What Happens After People Lose Medicaid Coverage?
At the start of the pandemic, Congress enacted the Families First Coronavirus Response Act (FFCRA), which included a temporary requirement that Medicaid programs keep people continuously enrolled and, in exchange, states received enhanced federal funding. Under the continuous enrollment provision, Medicaid enrollment has grown substantially compared to before the pandemic and the national uninsured rate has declined. Provisions in the Consolidated Appropriations Act (CAA), signed into law in December 2022, end the continuous enrollment provision on March 31, 2023, and phase down the enhanced federal Medicaid matching funds through December 2023. When the continuous enrollment provision ends, however, millions of people could lose Medicaid, potentially reversing recent gains in health insurance coverage.
A key question is whether people losing Medicaid will be able to transition to and retain other forms of coverage, including Affordable Care Act (ACA) marketplace plans with premium assistance or employer-sponsored health benefits.
This brief uses pre-pandemic data from the 2016-2019 Medical Expenditure Panel Survey (MEPS) to examine the extent to which people enroll in and retain other coverage during the 12 months following disenrollment from Medicaid/CHIP. See the “Methods” section at the end of this brief for more details. Key findings include:
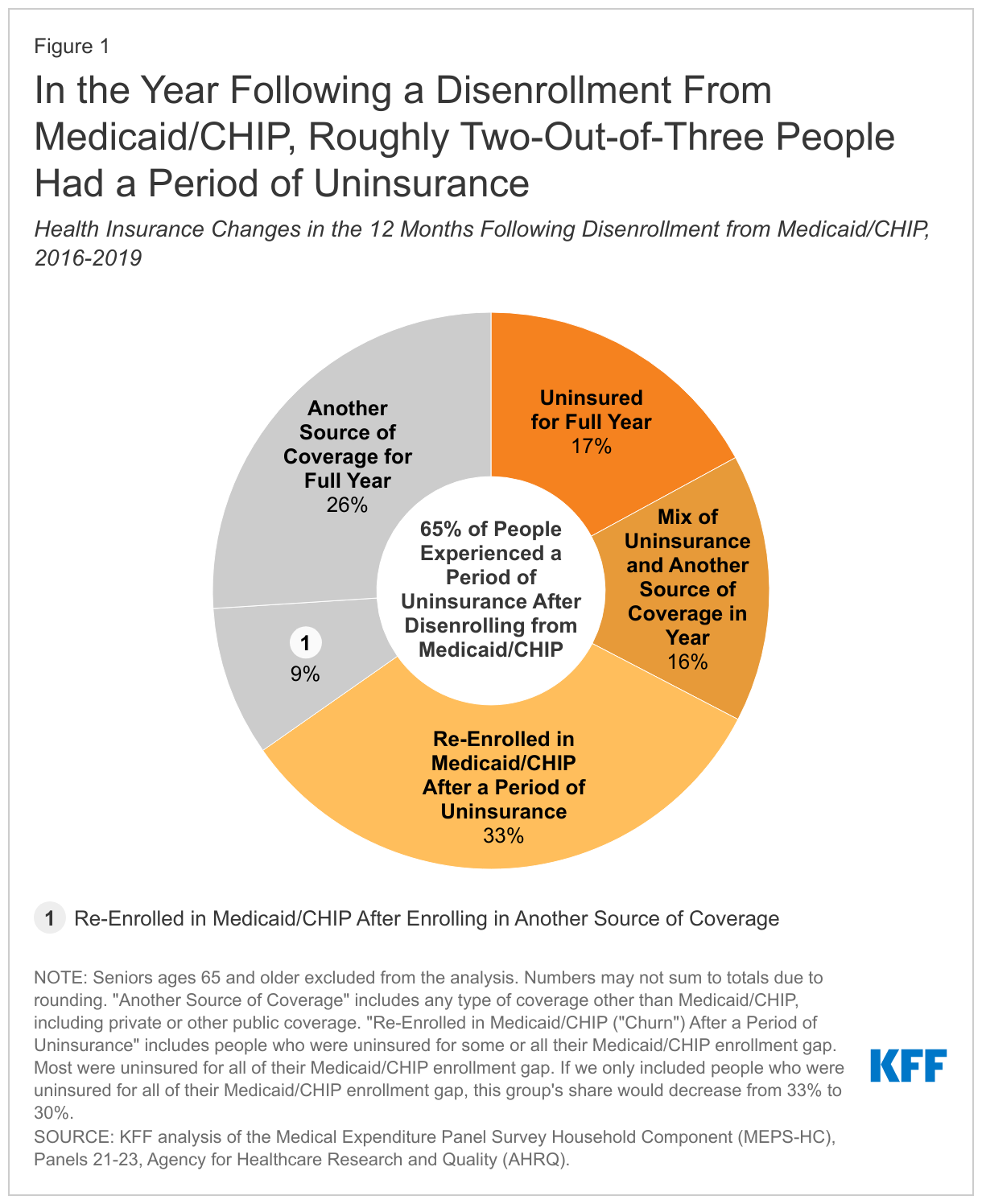
- In the year following a disenrollment from Medicaid/CHIP, roughly two-thirds (65%) of people had a period of uninsurance.
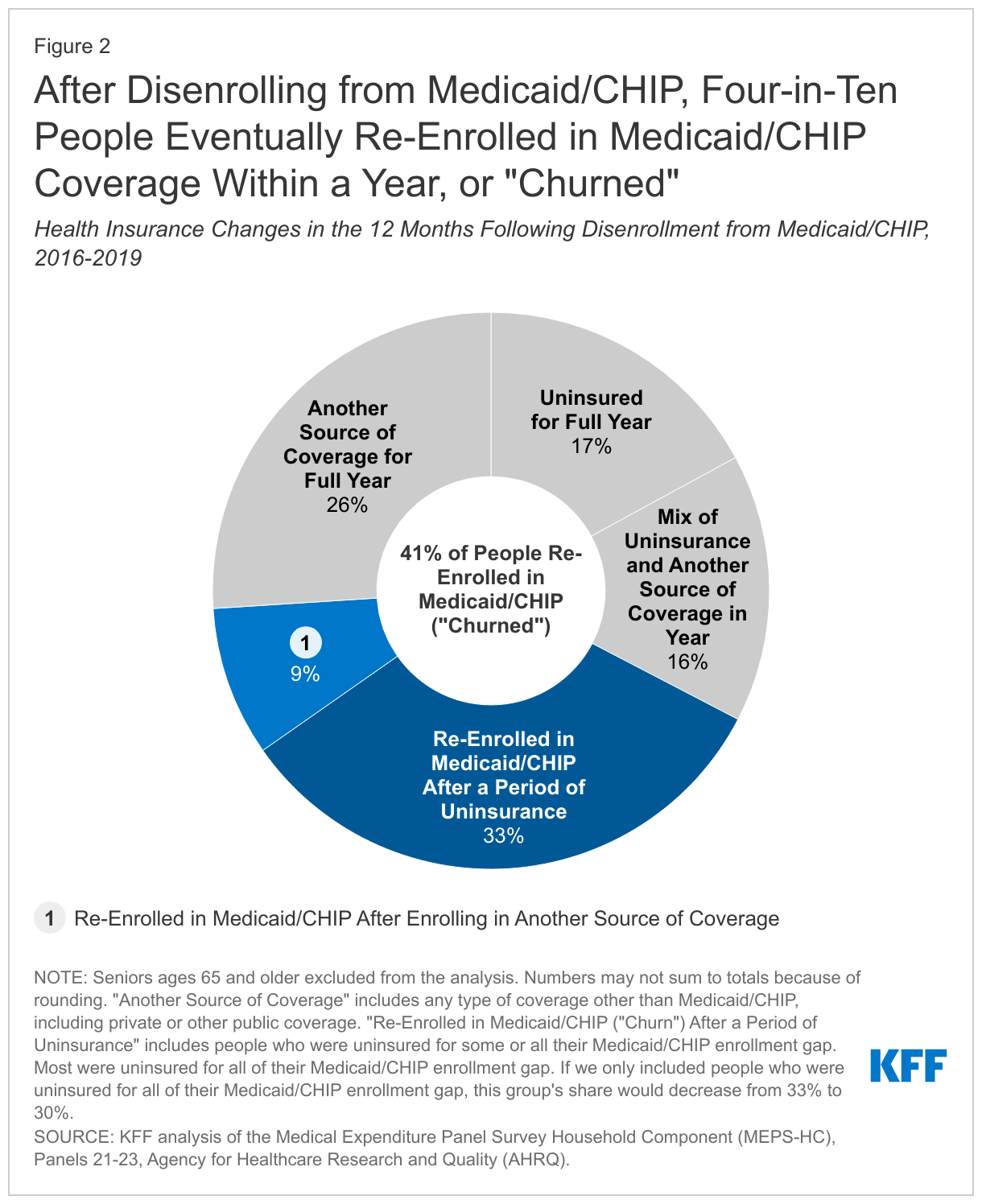
- Roughly four in ten (41%) people who disenrolled from Medicaid/CHIP eventually re-enrolled in Medicaid/CHIP within a year (or “churn”).
Key Findings
In the year that followed a disenrollment from Medicaid/CHIP, roughly two-thirds (65%) of people had a period of uninsurance while just 35% were continuously enrolled in coverage (Figure 1). The 65% of Medicaid/CHIP enrollees who experienced uninsurance after disenrolling consists of people who were: uninsured for the full year (17%), uninsured for some of the year and had another source of coverage during the year (16%), and uninsured after disenrolling but eventually re-enrolled in Medicaid/CHIP (or “churned”) before the end of the year (33%). The 35% of Medicaid/CHIP enrollees who maintained coverage for the full year after disenrollment from Medicaid/CHIP consist of people who: were enrolled in another source of coverage for the full year (26%) and had another source of coverage for some of the year but also re-enrolled in Medicaid/CHIP before the year ended (9%). Notably, most1 of the people who were covered for the full year after disenrollment had a period of overlapping coverage before losing Medicaid/CHIP during which time they had both Medicaid/CHIP and private health insurance.
Roughly four in ten (41%) people who disenrolled from Medicaid/CHIP would eventually go on to re-enroll in Medicaid/CHIP within a year (Figure 2). That group consists of people who re-enrolled in Medicaid/CHIP after a period of uninsurance (33%) and who re-enrolled after having other coverage (9%). Among all enrollees who churned, 79% were uninsured before they re-enrolled in Medicaid/CHIP. Churn occurs for several reasons. Enrollees may experience short-term changes in income that make them temporarily ineligible. Churn may also happen when people who are still eligible for Medicaid/CHIP lose coverage for administrative reasons, such as difficulties completing annual renewals. Ultimately, churning on and off Medicaid/CHIP can limit access to care and lead to delays in getting needed care. Even for people who have other coverage before re-enrolling in Medicaid/CHIP, churning can cause disruptions in coverage when it requires people to change their health care providers or to navigate through different benefit packages.
Implications
These findings highlight that many people do not transition to and retain other coverage after they disenroll from Medicaid/CHIP. Overall, 65% of the people had a gap in coverage during the year following disenrollment from Medicaid/CHIP and only 26% of people enrolled in and retained another source of coverage for the full year after losing Medicaid/CHIP coverage. Of people who disenroll from Medicaid/CHIP, 41% re-enrolled within the year. That number includes 33% who re-enrolled in Medicaid/CHIP after a period of uninsurance, suggesting that many people were still eligible when they lost Medicaid/CHIP coverage. Even among people who initially enrolled in other coverage, 34% did not retain it for the full year; these individuals eventually lost their other coverage (and become uninsured) or they re-enrolled in Medicaid/CHIP. Generally, people in our analysis who had overlapping coverage (i.e., Medicaid/CHIP and private coverage) prior to losing Medicaid/CHIP were less likely to become uninsured or churn compared to those who did not have overlapping coverage.
KFF estimates that between 5 and 14 million people will lose Medicaid coverage when states “unwind” the continuous enrollment provision this year. Beginning April 1, 2023, states can resume disenrollments for the first time since March 2020. Some of the people who will be disenrolled during the unwinding will be ineligible and will become uninsured if they do not transition to other coverage. Others will lose coverage for administrative reasons despite still being eligible. While the millions of people who lose coverage during the unwinding will face similar challenges as those included in this analysis, there are also important differences today. For one, Congress extended enhanced subsidies for the ACA marketplace, which were first included in the American Rescue Plan Act (ARPA) during the pandemic, making those plans more affordable through 2025. Additionally, because of the continuous enrollment provision, an increasing number of Medicaid enrollees today report also being enrolled in private insurance compared to before the pandemic, which should reduce coverage disruptions for these individuals when they disenroll from Medicaid. However, this only represents a subset of people who will be disenrolled during the unwinding process. Most individuals who will lose Medicaid during the unwinding because they are no longer eligible will still need to transition to (and retain) other health insurance to avoid a gap in coverage.
State Medicaid agencies and other stakeholders can take several steps to reduce coverage disruptions and churn during the unwinding period. Broadly, these actions could include improving state eligibility systems, streamlining renewal procedures, communicating with enrollees about the need to complete a renewal, and facilitating transitions to the ACA marketplace or separate CHIP coverage for people found ineligible for Medicaid. The federal government has issued guidance aimed at reducing coverage disruptions for Medicaid/CHIP enrollees and has imposed new reporting requirements to monitor states’ unwinding processes. Although our analysis provides a pre-pandemic baseline for peoples’ health insurance changes after losing Medicaid/CHIP coverage, state policies for the unwinding will have a major impact on whether people will be more successful in transitioning to other coverage after losing Medicaid compared to pre-pandemic trends.
Methods
Data Source
This analysis uses data from the Medical Expenditure Panel Survey (MEPS) for panels 21, 22, and 23, which were collected between 2016 and 2019. MEPS panels generally cover a two-year period (24 months), although panel 23 was extended for an additional year due to the coronavirus pandemic. Our analysis only used the first 2 years (24 months) of panel 23. Our estimates account for the MEPS survey design and use longitudinal weights. We used monthly insurance variables to identify Medicaid enrollees and health insurance outcomes during the study period.
Study Population and Exclusions
We limited our analysis to individuals who were disenrolled from Medicaid/CHIP within the first 13 months of the survey panel to allow for a full 12-month follow-up period. We further limited the analysis to people with at least four consecutive months of Medicaid/CHIP before they disenrolled to exclude anyone who was enrolled under presumptive eligibility or for emergency services but then determined to be ineligible. We excluded people ages 65 and older and those under 65 with Medicare because Medicare is the primary payer for acute care when people have both Medicare and Medicaid. Finally, we excluded a small number of individuals who were out of the survey’s scope during the study period (for example, if someone dies, moves out of the country, or becomes institutionalized). After these exclusions, our final sample included 1,160 respondents.
Health Insurance Status
For each month during the panel, we created an indicator that classified individuals as either enrolled in Medicaid; having other, non-Medicaid coverage; or as uninsured. For people with Medicaid, we also created another indicator that identified whether individuals had a secondary source of coverage while enrolled in Medicaid. Notably, in 2018, MEPS modified how they asked the health coverage questions for individuals living in the same household as the primary respondent. Up to 2018 health coverage questions were asked at the household level (e.g., “Has anyone in the family been covered by…?”), but the questionnaire was updated to ask these questions as the person level (e.g., “Was Person 1 covered by…?”). However, we expect that the change had minimal impact on how respondents reported health insurance coverage for household members.
- Thirty-five percent of people disenrolled from Medicaid/CHIP had health coverage for the full year after disenrollment. Of these people, 71% had both Medicaid/CHIP and private health insurance before losing Medicaid/CHIP. Typically, these individuals only had 1 to 4 months of overlapping coverage before disenrolling from Medicaid/CHIP. Generally, people with multiple sources of coverage before disenrolling were more likely have coverage for the full year and were less likely to churn compared to people who did not have overlapping coverage. ↩︎