The Implications of COVID-19 for Mental Health and Substance Use
Note: This brief was updated on March 20, 2023 to incorporate the latest available data.
Concerns about mental health and substance use remain elevated three years after the onset of the COVID-19 pandemic, with 90% of U.S. adults believing that the country is facing a mental health crisis, according to a recent KFF/CNN survey. The pandemic has affected the public’s mental health and well-being in a variety of ways, including through isolation and loneliness, job loss and financial instability, and illness and grief.
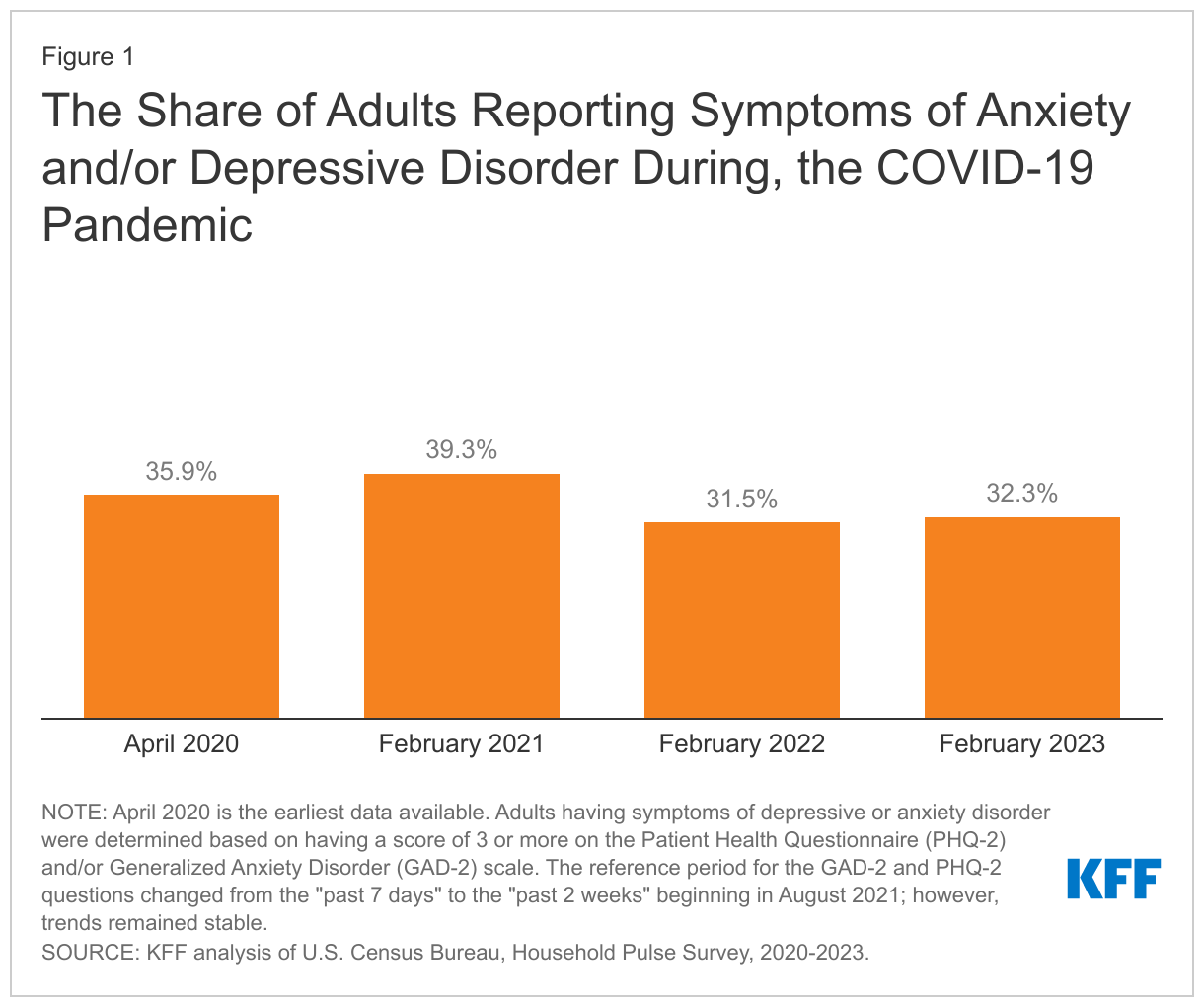
Over the course of the pandemic, many adults reported symptoms consistent with anxiety and depression, with approximately four in ten adults reporting these symptoms by early 2021, before declining to approximately three in ten adults as the pandemic continued (Figure 1). Additionally, drug overdose deaths have sharply increased – largely due to fentanyl – and after a brief period of decline, suicide deaths are once again on the rise. These negative mental health and substance use outcomes have disproportionately affected some populations, particularly communities of color and youth. As the end of the declaration of the public health emergency nears – on May 11, 2023 – many people continue to grapple with worsened mental health and well-being and face barriers to care.
This brief explores mental health and substance use during, and prior to, the COVID-19 pandemic. We highlight populations that were more likely to experience worse mental health and substance use outcomes during the pandemic and discuss some innovations in the delivery of services. We analyze and present findings using the most recent data available at the time of this publication – including the Household Pulse Survey and the CDC WONDER database. Key takeaways include:
- Symptoms of anxiety and depression increased during the pandemic and are more pronounced among individuals experiencing household job loss, young adults, and women. Adolescent females have also experienced increased feelings of hopelessness and sadness compared to their male peers.
- Deaths due to drug overdose increased sharply across the total population coinciding with the pandemic – and more than doubled among adolescents. Drug overdose death rates are highest among American Indian and Alaska Native people and Black people.
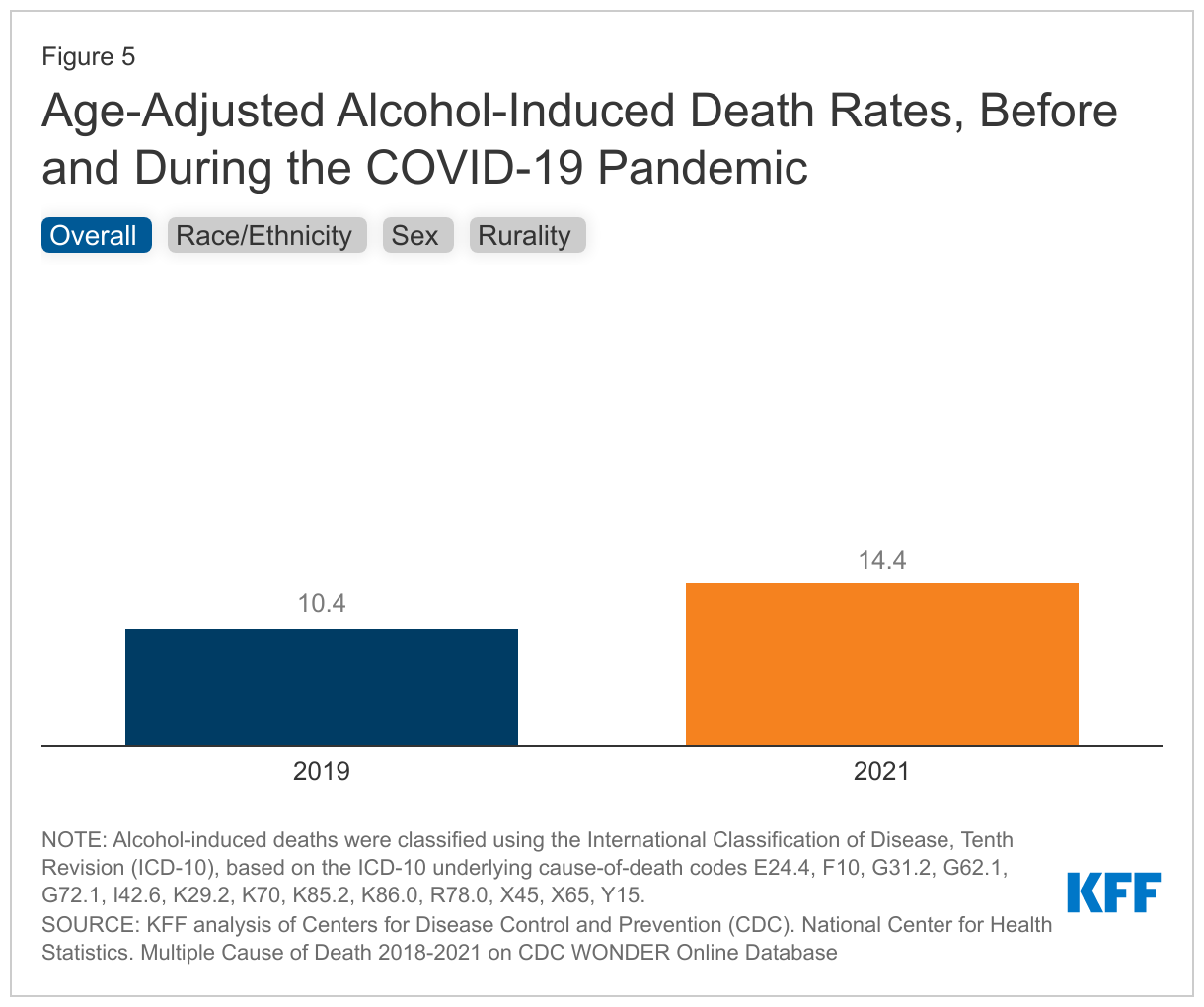
- Alcohol-induced death rates increased substantially during the pandemic, with rates increasing the fastest among people of color and people living in rural areas.
- After briefly decreasing, suicide deaths are on the rise again as of 2021. From 2019 to 2021, many communities of color experienced a larger growth in suicide death rates compared to their White counterparts. Additionally, self-harm and suicidal ideation has increased faster among adolescent females compared to their male peers.
- Several changes have been implemented in the delivery of mental health and substance use services since the onset of the pandemic, including the utilization of telehealth, steps to improve access to treatment for opioid use disorders, expansion of school-based mental health care, and the rollout of the 988 crisis line. As the public health emergency declaration comes to an end, it is possible that some of these changes will be interrupted.
Prevalence of Mental Illness and Substance Use During the Pandemic
Anxiety and depression
The pandemic was associated with a high prevalence of anxiety and depression symptoms in adults. Research suggests that these symptoms increased during the pandemic, but the extent of this increase is unclear.1 Throughout the pandemic, symptoms of anxiety and depression have been more pronounced among several populations.
For example, individuals experiencing household job loss were more likely than their counterparts to report symptoms of anxiety and/or depression (53% vs. 30%) in February 2023 (Figure 2). Job loss and unemployment – which have long been associated with adverse mental health outcomes – increased substantially early on in the pandemic.
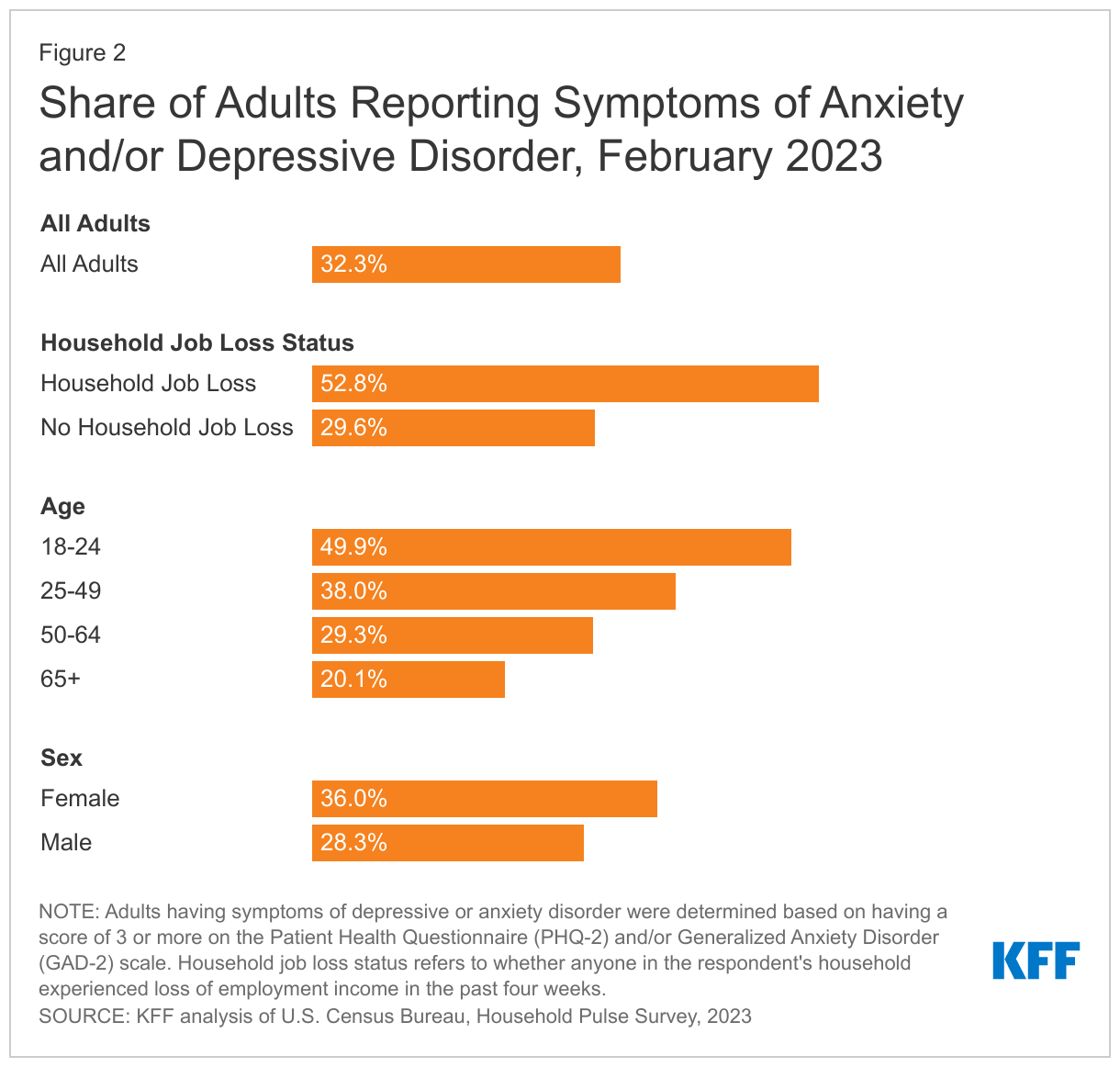
Fifty percent of young adults (ages 18-24) reported anxiety and depression symptoms in 2023, making them more likely than older adults to experience mental health symptoms (Figure 2). Young adults have experienced a number of pandemic-related consequences – such as closures of universities, transitioning to remote work, and loss of income or employment – that may contribute to poor mental health. Additionally, young adults in college settings may encounter increased difficulty accessing treatment.
Symptoms of anxiety and/or depression were also elevated among women (36%) compared to men (28%) in February 2023 (Figure 2). Even before the pandemic, women were more likely than men to report mental health disorders, including serious mental illness.
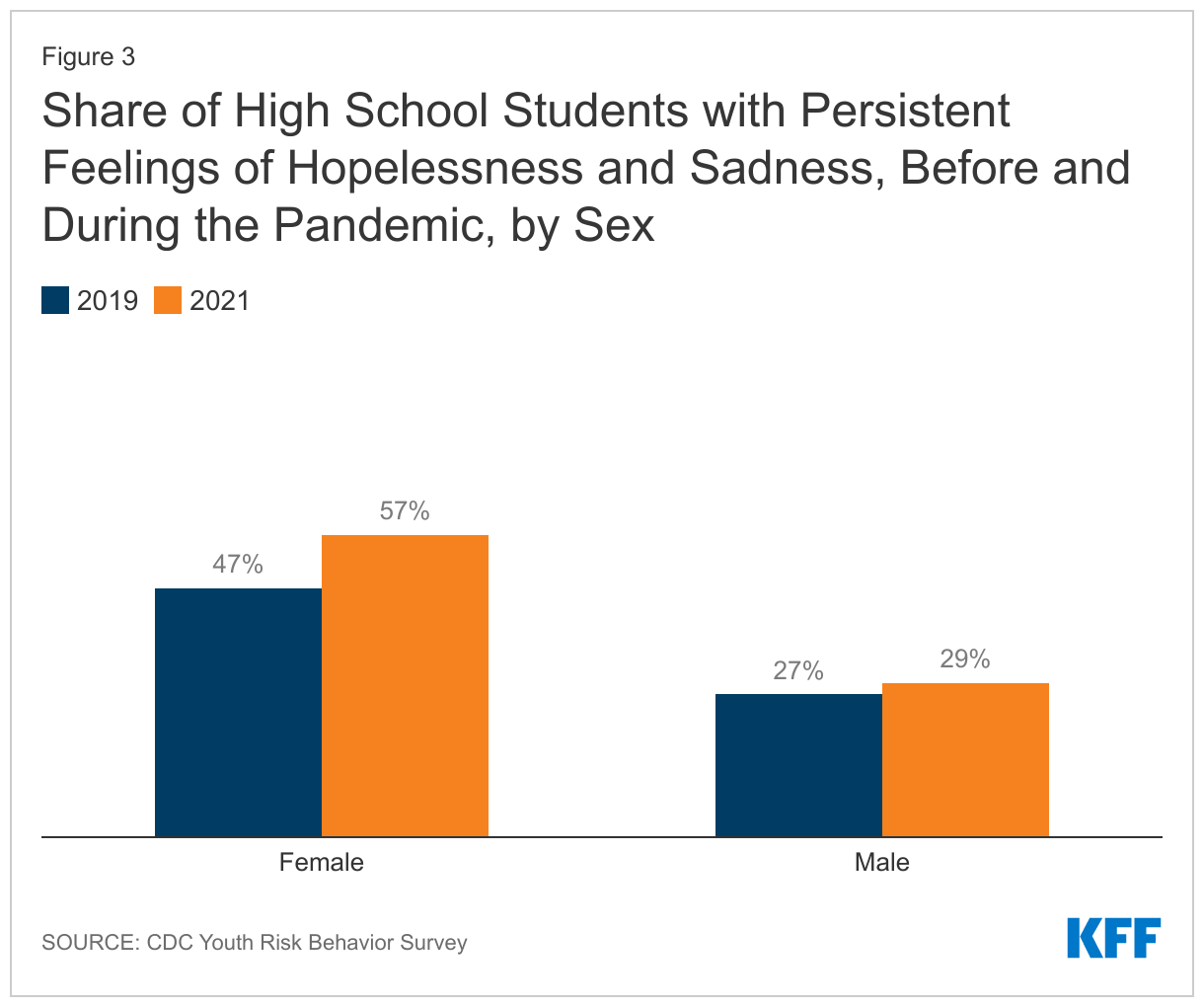
Concerns about youth mental health further increased with the onset of the pandemic and the recent uptick in gun violence. In a recent KFF/CNN survey, roughly half of parents (47%) said the pandemic had a negative impact on their child’s mental health, including 17% who said it had a “major negative impact”. Poor mental health has been more pronounced among adolescent females in particular. As shown in Figure 3, the gap in the share of adolescent females and males reporting feelings of hopelessness and sadness – symptoms indicative of depressive disorder – widened from 2019 (47% vs. 27%, respectively) to 2021 (57% vs. 29%, respectively). Many female adolescents also reported adverse experiences in 2021, which can negatively impact mental health.
Substance use and deaths
The pandemic has coincided with an increase in substance use and increased death rates due to substances. In 2021, there were over 106,600 deaths due to drug overdose in the U.S. – the highest on record. This spike in deaths has primarily been driven by substances laced with synthetic opioids, including illicitly manufactured fentanyl.
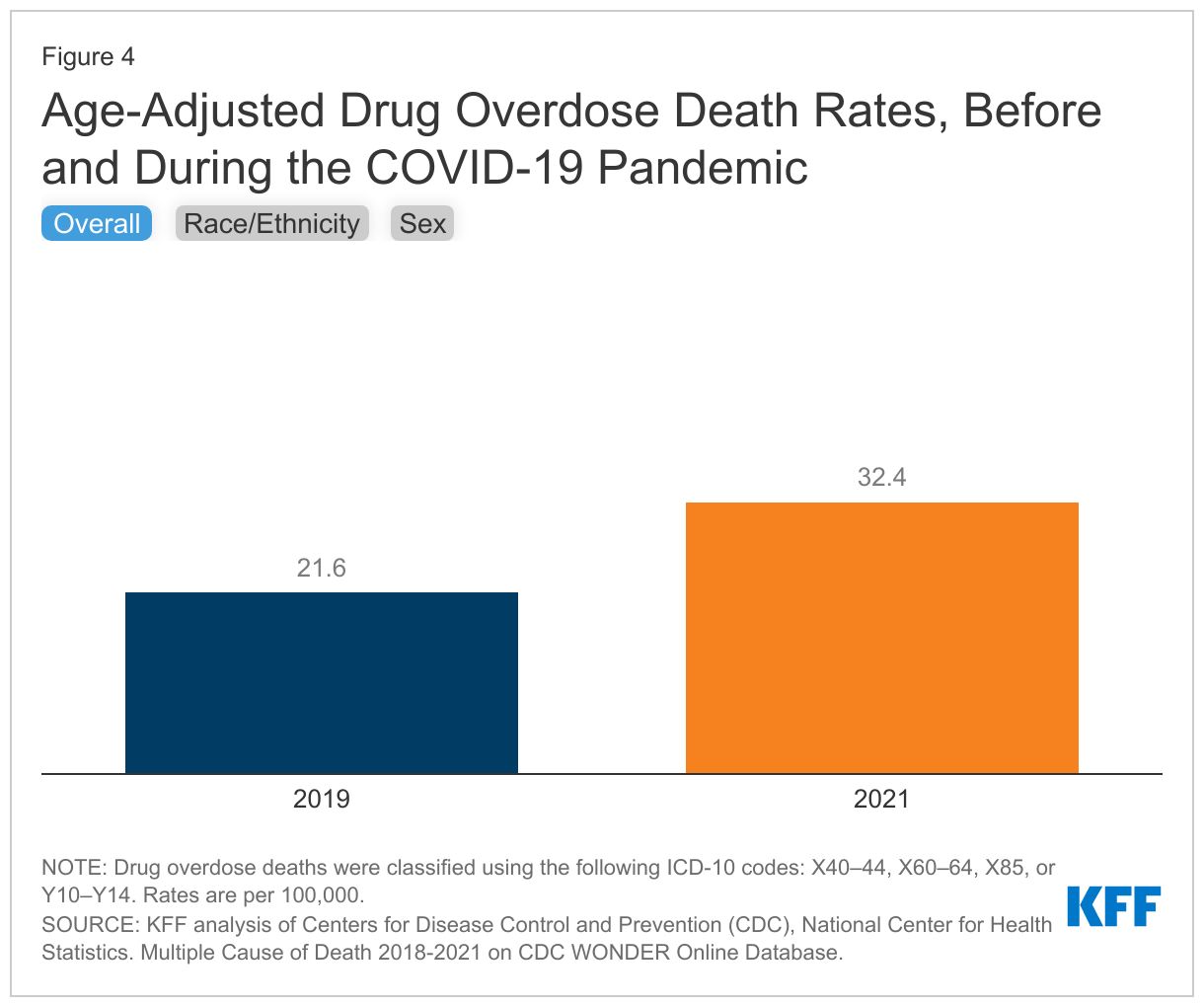
Further, the overall drug overdose death rate rose by 50% during the pandemic (Figure 4), but varied across states. While drug overdose death rates increased across all racial and ethnic groups, the increases were larger for people of color compared to White people. White people continue to account for the largest share of deaths due to drug overdose per year, but people of color are accounting for a growing share of these deaths over time. In 2021, the highest drug overdose death rates were among American Indian Alaska Native (AIAN) people (56.6 per 100,000), Black people (44.2 per 100,000), and White people (36.8 per 100,000) (Figure 4). Differences in drug overdose deaths by sex were also exacerbated during the pandemic. As shown in Figure 4, the gap in the drug overdose death rates between males and females increased from 2019 (29.6 vs. 13.7 per 100,000, respectively) to 2021 (45.1 vs. 19.6 per 100,000, respectively).
Research suggests that substance use among adolescents has declined, yet drug overdose deaths have sharply increased among this population, primarily due to fentanyl-laced substances. Among adolescents, drug overdose deaths have more than doubled from 2019 (282 deaths) to 2021 (637 deaths) following a period of relative stability.2 Male, Black, and Hispanic youth have experienced the highest increases in deaths due to drug overdose.
During the pandemic, excessive drinking increased along with alcohol-induced deaths. Alcohol-induced death rates increased by 38% during the pandemic, with rates the highest and increasing the fastest among AIAN people. AIAN people died of alcohol-induced causes at a rate of 91.7 per 100,000 in 2021, six times more than the next highest group – Hispanic people at a rate of 13.6. Black people also experienced significant increases in alcohol-induced deaths during COVID, with rates increasing more than 45% (Figure 5). Both rural and metropolitan areas experienced an increase in alcohol-induced deaths during the pandemic, but rural areas saw the largest increase (46% increase compared to 36%).
Suicidal ideation and deaths
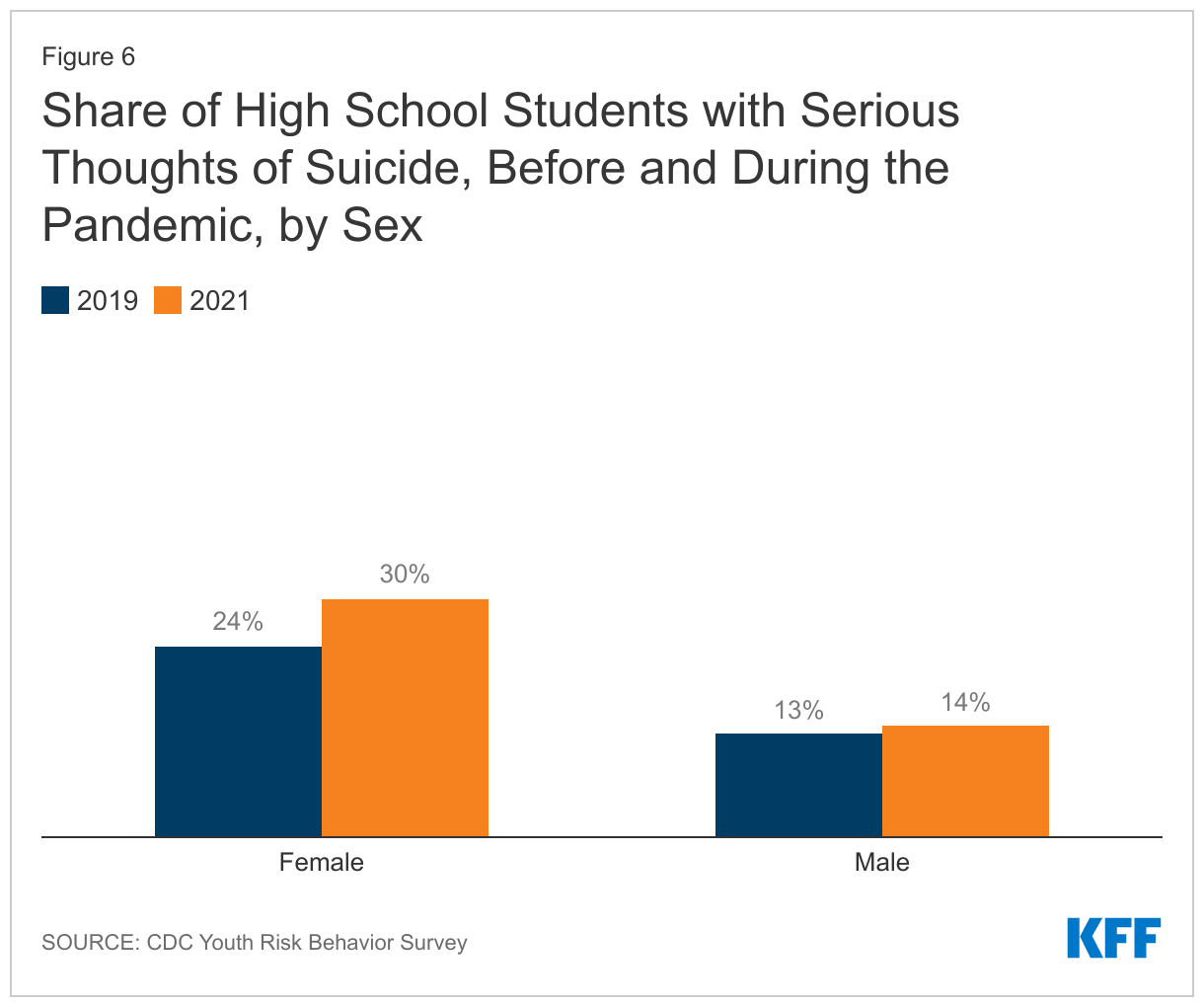
Concerns about suicidal ideation and suicide deaths have also grown during the pandemic. Notably, self-harm and suicidal ideation has increased among adolescent females. Thirty percent of adolescent females seriously considered attempting suicide in 2021 compared to 14% of their male peers (Figure 6). Other analyses found that as the pandemic progressed, emergency department visits for suicide attempts increased among adolescents, primarily driven by females.
Suicide deaths in the U.S. began to increase in 2021 after briefly slowing in 2019 and 2020, although some research suggests that some suicides may be misclassified as drug overdose deaths since it can be difficult to determine whether drug overdoses are intentional. From 2019 to 2021, many communities of color experienced a larger growth in suicide death rates compared to their White counterparts.3 In 2021, suicide deaths by firearm accounted for more than half (55%) of all suicides in the U.S., but varied greatly across states.
The pandemic has also raised concerns about mental illness, suicide, and substance use among other populations. Essential workers and people with chronic health conditions may have experienced worsened mental health due to increased risk of contracting or becoming severely ill from COVID-19. Many of these individuals, particularly those with chronic conditions, were already at-risk of experiencing poor mental health outcomes prior to the pandemic. LBGT+ people have historically faced mental health problems at higher rates than their non-LGBT+ peers. The pandemic has continued to negatively impact LBGT+ people’s mental health in disproportionate ways. In addition, people experiencing prolonged COVID-19 symptoms, or long COVID, may be more likely to develop new mental health conditions or to experience worsening of existing ones.
Changes in the Delivery of Mental Health and Substance Use Disorder Services
Leading up to the pandemic, many people faced barriers accessing mental health and substance use disorder services for reasons including costs, not knowing where to obtain care, limited provider options, and low rates of insurance acceptance. Young adults, Black adults, men, and uninsured people were less likely to receive services compared to their peers.
In recent years, access to care barriers may have worsened due to pandemic disruptions and closures, workforce shortages, and increased demand for services. In response to growing need, some policies and strategies were implemented to address access challenges, such as growth of telehealth, improved access to opioid use disorder treatment, the expansion of school-based mental health services, and the rollout of 988; however, challenges remain.
The delivery of mental health and substance use disorder services via telehealth grew sharply during the pandemic. By 2021, nearly 40% of all mental health and substance use disorder outpatient visits were delivered through telehealth. These behavioral health services via telehealth have also been more utilized in rural areas than urban areas during the pandemic. This underscores the role telehealth can play in improving access to behavioral health services in rural areas, which often face additional provider and resource shortages. Further, community health centers – which serve low-income and medically underserved communities, including communities of color and those in rural areas – experienced a large increase in behavioral health visits in 2021, largely driven by telehealth. During the pandemic, many state Medicaid programs expanded coverage of behavioral health telehealth services. This includes broadening the range of behavioral health services offered virtually and allowing for more provider types to be reimbursed for telehealth services. Many state Medicaid programs reported that telehealth has helped maintain and expand access to behavioral services during the pandemic. Some private payers have also improved coverage for mental health and substance use services by removing pre-pandemic telehealth coverage restrictions. Although telehealth can broaden access to care, in-person care may be necessary or preferred for some or for those experiencing challenges with technology and digital literacy.
As opioid-related overdose deaths have sharply increased, measures to improve access to treatment have been implemented. Following the onset of the pandemic, the federal government allowed for new flexibilities in opioid use disorder (OUD) treatment to ease access barriers, for example allowing for take-home methadone doses and covering telehealth treatment, and the Biden administration has proposed making these flexibilities permanent. Further, the 2023 Consolidated Appropriations Act eliminated the X-waiver requirement for prescribing buprenorphine, which substantially increases the number of providers who are authorized to prescribe buprenorphine to treat OUD. Voluntary guidelines for providers have also been issued to help reduce opioid overprescribing and misuse. At the same time, the Drug Enforcement Agency recently proposed returning to previous rules that required in-person visits before prescribing controlled substances to patients via telehealth, though there are some exceptions.
In response to growing mental health concerns among youth, integration of mental health services in school-based settings became a priority. Recent legislation aims to expand mental health care in schools – a setting that is easily accessible by children and adolescents. Specifically, legislation provides funding to expand and train mental health providers in schools; implement suicide, drug, and violence prevention programs; and provide trauma support services, among others. Further, recognizing Medicaid’s importance in covering and financing behavioral health care for children, CMS is now required to provide updated guidance on how to support and expand school-based behavioral health services. The recently passed Consolidated Appropriations Act (CAA) continues to build on prior pandemic-era legislation that promotes access to behavioral health care for children. For example, to ensure more stable coverage for low-income children the CAA requires states to provide 12 months of continuous eligibility for children in Medicaid and CHIP.
An easy-to-remember number for the suicide and behavioral health crisis hotline, 988, was launched in 2022. On July 16, 2022, the federally mandated crisis number, 988, became available to all landline and cell phone users, providing a single three-digit number to access a network of over 200 local and state funded crisis centers where those in need may receive crisis counseling, resources and referrals. After 988 implementation, national answer rates increased alongside increases in call volume. Long-term sustainable funding of local 988 crisis call centers remains uncertain in many states. In addition to 988, some states are developing behavioral health crisis response systems, such as mobile crisis or crisis stabilization units, which will enable a specialized behavioral health response for behavioral health crises that require intervention. The CAA included provisions aimed at strengthening and evaluating 988 and the developing behavioral health crisis continuum.
Despite steps taken to improve the delivery of mental health and substance use services, challenges remain. Provider workforce challenges are widespread, with nearly half of the U.S. population (47%) living in a mental health workforce shortage area. Shortages may contribute to access challenges and contribute to increases in psychiatric boarding in emergency rooms. Additionally, provider network directories are often outdated, further contributing to access challenges. While recent legislation has taken steps in response – including funding for at least 100 new psychiatry residency positions, grants for mental health peer support providers, and improvements to provider directories through the CAA – these are relatively small measures in the face of big access challenges. The lack of a diverse mental health care workforce may contribute to limited mental health treatment among people of color. Separately, even with insurance coverage, individuals with mental health needs face challenges accessing care. While Medicaid enrollees have limited out-of-pocket costs there is variation in who is eligible and the range of services covered across states. Additionally, the end of Medicaid’s continuous enrollment provision – on March 31, 2023 – could result in millions of disenrollments over the next year which could disrupt access to behavioral health services. Among private insurance enrollees, enrollees, with mental illness face high out-of-pocket costs; and these costs vary substantially across states. While most adults with mental illness have private insurance, rates of mental illness and substance use disorders are most prevalent among nonelderly adults with Medicaid.
Looking Ahead
Although steps have been taken to address negative mental health impacts stemming from the pandemic, mental health and substance use concerns remain elevated. Heightened racism and increasing gun violence may also contribute to poor mental health outcomes. Further, negative mental health impacts have been more pronounced among several populations, including communities of color, young adults and children – populations which have historically experienced increased barriers to care. Additionally, despite renewed discussions and new federal grants for state parity enforcement under the CAA, challenges with mental health parity persist – including lack of clarity on specific protections, low compliance rates, and slow federal enforcement. Finally, the COVID-19 public health emergency will end in May 2023, which may at least partially unravel steps taken toward delivering mental health services via telehealth and improving access to substance use disorder services.
History has shown that the mental health impact of disasters outlasts the physical impact, suggesting today’s elevated mental health needs will continue well beyond the coronavirus outbreak itself. As we emerge from the COVID-19 pandemic and the federal public health emergency draws to an end, it will be important to consider how the increased need for mental health and substance use services may persist long term, even as new cases and deaths due to COVID-19 hopefully subside.
This work was supported in part by Well Being Trust. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Endnotes
The Household Pulse Survey (HPS) is a rapid response survey that has provided real-time data during the pandemic and includes a 4-item Patient Health Questionnaire (PHQ-4) anxiety and depression screening scale. In order to understand how the prevalence of anxiety and depression may have shifted in the adult population during the onset of the pandemic, mental health estimates from HPS were compared against pre-pandemic data from the National Health Interview Survey, which also includes the 4-item PHQ scale. However, recent research finds that these comparisons may not be reliable given lower response rates and over estimation in HPS; and are no longer included in this brief.
KFF analysis of Centers for Disease Control and Prevention, Wide-ranging Online Data for Epidemiologic Research (WONDER). Accessed at: https://wonder.cdc.gov/mcd-icd10-expanded.html
KFF analysis of Centers for Disease Control and Prevention, Wide-ranging Online Data for Epidemiologic Research (WONDER). Accessed at: https://wonder.cdc.gov/mcd-icd10-expanded.html