10 Things to Know About U.S. Funding for Global Health
Note: This resource does not reflect recent changes that have been implemented by the Trump administration, including a foreign aid review and restructuring. For more information, see KFF’s Overview of President Trump’s Executive Actions on Global Health. This resource was originally published on February 4, 2025, and will be updated as needed to reflect additional developments.
Introduction
U.S. engagement in global health is multifaceted and includes a broad range of activities, one of which is financially supporting health efforts worldwide. As the largest donor to global health in the world, the U.S. supports bilateral efforts, directly funding implementation of global health activities in partner countries, and multilateral health institutions (i.e., international organizations that pool support from multiple donors for one or more areas of global health). Here are 10 things to know about U.S. funding for global health:
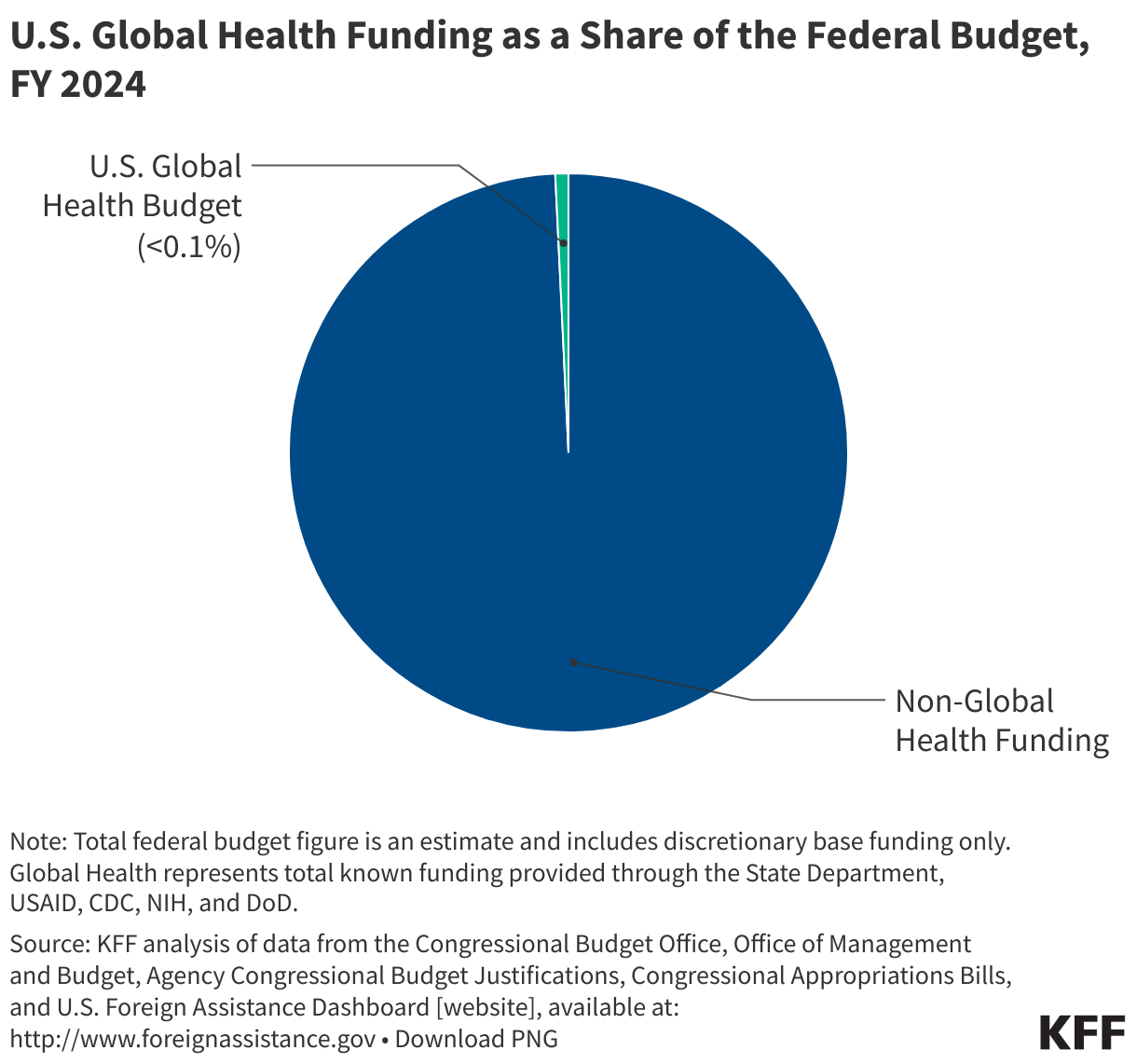
1. U.S. global health funding totals approximately $12 billion but only represents less than 1% of the federal budget.
U.S. global health funding, most of which is part of the broader U.S. foreign aid budget that includes funding for development, economic, and humanitarian assistance programs, totaled $12.4 billion (through regular appropriations) in FY 2025 but accounted for less than 1% of the federal budget, which totaled approximately $1.6 trillion (see Figure 1). In some years, on top of regular appropriations, global health funding is also provided through emergency supplemental funding to address disease outbreaks, but this funding generally makes up a small piece of the federal budget pie.
Figure 1
2. U.S. funding for global health is complex!
Funding supports multiple program areas at several agencies and departments for both bilateral and multilateral efforts and is provided both annually and in emergency situations.
Program Areas
The U.S. government supports global health efforts aimed at addressing numerous areas, funding programs to address HIV (through PEPFAR, the President’s Emergency Plan for AIDS Relief), tuberculosis (TB), malaria (through PMI, the President’s Malaria Initiative), maternal and child health (MCH), nutrition, family planning and reproductive health (FP/RH), neglected tropical disease (NTDs), global health security, as well as the vulnerable children program and other public health threats, which include programs for cross-cutting health activities like the Health Reserve Fund and the global health workforce through the Global Health Workforce Initiative (see more detail on program areas below).
Agencies/Departments
The U.S. supports these efforts via several agencies, departments, and accounts. Agencies and departments that receive funding for global health include the U.S. Department of State (State), U.S. Agency for International Development (USAID), Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH), and the Department of Defense (DoD). In addition, funding is provided through several accounts at State and USAID including: the Global Health Programs (GHP) account at State and USAID, Contributions to International Organizations (CIO) and International Organizations and Programs (IO&P) accounts at State, and the Assistance for Europe, Eurasia and Central Asia (AEECA), Development Assistance (DA), Economic Support Fund (ESF) and International Disaster Assistance (IDA) accounts at USAID (see more detail on agencies, departments, and accounts below).
Bilateral and Multilateral Funding
Funding is provided bilaterally, directly supporting the implementation of global health activities in almost 80 partner countries that span six regions across the globe (see more detail on bilateral efforts below), and multilaterally, providing support to international organizations that pool funding from multiple donors for one or more areas of global health. Multilateral health institutions the U.S. supports through financial contributions include the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), Gavi the Vaccine Alliance (Gavi), United Nations Children’s Fund (UNICEF), World Health Organization (WHO), Pan American Health Organization (PAHO), Joint United Nations Programme on HIV/AIDS (UNAIDS), United Nations Population Fund (UNFPA), TB Drug Global Drug Facility, and the Pandemic Fund (see more detail on these multilateral health efforts below).
Regular Annual and Emergency Supplemental Appropriations
Finally, U.S. funding for global health is comprised of funding provided through the regular appropriations process, which takes place annually (see more detail on the federal budget process below), and through emergency supplemental funding for disease outbreaks, which often takes place during public health emergencies.
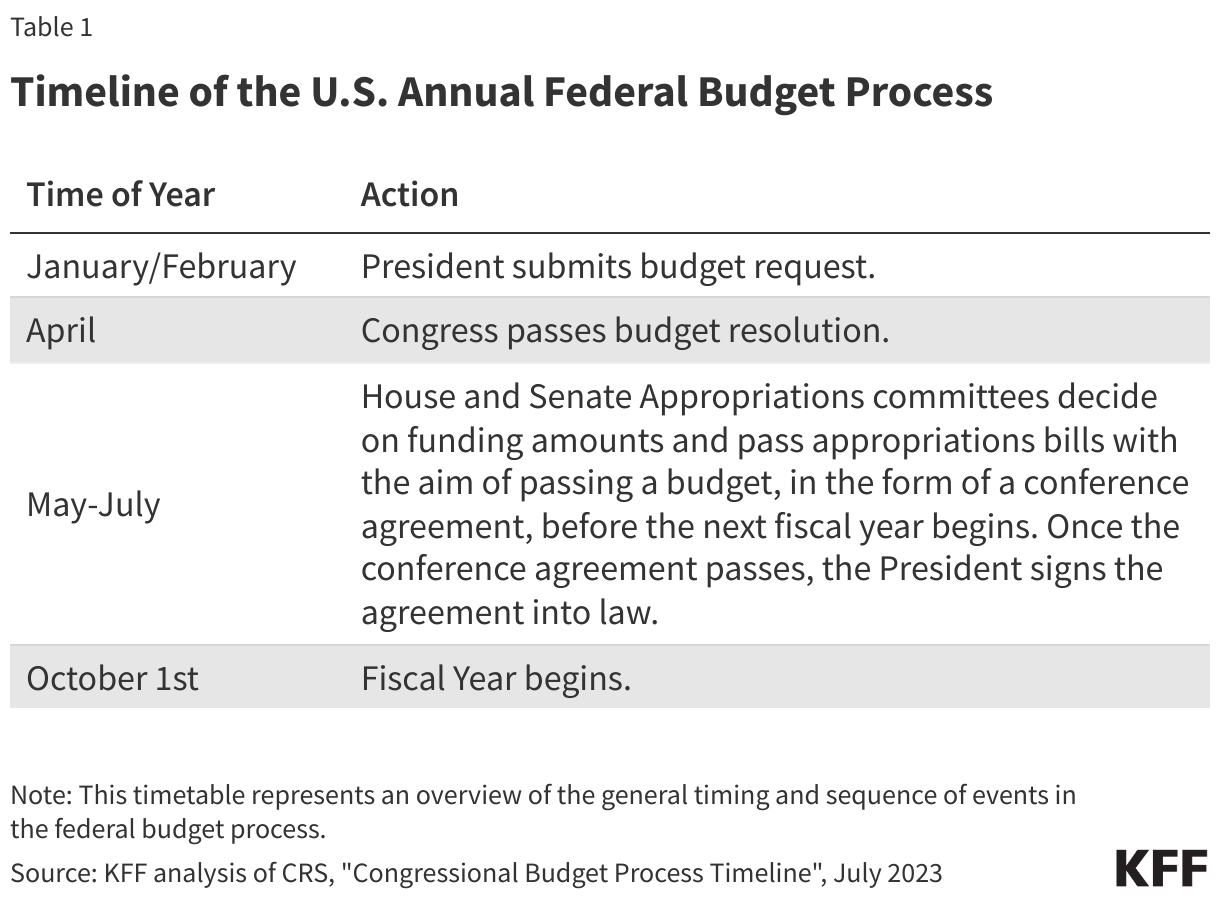
3. U.S. global health funding is determined annually through a multi-step process that involves the President and Congress.
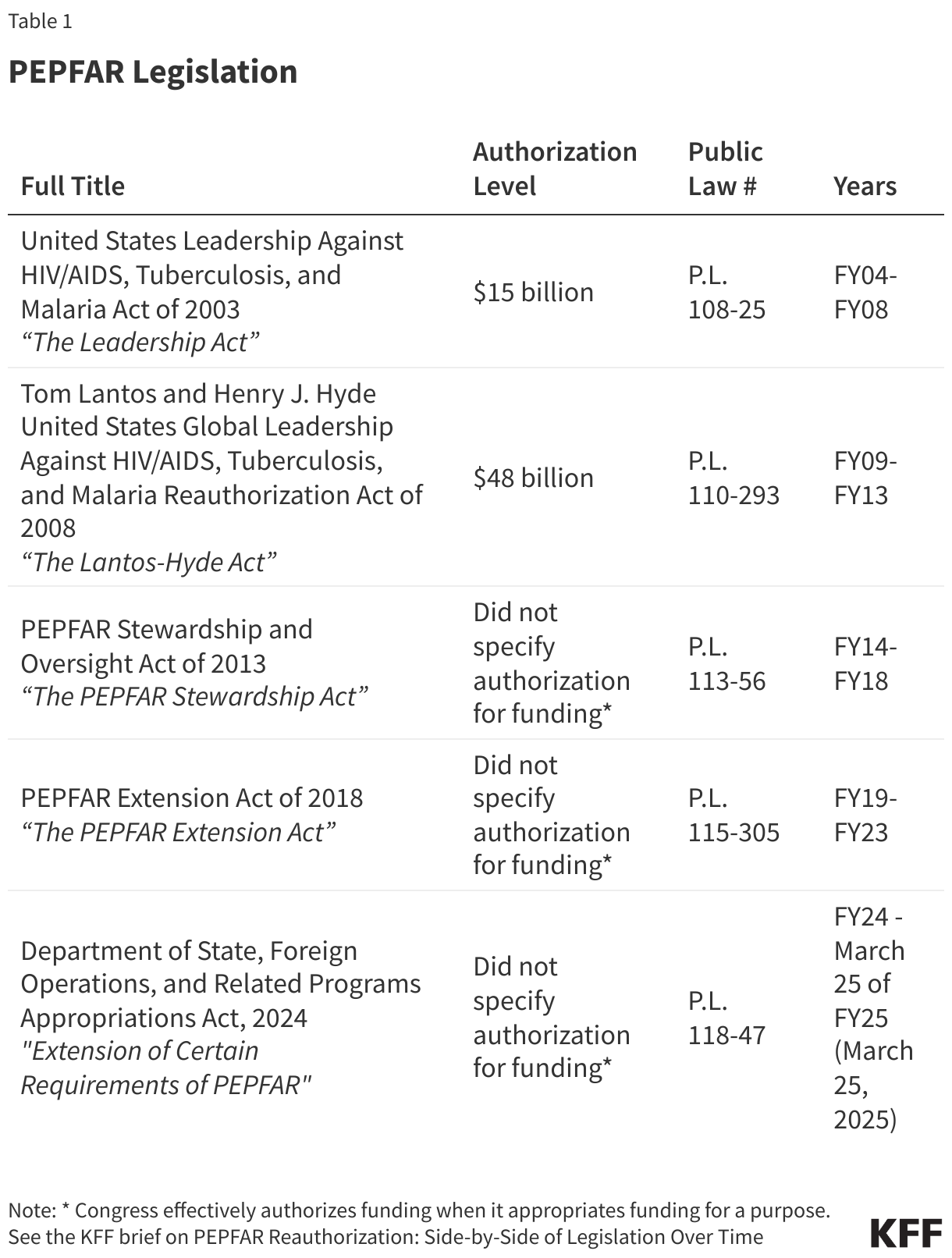
U.S. funding for global health is discretionary1 and determined annually through the U.S. federal budget process, which is initiated by the President and is ultimately set by Congress (see Table 1), which specifies most, but not all, funding (about 99% each year) by agency and program area in annual appropriations bills. Funding for some global health activities that are not specified by Congress are determined at the agency level (more details in the following section).
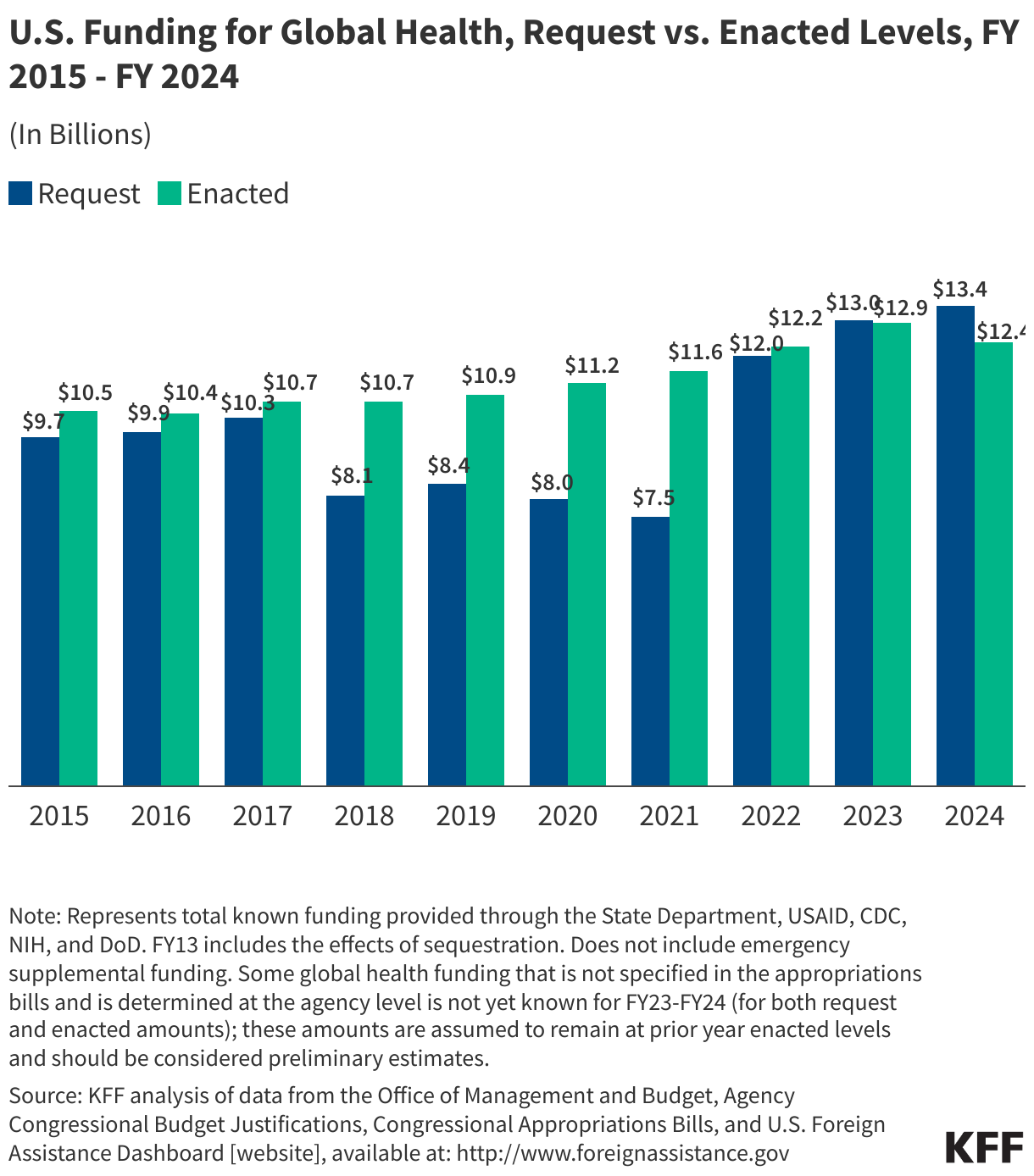
The President’s request often differs from Congress’ enacted levels; in some years, the difference between the request and enacted levels is negligible, while in others, it is significant. For instance, from FY 2018 – FY 2021, the President’s request was significantly lower than what Congress ultimately approved (see Figure 2). Until recently (FY 2023 and FY 2024), Congress provided higher funding levels than the President’s request over the past decade.
Figure 2
4. The majority of U.S. funding for global health is channeled through the Department of State and U.S. Agency for International Development.
The U.S. government funds and carries out its global health efforts through multiple agencies and departments, although most funding is provided by Congress to the Department of State (State) (52%), which advances U.S. objectives and interests worldwide through developing and implementing the President’s foreign policy; followed by the U.S. Agency for International Development (USAID) (33%), which supports long-term and broad-based economic growth in countries and advances U.S. foreign policy objectives; National Institutes of Health (NIH) (7%), which conducts biomedical and behavioral science research and is one of the world’s leading research entities on global health; and Centers for Disease Control and Prevention (CDC) (6%), which focuses on disease control and prevention and health promotion. In addition, a small portion (2.5%) of global health funding is channeled through the Department of Defense (DoD) (see Figure 3).
Figure 3
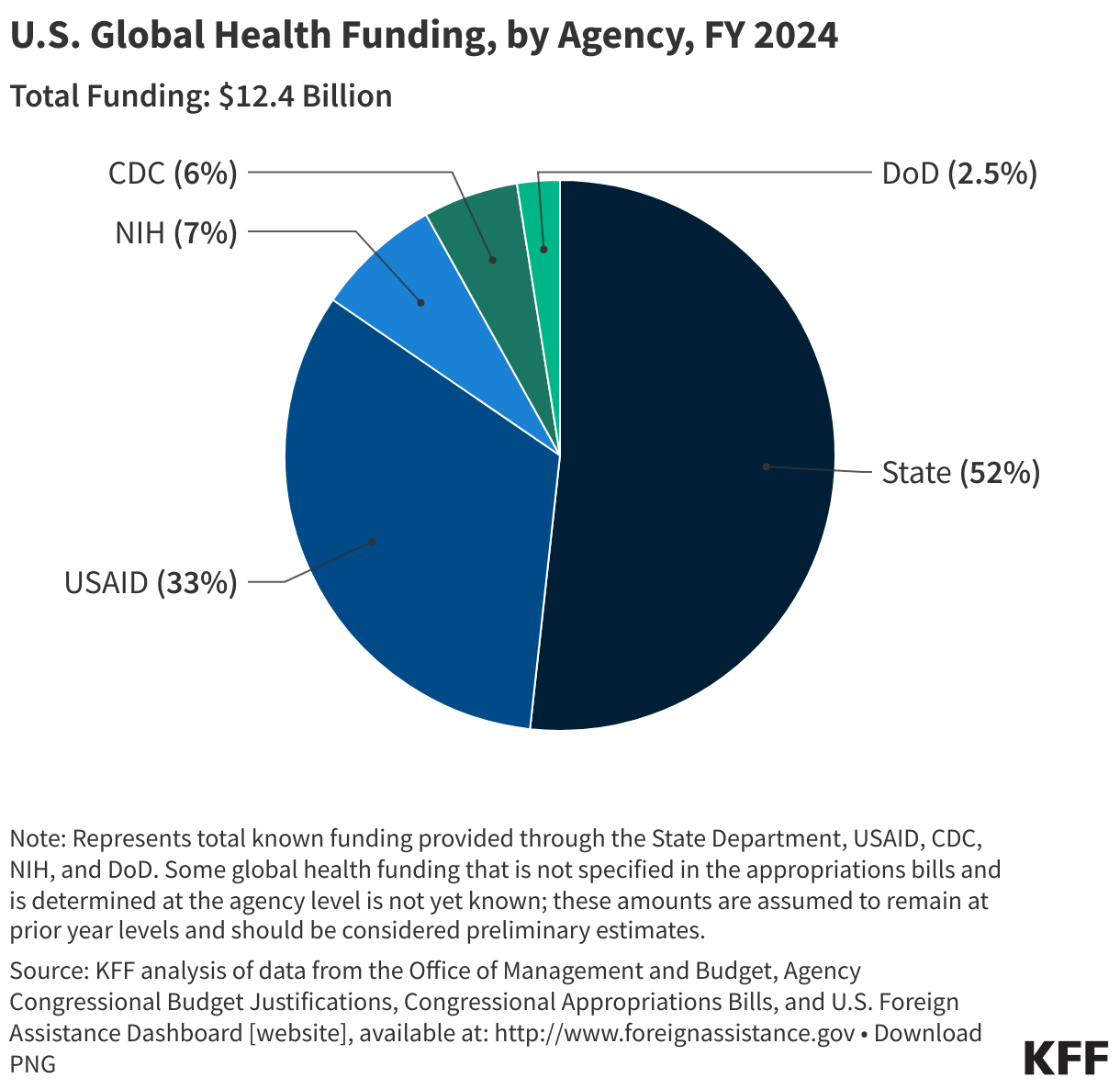
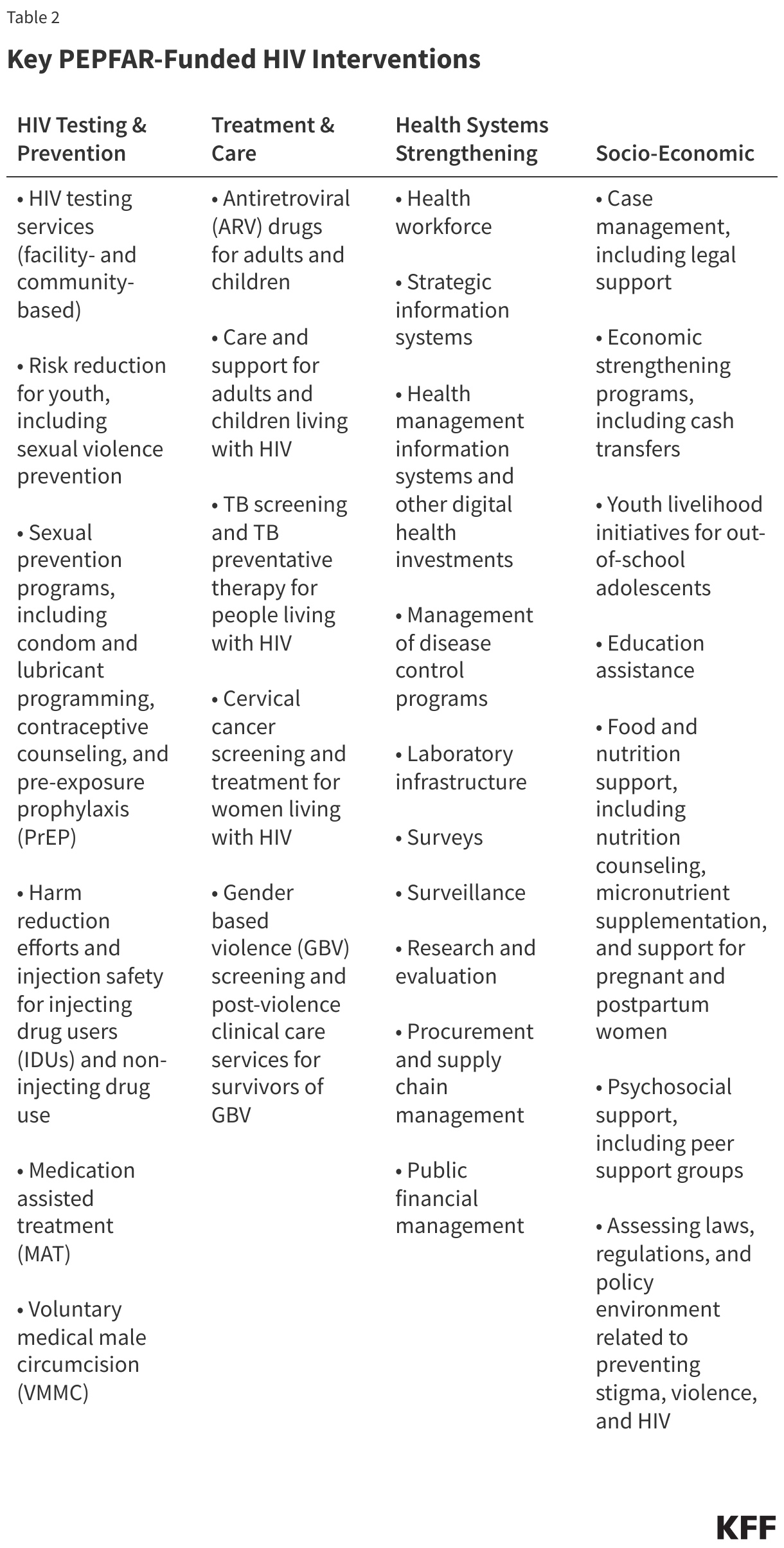
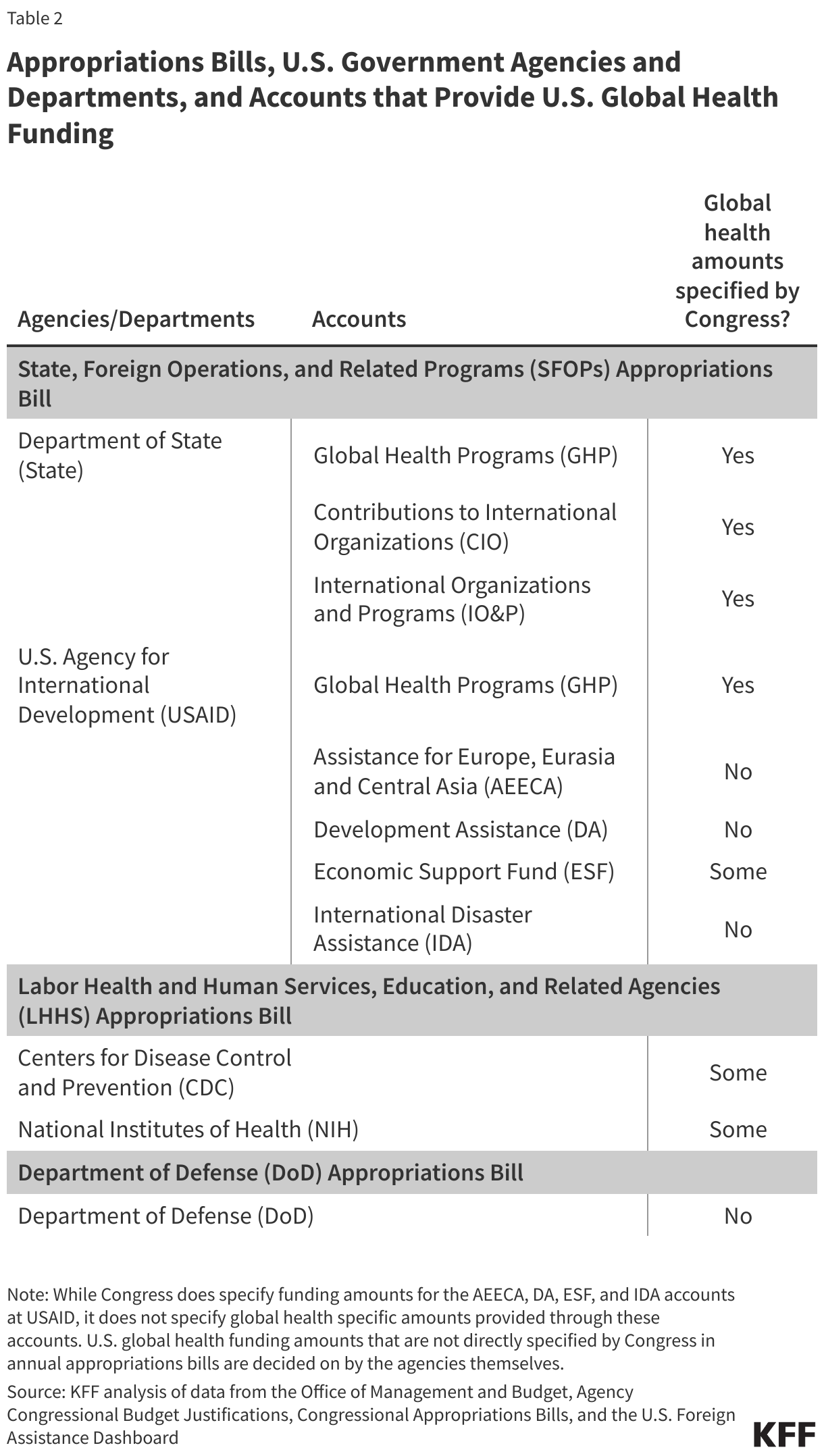
As mentioned earlier, most global health funding amounts are specified by Congress in annual appropriations bills, though some amounts are determined at the agency-level (see Table 2). State and USAID funding is provided in the State, Foreign Operations and Related Programs (SFOPs) appropriations bill; CDC and NIH funding is provided in the Labor, Health and Human Services (Labor HHS) appropriations bill, and DoD funding is provided in the Department of Defense appropriations bills. Within these bills, Congress specifies funding levels for global health program areas (e.g. HIV, TB, MCH, GHS, etc.) under the Global Health Programs (GHP), Contributions to International Organizations (CIO) and International Organizations and Programs (IO&P) accounts at USAID and State as well as for global health programs at CDC. Congress does not specify global health funding amounts under some accounts at USAID2 and some amounts3 at NIH and DoD, and instead provides this authority to the administration.
5. Global health funding has been mostly flat for more than a decade with some exceptions, including increases in some years to respond to outbreaks and for some program areas.
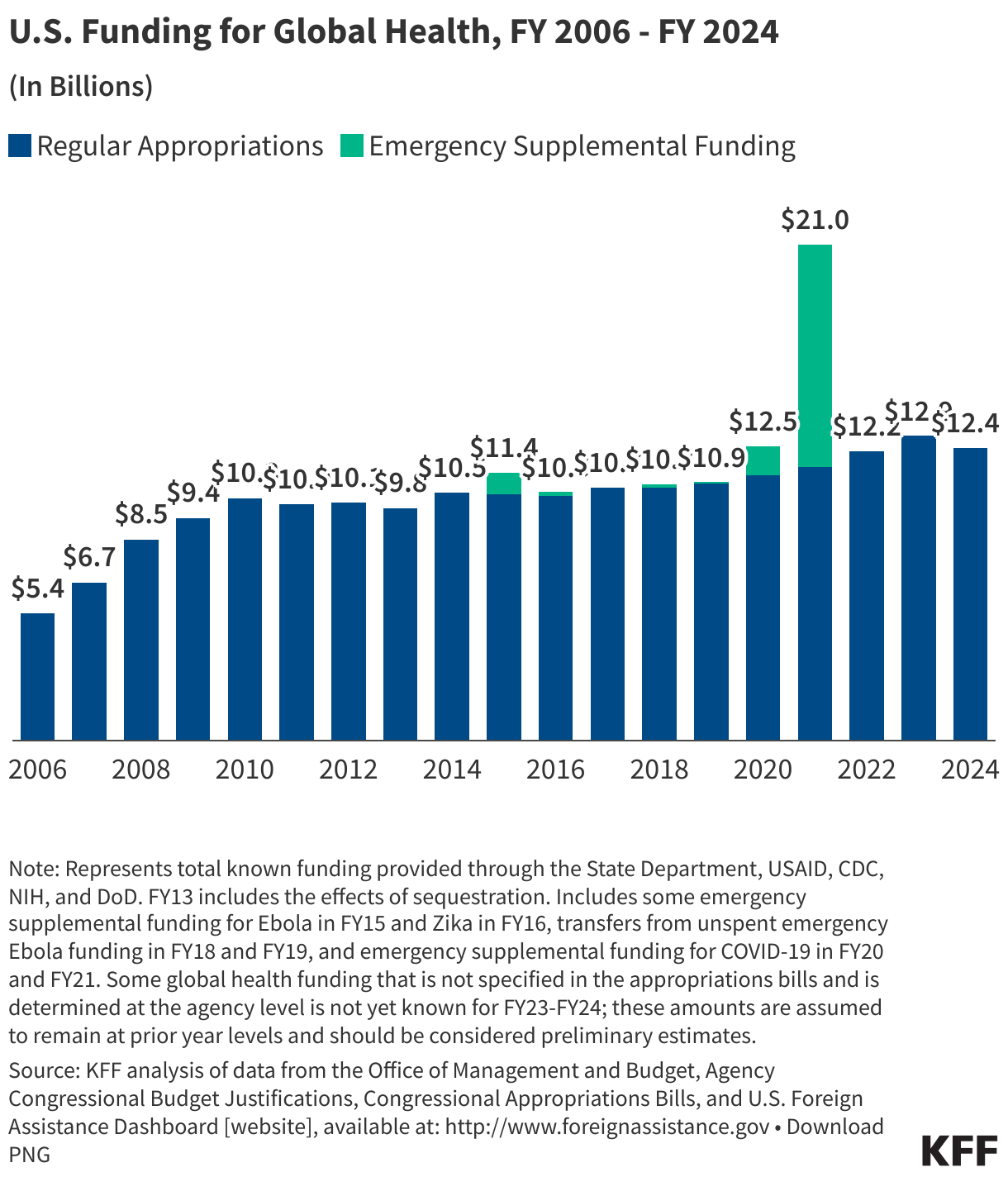
The U.S. investment in global health grew significantly in the early 2000s, in large part because of the creation of major global health organizations and initiatives like the Global Fund in 2001 and PEPFAR in 2003. However, funding has been relatively flat since 2010, with spikes in some years due to the U.S. emergency response to disease outbreaks. U.S. global health funding is comprised of funding provided through the regular appropriations process, with additional funding provided some years through emergency supplemental funding for disease outbreaks, such as Ebola (FY 2015), Zika (FY 2017), and COVID-19 (FY 2020-2021). All additional funding provided through emergency supplemental appropriations must be approved by Congress, and this funding is on top of any regularly appropriated funding. Overall, global health funding reached its highest level to date in FY 2021, largely due to the U.S. global response to the COVID-19 pandemic (that year, emergency funding represented 45% of U.S. global health funding and regular appropriations accounted for 55%); without emergency funding, the high point was in FY 2023 ($12.9 billion). In FY 2025, global health funding was provided through a continuing resolution (CR) which maintained the prior year (FY 2024) amount of $12.4 billion (see Figure 4).
Figure 4
6. Bilateral HIV accounts for the largest share (nearly 50% through regular appropriations) of U.S. global health funding.
The majority of U.S. global health funding is provided for specific areas including bilateral HIV or PEPFAR, tuberculosis, malaria or PMI, maternal and child health, nutrition, family planning and reproductive health, neglected tropical disease, and global health security (see Table 3), with some additional funding provided for other efforts including contributions to the World Health Organization (WHO) and Pan American Health Organization (PAHO).4
Since FY 2006, most U.S. global health funding over time through regular appropriations has been directed to bilateral HIV programs, accounting for approximately 50% of U.S. global health funding in most years (see Figure 5). The Global Fund (learn more about the Global Fund in the multilateral discussion below) accounted for the next largest share over the period, followed by maternal and child health and malaria. More recently, the U.S. has emphasized global health security more, with funding for these efforts increasing considerably during the COVID-19 pandemic and afterward. Consistent with this trend, in FY 2025, the latest year of data available, most funding was provided to HIV efforts ($5.4 billion or 44%), followed by the Global Fund ($1.7 billion or 13%) and maternal and child health and global health security (both $1.3 billion or 10%) (see Figure 6). These shares may differ during times of emergency, when significant funds have been provided on a one-time basis to address emerging outbreaks.5
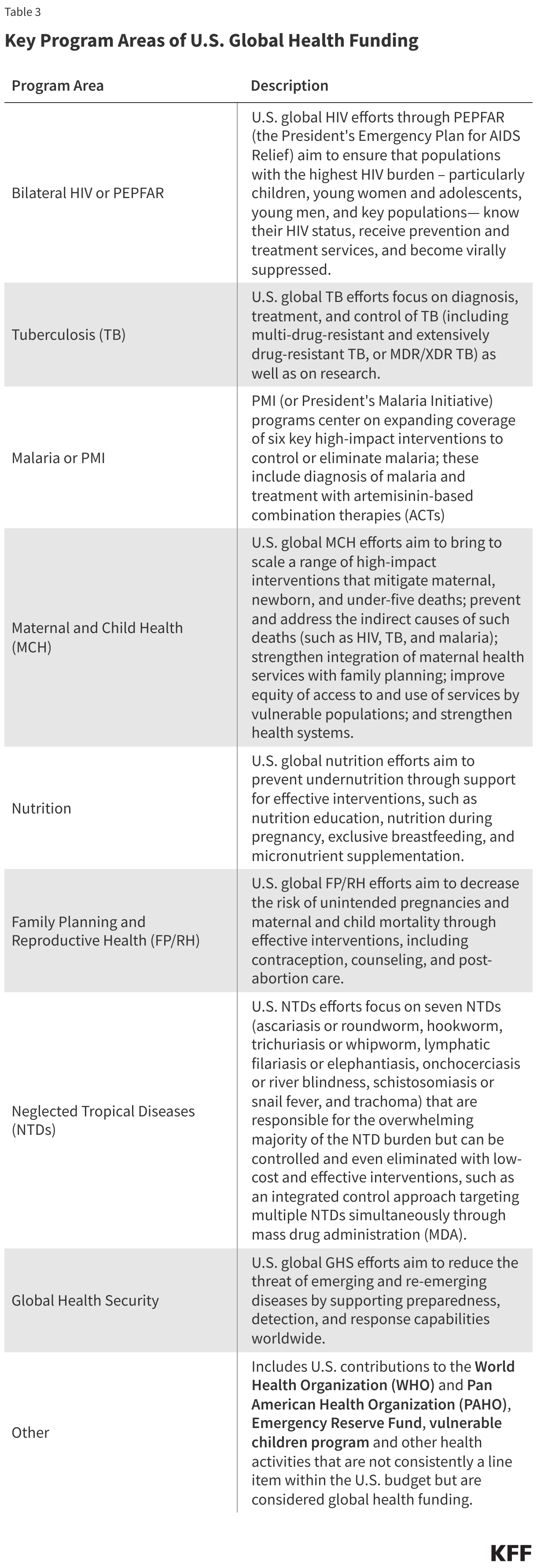
Figure 5
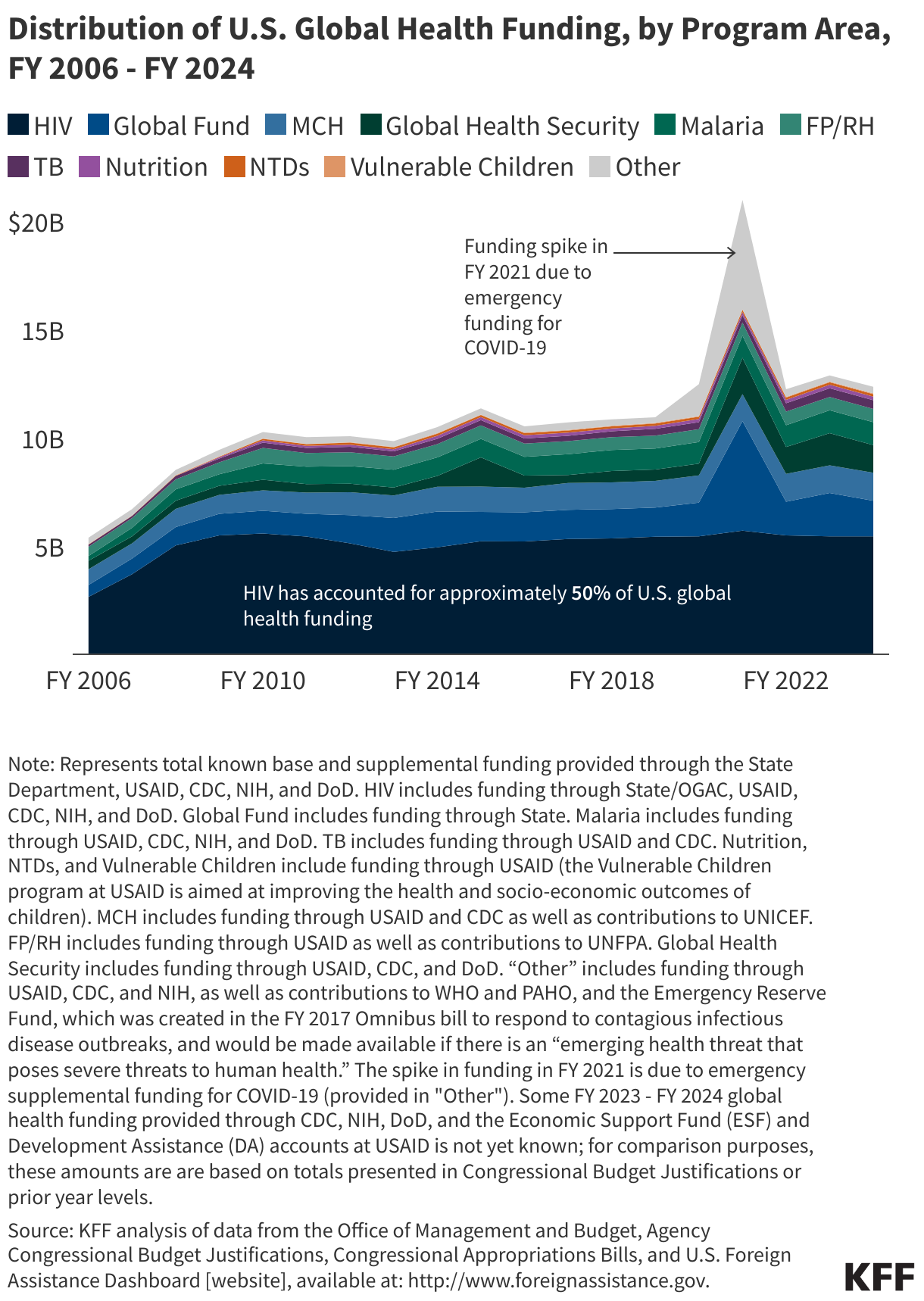
Figure 6

7. Most U.S. global health funding (approximately 80%) is for bilateral programs reaching almost 80 countries in six regions.
In FY 2023, the most recent year country-specific amounts are available, 81% of U.S. global health funding was provided bilaterally (country-to-country, directly funding implementation of global health activities in partner countries) spanning six regions (see Figure 7). While this funding was directed to almost 80 countries, with additional countries receiving support through U.S. regional programs and contributions to multilateral organizations, ten countries accounted for almost 60% of U.S. bilateral support for global health (Figure 8).
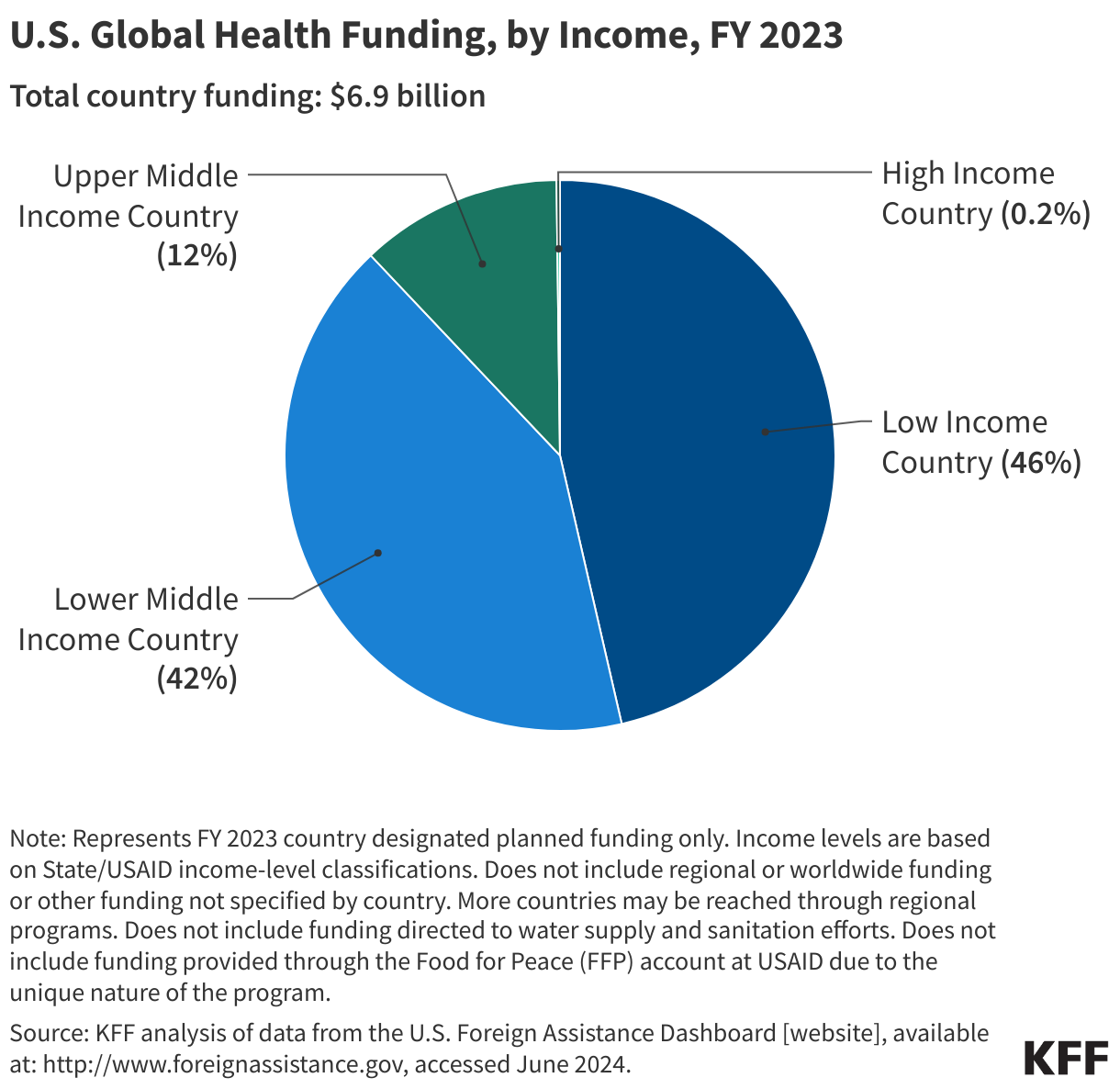
Looking by region, most U.S. bilateral support for global health programs in FY 2023 was provided in sub-Saharan Africa (84%), followed by South and Centra Asia (5%) and the Western Hemisphere (4%) (Figure 9). Looking by income, the majority (88%) of U.S. funding for global health was provided to low and lower-middle-income countries (46% and 42% respectively) (see Figure 10).
Figure 7
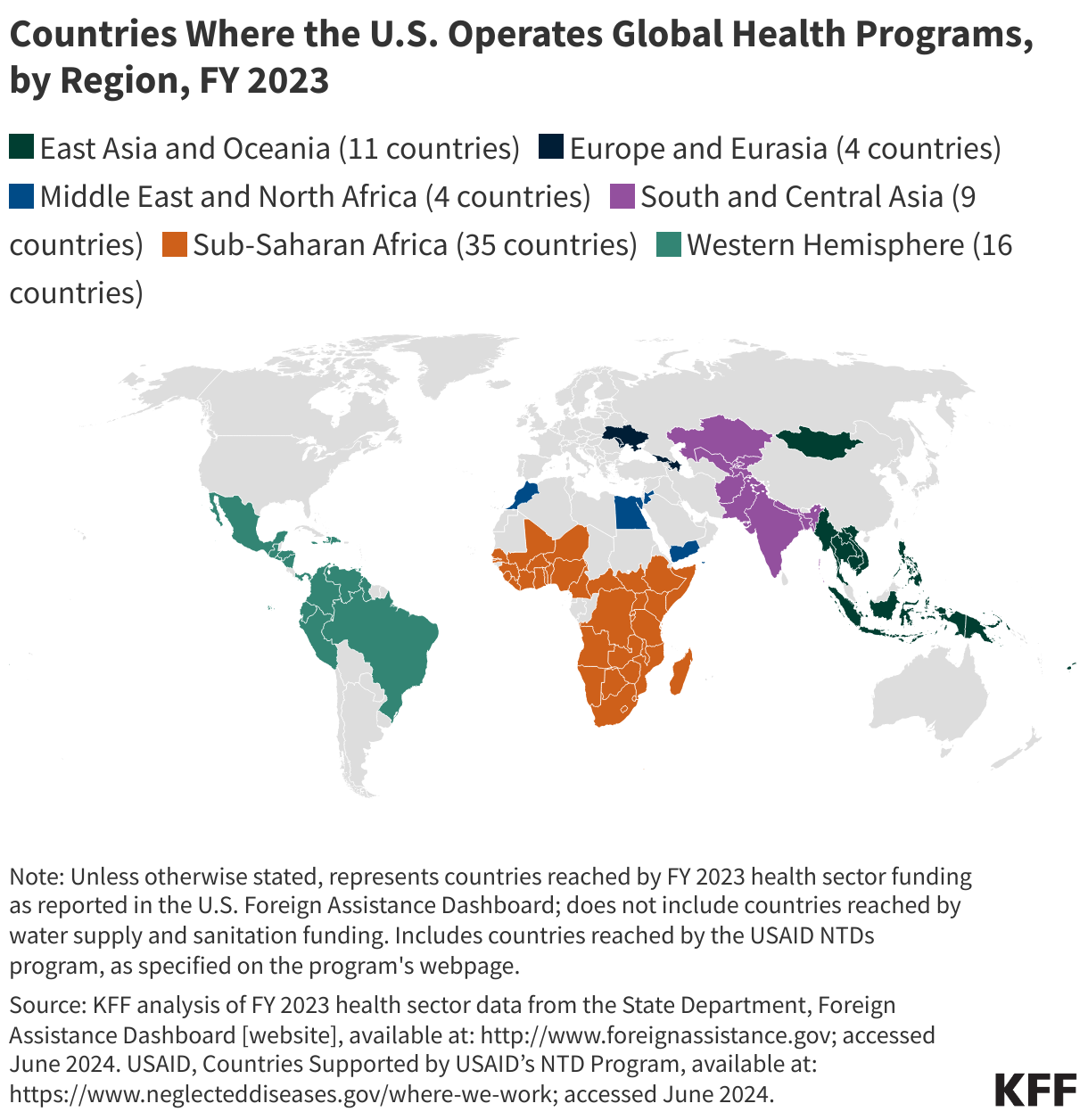
Figure 8
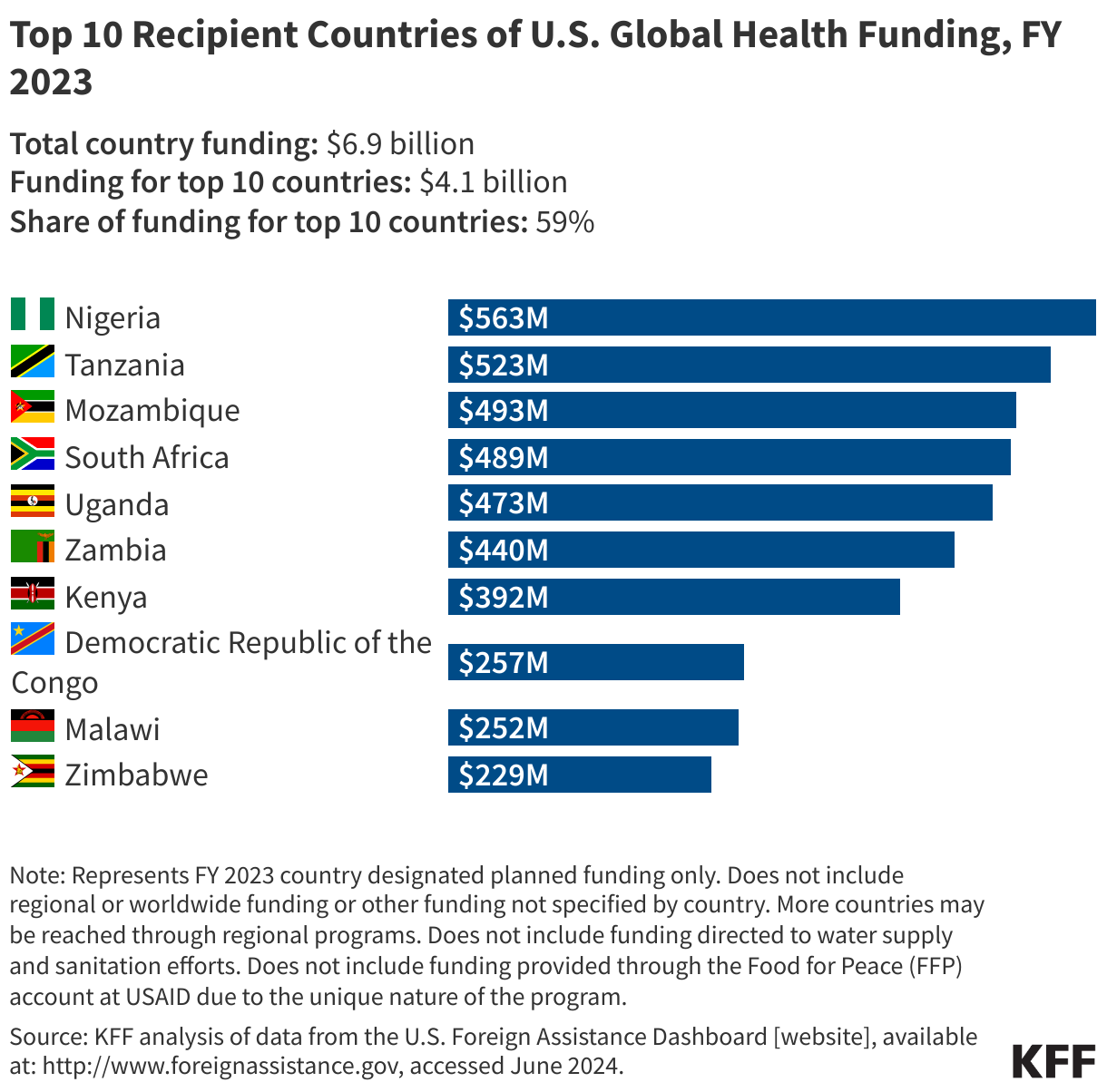
Figure 9
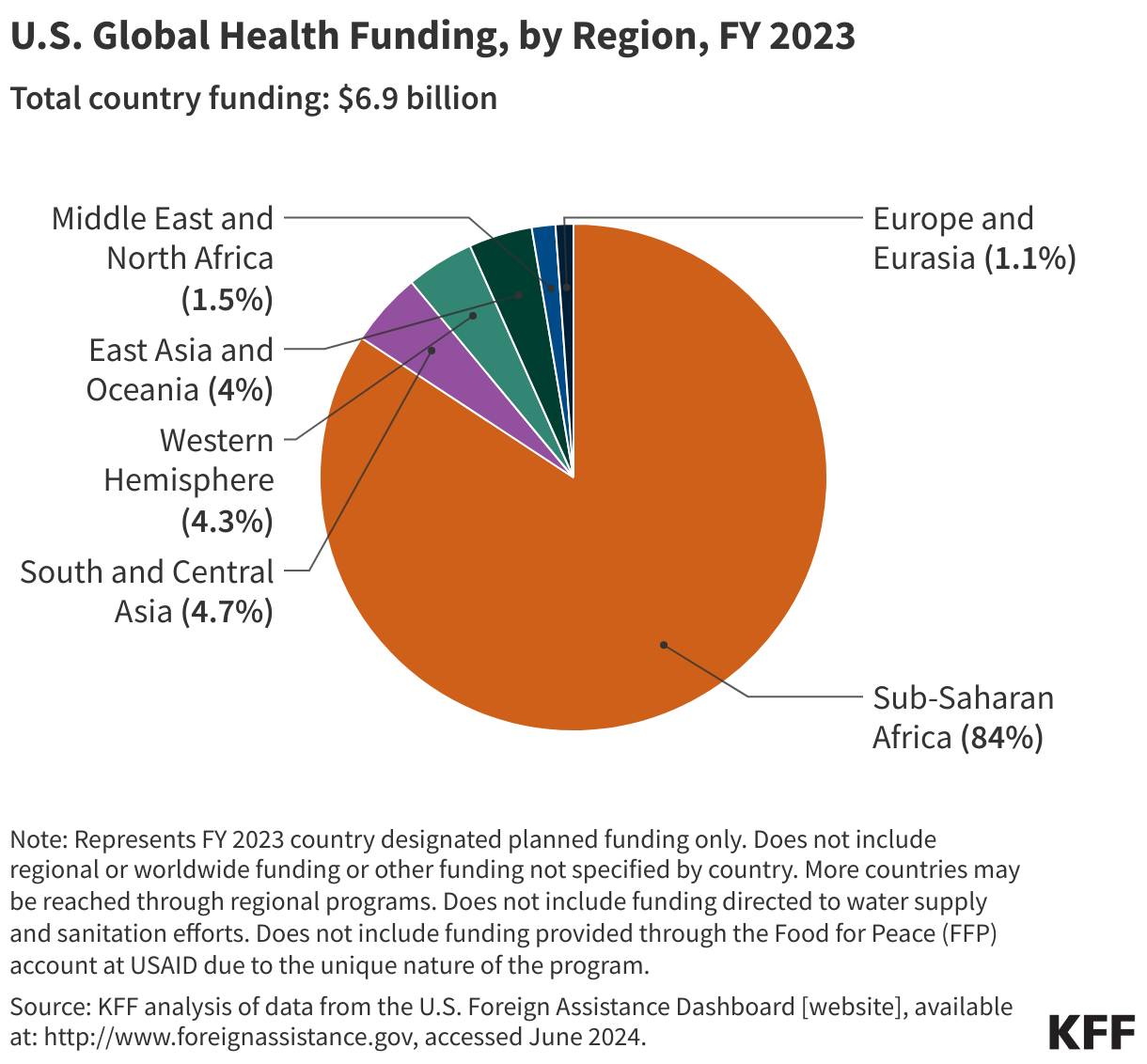
Figure 10
8. Approximately a fifth of U.S. global health funding supports multilateral organizations.
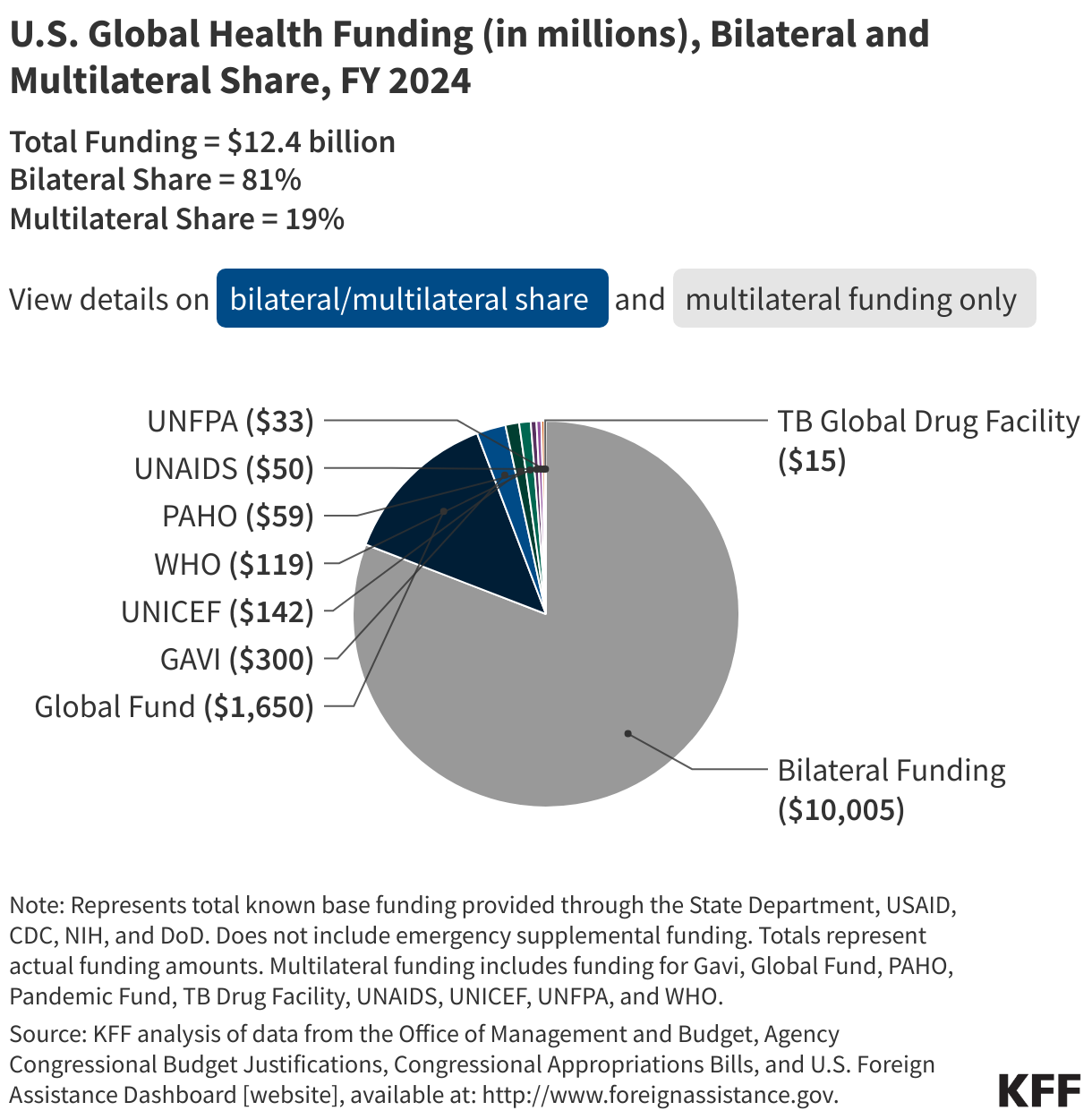
While the majority of U.S. funding for global health is provided bilaterally (81%), the U.S. has a long history of engagement with multilateral health organizations, which pool support from multiple countries for one or more areas of global health, and provides about a fifth (19%) of its global health funding to support6 these institutions (see Figure 10). Multilateral initiatives complement U.S. bilateral global health efforts, helping make progress toward U.S. goals in various program areas, and in some cases, multilateral support allows the U.S. to reach a larger number of countries.
As mentioned earlier, multilateral health institutions the U.S. supports include the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), Gavi the Vaccine Alliance (Gavi), United Nations Children’s Fund (UNICEF), World Health Organization (WHO), Pan American Health Organization (PAHO), Joint United Nations Programme on HIV/AIDS (UNAIDS), United Nations Population Fund (UNFPA), TB Drug Global Drug Facility, and the Pandemic Fund (see Table 4). The Global Fund is the largest multilateral recipient by far of U.S. global health funding followed by Gavi (see Figure 11).
The U.S. provides funding to these organizations every year, with the exception of UNFPA due to ongoing political debates about abortion and the invocation of the Kemp-Kasten Amendment, which has been used by the President to prohibit funding to UNFPA in some years (see the KFF Kemp-Kasten explainer for more detail). During its first term, the Trump Administration also temporarily suspended funding to the WHO in 2020, though these actions were reversed by the Biden Administration in 2021 and the funding was ultimately provided. Most recently in 2025, as one of the first actions taken during its second term, the Trump Administration issued an executive order to formally withdraw from the WHO and suspend funding. In addition, the Pandemic Fund, a newer multilateral financing mechanism launched in 2022 aimed at helping countries build their capacity to prevent, prepare for, and respond to epidemics and pandemics, has not received funding from the U.S. since 2022. However, Congress has included provisions in recent appropriations bills to transfer up to a certain amount of global health funding toward the entity if a public health emergency arises.
Nevertheless, the U.S. is often the largest or one of the largest donors to multilateral health efforts. For example, compared to other donors, the U.S. ranks first in donor support to the Pandemic Fund (accounting for 41% of its funding), the WHO (accounting for 14% of its funding), and the Global Fund (accounting for 33% of its funding) and third in donor support to Gavi (accounting for 13% of its funding). In 2025, several of these multilateral health institutions will have replenishment conferences where the U.S. and other donors will pledge their support for the next funding cycle (see the KFF tracker on U.S. support to four multilateral health institutions).
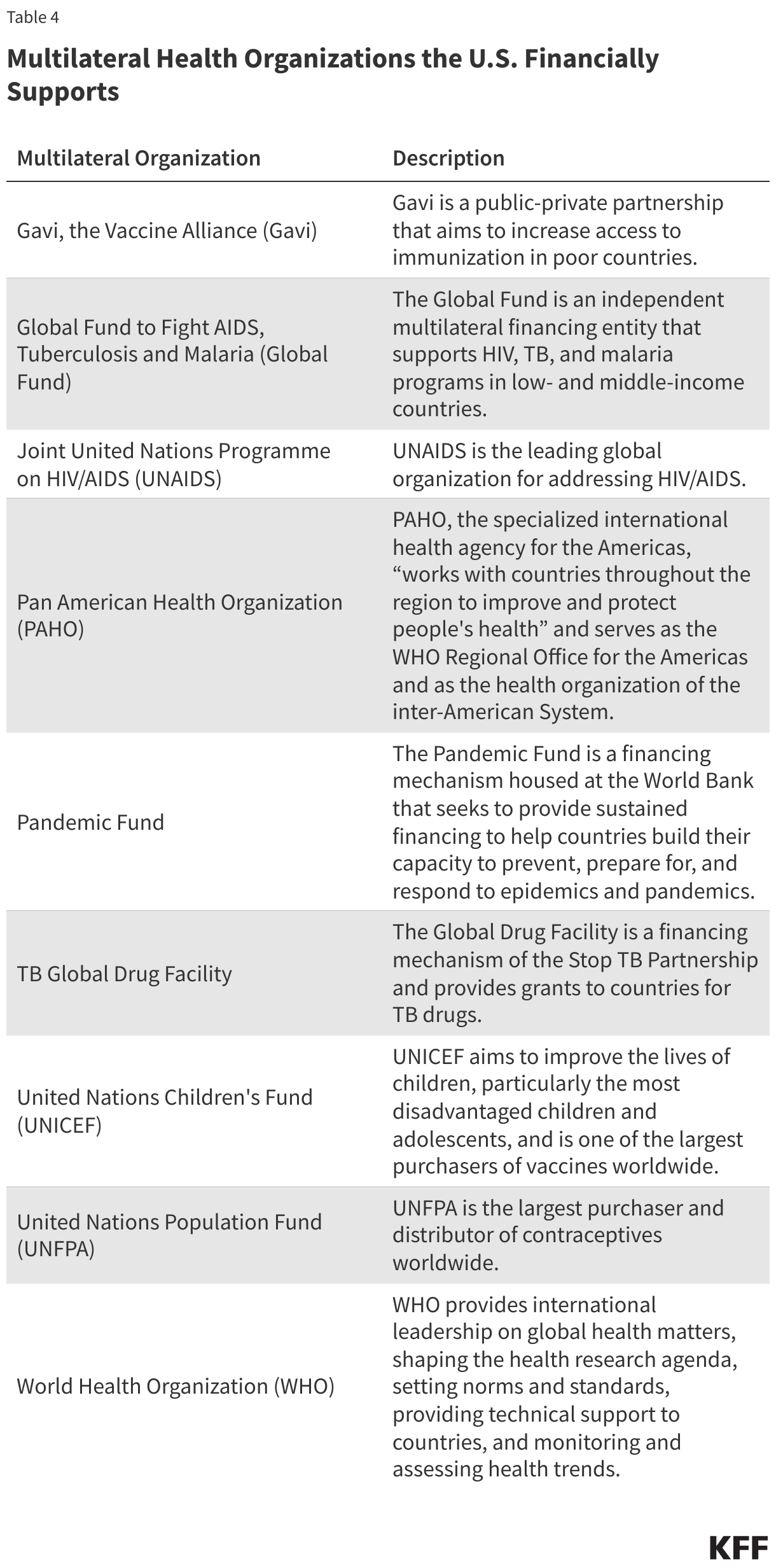
Figure 11
9. The U.S. provides over 40% of total donor government assistance for global health.
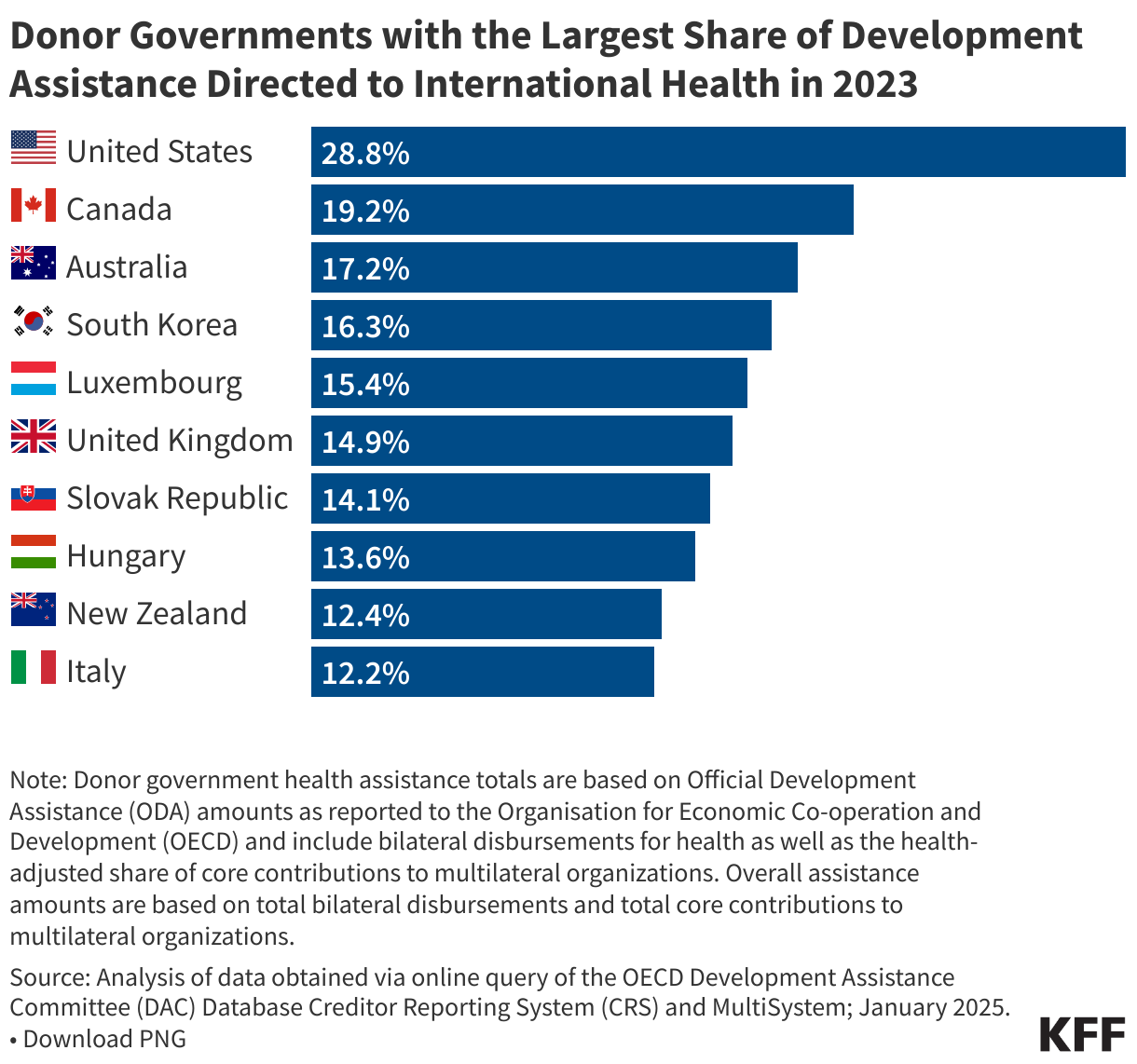
The U.S. plays an integral role in international assistance for health and provides support for global health in the form of Official Development Assistance (ODA) for health. ODA is financial support from donor governments to low- and middle-income countries for areas such as economic development, health, education, governance, or infrastructure, which is provided both bilaterally and through multilateral organizations. The U.S. is the largest donor to global health, providing 42% of all international health assistance among major donor governments (see Figure 12).7 In addition, the U.S. has historically devoted a larger share of its foreign assistance to health than any other donor government, contributing almost 30% of its foreign assistance to global health in 2023 (see Figure 13).
Figure 12
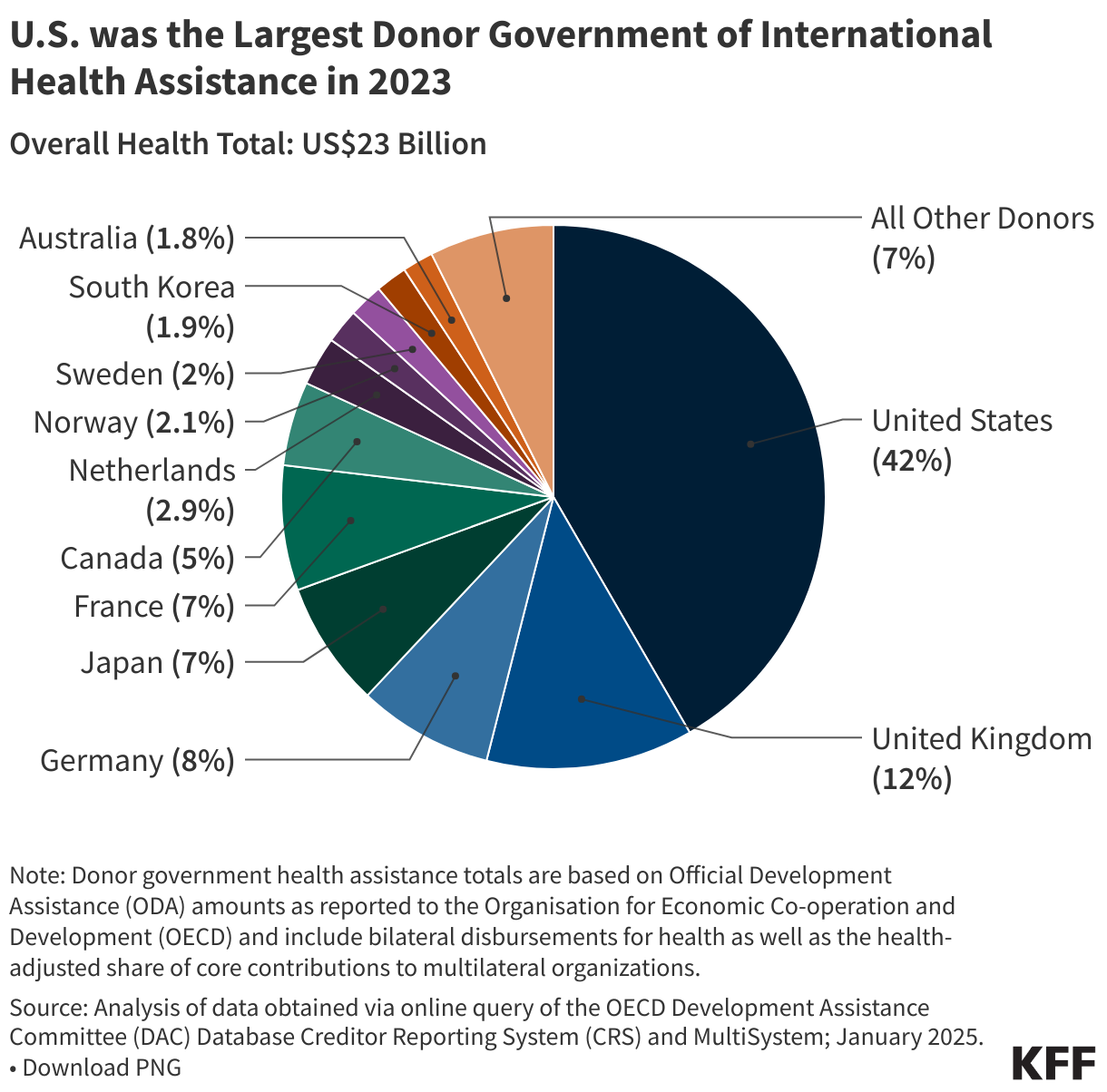
Figure 13
10. Congress and the Administration can place requirements and/or restrictions on U.S. global health funding.
Congress: In addition to specifying funding levels for global health programs, Congress can also specify statutory requirements and policy provisions that:
- direct how funds are spent,
- determine which organizations receive funding, and
- shape the implementation and scope of global health activities.
For instance, one statutory requirement that directs how U.S. foreign assistance, including global health funding, is spent is the Helms Amendment, which prohibits the use of foreign assistance to pay for the performance of abortion as a method of family planning or to motivate or coerce any person to practice abortion. In terms of more general global health policy provisions included in appropriations bills, an example of a common provision is one that directs agencies to provide reports to Congress on certain program areas. A more recent policy provision included in the FY 2024 appropriations bill was a one-year reauthorization of PEPFAR.
Administration: The administration can also place requirements and restrictions on global health funding. For instance, starting with the Reagan administration, the “Mexico City Policy” (MCP)8 has required foreign NGOs to certify that they will not “perform or actively promote abortion as a method of family planning” using funds from any source (including non-U.S. funds) as a condition of receiving U.S. global health assistance. It has been instituted and rescinded along party lines, and expanded over time, by executive action shortly after a new administration takes office. More recently, the Trump administration issued an executive order initiating the U.S. withdrawal from the World Health Organization (WHO) and halting all funding to the multilateral organization.
- As opposed to mandatory funding, which is funding that is dictated and set by law. Mandatory spending, which includes funding for entitlement programs such as Social Security, Medicare, Medicaid, and veteran’s programs, remains essentially unchanged from year to year, as funding levels for these programs are set by the laws that authorize and govern them. ↩︎
- Congress specifies some Economic Support Fund (ESF) funding amounts at USAID (i.e. funding for family planning and reproductive health through the ESF account is often specified by Congress but funding for HIV through this account is not specified by Congress) and does not specify funding amounts for the Assistance for Europe, Eurasia and Central Asia (AEECA), Development Assistance (DA), and CIO accounts at USAID. ↩︎
- Congress specifies some funding amounts for NIH and DoD in annual appropriations bills, including funding for the Fogarty International Center (FIC) at NIH and funding for global HIV at DoD. ↩︎
- Areas that receive global health funding and are not a part of the key program areas listed were combined into an “other” category. “Other” includes U.S. contributions to the World Health Organization (WHO) and Pan American Health Organization (PAHO), as well as funding for the Emergency Reserve Fund, which was created in the FY 2017 Omnibus bill to respond to contagious infectious disease outbreaks and would be made available if there is an “emerging health threat that poses severe threats to human health.” It also includes funding for “other public health threats,” which includes funding for health activities that are not consistently a line item within the U.S. budget (for example, in the FY 2024 budget, the U.S. provided funding to cross-cutting health activities through the Health Reserve Fund and to the global health workforce through the Global Health Workforce Initiative). ↩︎
- In the years where emergency supplemental funding for disease outbreaks has been provided, funding has gone to general global health activities, though sometimes funding is provided for specific global health programs including bilateral HIV (i.e. through emergency COVID-19 funding in FY 2021), the Global Fund (i.e. through emergency COVID-19 funding in FY 2021), and global health security (i.e. through emergency Ebola funding in FY 2015, FY 2018, and FY 2019; emergency Zika funding in FY 2016; and emergency COVID-19 funding in FY 2021). ↩︎
- Represents “assessed” or “core” funding— funding that is specified by Congress and generally used to support essential functions and operations. The U.S. also provides funding to multilateral organizations through “voluntary” or “non-core” contributions—funding that is used for specific projects or initiatives the U.S. seeks to support. Unlike core funding, non-core funding is not specified by Congress in annual appropriations bills. ↩︎
- Totals are based on Official Development Assistance (ODA) amounts as reported by donor governments to the Organisation for Economic Co-operation and Development (OECD) and include bilateral disbursements for health as well as the health-adjusted share of core contributions to multilateral organizations. Bilateral health amounts are based on three OECD sectors from the Credit Reporting System (CRS) database: (1) Health; (2) Population Policies & Programs and Reproductive Health (includes HIV/AIDS & STDs); and (3) Other Social Infrastructure and Services – Social Mitigation of HIV/AIDS. The health-adjusted share of donor government core contributions to multilateral organizations is calculated by applying the health share of a multilateral organization’s total disbursements (as reported in the CRS database) to the donor government’s core contribution for that multilateral organization (as reported in the OECD’s “Member use of the multilateral system” database). ↩︎
- The Mexico City Policy was renamed “Protecting Life in Global Health Assistance” by President Trump during his first term. ↩︎