Five Key Findings on Mental Health and Substance Use Disorders by Race/Ethnicity
Summary
Over two years into the COVID-19 pandemic, many people continue to grapple with worsened mental health associated with the prolonged impact of the pandemic, including social distancing, income loss, and death and illness. In 2020, 33% of all nonelderly adults reported having a mental illness or substance use disorder. Drug overdose deaths have increased over time – particularly during the pandemic – and these increases have disproportionately affected people of color. Following a period of increases, suicide deaths slowed in 2019 and 2020, although they have increased faster among people of color than White people. Drawing on a series of recent KFF analyses, this brief presents five key findings on mental health and substance use concerns by race/ethnicity. It finds:
- Rates of death by suicide are rising faster among people of color compared to their White counterparts.
- The recent rise in deaths associated with drug overdoses has disproportionately affected people of color.
- Overall rates of mental illness and substance use disorder are lower for people of color compared to White people but may be underdiagnosed among people of color.
- People of color have experienced worsening mental health during the pandemic.
- People of color face disproportionate barriers to accessing mental health care.
Rapidly rising rates of deaths by suicide and drug overdose among people of color, along with disproportionate impacts of the COVID-19 pandemic, further underscore inequities in access to mental health care and treatment and highlight the importance of centering equity in diagnostics, care, and treatment.
Key Findings
Rates of death by suicide are rising faster among people of color compared to their White counterparts.
Between 2010 and 2020, Black and American Indian or Alaska Native (AIAN) people experienced the largest increases in rates of death by suicide (Figure 1). AIAN and White people continue to experience the highest rates of deaths by suicide compared to all other racial and ethnic groups (23.9 and 16.8 per 100,000 in 2020, respectively). However, people of color are experiencing the largest increases in rates of death by suicide. AIAN and Black people experienced the largest absolute increases in suicide death rates (7.0 and 2.3 percentage points, respectively) from 2010 to 2020 (Figure 1). Moreover, Black and Hispanic people had larger percentage increases in their suicide death rates compared to White people over the same period (at 43% and 27%, respectively, compared to 12%).
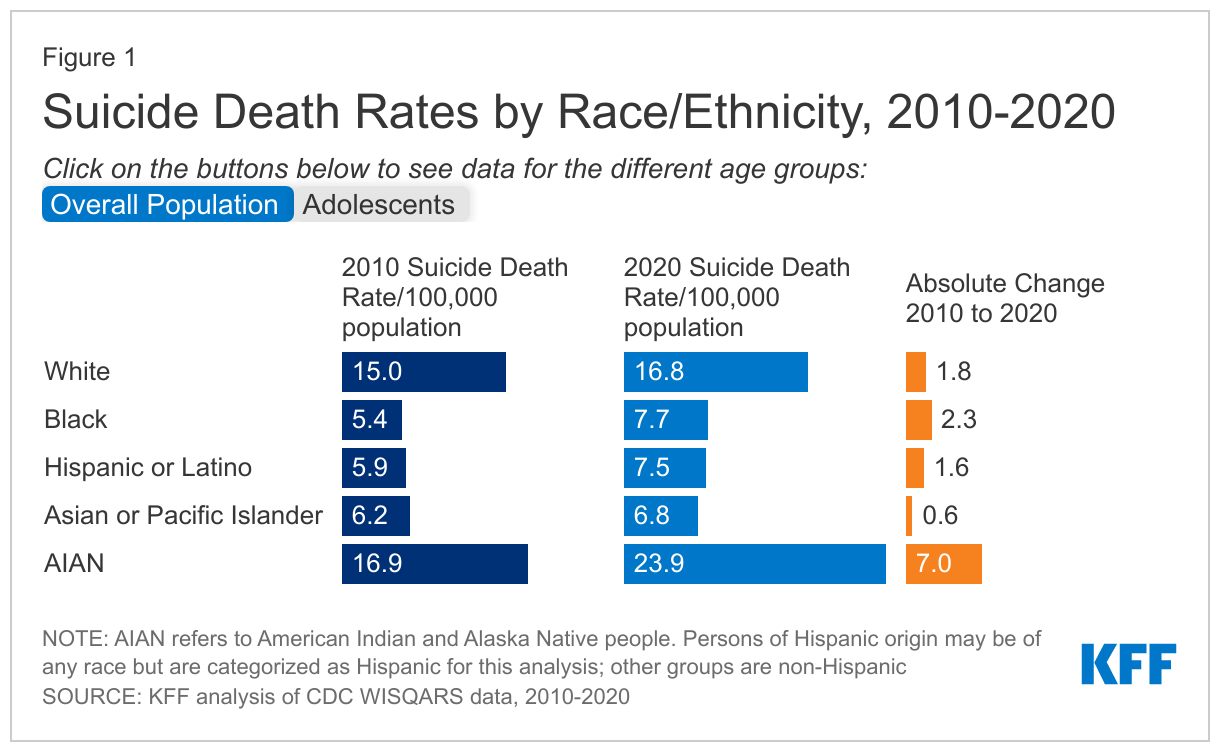
Between 2010 and 2020, suicide-related death rates among adolescents more than doubled for Asian adolescents and nearly doubled for Black and Hispanic adolescents (Figure 1). However, similar to the overall population data, AIAN adolescents accounted for the highest rates of deaths by suicide, over three times higher than White adolescents (22.7 vs. 6.3 per 100,000). In contrast, Black, Hispanic, and Asian adolescents had lower rates of suicide deaths compared to their White peers. Suicide remains the second leading cause of death among adolescents overall.
The recent rise in deaths associated with drug overdoses has disproportionately affected people of color.
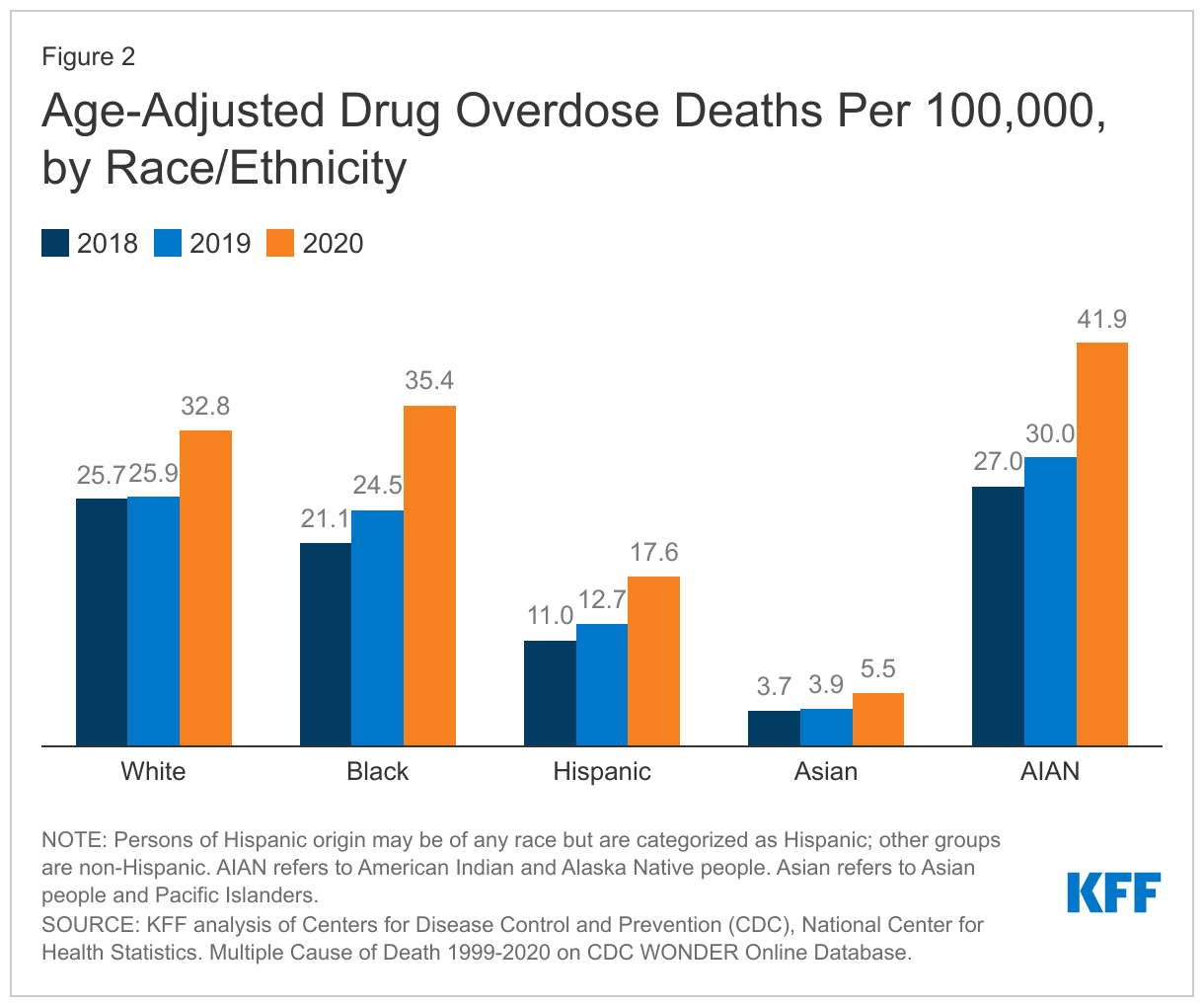
Drug overdose death rates increased across all racial and ethnic groups in recent years, but these increases were larger for people of color compared to their White counterparts. Reflecting these increases, drug overdose death rates among Black people surpassed rates of White people by 2020 (35.4 versus 32.8 per 100,000) (Figure 2). However, AIAN people continued to experience the highest rates of drug overdose deaths (41.9 per 100,000 in 2020) compared with all other racial and ethnic groups. Among adolescents, deaths due to drug overdose nearly doubled in 2020 and disproportionately affected adolescents of color. Further, it is possible that deaths by suicide are being undercounted due to misclassifications as drug overdose deaths. Fentanyl-related deaths, which have accounted for many drug overdose deaths during the pandemic, may be disproportionately affecting Black communities.
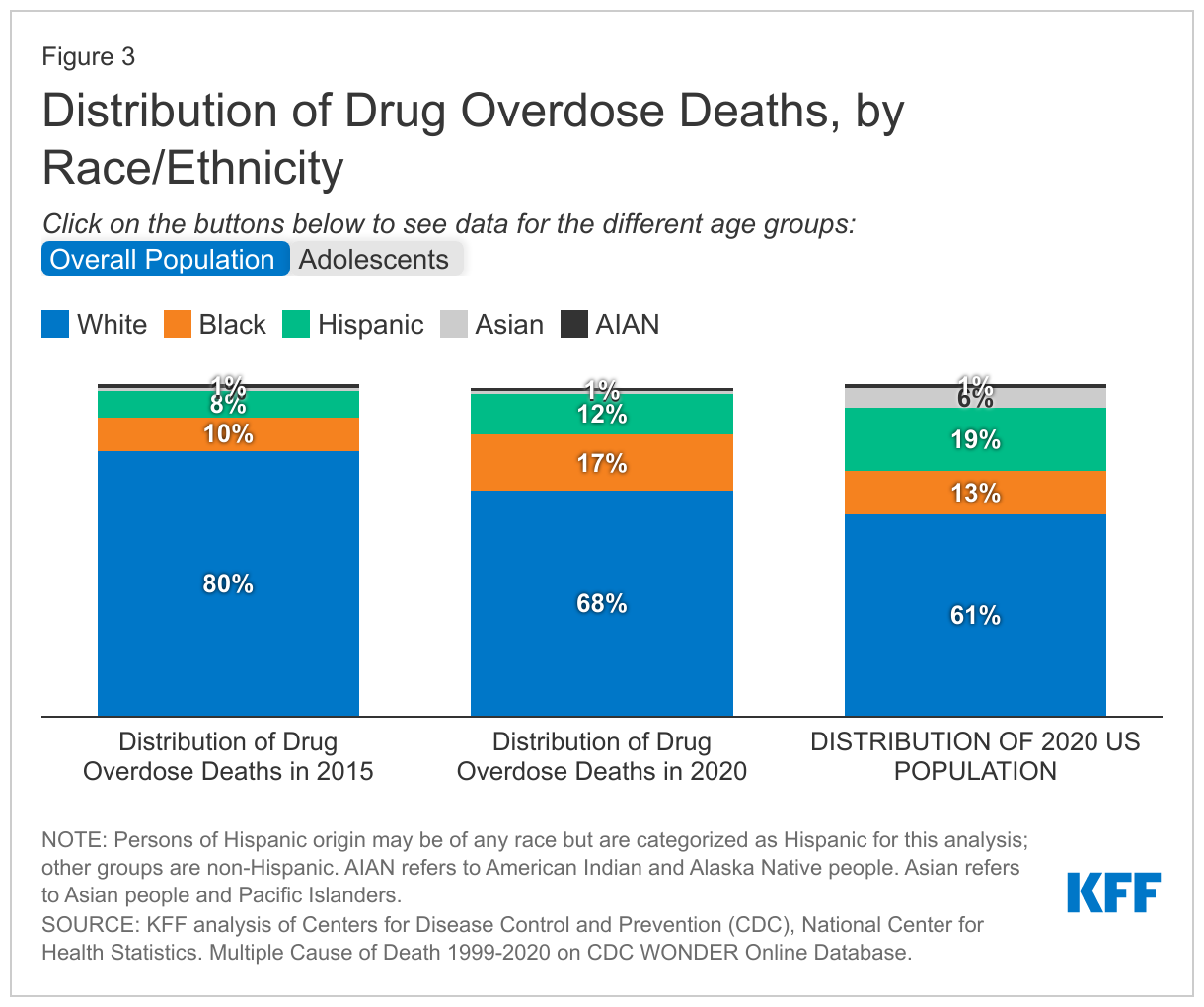
White people continue to account for the largest share of deaths due to drug overdose, but people of color are accounting for a growing share of these deaths over time. Between 2015 and 2020, the share of drug overdose deaths among White people fell, while at the same time the shares of these deaths among Black and Hispanic people rose. As a result of this increase, Black people accounted for a disproportionate share of drug overdose deaths relative to their share of the total population in 2020 (17% vs. 13%) (Figure 3). Similarly, reflecting an increase in deaths over the period, Hispanic adolescents accounted for a disproportionate share of drug overdose deaths relative to their share of the population as of 2020 (30% vs. 25%). These recent trends are contributing to emerging disparities in drug overdose deaths among some people of color, which may worsen if they continue.
Overall rates of mental illness and substance use disorder are lower for people of color compared to White people but may be underdiagnosed among people of color.
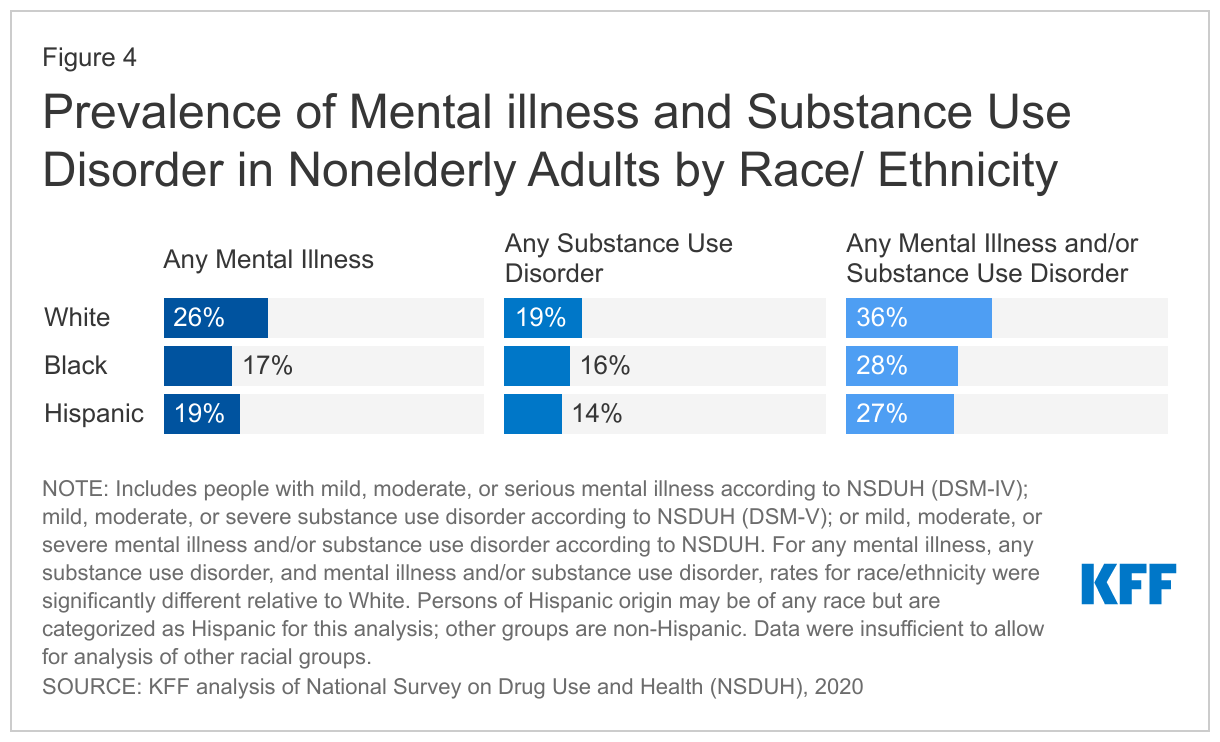
In 2020, people of color were generally less likely to report experiencing any mental illness or substance use disorders compared to their White peers. Just over a quarter of Black (28%) and Hispanic (27%) nonelderly adults reported having a mental illness or substance use disorder in 2020, compared to 36% of White nonelderly adults (Figure 4). Though overall mental health and substance use disorders were lower in people of color, other research found that the share of nonelderly adults reporting moderate or severe anxiety and/or depression were similar among White (9%), Black (9%), and Hispanic (8%) adults in 2019. Among adolescents, symptoms of anxiety and/or depression were higher among White (19%) and Hispanic (15%) adolescents and lower among Black adolescents (11%) in 2020.
A lack of culturally sensitive screening tools that detect mental illness, coupled with structural barriers may contribute to underdiagnosis of mental illness among people of color. Moreover, symptoms of mental illness or substance use disorder among people of color are more likely to be labeled as disruptive or criminal compared to their White counterparts. This practice can occur in childhood where behaviors that may be characterized as a mental health concern among White children are considered disruptive and penalized among children of color and may encourage underreporting of mental health issues. This labeling may, in turn, result in a disproportionate number of Black people being diverted into the justice system instead of treatment centers.
People of color have experienced worsening mental health during the pandemic.
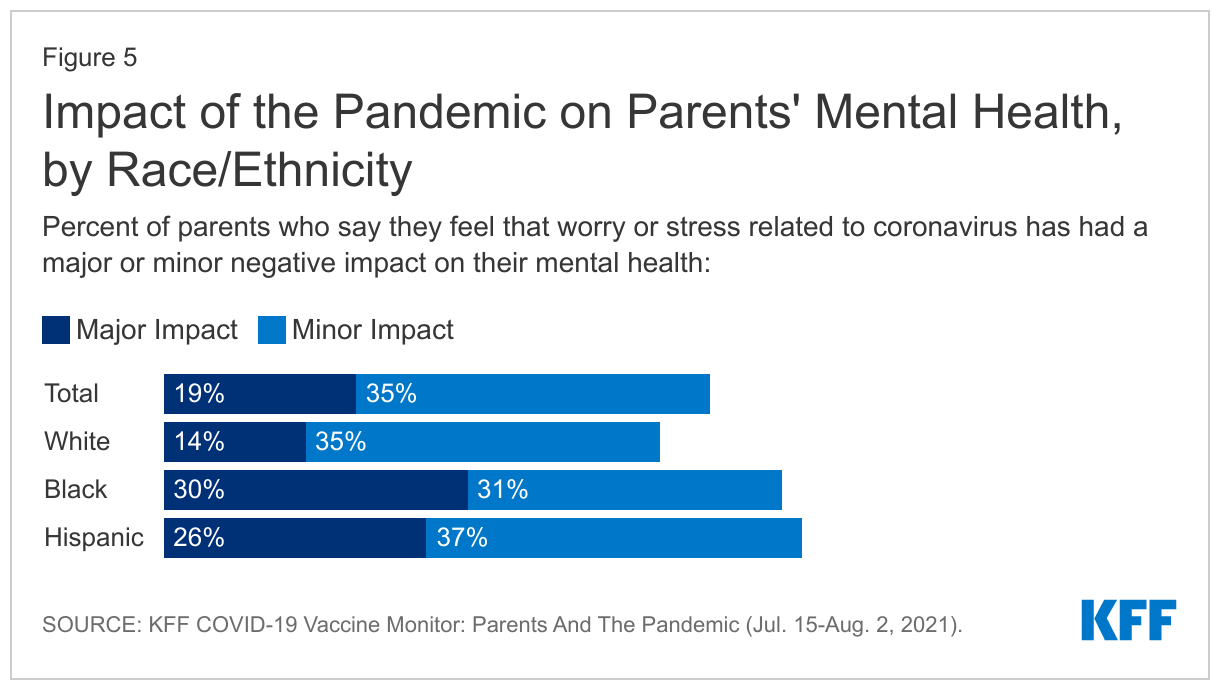
The COVID-19 pandemic has disproportionately impacted people of color in multiple ways that contribute to poor mental health (Figure 5). Compared to their White peers, people of color have experienced higher rates of COVID-19 infection and death and greater financial challenges, including difficulty paying household bills, during the pandemic, which may negatively impact their mental health. KFF COVID-19 Vaccine Monitor Survey data from late 2021 found that at least half of White, Hispanic, and Black adults said the pandemic negatively impacted their mental health. Additional KFF survey data suggests that the mental health of Black and Hispanic parents has been particularly negatively impacted. At least six in ten Black and Hispanic parents say stress related to the pandemic had a negative impact on their mental health compared to less than half of White parents (Figure 5). Further, Black and Asian people have reported negative mental health impacts due to heightened anti-Black and anti-Asian racism and violence during the pandemic.
People of color face disproportionate barriers to accessing mental health care.
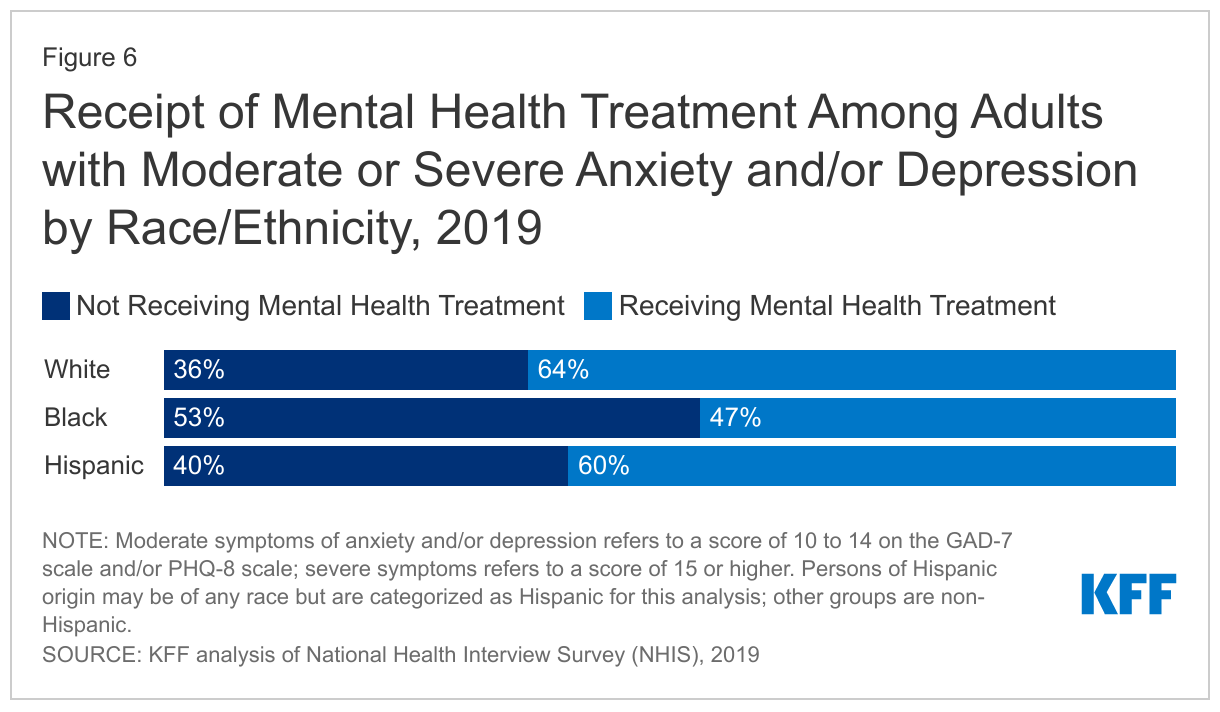
Leading up to the pandemic, people of color faced disparities in access to and receipt of mental health care, which may have worsened during the pandemic. While similar shares of White, Black, and Hispanic adults reported moderate to severe symptoms of anxiety and/or depression in 2019, a much larger share of Black adults (53%) with these symptoms did not receive care compared to their White (36%) counterparts (Figure 6). Other research shows Black and Hispanic people with mental illness or substance use disorder are less likely to receive treatment compared to the overall population.
People of color face increased barriers to accessing mental health care due to a range of factors both within and beyond the health care system. Research suggests that structural inequities may contribute to disparities in use of mental health care, including lack of health insurance coverage and financial and logistical barriers to accessing care, stemming from broader inequities in social and economic factors. These barriers may have been compounded by the pandemic, which had disproportionate negative financial impacts on people of color.
Lack of a diverse mental health care workforce, the absence of culturally informed treatment options, and stereotypes and discrimination associated with poor mental health may also contribute to limited mental health treatment among people of color. According to the American Psychology Association’s Center for Workforce Studies, although Hispanic and Black people accounted for 30% of the U.S. population, they only made up 9% of the psychology workforce as of 2015. This may be a barrier to treatment access and retention as a recent study found that racial/ethnic concordance among patients and providers plays a significant role in patients’ having positive experiences with their care providers. Moreover, some communities have concerns about the stigma associated with mental illness. For example, Black adults may view mental health conditions as signs of personal weakness and worry about discrimination and experiencing shame in acknowledging their mental health concerns.
Looking Ahead
Drug overdose and suicide deaths among people of color are on the rise, highlighting the inequities in access to and treatment for mental health and substance use disorders. A diverse behavioral health workforce, culturally sensitive screening tools, culturally competent care, and a reduction of structural barriers to care could help improve quality of care and address longstanding barriers to mental health care for people of color. Moreover, recognizing the impacts racism and discrimination and adverse childhood experiences have on both physical and mental health could play a role in developing culturally informed responses to these events. Meanwhile, many people of color continue to experience negative impacts of the COVID-19 pandemic, including worsened mental health, which may persist even as the pandemic subsides.
This work was supported in part by Well Being Trust. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.