A widely shared post from a medical doctor and lawyer with over 900,000 followers called the update long overdue and said it would finally hold vaccine makers to higher safety standards. Others expressed genuine confusion about study designs by expressing a lack of knowledge about how often placebo groups are used in clinical trials.
Polling Insights:
As regulatory guidelines surrounding vaccines change, KFF’s latest Tracking Poll on Health Information and Trust finds that fewer than half the public say they currently have at least “some” confidence in federal government health agencies to ensure the safety and effectiveness of vaccines approved for use in the U.S. While half or fewer across partisans express confidence, Democrats are somewhat more likely than independents and Republicans to say they have “a lot” or “some” confidence in federal health agencies to ensure vaccines are safe and effective.

Changing COVID-19 Booster Testing Standards Add to Uncertainty Around Safety
Social media conversations have also reflected concern and skepticism about COVID-19 boosters after HHS officials stated that these boosters may be held to stricter evidence requirements that could treat them as entirely new products. This framing has led to confusion about what qualifies as a “new vaccine,” particularly in contrast to updated COVID-19 boosters. While a new vaccine may target either a novel or existing pathogen using new technology or formulations, COVID-19 boosters are updates to previously approved vaccines designed to target evolving strains of the same virus. Unlike brand-new vaccines, which undergo extensive clinical trials, updated COVID-19 boosters were previously approved using existing safety data from the original vaccine, along with lab and animal studies showing that the updated shot produces a strong immune response to new variants. Experts warn that the shift could delay access to boosters as new strains of viruses spread, while weakening trust in long-standing safety procedures.
Confusion about boosters began to grow after the FDA questioned data around boosters and delayed full approval of Novavax’s updated COVID-19 vaccine, calling it a new product and requesting additional trial data. Novavax, a protein-based alternative to mRNA vaccines, has been authorized for emergency use since 2022 after a large placebo-controlled trial showed high efficacy and few serious adverse effects. The updated version targets newer variants and functions as a booster for individuals who have previously been vaccinated. Prior to the FDA’s decision to apply new product standards for all COVID-19 boosters for people under 65, some high-profile social media accounts reacted to the Novavax delay with concern about boosters. One X account with approximately 3.7 million followers called for the COVID-19 vaccines to be banned, calling them “worthless” and “dangerous.” Another post, from a physician with one million followers, falsely claimed that new variants are invented to justify continued booster campaigns.
mRNA Vaccine Concerns Gain Political Traction Despite Scientific Consensus

Misleading information about mRNA vaccines continues to circulate online, contributing to support for policy proposals that aim to ban the technology. Extensive research and real-world data show that mRNA vaccines have a strong safety profile and offer protection against severe illness, hospitalization, and death from infectious diseases, like COVID-19, and potentially cancer. But a group of legislators in Minnesota recently introduced a bill that would classify mRNA vaccines as “weapons of mass destruction,” with criminal penalties of up to 20 years in prison. Although unlikely to pass, the bill represents the growing reach of concern about mRNA technology. Similar measures have emerged in other states: Iowa, Montana and Idaho have considered proposals that would impose criminal penalties on providers.
Social media conversations continue to reflect unsubstantiated concern about mRNA vaccines, sometimes showing support for legislation aiming to ban them. One Texas doctor with over 500,000 followers, previously suspended for sharing false information about vaccines, said that Minnesota legislators were “lead[ing] the way” with the proposal. Another widely shared post featured a video of a doctor with a revoked medical license recommending that viewers and their families “not get vaccinated, ever again, with an mRNA vaccine.” These conflict with the broad scientific consensus supporting mRNA vaccines and contribute to doubt about COVID-19 vaccines. According to the FDA, serious adverse effects from the COVID-19 vaccines—which are predominantly mRNA-based in the United States—occur in fewer than 1 in 200,000 vaccinated individuals, and research has shown that COVID-19 vaccines have saved tens of millions of lives globally.
Polling Insights:
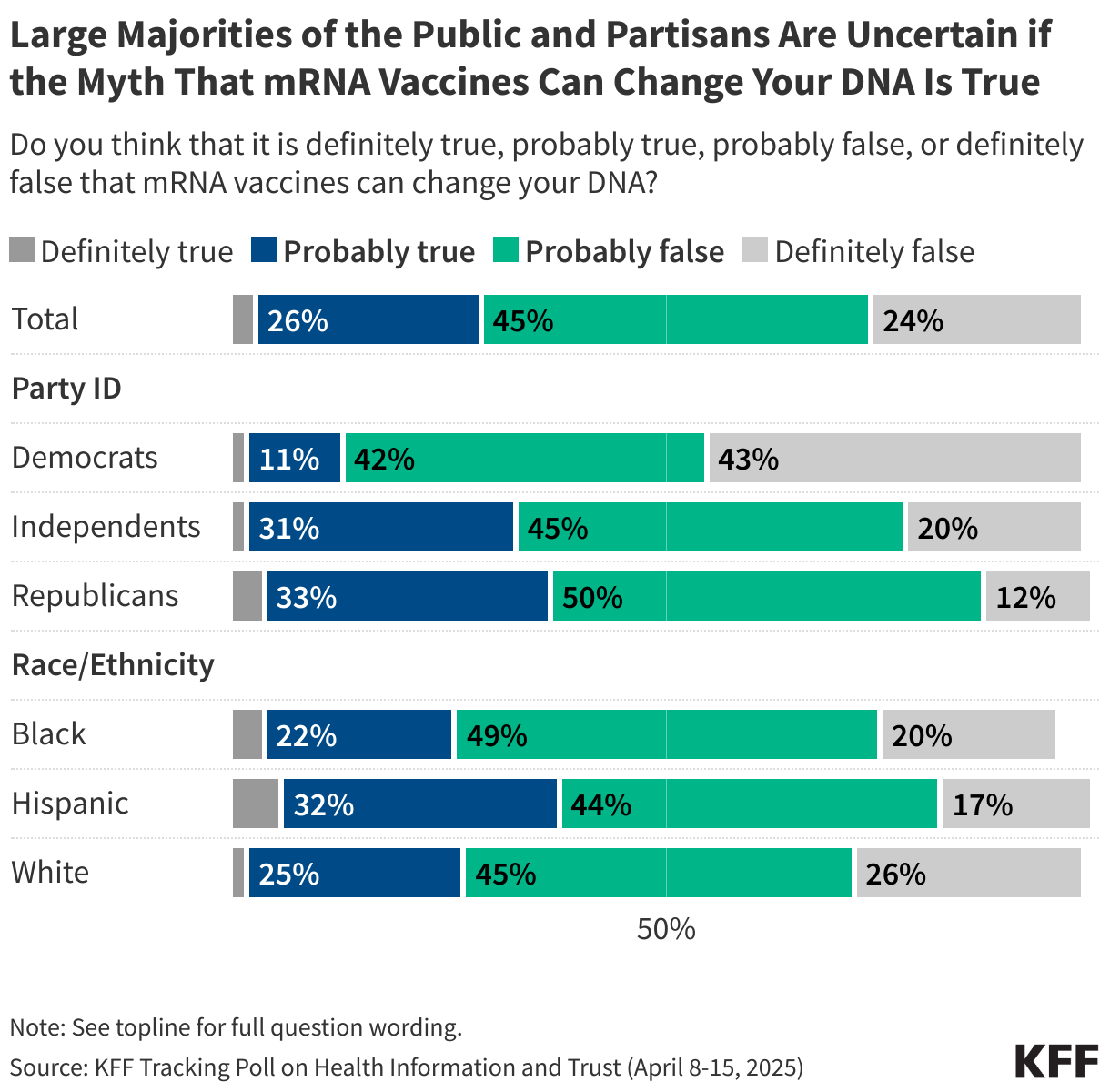
New KFF polling shows that mRNA technology is obscure to much of the public. About twice as many adults think vaccines that use mRNA technology are “generally safe” (32%) as say they are “generally unsafe” (16%), but about half (52%) report not knowing enough about this technology to say. In addition, nearly half of the public (45%) report having heard the false claim that mRNA vaccines can alter a person’s DNA — a myth related to COVID-19 vaccines that began circulating early in the pandemic. While just 3% think this false claim is “definitely true” and one quarter say it is “definitely false” (24%), most fall in the malleable middle, saying it is either “probably true” (26%) or “probably false” (45%). However, there are important differences by party identification and ethnicity when it comes to believing or leaning toward believing the myth that mRNA vaccines alter DNA, with at least one-third of Republicans (37%), independents (33%), and Hispanic adults (38%) saying the claim is either “definitely true” or “probably true.”
Reactions to HHS Report Amplifies Misleading Narratives About Health Care for Transgender Youth

Misleading narratives about gender-affirming care for transgender and nonbinary people are circulating following the May 1 release of a new HHS report about gender dysphoria. The 400-page report, commissioned by an executive order aimed at limiting youth access to gender-affirming care, states that it surveys existing literature on gender-affirming interventions for children and adolescents, concluding that “the evidence for benefit of pediatric medical transition is uncertain, while the evidence for harm is less uncertain.” Major medical groups, including the American Academy of Pediatrics and the American Psychological Association, criticized the report and continue to support access to transition-related care based on other reviews and studies that have found a positive impact of gender-affirming care on health. On the day the report was released, mentions of gender-affirming care spiked on social media. Some high-profile accounts, including a podcast host with almost five million followers, circulated quotes from the report’s foreword that highlighted potential risks associated with gender-affirming care while emphasizing uncertainty about the benefits.
The report spurred other incorrect claims, including the false notion that surgical interventions are common among minors, but such procedures are exceedingly rare. One study that looked at data from more than 22 million minors found that less than .01% of transgender and gender diverse minors ages 13 to 17 underwent gender-affirming surgery, and none under 12 received such care. The HHS report’s framing of “exploratory therapy,” a practice that can include gender identity conversion efforts, drew attention online, but a recent KFF brief explains that major health associations have condemned this therapy as harmful and unsupported by evidence. Social media posts also amplified claims that many youth regret care, but research shows regret is uncommon. While not all transgender people seek medical care, a 2021 meta-analysis found that among those who do, the prevalence of regret is 1%. The report further claimed that many transgender or nonbinary people seek to “detransition” (return to their sex assigned at birth). But studies show that most transgender and nonbinary people do not return to their sex assigned at birth, and the KFF/Washington Post Trans Survey found that about eight in ten trans adults (78%) report being more satisfied with their lives after transitioning.
AI & Emerging Technology
Deepfake Health Scams Target Young Women on TikTok

A March investigation by Media Matters, also reported by Rolling Stone, uncovered a network of TikTok accounts using deepfake personas to push health and wellness products, often targeting women with fertility or cosmetic concerns. The accounts created backstories and personal testimonies to enhance credibility and drive sales through TikTok Shop links. One account, for example, featured videos of an influencer claiming various identities, such as a doctor and former model, to endorse hair growth supplements. A reverse image search, though, showed that the woman was likely generated by deepfake technology. Following publication of the investigation, the accounts identified in the article were removed from TikTok. This tactic reflects a broader trend identified in a 2024 study published in Journal of Medical Internet Research, which concluded that the alternative health community on TikTok is more likely to use emotional storytelling to build trust than conventional health videos, a strategy that these deepfake personas are designed to mimic.
A 2024 KFF poll found that most TikTok users report seeing health-related content on the app, and among these users women are more likely than men to say they’ve seen information or advice about mental health (71% v. 61%) or birth control (41% v. 25%) on the app. In addition, about half of women of reproductive age – those ages 18 to 49 – report seeing information or advice on TikTok about prescription birth control (54%) or abortion (48%). While fewer than half (40%) of TikTok users say they trust information about health issues that they see on the app at least “somewhat,” this rises to half among women ages 18-49. Notably, younger adults and women are more likely than older adults and men, respectively, to say they use TikTok every day.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.

The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Sign up to receive KFF Monitor
email updates
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The Public Good Projects (PGP) provides media monitoring data KFF uses in producing the Monitor.