Considerations for Covering Over-the-Counter Contraception
Note: This policy watch was updated on April 17, 2024 to incorporate the latest available data.
In 2023, the FDA approved the first over-the-counter (OTC) daily oral contraceptive pill, Opill, and more recently, the first OTC at-home test for chlamydia and gonorrhea, Simple 2 Test. With these OTC products becoming available online and/or in stores soon, the implementation issues raised about the availability and affordability of these products and other OTC preventive supplies have garnered the attention of policymakers and advocates. Private insurers and Medicaid generally require a prescription to cover OTC products, so even though these products will be available without the need to obtain a prescription from a clinician, coverage without a prescription will be limited without federal or state action.
In October 2023, the Departments of the Treasury, Labor, and Health and Human Services issued a request for information to gather public input regarding the potential benefits, costs, and implementation considerations of requiring private health insurance plans to cover OTC preventive services and supplies without a prescription.
This policy watch addresses key considerations for the implementation of insurance coverage for non-prescribed OTC contraceptives based on the lessons learned from KFF’s 2023 study of Insurance Coverage of OTC Oral Contraceptives. KFF staff interviewed more than 80 individuals representing key players in states that require state regulated plans to cover certain OTC contraception methods without a prescription and without cost sharing.
Background
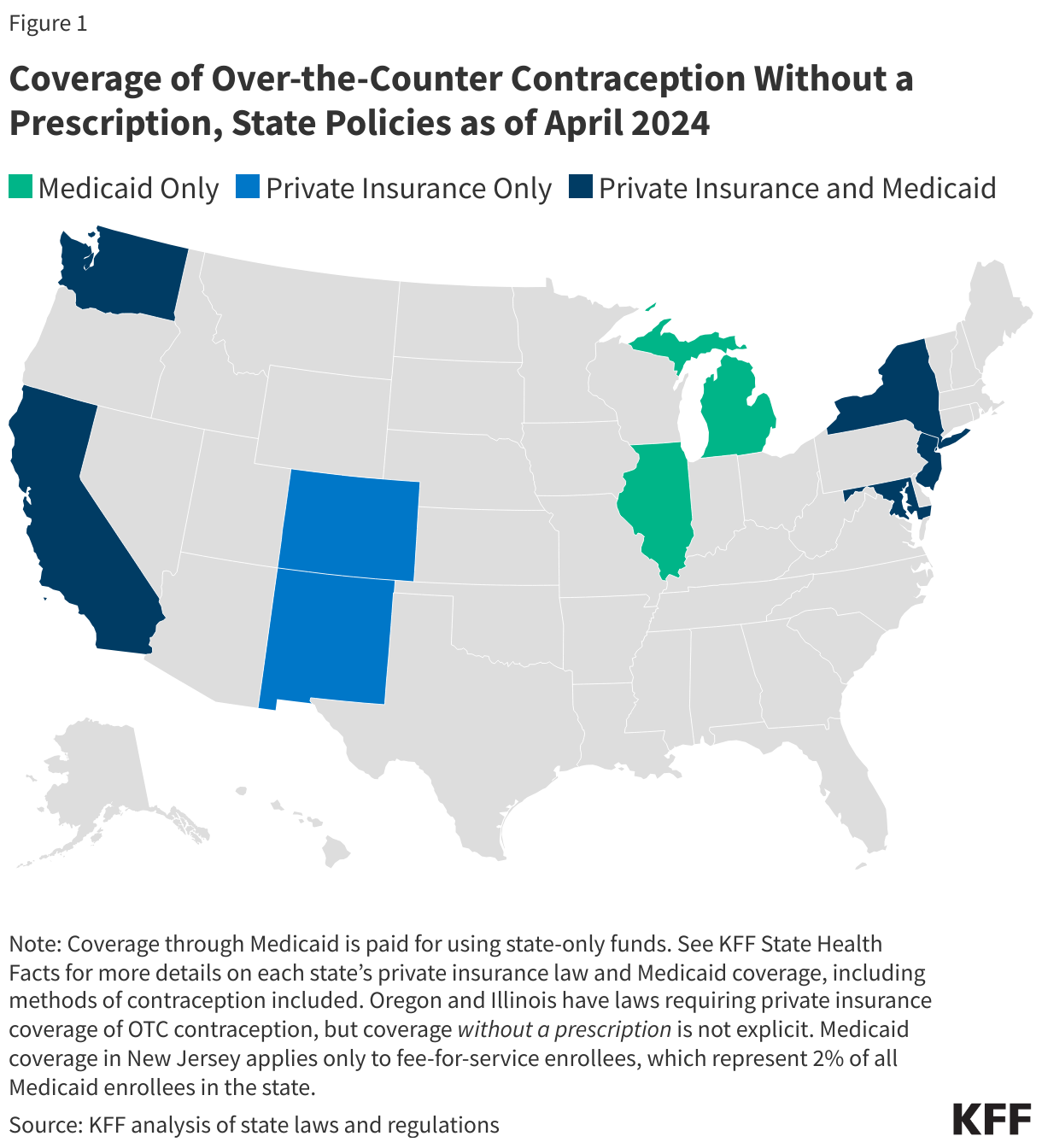
Current federal policy does not require insurance coverage of OTC contraceptives without a prescription (unlike the ACA contraceptive coverage requirements that mandate coverage with no patient cost-sharing with a prescription). To date, however, seven states have passed laws requiring state-regulated private health plans to cover certain OTC contraception, such as emergency contraception and condoms, without the need for a prescription and without cost-sharing (Figure 1). State health insurance requirements apply to individual plans, plans offered by public employers, and fully-insured plans offered by private employers, but not to self-funded plans offered by private employers, which cover nearly two-thirds of workers with employer-sponsored insurance. Seven states use state-only funds to provide coverage for certain non-prescribed OTC contraceptives for Medicaid beneficiaries. In other states, health plans rarely offer this coverage to their enrollees voluntarily.
Billing Protocols for OTC Contraceptives in States that Require Coverage
In states where coverage for OTC contraception is required without a prescription, there are generally two pathways for consumers to receive coverage.
- Direct billing at the pharmacy counter: This is the most commonly used billing method and requires consumers to obtain the product at the pharmacy counter. Depending on the insurer’s protocol, the pharmacist or technician must enter a National Provider Identifier (NPI), a unique, 10-digit number issued by the Centers for Medicare and Medicaid Services (CMS) to health care providers, including pharmacists, which is also used for billing purposes. This claim is then transmitted to the plan, the pharmacy is reimbursed, and the policyholder receives the product in much the same way that most prescribed drugs are processed.
- Purchasing the OTC contraceptive product outside the pharmacy, with the enrollee submitting a pharmacy claim to the plan: This method of coverage is used by few private health plans and is similar to the reimbursement process that was used for some at-home COVID-19 tests. While this option can expand access to coverage in certain situations, it potentially poses financial and logistical barriers for the enrollee because the policyholder needs to pay the cost upfront and navigate the plan’s claims and reimbursement process.
Considerations for Implementing Coverage of OTC Contraception
In general, most private insurance and Medicaid payment systems have been set up to process claims for prescribed drugs and currently lack the infrastructure to process claims for non-prescribed OTC drugs. Key players interviewed by KFF cited several common implementation challenges and possible approaches, including:
- Establishing universal NPI numbers for OTC products and standardized billing protocols: Interviewees noted that billing protocols for non-prescribed OTC contraception vary widely by health insurance plan, leading to confusion for some pharmacists. Some states that have implemented coverage of OTC contraceptives without a prescription for their Medicaid enrollees have created a universal NPI number for each covered OTC contraceptive to avoid the need to for pharmacists or pharmacies to enter their individual NPI numbers for an OTC product. In interviews with pharmacists, some said they were reluctant to enter their own NPI number for a product they did not prescribe, citing concerns about potential legal liability. A standardized billing process across payors would facilitate any federal or state requirement to cover OTC drugs.
- Increasing awareness and communication: There has been little specific outreach about this covered benefit to health plan enrollees and pharmacists, and there has been limited communication about billing protocols between pharmacies, pharmacy benefit managers (PBMs), health plans, and state insurance departments. Increasing awareness and improving communication across key players can help increase utilization of this covered benefit and facilitate coverage for OTC contraceptives.
- Mitigating pharmacist and pharmacy staff overload: The role and scope of pharmacists and pharmacy staff in health care have rapidly expanded over the years, with a growing number of pharmacists dispensing medication, administering vaccines, and counseling patients, among other services. Staff at major drugstore chains recently staged walkouts over difficult working conditions. Processing claims for OTC contraceptives adds another layer of responsibility for pharmacists who are already overstretched. Properly assessing pharmacy staffing needs, compensating pharmacists for the time it takes to process these claims, and streamlining the billing process were identified as factors that could alleviate these challenges and enable pharmacists and other staff to play a role in facilitating coverage of OTC contraceptives.
Broader Implications
Coverage for non-prescribed preventive health care items available over the counter could facilitate access to a broad range of OTC products that support sexual and reproductive health, including emergency contraceptive pills; condoms; folic acid supplements; and the newly-FDA-approved STI tests, and pave the way for new contraceptive products that may become FDA approved for OTC use in the future.
Across the spectrum of key players, the KFF research reveals that there is interest and engagement about the potential of OTC contraception to broaden the availability of and access to contraceptive options, but the extent to which this occurs will depend on many factors, including state and federal policies and guidance, pharmacy engagement, billing systems, and public and provider awareness, and modifications to current systems of coverage.
Additional KFF resources on Over-The-Counter Contraceptive Pills:
Report: Insurance Coverage of OTC Oral Contraceptives: Lessons from the Field
Issue Briefs: