Recent Changes in Children’s Vaccination Rates by Race and Ethnicity
Summary
As routine and seasonal vaccination rates continue to decline among children, racial disparities in vaccination rates persist. Declining vaccination rates leave children at increased risk for preventable illnesses, while disparities leave some children at greater risk relative to others. Research shows that many childhood diseases require a high level of vaccination within the population to achieve community-wide protection. As vaccination rates decline, risk for disease outbreaks increases. For example, as of November 2025, there have been 44 measles outbreaks (3 or more related cases) in the U.S. during 2025, and the number of measles cases reported for 2025 is the highest level reported in decades, a consequence of declining measles vaccination rates in many areas.
This analysis examines recent childhood vaccination rates by race and ethnicity for children’s recommended vaccines overall and for the measles, mumps, rubella (MMR) and seasonal flu vaccines specifically, based on KFF analysis of data from the Centers for Disease Control and Prevention (CDC) Morbidity and Mortality Weekly Report (MMWR) and the CDC Flu Vaccination Coverage Report (see Methods). It also discusses potential factors contributing to the ongoing disparities in vaccination rates and recent declines in levels of vaccination coverage.
Overall, the data show that children’s vaccination rates, including receipt of recommended childhood vaccinations as well as for MMR and seasonal flu vaccine specifically, have declined in recent years largely due to decreases in vaccinations among White and Asian children. At the same time, and despite the declines among White and Asian children, Black and AIAN children remain least likely to have received recommended childhood vaccinations and the MMR vaccine specifically. In contrast, for the seasonal flu vaccine, White children along with Black and AIAN children are less likely to have received the vaccination compared to their Asian and Hispanic peers.
Ongoing racial disparities in vaccination rates likely reflect a combination of factors including differences in access to care as well as varying levels of trust in vaccines.For example, the 2025 KFF/Washington Post Survey of Parents shows lower levels of confidence in the safety of some vaccines among Black parents compared to White parents. The recent declines in vaccination rates may reflect spread of vaccine misinformation, growing public skepticism about the safety and effectiveness of vaccines, and increasingly partisan views on vaccination. The KFF/Washington Post Survey of Parents shows Republican parents are nearly three times as likely to report skipping vaccinations for their children compared to parents who are Democrats. Most recently, the Centers for Disease Control and Prevention (CDC) posted information to its website indicating that “studies have not ruled out the possibility that infant vaccines cause autism” despite longstanding scientific evidence disputing this connection. Going forward, these declines could be exacerbated by changes in federal vaccine policy.
Children’s Vaccination Rates by Race and Ethnicity
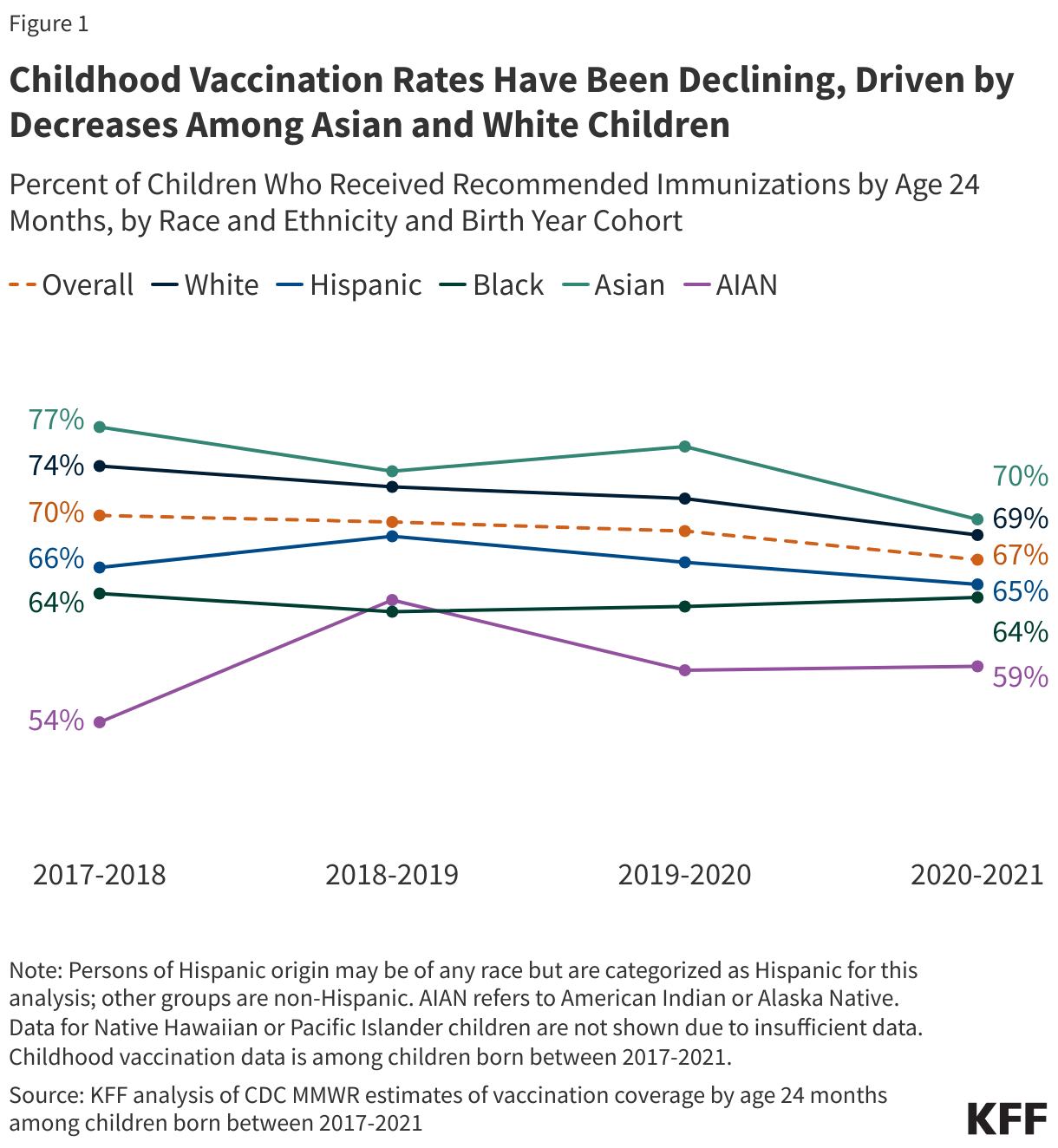
Largely driven by decreases among Asian and White children, rates of receipt of recommended childhood vaccinations for children ages 24 months or younger have declined. The U.S. Advisory Committee on Immunization Practices (ACIP) has established a recommended immunization schedule for children, which outlines the vaccines they should receive from birth through age two. Examination of vaccination rates by birth cohorts, which group children by the year they were born to allow for comparisons across groups and years, shows that vaccination coverage rates among Asian and White children up to age 24 months have declined, falling from 77% among Asian children in the 2017-2018 birth cohort to 70% in the 2020-2021 birth cohort and from 74% to 69% among White children across these cohorts (Figure 1). The rate for Hispanic children rose from 66% to 69% between the 2017-2018 and 2018-2019 cohorts but then declined again to 65% among the 2020–2021 birth cohort. Rates for Black children remained relatively stable over this period. Both Hispanic and Black children continue to have lower vaccination rates than Asian and White children, with only about two-thirds of each group receiving recommended childhood vaccinations. The rate for AIAN children has increased but is still lower than other groups at 59% among the 2020-2021 birth cohort. In addition to lower routine childhood vaccination rates among children ages 24 months and younger, the rate of school vaccine exemptions increased following the COVID-19 pandemic. Recent survey data suggest that parents who had a White child were less likely to agree that school and daycare vaccination requirements are important or necessary compared to parents of children of other racial and ethnic groups.
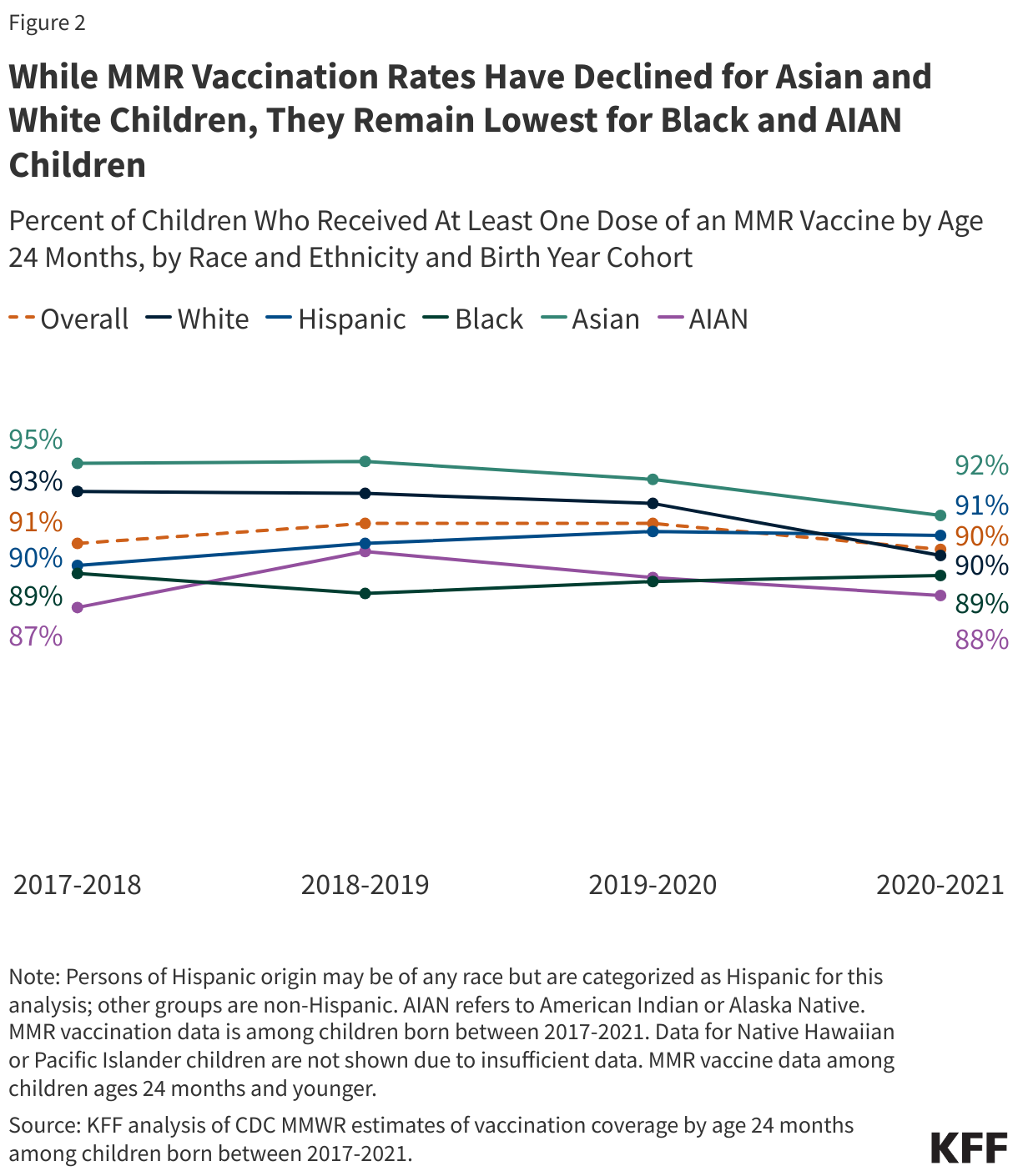
For the MMR vaccination specifically, Asian and White children have the highest rates of receiving at least one dose by age 24 months but their rates have been declining in recent years; rates for Black and AIAN children remain lower and below the Healthy People 2030 goal of 90.8% children receiving at least one MMR dose by their second birthday. Asian children have the highest MMR vaccination rate across racial and ethnic groups, although it fell from 95% among those born in 2017-2018 to 92% among those born in 2020-2021 (Figure 2). Similarly, the rate for White children fell from 93% to 90% across these birth cohorts. Rates for other groups remained largely stable across these cohorts, but rates for Black (89%) and AIAN (88%) children born in 2020-2021 remain lower and below the Healthy People 2030 vaccination goal.
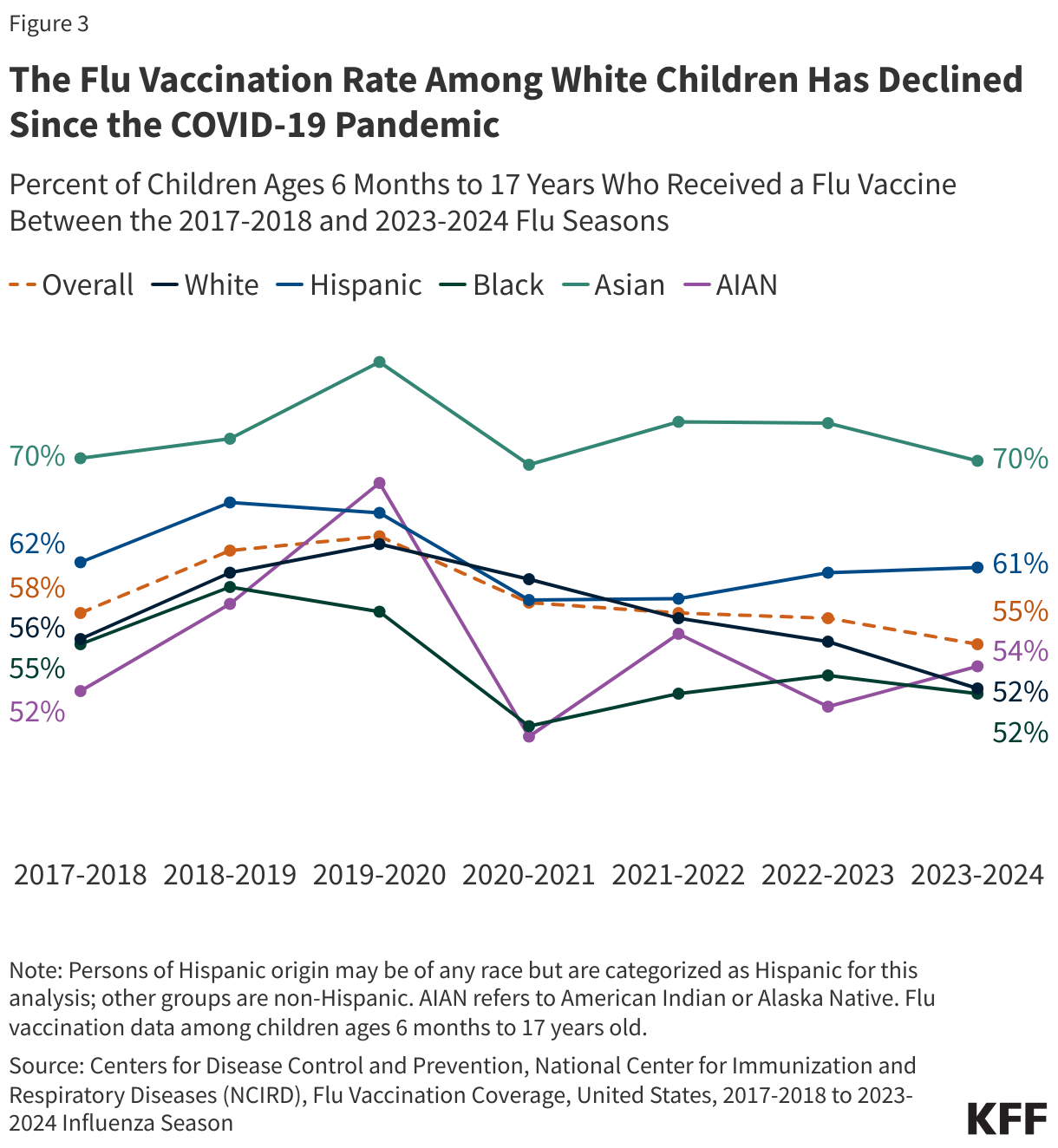
Flu vaccination rates among children ages 6 months to 17 years have fallen to their lowest level in over a decade, with a steady decline among White children since the pandemic. Prior to the COVID-19 pandemic, flu vaccination rates had been increasing, with rates highest among Asian and Hispanic children and lower levels among White, Black, and AIAN children. Vaccination rates fell among all groups moving into the 2020-2021 season following the onset of the COVID-19 pandemic. The rate for AIAN children dropped by nearly 20 percentage points and there were larger declines in vaccination rates for Black, Asian, and Hispanic children compared to their White counterparts. Rates rebounded slightly after 2020-2021 season for most groups although they remain below pre-pandemic levels and continued to decline for White children. As of the 2023-2024 flu season, Asian children (70%) had the highest flu vaccination rate, followed by Hispanic children (61%). In contrast, just over half of AIAN (54%), Black (52%), and White (52%) children received the flu vaccine (Figure 3). Preliminary data for the 2024-2025 season that are available for selected groups also show that only about half of White (46%) Black (48%), and Hispanic (53%) children received the vaccine.
Factors Affecting Vaccination Rates
Racial differences in vaccination rates may reflect a variety of factors including differences in social and economic factors that impact access to care as well as differing levels of trust in vaccines. For example, Black, Hispanic, and AIAN people fare worse compared to their White and Asian counterparts on some measures of access to care and across social and economic factors that may impact access to and use of care, including education and income. In a July 2025 KFF Health Tracking Poll, Black and Hispanic adults were among the most concerned about the availability and insurance coverage of the COVID-19 vaccine. The long legacy of the medical system’s abuse and mistreatment of people of color may also contribute to distrust of vaccines. For example, KFF/Washington Post survey data from October 2025 show that just over half (55%) of Black parents say they are confident the flu vaccines are safe for children compared to about two-thirds of White parents (64%), and Black parents are at least 10 percentage points less likely than White parents to express confidence in the safety of the Polio and MMR vaccines.
A growing partisan divide in attitudes toward childhood vaccinations may be contributing to declining vaccination rates among White children. KFF polling data show that the share of parents who say they keep their child up to date with recommended childhood vaccines like the MMR has been declining over time. For example, KFF Tracking Poll data show that the share of parents who report skipping or delaying some vaccines for their children increased between 2023 and 2025, driven largely by Republican-leaning parents. KFF/Washington Post survey data from October 2025 show that Republican parents are nearly three times as likely to report skipping vaccinations other than flu or COVID for their children compared to parents who are Democrats (22% vs. 8%). Other data show that White voters make up the nearly eight in ten of Republicans and Republican leaders.
Changing attitudes towards vaccines may reflect the spread of vaccine misinformation. Some public health leaders have noted that vaccine hesitancy related to COVID-19 may have had spillover effects on routine child immunizations. More recently, HHS Secretary Robert F. Kennedy Jr. has amplified claims about vaccines that have been rejected by scientists and public health officials. Kennedy has suggested without evidence that the number of recommended childhood vaccines has led to a rise in chronic disease in the U.S. Kennedy has also repeated false claims that vaccines, including MMR, can cause autism and that the measles vaccine causes the illness it prevents. Most recently, the CDC posted information to its website indicating that “studies have not ruled out the possibility that infant vaccines cause autism” despite longstanding scientific evidence disputing this connection. KFF/Washington Post survey shows that many parents are uncertain whether false or misleading claims about vaccines and measles are true, and the share who say these false claims are true is higher among Republican parents, particularly those who identify as supporters of the Make America Great Again (MAGA) movement.
Shifts in federal policy on vaccines may contribute to continued declines in childhood vaccinations. Since his appointment as Secretary of Health and Human Services, Robert F. Kennedy Jr. has made several changes to U.S. vaccine policy, including replacing ACIP, removing COVID-19 vaccine recommendations for healthy children and pregnant women, and cancelling funding for mRNA vaccine research. Secretary Kennedy pledged to examine and revise the recommended vaccine schedule to reduce the number of vaccines given to children and perhaps remove vaccines from the recommended schedule altogether. President Trump has echoed many of Secretary Kennedy’s criticisms of the vaccine schedule, saying that children in the U.S. receive too many vaccines and that parents should disregard current federal recommended childhood vaccine schedule and instead space out shots. In response to changes in federal policies and statements from Trump Administration officials, many states have taken steps to maintain access to vaccines and de-link state vaccine policies from federal recommendations. In contrast, other states have expanded exemptions from school vaccine requirements. This variation in state policies may result in uneven levels of vaccine protection across the country, which could leave some areas at increased risk for disease outbreaks and weaken the nation’s overall community-level protection.
Methods
Childhood Vaccination and MMR Data: This analysis uses CDC MMWR data from 2017-2020, 2018-2019, 2019-2020, and 2020-2021 to present childhood vaccination rates, including MMR. Coverage of recommended vaccinations among children under ages 24 months is measured using the combined 7-vaccine series, which includes ≥4 doses of DTaP, ≥3 doses of poliovirus vaccine, ≥1 dose of measles-containing vaccine, full series of Hib vaccine (≥3 or ≥4 doses, depending on product type), ≥3 doses of Hep B, ≥1 dose of varicella vaccine, and ≥4 doses of PCV.
Flu Vaccination Data: This analysis uses CDC Flu Vaccination Coverage Report data from 2017-2018, 2018-2019, 2019-2020, 2020-2021, 2021-2022, 2022-2023, and 2023-2024 to present CDC’s annual final flu vaccination coverage estimates.