Who Are Direct Care Workers and How Might Federal Policy Changes Impact the Workforce?
Long-term care (LTC) encompasses the broad range of paid and unpaid medical and personal care services that assist with activities of daily living (such as eating, bathing, and dressing) and instrumental activities of daily living (such as preparing meals, managing medication, and housekeeping). The Department of Health and Human Services (HHS) reports that after age 65, over half of people will at some point need help with at least two activities of daily living, over half will use paid LTC, and over one-third will use some nursing home care. People under 65 with disabilities also rely on LTC for assistance with activities of daily living and instrumental activities of daily living. Medicaid is the primary payer for long-term care (LTC), and KFF analysis of Medicaid claims data found that over half of people who used any Medicaid LTC were under 65.
Direct care workers play a pivotal role in providing LTC services. They perform demanding, high-stress work for low wages and often no benefits. This has contributed to the long-standing shortages and high turnover rates among direct care workers in both home care and institutional care settings. Recent federal policy changes could further exacerbate the challenge of retaining and growing the workforce to care for the aging population. Specific policy changes that could exacerbate these challenges include the following.
- Broad changes to Medicaid, including $911 billion in reductions to federal spending and Medicaid work requirements, could have implications for the direct care workforce given Medicaid’s outsized role in LTC spending and relatively high Medicaid coverage rates among direct care workers.
- Direct care workers may also feel the impacts of recent changes in immigration policy. Three in ten direct care workers are immigrants, including naturalized citizens and noncitizens, who include lawfully present and undocumented immigrants. The Trump Administration’s intensified immigration enforcement and restrictive policies are deepening anxiety and fear among immigrants of all statuses and could contribute to reduced immigration in the future, which could exacerbate workforce shortages.
- Two proposed rules from the Department of Labor may also have an impact on direct care workers. One rule would roll back minimum wage and overtime protections for home care workers. The other rule would make it easier for employers to classify direct care workers as independent contractors, which would strip them of some labor protections.
- CMS has also delayed enforcement of a provision in the Medicaid Access Final Rule that would have required states to establish an advisory group to provide recommendations on direct care worker provider rates.
This analysis uses the 2024 American Community Survey (ACS) to provide an overview of demographic and socioeconomic characteristics of the direct care workforce, including home health aides, personal care aides, and nursing assistants who work in nursing facilities, residential care facilities, home health, and settings that provide nonresidential services for older adults and younger adults with disabilities (see Methods). 2024 ACS data was released in late 2025 and is the most recent data available. Other KFF analyses on the direct care workforce in nursing homes include RNs and LPNs (collectively referred to as “nurses”), but this analysis excludes nurses and only includes aides that assist older adults and people with disabilities with essential daily tasks. Nurses provide key services for older adults and younger people with disabilities who use long-term care services but are excluded from this analysis because they are socioeconomically and demographically different than aides. Key takeaways include:
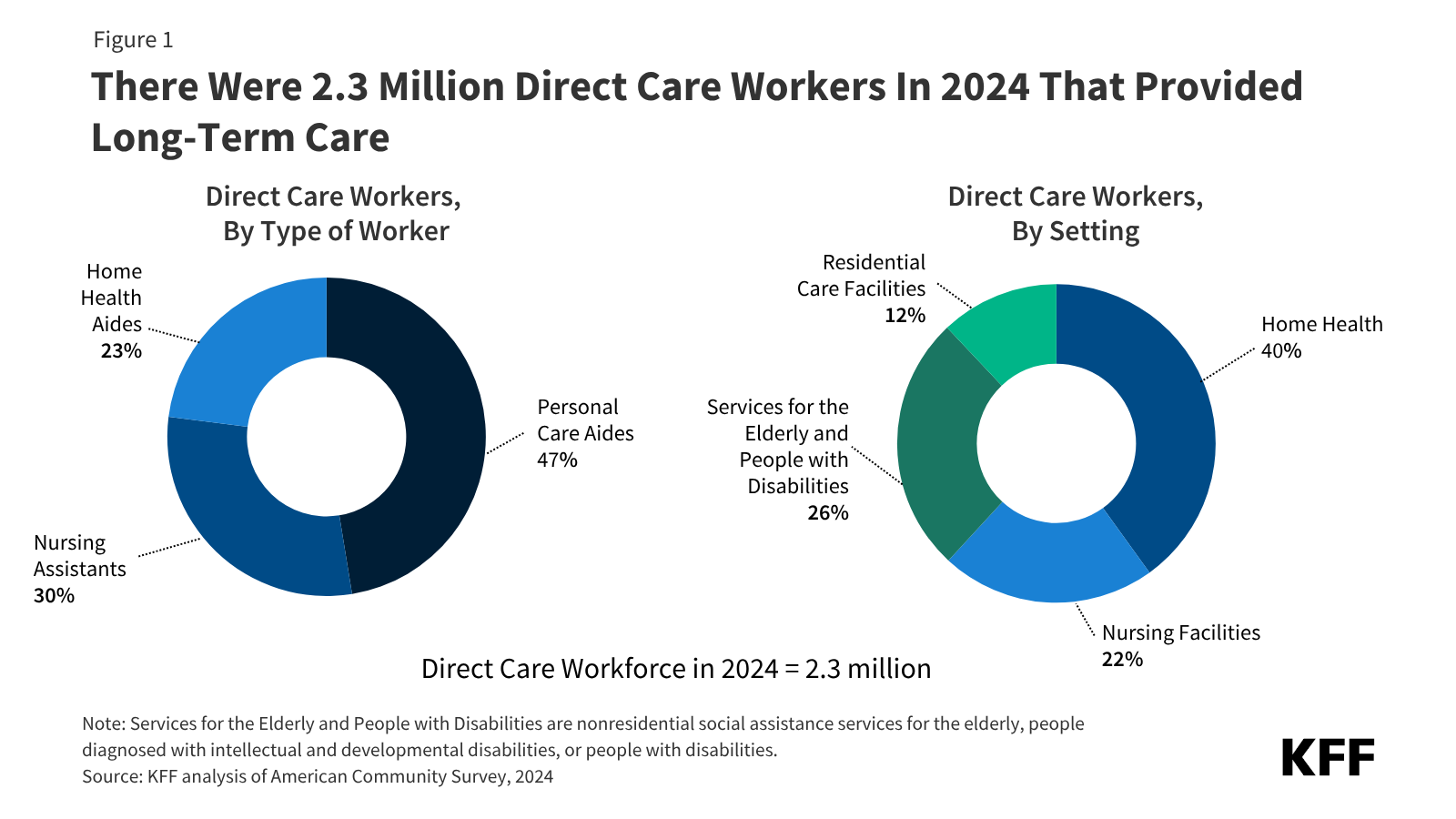
- In 2024, there were 2.3 million direct care workers who provided long-term care to people ages 65 and older and people under 65 with disabilities (Figure 1).
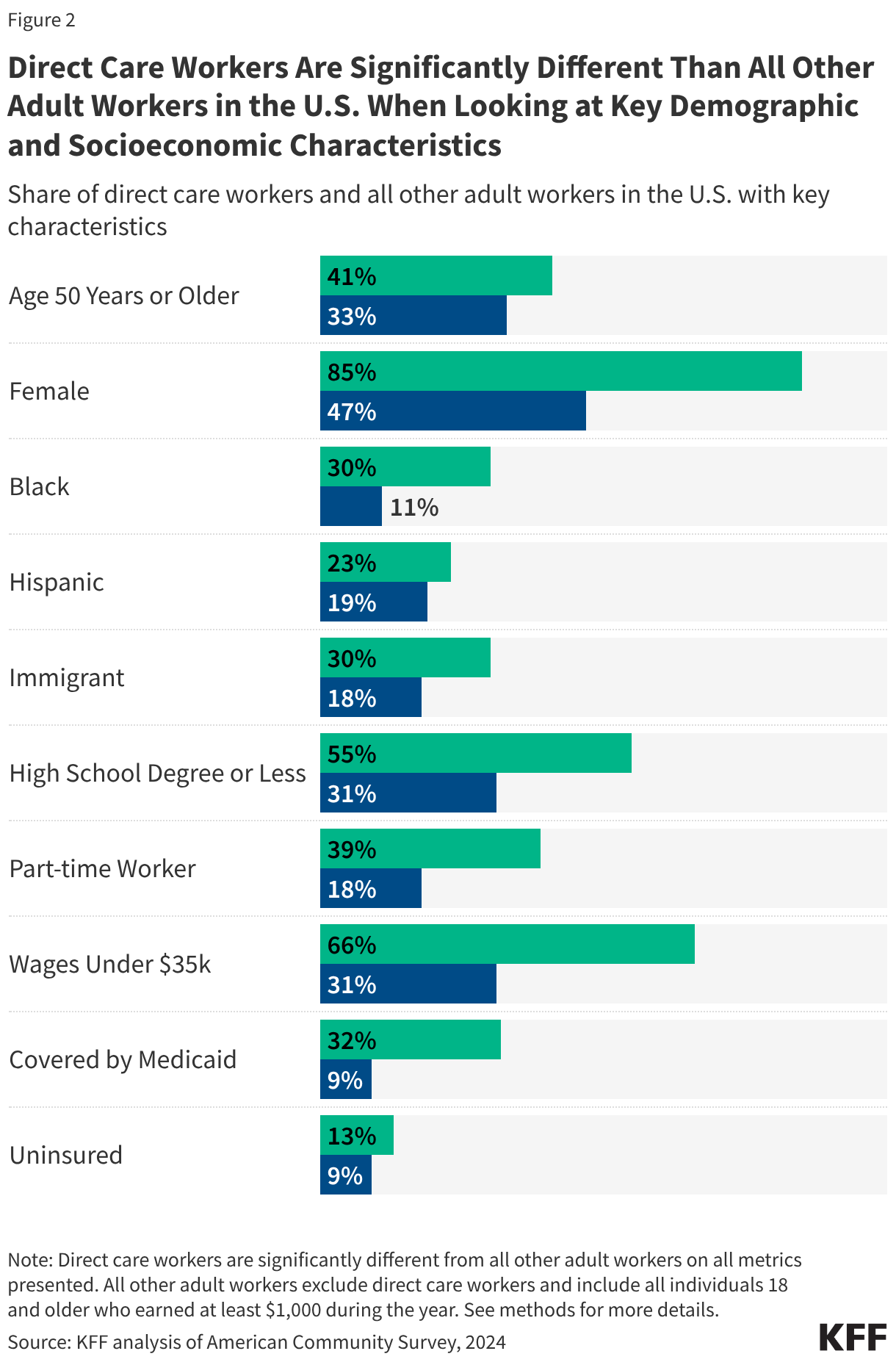
- Direct care workers are significantly more likely to be age 50 years or older, female, Black or Hispanic, or immigrants when compared to all other adult workers in the U.S. (Figure 2).
- Direct care workers are also significantly more likely to have a high school degree or less, work part-time, be low-wage, or be covered by Medicaid or be uninsured when compared to all other adult workers in the U.S. (Figure 2).
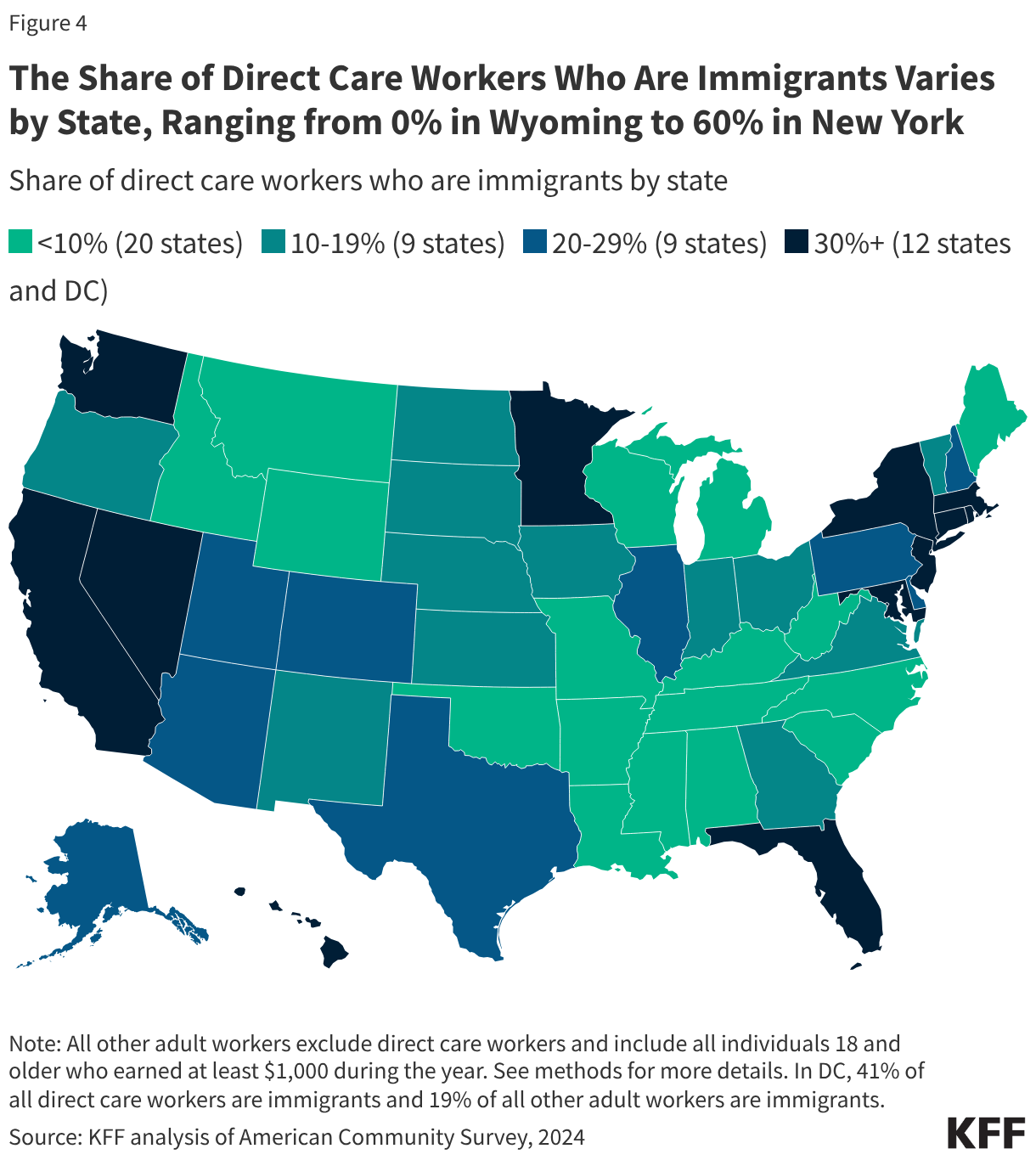
- The share of direct care workers who are immigrants varies by state, ranging from 0% in Wyoming to 60% in New York (Figure 4).
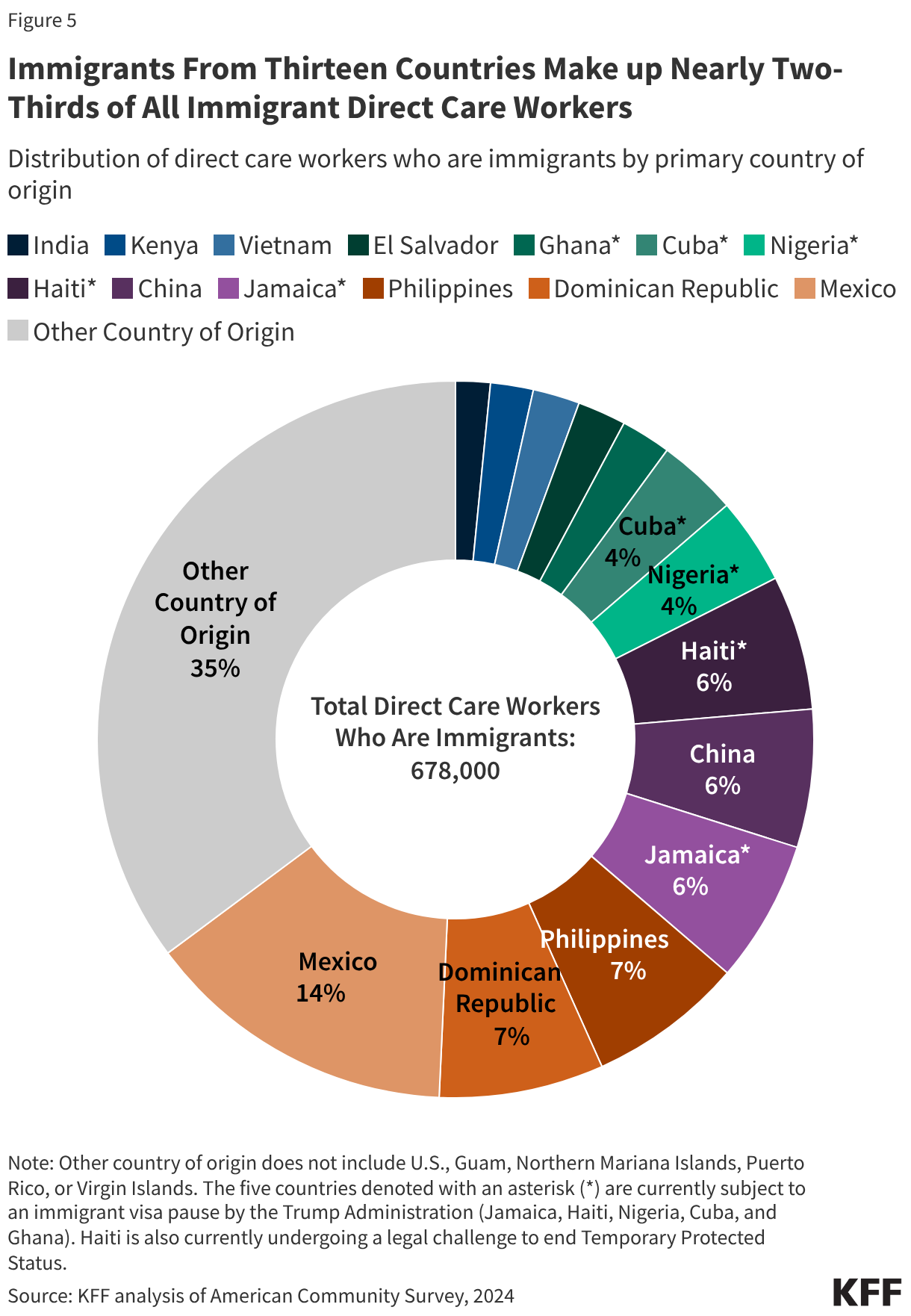
- At least one in five immigrant direct care workers is from a country within the 75 countries that are part of the Trump administration’s immigrant visa pause, which could further strain the workforce in future years (Figure 5).
In 2024, there were 2.3 million direct care workers who provided long-term care to people ages 65 and older and people under 65 with disabilities (Figure 1). Direct care workers include personal care aides, nursing assistants, and home health aides.Other sources use a similar definition of direct care workers but use data from the Bureau of Labor Statistics (BLS) to estimate the total number of workers, leading to different counts. The BLS data are more recent than the American Community Survey. See Box 1 for a definition of types of direct care workers included in this analysis.
Direct care workers provide long-term care services across a variety of settings, with 66% providing care in home care settings, 22% in nursing facilities, and 12% in residential care facilities (Figure 1). “Home care settings” include “home health” and “services for the elderly and people with disabilities” from Figure 1 and Box 1. Excluding Figure 1 and Box 1, this analysis presents these categories as one combined “home care” category. See Box 1 for definitions of the direct care worker and setting types.
Box 1: Who Are Direct Care Workers and Where Do They Work?
By Type of Worker:
Personal Care Aides:Personal care aides assist older adults and people with disabilities living at home with ADLs. Personal care aides also help with instrumental activities of daily living (IADLs), such as grocery shopping, meal preparation, and managing medications.
Nursing Assistants: Nursing assistants, or certified nursing assistants (CNAs), typically work in nursing homes and assist residents with ADLs. All CNAs must have completed a nurse aide training and competency evaluation program within 4 months of their employment. They must also pursue continuing education each year.
Home Health Aides: Home health aides assist older adults and people with disabilities living at home with medical care. They may help with checking vital signs, assist with medical equipment, and help with administering medication. They may also help with activities of daily living (ADLs), which include eating, bathing, dressing, assisting with walking/exercise, and using the bathroom.
By Setting of Care:
Home Health: Home health agencies are organizations that provide skilled rehabilitative or post-acute care as well as long-term personal care for patients. The same skilled services provided by skilled nursing facilities, such as nursing, occupational therapy, and physical therapy, are instead provided in the home, along with assistance with ADLs and IADLs.
Services for the Elderly and People with Disabilities: These are services or settings that provide nonresidential, social assistance services for older adults and younger adults with disabilities. These establishments typically focus on the welfare of these individuals in such areas as day care, non-medical home care or homemaker services, social activities, group support, and companionship. These services and settings can include adult day care centers, home care services for older adults, and companion services.
Nursing Facilities: Nursing facilities are residential settings that provide round-the-clock nursing and personal care to residents who either need short-term rehabilitation following a hospitalization or injury or long-term care to residents with chronic medical and/or mental health conditions requiring access to 24-hour skilled care and assistance with ADLs or personal care.
Residential Care Facilities: These settings include residential settings that serve individuals with intellectual and developmental disabilities, mental illness, or substance use disorder. These settings also include establishments that provide residential and personal care services for older adults or younger adults with disabilities who are unable to fully care for themselves. These settings can include assisted living facilities, continuing care retirement communities, and group homes for adults with disabilities. The care typically includes room, board, supervision, and assistance with activities of daily living.
Direct care workers are significantly more likely to be age 50 years or older, female, Black or Hispanic, or immigrants when compared to all other adult workers in the U.S. (Figure 2). Direct care workers are more likely to be age 50 years or older when compared to all other adult workers (41% vs 33%), as well as more likely to be female (85% vs 47%). They are also more likely to be Black than all other adult workers in the U.S. (30% vs 11%). They are also more likely to be Hispanic when compared to all other adult workers in the U.S. (23% vs 19%).Immigrants, including naturalized citizens and noncitizens, make up 30% of the overall direct care workforce, higher than the share of all adult workers in the U.S. who are immigrants (18%).
Direct care workers are also significantly more likely to have a high school degree or less, work part-time, be low-wage, and be covered by Medicaid or be uninsured when compared to all other adult workers in the U.S. (Figure 2). Direct care workers are more likely to have a high school degree or less than compared to all other adult workers (55% vs. 31%). They are also more likely to work part-time and make less than $35,000 annually (referred to as “low wage”) when compared to all other adult workers (39% vs 18%; 66% vs 31%). Direct care workers are also much more likely to be covered by Medicaid (32%) than all other adult workers (9%) and more likely to be uninsured when compared to all other adult workers (13% vs. 9%).
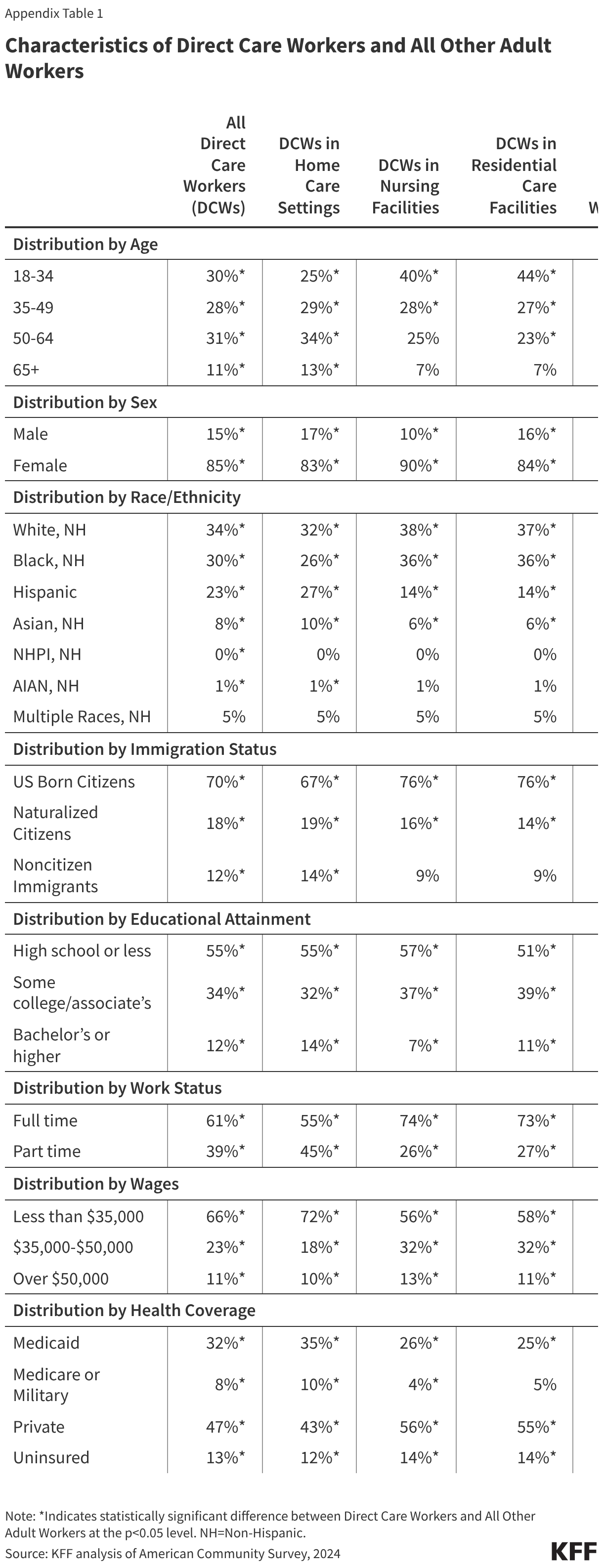
Direct care workers in home care settings are different than direct care workers in nursing homes or residential care facilities (Appendix Table 1). A higher share of direct care workers in home care settings are immigrants (33%) when compared to direct care workers in nursing facilities (25%) and residential care facilities (23%) (Figure 3). Additionally, a higher share of direct care workers in home care settings work part-time (42%) when compared to workers in nursing homes (24%) and residential care facilities (25%). Similarly, a higher share of home care workers are low-wage (72%) when compared to those working in nursing homes (56%) or residential care facilities (58%) (Appendix Table 1).
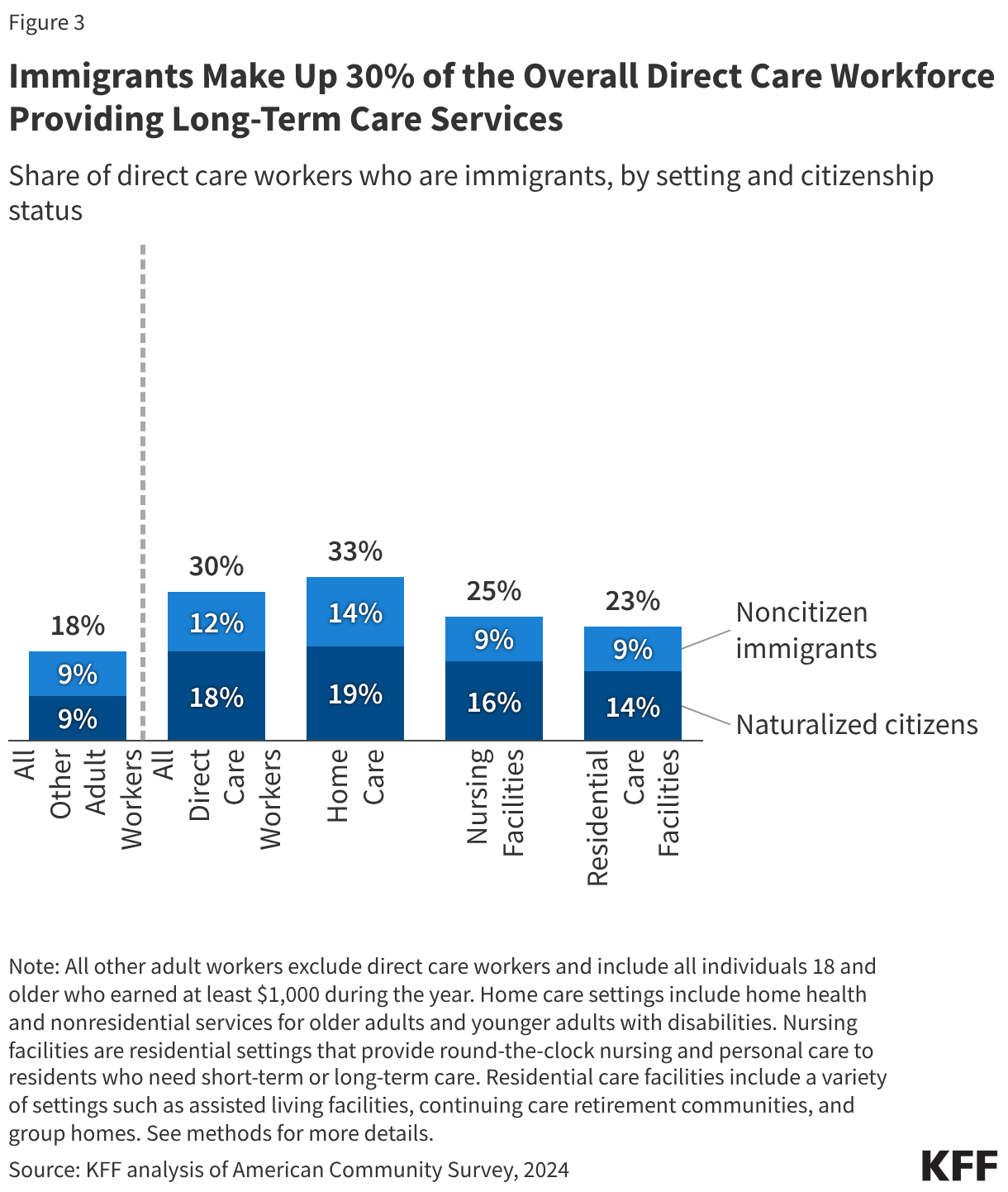
Immigrants make up 30% of the overall direct care workforce providing long-term care services (Figure 3). Naturalized citizens make up a significantly larger share of direct care workers in home care settings (19%) when compared to nursing facilities (16%) and residential care settings (14%). Home care workers are also significantly more likely to be noncitizen immigrants (14%) when compared to workers in nursing homes (9%) and residential care facilities (9%). Noncitizen immigrants include both lawfully present and undocumented immigrants.
The share of direct care workers who are immigrants varies by state, ranging from 0% in Wyoming to 60% in New York, and, in many cases, reflects the share of overall immigrant workers (Figure 4). In 20 states, including many Southern states, the share of direct care workers who are immigrants is under 10%. In 9 states, the share of direct care workers who are immigrants is between 10% and 19%. In 9 states, 20% to 29% of direct care workers are immigrants, and in the remaining 13 states (including DC), 30% or more of direct care workers are immigrants. The share of direct care workers who are immigrants is strongly positively correlated with the overall share of workers in a state that are immigrants.
Immigrants from 13 countries make up nearly two-thirds (65%) of all immigrant direct care workers providing long-term care in the U.S. (Figure 5). The remaining one-third of immigrant direct care workers come primarily from a mix of countries in South and Central America, Africa, and Asia. Six countries each account for 5% or more of immigrant direct care workers: Mexico (14%), Dominican Republic (7%), Philippines (7%), Jamaica (6%), China (6%), and Haiti (6%).
At least one in five immigrant direct care workers is from a country that is part of the Trump administration’s immigrant visa pause (Figure 5). Among the top 13 countries that make up nearly two-thirds of immigrant direct care workers, five of them are part of the Trump administration’s immigrant visa pause (Jamaica, Haiti, Nigeria, Cuba, and Ghana) that impacts 75 countries. While the immigrant visa pause is facing a court challenge, it currently remains in effect. On June 25, 2026, the Supreme Court issued a ruling allowing the Trump administration to proceed with terminating Haiti’s TPS designation, which could impact over 300,000 Haitian TPS holders. These policies could further strain the workforce in future years.
Methods
Data: These findings are based on KFF analysis of the 2024 American Community Survey (ACS) 1-year Public Use Microdata Sample (PUMS) files. The ACS includes a 1% sample of the U.S. population, and the subset of direct care workers used here includes 19,612 observations.
Identifying Direct Care Workers in ACS: Direct care workers are those who fall into the following occupation codes: Home health aides (3601); Personal care aides (3602); and Nursing assistants (3603). This analysis only includes those who work in the following industries: Home Health Care (8170), Nursing Care Facilities (8270), Residential Care Facilities (8290), and Individual and Family Services (8370). “Individual and family services” are also referred to as “services for the elderly and people with disabilities.” Home health care and individual and family services are collapsed into “Home care” for this analysis. These industries capture most workers providing long-term health services. The ACS only includes the primary industry and occupation of a respondent’s current or most recent (in case the respondent is not currently working) job.
We define the direct care workforce as all individuals 18 and older who earned at least $1,000 during the year and indicated that their job was in both the long-term care industry and occupation codes listed above. The comparison group “All Adult Workers in the U.S.” includes all individuals 18 and older who earned at least $1000 during the year.
Health Insurance Coverage in ACS: The ACS asks respondents about their health insurance coverage at the time of the survey. Respondents may report having more than one type of coverage; however, individuals are sorted into only one category of insurance coverage. See notes here for more information on the insurance coverage hierarchy.
Identifying Immigrants in ACS: Immigrants are identified as those who report their citizenship status (variable name: CIT) in ACS as being a “U.S. citizen by naturalization” or as “not a citizen of the U.S.”, with the former being grouped under “naturalized citizens” and the latter being grouped under “noncitizen immigrants” for the purpose of this analysis. Noncitizen immigrants include lawfully present and undocumented immigrants.
Appendix