How Community Health Centers Are Serving Low-Income Communities During the COVID-19 Pandemic Amid New and Continuing Challenges
Executive Summary
Community health centers are a national network of safety-net primary care providers serving low-income, medically underserved communities. In addition to providing comprehensive primary care services, health centers have aided in national, state, and local responses to the coronavirus pandemic by providing a range of services designed to slow the spread and lessen the severity of COVID-19. Based on findings from a national survey of health centers, this brief examines how the pandemic has affected health center patients and services as well as the ongoing challenges health centers and their patients face. Key findings include:
Impact of the Pandemic on Health Center Patients and Services
- Health centers increased their use of telehealth services in response to the pandemic. The pandemic necessitated a rapid expansion of health centers’ telehealth services as patients avoided in-person care due to the risk of infection, federal guidance to avoid nonessential care, and social distancing requirements. While in-person visits have rebounded, health centers’ use of telehealth services continues to be higher than before the pandemic.
- Health centers reported an increase in the number of patients seeking housing, food and nutrition, and transportation services due to the economic disruptions caused by the pandemic. Health centers provide a range of social and supportive services to complement primary care. Compared to before the pandemic, over half of responding health centers said they saw an increase in the number of patients seeking housing services, food and nutrition services, and transportation services. A majority of responding health centers reported providing health literacy (71%) and transportation services (63%) on-site, while at least four in ten reported providing SNAP, WIC, or other nutritional services (44%) and healthy food options, such as a food pantry or meal delivery (42%), on-site.
- In the wake of a growing need for mental health and substance use disorder (SUD) services during the pandemic, health centers added new services. Since the start of the pandemic, 64% of health centers reported adding at least one new mental health or SUD service (including new telehealth options). However, health centers indicated that staffing shortages and patients’ inability to access services through telehealth (e.g., due to lack of internet access or computers/phones) as the most common challenges to providing mental health and SUD services.
- The share of health centers providing medication-assisted treatment (MAT) for treating opioid use disorder (OUD) increased during the pandemic. Roughly half of health centers (48%) saw an increase in patients with OUD compared to the start of the pandemic. The number of health center patients nationally who received MAT for OUD grew by 27% from 2019 to 2020, spurred by an infusion of federal grants for behavioral health services at health centers in the years leading up to the pandemic and the ongoing need for these services.
Key Issues to Watch
- Health centers face ongoing challenges recruiting and retaining staff and financial implications related to changes to the 340B Drug Discount Program. Among responding health centers, recruiting new employees and retaining current employees were cited as top challenges by 78% and 54% of responding health centers, respectively, and are consistent with challenges reported in previous years. Looking ahead, health centers may face financial challenges as they transition out of the pandemic. A majority of health centers reported that certain actions by pharmaceutical manufacturers and pharmacy benefit managers (PBMs) related to access to and reimbursement for 340B drugs have had a negative effect on revenue.
- The unwinding of the Medicaid continuous enrollment requirement could lead to coverage disruptions for many health center patients and revenue declines for health centers. The loss of Medicaid coverage among health center patients could lead to an increase in uncompensated care costs for health centers. At the same time, the temporary infusion of federal COVID-19 grant funding for health centers will end and federal funding for some programs that helped health centers during the pandemic, such as the HRSA COVID-19 Uninsured Program, faces an uncertain future.
Issue Brief
Introduction
Community health centers are a national network of safety-net primary care providers serving low-income, medically underserved communities. In addition to providing comprehensive primary care services, health centers have aided in national, state, and local responses to the coronavirus pandemic by providing a range of specific services designed to slow the spread and lessen the severity of COVID-19. These include providing both rapid and PCR tests, administering vaccines, and distributing masks and testing supplies and oral antiviral pills, while continuing to treat the ongoing health needs of their patients.
Additional federal grant funding made available during the pandemic has helped health centers to respond to the needs of their patients and weather the financial uncertainty related to the pandemic. However, health centers face uncertainty on a number of fronts, including the unwinding of the Medicaid continuous enrollment requirement and the loss of temporary telehealth flexibilities when the COVID-19 public health emergency (PHE) ends, as well as the lack of additional federal COVID-19 funding for programs like the Health Resources and Services Administration’s (HRSA’s) COVID-19 Uninsured program.
To understand how the pandemic has affected health center patients and services as well as the challenges health centers and their patients face, KFF and the Geiger Gibson/RCHN Community Health Foundation Research Collaborative at the George Washington University surveyed health centers in the 50 states and District of Columbia (DC). This survey was conducted in late 2021 and focused on the pandemic’s effect on services, the effects of policies on health center programs, the impact of changes made to the 340B Drug Discount Program, preparedness for the PHE unwinding, and the challenges health centers face. This brief presents survey findings for all responding health centers and also reports data from an ongoing biweekly survey conducted by HRSA.
Impact of the Pandemic on Health Centers and Their Patients
Responding to Changing Patient Needs
Health centers’ use of telehealth services increased during the pandemic. The pandemic necessitated a rapid expansion of health centers’ provision of telehealth services amid a decline in in-person visits as patients avoided in-person care due to the risk of infection, federal guidance to avoid nonessential care, and social distancing requirements. As a result, the use of telehealth increased compared to prior to the pandemic and peaked in April 2020 when more than 50% of visits on average were conducted virtually. The most recent data as of May 2022 show that telehealth visits have decreased somewhat, with about 15% of visits on average provided virtually, but still remain higher than pre-pandemic levels.
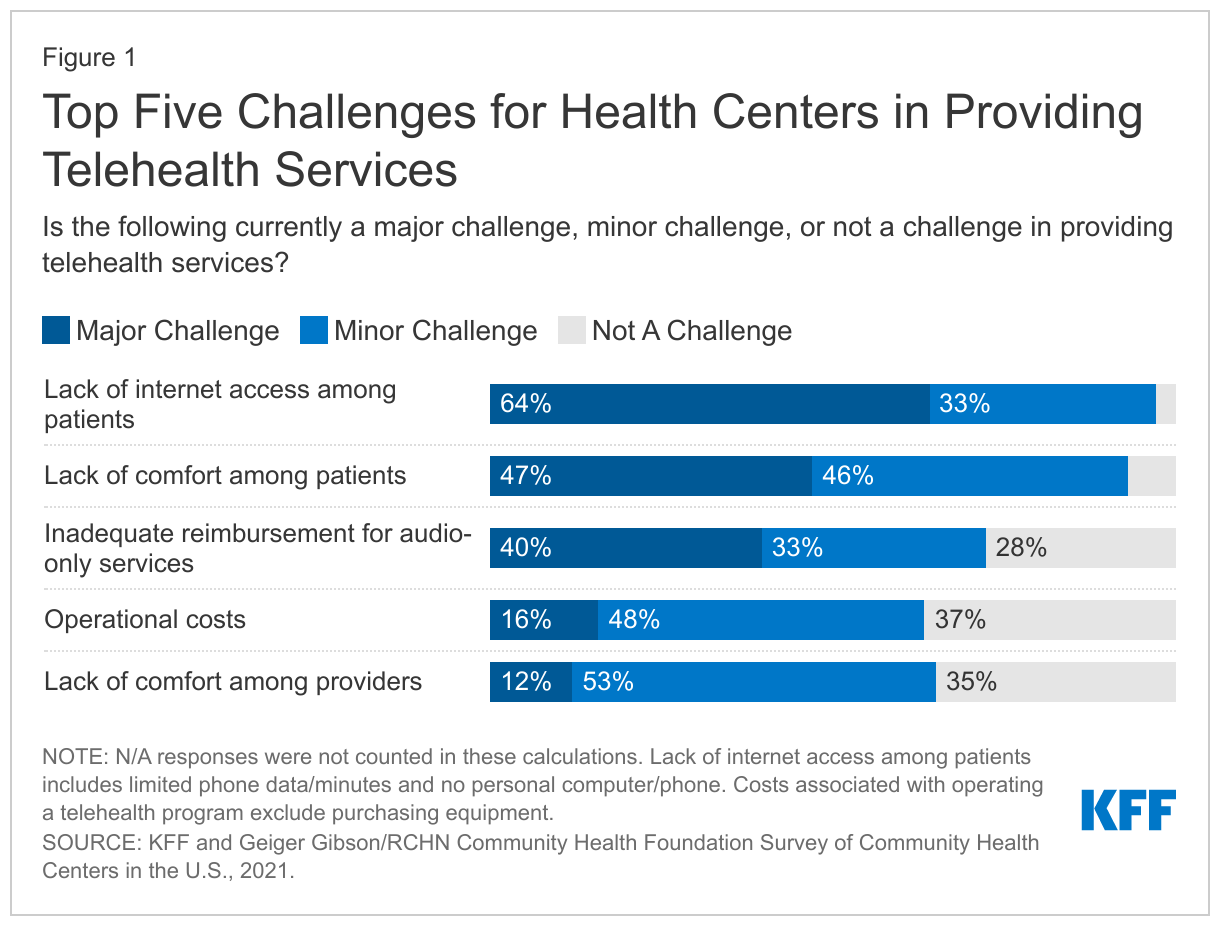
Telehealth has helped to maintain or improve access to care during the pandemic, but health centers reported challenges in providing virtual services to patients. Nearly all responding health centers cited lack of internet access among patients (97%) and lack of comfort using telehealth technology among patients (93%) as major or minor challenges to providing telehealth services (Figure 1). Additionally, over seven in ten responding health centers (72%) reported inadequate reimbursement for audio-only or telephonic telehealth services as a challenge.
Temporary policies enacted in response to the pandemic enabled health centers’ pivot to telehealth services; ending these policies could lead health centers to reduce the use of telehealth. During the public health emergency, many state Medicaid agencies, Medicare, and private insurers enacted temporary telehealth policies to improve accessibility and to provide enhanced reimbursement for telehealth. Additionally, the federal government, through the Federal Communications Commission, also provided one-time grant funding to providers (including health centers) to increase access to telehealth during the pandemic. Nearly eight in ten responding health centers (79%) reported that they would reduce the use of telehealth if these temporary telehealth flexibilities put in place by state Medicaid agencies and other payers do not remain in place.
Health centers contributed to COVID-19 vaccination, testing, and treatment efforts, reaching underserved and vulnerable populations. Supported by temporary federal grants in response to the pandemic as well as a number of national programs directly supplying health centers with tests, vaccines, therapeutics, and masks, health centers began providing new COVID-19-related services in 2020 and became an important national resource for equitably distributing these services in underserved communities. For example, according to data from a biweekly survey conducted by the Health Resources and Services Administration (HRSA), health centers have reported administering1 more than 20 million vaccine doses (roughly 4% of all vaccinations), with more than two-thirds (69%) of vaccine doses administered to people of color. Health centers that responded to our 2021 survey reported taking actions to increase COVID-19 vaccinations uptake, including by encouraging staff to talk to patients about the vaccine during visits (96%), posting information about the vaccine on social media (92%), and conducting community outreach (71%). The HRSA survey also revealed that roughly three in ten health centers utilized mobile vans, pop-up clinics, or other events out in the community to provide the vaccine and conduct outreach in May 2022.
Increased Demand for Services
Social Services
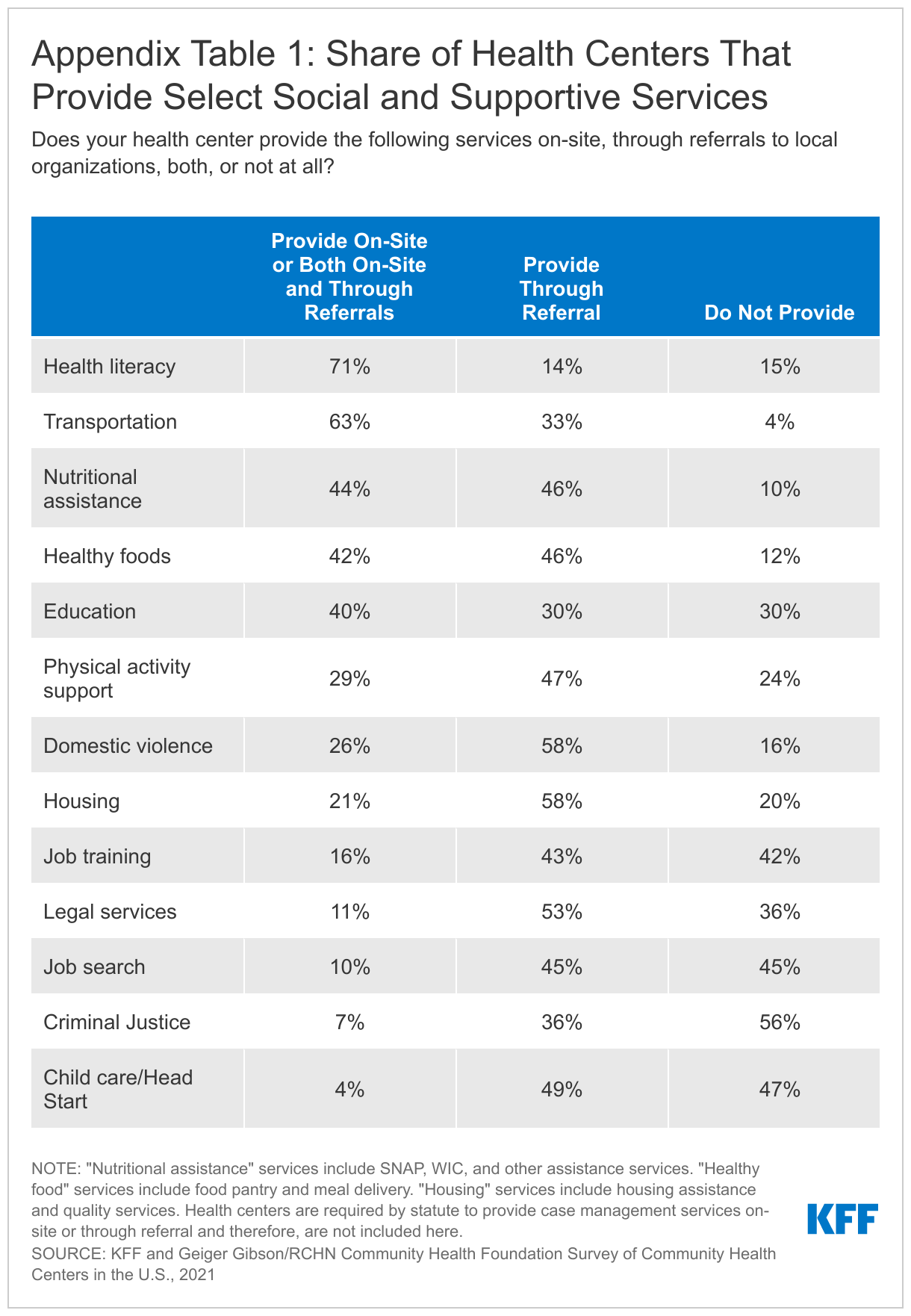
Health centers provided a range of social and supportive services both on-site and through referrals. A majority of responding health centers reported providing health literacy (71%) and transportation services (63%) on-site, while at least four in ten reported providing SNAP, WIC, other nutritional services (44%), healthy food services (42%), and education services (40%) (Appendix Table 1). We did not ask about case management, which is a required service of the Health Center Program and should be offered on-site or through referral at all health centers.
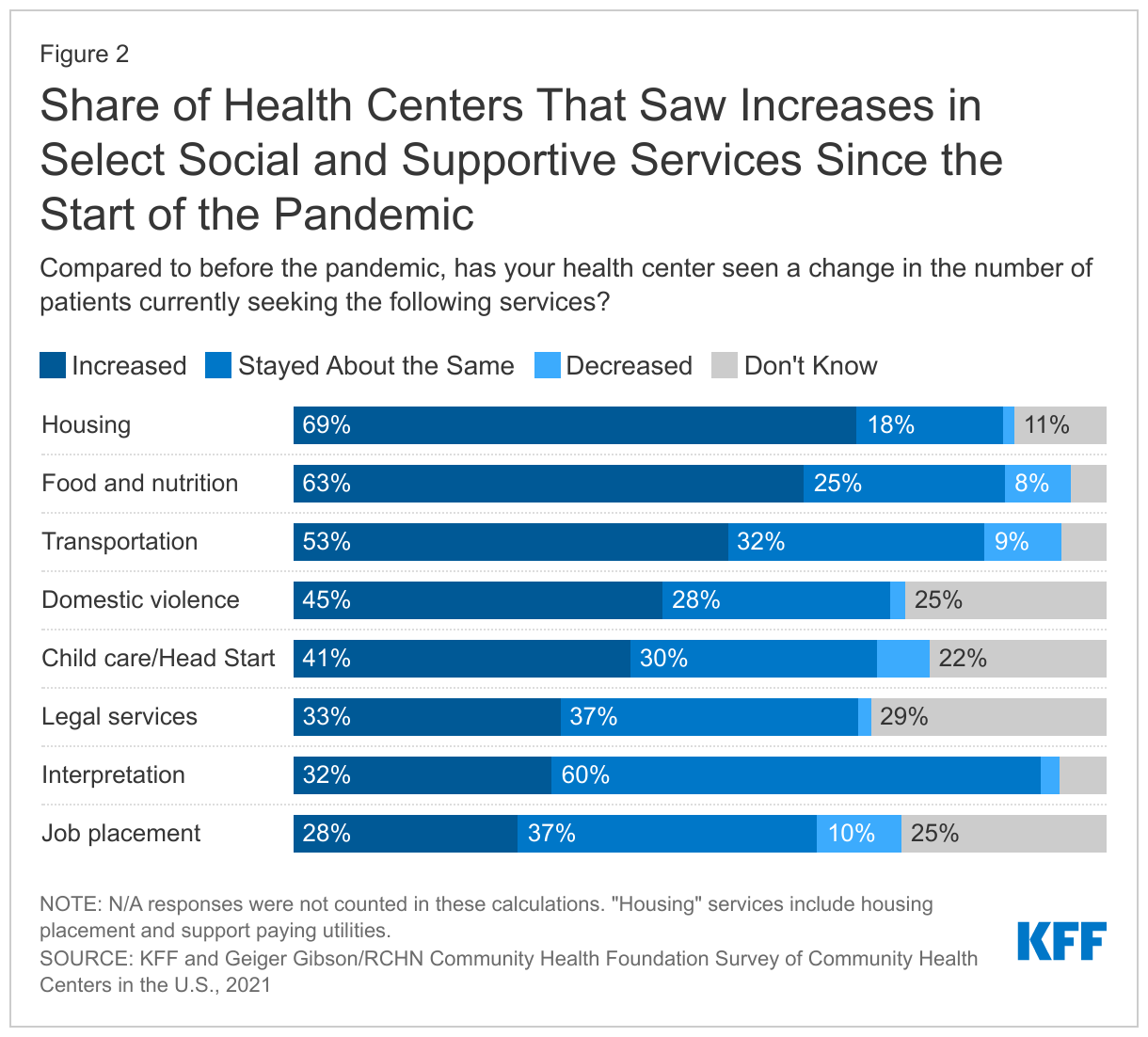
Health centers reported an increase in the number of patients seeking housing, food and nutrition, and transportation services during the pandemic. The pandemic caused economic disruptions, particularly for lower-income workers and families and contributed to an increased need for certain social services. Compared to before the pandemic, over half of responding health centers said they saw an increase in the number of patients seeking housing services (69%), food and nutrition services (63%), and transportation services (53%) (Figure 2).
Mental Health and Substance Use Disorder Services
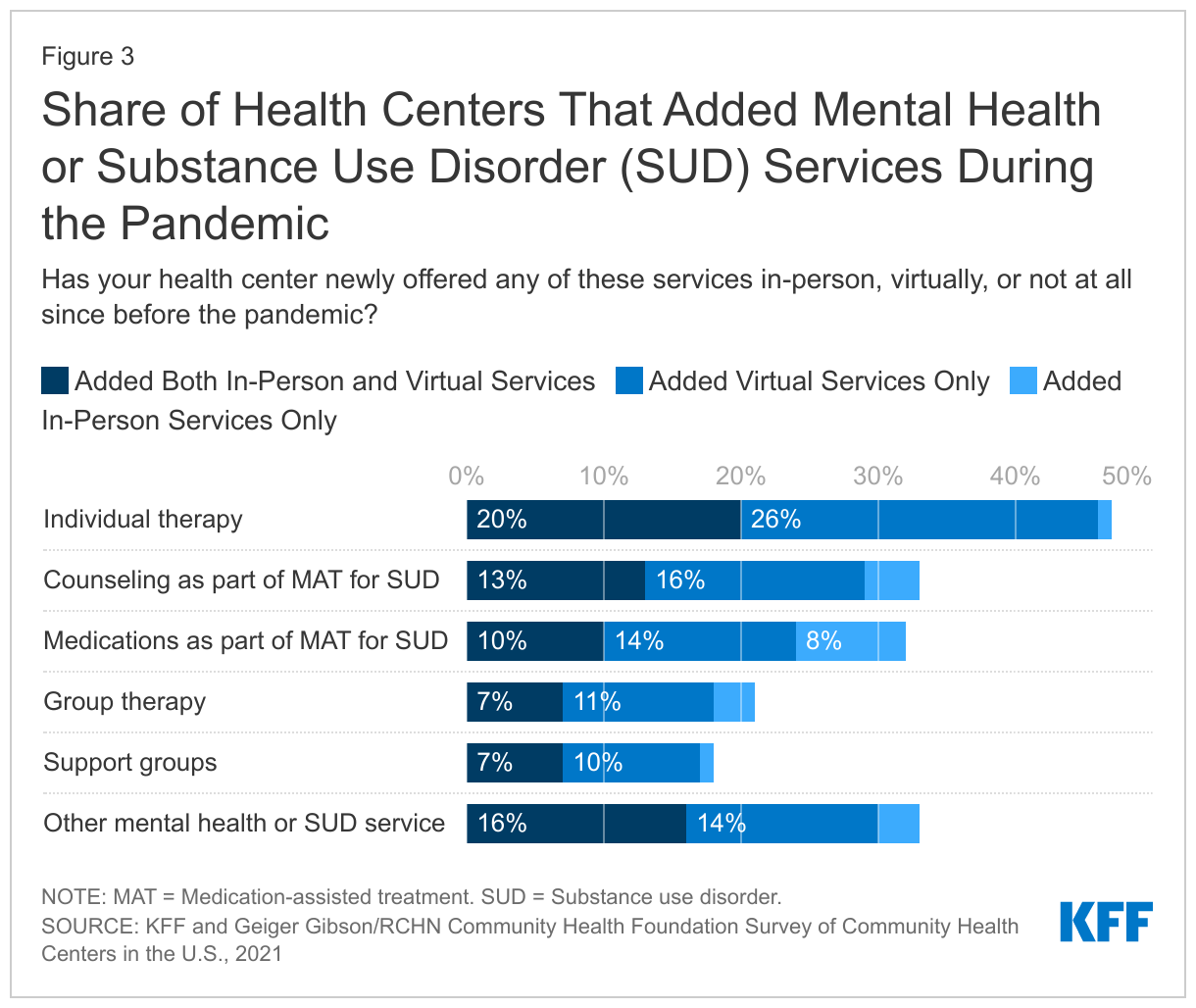
With an uptick in mental health problems, substance use disorders (SUD), and difficulty accessing behavioral health care during the pandemic, health centers have sought to expand access to these services. Going into the pandemic, nearly all health centers provided mental health services on-site and most provided SUD services. By late 2021, over six in ten (64%) health centers reported that they added a new mental health or SUD service. Almost half of responding health centers (47%) added individual therapy as a new service in-person, via telehealth, or both, while around one in five of responding health centers added group therapy and support groups as a new service (21% and 18%, respectively) (Figure 3). Additionally, about a third added counseling (34%) or medication (31%) for medication-assisted treatment (MAT) for opioid use disorder (OUD) as a newly offered in-person or virtual service since the start of the pandemic.
Opioid Use Disorder Services
Many health centers saw an increase in patients with OUD compared to the start of the pandemic. Health centers have historically played a significant role in addressing the opioid crisis as community-based providers with the capacity to provide medication-assisted treatment (MAT) for treating opioid use disorder (OUD). Increasingly, health centers are providing MAT, the standard of care, for OUD treatment. Prior to the pandemic, between 2016 and 2019, HRSA awarded more than $1.4 billion in federal grants to enable health centers to expand access to mental health and substance use disorder (SUD) services. Health centers used these grants to increase staff, improve the integration of behavioral health and primary care, and expand delivery of MAT services.
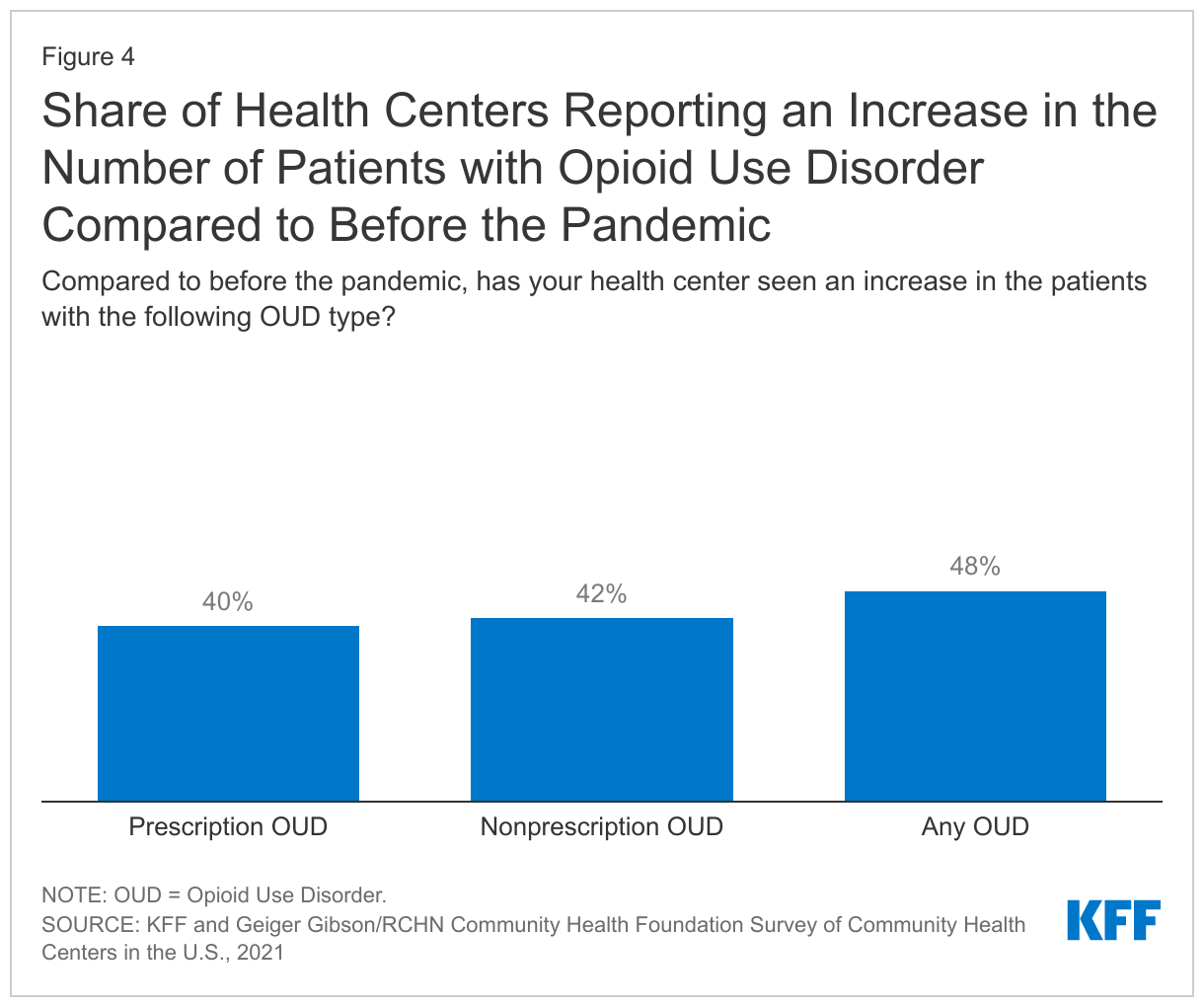
The number of health center patients nationally who received MAT for OUD has grown substantially during the pandemic, likely reflecting the infusion of funding for behavioral health services for health centers in the years leading up to the pandemic and the ongoing need for these services. Additionally, four in ten responding health centers saw an increase in patients with a prescription OUD and 42% saw an increase in non-prescription OUD compared to the start of the pandemic (Figure 4).
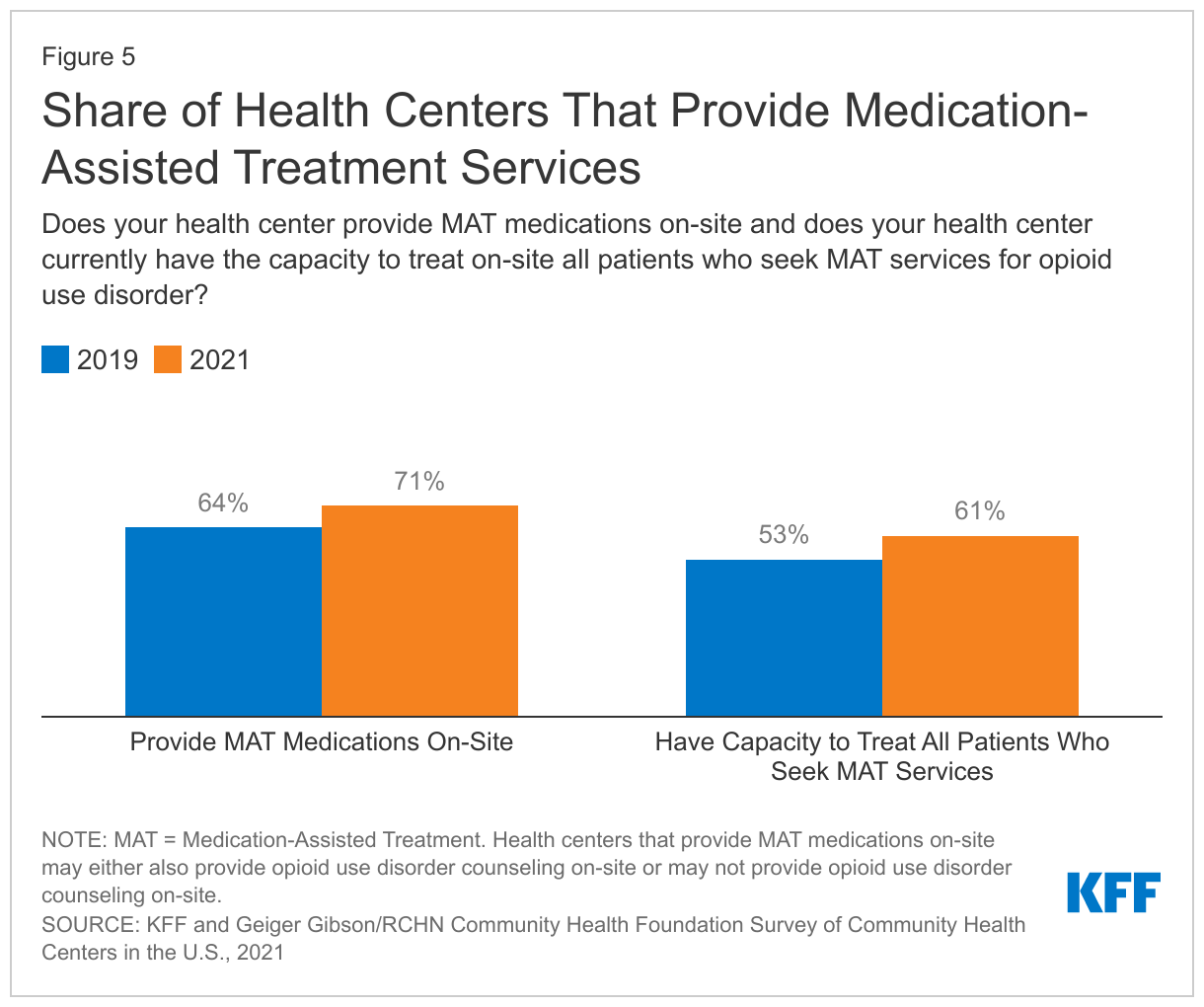
The share of health centers providing MAT increased during the pandemic. Drug overdose deaths increased by 39% nationally from March 2020 to December 2021 and, along with a reported increase in OUD patients, more health centers reported that they provided on-site MAT services for OUD. Over seven in ten (71%) responding health centers reported that their health center provides MAT medication on-site—62% provide MAT medications with OUD counseling and 9% provide only MAT medications—up from 64% in 2019 (Figure 5). The capacity of health centers to provide MAT services has also increased. Over six in ten (61%) responding health centers reported having the capacity to treat all patients who seek MAT services on-site, compared to 53% in 2019 (Figure 5).
Most health centers that provide MAT services for OUD offer more than one medication, giving providers more options to meet patients’ needs. OUD treatment includes the use of one of three medications (methadone, naltrexone, and buprenorphine) along with counseling. Of responding health centers that provide MAT services, two-thirds (67%) provided two OUD medications on-site, up from 60% in 2019, and 4% offer all three medications.
Challenges Facing Health Centers
Managing Patient Needs
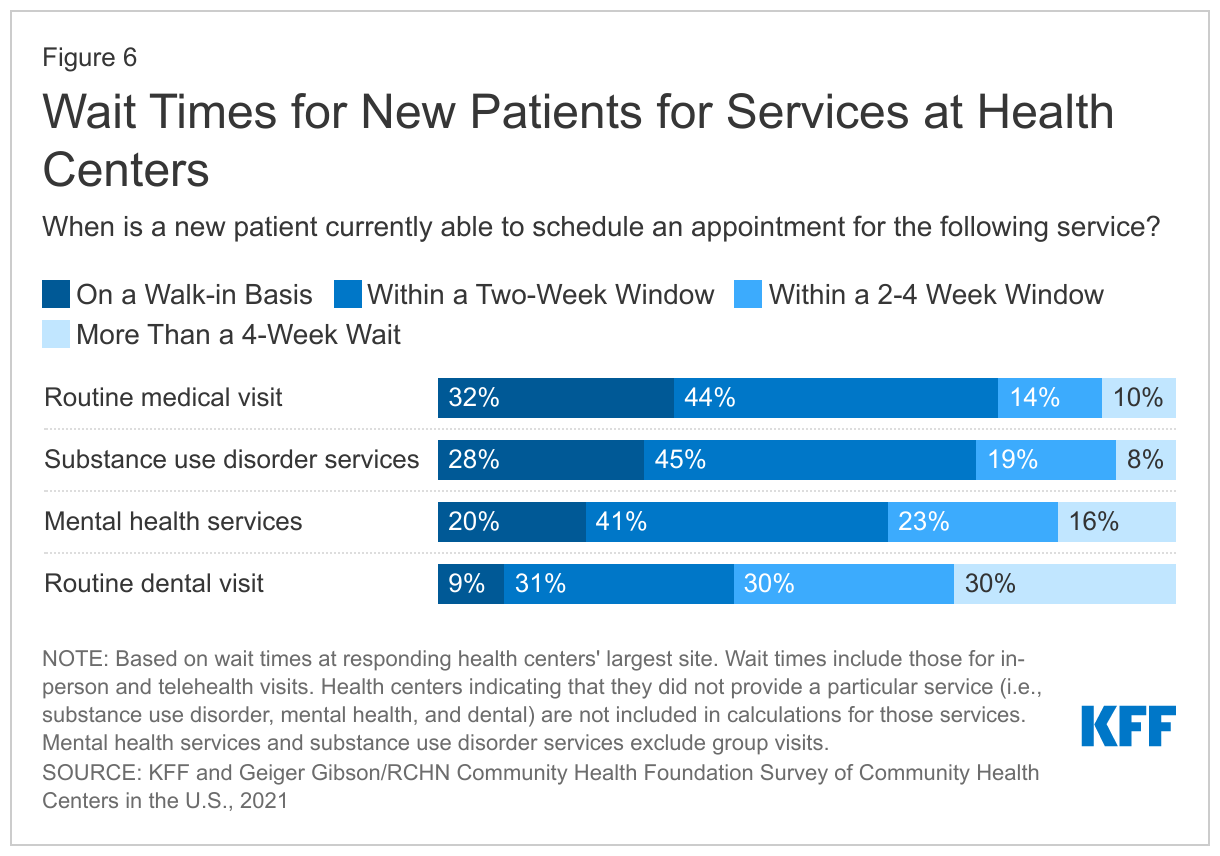
While most health centers reported being able to see new patients in a timely manner for routine medical and SUD services, fewer health centers said they could schedule mental health and dental visits within two weeks. Close to three-fourths of responding health centers said that new patients could schedule a routine medical visit (76%) or SUD service visit (73%) on a walk-in basis or within two weeks (Figure 6). Smaller shares of responding health centers said that new patients could make a mental health service appointment on a walk-in basis or within two weeks (61%) and 40% said that new patients could schedule routine dental visits in the same time frame. These findings may reflect both the effects of the pandemic, as well as continuing challenges in providing these services that predate the pandemic.
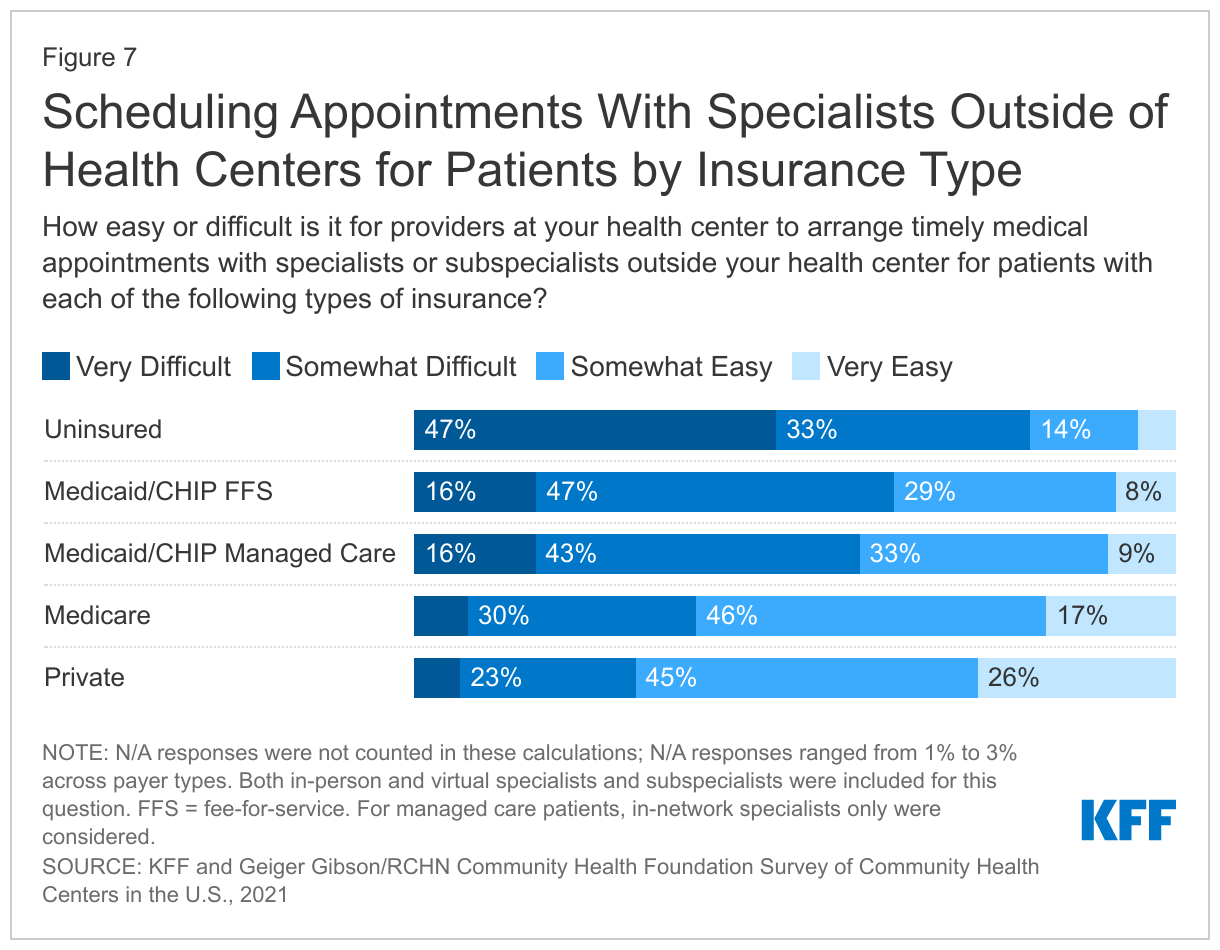
Health centers reported difficulties scheduling timely medical appointments for patients with specialists outside of their health centers, especially for uninsured and Medicaid patients (Figure 7). Over eight in ten (81%) responding health centers reported that it was very or somewhat difficult to schedule an appointment with a specialist for their uninsured patients, while 63% reported difficulties scheduling appointments for Medicaid fee-for-service patients (FFS), which was comparable to the share that reported difficulties for Medicaid managed care patients (58%). Over two-thirds of health center patients are uninsured or enrolled in Medicaid. Fewer health centers reported challenges scheduling appointments for their Medicare (37%) or privately insured patients (28%). Additionally, roughly half of responding health centers said that increased availability of telehealth during the pandemic made no difference in helping to obtain timely appointments with specialists outside their organization, despite the nearly universal increase in telehealth use during the pandemic at health centers and most other outpatient providers. Only about one-third of responding health centers said telehealth made scheduling appointments with specialists outside their organization easier while 10% or less said telehealth made obtaining outside appointments harder.
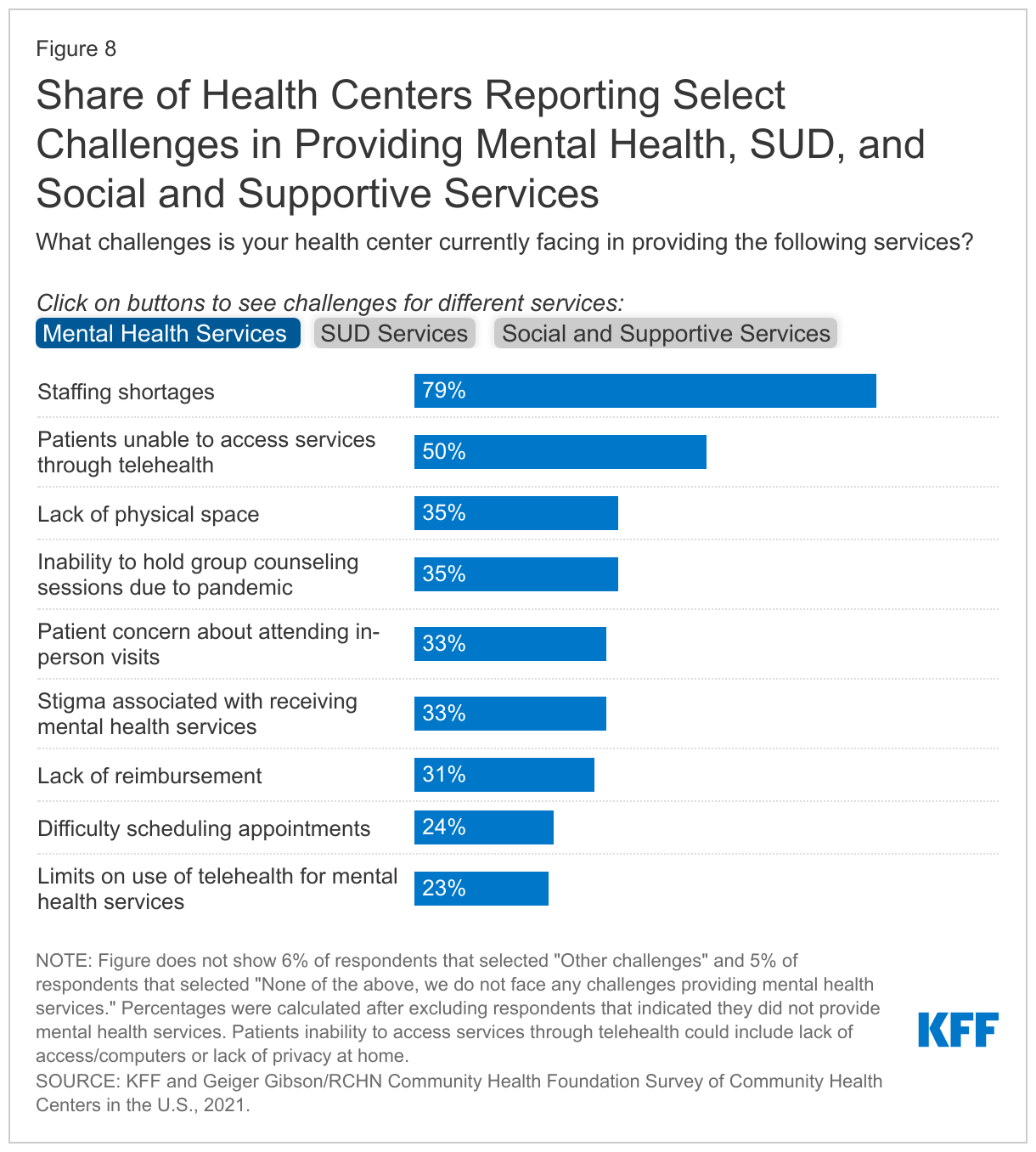
Despite the increased need for certain mental health, SUD, and social and supportive services, health centers cited staffing shortages as the top challenge to providing these services (Figure 8). Almost nine in ten (85%) responding health centers cited staffing shortages as a challenge in providing social and supportive services while nearly eight in ten (79%) and seven in ten (69%) reported staffing issues as a barrier to providing mental health and SUD services, respectively. While health centers have been able to shift to telehealth, especially for mental health visits, almost half of responding health centers cited patients’ inability to access mental health and SUD services through telehealth as a common challenge (50% for mental health and 49% for SUD services). Other barriers to providing social and supportive services included lack of reimbursement, cited by 71% of responding health centers, and lack of physical space for services, cited by 67% of health centers. Fewer health centers reported these barriers to providing mental health and SUD services.
Key Issues to Watch
Health centers face new challenges related to access to and reimbursement from the 340B Drug Discount Program. The 340B Drug Discount Program provides discounted prescription medications to safety net providers, including health centers, allowing them to pass on saving to their patients and to support operations. Virtually all responding health centers (96%) reported that they participate in the 340B Drug Discount Program either through on-site pharmacies or through contracts with outside pharmacies. Among responding health centers that participate in 340B, 86% indicated that they contract with an outside pharmacy to provide 340B drugs to their patients. Recently, pharmaceutical manufacturers have limited the sale of 340B drugs to contract pharmacies. In addition, some pharmacy benefit managers (PBMs), which help to administer and manage prescription drug benefits on behalf of health insurers or state Medicaid agencies, are paying lower rates to 340B-qualified entities than to non-340B entities. Nearly seven in ten (69%) responding health centers with contract pharmacies in the 340B program reported that manufacturers’ restrictions on contract pharmacies have had a negative impact on revenue, and over half (52%) of responding health centers said PBMs’ practice of paying lower rates to 340B entities has had a negative impact on their revenue. A smaller share of responding health centers (28%) said state policy decisions to shift pharmacy benefits from Medicaid managed care to Medicaid fee-for-service had a negative effect while 44% said they did not know the impact.
The end of the continuous enrollment requirement will likely affect millions of Medicaid enrollees, creating uncertainty for health centers and their patients. Provisions in the Families First Coronavirus Response Act (FFCRA) require states to provide continuous coverage for Medicaid enrollees until the end of the month in which the public health emergency (PHE) ends in order to receive enhanced federal funding. The current PHE is in place until mid-July 2022 though it is likely to be extended again. When the PHE ends, states will begin processing redeterminations and many health center patients could lose coverage if they are no longer eligible or face administrative barriers despite remaining eligible. Recent estimates show that between 5.3 million and 14.2 million Medicaid enrollees could lose coverage following the end of the PHE. Most health centers (66%) reported they have taken or plan to take actions to boost eligibility staff to assist their patients with renewals. However, the loss of Medicaid coverage among patients could have financial implications for health centers.
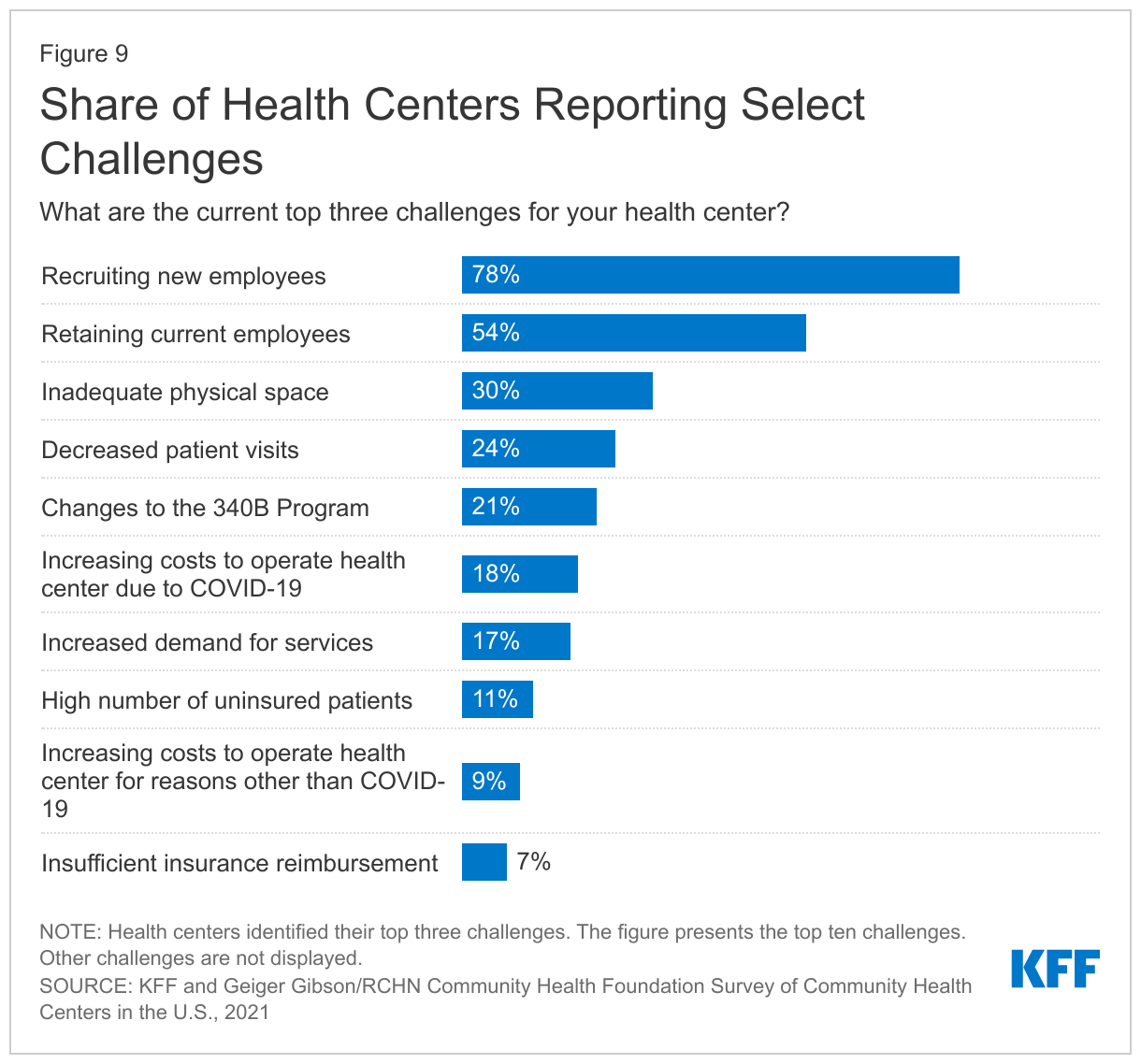
Staff recruitment and retention remain common concerns at health centers nationally. Consistent with challenges in providing key health services, among responding health centers, recruiting new employees and retaining current employees were cited as top overall challenges by 78% and 54% of responding health centers, respectively (Figure 9). These workforce issues, perennial challenges for health centers, have been exacerbated by the pandemic. Inadequate physical space (30%), decreased patient visits (24%), and changes to the 340B program (21%) were also among the top challenges for responding health centers. The share of health centers reporting increasing costs to operate health centers and a high number of uninsured patients as top challenges declined from previous years. In 2019, roughly half (52%) of health centers cited increased operating costs as a major challenge and 24% cited high numbers of uninsured patients. In contrast, in 2021, less than one-third cited increasing operational costs (whether due to COVID-19-related expenses or for other reasons) and just over 10% reported uninsured patients as a major challenge. However, the situation could shift again with the end of the public health emergency if expected coverage losses occur and lead to increased financial strain.
Conclusion
The COVID-19 pandemic has been disruptive for health centers, as for other health care providers, and health centers have adapted to meet patient needs. The pandemic led to declines in utilization of certain services and forced health centers to shift the services they offer and how they deliver care. In response, health centers pivoted to providing telehealth services and have played an active role in COVID-19 testing and vaccination efforts, aided by temporary federal COVID-19 relief funding. They have also responded to the mental health crisis that surfaced during the pandemic by increasing access to mental health, SUD, and OUD services.
Looking ahead, the financial and operational disruptions that health centers have confronted throughout the pandemic will not abate overnight when the PHE declaration ends. Patients will continue to need care, but many are likely to lose Medicaid coverage as states unwind the Medicaid continuous enrollment requirement and, in turn, health centers could see an increase in uncompensated care costs. At the same time, the temporary infusion of federal COVID-19 grant funding for health centers will end and future federal funding for some programs that helped health centers during the pandemic, such as the HRSA COVID-19 Uninsured Program, face an uncertain future. Moreover, ongoing actions by pharmaceutical manufacturers and PBMs limiting access to and reimbursement for 340B drugs have had a negative effect on some health centers’ budgets. In addition to these continued financial uncertainties, health centers are facing ongoing workforce challenges that have been exacerbated by the pandemic. How health centers transition out of the pandemic and address these concurrent challenges will affect how low-income communities access primary care and related services.
Methods
The National Survey of Community Health Centers and Their Response to the Coronavirus Pandemic and Changes to the 340B Program (“2021 survey”) was conducted by KFF and the Geiger Gibson Program in Community Health Policy at the George Washington University in partnership with the National Association of Community Health Centers (NACHC) and supported by the RCHN Community Health Foundation. The survey was fielded from September to December 2021 to the CEOs or project directors of 1,342 federally-funded health centers in the 50 states and the District of Columbia (DC) listed in the 2020 Uniform Data System (UDS). There were 357 responses from 48 states and DC, with a resulting 27% response rate. We verified that there were no duplicate responses from any one health center and that every response answered at least one question in addition to identifying information, which was our criteria for inclusion in the analysis. The survey data were weighted using 2020 UDS data on patient size (total patients), share of patients who are racial/ethnic minorities, and total revenue per patient.
Additional funding support for this brief was provided to the George Washington University by the RCHN Community Health Foundation.
Appendix
Endnotes
- Health centers report the number of vaccinations received by health center patients in the HRSA Health Center COVID-19 Survey. The survey’s questionnaire asks health centers to report the total number of patients receiving a vaccine, and HRSA has clarified that this count includes health center patients receiving vaccinations anywhere, including in settings other than the health center. However, we expect that health centers delivered the vast majority of vaccinations reported in the survey, and the number of patients reported through the survey receiving their vaccinations elsewhere is likely minimal. ↩︎