KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Job losses caused by the coronavirus pandemic have threatened to disrupt health coverage for millions of people as most working-age adults get coverage for themselves and their families through their work. Tracking real-time changes in coverage and the uninsured rate is difficult to do with much precision because the large national surveys that produce these estimates lag by months or years, and private surveys generally lack sufficient sample to measure coverage changes precisely. Many real-time surveys have faced challenges of high rates of survey nonresponse (not responding to the survey or particular questions) particularly among populations most likely affected by the economic downturn, including the Census Bureau’s Household Pulse Survey. However, various sources of administrative data allow us to piece together what might be happening to health coverage rates amid the pandemic.
Declines in employer sponsored insurance are far less than overall declines in employment. First, using administrative data insurers file with state regulators (compiled by Mark Farrah Associates TM), we can see how enrollment in employer plans has changed through the end of September. Although employment rates fell by 6.2% from March to September, enrollment in the fully-insured group market decreased by just 1.5% over the same period.
If we extrapolate this finding to the entire group market, including self-insured employer plans, this would suggest that a total of roughly 2 to 3 million people may have lost employer-based coverage between March and September. To be very clear, this is only a rough estimate. We do not have reliable data for self-insured employers (which insure about 6 in 10 people with employer coverage and tend to be larger), and those employers may have made different decisions than fully-insured employers did about layoffs and whether and how to maintain coverage for employees.
Loss of employer-based coverage may have been offset by strong enrollment in Medicaid and Marketplaces. Many of those who lost job-based health coverage would have qualified for Medicaid or for a special enrollment opportunity to purchase individual market health coverage (either on- or off- exchange). Preliminary administrative data for the Medicaid program shows enrollment increased by 4.3 million people (6.1%) from February through July 2020. More recent data for 30 states show that enrollment in managed care plans increased by about 5 million, or 11.3%, from March to September 2020. Nationally, MCOs cover over two-thirds of Medicaid beneficiaries. States attribute these increases to rising unemployment (and loss of employer sponsored insurance) as well as the “maintenance of eligibility” (MOE) requirements tied to a 6.2 percentage point increase in the federal match rate (FMAP) authorized by the Families First Coronavirus Response Act (FFCRA) – which prevents states from disenrolling Medicaid beneficiaries if they accept the additional federal funding.
Using the same administrative data above (from Mark Farah Associates TM), we find that enrollment in the individual market was fairly steady from March to September 2020. In normal years, there is typically more attrition during these months as more people leave the market than come in during special enrollment periods (SEP). However, SEP enrollment was higher this year in healthcare.gov and state based exchanges.
While much is unknown, a review of administrative data suggest that the uninsured rate may not have changed much during the pandemic to date. There is still much we do not know, and these administrative data do not account for other changes like people aging on to Medicare and population growth. Nonetheless, it appears that the decline in employer-based health insurance coverage may have been offset by gains in Medicaid and largely steady enrollment in the individual market.
There are several possible explanations for the relatively modest decrease in employer-based coverage despite massive job losses. First, many of the people who have lost employment likely were never enrolled in coverage through their job in the first place; lower wage workers are less likely to be covered by their employer’s plan and, similarly, job losses have been highest and most sustained among industries that tend to have lower coverage offer rates (e.g., retail, service, hospitality). Second, many people who lost their jobs may have been able to retain their health coverage temporarily. A number of employers elected to keep furloughed or laid off workers enrolled in their firm’s plan at least in the short term. In addition, an unknown number of permanently laid off employees may have elected COBRA (which would be classified as group coverage) at their own expense, although this number is likely small due to the high costs of such coverage. Employment rates are starting to recover but a larger share of people filing unemployment claims say their job loss is permanent compared to earlier in the pandemic, suggesting there may be more coverage loss to come.
That the uninsured rate may not have substantially changed this year could be taken as both good news and bad news. A largely flat uninsured rate would be good news because health insurance coverage rates tend to fall whenever there is an economic downturn in the United States. Between many employers maintaining coverage and the Affordable Care Act along with Medicaid serving as a safety net for those who did lose coverage, the uninsured rate in the U.S. does not appear to have risen nearly as much as it could have, given the scale of employment losses.
The bad news is that, if the uninsured rate has indeed held steady, there are still tens of millions of people without health coverage during the worst pandemic to hit the country in one hundred years. Despite some recent legislation and administrative action aimed at protecting the uninsured from some of the costs associated with COVID-19 testing and treatment, those without coverage still face tremendous financial and health risks.
Four out of ten people who were uninsured before the pandemic could be getting health insurance coverage for free, either through Medicaid or a zero-premium bronze plan on the exchange. Open Enrollment for 2021 coverage on the ACA exchange markets is now in its fifth week and early figures show that, while overall enrollment is strong, new enrollment is about the same as past years. The Trump Administration has drastically reduced funds for ACA outreach and marketing activities, as well as for navigators who help people enroll in Marketplace coverage. President-elect Biden has vowed to reinstitute funding for ACA marketing, outreach, and navigator programs. The federal Open Enrollment period will have ended by the time Biden takes office, but he could open a new SEP without limitations on who qualifies to enroll.
To date, the federal government has taken several steps to address the health and economic consequences of the COVID-19 pandemic, including sending billions of dollars to hospitals and other providers, providing economic stimulus payments to a majority of Americans, and requiring public and private insurers to provide free coverage of coronavirus testing. But the pandemic has exposed long-standing gaps in the U.S. health care system and brought fresh reminders of the health care affordability challenges facing many people, with and without insurance, including people with Medicare.
Medicare provides significant health and financial protections to more than 60 million Americans, but there are gaps in coverage and high cost-sharing requirements that can make health care difficult to afford, particularly for beneficiaries with modest incomes who lack supplemental coverage, such as employer-sponsored retiree health coverage, Medigap, or Medicaid. Beneficiaries are responsible for Medicare’s premiums, deductibles and other cost-sharing requirements, unless they have supplemental coverage or have incomes and assets low enough to qualify for the Medicare Savings Programs, which help cover Medicare Part A and Part B out-of-pocket costs, or the Medicare Part D low-income subsidy (LIS) program, which helps with Part D premiums and cost sharing only.
Beneficiaries in traditional Medicare with no supplemental coverage are vulnerable to high out-of-pocket expenses because Medicare, unlike marketplace and large employer plans, has no cap on out-of-pocket spending for covered services. But even those with supplemental coverage can face affordability challenges. Although Medicare Advantage plans are required to provide an annual out-of-pocket limit, beneficiaries enrolled in Medicare Advantage plans could still face high out-of-pocket costs, depending on the services they use, the drugs they take, and costs charged by their specific plan. And although beneficiaries with Medigap supplemental coverage have help with cost-sharing requirements for Medicare-covered services and protection against catastrophic expenses, premiums for these policies can be costly. With half of all Medicare beneficiaries living on an income of less than $30,000 per person, these affordability concerns could be compounded for some by the economic recession caused by the COVID-19 pandemic.
This report analyzes several policy options that could help make health care more affordable for people covered by Medicare:
For each of the options, we discuss implications and tradeoffs, including the added cost to the federal government of providing additional protection for beneficiaries. This report focuses on options to improve affordability of current Medicare benefits, rather than options that would expand the benefits Medicare covers, such as adding coverage of dental, vision, or hearing services. See Methodology for detail on data sources and methods.
Key Takeaways
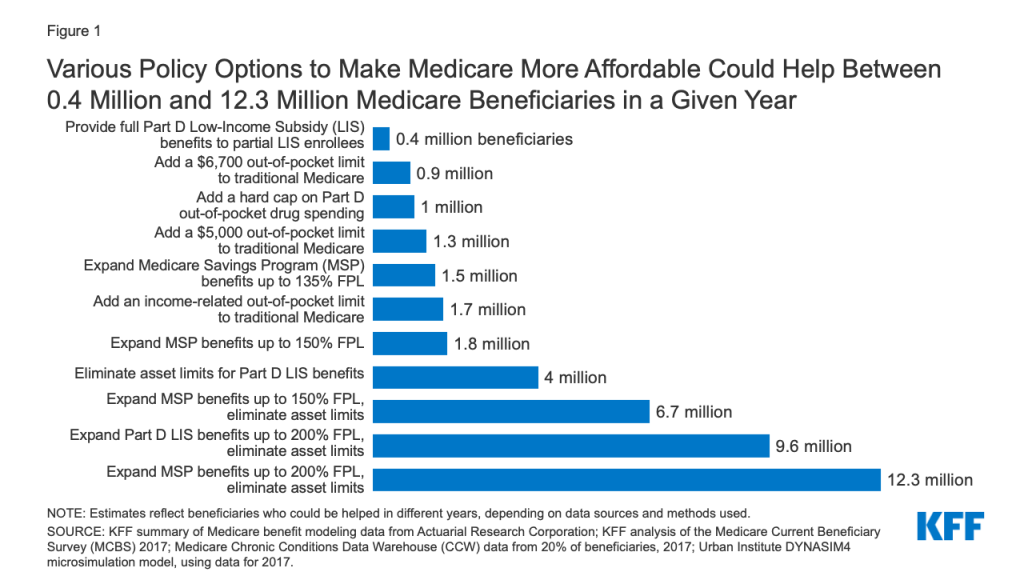
The policy options examined in this analysis to help make health care more affordable for people covered by Medicare vary in the number of beneficiaries who could be helped and how much help they could receive (Figure 1). Each option would also have cost implications for Medicare and/or other payers, as described more fully in the longer discussion of each option following the introduction.
Figure 1: Various Policy Options to Make Medicare More Affordable Could Help Between 0.4 Million and 12.3 Million Medicare Beneficiaries in a Given Year
Adding an annual out-of-pocket spending limit to traditional Medicare for Medicare Part A and B cost-sharing requirements would limit the risk of incurring high and potentially unaffordable expenses for nearly six million beneficiaries in traditional Medicare who have no supplemental coverage. The number of beneficiaries likely to be helped in any given year, and the average savings per beneficiary reaching the limit, would vary based on the amount of the out-of-pocket limit and what counts toward the limit. For example, adding a $6,700 out-of-pocket limit to Medicare Parts A and B would help 0.9 million beneficiaries in 2021, reducing their out-of-pocket costs for Medicare-covered services by approximately $2,700, on average, while adding an income-related limit would help 1.7 million beneficiaries, with average savings of nearly $2,200 in 2021. Adding an out-of-pocket limit would help people on Medicare with complex care needs, such as those who require one or more inpatient stays followed by a lengthy stay in a skilled nursing facility, or those who need high-cost medications that are covered under Medicare Part B. Adding an out-of-pocket limit to traditional Medicare would also lower Medigap premiums and premiums for employer or union-sponsored retiree health benefits for Medicare-eligible retirees, because the new out-of-pocket limit in traditional Medicare would reduce the amount of claims to be paid by these payers, while at the same time increasing Medicare Part B premiums, as Medicare assumes these costs above the limit.
Adding a hard cap on out-of-pocket prescription drug spending to the Part D benefit would eliminate potential exposure to high drug costs for nearly 39 million beneficiaries currently enrolled in Part D plans who are not receiving low-income subsidies. Had the Part D benefit included a cap in 2017, with no other changes in benefit design, it would have lowered out-of-pocket drug spending for approximately 1 million Part D enrollees with high drug costs, with average savings of approximately $1,400 per enrollee that year.
Expanding eligibility under the Medicare Savings Programs would help more low- and modest-income beneficiaries with Medicare premiums and cost-sharing requirements, with the number helped and the amount of assistance varying depending on the option. For example, expanding financial assistance under the Medicare Savings Programs by covering cost sharing for people currently receiving Part B premium assistance only would lower out-of-pocket costs for 1.5 million Medicare beneficiaries, with estimated average savings of $1,500 in 2020. Raising eligibility for the Medicare Savings Programs up to 150% or 200% of poverty and eliminating the asset test could help 7 million beneficiaries in total (expanding eligibility up to 150%) or 12.3 million beneficiaries (expanding eligibility up to 200%). Among these newly-eligible beneficiaries, estimated average savings would be $3,235 in 2020 for those who qualified for assistance with both premiums and cost sharing. For beneficiaries with incomes at 150% of poverty in 2020 ($19,140), this total savings represents 17% of their incomes. The group of beneficiaries who are helped under an approach that expanded eligibility up to 200% FPL with no asset test includes an estimated 3.9 million beneficiaries in communities of color, including 1.2 million Black beneficiaries, 1.9 million Hispanic beneficiaries, and 0.7 million beneficiaries in other racial and ethnic groups.
Expanding eligibility under the Part D Low-Income Subsidy program would help more low and modest income beneficiaries with their Part D prescription drug plan premiums and cost-sharing requirements, with the number helped and the amount of assistance varying depending on the option. For example, providing full Part D low-income subsidies to beneficiaries who would otherwise be eligible for partial subsidies would lower prescription drug-related costs for 0.4 million Medicare beneficiaries, with estimated saving ranging from $270 to $560 in 2020, depending on the level of help they are eligible for under current law. Raising eligibility for Part D premium and cost-sharing subsidies from 150% FPL to 200% FPL, and eliminating the asset test would lower prescription drug-related costs for 9.6 million Medicare beneficiaries. Part D enrollees who are not currently eligible for premium or cost-sharing assistance would see estimated savings of $850 in 2020 on their Part D prescription drug cost sharing and premiums, on average, if they qualified for full LIS benefits.
As noted above, each of these options would also have cost implications for Medicare that would vary depending upon specific policy features. In addition, some of these options would have spillover effects for other payers (Medicaid, employers and unions). These effects are discussed more fully below.
Medicare plays a primary role in providing health care to more than 60 million older adults and younger adults with disabilities, but many people on Medicare still struggle with high out-of-pocket health care costs. Medicare provides protection against the costs of many health care services, but traditional Medicare has relatively high deductibles and cost-sharing requirements and places no limit on beneficiaries’ out-of-pocket spending for services covered under Parts A and B. In addition, for beneficiaries in both traditional Medicare and Medicare Advantage, there is no hard cap on out-of-pocket spending under the Part D prescription drug benefit.
In light of Medicare’s cost-sharing requirements and lack of an annual out-of-pocket spending limit, beneficiaries in traditional Medicare with no supplemental coverage are vulnerable to high out-of-pocket expenses. But even those with supplemental coverage may face health care affordability challenges. Although Medicare Advantage plans are required to provide an annual out-of-pocket limit, beneficiaries enrolled in Medicare Advantage plans could still face high out-of-pocket costs, depending on the services they use, the drugs they take, and costs charged by their specific plan. And although beneficiaries with Medigap supplemental coverage have help with cost-sharing requirements for Medicare-covered services and protection against catastrophic expenses, premiums for these policies can be costly.
The burden of out-of-pocket spending among Medicare beneficiaries is significant. The average person with Medicare coverage spent $5,460 out of their own pocket for health care, including premiums and service-related costs, in 2016. One in six Medicare beneficiaries reported problems getting care or delayed care due to cost, or had problems paying medical bills in 2017, with higher rates reported among beneficiaries in fair or poor health, those with low incomes, and those without supplemental coverage. Out-of-pocket spending on health care costs consumes a large share of individual Social Security income – 41% on average in 2013 – and is projected to consume a growing share of income for older adults over time. The economic downturn brought about by the pandemic, resulting in job losses and involuntary retirement among older adults, coupled with rising health care costs, could strain financial resources among some older adults for years to come, posing a threat to retirement security.
Although paying for health care costs can be burdensome for people with Medicare, beneficiaries with low incomes can get help paying their Medicare Part A and Part B premiums and cost-sharing expenses from Medicaid through the Medicare Savings Programs (MSPs), and Part D premiums and cost sharing from Medicare through the Part D Low-Income Subsidy (LIS) program. Most, but not all beneficiaries who get help through the Medicare Savings Programs are also eligible for full Medicaid benefits, which can include long-term care services, and often other services such as dental and vision.
Although difficult to measure precisely due to data limitations, we estimate that the share of Medicare beneficiaries with incomes below 150% FPL who are enrolled in the Medicare Savings Programs is somewhere between 50% and 65%, and 55% to 70% are enrolled in the Part D Low-Income Subsidy Program (although not everyone with incomes at this level are eligible to begin with due to the asset tests in both programs).1 Eligibility for the Medicare Savings Programs and the Medicare Part D Low-Income Subsidy program is generally stricter than coverage under Medicaid in states that elected to expand Medicaid under the ACA, and stricter than eligibility for premium tax credits and cost-sharing reduction subsidies in the ACA marketplace. Both the Medicare Savings Programs and Part D LIS impose an asset test, in addition to an income test.
Many low-income Medicare beneficiaries do not qualify for the MSPs or LIS, either because of assets above allowable limits or income that, while still low, is just above current thresholds. For example, nearly one million beneficiaries with incomes less than 150% FPL had assets above the highest allowable limit for LIS in 2017 ($12,320 for individuals/$24,600 for couples) but less than $30,000 in assets in 2017.2 Furthermore, certain groups of beneficiaries are less likely than others to be receiving assistance from the Medicare Savings Programs, which could expose them to higher health care costs. For example, nearly one in five Black and Hispanic Medicare beneficiaries (18%, respectively) have incomes below 150% of poverty but are not enrolled in the Medicare Savings Programs, compared to 14% of White beneficiaries.3 Similarly, 17% of beneficiaries ages 85 and older and 16% of beneficiaries ages 74 to 85 have incomes below 150% of poverty and are not enrolled in these programs, compared to 14% of beneficiaries ages 65 to 74.4
In the midst of the health and economic crisis brought about by the COVID-19 pandemic, and in light of the gaps in Medicare’s financial protections and in existing financial assistance programs available to low-income beneficiaries, there are several options policymakers could consider that would help to ease the financial burden on lower-income Medicare beneficiaries and those who are exposed to high out-of-pocket costs. This brief analyzes four policy options, and provides estimates of the potential number of beneficiaries who could be helped by each policy option. It also examines the potential out-of-pocket savings for beneficiaries for each option, and possible budgetary effects for federal and state governments. (See Methodology for details on the data and methods used in this analysis.)
Options to Improve Medicare’s Financial Protections
Add an Out-of-Pocket Limit to Traditional Medicare
Traditional Medicare currently places no limit on the out-of-pocket costs that beneficiaries are required to pay each year for services covered under Part A (hospital insurance) and Part B (supplementary medical insurance). This gap in Medicare’s financial protection is a relic from an earlier era, and makes coverage under traditional Medicare unlike Medicare Advantage plans and private coverage offered by employers or in the ACA marketplace, where annual out-of-pocket limits are generally required by law.
Most beneficiaries in traditional Medicare have supplemental coverage that helps cover cost-sharing requirements, such as the Medicare Savings Programs, employer or union-sponsored retiree health benefits, and Medigap policies. In addition, beneficiaries enrolled in Medicare Advantage plans in 2020 have the protection of an out-of-pocket limit for services covered under Medicare Parts A and B, not to exceed $6,700 for in-network services, and $10,000 for services provided out-of-network. But premiums for retiree health and Medigap supplemental coverage can be expensive, and not all beneficiaries want to accept the network restrictions that come with enrolling in a Medicare Advantage plan in order to get an out-of-pocket spending cap.
The nearly six million beneficiaries who do not have supplemental coverage can face significant expenses for medical care if they get sick – including a $1,408 hospital deductible in 2020, daily costs for extended stays in a hospital or skilled nursing facility, and 20% coinsurance for high-cost physician-administered drugs, such as chemotherapy drugs. These costs can be a particular concern for beneficiaries with modest incomes with no supplemental coverage. Nearly 4 in 10 (39%) beneficiaries in traditional Medicare with no supplemental coverage have incomes less than $20,000 a year, nearly 3 in 10 (29%) are in fair or poor health, nearly a quarter (23%) are people of color, and 15% are age 85 or older.
Using a model developed in consultation with the Actuarial Research Corporation, we examined three options for adding an out-of-pocket limit to traditional Medicare, with no other changes in deductibles or cost-sharing requirements:
A uniform $5,000 out-of-pocket spending limit.
A uniform $6,700 out-of-pocket spending limit.
An income-related out-of-pocket spending limit, beginning at $3,350 for beneficiaries with incomes up to 150% of poverty and scaling up to $9,500 for beneficiaries with incomes above 1,000% of poverty (no asset test would apply).
Below we provide estimates of the number of people who could be helped under these different options and estimated budgetary effects in terms of both out-of-pocket spending, and federal and state government spending. The estimates we present below assume the out-of-pocket spending limit would apply to beneficiaries’ own out-of-pocket spending and to spending paid by Medicaid on behalf of dually-eligible beneficiaries. Payments made by employer and union-sponsored plans for deductibles and cost-sharing requirements on behalf of retirees and payments from Medigap insurers would not count toward the out-of-pocket spending limit.
Beneficiary Effects
Adding an out-of-pocket spending limit to Medicare would help the relatively small number of beneficiaries in traditional Medicare with exceedingly high medical costs in any given year, but disproportionately benefit those with serious illnesses who do not have supplemental coverage, including beneficiaries who take high-cost Part B drugs for cancer or other diseases, beneficiaries with one or more inpatient hospital admission, and those who have extended stays in a skilled nursing facility, including beneficiaries with SARS-CoV-2 who account for a disproportionate share of people in the U.S. hospitalized with COVID-19.
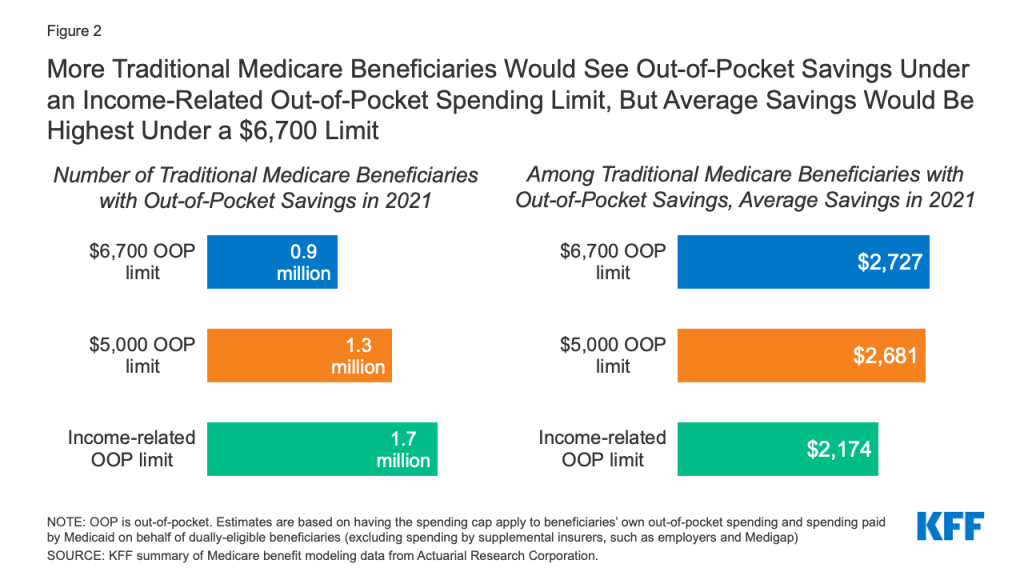
Based on the three out-of-pocket spending limits we evaluated, the estimated number of traditional Medicare beneficiaries who could see lower out-of-pocket health care costs if this proposal were implemented in 2021 would range from 0.9 million to 1.7 million (Figure 2):
Figure 2: More Traditional Medicare Beneficiaries Would See Out-of-Pocket Savings Under an Income-Related Out-of-Pocket Spending Limit, But Average Savings Would Be Highest Under a $6,700 Limit
0.9 million Medicare beneficiaries would benefit from a $6,700limit on out-of-pocket spending in 2021, or 2% of all traditional Medicare beneficiaries overall, reducing their out-of-pocket spending on Medicare-covered services by more than $2,700.
1.3 million Medicare beneficiaries would benefit from a $5,000 limit on out-of-pocket spending in 2021 (3% of all traditional Medicare beneficiaries), reducing their out-of-pocket spending on Medicare-covered services by just under $2,700.5
1.7 million Medicare beneficiaries would benefit from an income-related spending limit (4% of all traditional Medicare beneficiaries), reducing their out-of-pocket spending on Medicare-covered services by $2,200.
The estimated number of people expected to benefit directly from a limit on out-of-pocket spending in a given year is highest under the income-related limit because this option provides a lower limit of $3,350 for beneficiaries with incomes up to 150% of poverty than the limit for beneficiaries with higher incomes. Since many Medicare beneficiaries have relatively low incomes, more beneficiaries would have spending that reaches this lower spending limit, than with a uniform $5,000 or $6,700 spending limit that applies to all beneficiaries. Among these three options, fewer beneficiaries would have spending high enough to reach a uniform $5,000 limit than under the income-related approach, and fewer still would have spending high enough to reach the $6,700 limit.
Beneficiaries with higher levels of utilization would be expected to save more than the average under each option, such as Medicare beneficiaries with two or more hospital stays and those who are hospitalized and then have a skilled nursing facility stay. For example, under the $6,700 spending limit, 0.3 million Medicare beneficiaries with two hospital stays would experience a $3,500 reduction in out-of-pocket costs in 2021, and 0.2 million beneficiaries who are hospitalized and have a lengthy skilled nursing facility stay would see a $4,100 reduction in out-of-pocket costs.
Although the number of beneficiaries helped by an annual out-of-pocket limit in any given year may be relatively small, an annual out-of-pocket limit would help a larger number of beneficiaries over a longer timeframe of multiple years. For example, a prior analysis conducted by ARC for KFF and MedPAC found that the share of traditional Medicare beneficiaries with cost-sharing liability above an annual out-of-pocket maximum of $5,000 for one or more years would increase from 6-7% in the first year to 19% after five years and 32% over 10 years. In other words, over 10 years, nearly one-third of Medicare beneficiaries would have annual cost-sharing liability above the annual out-of-pocket limit in one or more years over that time period.
Having a spending cap in traditional Medicare would provide beneficiaries with the peace of mind that comes from knowing they would not be responsible for thousands of dollars in liability if they incur high medical costs at some point in the future. However, under each of these options, most beneficiaries in traditional Medicare would see no change in their out-of-pocket costs for Medicare-covered services in a given year, since they would not have spending high enough to reach the limit; however their Part B premiums would be expected to increase modestly, due to an overall increase in Part B spending.
The addition of a spending limit to traditional Medicare could mean fewer beneficiaries enroll in Medicare Advantage to obtain the protection of the out-of-pocket cap. It could also mean fewer people choose Medigap to supplement traditional Medicare, generating savings on Medigap premiums for those who drop their policies, which could amount to more than $2,000 in savings in a given year.6 Beneficiaries who choose to keep Medigap even with an out-of-pocket limit in traditional Medicare could see a reduction in their premiums, because Medigap insurers would not be liable for costs that enrollees incur above the new limit. With savings from a reduction in claims associated with spending above the new out-of-pocket limit, Medigap insurers could pass savings on to policyholders in the form of lower premiums to meet loss ratio requirements. Similarly, employers and unions that continue to sponsor retiree health benefits for Medicare-eligible retirees would likely realize savings associated with a Medicare out-of-pocket spending limit, which could lead to a reduction in plan costs for sponsors (employers and unions) and a reduction in premiums for retirees.
Budget Effects
According to model estimates, the net one-year federal cost of adding an out-of-pocket spending limit to traditional Medicare in 2021 would range from approximately $11 billion under the $6,700 limit to $15 billion under the $5,000 limit and $16 billion under the income-related limit. These estimates are based on the spending limit applying to beneficiaries’ own out-of-pocket spending plus Medicaid cost-sharing payments on behalf of dually-eligible beneficiaries. But the federal budget effects under each spending limit would be lower if the spending limit applied only to beneficiaries’ own out-of-pocket spending, and higher if the limit applied to spending by all payers, including beneficiaries, Medicaid, and supplemental insurers such as employers and Medigap. The net federal cost increases as more payer spending counts towards the limit because a larger number of beneficiaries would reach the spending limit and Medicare would assume liability for more beneficiaries’ costs above the limit, displacing spending by Medicaid and supplemental insurers (Table 1).
For example, under the $6,700 spending limit, net federal spending in 2021 would increase by $5.4 billion if the spending limit applies to beneficiary out-of-pocket costs only; $10.9 billion if the limit applies to beneficiaries’ out-of-pocket costs and payments made on their behalf by Medicaid; and $18.6 billion if the limit applies to spending by beneficiaries, Medicaid, and supplemental insurers, including employer-sponsored retiree plans and Medigap. Under the income-related spending limit, net federal spending in 2021 would increase by $8.2 billion if the spending limit applies to beneficiary out-of-pocket costs only; $16.2 billion if the limit applies to beneficiaries’ out-of-pocket costs and payments made on their behalf by Medicaid; and $24.7 billion if the limit applies to spending by beneficiaries, Medicaid, and supplemental insurers, including employer-sponsored retiree plans and Medigap. Net federal spending effects for the $5,000 limit are similar to the income-related limit.
These Medicare spending estimates factor in higher Medicare payments to Medicare Advantage plans, which would result from adding an out-of-pocket spending limit to traditional Medicare (a benefit that Medicare Advantage plans are currently required to provide). This is because, in the absence of changes to how Medicare Advantage benchmarks are calculated (an amount used in determining how plans are paid), the new spending limit would increase per capita costs in traditional Medicare, leading to higher benchmarks, which would in turn likely lead to higher Medicare Advantage plan bids and higher payments to plans.
Other payers. Having the spending limit apply to Medicaid cost-sharing payments for dually-eligible beneficiaries would reduce state Medicaid liability by between $2 billion and $3 billion in one year alone (2021), depending on the spending limit, which could be an important consideration at a time when state budgets have been decimated by tax revenue losses resulting from the COVID-19 pandemic.
If, however, the spending limit applied to payments by supplemental payers such as employers and unions on behalf of retirees, it would result in savings for those payers (although we did not model these estimates) and significantly higher costs for Medicare Even if the Medicare limit did not count spending by employer/union plans on behalf of retirees, employers/unions could realize savings if they modify their benefits to limit their own liability. There is some risk that the added protection in Medicare would accelerate the erosion of retiree health benefits.
A new out-of-pocket limit for traditional Medicare could also have spillover effects for Medigap policyholders and insurers. If Medigap policyholders decide to drop their policies due to the added protection of an out-of-pocket limit under Medicare, they would incur higher costs for Medicare-covered services (while also seeing lower premiums), which could lead to lower utilization of these services as well as lower and Medicare spending. The reduction in spending for Medicare-covered services due to lower utilization could partially offset additional costs to the federal government associated with adding an out-of-pocket limit. We did not incorporate any such potential changes in the model. If, instead, beneficiaries choose to retain their Medigap policies, they would likely see a reduction in premiums, as noted above (See our previousanalyses of Medicare benefit redesign options for more discussion of possible behavioral responses by individuals and other payers to an out-of-pocket limit.)
Establish a Hard Cap on Out-of-Pocket Spending In Medicare Part D
In 2020, 46.5 million of the more than 60 million people covered by Medicare are enrolled in Part D, which is a voluntary outpatient prescription drug benefit for people with Medicare, provided through private plans approved by the federal government. The Medicare Part D standard benefit includes several phases, including a deductible, an initial benefit period, a coverage gap, and catastrophic coverage. Under the current structure of Part D, when enrollees reach the catastrophic coverage phase, they pay 5% of their total drug costs. Some beneficiaries with low incomes and modest assets are eligible for assistance with Part D plan premiums and cost sharing through the Part D Low-Income Subsidy program, including assistance with catastrophic drug costs, but in 2020, 33.9 million Part D enrollees are not receiving this assistance.
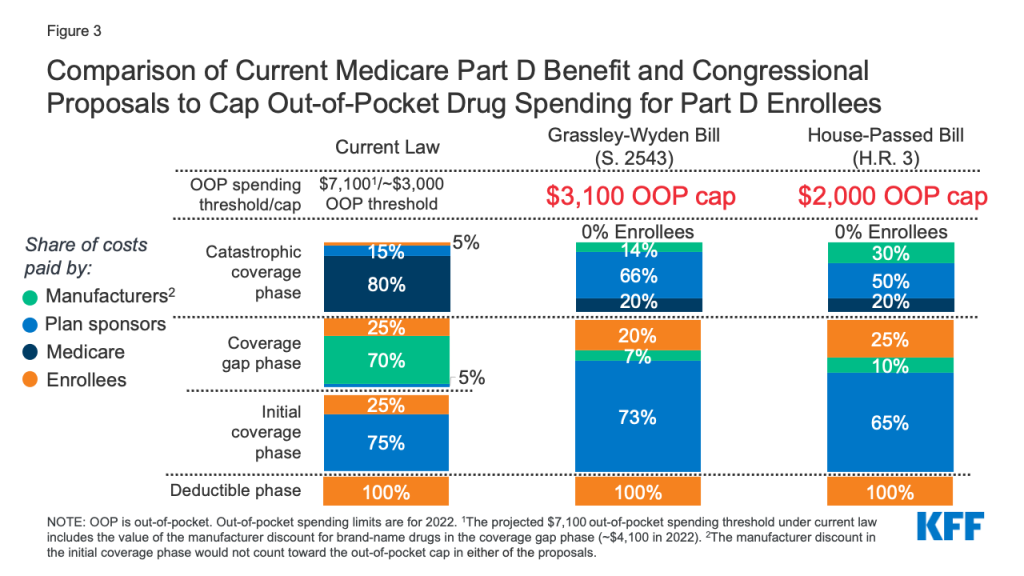
A growing number of policymakers have expressed concern about the absence of a hard cap on out-of-pocket spending for Part D enrollees, with bipartisan support for proposals that would modify the design of the Part D benefit and establish an out-of-pocket spending limit. This proposal was included in drug price legislation that passed the House of Representatives in December 2019 (H.R. 3, Elijah E. Cummings Lower Drug Costs Now Act), legislation sponsored by Senators Chuck Grassley (R-IA) and Ron Wyden (D-OR) of the Senate Finance Committee (S. 2543, Prescription Drug Pricing Reduction Act of 2019), and a Trump Administration FY2020 budget proposal (Figure 3). The Medicare Payment Advisory Commission has also recommended eliminating beneficiary out-of-pocket spending for high drug costs in Part D, along with changes to liability for costs above the spending limit.
Figure 3: Comparison of Current Medicare Part D Benefit and Congressional Proposals to Cap Out-of-Pocket Drug Spending for Part D Enrollees
Beneficiary Effects
Adding an out-of-pocket spending limit in Part D would provide substantial savings for beneficiaries who have high drug costs, and protection against exposure to high drug costs for those who may need costly medications at some point in time. Beneficiaries with out-of-pocket spending above the catastrophic threshold may be taking one high-cost specialty drug, for conditions such as cancer, multiple sclerosis, or hepatitis C, or multiple relatively expensive drugs.
In 2017, over one million Part D enrollees had out-of-pocket spending in the catastrophic phase, with average annual out-of-pocket costs exceeding $3,200 – over six times the average for all enrollees who did not receive Part D Low-Income Subsidies that year. Part D enrollees without low-income subsidies who had high out-of-pocket drug costs in 2017 would have saved approximately $1,400 per person, on average (or $1.4 billion in the aggregate) if Part D had a hard cap on out-of-pocket spending that year, rather than requiring enrollees to pay up to 5% coinsurance in the catastrophic phase, assuming no other changes to the benefit design.
For now, there are no currently approved prescription drug treatments for COVID-19 covered under Part D. If a treatment or cure is developed, covered under Part D, and with a high price tag, a hard cap on out-of-pocket drug spending under Part D would help to address affordability concerns for beneficiaries with COVID-19 who do not receive low-income subsidies.
Budget Effects
Adding a hard cap to out-of-pocket drug spending under Part D without any other changes to the Part D benefit design would increase Medicare spending by shifting costs incurred by Medicare beneficiaries to Medicare (and by extension, taxpayers). However, the budgetary effects of adding a hard cap on out-of-pocket drug spending under Part D have not been estimated by CBO for this proposal alone. All three of the proposals mentioned above with available budget estimates – H.R.3, the Grassley/Wyden proposal, and the Trump Administration’s FY2020 budget proposal – include a hard out-of-pocket cap in addition to other changes to the Part D benefit design that would reallocate liability for catastrophic costs by reducing Medicare’s share of catastrophic costs and increasing the share paid by Part D plans and manufacturers. Therefore, the budgetary effects of these proposals are estimated together.
According to CBO, the Part D benefit redesign proposals in H.R. 3 would increase federal spending by $9.5 billion over 10 years (2020-2029); the benefit redesign proposals in the Grassley/Wyden legislation would decrease federal spending by $3.4 billion over 10 years (2021-2030); and the Administration’s redesign proposals would decrease federal spending by $1.8 billion over 10 years (2020-2029). Higher spending under H.R. 3 is likely due to a substantially lower proposed out-of-pocket cap ($2,000) compared to the Grassley/Wyden legislation ($3,100). The Administration’s proposal did not specify a dollar amount for the cap.
The total on-budget cost of these proposals is offset in part by policies that shift reinsurance costs (i.e., costs above the catastrophic threshold) from the Medicare program to Part D plan sponsors and/or drug manufacturers, which is designed to give Part D plans stronger incentives to lower costs. (For a fuller discussion of these proposals and budgetary effects, see the section “Modify the Medicare Part D Benefit Design” in A Look at Recent Proposals to Control Drug Spending by Medicare and its Beneficiaries).
Expand Eligibility for Financial Assistance with Medicare Part A and B Premiums and Cost Sharing
Under the Medicare Savings Programs, state Medicaid programs help pay for Medicare Part A and B premium and/or cost-sharing assistance for Medicare beneficiaries who have income and assets below specified levels (Tables 2 and 3). Enrollment in the Medicare Savings Programs is open to all Medicare beneficiaries, including those in traditional Medicare and in Medicare Advantage plans. Most low-income Medicare beneficiaries who qualify for Medicare premium and cost-sharing assistance also qualify for full Medicaid benefits such as long-term services and supports7 ; these beneficiaries are referred to as full-benefit dually eligible beneficiaries. (These full-benefit dually eligible beneficiaries are not the subject of the policy approaches discussed below.)
Low-income beneficiaries who receive only financial assistance through the Medicare Savings Programs – meaning they only qualify for payment of Medicare Part A and/or B premiums and, in some cases, Part A and Part B cost sharing but not full Medicaid benefits – are referred to as partial-benefit dually eligible beneficiaries. In 2017, there were about 3.1 partial-benefit dually eligible Medicare beneficiaries receiving financial assistance through the Medicare Savings Programs.8 There are three eligibility categories for this assistance, corresponding to different income and asset levels (Table 2)9 :
Qualified Medicare Beneficiaries (QMB-only) receive assistance with their Medicare Part A and B premiums as well as deductibles and cost-sharing requirements. To qualify, beneficiaries generally must have incomes of no more than 100% FPL ($12,760/individual and $17,240/couple in 2020) and assets no higher than $7,860/individual and $11,800/couple.
Specified Low-Income Medicare Beneficiaries (SLMB-only) receive assistance with their Medicare Part B premiums only. To qualify, beneficiaries generally must have incomes between 101% and 120% FPL ($15,312/individual and $20,688/couple in 2020) and assets no higher than $7,860/individual and $11,800/couple.
Qualifying Individuals (QI) receive assistance with their Medicare Part B premiums only. To qualify, beneficiaries generally must have incomes between 121% and 135% FPL ($17,226/individual and $23,274/couple in 2020) and assets no higher than $7,860/individual and $11,800/couple.
The federal government sets minimum income and asset eligibility requirements for the Medicare Savings Programs, but states can choose to expand eligibility to provide premium and cost-sharing assistance to beneficiaries with higher incomes and/or assets (Table 3). There are six states, as well as the District of Columbia, that have elected to modify income eligibility criteria, either by raising the qualifying federal poverty limits or applying a more generous income disregard (Connecticut, Illinois, Indiana, Maine, Massachusetts, and Mississippi). Nine states and the District of Columbia have elected to eliminate the asset test (Alabama, Arizona, Connecticut, Delaware, Louisiana, Mississippi, New York, Oregon, and Vermont), while three states have elected to have a higher asset limit (Maine, Massachusetts, and Minnesota). Those states with different eligibility requirements use state dollars to provide coverage to lower income beneficiaries who would not otherwise qualify under federal rules.
Because federal rules under the Medicare Savings Programs impose an income and asset test, not all low-income Medicare beneficiaries qualify for financial assistance with Medicare premiums and cost-sharing requirements. Some do not qualify because their income is just above the eligibility threshold, even if they have very little savings or other assets. For example, a widow living on $20,000 with just $5,000 in savings would not qualify for any assistance under these programs. Others with low incomes may not qualify if their savings exceed the maximum allowed ($7,860 for an individual in 2020).
The eligibility requirements for the Medicare Savings Programs are generally stricter than those established under the Affordable Care Act for the Medicaid expansion or Marketplace coverage. For example, under the ACA, non-elderly people who live in states that expanded Medicaid up to 138% are not subject to an asset test to determine eligibility for the Medicaid program. The ACA also provides premium tax credits and cost-sharing reduction (CSR) subsides for qualifying individuals who enroll in a health plan through the marketplace, which are not subject to an asset test. Premium tax credits are available for people with incomes up to 400% FPL, while cost-sharing subsidies are available for people with incomes up to 250% FPL.
To limit the financial burden of health care costs on low-income Medicare beneficiaries, some policymakers have proposed to modify eligibility criteria for both the Medicare Savings Programs and the Part D Low-Income Subsidy program (discussed below). Some of these changes were recently proposed by policymakers in response to the COVID-19 pandemic and included in legislation that passed the House of Representatives in December 2019 (H.R. 3, Elijah E. Cummings Lower Drug Costs Now Act).
This brief explores four approaches to increase financial assistance through the Medicare Savings Programs:
Provide assistance with Medicare Part A and Part B cost-sharing requirements to beneficiaries who currently qualify for Part B premium assistance (but not for assistance with deductibles or cost sharing) through the Medicare Savings Programs (e.g. SLMBs and QI enrollees with incomes up to 135% FPL).
Expand eligibility for the Medicare Savings Programs (either premium assistance only or both premium and cost-sharing assistance) to beneficiaries with incomes up to 150% FPL (up from 135% currently), keeping the current asset limits in place.
Expand eligibility for the Medicare Savings Programs (either premium assistance only or both premium and cost-sharing assistance) to beneficiaries with incomes up to 150% FPL and eliminate the current asset limits.
Expand eligibility for the Medicare Savings Programs (either premium assistance only or both premium and cost-sharing assistance) to beneficiaries with incomes up to 200% FPL and eliminate the current asset limits.
This analysis is based on national estimates and, due to a lack of state-level data, does not adjust for state-level variations in eligibility. This may affect the estimates we present here of the number of people who could benefit as well as the potential impact on Medicare and Medicaid spending. For example, we may overestimate the number of people who could benefit from eliminating the asset limits because nine states and the District of Columbia do not impose asset requirements in determining eligibility for the Medicare Savings Programs. We believe our estimates serve as a reasonable approximation of the magnitude of the potential effect of these policy approaches.
Beneficiary Effects
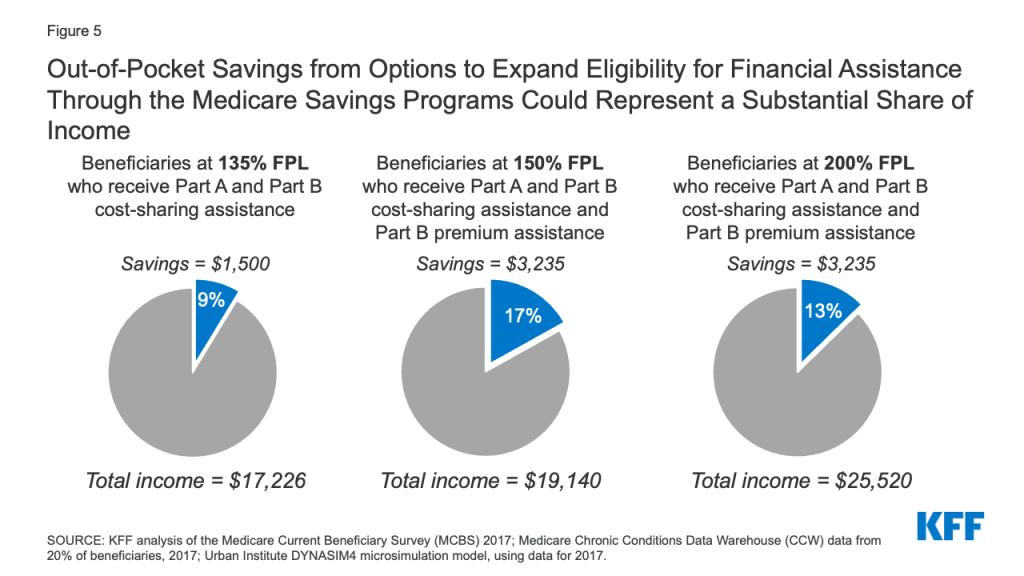
Providing assistance with Medicare cost-sharing requirements to low-income Medicare beneficiaries who are currently eligible for help with Part B premiums only (e.g. SLMBs and QI enrollees with income below 135% of poverty) would help an estimated 1.5 million beneficiaries (Figure 4). This additional financial assistance would generate average per capita out-of-pocket savings of about $1,500 per person in 2020, based on our analysis of Medicare Part A and B liability. This estimate assumes that beneficiaries do not have any other form of supplemental insurance that would cover some or all cost-sharing. In other words, a beneficiary currently eligible for Part B premium assistance only with an income approximating 135% of poverty ($17,226 in 2020), would see savings that represent 9% of annual income (more for beneficiaries with incomes below that level) (Figure 5).
Figure 4: Expanding Financial Assistance through the Medicare Savings Programs Could Help Between 1.5 Million and 12.3 Million Medicare Beneficiaries, Depending on Policy Choices
Expanding eligibility for financial assistance with Medicare premiums and cost-sharing requirements to all low-income Medicare beneficiaries with incomes up to 150% of poverty (up from the current 135% FPL limit), keeping the current asset limits in place, would help an estimated 1.8 million Medicare beneficiaries. This includes 1.5 million beneficiaries currently receiving Part B premium assistance only (as noted above), plus an additional 0.3 million beneficiaries with incomes between 135% and 150% FPL. This estimate is based on the number of beneficiaries at this income level who received partial LIS benefits in 2017, and as such might overstate eligibility somewhat since LIS asset limits are higher than MSP asset limits, but it may also understate how many could potentially qualify because not everyone eligible for LIS currently participates.
Low-income Medicare beneficiaries who were not already receiving financial assistance through the Medicare Savings Programs could see average out-of-pocket savings of approximately $3,235 per person, including $1,735 in Part B premiums, based on the standard monthly Part B premium in 2020, and $1,500 for Part A and B cost sharing in 2020.10 For beneficiaries with incomes between $17,226 and $19,140 (135% to 150% FPL in 2020), this total savings represents between 17% and 19% of their incomes (Figure 5).
Figure 5: Out-of-Pocket Savings from Options to Expand Eligibility for Financial Assistance Through the Medicare Savings Programs Could Represent a Substantial Share of Income
Expanding Medicare Savings Program eligibility to provide premium assistance only, or both premium and cost-sharing assistance to beneficiaries with incomes up to 150% FPL and eliminating the asset limits would help an estimated 6.7 million beneficiaries.11This includes the 1.8 million beneficiaries who would be helped by expanding eligibility for assistance with premiums and cost sharing up to 150% FPL under current asset limits, plus 4.9 million beneficiaries with incomes up to 150% FPL with assets higher than current limits.
Among newly-eligible beneficiaries, policymakers could choose to provide different levels of assistance, such as assistance with both premiums and cost sharing to those with somewhat lower incomes and assistance with premiums only to those with somewhat higher incomes. If beneficiaries qualified for both premium and cost-sharing assistance, estimated out-of-pocket savings would be $3,235 in 2020, similar to the approach described above. If beneficiaries qualified for premium assistance, but not cost-sharing assistance (as is the case today for SLMBs and QIs), estimated out-of-pocket savings on premiums would be $1,735 in 2020.
Expanding Medicare Savings Program eligibility to provide premium assistance only, or both premium and cost-sharing assistance to individuals with incomes up to 200% FPL and eliminating the asset limits would help an estimated 12.3 million beneficiaries.12This includes the 6.7 million individuals with incomes up to 150% FPL (as in the previous approach ) and an additional 5.6 million beneficiaries with incomes between 150% and 200% FPL. As in the previous approach, financial assistance could be provided for premiums only, or both premium and cost-sharing requirements; beneficiaries who qualify for assistance with both premiums and cost sharing could save $3,235 in 2020, while those who newly qualify for premium assistance alone could save $1,735 in 2020.
Among the beneficiaries would be helped under an approach that expanded eligibility for the Medicare Savings Programs up to 200% FPL with no asset test are an estimated 3.9 million beneficiaries in communities of color (31% of the total 12.3 million beneficiaries), including 1.2 million Black beneficiaries, 1.9 million Hispanic beneficiaries, and 0.7 million beneficiaries in other racial and ethnic groups.
Another approach, which we are unable to analyze due to data limitations, would be raising, but not eliminating, the asset test – for example, raising it to $50,000, up from the highest allowable limits currently ($7,860 for individuals/$11,800 for couples). This approach would allow more beneficiaries to qualify for the Medicare Savings Programs, without providing financial assistance to the very small share of Medicare beneficiaries with low incomes but significant savings.
Budget Effects
The budgetary effects of these policy approaches have not been estimated by CBO. While H.R. 3 included a provision to expand financial assistance with Medicare Part A and Part B premiums and cost sharing to beneficiaries with incomes up to 150% FPL (keeping the current asset limits in place), CBO scored this provision together with several other Medicare low-income benefit improvements in H.R. 3, including expanding eligibility for full Part D Low-Income Subsidy benefits to individuals up to 150% FPL (up from 135% FPL), providing automatic eligibility for Medicare premium and cost-sharing subsidies to certain low-income residents of the territories, and providing automatic eligibility for Part D Low-Income Subsides to certain Medicaid beneficiaries. Taken altogether, CBO estimated that these provisions would cost an estimated $49.8 billion over 10 years (2020-2029).
The budget effects of various approaches to expand eligibility for the Medicare Savings Programs would depend in part on design features. Of the approaches discussed above, the most costly of these approaches would be to expand eligibility for both Part A and Part B premium and cost-sharing assistance to beneficiaries with incomes up to 200% FPL with no asset limits. The cost could be scaled back by providing different levels of financial assistance to people at different income levels up to 200% of poverty, or by raising the income and asset test thresholds above current levels, but not to 200% of poverty and by retaining the asset test at a higher level.
These approaches would also have differential effects on federal and state budgets depending on how they were financed, and baseline eligibility criteria in each state. Because the Medicare Savings Programs are currently financed jointly by states and the federal government, any expansion in benefits or eligibility would increase costs for Medicaid if the current financing structure was used to pay for the expansion. However, if costs for Medicare premiums and cost sharing were shifted from Medicaid to Medicare, states would realize savings, shifting the impact to the Medicare program and its beneficiaries (as discussed below).
Eliminating asset tests for the Medicare Savings Program could provide some modest offsetting savings for states if they experience lower administrative expenses due to no longer having to determine beneficiaries’ assets. However, eliminating asset limits could raise the concern that some people with low incomes but significant savings would benefit from the eligibility expansion. Raising the asset limit, but not eliminating it, would maintain the need for states to determine assets, but since fewer beneficiaries would qualify for assistance than if the asset limits were eliminated, retaining the asset test would put less pressure on federal and state budgets and would address potential concerns over beneficiaries with high assets being able to qualify.
Another approach would be to have the federal government pay for the cost of the expansion, and not impose any additional costs on states, following the model of the Part D LIS program, which is fully federally financed. The cost to the federal government would reflect how many people are covered by the expansion, whether the expansion covers premiums alone or premiums and cost sharing, and whether the federal government would also assume the state share of costs for current Medicare Savings Program recipients or just the expansion groups.
If additional costs incurred by the federal government lead to an increase in Part A spending, this could put more pressure on Part A trust fund solvency, which CBO now projects will be depleted in 2024. Likewise, an increase in Medicare Part B spending would lead to higher premiums paid by beneficiaries who do not qualify for the Medicare Savings Program. On the other hand, lower-income beneficiaries who currently purchase Medigap (about 2.1 million beneficiaries) who newly qualify for financial assistance through the Medicare Savings Programs might choose to drop their policies, since the benefits would likely substitute for Medigap, and would therefore save the amount they would have spent on Medigap premiums ($150 per month, on average).
Expand Eligibility for Financial Assistance with Part D Plan Premiums and Cost Sharing
The Part D Low-Income Subsidy (LIS) Program helps beneficiaries with their Part D premiums, deductibles, and cost sharing, providing varying levels of assistance to beneficiaries at different income and asset levels up to 150% FPL, which is higher than the income eligibility threshold for the Medicare Savings Program, as noted above (Table 4). In 2017, 13.7 million Medicare beneficiaries received either full or partial LIS benefits, representing 31% of all Part D enrollees that year.13
Both full-benefit and partial-benefit dual eligible beneficiaries in the Medicare Savings Programs automatically receive full LIS benefits, meaning they pay no Part D premium or deductible and only modest copayments for prescription drugs until they reach the catastrophic threshold, when they face no cost sharing. Individuals who do not automatically qualify for LIS can enroll if they meet certain income and asset requirements set by the federal government, and can receive full or partial LIS benefits depending on their income and assets. Some beneficiaries who receive partial LIS benefits pay no monthly premium while others pay a partial monthly Part D premium (with subsidies of 75%, 50%, or 25% of the monthly premium, depending on their income); all partial LIS recipients also pay an $89 annual deductible, 15% coinsurance up to the out-of-pocket threshold, and modest copayments for drugs above the catastrophic threshold.
As with the Medicare Savings Programs, the asset test for the Part D Low-Income Subsidy program disqualifies many otherwise income-eligible low-income people. Expanding financial assistance with Part D prescription drug plan premiums and cost sharing by lifting the asset test and broadening income eligibility could provide substantial savings to beneficiaries, particularly those who take high-cost drugs.
Below we discuss three policy options to make prescription drug costs more affordable for low-income people on Medicare, with the number of beneficiaries who could be helped and estimated savings under each option:
Provide full LIS benefits for beneficiaries currently receiving only partial LIS benefits.
Eliminate the asset limits for LIS program eligibility, keeping the current income limits.
Expand LIS program eligibility to individuals with incomes up to 200% FPL (up from 150% FPL) and eliminate the asset limits.
Beneficiary Effects
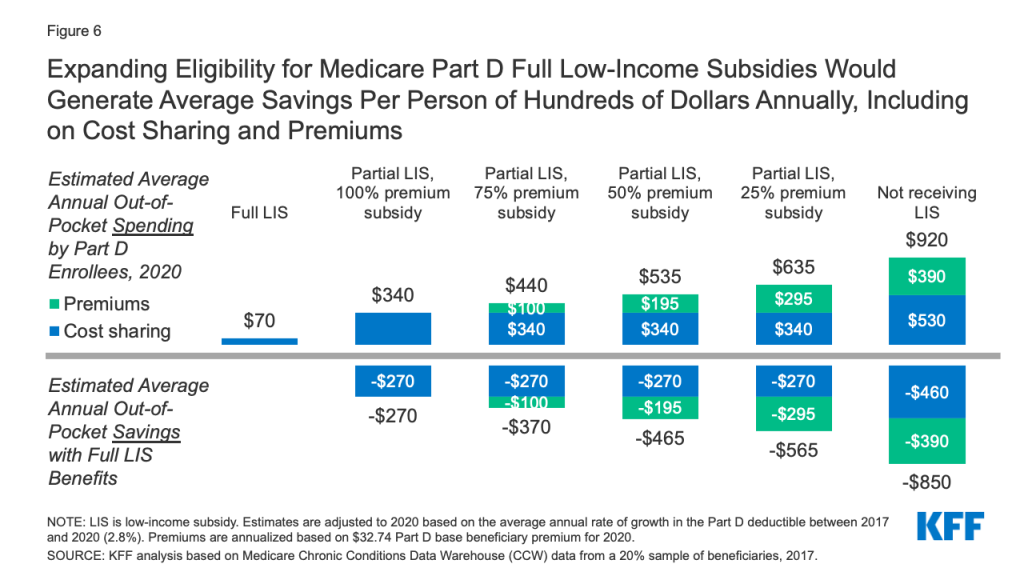
Providing full Medicare Part D LIS benefits to Part D enrollees currently receiving partial LIS benefits would help an estimated 0.4 million beneficiaries, based on 2017 enrollment. This option is similar to a provision that was included in H.R. 3. Estimated average out-of-pocket savings per partial LIS enrollee who receives full LIS benefits would range from approximately $270 to $565 in 2020, depending on the level of premium assistance partial LIS beneficiaries were receiving, as detailed below (Figure 6):
Figure 6: Expanding Eligibility for Medicare Part D Full Low-Income Subsidies Would Generate Average Savings Per Person of Hundreds of Dollars Annually, Including on Cost Sharing and Premiums
Partial LIS enrollees who receive a 25% premium subsidy (the lowest premium subsidy level for partial LIS enrollees) would save approximately $565 on their total out-of-pocket drug costs, including approximately $270 in savings on cost sharing by moving from 15% coinsurance to modest copayments for their prescriptions and no out-of-pocket costs above the catastrophic threshold, plus $295 in annual premium savings.
Partial LIS enrollees who receive a 75% premium subsidy would save $370 on their total out-of-pocket drug costs, including approximately $270 in savings on cost sharing plus $100 in annual premium savings.
Partial LIS enrollees who receive a 50% premium subsidy would save approximately $465 on their total out-of-pocket drug costs, including approximately $270 in savings on cost sharing plus $195 in annual premium savings.
Partial LIS enrollees who pay $0 premium would gain no additional premium subsidy but would save $270 on their out-of-pocket drug costs.
These averages understate the potential cost savings for the smaller share of low-income enrollees with extraordinarily high drug costs, such as partial LIS beneficiaries who take high-cost specialty drugs. This is because for high-cost drugs, with total prices in the thousands of dollars, 15% coinsurance can translate into substantial out-of-pocket costs. For example, partial LIS enrollees taking Humira or Enbrel for rheumatoid arthritis would pay around $1,700 for a year’s worth of these medications in 2020, while full LIS enrollees would pay less than $20 annually. Thus, if partial LIS enrollees received full LIS benefits, they would save just under $1,700 in 2020 on cost sharing for one of these medications alone. Annual savings would be similar for other high-cost specialty drugs, with the majority of savings occurring below the catastrophic threshold where partial LIS enrollees currently pay 15% coinsurance but full LIS enrollees pay low flat copays for brand-name drugs of either $3.90 or $8.95, depending on their income and asset levels.
Eliminating the asset limits for LIS program eligibility while keeping the current income limits would help an estimated 4.0 million low-income Medicare beneficiaries with incomes below 150% of FPL who currently do not qualify for any help under the LIS program because their assets exceed current limits.
Estimated out-of-pocket savings per person gaining LIS coverage would be highest for beneficiaries with no LIS who qualified for full LIS. Average total out-of-pocket Part D spending is around $920 in 2020 for beneficiaries with no LIS (including premiums and cost sharing), compared to only $70 for beneficiaries with full LIS (cost sharing only). Therefore, estimated savings would be approximately $850 for these beneficiaries, including savings of $460 on cost sharing and $390 on annual Part D premiums (Figure 6).
For beneficiaries with no LIS who qualified for partial LIS, estimated out-of-pocket savings would range from approximately $290 to $580 in 2020, depending on the level of premium assistance beneficiaries received: $290 is savings on cost sharing only for beneficiaries who go from no LIS to partial LIS, with the lowest level of premium subsidy (25%), and $580 is savings on both cost sharing and premiums for beneficiaries who go from no LIS to partial LIS, with a full premium subsidy.
Expanding LIS program eligibility to individuals with incomes up to 200% FPL and eliminating the asset limits would help an estimated 9.6 million low-income Medicare beneficiaries who would not otherwise qualify for LIS benefits. This includes 4.0 million beneficiaries with incomes up to 150% who would gain assistance if the asset limits were eliminated, and another estimated 5.6 million beneficiaries with incomes between 150% and 200% FPL. Estimated average savings for these beneficiaries would be the same as described above under the option to eliminate the asset limits for LIS program eligibility.
Budget Effects
The budgetary effects of these options have not been estimated by CBO. As mentioned in the discussion of budgetary effects under the Medicare Savings Programs, increasing financial assistance to the level of full LIS benefits for beneficiaries with incomes up to 150% FPL (up from 135% FPL) was a provision in H.R.3 and was scored with other low-income provisions in the legislation. CBO estimated that these program improvements for Medicare low-income beneficiaries would cost an estimated $49.8 billion over 10 years (2020-2029).
Unlike the Medicare Savings Programs, the LIS program is financed only by the federal government, so any expansion in benefits would be borne by the federal government, and not states. As with the Medicare Savings Programs, the budget effects of options to expand eligibility under the LIS program would depend on the design features, and could be dialed up or down. The most expensive option in terms of federal budget effects would be extending full LIS benefits to individuals with incomes up to 200% FPL without regard to assets, but the cost could be scaled back by providing different levels of financial assistance to individuals at different income thresholds.
In light of affordability challenges facing lower and middle-income people on Medicare, compounded by the increased financial pressure resulting from the coronavirus pandemic, many Medicare beneficiaries could realize significant savings from policy options to decrease their out-of-pocket spending on health care premiums and other medical expenses. While these potential benefit improvements and expansions of eligibility for low-income assistance would ease financial pressures among beneficiaries, these changes would increase costs for the federal government and could increase or decrease costs for states depending on how certain options were financed. At a time when both anxiety about the affordability of medical care and economic insecurity are at a high level, these policy changes could get increased attention from policymakers.
Juliette Cubanski, Meredith Freed, and Tricia Neuman are with KFF. Anthony Damico is an independent consultant.
Tables
Table 1: Comparison of Budgetary Effects of Options to Add an Annual Out-of-Pocket Spending Limit to Medicare, Assuming Full Implementation in 2021
Budget Effects (in billions)
Out-of-pocket spending limit
Limit applies to
Net change in Medicare liability for Part A/B services
Net change in total Medicaid liability
Net change in federal Medicaid liability
Net change in state Medicaid liability
Total Federal Budget Effects in 2021
Total 10-Year Federal Budget Effects (2020-2029)
$5,000
Beneficiary OOP
$6.0
-$0.8
-$0.4
-$0.3
$8.3
$114.1
Beneficiary OOP and Medicaid
$12.5
-$5.9
-$3.4
-$2.5
$15.0
$205.5
All non-Medicare spending
$19.4
-$6.0
-$3.5
-$2.5
$24.6
$332.9
$6,700
Beneficiary OOP
$3.8
-$0.5
-$0.3
-$0.2
$5.4
$74.1
Beneficiary OOP and Medicaid
$9.2
-$4.6
-$2.7
-$1.9
$10.9
$150.3
All non-Medicare spending
$14.7
-$4.8
-$2.8
-$2.0
$18.6
$253.5
Income-related(% of FPL):0-150%: $3,350151-800%: $6,700801-900%: $7,500901-1,000%: $8,5001,001%+: $9,500
Beneficiary OOP
$5.9
-$1.0
-$0.6
-$0.4
$8.2
$118.7
Beneficiary OOP and Medicaid
$13.9
-$7.3
-$4.2
-$3.1
$16.2
$228.0
All non-Medicare spending
$20.0
-$7.5
-$4.3
-$3.1
$24.7
$345.1
NOTE: OOP is out-of-pocket. FPL is federal poverty level.SOURCE: KFF summary of Medicare benefit modeling data from Actuarial Research Corporation.
Table 2: Eligibility for Medicare Savings Programs in 2020
Beneficiary Group
Level of Medicaid Benefits
FPL Threshold
Monthly Income Limit
Asset Limit
Benefits
Individual/ Married
Individual/ Married
Part A Premiums
Part B Premiums
Part A & B Cost sharing
Qualified Medicare Beneficiary (QMB)
QMB-plus
Full
≤100%
$1,084/$1,457
$2,000/$3,000
√
√
√
QMB-only
Partial
≤100%
$1,084/$1,457
$7,860/$11,800
√
√
√
Specified Low-Income Medicare Beneficiary (SLMB)
SLMB-plus
Full
101-120%
$1,296/$1,744
$2,000/$3,000
√
√
SLMB-only
Partial
101-120%
$1,296/$1,744
$7,860/$11,800
√
Qualifying Individual (QI)
QI
Partial
121-135%
$1,456/$1,960
$7,860/$11,800
√
Qualified Disabled and Working Individuals (QDWI)
QDWI
Partial
≤200% FPL*
$4,339/$5,833
$4,000/$6,000
√
NOTE: FPL is federal poverty level. Alaska and Hawaii have higher income eligibility limits. Income limits include $20 monthly income disregard. Resource limits do not include $1,500 for burial expenses. *QDWI income thresholds are based on 200% of FPL and do not count half of income earned from work. Full-benefit dually eligible beneficiaries qualify for full Medicaid benefits and receive financial assistance through the Medicare Savings Programs. Partial-benefit dually eligible beneficiaries receive only financial assistance through the Medicare Savings Programs, but do not receive full Medicaid benefits.SOURCE: KFF summary of information from National Council on Aging, “Medicare Savings Programs Eligibility and Coverage Chart, 2020,” updated March 2020; Medicaid and CHIP Payment and Access Commission, “Report to Congress on Medicaid and CHIP, Chapter 3: Improving Participation in the Medicare Savings Programs,” June 2020.
Table 3: Eligibility for Medicare Savings Programs (MSPs) in States with Different Income and/or Asset Limits than Federal Limits in 2020
State
Monthly Income Limit
Asset Limit
QMB
SLMB
QI
United States
$1,084/ $1,457
$1,296/ $1,744
$1,456/ $1,960
$7,860/ $11,800
Alabama
Same as federal
No limit
Arizona
Same as federal
No limit
Connecticut
$2,245 / $3,032
$2,458 / $3,319
$2,617 / $3,535
No limit
Delaware
Same as federal
No limit
DC*
$3,190/ $4,310
N/A*
N/A*
No limit
Illinois
Same as federal plus $25 disregard
Same as federal
Indiana
$1,615 / $2,175
$1,827 / $2,463
$1,987 / $2,678
Same as federal
Louisiana
Same as federal
No limit
Maine
$1,670 / $2,255
$1,882 / $2,543
$2,043 / $2,758
$58,000 / $87,000
Massachusetts
$1,402 / $1,888
$1,615 / $2,176
$1,774 / $2,391
$15,720 / $23,600
Minnesota
Same as federal
$10,000 / $18,000
Mississippi
Same as federal plus $50 disregard
No limit
New York
Same as federal
No limit
Oregon
Same as federal
No limit
Vermont
Same as federal
No limit
NOTE: QMB is Qualified Medicare Beneficiary. SLMB is Specified Low-Income Medicare Beneficiary. QI is Qualifying Individual. Monthly income includes $20 monthly income disregard, except in those states that have higher income disregards or no disregard: CT includes no standard disregard; ME increased income disregard to $75 for single and $100 for couples. Maine’s asset limits apply to liquid assets only. *QMB is the sole program in DC.SOURCE: KFF summary of information from National Council on Aging, “Medicare Savings Programs Eligibility and Coverage Chart, 2020,” updated March 2020; Medicaid and CHIP Payment and Access Commission, “Report to Congress on Medicaid and CHIP, Chapter 3: Improving Participation in the Medicare Savings Programs,” June 2020.
Table 4: Eligibility for Part D Low-Income Subsidy (LIS) Program in 2020
Beneficiary Group
Monthly Income Limit
Asset Limit
Premium
Cost Sharing
Individual/ Married
Individual/ Married
Deductible
Initial Coverage
Catastrophic
Full Low-Income Subsidy
Full-benefit duals
income ≤100% FPL
State Medicaid/ MSP
State Medicaid/ MSP
$0
$0
$1.30 generic; $3.90 brand
$0
income >100% FPL
State Medicaid/ MSP
State Medicaid/ MSP
$0
$0
$3.60 generic; $8.95 brand
$0
Non-full-benefit duals (QMB-only, SLMB-only, QI) OR non-duals
income ≤135% FPL & lower asset levels
$1,456/ $1,960
$7,860/ $11,800
$0
$0
$3.60 generic; $8.95 brand
$0
Partial Low-Income Subsidy
Non-duals
income ≤135% FPL & higher asset levels
$1,456/ $1,960
$7,860 to $13,110/ $11,800 to $26,160
$0
$89
15% coinsurance
$3.60 generic; $8.95 brand
income between 135%-150% FPL
$1,615/ $2,175
$13,110/ $26,160
Scaled
$89
15% coinsurance
$3.60 generic; $8.95 brand
NOTE: FPL is federal poverty level. Alaska and Hawaii have higher income eligibility limits. Income limits include $20 monthly income disregard. Resource limits do not include $1,500 for burial expenses.SOURCE: KFF summary of information from National Council on Aging; “Part D LIS/Extra Help Eligibility and Coverage Chart, 2020” updated January 2020; Centers for Medicare & Medicaid Services, “Letter to All Part D Plan Sponsors: 2020 Resource and Cost-Sharing Limits for Low-income Subsidy (LIS),” November 1, 2019.
Methodology
Data and Methods for Adding an Out-of-Pocket Limit to Traditional Medicare
To analyze the effects of an out-of-pocket limit, KFF collaborated with Actuarial Research Corporation (ARC) to develop a model to assess the spending effects for Medicare, beneficiaries, and other payers of options to add an annual out-of-pocket limit to Medicare, assuming full implementation in 2020. The model is primarily based on individual-level data from the Centers for Medicare & Medicaid Services (CMS) Medicare Current Beneficiary Survey (MCBS), which are calibrated to match aggregate Congressional Budget Office (CBO) Medicare spending and enrollment estimates and projections.
We first developed a current-law baseline for 2020 by identifying Medicare reimbursements for each individual in traditional Medicare (excluding beneficiaries enrolled in Medicare Advantage plans), inferring the individual’s cost-sharing obligations under current law, and dividing those obligations between the individual and their supplemental insurer as appropriate. We calculated Medicare and supplemental plan premiums and added these amounts to beneficiaries’ out-of-pocket costs. Next, we simulated the effects of adding an out-of-pocket limit by modifying cost-sharing obligations based on various limits. We assumed that beneficiaries would use more services with an annual spending limit and that some beneficiaries would switch into or out of traditional Medicare, Medigap, or Medicare Advantage in response to this change.
Although MCBS includes Medicare beneficiaries who are enrolled in Medicare Advantage, we excluded this group when evaluating the individual-level spending effects of adding an out-of-pocket limit because the option modifies traditional Medicare. The model does incorporate indirect effects on aggregate Medicare Advantage spending and enrollment, based on the assumptions that changes in traditional Medicare reimbursement would be reflected in Medicare Advantage payments, and that aggregate Medicare Advantage payments will change to the extent that some beneficiaries switch between traditional Medicare and Medicare Advantage.
Data and Methods for Options to Improve Financial Protections for Low-Income Beneficiaries
For these options, our analysis uses data from the following sources: the CMS Medicare Current Beneficiary Survey 2017 Survey file; a 20% sample of Medicare beneficiaries from the CMS Chronic Conditions Data Warehouse (CCW), 2017; and the Urban Institute’s DYNASIM4 microsimulation model, using data for 2017.
Some people dually eligible for Medicare and Medicaid have incomes and/or assets higher than the MSP and LIS eligibility limits because some states do not have asset tests and/or have higher income limits for their Medicare Savings Programs. States may also allow people with higher incomes and/or assets to qualify for Medicaid through specific pathways, such as the nursing home or medically needy pathways. All Medicare beneficiaries who are dually eligible for Medicaid automatically qualify for Part D LIS benefits, irrespective of their incomes and assets. The total number of people receiving MSP and Part D LIS benefits in 2017 came from the CCW.
We estimated the number of additional people who could be eligible for Medicare Savings Program benefits and Part D LIS benefits if eligibility criteria were changed to allow all people with incomes below 150% of the poverty level (FPL) to be eligible, with no limits on assets. The MCBS provided information about the distribution of income among people receiving Medicare Savings Program and Part D LIS benefits. The data from the DYNASIM model was used to estimate the total number of people with incomes below 150% of the FPL. The estimated number of MSP beneficiaries with incomes below 150% of the FPL was subtracted from the estimated total number of people with incomes below 150% of the FPL to estimate the number of additional people who would be eligible for the MSPs if the income threshold was 150% of the FPL and no asset test was imposed. The same process was used to estimate the number of Part D LIS beneficiaries who would be eligible if the income threshold was 150% of the FPL and no asset test was imposed.
We then estimated the number of additional people who would be eligible for MSPs and LIS if the income threshold was raised from 150% to 200% of the FPL, with no restrictions on assets. The MCBS was used to estimate the number of MSP beneficiaries who have incomes between 150% and 200% of the FPL. That estimate was then subtracted from the total number of people with incomes between 150% and 200% of the FPL, with the latter estimate coming from the DYNASIM model, to produce an estimate of the number of additional people who would be eligible for MSP and LIS if the income threshold was raised from 150% to 200% of the FPL, with no asset test.
The resulting estimates overstate the number of people who would be newly eligible for the MSPs and LIS under the expanded eligibility criteria because the estimates do not account for the Medicare beneficiaries who are eligible for these programs under existing income and asset limits but are not enrolled.
To estimate average savings that beneficiaries might achieve through expansions in eligibility for the Medicare Savings Programs, we estimated average annual Medicare Part A and B liability for individuals not receiving cost-sharing assistance through the MSPs using the 2017 CCW. Liability was based on beneficiaries in traditional fee-for-service who do not have Medicaid and represents the amount of cost sharing that beneficiaries would incur if they do not have any form of supplemental coverage. We inflated the 2017 average amount to a 2020 value using the average of the values for the average annual rate of growth in the Part A deductible between 2017 and 2020 (2.3%) and the average annual rate of growth in the Part B premium between 2017 to 2020 (2.6%); averaging these two values gave us a growth rate of 2.4%. This method assumes no change in utilization between 2017 and 2020. Savings on Part B premium is calculated based on the 12 months of the standard Part B premium for 2020.
A similar process was used to calculate how much individuals would save if they received cost-sharing assistance through the LIS program. We calculated average annual cost sharing on prescription drugs for non-LIS, partial LIS, and full LIS enrollees using Part D prescription drug event claims from the 2017 CCW. We inflated average spending on prescription drug cost sharing for these three groups of enrollees using the average annual growth rate in the Part D deductible from 2017 to 2020 (2.8%). We calculated average savings on cost sharing by taking the difference in average spending between various groups (such as the difference between average spending by full LIS enrollees and partial LIS). The calculation of premium savings is based on the Part D base beneficiary premium for 2020 ($32.74 per month); premium savings range depending on the level of premium subsidy received (full LIS enrollees receive a full premium subsidy; partial LIS enrollees receive premiums subsidies ranging from 100% to 25% of the monthly premium; non-LIS enrollees receive no premium subsidy). Estimated out-of-pocket savings for specific drugs is based on 2020 data from the Medicare Plan Finder. Using the plan finder for zip code 20902 in Maryland, we entered specific drugs and retrieved annual cost-sharing information for non-LIS, partial LIS, and full LIS enrollees, using amounts for the lowest-cost plan in the zip code based on prices at Costco, CVS, and Giant pharmacies located within this zip code. As with the overall average cost sharing savings calculation, we calculated savings on cost sharing for specialty drugs by taking the difference in spending on specific drugs across the three enrollee groups (non-LIS, partial LIS, and full LIS enrollees).
Endnotes
The lower bound estimate in both ranges is based on the number of beneficiaries with income below 150% FPL based on KFF analysis of the Centers for Medicare & Medicaid Services (CMS) Medicare Current Beneficiary Survey, 2017; the upper bound estimate is based on the number of beneficiaries with income below 150% FPL based on KFF analysis of Urban Institute DYNASIM4 microsimulation model, 2017. ↩︎
Unpublished estimates of KFF analysis of Urban Institute DYNASIM4 microsimulation model, 2017. Asset data in the DYNASIM4 model corresponded to $12,140 for individuals and $24,250 for couples in 2017, so these estimates slightly overstate the number of people with assets above the allowable limit in 2017 ($12,320 for individuals, $24,600 for couples). ↩︎
KFF analysis of the CMS Medicare Current Beneficiary Survey, 2017; differences are statistically significant. ↩︎
KFF analysis of the CMS Medicare Current Beneficiary Survey, 2017; differences are statistically significant. ↩︎
The savings estimates for the $5,000 and $6,700 limits are similar because of the shape of the out of pocket and Medicaid spend distributions, particularly the portion between the two limits of $5,000 and $6,700. While individuals with eligible spending above $6,700 would have their spending reduced by an additional $1,700 under the lower limit, this additional reduction is roughly offset by individuals with spending between the two limits, who have modest reductions in spending under the lower threshold but are not affected at all by the policy at the higher limit. ↩︎
Full Medicaid benefits generally include services not covered by Medicare, such as inpatient hospital and nursing facility services when Medicare limits on covered days are reached. States may also choose to cover additional benefits, including durable medical equipment, personal care and other home- and community-based services (HCBS), dental care, vision, and hearing services. ↩︎
Another 8.9 million received full Medicaid benefits in addition to financial assistance through the Medicare Savings Programs. KFF analysis of the CMS Chronic Conditions Data Warehouse Medicare data from a 20% sample of beneficiaries, 2017. ↩︎
There is one other category of Medicare Savings Programs: Qualified Disabled and Working Individuals (QDWI); these are individuals who have lost free Medicare Part A benefits because of their return to work but are eligible to purchase Medicare Part A. Through the Medicare Savings Programs, QDWIs receive assistance with their Medicare Part A premiums only. Enrollment in QDWI represents about 325 individuals. ↩︎
We do not include estimates for savings on Part A premiums because about 99% of beneficiaries do not have to pay a Part A premium. ↩︎
This estimate may overstate the number of beneficiaries who could be helped by this expansion since some beneficiaries live in states that have higher income and/or asset limits and are currently eligible but not enrolled in the program. KFF analysis of Urban Institute DYNASIM4 microsimulation model and 2017 Medicare Current Beneficiary Survey. ↩︎
President-elect Joe Biden campaigned on major health reforms, including building on the Affordable Care Act, better managing the COVID-19 pandemic and lowering prescription drug costs, but a narrowly divided Congress could stifle efforts to enact such major legislation. The Biden administration instead may choose to move forward on a variety of policy changes administratively, without Congressional action, to achieve some of the same goals.
A new KFF resource outlines more than 50 potential administrative actions that the Biden administration could take on key health policy issues, many of which would reverse or modify controversial regulations or guidance implemented by the Trump administration that sparked significant legal or partisan pushback. The list of actions is drawn from specific campaign pledges made by President-elect Biden and proposals from prominent Democratic policymakers.
The compilation includes actions involving the federal response to the pandemic; the Affordable Care Act and private health insurance; Medicaid; sexual and reproductive health; mental health and substance abuse; immigration and health; long-term care; HIV/AIDS policy, and LGBTQ health. The list does not include potential policy actions in some areas, such as lowering drug prices and Medicare policies, where there is no clear indication about whether and how the incoming Biden administration would alter Trump administration policies.
The brief notes that the Biden administration may identify other administrative actions it can take in health care, especially if its policy agenda is stymied by Congress.
President-elect Joe Biden campaigned on supporting and building upon the Affordable Care Act (ACA), better managing the coronavirus pandemic and lowering prescription drug costs. However, with the political balance of the Senate uncertain, some Biden proposals, like creating a new public option and lowering the Medicare age to 60, are less likely to be enacted. Even so, as president, Biden could exercise executive branch authority to move forward on a variety of policy changes he has advocated through administrative action without Congress.
The table below includes potential administrative actions under the incoming Biden Administration, based on campaign pledges, and actions that would reverse or modify controversial regulations or guidance issued by the Trump Administration. The table also describes actions Biden could take as president that have received a great deal of attention from other prominent Democrats or are generally consistent with his campaign proposals, and that may therefore be priorities in Biden’s Administration. This table is not an exhaustive list of possible Biden Administration actions and does not include potential administrative actions pertaining to all health policy areas, including Medicare and prescription drug costs, where there is no clear indication of whether or how the Biden Administration would modify Trump Administration policies. If Biden’s health proposals are stymied by a divided Congress, he may look to use administrative actions beyond what’s detailed here to advance his health care agenda.
In this table, we note whether executive actions require regulatory change, as an indication of how much time it may take the Biden Administration to implement these changes. For some regulatory changes, the Biden Administration will need to issue a new Notice of Proposed Rule Making (NPRM) and allow a public comment period before revising the regulation. Rules made through annual payment notices, such as the Notice of Benefit and Payment Parameters (NBPP) may be revised annually.
By contrast, the Biden Administration may more quickly be able to reverse Trump Administration regulations that are proposed but not yet final as well as policies made through sub-regulatory agency guidance or executive order. Some sub-regulatory actions, such as renewing the COVID-19 Public Health Emergency Declaration that is currently set to expire on Inauguration Day, will require attention on Biden’s first day in office. Biden would also likely rescind pending rules that would sunset HHS regulations if not reviewed every 10 years (which could increase administrative burden for the agency and result in regulations with beneficiary protections expiring).
Renew Declaration that COVID-19 is a National Emergency
Renew declaration that COVID-19 is a national emergency, under the National Emergencies Act (NEA). The current emergency declaration is due to expire on February 28, 2021. President Trump proclaimed COVID-19 to be a national emergency under the NEA effective March 1, 2020 and granted the Secretary of Health and Human Services (HHS) authority under Section 1135 of the Social Security Act (SSA) to temporarily waive or modify certain requirements of Medicare, Medicaid, the Children’s Health Insurance Program (CHIP), the Health Insurance Portability and Accountability Act (HIPAA), and other provisions through the duration of a public health emergency declaration (see below). An NEA declaration expires automatically after one year.
Renew Declaration that COVID-19 is a Public Health Emergency
Renew declaration that COVID-19 is a public health emergency (PHE), under Section 319 of the Public Health Service Act. The current emergency declaration is due to expire on January 20, 2021 (Inauguration Day). A PHE declaration allows the Secretary of HHS to take certain actions to respond to the emergency including, if an emergency has also been declared under either the NEA or the Stafford Act, the authority under Section 1135 of the SSA to waive or modify certain Medicare, Medicaid, CHIP and HIPAA requirements. The Secretary of HHS first declared COVID-19 to be a PHE on January 31, 2020 and has renewed it several times since, including most recently on October 23, 2020. A PHE declaration expires automatically after 90 days unless renewed by the Secretary.
Restore U.S. Membership in the World Health Organization
Retract notification of withdrawal of membership in the World Health Organization (WHO). Notification was formally transmitted to the UN Secretary General by the Trump Administration on July 6, 2020 and it becomes effective one-year later on July 6, 2021. Biden has said he would restore the U.S. relationship with WHO
✓
Join COVAX
Announce that the United States will join the COVAX, a multilateral initiative designed to pool resources and guide coronavirus vaccine research, development, procurement, and distribution across countries. The U.S. remains one of the only countries to have not joined.
✓
Restore Directorate for Global Health Security and Biodefense
Restore the National Security Council’s Directorate for Global Health Security and Biodefense. The Directorate, charged with overseeing pandemic response, was first created under the Obama Administration. It was dissolved by the Trump Administration under an NSC reorganization in 2018. Biden has said he would restore the Directorate.
✓
Convene Daily White House COVID-19 briefings
Convene daily White House COVID-19 briefings led by scientists and public health experts to update the public on the status of the pandemic and the federal response. The Trump Administration, which held briefings in the spring, has largely ended them. Biden has said he would immediately establish daily expert-led briefings.
Launch National COVID-19 Vaccine Campaign
Launch a nationwide campaign on COVID-19 vaccines to promote acceptance and counter misinformation. HHS has said it has a campaign, but nothing has been launched, and each state has been asked to prepare its own communications plan.
Establish Pandemic Testing Board
Establish a national system to manage COVID-19 testing capacity issues across the country. Biden has said he would create a Pandemic Testing Board, with members from the public and private sectors, to oversee a nationwide testing campaign which would include surge production of test kits and lab supplies; coordination of distribution across the country; and clear guidance on who needs a test, among other things.
Issue Strong National Social Distancing Guidance to States and Localities
Issue national guidance with strong, clear recommendations for states, localities, and individuals, on social distancing including for schools, and on face mask requirements. Biden has said he would provide clear, consistent, and evidence-based guidance. He has also said he would work with Governors and local authorities to encourage mask mandates. The Trump Administration has given inconsistent and contradictory messaging on social distancing, resulting in significant variation across the country.
Expand Use of the Defense Production Act (DPA)
Expand the use of the DPA to address ongoing nationwide shortages of COVID-19 supplies. Biden has said he would use the DPA to increase production of masks, face shields, and other PPE, and ensure equitable distribution in at-risk communities, particularly those with vulnerable populations.
Establish COVID-19 Racial and Ethnic Disparities Task Force
Establish a COVID-19 Racial and Ethnic Disparities Task Force to address the disproportionate impact of the pandemic on people of color. Biden has said he will create such a Task Force to provide recommendations and oversight on disparities in the public health and economic response, and it will become a permanent Infectious Disease Racial Disparities Task Force after the emergency has ended.
Create National COVID-19 Data Dashboard
Create a national COVID-19 dashboard to provide the public with transparent, clear, and up-to-date data on the pandemic. Biden has said he would create a National Pandemic Dashboard with real-time data.
Review Entry and Detention policies based on public health criteria
Implement policies to reduce COVID-19 risk among individuals in immigration detention facilities and reduce the number of individuals held in detention to mitigate risk of spread. Biden has said he would reduce the number of people in custody by releasing to their families or community-based care organizations those individuals in immigration detention, parents and children, who pose no risk to the community.
Restore the minimum number of navigator programs in each federal Marketplace state to two (reversing Trump Administration reduction to 1)
Restore the requirement for navigators to maintain a physical presence in their service area
Reverse other Trump Administration changes that reduced services provided by navigators
✓
Ensure availability of healthcare.gov and strengthen standards for web brokers and brokers selling marketplace plans
Ensure “no wrong door” enrollment process to help potential enrollees find financial assistance
Maintain access to Healthcare.gov. A recent proposed regulation would allow states to eliminate use of healthcare.gov or state-run marketplace websites and rely entirely on web broker sites, instead.
Strengthen standards for commercial web-broker sites (called enhanced direct enrollment sites, or EDEs) to require the same consumer protections and information of healthcare.gov. The Trump Administration has reduced standards for web brokers, which can also sell short-term plans and other non-ACA-compliant plans. Secret shopper investigations found EDEs that did not correctly screen for Medicaid eligibility and/or that selectively displayed plan information in ways intended to steer consumer choice.
✓
Reverse guidance for Section 1332 state waivers
Restore consumer protection standards under Section 1332 waivers
Revise Trump Administration standards for state waivers under Section 1332 of the ACA that changed federal standards in ways that could result in a decline in coverage or affordability, particularly for key vulnerable populations, including people with low incomes or pre-existing conditions. Recently the Trump Administration proposed to codify these waiver standards in regulation; it remains to be seen whether the proposed regulation will be finalized before January 20, 2021.
✓
✓
Increase Marketplace enrollment by extending open and special enrollment opportunities
Extend open enrollment duration, reversing a 2017 Trump Administration change that shortened the annual open enrollment to 45 days (November 1 – December 15)
Follow lead of state-run marketplaces, nearly all of which established an emergency pandemic special enrollment period (SEP) of at least several months during which individuals could enroll regardless of a qualifying event. CMS has broad authority to authorize emergency SEPs, which it has done in the past following hurricanes and other disasters
The number of SEPs in the federal marketplace fell from 1.6 million in 2015 to 535,000 in 2017 as a result. A recent proposed regulation would require state-run marketplace to adopt similar verification requirements by 2024.
✓
✓
Restore federal marketplace user fees
Reverse the 2018 Trump Administration cuts to user fees on healthcare.gov plans, which help finance a large portion of marketplace operating expenses, including review of plan compliance with ACA rules, navigator assistance, and marketing and outreach, and could be used for more marketing and outreach
A recent proposed regulation would further reduce healthcare.gov user fees (to 2.25% in 2022, vs 3% in 2021 and 3.5% previously) and provide for even lower user fees in states that eliminate use of healthcare.gov
✓
✓
Increase Marketplace subsidies
While Biden could not implement his proposed expansion of ACA subsidies without Congress, he could revise the Trump Administration method for indexing marketplace subsidies that beginning in the 2020 plan year resulted in a modest reduction in marketplace subsidies across the board. As a result of this change, the maximum out-of-pocket limit on cost-sharing in all plans would also increase by 6.4% to $9,100 in 2022.
✓
✓
Suspend enforcement of APTC repayment for tax years during the pandemic, an administrative option similar to House Democrats’ proposal to substantially relax the APTC repayment caps as part of COVID-19 relief. Both the Trump and Obama Administrations used executive authority to temporarily suspend enforcement of other ACA tax provisions, including the employer mandate penalty (Obama) and individual mandate penalty (Trump)
Revise Trump Administration standards for short-term policies that expanded the period of enrollment to nearly three years, for example by limiting future enrollment or reducing opportunities for renewal. These plans typically will not cover individuals with pre-existing conditions, like HIV or pregnancy.
Strengthen standards for short-term policies to limit their sale and/or apply stronger consumer protections.
✓
✓
Reverse association health plan regulation
Revise Trump Administration standards for association health plans (AHPs), which allowed certain AHPs to be considered single employer plans (and so exempt from rules applying to individual and small employer group coverage)
Restore prior regulations that “looked behind” association health plans to determine characteristics of AHP enrollees and require otherwise applicable ACA market standards to apply to AHP coverage for small employers and for individuals
✓
✓
Strengthen Essential Health Benefits
End flexibility for health plans to substitute benefits within and across EHB categories
Revise 2018 Trump Administration rules for Essential Health Benefits that gave insurers flexibility to substitute benefits within and across EHB categories
Revise Section 1115 state demonstration waiver policy to focus on increasing and expanding coverage
Rescind CMS guidance that invites state waivers to condition Medicaid eligibility on work requirements and to elect capped financing
Revise Section 1115 waiver approval criteria to again include the impact on increasing coverage
Stop defending waiver approvals involving work requirements and other restrictive provisions in lawsuits in AR, NH, IN, and MI
Reject pending work requirement waivers in AL, ID, MS, MT, OK, SD, and TN
Reject pending waiver seeking modified block grant financing, closed prescription drug formulary, and other restrictions in TN
Reject pending waivers in SC and TN that would exclude providers like Planned Parenthood from offering Medicaid family planning services because they also offer abortion services outside of Medicaid
Approve pending waivers to extend postpartum coverage period beyond 60 days in IL, IN, MO, and NJ
Review provisions in currently approved waivers and waiver renewal requests to determine whether authorities are not promoting program objectives and should be withdrawn, such as work requirements and restriction on free choice of provider for family planning services
✓
Ensure eligible people can enroll in and maintain Medicaid coverage
final Medicaid managed care rule that relaxes network adequacy, quality oversight, and beneficiary protections
interim final Medicaid COVID-19 maintenance of effort rule that allows states to make certain changes to eligibility and benefits while receiving temporary enhanced federal matching funds during the COVID-19 public health emergency
final regulations removing sexual orientation and gender identity as prohibited bases of discrimination in state Medicaid programs, Medicaid managed care, and PACE programs
✓
✓
Maintain Medicaid coverage and beneficiary protections
Rescind pending regulations that would
withdraw HHS agency guidance if not included in a repository (which could increase administrative burden for the agency and result in guidance with beneficiary protections lapsing)
adopt stricter standards for SSI continuing disability reviews (which could limit Medicaid eligibility)
✓
✓
Expand support for states to respond to COVID-19 pandemic
Renew the COVID-19 public health emergency and national emergency declarations to allow states to retain Medicaid emergency authorities tied to these declarations while the pandemic continues
Approve pending COVID-19 waiver requests to use Medicaid funds to help states respond to COVID-19
encouraging states to waive Medicaid prior authorization and revise co-pay requirements
Encourage states to adopt policies to keep people enrolled in Medicaid during the public health emergency
Support Medicaid essential providers by encouraging states to adopt retainer payments similar to Medicare advance payments
Strengthen and expand long-term care services and supports
See Long-Term Care Section for information about policies pertaining to skilled nursing facilities, nursing facilities, and home and community-based services.
Restore Title X Family Planning Program regulations to require pregnancy options counseling to include abortion and allow clinics to provide abortions with non-federal funds
Issue new regulations to replace Trump Administration Title X regulations in order to:
Require Title X family planning sites to provide non-directive pregnancy options counseling that includes abortion and referrals to abortion services upon request
Allow Title X sites to use non-federal funds to provide abortion services
Note: Litigation challenging this regulation is ongoing, and the parties have petitioned for Supreme Court review.
✓
✓
Prohibit state Title X grantees from banning family planning providers that also provide abortions from participating in the program
Issue regulations similar to Obama Administration regulations that prohibit states from blocking family planning providers that also provide abortions from participating in Title X
✓
✓
Simplify payment for abortion coverage in Marketplace plans
Revise regulations to replace Trump Administration regulations requiring ACA Marketplace plans to charge enrollees a separate monthly premium for non-Hyde abortion coverage. (The Trump regulations are currently blocked by court orders.)
✓
✓
Revise ACA contraceptive coverage regulations to guarantee coverage for more women
Replace the Trump Administration regulations to narrow the scope of employers who are exempt to assure more women have no cost contraceptive coverage
✓
✓
Restore guidance to affirm the Medicaid “free choice of provider” provision
Issue guidance similar to Obama Administration guidance that reaffirmed the Medicaid “free choice of provider” provision, which allows beneficiaries to receive family planning services from any qualified, participating provider
See Medicaid Section for information about state waivers and the impact on women’s health
✓
Rescind Mexico City Policy
Rescind the “Protecting Life in Global Health Assistance” policy (formerly known as the Mexico City Policy and called the Global Gag Rule by opponents) which had been reinstated and expanded by President Trump. The expanded policy requires foreign non-governmental organizations to certify that they will not “perform or actively promote abortion as a method of family planning,” even with their own funds, as a condition of receiving most U.S. global health assistance.
✓
Affirm reproductive health rights, including abortion, globally
Re-enter the United States into the World Health Organization and exit the anti-abortion Geneva Consensus Declaration
Restore funding to UNFPA; the Trump Administration has invoked the Kemp-Kasten amendment to withhold funding from the agency
✓
Allow NIH funding of research involving fetal tissue
Reverse the Trump Administration policy to require ethics review for any research grant that involves fetal tissue from elective abortions
✓
Restore ACA non-discrimination regulations to protect patients who have had an abortion or are seeking an abortion
Revise regulations to replace Trump Administration 1557 regulations (currently blocked by court orders) that permit providers to discriminate against patients on the basis of termination of pregnancy, and would allow providers to deny care to patients in need of abortion or other health care services that violate a provider’s religious beliefs
See LGTBQ Health section for details on anti-discrimination regulatory provisions
✓
✓
Reverse policies that promote and expand religious conscience protections for medical providers over civil rights
Rescind Trump Administration regulations expanding and consolidating the Office for Civil Rights authority of 25 federal health care conscience laws, allowing a broad range of people, entities, corporations, states, etc. to object to facilitating abortion, sterilization procedures, assisted suicide, advance directives and other medical care. (Regulations have been blocked by court orders and have not been implemented.) The Biden Administration could revert to 2011 regulations implemented by the Obama Administration or promulgate new regulations with greater civil rights protections
Repeal executive order directing federal agencies to expand religious protections, which had potentially laid groundwork for denying care to people who seek abortion care
See LGBTQ section for details on the how the Trump regulations permitted discrimination based on LGBTQ status
✓
✓
Improve health care access for incarcerated women
Condition receipt of federal criminal justice grants on adequate provision of primary care and gynecological care for incarcerated women
Protect and prioritize survivors of sexual assault
Issue new guidance to protect survivors of sexual assault on college campuses to reverse Trump Administration Title IX guidance, which permits colleges to allow alleged perpetrators to cross-examine their accusers and apply a stricter standard of evidence for sexual assault cases than for all other student conduct cases
Establish a national center of excellence for reducing veteran suicide and publish a comprehensive public health approach to addressing suicide in veterans
Standardize VA performance around urgent mental health services and eliminate wait times for veterans with suicidal ideation to ensure immediate treatment
Direct the VA to more ER psychiatric staff and peer specialists and expand crisis line capacity
Implement mental health promotion programs that encourage veterans to seek out help from the VA
✓
Address suicide among LGBTQ youth
Ensure school and community-based suicide prevention programs follow best practices set by the U.S. Department of Education
✓
Increase school-based mental health services
Increase the number of psychologists, counselors, nurses, social workers, and other health professionals in schools
Direct the Secretary of Education to complete a study of mental health needs and services in schools.
Support research to develop more effective teen suicide prevention programs
✓
Enforce Mental Health Parity
Increase access to mental health treatment by enforcing full mental health parity
✓
Fight the Opioid Crisis
Direct the Justice Department to investigate the role of pharmaceutical companies and executives in the opioid crisis, and consider criminal and civil enforcement
Direct public insurance programs (e.g. Medicaid, Medicare, and the VA) to accelerate integration of substance use disorder care into standard health care practice
Remove “undue” regulatory restrictions on the prescribing of medications used to treat substance use
Direct the FDA and FTC to investigate “misleading” advertising of substance use treatment facilities not offering evidence-based services
Direct HHS to develop provider trainings on pain management and require those seeking a DEA license to prescribe pain relievers to undergo training
Ensure a multi-agency approach to stem the flow of illicit drugs from other countries into the United States
Reinstate Deferred Action for Childhood Arrivals (DACA) program and review Temporary Protected Status (TPS) designations
Reinstate the DACA program, reversing Trump administration attempts to terminate and limit the program, which grants permission to certain undocumented youth who came to the U.S. as children to stay in the U.S. and work for temporary renewable periods. Following the June 2020 Supreme Court ruling that the Trump administration’s attempt to terminate the program violated federal law, the administration issued a memorandum that eliminated eligibility for new applicants and reduced the renewal period from two years to one. The memorandum remains subject to ongoing litigation, with recent court rulings finding it unlawful and ordering the Trump administration to fully reinstate the program.
Review TPS designations to prevent people from being returned to countries that are unsafe. The Trump administration ended TPS designations for people from several countries; these terminations have been subject to ongoing litigation.
✓
Reverse policies that limited pathways to lawfully enter the United States
End policies that limited avenues to claim asylum, including the Migrant Protection Protocols, under which families with children are sent to Mexico to await their U.S. asylum cases; direct resources to facilitate processing of asylum applications; and increase government resources to support migrants awaiting assessment of their asylum claims.
Reverse a proclamation suspending entry of immigrants unless they provide proof of health insurance within 30 days of entry or have financial resources to pay for reasonably foreseeable health insurance costs, which the courts have blocked from implementation
✓
Reprioritize enforcement policies to protect immigrant families and children
Reverse policies that separate families at the border, including ending the prosecution of parents for minor immigration violations, and prioritize the reunification of any children still separated from their families
Reverse a 2017 executive order that expanded the scope of individuals targeted for removal and reprioritize enforcement activities to focus on removing threats to national security and public safety, end workplace raids, and prevent enforcement actions in sensitive locations, such as hospitals and schools
✓
Revise policies on immigrant detention for families
Revise Trump administration regulatory changes that expanded the federal government’s ability to detain migrant children with their parents for indefinite periods of time, which has been blocked from implementation by the courts
Reinvest in alternatives to detention and non-profit case management programs and take steps to protect immigrant families, pregnant women, and children
✓
✓
Reverse changes to public charge policies
Revise Trump administration regulatory changes to public charge inadmissibility policies that imposed new barriers to obtaining LPR status or immigrating to the U.S. and newly took into account potential future use of certain health, nutrition, and housing programs, including non-emergency Medicaid for non-pregnant adults, when determining whether to allow entry or adjustment to LPR status. Implementation of the changes to public charge have been subject to ongoing litigation.
Restore mandatory penalties for nursing facility violations of federal requirements when residents were in “immediate jeopardy” but did not suffer harm
Strengthen protections against inappropriate resident discharge
Require Office of Inspector General audit of nursing home cost reports and ownership data
Support nursing homes’ response to COVID-19 pandemic
Ensure effective point-of-care testing and contact tracing is available at every facility and ensure updated public health guidance on testing frequency for residents and staff is followed
Invoke the Defense Production Act to increase production of personal protective equipment and ensure effective distribution to frontline essential workers and at risk populations
Require facilities to conduct regular open sessions with residents and families and allow entry of state long-term care ombudsman while facilities are closed to visitors
Advance policies that strengthen home and community-based services
Identify best practices in self-directed home and community-based services and encourage states to adopt these policies
Fully implement and enforce the Medicaid home and community-based settings rule
ReinstateWhite House Office of National AIDS Policy
Reinstate White House Office of National AIDS Policy (ONAP), left vacant by Trump Administration.
Release a new comprehensive National HIV/AIDS Strategy
Release a new comprehensive National HIV/AIDS Strategy, building on the strategy first implemented under the Obama Administration, which currently runs through 2020 (HHS released a draft strategy in December 2020 under the Trump Administration but it has not been finalized)
Revise regulation implementing Section 1557 of the ACA
Revise regulations to replace Trump Administration 1557 regulations that permit providers to discriminate against patients on the basis of gender identity, sex-stereotyping, and sexual orientation
See Women’s Health section for details on anti-discrimination regulatory provisions related to protections for people who have terminated a pregnancy
See ACA-Other Private Insurance section for details.
✓
✓
Update FDA blood donation policy
Update FDA blood donation policy to ensure it is based on science (not an individual’s identity). The current policy includes a 3 month deferral period for men who have sex with men (recently reduced from 12 months due to the COVID-19 pandemic).
Rescind “Deploy or Get Out” Policy
Rescind Department of Defense (DoD) “deploy or get out” policy requiring service members who have been “non-deployable” for 12 months to be processed for separation from military, reportedly used to discharge members with HIV
✓
Rescind Mexico City Policy
Rescind the “Protecting Life in Global Health Assistance” policy (formerly known as the Mexico City Policy and called the Global Gag Rule by opponents) which had been reinstated and expanded by President Trump. The expanded policy requires foreign non-governmental organizations to certify that they will not “perform or actively promote abortion as a method of family planning,” even with their own funds, as a condition of receiving most U.S. global health assistance, including the President’s Emergency Plan for AIDS Relief (PEPFAR).
Revise regulation implementing Section 1557 of the ACA
Revise Trump Administration 1557 regulations that permit providers to discriminate against patients on the basis of gender identity, sex-stereotyping, and sexual orientation
See Women’s Health section for details on anti-discrimination regulatory provisions related to protections for people who have terminated a pregnancy
✓
✓
Reverse policies that promote and expand religious conscience protections for medical providers over civil rights
Rescind Trump Administration regulations expanding and consolidating the Office for Civil Rights authority of 25 federal health care conscience laws, allowing a broad range of entities to object to providing care or culturally competent care to LGBT individuals. (Regulations have been blocked by court orders and have not been implemented.) The Biden Administration could revert to 2011 regulations implemented by the Obama Administration or promulgate new regulations with greater civil rights protections.
Repeal executive order directing federal agencies to expand religious protections, which had potentially laid groundwork for denying care to LGBTQ individuals, couples, and families
See Women’s Health section for details on the how the Trump regulations permitted discrimination based on people seeking abortion services, and sterilization
✓
✓
Expand data collection related to gender identity and sexual orientation
Ensure collection of data on sexual orientation and gender identity in federal surveys and federally funded programs and address gaps in data collection and research related to LBGTQ+ health
As part of that distribution effort, KHN reports that optometrists and dentists are pushing for authority to immunize patients.
Preventing racial disparities in uptake of a COVID-19 vaccine will be important for helping to mitigate the disproportionate impacts of the virus on people of color. A new brief discusses how current national recommendations and state vaccine allocation plans address racial equity.
Drew Altman wrote about the impact of the coronavirus pandemic on national health spending. “We have never seen a year in which health spending actually goes down. Now the seemingly impossible is happening, but the reason – COVID-19 – makes it both anomalous and more tragic than a cause for celebration,” he said. The column draws from a Peterson-KFF Health System Tracker chart collection summarizing what is known so far about how health costs and utilization have changed during the pandemic.
Here are the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: Total cases worldwide reached 65.2 million this week – with an increase of over 4.2 million new confirmed cases in the past seven days. There were over 73,800 new confirmed deaths worldwide, bringing the total for confirmed deaths past 1.5 million.
U.S. Cases and Deaths: Total confirmed cases in the U.S. passed 12.9 million this week. There was an increase of over 1.2 million confirmed cases between November 26 and December 3. Approximately 12,900 confirmed deaths in the past week brought the total in the United States to 276,300.
Growth in Medicaid MCO Enrollment during the COVID-19 Pandemic (Issue Brief)
Dec. 3 Web Briefing: What Happens Once There Is A Covid-19 Vaccine? Key Challenges To Vaccinating America (Archived Recording)
Addressing Racial Equity in Vaccine Distribution (Issue Brief)
Updated: COVID-19 Coronavirus Tracker – Updated as of December 4 (Interactive)
Updated: State Data and Policy Actions to Address Coronavirus (Interactive)
Ensuring Equitable Distribution Of Coronavirus Vaccines Worth Billions To Developed Nations, Report Shows; Public Trust Vital For Successful Programs, WHO Says (KFF Daily Global Health Policy Report)
With the possibility of a COVID-19 vaccine growing closer, increasing attention is focused on how it may be distributed, a responsibility that will largely fall to state, territorial, and local governments. States remain in varying stages of preparation, although all have submitted initial vaccine distribution plans to the Centers for Disease Control and Prevention (CDC). Recent KFF analysis of these plans identified common themes and concerns across several key areas. However, one overarching issue to consider is how to provide equitable access to a vaccine, particularly for people of color, who are bearing the disproportionate burden of the virus and have faced longstanding disparities in health. National recommendations regarding vaccine distribution have emphasized the importance of ensuring equitable access, particularly for disproportionately affected groups, including people of color.
Preventing racial disparities in uptake of a COVID-19 vaccine will be important for helping to mitigate the disproportionate impacts of the virus for people of color and preventing widening racial health disparities going forward. Moreover, reaching high vaccination rates across individuals and communities will be key for achieving broader population immunity through a vaccine. This brief provides an overview of barriers to vaccination that disproportionately affect people of color and discusses how current national recommendations and state vaccine allocation plans address racial equity.
Barriers to Vaccination
Data for existing vaccinations show people of color are less likely to be vaccinated compared to their White counterparts. For example, analysis shows that flu vaccination rates remain below the target level of 70% across racial and ethnic groups and that less than four in ten Black, Hispanic, and American Indian or Alaska Native adults were vaccinated compared to nearly half of White adults (Figure 1). Additional analyses show that this pattern persists across states and among older adults.
Figure 1: Influenza Vaccination Rates among Adults by Race and Ethnicity, 2018-2019 Season
There are a range of barriers to vaccination that disproportionately affect people of color. These include access-related challenges, such as higher uninsured rates (Figure 2) and other barriers to care. Research shows that people who are uninsured have worse access to care than people who are uninsured, and many go without needed care due to cost. Although the government has indicated that the COVID-19 vaccine will be made available at no cost, it will be important for people to know how they can access it for free in order to reduce potential cost concerns as a barrier, particularly for people who are uninsured.
Figure 2: Uninsured Rate Among the Nonelderly Population by Race/Ethnicity
Historic and ongoing racism and discrimination also create barriers to vaccination among people of color. A recent KFF/The Undefeated survey found that Black adults are less likely than other groups to say they would get a coronavirus vaccine if it was free and determined safe by scientists, with most citing safety concerns or distrust of the health care system as reasons why they would not get the vaccine. These findings likely reflect the medical system’s historic abuse and mistreatment of people of color, particularly Black Americans, as well as ongoing experiences with racism and discrimination in health care today. For example, the survey showed that seven in ten Black adults believe race-based discrimination in health care happens very or somewhat often, and Black adults were more likely than White adults to report certain negative experience with health care providers, including feeling that a provider didn’t believe they were telling the truth, being refused a test or treatment they thought they needed, and being refused pain medication (Figure 3).
Figure 3: Share of Adults Reporting Certain Negative Health Care Experiences by Race/Ethnicity
National Recommendations and State Distribution Plans
National recommendations emphasize the importance of equitable allocation of a COVID-19 vaccine for mitigating health disparities and prioritize some groups for initial access to a vaccine. The National Academies of Medicine (NAM) issued a framework for equitable allocation of a coronavirus vaccine, which identified mitigating health inequities as an underlying ethical principle. It recommended prioritizing allocation to areas identified as vulnerable through the CDC’s Social Vulnerability Index (SVI), which determines an area’s social vulnerability based on 15 social factors, including racial/ethnic distribution. The Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices (ACIP) will make final recommendations for vaccine allocation. Its ethical principles for developing recommendations include promoting justice and mitigating health inequities. ACIP has proposed prioritizing certain groups to receive initial access to the vaccine, including health care workers, long-term care facility residents, other essential workers, and older adults and adults with high-risk medical conditions. On December 1, 2020, ACIP recommended that vaccination, once authorized or approved by the FDA, initially be offered to health care workers and residents of long-term care facilities; additional recommendations are expected to follow. In contrast to the NAM and ACIP allocation approaches, HHS announced that initial allocations of the vaccine will be made to states based on their total number of adults and that states could make their own prioritization decisions within the amount allocated to them.
Prioritization of certain groups may help address disparities, but it will also be important to address equitable allocation within priority groups. Prioritization of certain groups may help to address racial disparities since people of color are disproportionately likely to be essential workers and to have high-risk underlying health conditions. However, ensuring equitable access within priority groups also will be important since racial disparities persist within them. For example, analysis shows that people of color account for the majority of COVID-19 cases and/or deaths known among health care workers, and nursing homes with relatively high shares of Black and Hispanic residents were more likely to report COVID-19 cases and deaths.
Recent KFF analysis of state vaccine distribution plans found that states vary in the in the extent to which they focus on racial equity. Just over half of the states with publicly available plans (25 of 47, or 53%) have at least one mention of incorporating racial equity into their considerations for targeting of priority populations. Some states expect to explicitly prioritize people of color, while others report using broader measures, such as the SVI (as recommended by the NAM) and/or a health equity team or framework to guide prioritization decisions. Only a subset (12 of 47, or 26%) of plans specifically mention or consider efforts to include providers that will be needed to reach diverse populations. About half of plans (23 of 47, or 49%) mention targeted efforts to reach diverse communities or underserved populations as part of their communications plans. Some states have made equity a primary guiding principle and central focus of their vaccine distribution plans. For example, states like Maine, California, Louisiana, Oregon, and Washington are embedding workgroups, task forces, or teams focused on health equity into the organizational structures designing and leading distribution plans. These states have also articulated plans to directly engage communities into their planning processes and to develop tailored communication materials that are linguistically and culturally appropriate for different populations. Prioritizing racial equity in vaccination efforts may help reduce disparities in vaccination uptake and the burden of the virus on people of color, but some have suggested that there are potential legal and ethical questions associated with any allocation plan that explicitly uses race as a criterion.
As distribution plans continue to develop, addressing access challenges and conducting effective outreach and communication can help reduce barriers to vaccination among people of color. Making the vaccine available in places and that can be easily accessed through multiple modes (e.g., car or walk-up) during hours that accommodate different work schedules and ensuring people know how to obtain the vaccine at no cost may reduce access-related barriers, particularly for people who are uninsured and may not have an established relationship with a health care provider. Moreover, prior experience with outreach and communications efforts to enroll people in coverage under the Affordable Care Act (ACA) illustrated that utilizing trusted messengers who have shared backgrounds and experiences with the people they are trying to reach and utilizing linguistically and culturally appropriate materials can be effective methods to reach diverse populations. The data and research also suggest that it will be important for providers, officials, and institutions to proactively work to earn trust with individuals and communities and directly address safety and other concerns, recognizing historic and ongoing racism and discrimination within the health care system and that some people may not want to be prioritized to receive the vaccine when it initially becomes available.
Conclusion
In sum, plans to roll out a vaccination once one becomes available are still under development and will likely continue to evolve over time. As these plans develop, it will be important to consider their implications for equitable access to the vaccine, particularly for people of color. Reducing access-related challenges and utilizing targeted and culturally appropriate and respectful outreach and communications may help reduce barriers to vaccination for people of color. Providing equitable access to a vaccine will be important for reducing the disproportionate effects of the virus for people of color, preventing widening health disparities going forward, and achieving population immunity through a vaccine.
A new KFF survey of obstetrician-gynecologists (OBGYNs) offers insight into how the coronavirus pandemic has affected the provision of sexual and reproductive health care, including the growth of telehealth and the ongoing challenges and limitations of such medical visits.
Key findings from the survey, which was conducted from July to September 2020, include:
The majority of OBGYNs worry that patients who have experienced delays in sexual and reproductive health care will face negative health consequences as a result and most also say it has been more difficult to provide reproductive health care during the COVID-19 pandemic.
While few OBGYNs reported using telehealth visits prior to the pandemic, the vast majority had incorporated them by the summer. Almost all reported some type of challenge associated with telehealth visits.
Almost all OBGYNs reported continuing in-person contraceptive services, but half are prescribing hormonal contraceptive pills via telehealth.
The majority of OBGYNs reported that their practice had experienced at least one financial or staffing challenge; more than half reported a decline in patients seeking care.
OBGYNs have continued to provide sexual and reproductive health care during the COVID-19 pandemic, but they have been faced with great challenges and change within their practices. More than half of OBGYNs saw a decline in patient visits from March to June 2020. Most attributed the decline to fewer patients seeking care or practice specific limitations, rather than state restrictions on health care services.
Few OBGYNs reported using telehealth visits prior to the pandemic, but the vast majority said they had incorporated telehealth into their practice as of June 2020. Almost all reported some sort of challenge related to delivering care via telehealth, including limitations in conducting a physical exam, patients having difficulty using telehealth, and the inability to conduct diagnostic testing. If they were to continue to offer telehealth after the resolution of the COVID-19 emergency, most OBGYNs said they would need to be reimbursed at a comparable rate to that of in-person care.
Four in five OBGYNs said their practice experienced at least one financial or staffing challenge as a result of the COVID-19 pandemic. The most commonly cited experiences were reducing operating hours, reduction in pay for clinicians, and furloughing or laying off non-clinical staff.
Almost all OBGYNs reported they are continuing to provide many contraceptive services in-person during the COVID-19 pandemic. Half reported prescribing hormonal contraceptive pills via telehealth, but very few are utilizing telehealth for sexually transmitted infection (STI) testing, or for providing instruction on self-administered contraceptive injections or intrauterine device (IUD) removal.
The majority of OBGYNs said that it was more difficult to address reproductive preventive care and manage chronic gynecological conditions during the COVID-19 pandemic. About six in ten OBGYNs are very or somewhat worried that patients who face delays in sexual and reproductive health care, such as contraceptive care, STI treatment, or obtaining an abortion, will face negative health consequences.
Introduction
The COVID-19 pandemic has had a profound impact on health care access and delivery. While patients’ other health care needs have generally not declined, providers have been tasked with figuring out how to address these needs while mitigating risk to both patients and staff related to the COVID-19 pandemic. Many providers have altered their practice models dramatically, including the rapid adoption of telehealth and reconfiguring practice workflows. While obstetrician-gynecologists (OBGYNs) do not represent the entirety of sexual and reproductive health (SRH) care providers, their experiences offer us insight into the field at a time of great change and adaptation.
At the time the novel coronavirus had started to spread widely within the U.S., KFF was underway fielding a national survey of OBGYNs to understand SRH care provision across the U.S. Realizing that practice patterns had likely changed due to the pandemic, we took the opportunity after the initial survey release to add a subset of questions related to provision of care during the COVID-19 pandemic. A nationally representative sample of 855 office-based U.S. OBGYNs answered the COVID-19 supplemental questions from July 8, 2020 to September 1, 2020. In this brief, we report on how the COVID-19 pandemic has impacted the provision of SRH care by U.S. OBGYNs.
The margin of sampling error for these questions is +/-6 percentage points at the 95% confidence level. All comparisons noted in this brief are statistically significant (p <0.05). A summary of physician and practice characteristic definitions can be found in the methodology section.
Declines in Visit Volume
At the time of the survey, more than half (54%) of OBGYNs said they had seen a decrease in the number of patient visits since the COVID-19 pandemic started in March 2020. Approximately a third (35%) saw about the same number of patients, while a minority (10%) saw more patients since the beginning of the pandemic (Figure 1). Those who were in small practices, defined as ≤ 3 full-time equivalent (FTE) doctors or advanced practice clinicians, appear to have been hit the hardest, with 73% of OBGYNs at small practices reporting a decrease in patients compared to 46% and 48% of OBGYNs at medium (4-10 FTE) and large practices (>10 FTE). Also, more OBGYNs age 65+ reported seeing declines in patient visits, compared to all younger age groups (80% for age 65+, 59% for age 55-64, 58% for age 45-54, 38% for age <45); this is also the age group that had the largest share of OBGYNs who did not utilize any telehealth in June 2020 (Table 2).
When those who reported a decrease in patient volume were asked to identify the primary driver of the decline, most attributed the decline to fewer patients seeking care (45%) or practice specific limitations (37%). State restrictions on health care services was less commonly (7%) cited as the primary reason for declines in patient volume (Figure 1).
Figure 1: Most OBGYNs Saw Declines in Visits During the COVID-19 Pandemic, Attributed To Fewer Patients Seeking Care
Telehealth Utilization
During the COVID-19 pandemic, the use of telehealth grew rapidly among OBGYNs. Prior to the start of the COVID-19 emergency in the U.S. (March 1, 2020), the vast majority (86%) of OBGYNs said they did not conduct any telehealth visits. By June 2020, however, almost all (84%) reported conducting telehealth visits (Figure 2).
Figure 2: Few OBGYNs Used Telehealth Prior To the COVID-19 Pandemic. Three Months Later the Vast Majority Were Doing So
The average share of overall practice visits that OBGYNs reported conducting via telehealth grew from 1.5% before the COVID-19 emergency to 18% in June 2020. Physicians who had been using telehealth before the pandemic reported using telehealth for a significantly higher share of visits on average in June 2020 compared to those with no prior experience (35% vs. 16%). The average share of total visits conducted via telehealth also differed by physician characteristics, with higher shares of telehealth visits reported among female physicians and those under age 54. There were also differences by practice location, with those practicing in urban locations, the West and Northeast (areas initially hit hardest by the pandemic) and in Medicaid Expansion states reporting a higher share of telehealth visits (Table 1). No differences were identified by practice size.
Table 1: Average share of total visits conducted via telehealth in June 2020, by demographics
Thinking about telehealth visits (e.g. virtual visits conducted via video or phone), what percentage of your practice visits were via telehealth in June 2020?
Average
Overall
18%
Used Telehealth Prior to the COVID-19 Pandemic
Yes
35*
No
16
Gender
Female
20*
Male
14
Age
<45
21
45-54
23*
55-64
11
65+
14
Region
West
26*
Northeast
21*
Midwest
16
South
13
Urbanicity
Urban
19*
Suburban
18
Rural
11
Practice in Medicaid Expansion State
Yes
21*
No
12
* Indicates a statistically significant difference (p<0.05) from reference group in bold
When looking at how often OBGYNs utilized telehealth for patient visits, most did so for a minority of visits in June 2020; few (9%) were using telehealth for >50% of their total visits (Figure 3). Therefore, while the majority of OBGYNs have used some telehealth during the COVID-19 pandemic, most continued to deliver the bulk of their visits via in-person care.
Figure 3: Most OBGYNs Not Using Telehealth Prior To the Pandemic. In June 2020, Most Were Doing So for a Minority of Visits
While there was a major spike in telehealth adoption by June 2020, a small but sizable share of OBGYNs (14%) did not conduct any telehealth visits. A higher share of male OBGYNs compared to female, and older doctors compared to younger doctors reported no telehealth use in June 2020. Additionally, while there has been much discussion about the potential for telehealth to expand access in rural regions where transportation barriers can be a limiting factor in obtaining care, OBGYNs in rural areas were more likely than those in urban and suburban areas to have not adopted telehealth during the pandemic. About 1 in 4 OBGYNs practicing in rural areas, small practices and in states without Medicaid expansion reported no telehealth use (Table 2).
Table 2: Who has not adopted telehealth into their practice during the COVID-19 pandemic?
Share of OBGYNs who reported no telehealth use in June 2020
Overall
14%
Used Telehealth Prior to the COVID-19 Pandemic
Yes
1*
No
16
Gender
Female
9*
Male
23
Age
<45
6*
45-54
9*
55-64
20
65+
28
Practice Size1
Large
9*
Medium
10*
Small
22
Urbanicity
Urban
12*
Suburban
8*
Rural
29
Practice in Medicaid Expansion State
Yes
9*
No
24
Question wording: “Thinking about telehealth visits (e.g. virtual visits conducted via video or phone), what percentage of your practice visits were via telehealth in June 2020?” Those who indicated 0% telehealth visits classified as no telehealth use.*Indicates statistically significant difference (p<0.05) from reference group in bold1Practice size defined by number of full-time equivalent (FTE) doctors and advance practice clinicians: small ≤3 FTE, medium 4-10 FTE and large >10 FTE.
Telehealth Challenges
Among OBGYNs who provided telehealth care in June 2020, nine in ten (90%) experienced a telehealth-related challenge. The most cited challenge was the limitation in conducting physical exams (76%), followed by their patients having trouble using telehealth (63%), the inability to conduct diagnostic testing via telehealth (51%), lack of guidance on telehealth best practices (29%) and lack of training on how to use telehealth effectively (26%). A small minority cited high financial costs associated with establishing a telehealth program as a challenge (6%) (Figure 4).
Figure 4: Nine in Ten OBGYNs Cite Challenges To Delivering Care via Telehealth
For OBGYNs who had not been using telehealth prior to the pandemic, a higher share reported telehealth challenges (93%) compared to those who had used telehealth prior (75%). Those without prior telehealth use more often cited lack of training (29% vs. 5%), lack of guidance on best practices (32% vs. 14%) and limitations in conducting a physical exam (80% vs. 54%) as challenges, compared to those with prior telehealth use (Figure 5).
Figure 5: OBGYNs With Prior Telehealth Experience Cited Fewer Telehealth-Related Challenges Compared To New Users
When thinking about the sustainability of telehealth beyond the COVID-19 emergency in the U.S., reimbursement was an issue cited by many. About half of OBGYNs (52%) reported they would need to be reimbursed at the same rate for telehealth compared to in-person care to continue conducting telehealth visits (Figure 6). About one in four (28%) said they would need to be reimbursed at 75-99% compared to in-person care to continue to offer telehealth. Few (11%) would accept <75% reimbursement for telehealth compared to in-person care, and 7% said they would not offer telehealth at all after the resolution of the COVID-19 emergency. Notably, a larger share of OBGYNs practicing in public clinics said they would not offer telehealth in the future, compared to those in private practice (16% vs. 5%).
Figure 6: Most OBGYNs Expect To Be Reimbursed for Telehealth at a Comparable Rate To In-Person Care
Financial and Staffing Challenges
Four in five (81%) OBGYNs said their practice experienced at least one financial or staffing challenge as a result of the COVID-19 pandemic. The most commonly cited experiences were reducing operating hours (56%), reducing pay for clinicians (39%) and furloughing or laying off non-clinical staff (37%). Fewer reduced pay for non-clinical staff (17%), furloughed or laid off clinicians (16%) or closed the practice temporarily (13%) (Table 3). Half of OBGYNs reported that their practice experienced more than one of these challenges.
Table 3: Challenges Experienced by OBGYN Practices During the COVID-19 Pandemic
Which of the following, if any, has your practice experienced because of the impact of COVID-19?
Reduced operating hours
56%
Reduced pay for clinicians
39%
Reduced pay for non-clinical staff
17%
Furloughed or laid off clinicians
16%
Furloughed or laid off non-clinical staff
37%
Closed the practice temporarily
13%
Closed the practice permanently
1%
Merged with another practice
3%
At least one of the above
81%
More than one of the above
50%
None of the above
19%
Financial and staffing challenges affected different shares of OBGYNs depending on practice type and setting (Figure 7). Temporarily closing their practices was reported by a higher share of OBGYNs in the Northeast (26%) compared to the West (10%), Midwest (9%) and South (10%); this was also the case for OBGYNs in small practices (22%) compared to those in medium (11%) and large practices (6%). Reducing operating hours was more common among OBGYNs in urban (59%) and suburban (71%) practices compared to those in rural practices (41%), as well as OBGYNs working in private practice (60%) compared to public clinics (37%). Additionally, a higher share of OBGYNs in private practice than public reported reduced pay for clinicians (42% vs. 22%).
Figure 7: Higher Shares of Certain OBGYNs Reported Modifying Practice Operations During the COVID-19 Pandemic
Delivery of Reproductive Health Care
mode of Delivery
Despite the rapid growth in telemedicine visits, the vast majority of OBGYNs continued to provide basic contraceptive services and STI testing during the COVID-19 pandemic via in-person care. This includes LARC placement (92%), IUD removal (95%), contraceptive injections (93%), prescription of hormonal contraceptive pills (75%) and STI testing for symptomatic patients (94%) (Table 4).
Table 4: Most OBGYNs Continued to Provide SRH Services In Person During July-August 2020
Indicate if, and how, you are currently providing the following services during the COVID-19 emergency?
Providing in-person
Providing via telehealth
Not currently providing this service
LARC placement
92%
n/a
5%
IUD removal
95%
2%a
2%
Contraceptive injections
93%
3%b
3%
Prescription of hormonal contraceptive pills
75%
51%
<1%
STI testing for symptomatic patients
94%
9%
1%
Notes: Respondents could select multiple response options.a Instructing patients on IUD self-removal; b Instructing patients on SQ self-injection
Some OBGYNs reported utilizing telehealth to deliver these services. Nearly half (51%) of OBGYNs report prescribing OCPs via telehealth since the COVID-19 pandemic began. Younger OBGYNs age <45 (64%) and 45-54 (63%) were about twice as likely to provide OCPs via telehealth than older OBGYNs age 55-64 (34%) and 65+ (28%). Prescribing OCPs via telehealth was also more common among female OBGYNs compared to male (61% vs. 33%), OBGYNs in urban locations compared to rural (55% vs. 35%), and those in large practices compared to small (64% vs. 44%). Providers in the West (67%) reported higher rates of providing OCPs via telehealth compared to those in the Midwest (45%) and South (44%), as well as those in states with Medicaid expansion compared to states without Medicaid expansion (57% vs. 39%) (Table 5).
Table 5: Provision of OCPs via Telehealth Varies by Physician and Practice Characteristics
Share who had prescribed OCPs via telehealth during the COVID-19 pandemic
Overall
51%
Gender
Female
61*
Male
33
Age
<45
64*
45-54
63*
55-64
34
65+
28
Practice Size1
Large
64*
Medium
51
Small
44
Urbanicity
Urban
55*
Suburban
49
Rural
35
Region
West
67*
Northeast
52
Midwest
45
South
44
Practice in Medicaid Expansion State
Yes
57*
No
39
Question wording: “Please indicate if, and how, you are currently providing prescription of hormonal contraceptive pills during the COVID-19 emergency.” Table represents those who are providing this service via telehealth.*Indicates statistically significant difference (p<0.05) from reference group in bold1Practice size defined by number of full-time equivalent (FTE) doctors and advance practice clinicians: small ≤3 FTE, medium 4-10 FTE and large >10 FTE.
Despite innovations in telehealth for use in STI care and contraception, very few OBGYNs reported utilizing telehealth for STI testing (9%), or for providing instruction on self-administered contraceptive injections (3%) or IUD removal (2%) (Table 4). Providers who were using telehealth for >25% of their patient visits in June 2020 reported higher use of telehealth for STI testing (20% vs. 6%), contraceptive injections (8% vs. 1%) and OCP prescription (63% vs. 48%) than providers using telehealth for ≤25% of their visits.
Very few OBGYNs reported that they were not providing the aforementioned services at all at the time this survey was fielded (July 8 to September 1, 2020). In the Northeast (14%), the region hit particularly hard early on in the COVID-19 pandemic, a higher share of doctors reported they were not providing LARC placement at the time of the survey compared to those in the West (4%), Midwest (2%) and South (3%). Similarly, a somewhat higher share of OBGYNs in the Northeast were not providing contraceptive injections (8%) compared to the Midwest (1%) and South (1%) [no statistically significant difference was found from the West (3%)]. It is possible that practices have resumed provision of these services since the fielding of this survey.
Access and Delays in Care
The majority of OBGYNs said it was more difficult to address their patients’ needs during the COVID-19 pandemic; this was true for both reproductive preventive care needs (71%), like STI and cervical cancer screening, as well as chronic gynecological conditions (77%), like addressing fibroids, endometriosis and menopausal symptoms (Figure 8).
Figure 8: Majority of OBGYNs Say COVID-19 Has Made It More Difficult To Address Patients’ Needs
Most OBGYNs expressed concern that patients who experience delays in SRH care as a result of the COVID-19 emergency will face negative health consequences. At least six in ten OBGYNs reported being very or somewhat worried about delays in contraceptive care, prenatal care, follow-up care for abnormal pap smears, STI treatment, and obtaining an abortion (Figure 9).
Figure 9: Most OBGYNs Very or Somewhat Worried About Delays in Reproductive Health Care Due To COVID-19
Negative health consequences due to delays in obtaining an abortion were of particular concern to certain groups of OBGYNs. A higher share of female compared to male, urban and suburban compared to rural, and younger compared to older OBGYNs said they were very or somewhat worried about delays in abortion care. Additionally, a higher share of OBGYNs who provide abortions said they were very or somewhat worried about delays in abortion care, compared to OBGYNs who do not provide abortions (Figure 10).
Figure 10: Worry About Delays in Abortion Care Varies by Physician Characteristics
Conclusions and Implications
Since the onset of the COVID-19 pandemic, OBGYNs across the country have been faced with the challenge of how to provide quality sexual and reproductive health (SRH) care to patients during a public health emergency. Our survey finds that most OBGYNs are continuing to provide SRH services, however not without great adaptation. Almost all have changed the way they deliver care, including quickly adopting telehealth, and most have changed, at least temporarily, the way their practice operates, including reducing operating hours and staffing. This rapid response has likely put stressors on both patients and providers. While we were not able to elicit the patient perspective in this survey, we saw that OBGYNs reported declines in patient volumes, largely attributed to fewer patients seeking care, and that OBGYNs worry about the negative health consequences that may result from delays in care. This suggests that patients are facing heightened barriers to accessing care, and that OBGYNs are facing new challenges to providing that care.
While our study provides a snapshot into how OBGYNs adapted their care provision during the Summer of 2020, we recognize that in a rapidly changing environment much has likely evolved since this survey was fielded, and will continue to evolve in the months to come. As the pandemic surges in much of the country, practices may need to reevaluate how they are providing care. OBGYNs, as well as other health care providers, will need to continue to make decisions about how best to meet the sexual and reproductive health care needs of their patients, at a time when patient need for these services has not diminished.
Methodology
Summary
The 2020 KFF National Physician Survey on Reproductive Health obtained responses from a nationally representative sample of OBGYNs practicing in the United States who provide sexual and reproductive health care to patients in office-based settings. The survey was designed and analyzed by researchers at KFF (the Kaiser Family Foundation). An independent research company, SSRS, carried out the fieldwork and collaborated on questionnaire design, pretesting, sample design, and weighting. KFF paid for all costs associated with the survey. Survey responses were collected via paper and online questionnaires from March 18 and September 1, 2020, from a random sample of 1,210 OBGYNs. All OBGYNs included in the sample were sent an invitation letter encouraging them to participate as well as an incentive, described below. The initial sample release in March 2020 corresponded with the emergence of the COVID-19 pandemic. As such, after the initial sample release, additional questions were added related to how the COVID-19 pandemic impacted providers. Among the 1,210 OBGYNs, 855 OBGYNs completed the additional questions related to COIVD-19. The samples were weighted to match known demographics. Taking into account the design effect, the margin of sampling error for the total sample is +/-4 percentage points at the 95% confidence level. The margin of error for the sample who completed the COVID-19 supplemental section +/-6 percentage points. All statistical significance testing was set at p <0.05.
Sample Design
The sample of OBGYNs was procured from IQVIA via their OneKey Database. The OneKey database integrates provider information from various sources (e.g., IMS Health, SK&A, and Healthcare Data Solutions) and is continually updated through telephone and desktop research. The IQVIA OBGYN population universe is about 46,815 and a sample of 6,288 records were selected for this study. Using the survey questionnaire, the sample was then further screened to include only those who are board certified, spend at least 60% of their time providing direct patient care, and provide sexual and reproductive health care to at least 10% of their patients in an office-based setting.
A two-wave sample release design was used for this study to enable adjustments to the sample release and improve representativeness as a result of non-response. In Wave 1, the sample included an oversample of OBGYNs who work in rural areas, work in a public setting and those that had 25% or more of their patients covered by Medicaid, in order to obtain a reliable sample of these key groups of interest. ZIP code of the office, profit status of the facility and median income of the practice location were used as proxies to target these groups respectively. After the initial sample release, SSRS reviewed the productivity of the sample to model the second release. The number of OBGYNs working in a public setting was lower than anticipated, therefore Wave 2 again included an oversample of OBGYNs in public practice.
Contact Design
In an effort to maximize the survey completion rate, OBGYNs were contacted by multiple modes (mail, email) and offered the opportunity to complete the questionnaire either on paper or online. Those who completed the paper survey mailed back their responses using a prepaid reply envelope. OBGYNs were sent an up-front cash $2 bill incentive as well as an incentive check for $75 in the first two mailings to encourage respondents to complete the survey. Respondents received up to five communications for the main survey, four postal mailings and one email. The Wave 1 release corresponded with the emergence of the COVID-19 pandemic. As such, after the initial sample release, additional questions were added related to how the COVID-19 pandemic impacted providers. Wave 1 completes were recontacted and asked to complete these questions, with up to two additional communications, one postal and one email. The Wave 2 release was sent the main survey as well as the COVID-19 questions to complete.
Contact Schedule for Survey: Fielding from March 18 to September 1, 2020
Response Rate
The response rate for the OBGYNs was 22.1% and was calculated using AAPOR’s RR3 (53% completes by web, 47% by mail).
Weighting
The sample was weighted in stages. The first stage of the weighting was the application of a base weight to account for the disproportionately-stratified samples and response rates across sample strata. In the second stage of weighting, the OBGYN sample was post-stratified to match the IQVIA frame on key variables. In the final stage, self-reported sample demographics were matched to population parameters from the AMA database. Qualified respondents’ weights were then rebalanced to the total complete sample size. Because a selection of questions about COVID-19 were added to the survey after the first wave of sample had been released, a second weight was calculated based on respondents who received the supplement and was used for analyses of those questions.
Analysis
A series of data quality checks were run, including removing duplicate cases (n = 32). We compared survey responses by key physician and practice demographics. Gender, age and race were determined by physician self-report. Practice type was determined by physician self-report; those who indicated they work in private practice or a health maintenance organization were classified as “private,” while those who indicated they work in a community health center, a family planning clinic or a government operated health department were classified as “public.” Practice size was determined by the number of full-time equivalent (FTE) physicians or advance practice clinicians (small ≤ 3, medium 4-10, large >10). Urbanicity and region were determined by the ZIP code of the practice, using U.S. census definitions and breaks.
Demographics of Survey Respondents for the COVID-19 Supplement
Demographics of Survey Respondents for COVID-19 Supplement
Characteristic
Weighted n (%)
Overall OBGYNs
855 (100%)
Gender
Female
552 (65%)
Male
294 (34%)
Age
<45
312 (37%)
45-54
214 (26%)
55-64
174 (21%)
65+
136 (16%)
Race
White
587 (69%)
Black
84 (10%)
Asian
115 (13%)
Other
67 (8%)
Practice type
Public
133 (16%)
Private
704 (82%)
Practice size
Large (>10 FTE)
176 (21%)
Medium (4-10 FTE)
423 (49%)
Small (≤ 3 FTE)
241 (28%)
Urbanicity
Urban
488 (57%)
Suburban
166 (19%)
Rural
136 (16%)
Region
West
199 (23%)
Northeast
168 (20%)
Midwest
178 (21%)
South
305 (36%)
A small percentage of respondents left demographic questions blank or their responses were unspecified, including n= 8 (1%) for gender, 18 (2%) for age, 3 (<1%) for race, 18 (2%) for practice type, 15 (2%) for practice size, 65 (8%) for urbanicity and 5 (1%) for region.
In this Foreign Affairs article, Josh Michaud and Jen Kates lay out the challenges in vaccinating people in low-income countries around the world and review early plans to ensure safe and effective vaccines are made available and delivered to people across the globe.
The legal and policy landscape regarding protections based on sexual orientation and gender identity in health care and other areas has shifted markedly in the last decade. Most recently, on June 15, 2020 in Bostock vs. Clayton County, the Supreme Court of the United States ruled that, under Title VII of the Civil Rights Act of 1964, it is unlawful sex discrimination for an employer (with at least 15 employees) to fire an employee because of their sexual orientation or gender identity. It is likely that this ruling will have implications for employers’ decisions regarding health insurance coverage for employees with same-sex spouses, among other areas of employment.
Using the latest data from our annual Employer Health Benefits Survey (EHBS), we assessed access to employer sponsored health insurance (ESI) coverage for same-sex spouses during the first half of 2020 (prior to the Bostock decision), as well as trends over time; ESI remains the primary way people in the U.S. receive health coverage, either directly or as a spouse or other dependent.1,2 We find that, as of mid-2020, while employer offer of same-sex spousal coverage has increased over time, it remains less common than opposite sex spousal coverage.3 These increases follow two other Supreme Court rulings (United States v Windsor and Obergerfell v Hodges) which guaranteed the right to marriage nationwide and paved the way for wider access to health insurance through the workplace (see Appendix).4
Findings
Firms Offering
In 2020, about three-quarters (74%) of firms offering health insurance coverage to opposite-sex spouses also provided coverage to same-sex spouses, a substantial increase from 43% in 2016 (see Figure 1).5 Of the remaining 26% of firms, 5% reported that they do not offer this benefit (similar to the share in 2018) and 21% reported they had not encountered this as a benefits issue, a finding driven by small employers (those with fewer than 200 workers), who represent the majority of employers overall (97%).6 It is becoming less common for employers to report not encountering this benefits issue.
The likelihood of employers offering both opposite-sex spousal coverage and same-sex spousal coverage increases with firm size (see Figure 2). Among firms offering opposite sex spousal coverage, large firms (those with 200 or more employees) were more likely to offer coverage to same-sex spouses compared to smaller firms (89% vs 73%). Almost nine in ten (89%) large firms with opposite-sex spousal coverage offered such coverage, 9% did not, and 2% reported they had not encountered this benefits issue. Among the largest firms (those with a 1,000 or more workers), 95% offered coverage to same-sex couples. By contrast, just 73% of small employers (3-49 workers) offered coverage to same-sex spouses. Four (4%) percent did not and 23% said they had not encountered it.
Covered Workers
While the majority of firms in the United States are small, the majority of covered workers are employed by large firms (200 or more workers) (see Figure 3).7 In 2020, among employees who worked at firms offering opposite-sex spousal health benefits, 91% also had access to same-sex spousal coverage, up somewhat from 88% in 2018 and 84% in 2016 and 2017 (see Figure 4). Five percent (5%) did not have access to this benefit, and 4% worked at firms who reported they had not encountered this benefits issue.
As with firms offering same-sex spousal coverage, the share of employees with access to this benefit increases with firm size (see Figure 5). Most covered workers (96%) at large firms (those with 200 or more employees) who have access to opposite-sex spousal coverage also have access to same-sex spousal coverage. Just 4% did not, and less than1% worked at firms that reported they had not encountered the issue. Among workers at the largest firms (1,000+ workers), nearly all (98%) had access to same-sex spousal coverage. Those least like to have access were employees at firms with 50-199 workers, 15% of whom did not have same-sex spousal coverage when opposite sex coverage was available.
Workers at small firms offering opposite-sex spousal coverage were less likely to have access to health insurance benefits for same-sex spouses, though a majority did (77%). Nine percent (10%) did not have access to this benefit and another 13% worked at firms that report they have not encountered this issue.
Conclusion
These findings indicate that access to employer coverage for same-sex spouses is increasing in the U.S., though it still is less than access to opposite sex spousal coverage. Coverage varies substantially by employer size, with employees at small firms having less access while those at the largest firms have almost uniform access to this benefit. In some cases, lack of access could be a policy decision, though that appears to be on the decline, with smaller shares of firms saying explicitly that they do not offer same-sex spousal coverage. Moreover, it is likely that the Bostock decision will have further implications for same-sex spousal coverage, with more firms being required to offer this benefit under the sex protections in Title VII. However, Title VII nondiscrimination protections do not apply to the 5% of employees at firms with less than 15 employee. Further, the Bostock court cautioned that employers could potentially secure religious liberty exemptions from extending sex protections to encompass sexual orientation and gender identity and it is yet to be seen how such exemptions interact with Title VII.
Methods
The annual survey was conducted between January and July of 2020 and included 1,765 randomly selected, non-federal public and private firms with three or more employees. In 2020, the response rate among firms which offer health benefits was 22%. The Bostock vs. Clayton County decision was released during the survey fielding period. Fifteen (15%) percent of the covered worker weight and 11% of the employer weight among offering firms was represented by respondents who completed the survey after June 15th. Some firms may have changed their coverage in the month following the Supreme Court decisions. Neither the percent of firms nor the percent of covered workers enrolled at firms who offer same-sex benefits is statistically different before and after June 15. For fuller methods see The Kaiser Family Foundation 2020 Annual Employer Health Benefits Survey available at: www.kff.org/ehbs.
This work was supported in part by the Elton John AIDS Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Appendix
Supreme Court Marriage Cases – Background
Prior to the Windsor and Obergefell decisions, same-sex couples faced limited options for obtaining spousal coverage through an employer and when they did, this benefit was treated differently under federal law from benefits received by heterosexually married couples. While some employers offered domestic partner benefits for same-sex partners8 and a growing number of states began to recognize same-sex marriage9 , in 2012, less than half of all workers with health coverage had access to same-sex health benefits.10 In addition, because the federal government did not recognize same-sex marriages, where such benefits were offered, they were not considered tax exempt which meant that same-sex couples faced higher tax burdens compared to heterosexual counterparts.
In June 2013, in Windsor, the Supreme Court overturned a major portion of the Defense of Marriage Act (DOMA) which had, for federal purposes, defined marriage as between a man and a woman. The Windsor decision required federal recognition of same-sex marriages, even if a couple lived in a state that did not recognize same-sex marriage. As a result, employer-sponsored health benefits provided to legally married same-sex couples were now considered tax exempt.11Windsor, however, did not require states to issue same-sex marriage licenses or recognize those performed elsewhere, leading to a patchwork of recognition across the U.S. and lack of access to legal same-sex marriage for many couples where they lived. In 2015, the Supreme Court’s ruling in Obergefell legalized same-sex marriage nationwide, requiring all states to recognize same-sex marriages and issue marriage licenses to same-sex couples. While neither decision required private employers to offer same-sex spousal coverage if they offered coverage to opposite-sex spouses12 , it was expected that wider access to marriage would lead to greater access to coverage. In fact, one study found that the legalization of same-sex marriage in New York was associated with an increase in employer-sponsored insurance among same-sex couples.13 In addition, an increasing number of states (22 states and DC as of 2019) have protections in place that prohibit employers from discriminating against individuals based on sexual orientation, and presumably would require employers offering opposite-sex spousal coverage to extend that benefit to same-sex spouses.14 Furthermore, employers who refuse to offer same-sex spousal coverage while providing coverage to opposite-sex spouses could face legal challenges. Still, employers are not required to provide same-sex spousal coverage parity to their employees.
Massachusetts became the first state to recognize same-sex marriage in 2003. By June 2013, 12 states and the District of Columbia recognized gay marriage. (See Honan, E. June 26, 2013. “Factbox: List of states that legalized gay marriage.” Reuters. Retrieved from:
http://www.reuters.com/article/us-usa-court-gaymarriage-states-idUSBRE95P07A20130626.) ↩︎
However, the Windsor decision ensures federal employees and contractor employees, have access to same-sex spousal coverage at parity with opposite-sex spousal coverage offerings and the Obergefell ruling means that spousal coverage benefits should be extended to state and municipal employees across the nation to the same degree as their heterosexual counterparts. ↩︎
Gonzales G. “Association of the New York State Marriage Equality Act with Changes in Health Insurance Coverage.” JAMA. 314(7). 2015. ↩︎
Human Rights Campaign. Map of State Laws and Policies- Statewide Employment Laws and Policies. Available at: http://www.hrc.org/state_maps. Accessed 10/15/20. ↩︎