5 Key Facts About Medicaid Coverage for People Living in Rural Areas
 Approximately 66 million people in the United States live in rural areas – about 20% of the population. Individuals living in rural areas may experience unique health care challenges compared to individuals living in urban areas. They report poorer physical and mental health, and have lower incomes and higher rates of poverty than individuals living in urban areas. Additionally, individuals in rural areas may have less access to health care services due, in part, to provider shortages in rural areas, and many rural hospitals have closed or are at risk of closure.
Approximately 66 million people in the United States live in rural areas – about 20% of the population. Individuals living in rural areas may experience unique health care challenges compared to individuals living in urban areas. They report poorer physical and mental health, and have lower incomes and higher rates of poverty than individuals living in urban areas. Additionally, individuals in rural areas may have less access to health care services due, in part, to provider shortages in rural areas, and many rural hospitals have closed or are at risk of closure.
Evidence suggests that Medicaid helps mitigate some of these challenges. Medicaid covers nearly half of all births in rural areas and one-fifth of inpatient discharges in rural hospitals. Studies have shown that the Affordable Care Act (ACA) Medicaid expansion is associated with improved hospital financial performance and lower likelihood of hospital closure, particularly for rural hospitals; significant increases in the number of visits to providers for services such as mammograms and substance use disorders in rural areas; and higher staffing levels in rural community health centers.
The One Big Beautiful Bill passed by the House is projected to reduce federal Medicaid spending by $793 billion over 10 years, based on Congressional Budget Office (CBO) estimates, which could have a significant impact on rural communities and individuals living in rural areas who rely on Medicaid for health care coverage. The Senate finance committee’s draft reconciliation language includes similar provisions as the House, but with potentially more significant funding cuts for hospitals, particularly in states that have adopted the ACA expansion. Polling data show that among both parties, most people living in rural areas say Medicaid is “very important” for people in their local community and that they or a family member has received help from Medicaid at some point. Many are worried about the effects of the federal spending reductions to their communities. Furthermore, researchers estimate that more than 300 rural hospitals might be at risk of closure if the federal Medicaid spending cuts as outlined in the House bill are enacted.
1. Nearly 1 in 4 people in rural areas have Medicaid coverage.
Medicaid is the second largest source of health care coverage in both rural and urban areas. However, Medicaid covers a somewhat higher share of people (including those who have both Medicaid and Medicare coverage) in rural areas compared to urban areas, 24% and 21%, respectively. Employer-sponsored insurance is the largest source of health care coverage in rural and urban areas but covers a lower share of people in rural areas (42%) compared to urban areas (50%). Rates of uninsurance are similar across both rural and urban areas.
States have wide variation in their rates of Medicaid coverage in rural areas and in their shares of Medicaid enrollees who are living in rural areas (Appendix Table 1). In six states, at least half of Medicaid enrollees are living in rural areas – Vermont, Wyoming, South Dakota, Mississippi, Montana and Kentucky (Appendix Table 1).

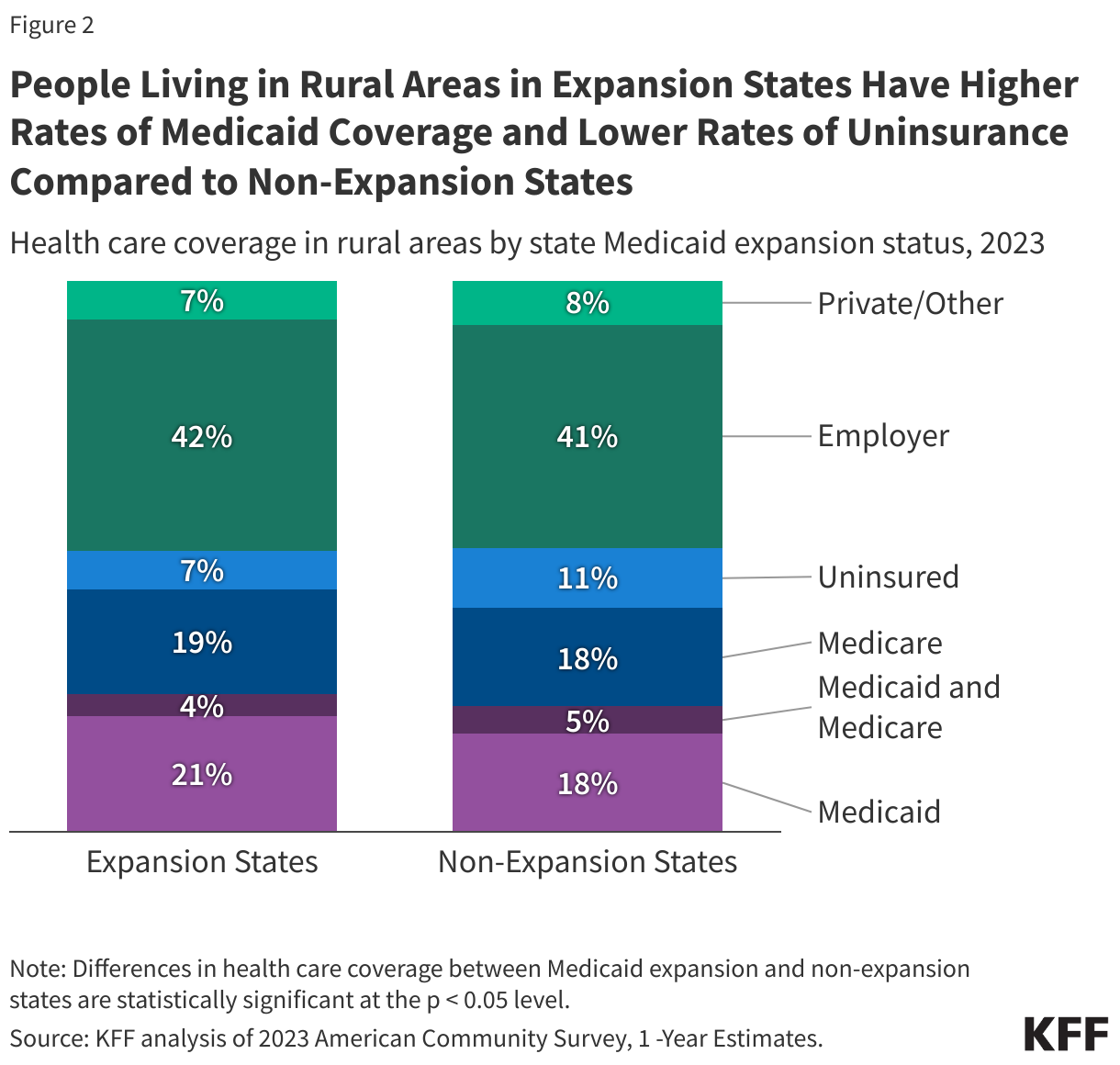
2. People living in rural areas in expansion states have higher rates of Medicaid coverage and lower rates of uninsurance compared to non-expansion states.
States that expanded Medicaid have a somewhat larger share of individuals enrolled in Medicaid (including those dually enrolled in Medicaid and Medicare) in rural areas (25%) than states that did not expand Medicaid (22%). This contributes to a lower uninsured rate in rural areas – in expansion states, 7% of people are uninsured compared to 11% in states that did not expand Medicaid. Expansion and non-expansion states have similar rates of employer-sponsored health insurance coverage in rural areas (42% vs 41%).
Research shows that Medicaid enrollees, in general, have substantially better access to care than people who are uninsured and are less likely to postpone or go without needed care due to cost, as federal rules generally limit out of pocket Medicaid costs. A study focused specifically on rural Medicaid enrollees found that gaining Medicaid coverage significantly increased the likelihood that rural residents felt their health care needs were addressed from when they were uninsured.
3. Children and expansion adults represent over half of rural Medicaid enrollees.
In rural areas, children are the largest Medicaid eligibility group, constituting 36% of enrollees, followed by expansion adults who represent 20% of rural Medicaid enrollees. When looking only at Medicaid enrollees who live in the most rural areas (i.e. rural areas not adjacent to metropolitan areas), the share of expansion adults increases to 24% of enrollees (Appendix Figure 1). In expansion states, the share of rural Medicaid enrollees who are eligible through the ACA expansion jumps to 30% (data not shown), a group that is more at risk of losing Medicaid coverage given the targeting of federal spending reductions to expansion states. A majority (63%) of rural enrollees are White, with smaller shares of Black (12%) and Hispanic (10%) enrollees. This is a notably different demographic make-up compared to urban enrollees, where only one-third of urban enrollees are White (data not shown).

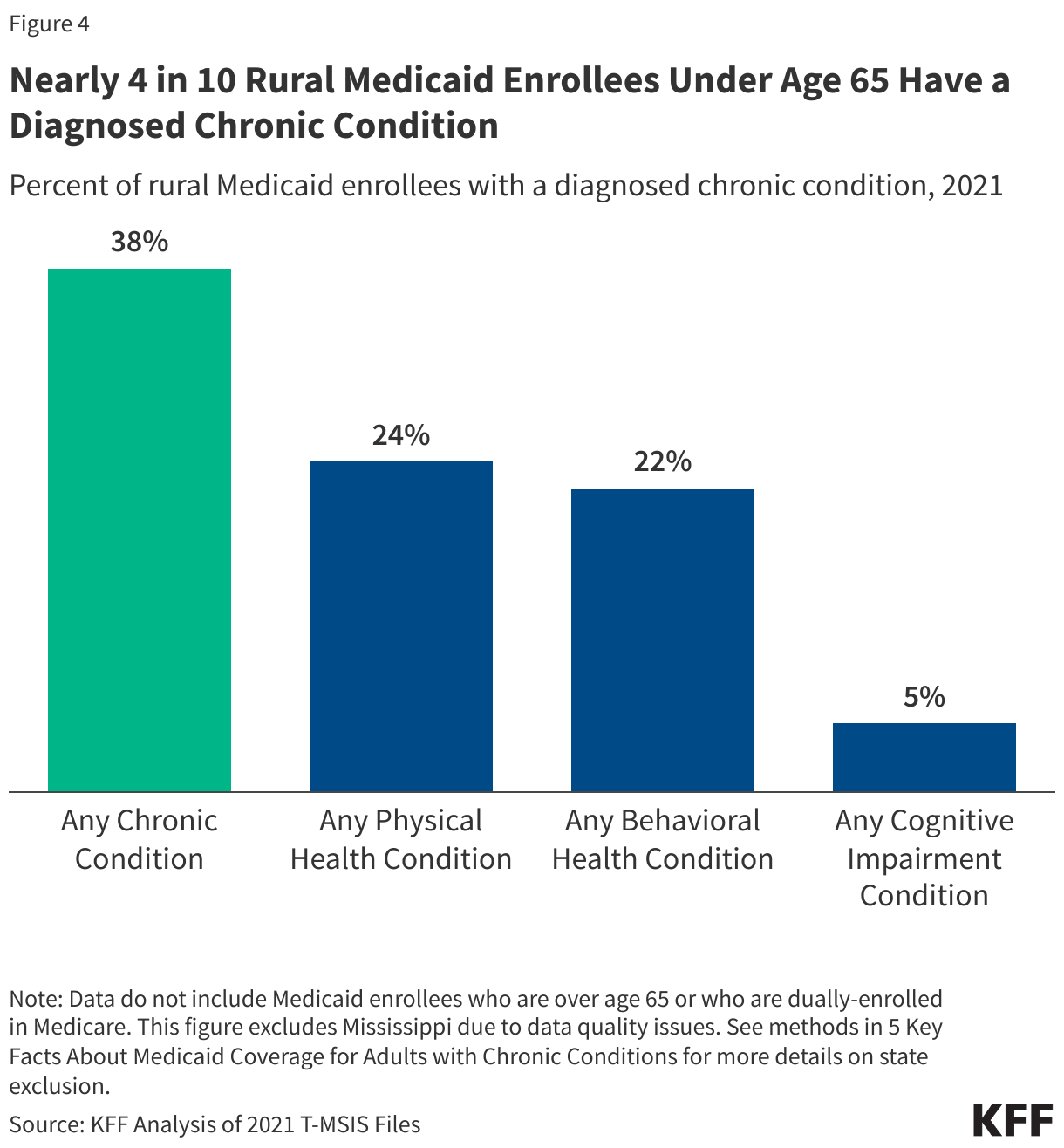
4. Nearly 4 in 10 rural Medicaid enrollees under age 65 have a diagnosed chronic condition.
Chronic conditions are conditions that last at least one year and require ongoing medical care or limit daily activities (e.g. heart disease, diabetes, cancer, mental illness, etc.). Thirty-eight percent of rural Medicaid enrollees under age 65 and not dually enrolled in Medicare have at least one diagnosed chronic condition. Of those with at least one chronic condition, approximately one-quarter have three or more chronic conditions (data not shown). The most diagnosed chronic conditions for these rural Medicaid enrollees are physical (which include high blood pressure, obesity and high cholesterol), with 24% of rural Medicaid enrollees having at least one diagnosed physical health condition. Behavioral health conditions, which include mental health and substance use conditions, are diagnosed in 22% of rural Medicaid enrollees and 5% of rural Medicaid enrollees have a diagnosed cognitive impairment condition, including dementia and intellectual and developmental disabilities, which often cause functional limitations that require long-term care.
Rates of diagnosed chronic conditions are calculated from Medicaid claims data, which reflect only diagnoses recorded during medical visits in 2021 and do not measure overall prevalence. Prevalence rates from surveys are generally higher than claims-based estimates because not everyone is screened, treated, or has a recorded diagnosis for their chronic conditions in claims data in any given year. The numbers exclude Medicaid enrollees who also have Medicare (since Medicare is the primary payer for outpatient and acute care services), as well as enrollees ages 65 and older, nearly all of whom also have Medicare coverage (see Methods for more details).
5. A higher percentage of rural Medicaid enrollees used care in expansion states than in non-expansion states.
Eighty-two percent of Medicaid enrollees living in rural areas in expansion states had at least one health care claim in the year compared to 74% of rural Medicaid enrollees in non-expansion states. Enrollees living in urban areas in expansion states also utilized care at higher rates than those living in non-expansion states, although by a smaller margin than rural enrollees, 80% to 74%, respectively (data not shown).

Methods |
| American Community Survey Data: This analysis uses the 2023 American Community Survey (ACS) 1-year estimates to calculate Medicaid coverage rates in rural areas in Figures 1 and 2.
Medicaid Claims Data: This analysis uses the 2021 T-MSIS Research Identifiable Demographic-Eligibility and Claims Files (T-MSIS data) to identify rural Medicaid enrollees and their demographics, chronic conditions and utilization of care in Figures 3-5, Appendix Table 1 and Appendix Figures 1-2. State Exclusion Criteria:
Defining Rural Medicaid Enrollees in ACS and Medicaid Claims Data: Medicaid enrollees living in urban areas are defined as those living in a metropolitan area, while Medicaid enrollees living in rural areas are defined as those living in nonmetropolitan areas. A metropolitan area is a county or group of counties that contains at least one urban area with a population of 50,000 or more people. Nonmetropolitan areas include micropolitan areas—which are counties or groups of counties that contain at least one urban area with a population of at least 10,000 but less than 50,000—and noncore areas (areas that are neither metropolitan nor micropolitan). Appendix tables and figures further break down rural areas into those that are adjacent to metropolitan areas and those that are not adjacent to metropolitan counties (defined as the “most rural” areas in this brief). This analysis categorized counties and county equivalents based on 2024 Urban Influence Codes from the USDA, as follows:
Defining Chronic Conditions (Figure 4): This figure reflects diagnosed chronic conditions for rural Medicaid enrollees who are under age 65 and not dually enrolled in Medicare. This analysis used the CCW algorithm for identifying chronic conditions (updated in 2020). This analysis also included in its definition of chronic conditions substance use disorder, mental health, obesity, HIV, hepatitis C, and intellectual and developmental disabilities. In total, 35 chronic conditions were included and were further grouped into 3 broad categories: behavioral health, physical health, and cognitive impairment conditions. Specific conditions within these groupings include:
Defining Utilization of Care (Figure 5): An enrollee is determined to have utilized care in the year if they have a claim in the inpatient, long-term care, prescription drug or other services files in the T-MSIS data. |
Appendix


