Key Facts on Deferred Action for Childhood Arrivals (DACA)
Note: This content was updated on July 1, 2025 to reflect new regulations eliminating ACA Marketplace eligibility for DACA recipients.
The Deferred Action for Childhood Arrivals (DACA) program was created to protect eligible young adults who were brought to the U.S. as children from deportation and to provide them with work authorization for temporary, renewable periods. As of September 30, 2024, there were roughly 538,000 active DACA recipients from close to 200 different countries of birth residing all over the U.S. While individuals with DACA status can be authorized to work, they had previously been ineligible for federal health coverage through Medicaid, the Children’s Health Insurance Program (CHIP), and the Affordable Care Act (ACA) health insurance Marketplaces. These restrictions result in higher uninsured rates among DACA recipients, contributing to barriers to accessing health care.
The Biden Administration published regulations to expand eligibility for ACA Marketplaces, including tax credits to help pay for premiums and cost-sharing, to DACA recipients as of November 1, 2024. However, as of January 2025, DACA recipients in 19 states are ineligible to enroll in ACA Marketplace coverage due to pending court challenges. On June 25, 2025, the Centers for Medicare and Medicaid Services (CMS) finalized a rule that will once again exclude DACA recipients from the definition of “lawfully present” immigrants for the purposes of health coverage, making them ineligible to purchase coverage through the ACA Marketplaces across the U.S. beginning 60 days after the final rule’s publication. The future of the DACA program as a whole also remains uncertain with a case challenging the legality of the program making its way to the Supreme Court in 2025.
This brief provides an overview of DACA and who DACA recipients are and provides data on health coverage, work status, and income among individuals who meet eligibility criteria for DACA since there are no administrative data on these measures available for DACA recipients. It also discusses potential impacts of ending the DACA program. It is based on analysis of data on DACA recipients from the United States Citizen and Immigration Services and analysis of individuals who are likely eligible for DACA using 2022 Current Population Survey Annual Social and Economic Supplement (CPS-ASEC) data (see methods for more details).
Overview of DACA
DACA was originally established via executive action in June 2012 to protect certain undocumented immigrants who were brought to the U.S. as children from removal proceedings and to receive authorization to work for renewable two-year periods. To be eligible, individuals must have arrived in the U.S. prior to turning 16 and before June 15, 2007; be under the age of 31 as of June 15, 2012 (i.e., under age 44 as of 2025); be currently enrolled in school, have completed high school or its equivalent or be a veteran; and have no lawful status as of June 15, 2012. The program has enabled over 900,000 immigrants to stay in the U.S., go to school, and contribute to the economy through employment.
The Biden Administration published a final rule in 2022 to codify DACA largely consistent with its existing eligibility requirements and scope, but its implementation remains limited subject to court rulings. Promulgation of this rule followed a rescission of the program by the Trump Administration in 2017, which was ruled unlawful by the Supreme Court in 2020. Subject to ongoing litigation and current court rulings, current DACA approvals and work authorizations remain in effect, and the Department of Homeland Security (DHS) will continue to process DACA renewal requests and related requests for employment authorization. It is also accepting initial DACA and employment authorization requests, however, it cannot process initial requests under the current court orders, so these requests remain on hold.
While DACA protects an individual from removal action for a certain period of time, it does not provide a pathway to U.S. citizenship, and people with DACA status previously were ineligible for any federally funded health coverage. Individuals with DACA status can be authorized to work, and studies have found that DACA eligibility helps improve physical and mental health, particularly among individuals with low incomes, and can improve the well-being of children of DACA recipients. However, individuals with DACA have limited options for health insurance coverage if they do not have access to employer-sponsored insurance since they previously were ineligible for federal health coverage programs, including Medicaid, the Children’s Health Insurance Program (CHIP), and the ACA health insurance Marketplaces.
The Biden administration expanded Marketplace coverage with subsidies to DACA recipients, but implementation of the expansion is blocked in 19 states due to pending litigation. On May 3, 2024, the Biden administration published regulations that updated the definition of lawfully present to include DACA recipients for purposes of eligibility to purchase coverage through the ACA Marketplaces and to receive tax credits to help pay for premiums and cost sharing effective November 1, 2024. The Biden administration estimated that this eligibility expansion could extend coverage to nearly 100,000 uninsured DACA recipients. However, as of January 2025, DACA recipients in 19 states are ineligible to enroll in ACA Marketplace coverage due to court decisions. Additionally, on June 25, 2025, the Centers for Medicare and Medicaid Services (CMS) finalized a rule that will once again exclude DACA recipients from the definition of “lawfully present” immigrants for the purposes of health coverage, making them ineligible to purchase coverage through the ACA Marketplaces beginning 60 days after the final rule’s publication in all states. Elimination of the coverage expansion could leave thousands of DACA recipients without an affordable coverage option.
Characteristics of DACA Recipients
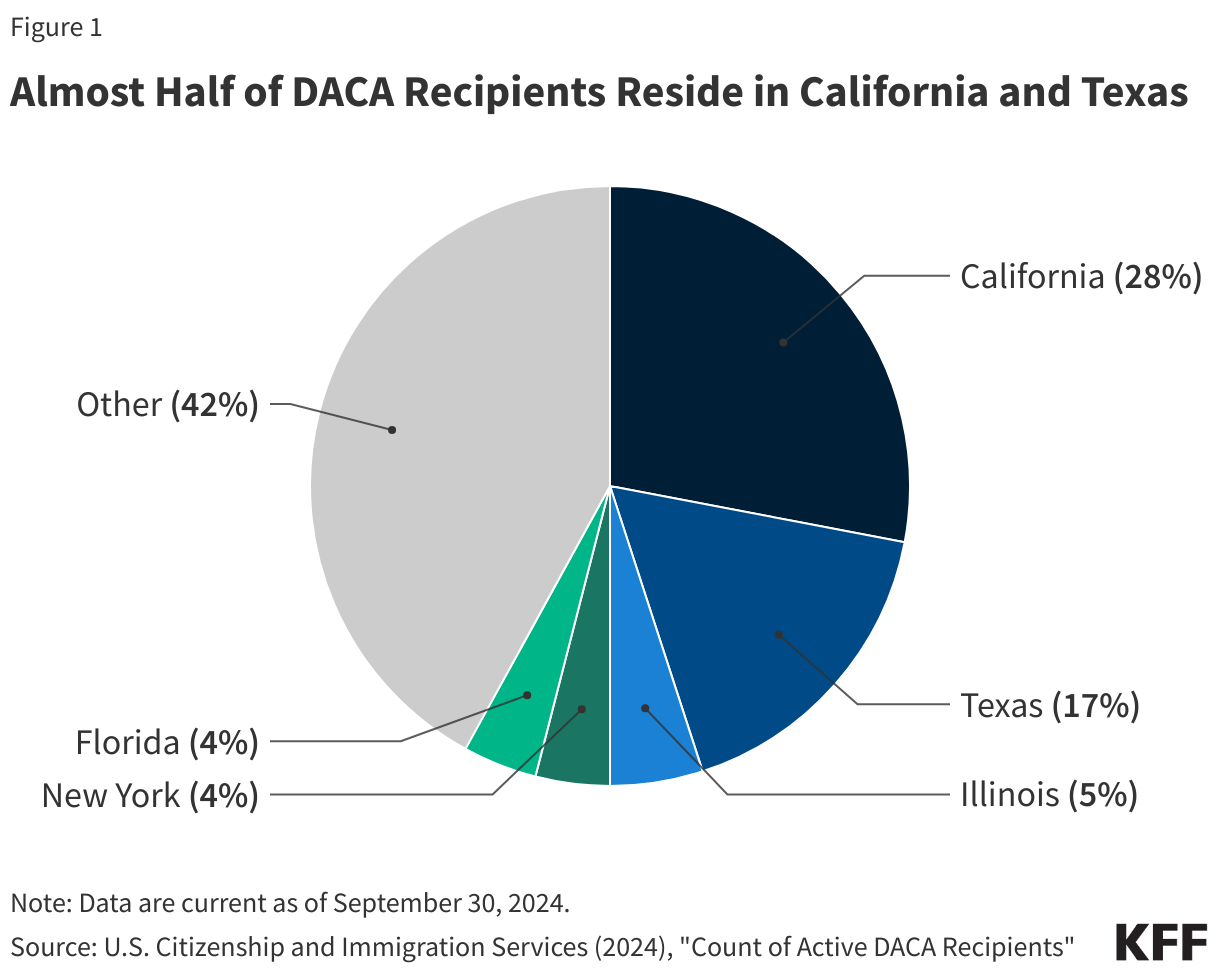
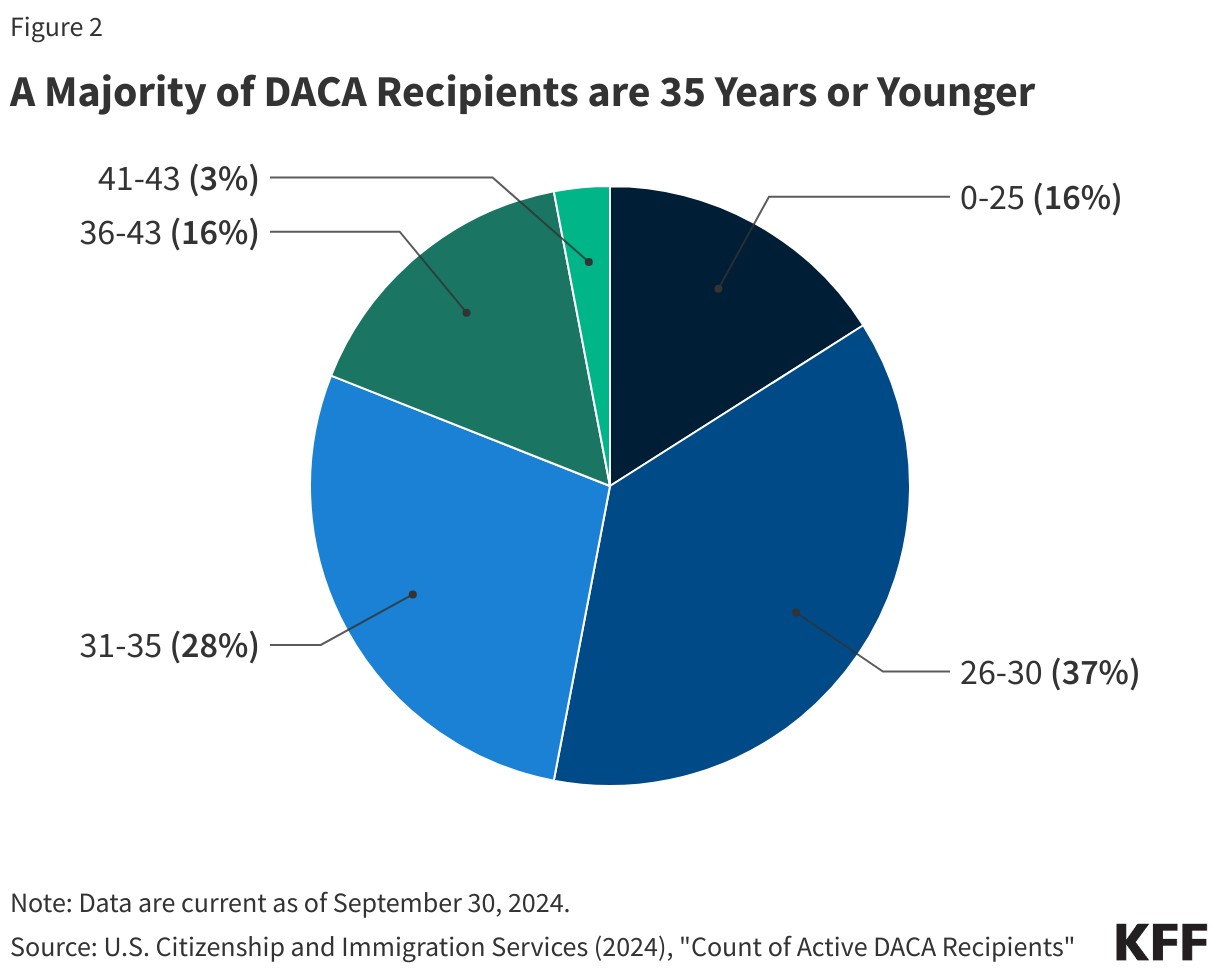
As of September 30, 2024, there were roughly 538,000 active DACA recipients in the U.S. Over one in four (28%) active DACA recipients reside in California, with another 17% living in Texas, 5% in Illinois, 4% in New York, 4% in Florida, and the remaining 42% distributed in other states across the country (Figure 1). DACA recipients are young, with the majority under age 36 (Figure 2), and over half are female. Seven in ten DACA recipients are single, while nearly three in ten are married. The top countries of birth for active DACA recipients include Mexico (81%), El Salvador (4%), and Guatemala (3%).
Health, Work Status and Income among Individuals Likely Eligible for DACA
No administrative data are available on health, health coverage, work status, and income among DACA recipients. As such, using 2022 CPS-ASEC data we present data for undocumented immigrants likely eligible for DACA based on them meeting age, education, and length of residence requirements. (See methods for more details.)
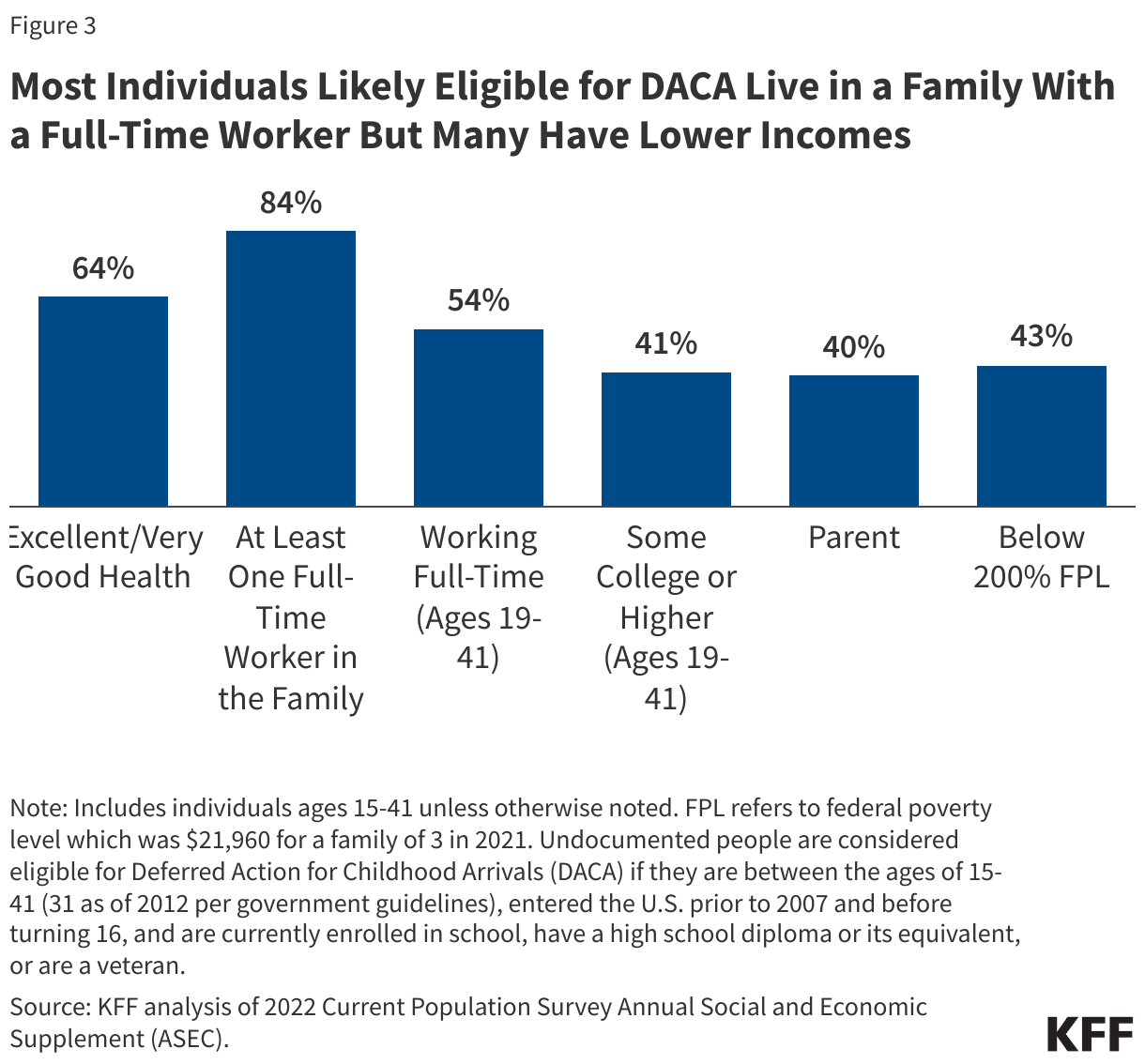
Most individuals likely eligible for DACA are healthy and the large majority live in a family with at least one full-time worker (Figure 3). Among individuals who are likely eligible for DACA, nearly two-thirds (64%) report their health as excellent or very good, while an additional 28% report their health as good. In comparison, 71% of U.S.-born individuals ages 15-41 report being in excellent or very good health, with an additional 22% reporting being in good health. These findings reflect that younger individuals tend to be healthy. The large majority (84%) of individuals likely eligible for DACA live in a family with at least one full-time worker and over half (54%) of adults are working full-time themselves. Despite high rates of employment, 43% of individuals likely eligible for DACA have incomes below 200% of the federal poverty level (FPL) compared with 26% of U.S.-born individuals in the same age group (Figure 3). This income disparity likely reflects disproportionate employment in lower wage jobs among individuals likely eligible for DACA.
Uninsured Rates for Individuals Likely Eligible for DACA
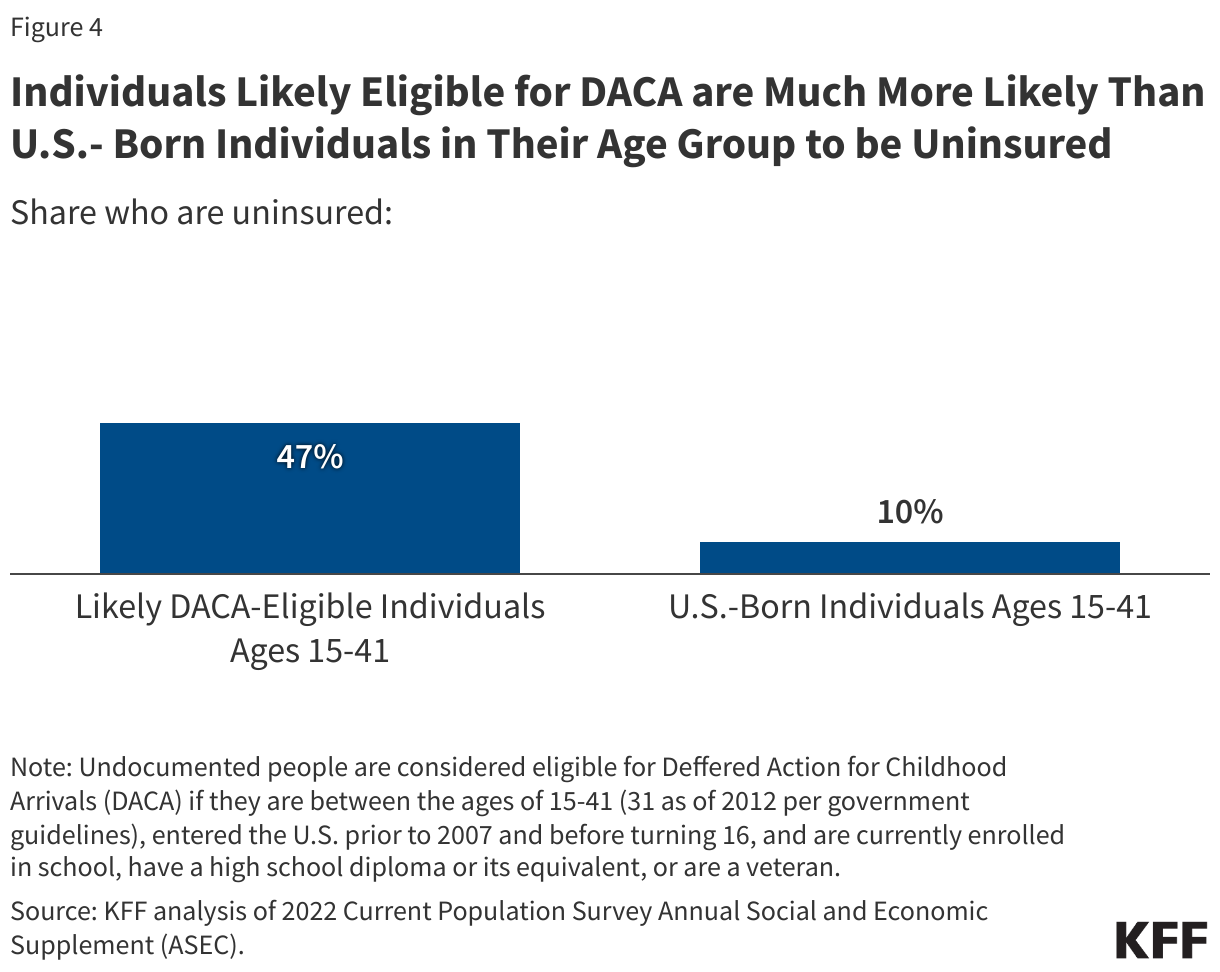
Individuals likely eligible for DACA are much more likely than U.S.-born individuals in their age group to be uninsured (Figure 4). Overall, based on 2022 data, 47% of individuals likely eligible for DACA were uninsured, compared to 10% of U.S.-born individuals in their age group. These estimates are higher than other estimates of uninsured rates among DACA recipients based on survey data, likely reflecting differences in the group being analyzed and data source. Although most individuals who are likely eligible for DACA are in a family with a full-time worker, as noted above, they are more likely to be low-income, which likely reflects disproportionate employment in low-wage jobs that are less likely to offer employer-sponsored health insurance. Those without access to affordable coverage through an employer or who cannot afford coverage on the individual market are left with limited options since they previously were prohibited from enrolling in Medicaid, CHIP, and Marketplace coverage. With the Biden administration coverage expansion, DACA recipients are now eligible for Marketplace coverage in some states. Those who are uninsured are largely reliant on care through community health centers and public health services and can receive treatment for emergency conditions. California, which is home to the largest share of DACA recipients (28%), provides fully state-funded coverage to individuals regardless of immigration status for which DACA recipients can qualify.
Key Issues Looking Ahead
The number of young adults who may benefit from DACA is dwindling over time, and the future of the program remains uncertain. Given the requirements to have entered the U.S. prior to June 15, 2007, and to be under the age of 31 as of June 15, 2012, the number of people who could be eligible for DACA is decreasing over time. The American Dream and Promise (DREAM) Act of 2023 would provide a pathway to lawful permanent resident status and eventually citizenship for undocumented immigrants who were brought to the U.S. as children and who meet certain requirements. Different versions of this Act have been proposed in the U.S. Congress since 2001, but have never been passed, and there does not appear to be a current pathway to passage for such legislation. The future of the DACA program remains uncertain due to ongoing litigation. Since 2021, the DHS has been unable to process first-time DACA applications due to court challenges but has continued to process DACA renewal requests and related requests for employment authorization. In January 2025, a federal appeals court ruled against the legality of the DACA program in Texas, the state that filed the lawsuit. However, there is currently a stay on the ruling until there are further orders by the appeals court or the Supreme Court. As a result, there is no change to the status of the DACA program as of January 2025, with active DACA recipients nationwide continuing to be eligible to renew their status while the processing of first-time DACA applications by the DHS continues to be on hold.
President Trump attempted to end DACA during his first term but was blocked by the Supreme Court in 2020; how he will treat the program during his second term remains unclear. After the attempt to end DACA had failed in 2020, the Trump administration said that it would try again to eliminate DACA protections, suggesting it would be unlikely to appeal the decision if a court decides to eliminate the DACA program. While the second Trump administration has implemented a number of restrictive immigration policies, in an interview prior to his inauguration, President Trump indicated that he would work on addressing the status of “Dreamers” and indicated a willingness to work with Democrats on the issue, although the details of this proposed plan remain unclear.
Elimination of the DACA program would have implications for the health and well-being of DACA recipient families. There are over half a million DACA recipients, a majority of whom are working and many of whom have U.S.-born children, who could be at risk of deportation if the program is eliminated. Eliminating the DACA program could increase negative physical and mental health outcomes among recipients and their families due to increased likelihood of deportation, family separation, loss of employment, and increased barriers to health care. Research shows that DACA increases access to employer-sponsored health insurance, and expanded coverage is associated with reduced barriers to health care and increased access to culturally competent care. Research also finds that children of mothers that are eligible for DACA were more likely to participate in the Special Supplemental Nutrition Program for Women, Infant, and Children, compared to children of mothers who were ineligible. Uncertainty about DACA has been shown to increase negative mental health outcomes and worse self-reported health among DACA recipients, while program protections lead to improved mental health. A study found that children of mothers eligible for DACA experienced a significant decrease in anxiety disorder diagnoses compared to children whose mothers were ineligible.
Elimination of the DACA program could also have negative economic and workforce impacts. DACA has reduced unemployment rates and allowed DACA recipients to contribute to the workforce and their communities. Research also shows that DACA is associated with increased wages among U.S.-born workers with little to no decrease in their employment in labor markets with higher shares of DACA recipients, suggesting that DACA recipients act as complements instead of substitutes for U.S.-born workers in the labor market. Elimination of the DACA program would lead to loss of employment among DACA recipients since they would lose work authorization.
Methods
Data on individuals likely eligible for DACA are based on KFF analysis of Current Population Survey Annual Social and Economic Supplement (CPS-ASEC) 2022 data. For this analysis, KFF drew on the methods underlying the 2013 analysis by the State Health Access Data Center (SHADAC) and the recommendations made by Van Hook et al., which uses the Survey of Income and Program Participation (SIPP), to develop a model that predicts immigration status for each person in the sample. It then applies the model to a second data source, controlling to state-level estimates of total undocumented population as well as the undocumented population in the labor force from the Pew Research Center. For more details on the immigration imputation used in this analysis, see here.
Undocumented individuals were then identified as likely eligible for DACA if they met age, education, and length of residence requirements, including being between ages 15 to 41 (as of 2022, the year of data being analyzed); being enrolled in school, having completed high school or an equivalent, or being a veteran; and having entered the U.S. prior to 2007 and before the age of 16. Our estimates of the DACA-eligible population differ from administrative data on the DACA population on several demographic characteristics. Most notably, our estimated DACA-eligible population is older and less likely to be female.