Unwinding the PHE: What We Can Learn From Pre-Pandemic Enrollment Patterns
Executive Summary
The Families First Coronavirus Response Act (FFCRA), passed during the coronavirus pandemic, includes a Medicaid continuous enrollment requirement that prohibits states from disenrolling people from Medicaid in exchange for additional federal funds. The continuous enrollment requirement has prevented coverage loss and churn (moving off and then back on to coverage) among enrollees during pandemic and, along with other factors, has contributed to the substantial enrollment growth in Medicaid. From February 2020 to January 2022, total Medicaid/CHIP enrollment has increased by 15.7 million enrollees (22.1%). The continuous enrollment requirement will last until the end of the month in which with national public health emergency (PHE) ends. Currently, the PHE is in effect through mid-July 2022 and, at this time, it is expected that the continuous enrollment requirement will end August 1, 2022. The Biden administration has said it will give states 60 days’ notice before the PHE ends, and so if state are not notified by mid-May, the PHE will likely be extended further.
To help inform the current policy discussion and better understand the factors that contribute to Medicaid enrollment changes, this brief examines typical enrollment patterns for Medicaid and CHIP1 and uses 2018 Medicaid claims data to gain insight into the effects of the continuous enrollment requirements by eligibility group. Overall, we find that:
- Roughly 2% of Medicaid enrollees come on or leave the program in an average month, although there is variation across eligibility groups.
- A policy to require continuous enrollment would result in sharp reductions in monthly disenrollment rates and would also reduce monthly enrollment rates due to reductions in churn.
- Based on data from 2018, the effect of continuous coverage would have greater impact on enrollment for children and non-elderly adults as they are more likely to experience higher rates of churn or income fluctuations affecting eligibility.
These findings from the simulation may help explain how the current continuous enrollment requirement may have contributed to Medicaid enrollment increases and what may happen with the unwinding of the PHE. A description of the data and methods underlying this analysis is in the Methods section at the end of the brief.
What factors contribute to enrollment changes over time?
Medicaid enrollment is driven by several factors, including economic conditions and policy choices. Medicaid is a countercyclical program, meaning that typically during economic downturns, more people qualify and enroll in Medicaid. Economic downturns were the primary driver of Medicaid enrollment growth in the 2001 recession and again during the Great Recession beginning in 2007. Medicaid enrollment also reflects policy changes. For example, Medicaid enrollment growth peaked in FY 2015 due to implementation of the Affordable Care Act (ACA) coverage expansions. Also, prior to the pandemic, enrollment declined in FY 2018 and FY 2019 and was relatively flat in FY 2020 before increasing sharply in 2021.
Enrollment trends reflect the net effect of people coming onto the program as well as people leaving the program. People typically enroll or disenroll from coverage for three main reasons:
- Change in income (for example, a drop in income may make someone newly eligible, while an increase in income may make someone ineligible for Medicaid);
- Change in circumstance other than income (for example, children may age out of coverage, people may move to another state or die); and
- Barriers to renewing coverage that are not based on ongoing eligibility but may result in disenrollment (for example, forms to renew coverage may be confusing or someone may miss a deadline resulting in disenrollment).
It is often difficult to understand the relative magnitude of each of these factors in contributing to net enrollment changes over time.
What do data show about enrollment patterns?
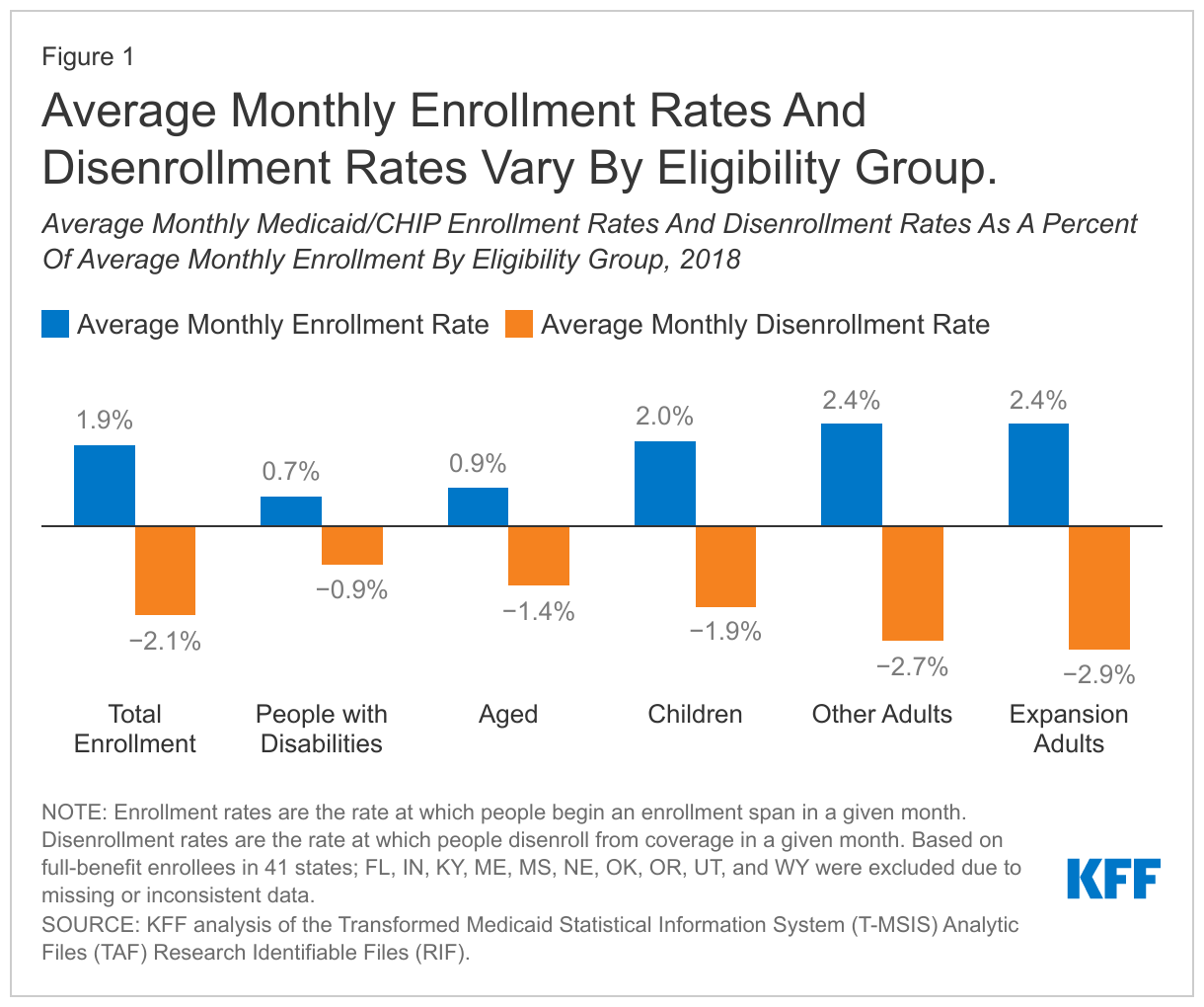
In general, data show that about as many people enroll in Medicaid in a given month as disenroll, with small differences leading to changes in net monthly enrollment. In 2018, the average monthly disenrollment rate was 2.1% while the monthly enrollment rate (people beginning an enrollment span) was 1.9%, which resulted in a net monthly enrollment decline of 0.2% (Figure 1). Earlier research attributed this enrollment decline to a robust economy and to policies and processes in place that may have boosted disenrollment, such as more frequent checks on income or barriers to renewing coverage. At the same time, our analysis of data for other recent years showed similar patterns (approximately 2% of enrollees coming on or off the program each month), with the difference in monthly new enrollment and disenrollment rates leading to an overall increase or decrease in enrollment. As noted above, we expect patterns would have been different (with much higher enrollment rates relative to disenrollment rates) during the Great Recession and after the implementation of the ACA.
Average monthly enrollment and disenrollment rates vary by eligibility group (Figure 1). In 2018, both enrollment and disenrollment rates for elderly enrollees and enrollees with a disability were lower than rates for children and adults. In other words, in a given month, fewer elderly and disabled enrollees were entering and leaving the program relative to total enrollment in those groups compared to children and non-elderly adults. The elevated enrollment rates and disenrollment rates among children and adults reflect that they are more likely to experience income fluctuations affecting eligibility and also leading to higher rates of churn.
Not all enrollment and disenrollment reflects people newly entering or permanently leaving Medicaid. Another analysis that examined churn within Medicaid shows that, among people enrolled in 2018, approximately 10% experienced a gap in enrollment of less than a year. This suggests that the enrollment in each month reflects individuals who had been enrolled, then disenrolled, and then were re-enrolling after a gap in Medicaid coverage, as well as those who were newly eligible. Similarly, disenrollments in each month reflect some people who may re-enroll in Medicaid after a short gap, as well as those who transitioned from Medicaid to other coverage or become uninsured. As noted above, children and non-elderly adults experience the highest rates of churn compared to people with disabilities or enrollees ages 65 and over.
What happens to enrollment patterns under a continuous enrollment requirement?
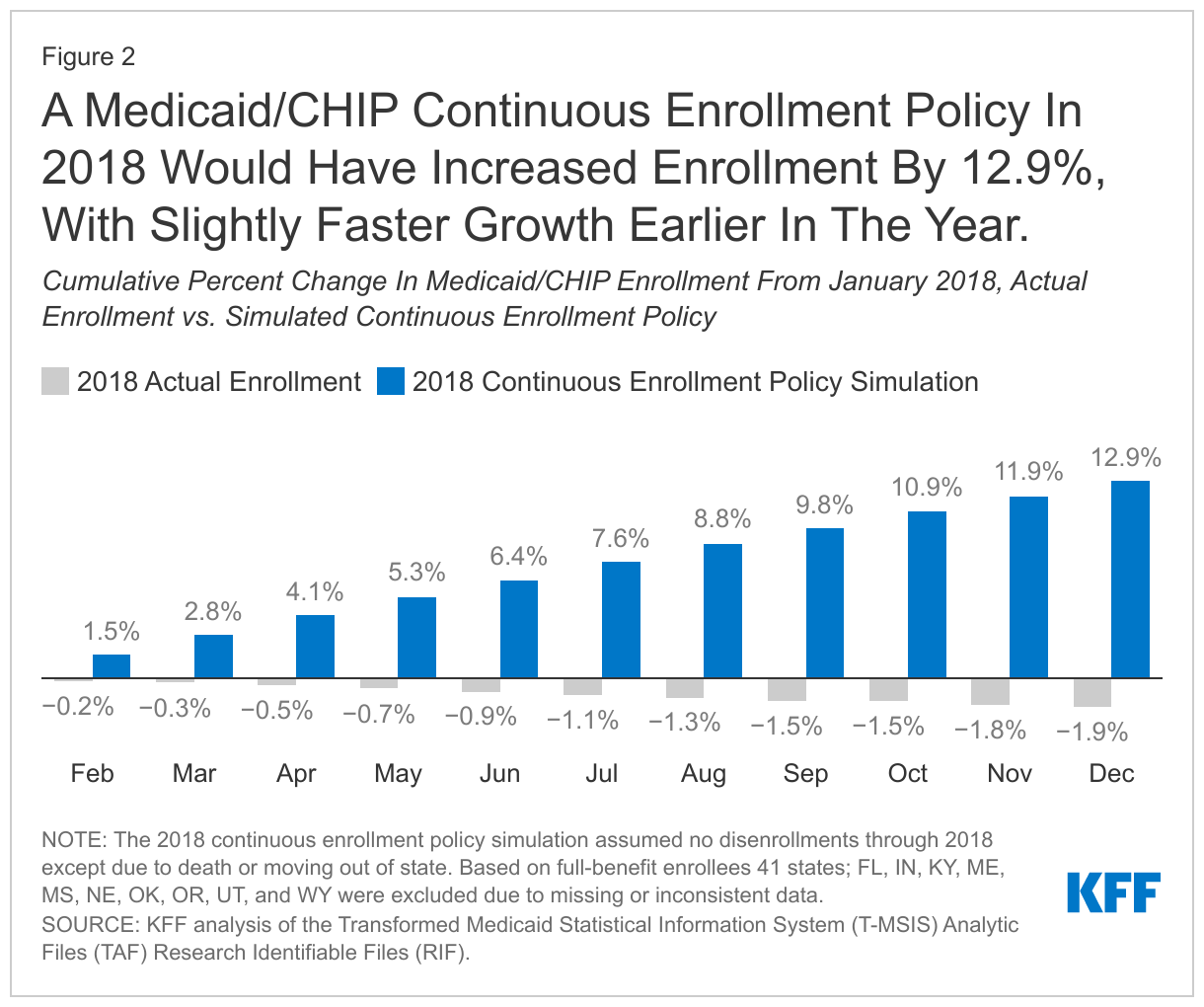
To help understand the effects of the current Medicaid continuous enrollment policy, we examined what would have happened if there were a similar policy prohibiting disenrollment in place in 2018. Halting disenrollment (except for enrollees who were disenrolled due to a move out of state or death) lowered the average monthly disenrollment rate compared to actual 2018 (0.2% vs. 2.1%, respectively). Halting disenrollments in the simulation also lowered the average enrollment rate compared to actual 2018 (1.4% vs. 1.9%, respectively) due to eliminating churn. Over the course of the year, the simulated continuous enrollment policy resulted in a net increase in enrollment (12.9%, Figure 2) from January to December 2018 compared to the slight decrease in enrollment observed in actual 2018 (-1.9%). When looking at the monthly enrollment changes, the first few months of the simulation experienced slightly faster growth than the later months.
The simulated continuous enrollment policy led to much higher enrollment growth for children and non-elderly adults compared to people with disabilities and those ages 65 and older (Figure 3). This result was also expected, as these groups typically have higher turn-over (i.e., greater disenrollment and enrollment rates) and so they would experience bigger effects from a policy to stop disenrollment.
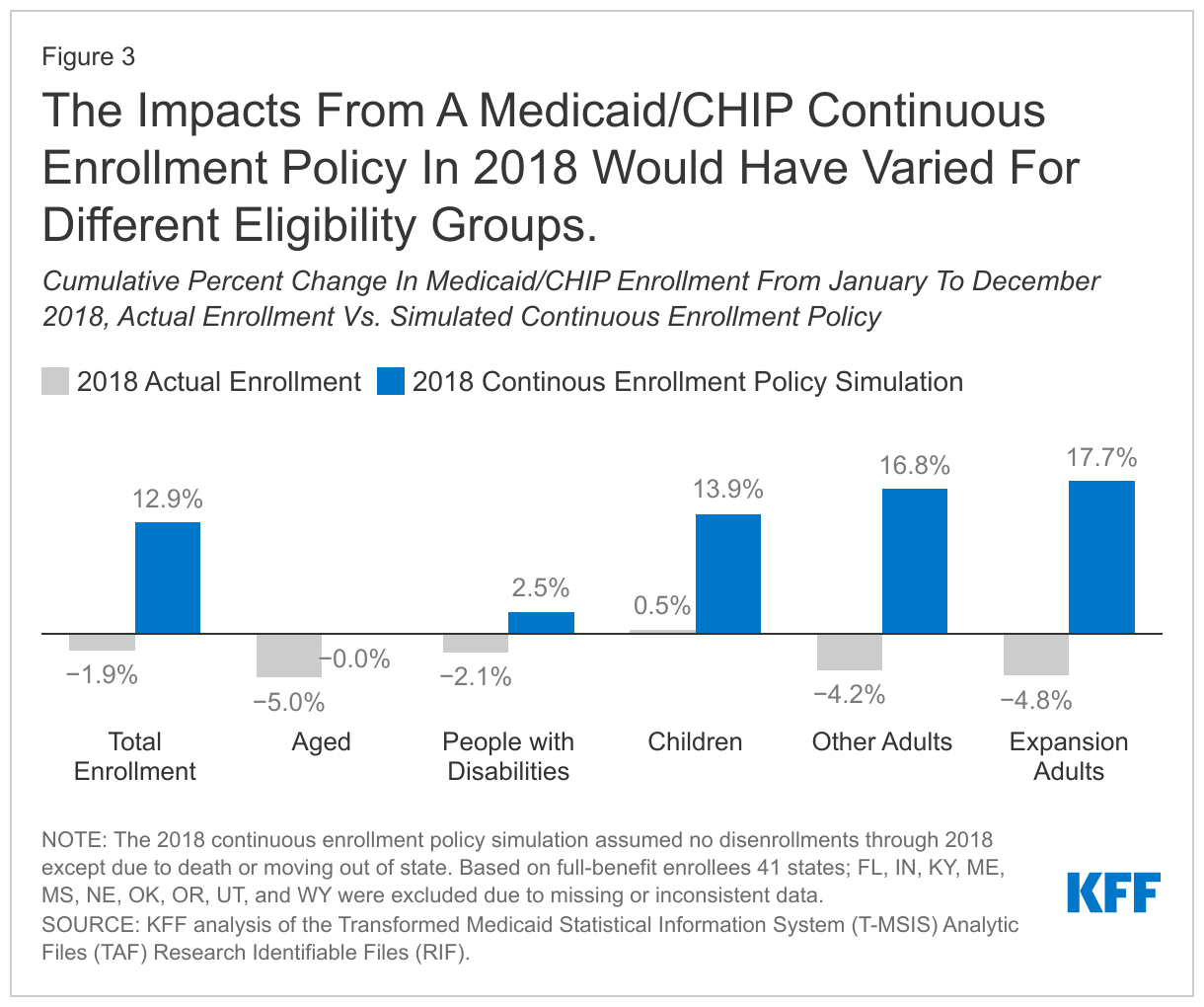
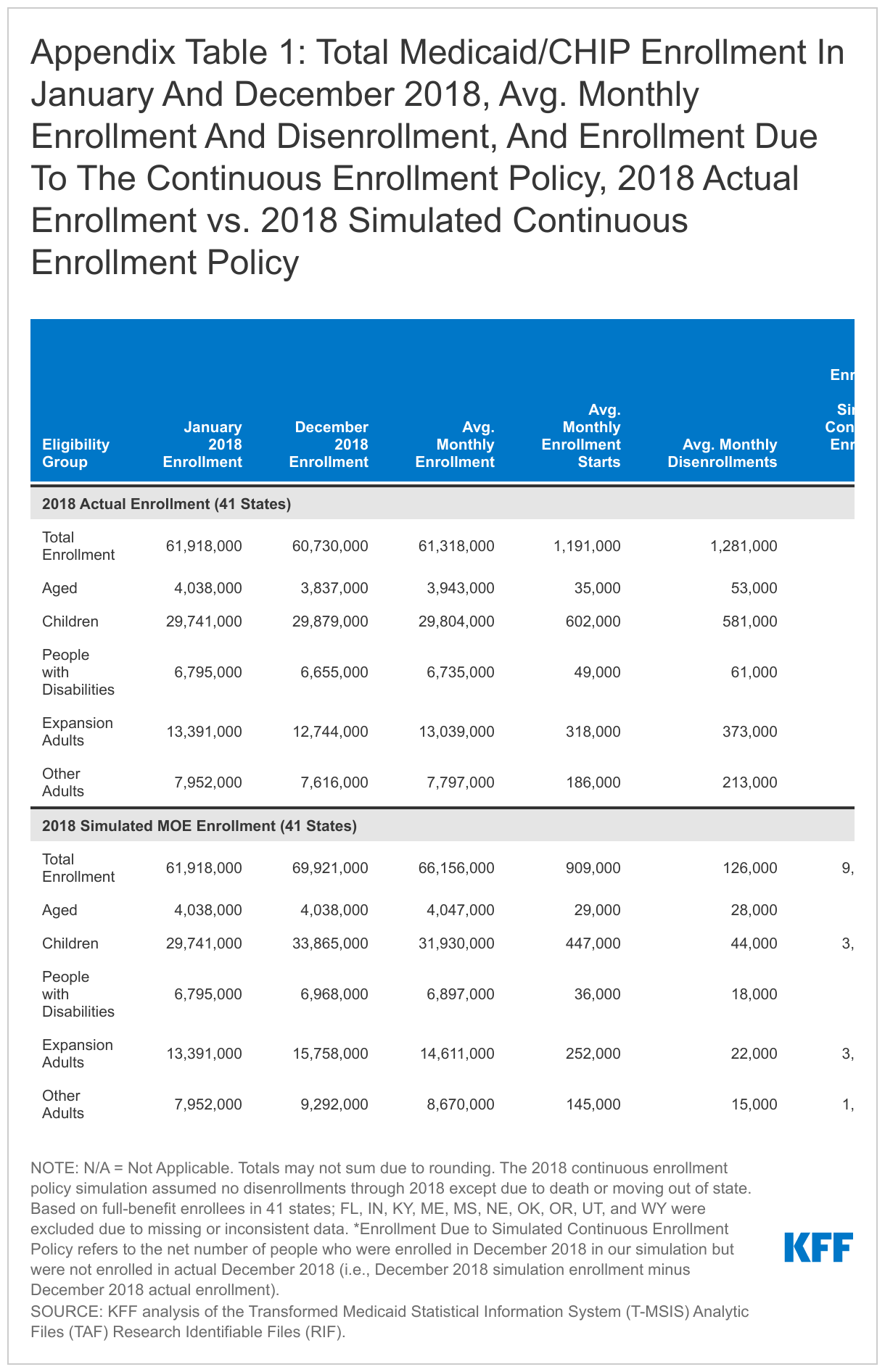
Children and expansion adults accounted for 76% of the enrollment change due to the simulated continuous enrollment policy for 2018 (Appendix Table 1). These findings are as of December 2018, or after 12 months of the simulated continuous enrollment policy. While the total number of enrollees are not complete because we exclude 10 states from the analysis, we estimate that actual enrollment declined by 1.2 million or 1.9% in 2018 for the 41 states included in our analysis. Under the simulated continuous enrollment policy, enrollment would have increased by 8.0 million or 12.9%. The net change would be an increase of 9.2 million in enrollment. We estimate that, of this net growth, children account for 43% of this net change and expansion adults make up 33% of the change. Other non-elderly adults not enrolled through the Medicaid expansion made up 18% of the net change. These three eligibility groups represent the largest share of total Medicaid/CHIP enrollment2 and also experienced higher average monthly enrollment and disenrollment rates in actual 2018. People with disabilities made up 3% of enrollment due to this net enrollment growth and people ages 65 and older made up 2%.
What to watch going forward?
Understanding historic enrollment patterns and the effects of a simulated policy to halt disenrollment in 2018 can help inform the current continuous enrollment requirement in place. Key findings suggest that, first, halting disenrollment has a significant effect on overall enrollment growth. Second, growth may be steeper when the policy is first put into place, but growth rates may slow as a result of lower churn. Third, the policy would have a significantly disproportionate effect on children and non-elderly adults relative to people with disabilities and those ages 65 and older. Finally, the simulated growth patterns reflect recent experience with Medicaid growth. We observed steep growth in Medicaid enrollment in calendar year 2020 when the continuous coverage policy was put into effect but, similar to the simulation, observed growth rates have slowed over time.
Overall growth rates may be harder to compare given the sharp differences in economic conditions in 2018 compared to recent experience. The fact that observed growth rates from February 2020 through January 2021 showed 13.5% growth, slightly higher than the one-year results of the simulation (12.9%), suggest that much of current growth is attributable to the continuous coverage rather than new enrollment. The economic effects of the COVID-19 recession are complex. Unlike prior recessions that resulted in large shifts in income and losses of employer coverage, this recession largely affected low-wage workers who may have already been eligible for Medicaid.
Finally, as the PHE expires and states are able to resume more routine renewals and disenrollments, our analysis (in addition to current enrollment reports) shows that a large share of non-elderly adults and children could be at risk of losing coverage, even if many continue to be eligible. Efforts to conduct outreach, education and provide enrollment assistance can help ensure that those who remain eligible are able to retain coverage and those who are no longer eligible can transition to other sources of coverage. The Centers for Medicare and Medicaid Services (CMS) released new guidance in March 2022 emphasizing continuity of coverage for enrollees after the end of the continuous enrollment requirement, and the guidance also extended the timeline for states to complete all redeterminations after the continuous enrollment requirement ends from 12 to 14 months (states will still need to initiate all redeterminations within 12 months). However, a recent survey of state officials shows that, as of January 2022, many states had not made key decisions about how to handle the resumption of disenrollments after the end of the PHE. State policy choices about how to prioritize pending eligibility actions, engage with stakeholders, conduct outreach to enrollees, and provide enrollment assistance will have important implications for the continuity of coverage for millions of Medicaid enrollees, especially non-elderly adults and children.
The authors thank former KFF Vice President Rachel Garfield for her role in writing this report and technical assistance with the analysis.
Methods
Data Source and Linkage
Our analysis is based on the Transformed Medicaid Statistical Information System (T-MSIS) Analytical Files (TAF) Research Identifiable Files (RIF). We include beneficiaries who were enrolled at any point in 2018. We use the 2018 Demographic Eligibility (DE) Base file to determine eligibility pathway based on last-best eligibility data. We draw enrollment dates from the 2017-2019 DE Dates files. Our analysis uses enrollment dates from 2017 and 2019 so that we are able to identify people who were enrolled from December 2017 into January 2018, as well as December 2018 into January 2019. Data for 2019 are from the preliminary version of the T-MSIS RIF. All other DE Base and DE Dates files are final versions (Release 1).
State Exclusion Criteria
We use 41 states in our analysis. We excluded 10 states (FL, IN, KY, ME, MS, NE, OK, OR, UT, and WY) due to missing or inconsistent data based on state-level information available at the DQ Atlas as well as our own analysis We relied on data quality assessments from DQ Atlas to exclude states that have a “medium concern”, “high concern”, or “unusable” data quality assessment for: (1) the average monthly Medicaid/CHIP enrollment compared to an external enrollment benchmark (Medicaid/CHIP Performance Indicator Data) (excluded five states (IN, KY, ME, MS, NE)); (2) the average length of enrollment gaps, and (3) the percent of beneficiaries with overlapping Medicaid and S-CHIP enrollment spans (no states were excluded based on measures 2 or 3). We further excluded states based on: (4) the percent of beneficiaries missing an eligibility group code (threshold of >=10%, excluded OR); (5) the percent of beneficiaries with only one enrollment span (threshold of >=99.5, excluded FL, KY, and WY); and (6) the percent of beneficiaries with three or more enrollment spans in a year (threshold of >=5%, excluded OK). Notably, our exclusion criteria related to the number of enrollment spans in a year (measures 5 and 6) are less restrictive than that in the DQ Atlas because we did not want to make assumptions about the number of enrollment spans in our analysis, but did want to remove extreme cases that are the most likely to represent inaccurate enrollment dates.
Beneficiary Linking, Eligibility Classification, and Exclusion
We linked individuals across years using BENE_ID, which are unique enrollee identifiers created by the Chronic Conditions Warehouse and are recommended for use when combining data for multiple years. We also use BENE_ID to link the DE Base and DE Dates files. We assigned restricted benefit status and eligibility group code using a last-best approach for 2018, which assigns eligibility based on the most recent eligibility code in 2018. We classified eligibility groups using a hierarchy that first checked if the eligibility group code was missing, then checked for medically needy eligibility, disability (under age 65), and expansion adult. Any enrollees in the DE Base file that had a non-missing eligibility code and had not been assigned an eligibility group through this hierarchy were then were assigned by age to children (ages 20 and under), adults (ages 21 to 64), and aged (ages 65 and over).
The 2018 DE Base files for 41 states in our analysis contained 74.0 million observations coded as full-benefit after removing a small number of “dummy” records that represent enrollees who have claims data but no eligibility data provided by the states. We removed observations missing eligibility codes (151,000 observations), people qualifying through a medically needy pathway (1.5 million observations), people missing a BENE_ID for linking files (953,000 observations), and people with duplicated BENE_ID (102,000 observations). After merging with the DE Dates files, there were less than 3,000 enrollees who did not have a matching BENE_ID in the DE Dates and DE Base files and were dropped from the final sample. Our final sample included 71.3 million unduplicated, full-benefit enrollees.
Calculating Enrollment Trends
The DE Dates files provide a start and end date for every enrollment span in our time period. However, the earliest start date in any DE Date file in January 1st of that year, and the latest end date is December 31st of that year. Using the 2017 and 2019 DE Dates files, linked by BENE_ID, we were able to identify people who started enrollment spans in January 2018 (versus people who were continuously enrolled from December 2017) and people who disenrolled in December 2018 (versus people who were continuously enrolled into January 2019). Before calculating monthly enrollment and disenrollment rates, we merged all overlapping and contiguous enrollment spans for enrollees, which we defined as enrollment spans that are separated by one day or less. For example, if a person has two enrollment spans with an end date and a start date that are one day apart (i.e., the person disenrolled and re-enrolled the next day), we considered these spans to be contiguous and merged them into one enrollment span. After merging overlapping and contiguous enrollment spans, we counted the number of enrollment starts and disenrollments in a month (the enrollment and disenrollment rates). Enrollment counts are de-duplicated counts of people enrolled at any point in the month. Average monthly net change in enrollment is the average of monthly enrollment change from January 2018 to December 2018.
Simulating A Continuous Enrollment Policy
To simulate a continuous enrollment policy in 2018, we assume that no one is disenrolled from Medicaid and CHIP except in cases of death or moving to a different state. We used the 2018 DE Base file to identify death dates. We used the 2018 and 2019 DE Bases files to identify people who moved states and then re-enrolled in Medicaid and CHIP (and used BENE_ID for linking files). Notably, we do not have information about why a person was disenrolled or length of time before they enrolled in another state (we only can see that they were enrolled in another state after disenrollment). In total, there were 1.5 million people disenrolled in the simulation due to death or moving out of state.
After accounting for death and moving, we de-duplicated enrollees with multiple spans in 2018. We then used each enrollee’s earliest enrollment date in 2018 (or, if continuously enrolled from 2017, kept the date from 2017), and extended coverage through the year unless the enrollee had a death date or “move out” date. Finally, using this simulated sample, we calculated monthly enrollment rates, disenrollment rates, and total enrollment as described above.
Our simulation has important differences from the current continuous enrollment requirement under the FFCRA. First, our simulation applies to Medicaid and CHIP; however, while the current continuous enrollment requirement under the FFCRA does not apply to separate CHIP programs. In total, 3.6% of enrollees in our sample were only enrolled in separate CHIP programs throughout 2018 (and never enrolled in Medicaid through the year). Additionally, our simulation does not match the economic conditions of the pandemic, and the simulation does not account for other related factors such as elevated death rates or state or federal policy actions facilitating enrollment in Medicaid, CHIP, or Marketplace coverage.
Appendix
- Our simulation of a continuous enrollment policy in 2018 applies to both Medicaid and the Children’s Health Insurance Program (CHIP). Although the continuous coverage policy under the FFCRA does not apply to separate CHIP programs, it does apply to CHIP Medicaid expansion programs. See the Methods section for more details on the simulation. ↩︎
- January 2018 enrollment was the same in the simulation analysis and in actual 2018. The share of total full-benefit Medicaid/CHIP enrollment for each eligibility group in January 2018 were as follows: children (48%), expansion adults (22%), other adults (13%), people with disabilities (11%), and individuals ages 65 and older (7%). See Appendix Table 1 for enrollment counts. ↩︎