Medicaid Enrollment Growth: Estimates by State and Eligibility Group Show Who may be at Risk as Continuous Enrollment Ends
In the Consolidated Appropriations Act, 2023, signed into law at the end of 2022, Congress set an end to the Medicaid continuous enrollment provision on March 31, 2023 and phased down the enhanced federal Medicaid matching funds through December 2023. At the start of the pandemic, Congress enacted the Families First Coronavirus Response Act, which included a requirement that Medicaid programs keep people continuously enrolled during the COVID-19 public health emergency in exchange for enhanced federal funding. As a result, enrollment in Medicaid and the Children’s Health Insurance Program (CHIP) has grown substantially compared to before the pandemic, contributing to declines in the uninsured rate which dropped to the lowest level on record in early 2022. But, millions of people could lose coverage when the continuous enrollment provision ends, reversing recent gains in coverage.
This analysis estimates Medicaid enrollment growth by state and eligibility group between February 2020, before the pandemic, and March 31, 2023, at the end of the continuous eligibility period. These estimates can help paint a picture of the overall number and composition of enrollees who may risk coverage loss after the continuous enrollment provision ends. Prior to the continuous enrollment period, typical patterns of enrollment included disenrollments throughout the year. Some enrollees disenroll and then re-enroll within a short period of time (or “churn” in and out of Medicaid). The continuous enrollment provision halted disenrollment and churn, resulting in overall program growth. While states will need to conduct renewals for all enrollees, understanding the overall growth in enrollment and the composition of that growth can help inform understanding the range of potential outcomes as the continuous enrollment unwinds. How individual states implement the unwinding will affect the ultimate loss of coverage.
We use a combination of enrollment data from the Centers for Medicare and Medicaid Services (CMS) Performance Indicator Project (PI data), Medicaid claims data (T-MSIS data), and some state-specific data to inform the analysis (see Methods for a detailed explanation of the methods used in this analysis). While our estimates are based on the best available public data on states’ Medicaid and CHIP enrollment, they will likely differ somewhat from data maintained by individual states because we use modeling and assumptions to project enrollment through March 2023 and to allocate states’ adult enrollment across eligibility groups.
Distribution and Rates of Enrollment Growth By Eligibility Group
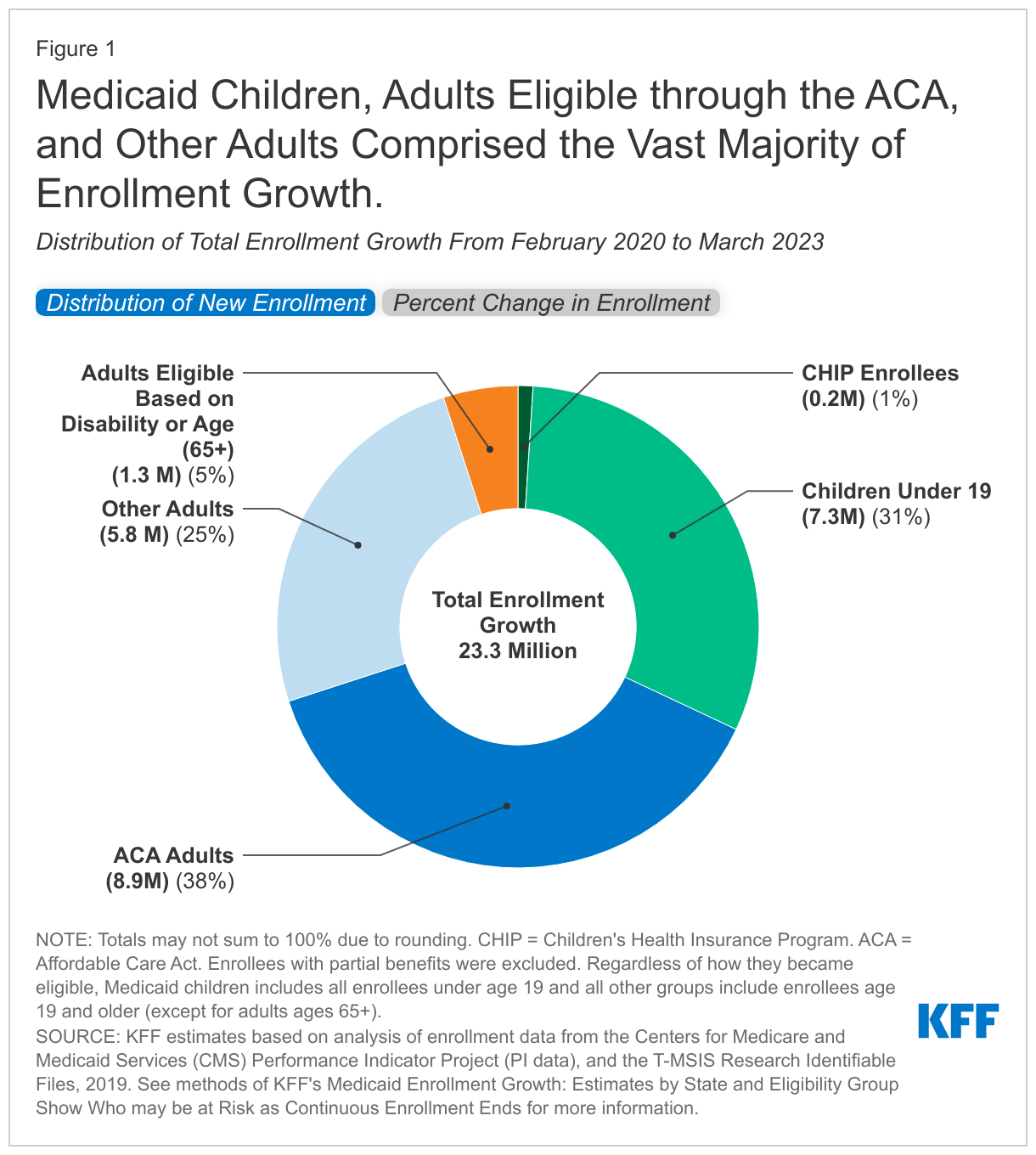
By the time the continuous enrollment period ends, we estimate that enrollment in Medicaid and CHIP will have grown by 23.3 million enrollees; nearly two-thirds of the enrollment increase is among low-income adults under age 65 (63%) and nearly one-third is among children (Figure 1, tab 1). The increase in low-income adults includes 8.9 million (38%) adults in the Affordable Care Act (ACA) Medicaid expansion group and 5.8 million (25%) other adults (mostly low-income parents) who do not qualify based on disability. Estimated enrollment increases have been smaller for adults eligible based on disability or age (1.3 million) and for CHIP enrollees (0.2 million).
Adults are experiencing the highest rates of enrollment growth during the continuous enrollment period (Figure 1, tab 2). There are very low rates of growth in CHIP, likely because the continuous enrollment provision does not apply to separate CHIP programs and some children may be moving from CHIP into Medicaid. Several factors contribute to the variation in growth rates among Medicaid eligibility groups. First, several states newly expanded Medicaid under the ACA during the continuous enrollment period resulting in high enrollment growth in those states. Adult groups and children typically experience higher rates of churn, which is when enrollees disenroll and then re-enroll within a short period of time and may occur due to temporary changes in income or administrative barriers during renewal that may result in a lapse in coverage even if an individual remains eligible for Medicaid. A recent KFF analysis found that churn rates for children more than doubled following annual renewal, signaling that many eligible children lose coverage at renewal. By halting disenrollment, the continuous enrollment provision has also halted this churning among Medicaid enrollees. People who qualify based on age or disability are historically less likely to churn on and off Medicaid as they are more likely to live on fixed income and therefore, less likely to experience changes in eligibility.
Distribution and Rates of Enrollment Growth By State
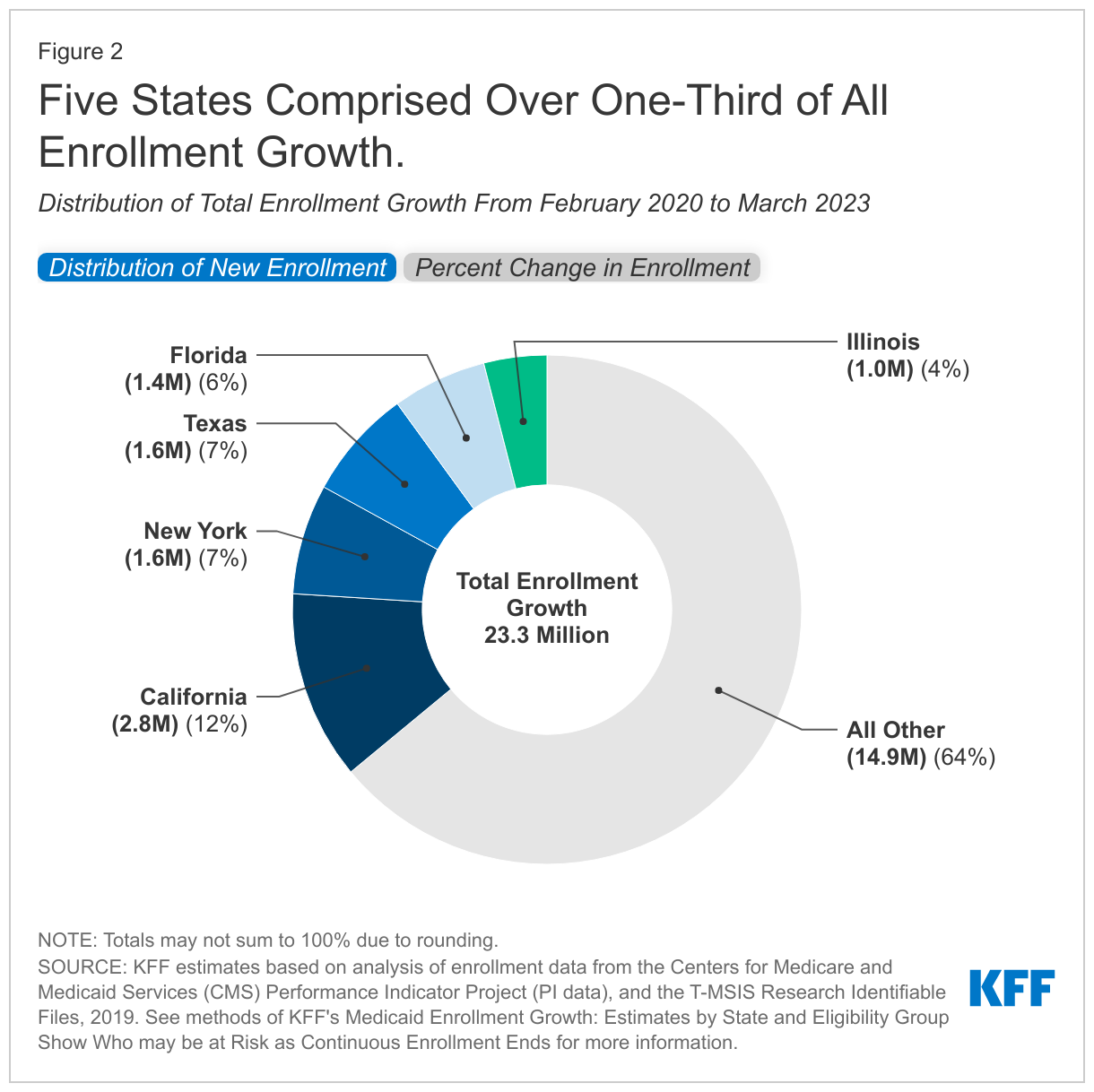
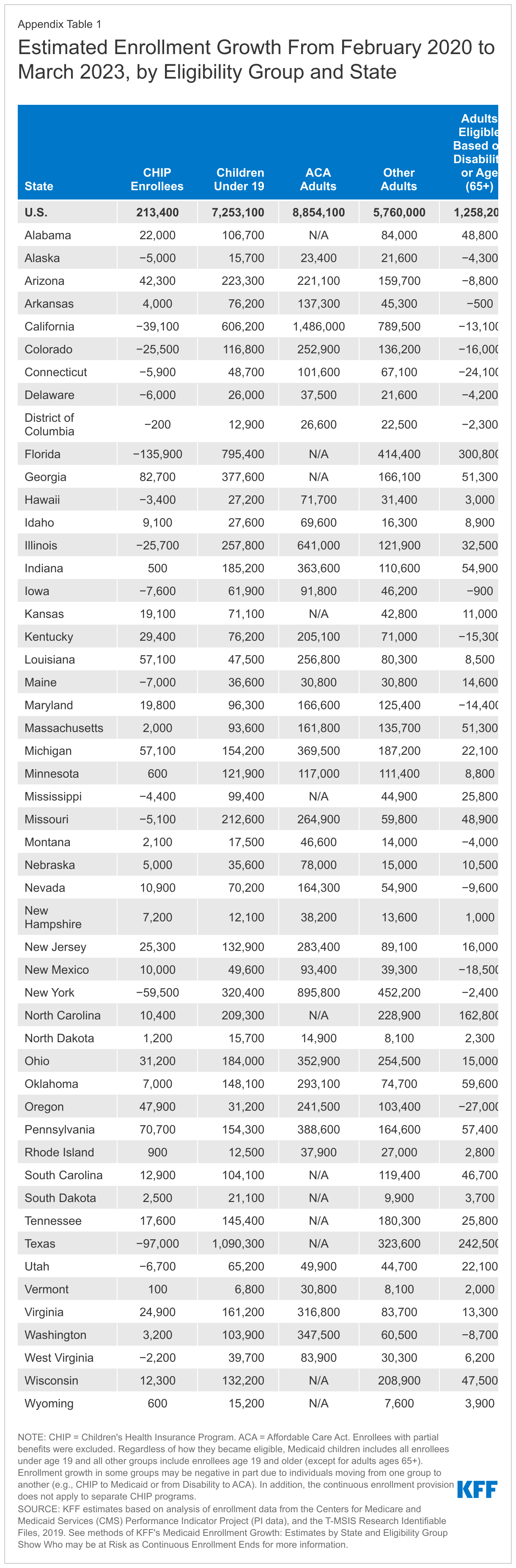
The increase in enrollment is concentrated in a small number of states with large populations and consequently large Medicaid programs. Our analysis shows that California, New York, Texas, Florida, and Illinois account for over one-third of the increase in Medicaid/CHIP enrollment (Figure 2, tab 1). Because Texas and Florida have not adopted the ACA Medicaid expansion, children and other adults account for higher percentages of enrollment gains in those states (Appendix Table 1).
Growth rates in Medicaid/CHIP enrollment vary considerably by state (Figure 2, tab 2). Rates range from 22% in Connecticut to 81% in Oklahoma. States that implemented Medicaid expansion after 2020 (Oklahoma, Missouri, Nebraska, Utah, and Idaho) have particularly high enrollment growth. Beyond Medicaid expansion, several factors may contribute to variation including:
- Churn rates prior to the pandemic (states with higher rates of churn would be likely to have faster growth on account of the continuous enrollment provision),
- The economic effects of the pandemic (in states where more people are out of work, enrollment growth may be faster), and
- State policies to conduct outreach about coverage (states that increased outreach efforts during the pandemic are likely to experience faster growth).
Looking Ahead to Unwinding
We estimate Medicaid/CHIP enrollment will reach nearly 95 million in March 2023, with enrollment growth since February 2020 accounting for one in four enrollees (Appendix Table 1). While the number of Medicaid enrollees who may be disenrolled during the unwinding period is highly uncertain, studies estimate that between 5% and 17% of current enrollees might be disenrolled. Earlier KFF analysis estimates that between 5.3 million and 14.2 million people will lose Medicaid coverage during the unwinding of the continuous enrollment provision. These projected coverage losses are consistent with, though a bit lower than, estimates from the Department of Health and Human Services (HHS) suggesting that as many as 15 million people will be disenrolled.
It is expected that the groups that experienced the most growth due to the continuous enrollment provision—ACA expansion adults, other adults, and children—will experience the largest enrollment declines. In states that haven't expanded Medicaid, many low-income parents and new mothers will be most at risk of losing coverage. HHS estimates that of those disenrolled, 6.8 million will likely still be eligible. Many children may remain eligible even if their parents are no longer eligible because most states’ income limits for children are considerably higher than for adults, and many adults eligible based on disability or age (65+) may remain eligible if they are living on fixed incomes.
Actual enrollment outcomes will vary across states depending on an array of state policy decisions including how states prioritize renewals and efforts to conduct outreach and enrollment assistance. These policies can help ensure that those who remain eligible for Medicaid are able to retain coverage, and that those who are no longer eligible can transition to other sources of coverage, particularly the ACA marketplace. Our state-by-state estimates of enrollment gains by eligibility group can help illustrate how many people are at risk of coverage loss (for enrollment increases by state and eligibility group see Appendix Table 1). As states start to resume renewal procedures for all current Medicaid enrollees, there is substantial uncertainty as to how much of the Medicaid enrollment growth during the pandemic will be sustained, how many people will transition to other coverage, and how many people could end up uninsured. Because a large share of people are covered by Medicaid, including an analysis that shows that over half of all children are covered by Medicaid and CHIP, declines in Medicaid coverage could directly impact the number of uninsured. Our recent analysis of coverage outcomes after disenrolling from Medicaid or CHIP found that nearly two-thirds of people experienced a period of uninsurance. Policies to smooth the transition from Medicaid to other coverage sources could reduce that rate as the Medicaid continuous enrollment period unwinds.
Appendix Table
Methods
Data: This analysis uses date from the Centers for Medicare and Medicaid Services (CMS) Performance Indicator Project Data (PI data) and the T-MSIS Research Identifiable Demographic-Eligibility (T-MSIS data). We used PI data from February 2020 through August 2022 and TMSIS data from 2019, Release 1.
Overview of Approach: To estimate enrollment by state and eligibility through the end of the continuous eligibility period (March 2023), we:
- Use PI data through August 2022 to estimate enrollment by subpopulation (Medicaid child, Medicaid adult, and CHIP),
- Estimate growth in Medicaid through March 2023 assuming growth continues at a similar pace to last summer, and
- Apportion enrollment among Medicaid adults to eligibility groups with T-MSIS data.
Definitions and Limitations: Our estimates are likely to be very similar to states’ PI-reported enrollment for Medicaid children, Medicaid adults, and CHP enrollees, but will differ from estimates of enrollment maintained by individual states. There are three primary reasons for these differences: the exclusion of some enrollees, the use of age-based eligibility for children, and our estimates of adult enrollment by eligibility group use a national model and our own assumptions. Specifically:
- The PI enrollment data exclude people who are not eligible for full Medicaid coverage, such as enrollees who are only eligible for coverage of Medicare premiums, family planning services, or emergency care. Such enrollees are excluded from the enrollment totals in this analysis, resulting in lower estimates of total enrollment than in data maintained by individual states.
- We define children as Medicaid enrollees who are grouped with children in the PI data, which are based on age rather than eligibility group.
- We use national growth rates from a simulation model that estimates how enrollment would change under a continuous enrollment scenario for Medicaid enrollees over age 18 in all states. There is great uncertainty as to how enrollment will change over the three-year continuous enrollment period and the simulation model relied on an 11-month observation period.
We provide more detail about each step in the details below.
1. Enrollment Among Groups: The PI data provide state enrollment for all Medicaid and CHIP adults, all children (defined as anyone under the age of 19), and everyone in CHIP.
- We removed CHIP enrollees from the Medicaid adult and child groups using T-MSIS data to estimate the percent of CHIP enrollees who are children in each state.
- Arizona did not report separate adult and child enrollment but did report total Medicaid and CHIP enrollment. We used the 2019 T-MSIS data to apportion Arizona’s enrollment among the child and adult populations.
2. Estimated Growth Through March 2023. From step 1, we had monthly enrollment by state for Medicaid adults, Medicaid children, and all CHIP enrollees.
- We projected growth through March 2023 at the national level for each subpopulation using growth rates from May 2022 through August 2022.
- We allocated national enrollment to states using the enrollment distributions from August 2022 for Medicaid adults, Medicaid children, and all CHIP enrollees.
3. Apportion Adult Enrollment to Eligibility Categories. We divided Medicaid adult enrollment into eligibility groups using the T-MSIS data. We analyzed these eligibility groups separately because enrollment patterns of adults eligible based on age or disability are different from those of other adults.
- We used the T-MSIS data from 2019 to estimate the eligibility group distribution for of adult Medicaid enrollees in each state as of February 2020.
- We used a simulation model with T-MSIS data to estimate enrollment growth by eligibility group in 2019 under a scenario in which enrollees were not disenrolled unless they died or moved out of state. This model is similar to our earlier analyses of enrollment during continuous enrollment period, but differs in that earlier analyses did not match the PI data and did include enrollees who were eligible for partial benefits.
- We restricted the analysis to adults ages 19 and older who were eligible for full Medicaid benefits and deduplicated enrollees with multiple periods of enrollment in 2019.
- We identified deaths and inter-state moves in the Demographic-Eligibility file.
- We conducted a sensitivity analysis with 2018 T-MSIS data and found similar results.
- We used the outputs from the simulation model to estimate the growth rates for each adult eligibility group during the continuous enrollment period and then scaled those eligibility-group specific growth rates so that the weighted average of groups’ rates equaled the growth rates we observed in the PI data.
- We projected eligibility-group enrollment among adults using the scaled growth rates and calibrated the totals so that total adult enrollment continued to equal the enrollment states reported in the PI data.
- We used the projected enrollment by adult eligibility groups to estimate how the composition of adult Medicaid enrollees changed during the continuous enrollment period. We applied the changes in the distribution of adult enrollees to each state’s adult enrollment distribution from 2019.
- We assumed the major distributional changes occurred between February 2020 and September 2022, that distribution changes slowed during FY 2022, and that by FY 2023, enrollment growth was similar among all eligibility groups.
- The T-MSIS data did not include adults in the ACA group for Virginia which expanded Medicaid in 2019 or for states that expanded Medicaid after 2019: Idaho (2020), Missouri (2022), Nebraska (2020), and Oklahoma (2022). For those states, we used publicly available data to estimate the percentage of adults enrolled in ACA coverage and adjusted enrollment in the other groups proportionally.