Over-the-Counter Oral Contraceptive Pills
Editorial Note: Originally published on September 27, 2024, this brief was updated on March 10, 2026 to incorporate new federal policy developments on contraceptive coverage.
Overview
Oral contraceptives are the most commonly used method of reversible contraception in the U.S. Oral contraceptive pills were first approved for prescription use by the U.S. Food and Drug Administration (FDA) in 1960. Over 70 years later, on July 13, 2023, the FDA approved Opill, the first daily oral contraceptive pill to become available over-the-counter (OTC) without a doctor’s prescription. It has been available online and in stores since March 2024 to people of all ages. The formulation in Opill was initially approved for prescription use by the FDA in 1973 (by a different manufacturer and with a different brand name). This issue brief provides an overview of OTC oral contraceptives and laws and policies related to insurance coverage.
Safety, Efficacy, and Convenience
Oral contraceptive pills are highly effective at preventing pregnancy with “perfect use”, with a failure rate of less than 1%. However, the failure rate with “typical use,” which accounts for inconsistent or incorrect use, is 9%. Oral contraceptive pills must be taken once per day and are primarily used for pregnancy prevention, but they can also be used to address other health conditions such as menstrual pain, irregular menstruation, fibroids, endometriosis-related pain, menstrual-related migraines, and acne management. Oral contraceptives, especially progestin-only pills, are safe for most women.
Oral contraceptive pills, especially progestin-only pills, are safe for most people to use and have a very low risk of serious side effects or contraindications. Possible side effects from the pill include headache, nausea, breast tenderness, and breakthrough bleeding. Research has found that people, including those under the age of 18, are able to understand label instructions and contraindications for OTC contraception without clinician involvement.
Although it is not as far along in the FDA approval process, another pharmaceutical company, Cadence, is working toward FDA approval of an OTC version of its combined (progestin and estrogen) oral contraceptive pill, Zena. Combined oral contraceptive pills have more contraindications and small, but higher, risks of serious side effects than progestin-only pills like Opill. They are believed to be slightly more effective at preventing pregnancy than progestin-only pills and while they also must be taken every day, there is more flexibility on the precise timing.
Over-the-counter (OTC) status is an FDA designation meaning that a drug or product is available without a prescription from a health care provider. The ability to access oral contraceptives without a prescription from a clinician can save time spent on travel, at a doctor’s office, and off work. Studies suggest that OTC access to oral contraceptives could increase the use of contraception, facilitate continuity of use, and reduce the risk of unintended pregnancy.
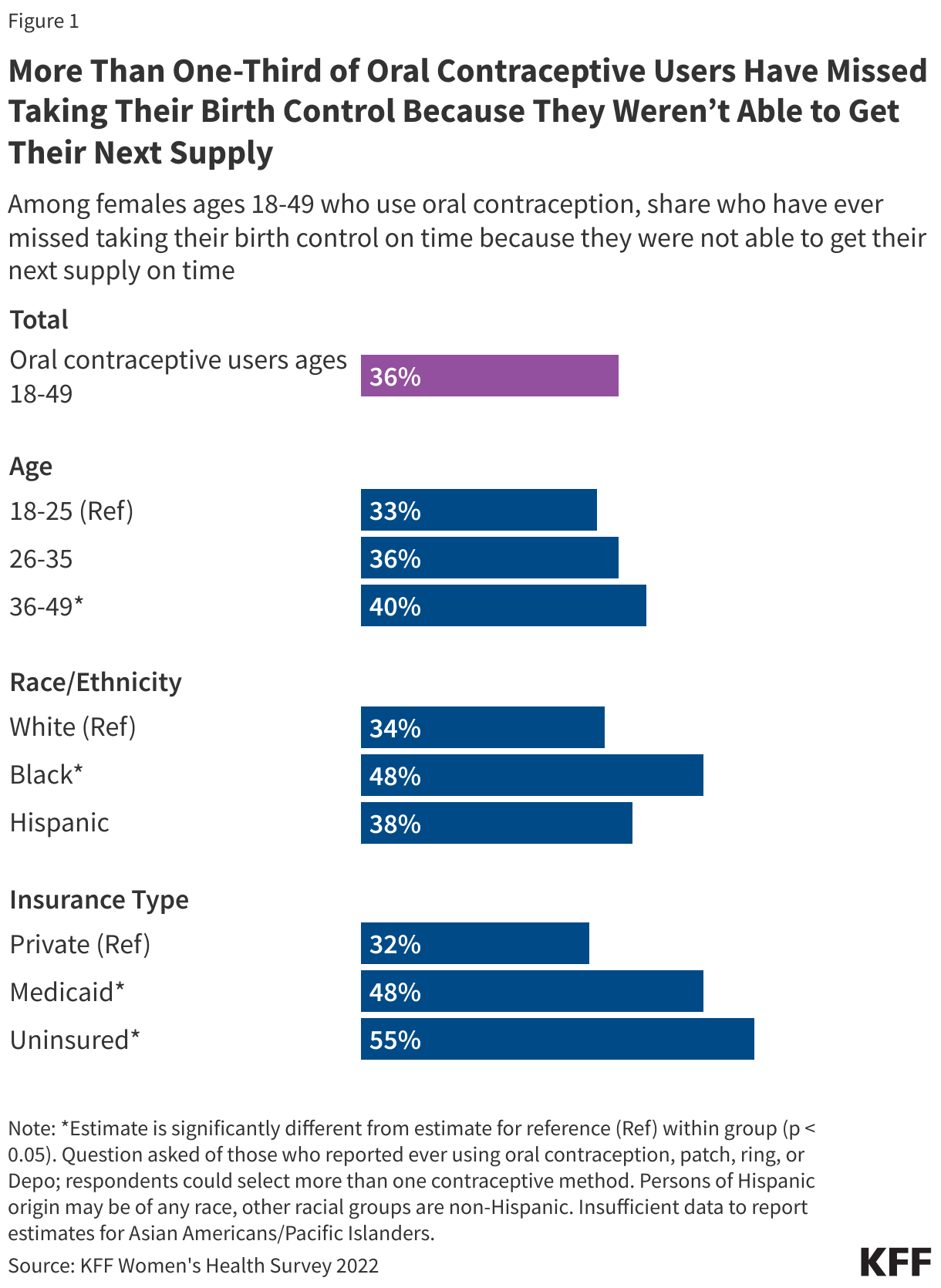
Previous KFF research found that more than one-third (36%) of reproductive-age female respondents who use oral contraception have missed taking it on time because they were not able to get their next supply (Figure 1). The added convenience and time saved by obtaining oral contraception OTC instead of having to visit a doctor could reduce the share of women who miss taking their contraception on time.
Consumer Awareness and Use
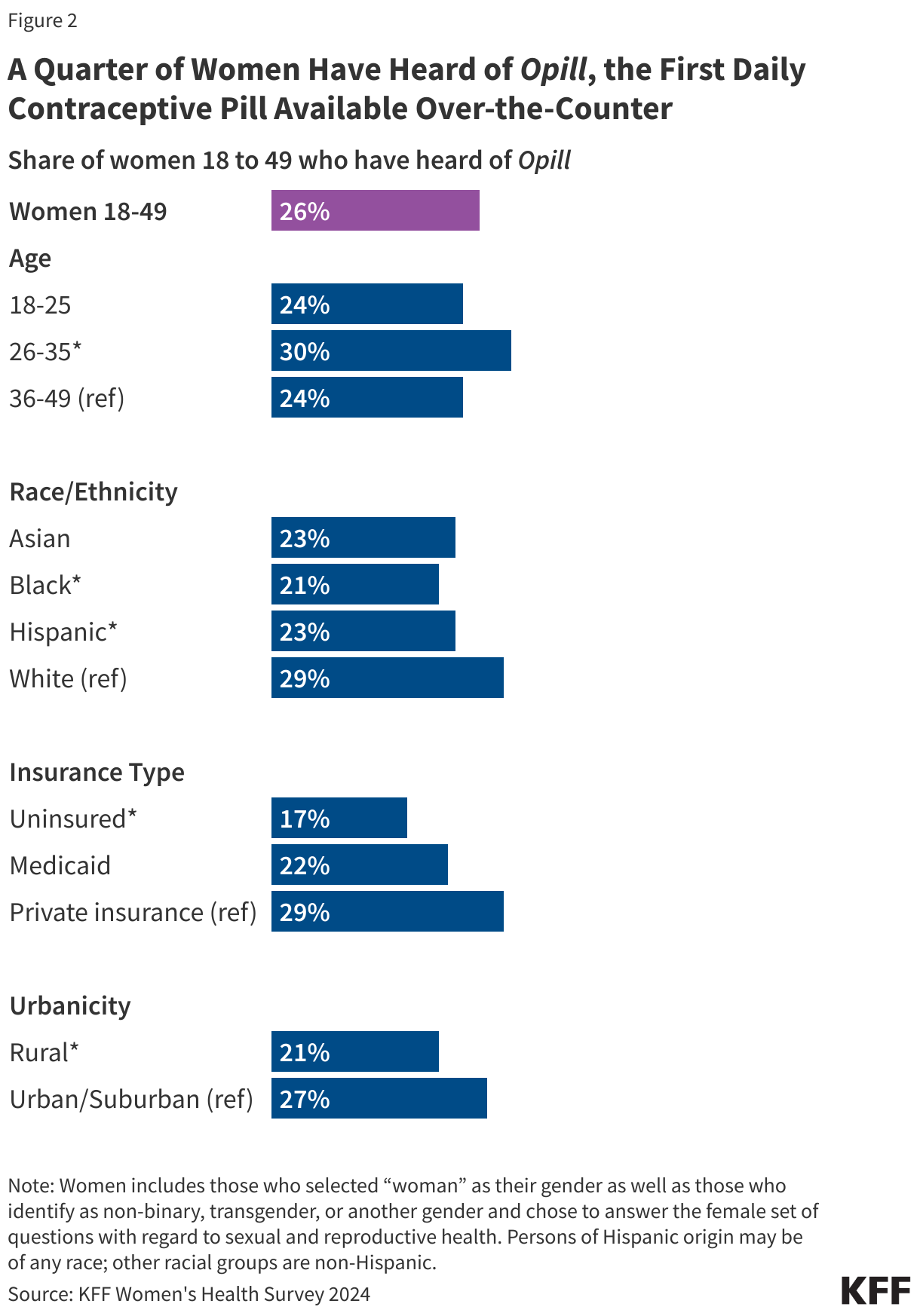
The nationally representative 2024 KFF Women’s Health Survey found that awareness of Opill is generally low, with just a quarter (26%) of women 18 to 49 saying they have heard of the new daily oral contraceptive pill (Figure 2). Compared to women ages 36 to 49 (24%), significantly larger shares of women ages 26 to 35 say they have heard of Opill. Smaller shares of Black (21%) and Hispanic (23%) women say they have heard of the new oral contraceptive compared to White women (29%).
Research suggest that OTC oral contraceptives can especially benefit populations who have historically faced barriers to accessing contraceptive care, such as young adults and adolescents, those who are uninsured, and those living in contraceptive deserts or areas with limited access to health centers offering the full range of contraceptive methods. However, smaller shares of women who are uninsured (17%) and who live in rural areas (21%) have heard of Opill compared to those with private insurance (29%) and those living in urban or suburban areas (27%).
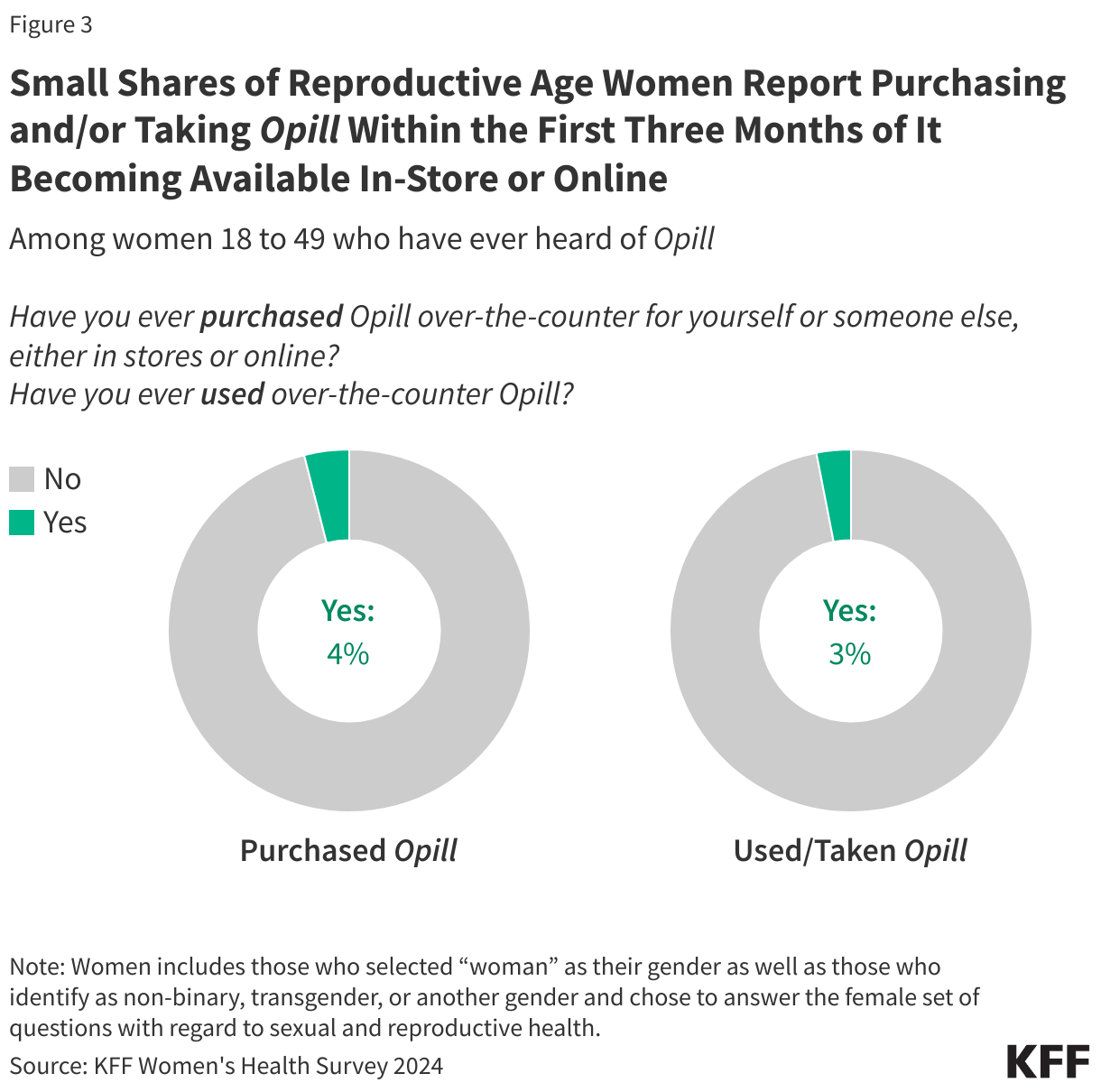
Among women 18 to 49 who have ever heard of Opill, just 4% say they have ever purchased the over-the-counter contraceptive pill for themselves or for someone else (Figure 3). An even smaller share (3%) say they have used or taken Opill since the contraceptive became available in stores and online earlier in 2024.
A separate cross-sectional study from 2025 found that individuals who used an OTC oral contraceptive were more likely to be uninsured and reside in rural areas. The authors noted that many OTC oral contraceptive users previously used a less effective method or no method at all, suggesting that OTC availability could improve access to more effective birth control.
Other OTC Contraception
Levonorgestrel emergency contraceptive (EC) pills, known as “the morning after pill” and marketed as Plan B One-Step and other brands, are a form of backup birth control intended to be taken several days after unprotected sex or contraceptive failure. Levonorgestrel EC pills were the first hormonal contraception to have switched from prescription to OTC status, in 2006. Unlike daily oral contraceptives, emergency contraception is not intended for daily use and is FDA approved for use by women within 72 hours (3 days) after unprotected intercourse or contraceptive failure to prevent pregnancy.
Other contraceptive products that are available over the counter without a prescription include male and female condoms, spermicides, and contraceptive sponges. These contraceptive methods are less effective than oral contraception at preventing pregnancy. FDA’s approval of Opill makes it the most effective form of contraception available over the counter intended for regular use.
Federal Laws on OTC Contraceptive Coverage
Private Insurance
The Affordable Care Act (ACA) requires most private health plans (group and individual) to cover, without cost sharing, the full range of FDA-approved contraceptive methods, which includes oral contraceptive pills. The ACA tasks the Health Resources and Services Administration (HRSA) with coverage requirements for a range of preventive services for women, which now includes contraception, that must be covered by insurance. Right after the ACA was passed, HRSA tasked the Institute of Medicine (IOM) to identify gaps in preventive recommendations. This committee identified contraceptive services and supplies as one of the eight gaps in preventive health services to promote women’s health. The IOM recommended that all FDA-approved contraceptives be included as preventive services, and the HRSA coverage requirement for contraception included that they be covered “as prescribed,” which was reflected in the original guidance issued by the Obama administration in 2013.
Currently, HRSA has commissioned the Women’s Preventive Services Initiative (WPSI) as the expert body it relies on to update and expand preventive services coverage recommendations, which WPSI last updated in 2021. The current coverage requirement posted by HRSA no longer includes a prescription requirement for coverage of contraception, but the U.S. Departments of Labor, Health and Human Services, and Treasury (federal tri-agency) guidance has not been revised to drop the “as prescribed” requirement.
The prescription requirement is currently only mentioned in federal FAQs clarifying ACA coverage requirements, with the most recent one issued by the Biden administration in July 2022. The FAQ references coverage of emergency contraception and states that plans must cover OTC contraceptives when the product is prescribed. It also states that plans are “encouraged to cover OTC emergency contraceptives with no cost sharing when they are purchased without a prescription.” In October 2024, the Biden administration proposed a new rule that would have broadened the ACA’s coverage requirements and, if finalized, would have required private insurers and states with ACA Medicaid expansion to cover OTC contraceptives without a prescription. However, the proposed regulation was withdrawn in January 2025, before the change in administration.
OTC medications and products do not require a prescription for purchase, but most people wishing to avoid cost-sharing for them need to obtain one. The prescription requirement re-introduces some of the same barriers that were intended to be reduced with OTC status such as eliminating the need to make and wait for a doctor appointment or find a pharmacy whose pharmacists are licensed and available to prescribe contraception (where permitted by state law).
Medicaid
Medicaid is the public health insurance program that covers approximately 20% of low-income children, adults, seniors, and people with disabilities. Medicaid is jointly financed by the federal government and the states. Federal statute sets broad minimum standards in exchange for federal matching funds and states have flexibility in determining other aspects of their Medicaid programs such as covered services and provider payment models.
Coverage for contraceptives is a key element in Medicaid coverage of family planning services. All states cover prescription drugs, even though it is technically an “optional” benefit category under federal law. Federal rules require state Medicaid programs that cover prescription drugs (including OTC drugs with a prescription) to cover all prescription drugs from manufacturers that have entered into a federal rebate agreement with the U.S. Secretary of Health and Human Services, though states may determine whether and how to employ utilization management controls. In order to obtain federal matching funds, a prescription is required for over-the-counter drugs and products.
Federal law also requires state Medicaid programs to cover family planning services and supplies without cost-sharing to enrollees. The federal Medicaid law does not define what services must be included and also does not explicitly cite OTC contraceptives as part of the coverage requirement, but most state Medicaid programs cover a range of contraceptive methods, and some cover OTC methods. The ACA requires states to cover at least one form of all 18 FDA-approved contraceptive methods for enrollees who qualify through the ACA’s Medicaid expansion. In general, these services are defined and determined by the states within broad federal guidelines.
With few exceptions (such as prenatal vitamins, fluoride preparations for pregnant people, and tobacco cessation products), federal law does not require states to cover OTC drugs and products in their Medicaid programs. However, state Medicaid programs can opt to cover them by submitting a state plan amendment (SPA) to CMS, the federal agency that administers Medicaid in partnership with state Medicaid agencies. For example, CMS approved SPAs Delaware, Montana, and Florida requesting to cover select OTC drugs generally. After obtaining approval from CMS to cover OTC products generally, states can choose which OTC products their program will cover. However, even when a drug is available to purchase without a prescription, enrollees usually need a prescription to obtain coverage under Medicaid and states cannot obtain federal matching dollars unless it is prescribed. If states wish to include coverage for OTC products without a prescription, state Medicaid programs may opt to use state-only funds.
State Laws on OTC Contraceptive Coverage
State-regulated private health insurance
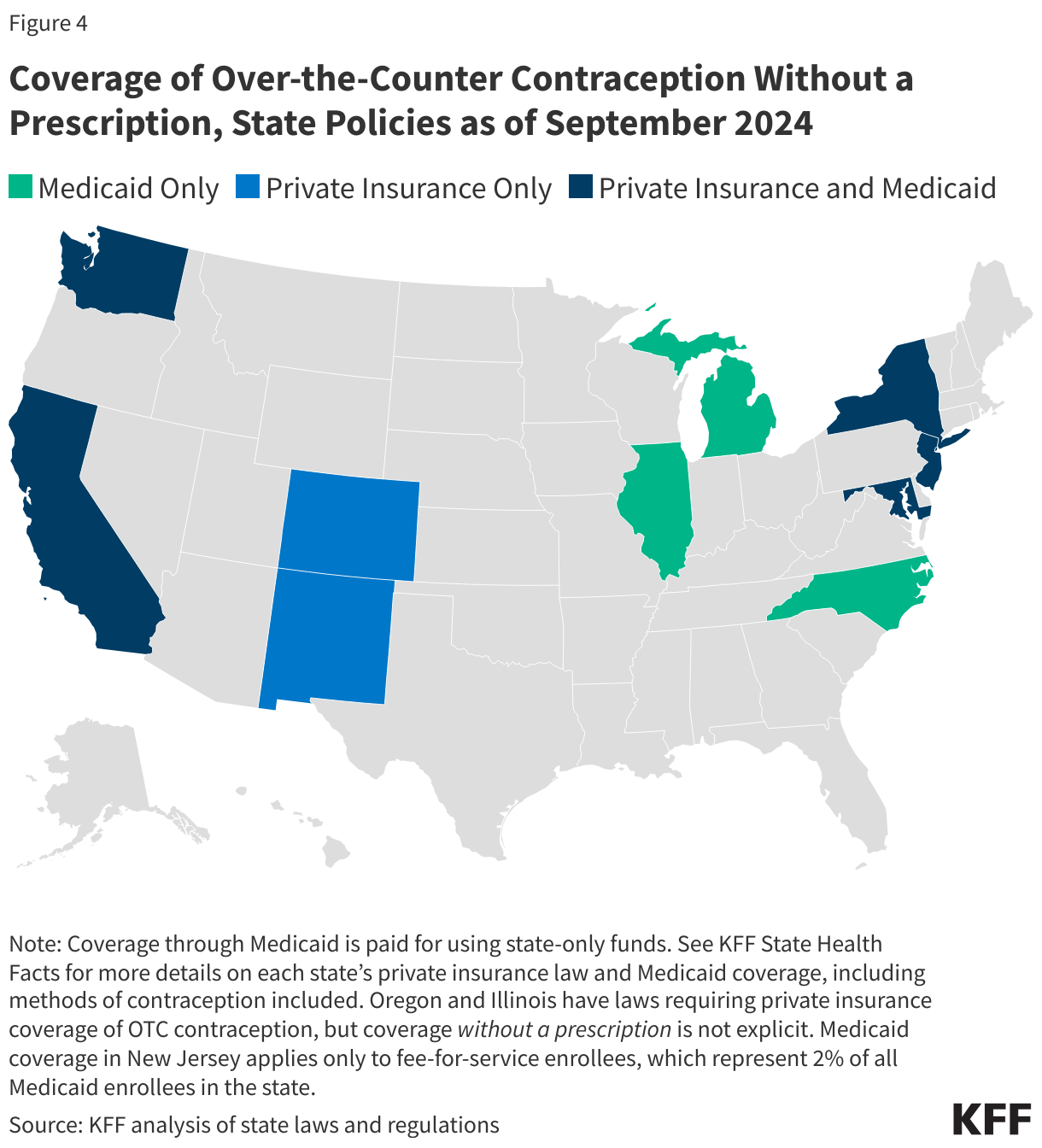
To reduce access barriers to OTC contraception while also avoiding cost sharing, nine states (CA, CO, DE, MD, ME, NJ, NM, NY, and WA) have laws or regulations requiring state-regulated private health insurance plans (individual, small group, and large group markets) to cover, without cost sharing, at least some methods of OTC contraception without a prescription (Figure 4). With the exception of New York, which applies only to emergency contraception, the language of these laws is broad enough to encompass an OTC daily oral contraceptive such as Opill without a change in policy. (See KFF State Health Facts for more details on each state’s law, including contraceptive methods covered.)
Illinois and Oregon require private health plans to cover OTC contraception; however, while the laws do not state that a prescription is required in order for it to be covered by insurance, the laws also do not explicitly stipulate that plans must cover them without a prescription. Massachusetts requires private plans to cover OTC emergency contraception with a prescription or pursuant to a standing order or protocol. A standing order allows a physician of a state health department or other state agency to authorize pharmacists to prescribe drugs or provide care under certain conditions set forth in the order.
While federal law applies to all plans, state law applies to only individual plans and fully-insured group plans. Therefore, many people who live in states that require coverage of OTC contraception without a prescription may not have this coverage if they are enrolled in a self-funded employer-sponsored health plan (67% of covered workers nationally).
Medicaid
To increase access to contraception, eight states (CA, IL, MD, MI, NC, NJ, NY, and WA) have opted to use state-only funds to cover at least some methods of OTC contraception for their Medicaid enrollees (primarily emergency contraception) without a prescription (Figure 4). With the exception of California and North Carolina, the language of these state-level policies does not appear broad enough to encompass an OTC daily oral contraceptive pill such as Opill without a change in policy (See KFF State Health Facts for more details on each state’s policy, including contraceptive methods covered.)
Challenges to the Broad Adoption of OTC Oral Contraception
There are some limitations to the potential reach of an over-the-counter progestin-only pill (POPs). While both progestin-only pills and combined pills (COCs) are safe and effective at preventing pregnancy, POPs are believed to be slightly less effective than COCs. It is recommended that users of POPs take the pill at the same time every day, which could be a barrier for people who are not able or would forget to do this. However, there is limited evidence that adhering to this precise timeframe actually reduces the efficacy of POPs. Clinical guidelines state that users have a three-hour window to take the POPs before back-up contraception is needed, though there have been recent efforts to reevaluate these guidelines as some evidence suggests there is a larger margin of error for some POPs and people have more flexibility in when they can take their pills without affecting effectiveness.
Opill’s reach may be limited because few women who use oral contraceptive pills use POPs and instead opt to use COCs. Currently, breastfeeding women are the primary users of POPs because these pills are safe for this population, and they are not advised to use COCs during this time. Whether users of COCs will opt to switch to Opill for reasons such as convenience or cost is not yet known.
Additionally, retailers can choose whether and how to stock Opill. Retailers who choose to sell it will also decide which supply option (one, three, or six-month packs) to stock. As is the case with emergency contraception at many retailers who stock it, Opill could be kept in a locked case on the shelf or behind the pharmacy counter to reduce the chance of theft, which could create access barriers.
The extent to which over-the-counter oral contraception is accessible will depend, in large part, on affordability and coverage. The suggested retail price for Opill is $19.99 for one month’s supply, $49.99 for three month’s supply, or $89.99 for a six month’s supply. KFF’s 2022 Women’s Health Survey found that 11% of women would not be willing or able to pay anything for an OTC oral contraceptive, and 39% would pay $1-$10 per month. Only 16% said they would pay more than $20 a month. Other research that asked specifically about a progestin-only pill found that adult women would be willing to pay $15 per month and teens ages 15-17 would pay $10.
Insurance coverage of OTC oral contraception without a prescription would eliminate out-of-pocket costs, but for those who prefer not to use their insurance or those who do not have insurance, the price point will matter. Furthermore, while some states require private plans and Medicaid to cover non-prescribed OTC contraception, not everyone in those states is entitled to this coverage. Absent federal guidance, guaranteed coverage of OTC oral contraception without a prescription will continue to depend on where people live and their type of health plan.