
Implementing Coverage and Payment Initiatives: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2016 and 2017
Long-Term Services and Supports Reforms
| Key Section Findings |
Additional information on LTSS expansions implemented in FY 2016 or planned for FY 2017 as well as state-level details on capitated MLTSS models can be found in Tables 12 and 13. |
LTSS System Rebalancing
Medicaid is the nation’s primary payer for long-term services and supports (LTSS), covering a continuum of services ranging from home and community-based services (HCBS) that allow persons to live independently in their own homes or in other community settings to institutional care provided in nursing facilities (NF) and intermediate care facilities for individuals with intellectual disabilities (ICF-ID). In 2013, spending on HCBS (51 percent of total LTSS expenditures) surpassed spending on institutional LTSS (49 percent of total LTSS expenditures) for the first time in the history of the program. The trend toward spending for services in the community continues, with the percentage of spending for HCBS in 2014 growing to 53 percent of total LTSS spending.1 This achievement represents a fundamental rebalancing of program expenditures over the last twenty years; in 1995, Medicaid reported that 82 percent of national expenditures on LTSS was in institutional settings, and that share is now less than half.2
This year’s survey shows, once again, that a large majority of states are employing a variety of tools and strategies to expand the number of people served in home and community-based settings for LTSS, including serving more people through existing or expanded Section 1915(c) HCBS waivers, new Section 1915(i) HCBS State Plan Option or Section 1915(k) Community First Choice State Plan Amendments, PACE program growth,3 and incentives to support system rebalancing through use of managed long-term services and supports (MLTSS). Expanding the numbers of individuals served through HCBS waivers and SPAs remains the most popular strategy, with 42 states in FY 2016 and 41 states in FY 2017 reporting they plan to increase the number of Section 1915(c) waiver slots, serve more individuals under existing Section 1915(c) waiver program caps, or are adding Section 1915(i) or Section 1915(k) state plan options to serve more individuals (Figure 7). Four states reported implementing a new Section 1915(i) state plan option for targeted populations in FY 2016, with five states intending to implement a Section 1915(i) state plan option for targeted populations in FY 2017. Three states implemented a new Section 1915(k) state plan option in FY 2016 (Connecticut, New York and Washington), while one state intends to implement Section 1915(k) in FY 2017 (Wyoming).
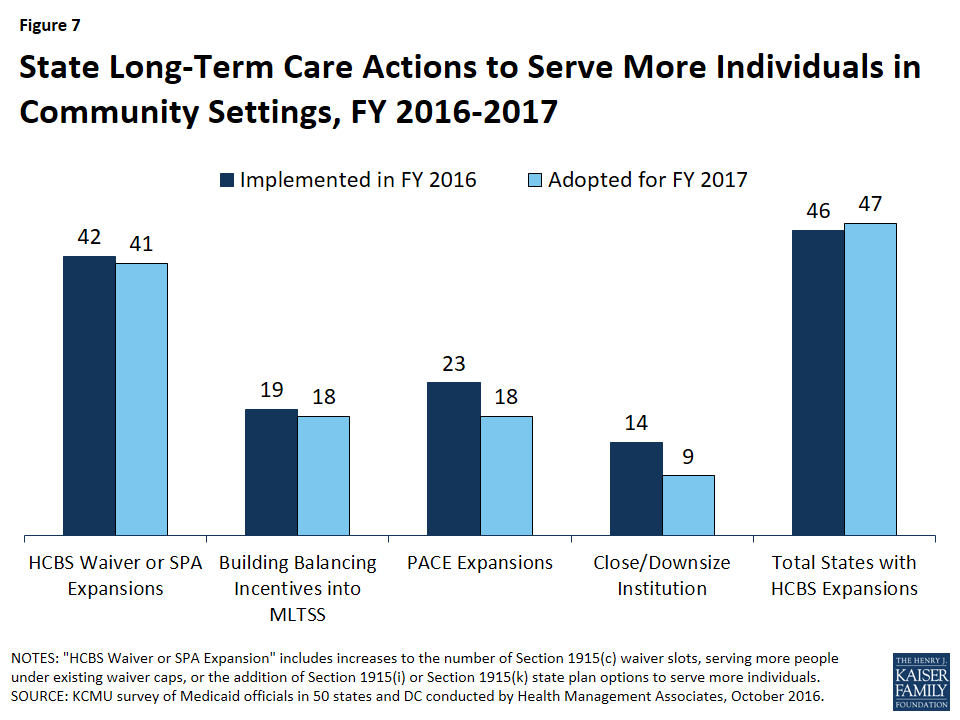
Figure 7: State Long-Term Care Actions to Serve More Individuals in Community Settings, FY 2016-2017
Several states are also using MLTSS strategies intended to serve more individuals in home and community-based settings. Nineteen (19) states in FY 2016 and 18 states in FY 2017 report they include or will include specific rebalancing incentives (performance targets and/or financial incentives) in managed care contracts to encourage MCOs that cover LTSS to expand access to HCBS. This includes a number of states that provide HCBS for some or all populations under Section 1115 waivers, in connection with MLTSS, instead of through Section 1915(c).4 For example, Tennessee, which transferred its Section 1915(c) waiver services for several LTSS populations to a Section 1115 waiver with its expansion to MLTSS in 2010 (TennCare CHOICES), reported that it expects to convert its remaining Section 1915(c) waiver for persons with intellectual and developmental disabilities to Section 1115 authority in FY 2017. The state anticipates significant expansion in HCBS capacity for this population under its managed care approach. See the MLTSS section below for more detail on the use of MLTSS in state Medicaid programs.
PACE continues to be reported as a rebalancing tool, with 23 states in FY 2016 and 18 states in FY 2017 expecting growth in these programs. For most of these states, growth will come within existing PACE sites; however, Florida, New Jersey, Rhode Island, Texas, and Maryland reported that they expect to add at least one new PACE site.
Further, 14 states in FY 2016 and nine states in FY 2017 expect to close or downsize a state institution and transition residents into community settings. This strategy is still an important tool of rebalancing. In addition, both Indiana and Massachusetts imposed a moratorium on new nursing facility beds in FY 2016.
States were also asked if they have adopted or plan to adopt new restrictions on the number of people served in the community in FY 2016 or FY 2017. Two states (Missouri and North Carolina) reported that they were acting to restrict PACE programs. Missouri terminated its PACE site in FY 2016, and North Carolina, citing concern over the rate of growth in the program, placed a limit on the number of individuals each PACE site can enroll each month. Virginia reported that it intends to cap enrollment in its Alzheimer’s Assisted Living Section 1915(c) waiver, which currently serves 56 people and cannot meet the new CMS regulatory standards for home and community-based settings; a stakeholder group is meeting to formulate plans for individuals who are currently served under the waiver. While New Jersey is expanding HCBS through other initiatives, the state also increased the number of institutional LTSS beds in FY 2016; 60 additional long-term care beds for individuals who have Huntington Disease were approved by the New Jersey Department of Health in FY 2016.
Table 12 shows state use of LTSS rebalancing tools in FY 2016 and FY 2017.
Housing Supports
In June 2015, CMS issued an Informational Bulletin to clarify when and how Medicaid reimburses for certain housing-related activities, including individual housing transition services, individual housing and tenancy sustaining services, and state-level housing related collaborative activities.5 CMS’s intent was to assist states in designing benefits that support community integration for seniors, individuals with disabilities, and individuals experiencing chronic homelessness.
Many of the services outlined in CMS’s Informational Bulletin were developed under the auspices of federal grant programs, including the Money Follows the Person (MFP) rebalancing demonstration. MFP is a federal grant program, enacted under the Deficit Reduction Act of 2005 and extended through September 2016 by the Affordable Care Act, which operates in 44 states. Enhanced federal funding under MFP has supported the transition of over 52,000 individuals from institutional to home and community-based settings of LTSS as of mid-2015.6 Under MFP, states identified the lack of affordable and accessible housing as a major barrier to assisting individuals to leave institutional settings of care. With MFP resources, many states have offered new housing related services, incorporated housing expertise within the Medicaid program to increase the likelihood of successful community living for persons who need supports, and engaged in strategic activities to assist in identifying and securing housing resources for individuals who choose HCBS.
After September 2016, states can continue to transition individuals under MFP through 2018 (with CMS approval) and have through 2020 to use their remaining funding.7 As of July 2016, 23 states reported that they currently offer housing-related services under a state plan, Section 1915(c), or 1115 waiver authority that the state intends to continue after the expiration of the MFP grant program. Most of these states are using current Section 1915(c) waivers that provide community transition services and environmental modifications for seniors, individuals with physical disabilities and/or individuals with intellectual or developmental disabilities. Other states, including Alabama, Kansas, Massachusetts, Michigan, and Ohio, plan to continue to offer housing coordinators or other search services to assist waiver beneficiaries. States have noted that some demonstration services and program supports will terminate when MFP funding expires.
Beyond MFP, 16 states reported that they have or will implement or expand housing-related services, as outlined in the Informational Bulletin, in FY 2016 or FY 2017; one state has done so in 2016, eight states plan to do so in 2017, and seven states plan to implement or expand housing-related services in both years (Exhibit 7). States report planning to use an array of authorities, in addition to Section 1915(c) waivers, for offering housing related services. For example, the District of Columbia proposes to offer health home services that support links to housing, and California proposes to offer housing-related services using a health home-based Whole Person Care Pilot under a Section 1115 waiver. New Jersey plans to use a Section 1115 waiver to offer a supported housing benefit to a wide range of Medicaid beneficiaries, including people who are homeless, at-risk of homelessness, residing in nursing facilities, are jail involved, or have a behavioral health diagnosis. Connecticut proposes to provide transition supports and tenancy sustaining supports using a Section 1915(i) State Plan Amendment. Under its Section 1115 waiver, Washington plans to provide supportive housing services (including individual housing transition services and individual tenancy sustaining services) to Medicaid beneficiaries age 18 or older who meet HUD’s definition of “chronically homeless” or have frequent or lengthy institutional contacts or adult residential care stays or have frequent in-home caregiver/provider turnover or meet specific risk criteria.8
| Exhibit 7: States Implementing or Expanding Housing-related Services Outlined in the CMS Informational Bulletin | ||
| FY 2016 only | FY 2017 only | both FY 2016 and FY 2017 |
| OH | CT, DC, DE, FL, HI, NJ, RI, VT | CA, LA, MA, NC, OK, TN, WA |
HCBS Benefit Changes
Ten (10) states in FY 2016 and 14 states in FY 2017 reported a wide variety of HCBS benefit additions or expansions. HCBS benefits include those in Section 1915(c) waivers, Section 1915(i) authority, Section 1915(k) authority (known as “Community First Choice” or “CFC”), and State Plan personal care services, home health services and private duty nursing (Exhibit 8).9 For example, three states in FY 2016 (Connecticut, New York, and Washington) and one in FY 2017 (Wyoming) reported implementing or planning to implement CFC and one state (Texas) reported enhancing its CFC benefit in FY 2016 to add transportation and respite services for persons with intellectual and developmental disabilities; one state in FY 2016 (Texas) and two in FY 2017 (Florida and South Carolina) reported behavioral health-related HCBS service additions; two states (Colorado and DC) reported increasing access to consumer directed service options in FY 2016; two states (Pennsylvania and Tennessee ) reported employment services expansions in FY 2017 and one state (Wisconsin) reported adding consultative and therapeutic services for caregivers and training services for unpaid caregivers in FY 2016.
HCBS benefit restrictions reflect the elimination of a covered benefit or the application of utilization controls for existing benefits. For FY 2016, West Virginia applied service limitations in its home and community-based services waiver serving persons with intellectual and developmental disabilities and eliminated a benefit in two other HCBS waivers. For FY 2017, Tennessee is limiting coverage for facility-based day services (Exhibit 8).
| Exhibit 8: HCBS Benefit Enhancements or Additions and Restrictions or Eliminations | ||
| Benefit | FY 2016 | FY 2017 |
| HCBS Enhancements or Additions | CA, CO, CT, DC, MS, MT, NY, TX, WA, WI | CT, DC, FL, ID, IN, KY, MA, MN, MT, PA, SC, SD, TN, WY |
| HCBS Restrictions or Eliminations | WV | TN |
Capitated Managed Long-Term Services and Supports (MLTSS)
As of July 1, 2016, almost half of states (23 states) covered LTSS through one or more of three types of capitated managed care arrangements: a Medicaid MCO (covering Medicaid acute care and LTSS), a PHP (covering only Medicaid LTSS), or an MCO arrangement for dually eligible beneficiaries (covering Medicaid and Medicare acute care and Medicaid LTSS services in a single contract, under the financial alignment demonstration for dual eligibles). Of the 23 states that reported using one or more of these MLTSS models, eight states reported using two models, and one state (New York) reported using all three. Among states with MLTSS arrangements, 18 states offer a Medicaid MCO that covers both Medicaid acute services and Medicaid LTSS. (Michigan, South Carolina, and Virginia are not among these 18 states; however, they use Medicaid MCOs that cover Medicaid acute and Medicaid LTSS (as well as Medicare acute care) in financial alignment demonstration (FAD) initiatives for duals.) Just five states reported offering a Medicaid LTSS PHP. Of the states with capitated MLTSS, 15 offered some form of managed care plan on a statewide basis for at least some LTSS populations as of July 1, 2016.
Nine states offered an MCO-based FAD (California, Illinois, Massachusetts, Michigan, New York, Ohio, South Carolina, Texas, and Virginia) as of July 1, 2016.10 The FAD model involves a three-way contract between an MCO, Medicare and the state Medicaid program.11,12 Two states reported new FAD initiatives: in FY 2016, New York launched a second FAD initiative, contracting with a managed care plan to serve dual eligibles with ID/DD, and Rhode Island is launching a FAD initiative in FY 2017. Massachusetts also operates an administrative alignment demonstration (without financial alignment) for dually eligible beneficiaries (Senior Care Options (SCO) program). Minnesota only operates an administrative alignment demonstration (without financial alignment) for dually eligible beneficiaries (Minnesota Senior Health Options program).
Other states not participating in a formal demonstration have taken action to encourage improved coordination and integration of services for the dually eligible population under MCO arrangements. Five states (Arizona, Hawaii, Minnesota, Tennessee, and Wisconsin) reported that they require Medicaid-contracting MCOs to also offer a Medicare Dual Eligible Special Needs Plan (D-SNP)13 to allow a beneficiary to choose to receive Medicare as well as Medicaid benefits from the same plan (though not through a single contract). Florida contracts for MLTSS with MCOs that are chronic disease SNPs14 for dually eligible beneficiaries. New Jersey and Idaho reported that at least one plan in each state is a Fully Integrated Dual Eligible (FIDE) SNP,15 which allows beneficiaries to choose a single MCO to offer both Medicare and Medicaid benefits, creating an opportunity for improved coordination and integration.
Table 13 provides state-level details on MLTSS models.
MLTSS Enrollment
This year’s survey also asked states with capitated MLTSS arrangements whether, as of July 1, 2016, certain populations were enrolled on a mandatory or voluntary basis or were always excluded. On the survey, states selected from “always mandatory,” “always voluntary,” “varies (by geography or other factor),” or “always excluded” for the following populations: seniors, persons with ID/DD, non-elderly adults with physical disabilities, and full-benefit dually eligible beneficiaries. As shown in Exhibit 9 below, seniors were most likely to be enrolled on a mandatory basis statewide (13 states), while persons with ID/DD were least likely to be enrolled on a mandatory basis (8 states) and also most likely to be excluded from MLTSS enrollment (4 states). No state with a MLTSS program always excludes individuals who have full dual eligibility status from enrollment.
| Exhibit 9: MLTSS Enrollment by Populations, July 1, 2016 (# of States) |
||||
| Seniors | Persons with ID/DD | Nonelderly Adults with Physical Disabilities | Full Benefit Dual Eligibles | |
| Always mandatory | 13 | 8 | 12 | 9 |
| Always voluntary | 5 | 6 | 4 | 7 |
| Varies (by geography or other factor) | 4 | 5 | 4 | 7 |
| Always excluded | 1 | 4 | 3 | 0 |
MLTSS Benefits
Almost every MLTSS state (22 states) includes both institutional and HCBS in the same contractual arrangement, though this sometimes varies within a state across populations. For example, Minnesota offers both institutional and HCBS in the same MCO for seniors, but only institutional LTSS are included in an MCO for individuals with disabilities who are under the age of 65. One state (North Carolina) reported covering only HCBS in its MLTSS program for persons with intellectual and developmental disabilities.
MLTSS Population Changes
The growth in the use of MLTSS has continued since the prior survey reporting period. In FY 2015, six states (California, Michigan, New Jersey, New York, South Carolina, and Texas) implemented MCO arrangements for LTSS for at least some populations, some of these in conjunction with implementing a FAD. In FY 2016, four states implemented or expanded MLTSS to new parts of the state, while four states expanded MLTSS to new populations. South Carolina and Wisconsin anticipate geographic expansion in MLTSS in FY 2017, while five states anticipate adding populations to MLTSS in FY 2017 (Exhibit 10).
| Exhibit 10: MLTSS Population Expansions, FY 2016 and FY 2017 | ||
| FY 2016 | FY 2017 | |
| Geographic Expansions | IA, ID, SC, WI | SC, WI |
| New Population Groups Added | IA, NJ, NY, SC | IL, NY, SC, TN, TX |
Only two states reported any reduction in the use of MLTSS. Massachusetts imposed a temporary cap on enrollment in OneCare (its FAD model) in FY 2016, but that cap was subsequently lifted. Idaho noted that its one MLTSS PHP is expected to reduce its service plan area in FY 2017.
MLTSS Quality
Most states with MCO programs track state-identified quality measures and require other health plan quality-related activities to improve health care outcomes and plan performance under MLTSS. Thirteen (13) states with MCOs offering LTSS reported having LTSS quality measures in place in FY 2015. In FY 2016, a total of six states implemented new or expanded MLTSS quality measures, bringing the total to 15 states. Five of these 15 states plan to expand quality measures for LTSS in FY 2017. See Exhibit 11 for information on states with quality measures for MLTSS.
CMS has identified a gap in the national availability of tested, reliable and valid quality measures for HCBS. A variety of efforts are underway to address this gap. The US Department of Health and Human Services has contracted with the National Quality Forum to create a conceptual framework for HCBS quality measurement; to synthesize existing evidence, measures, and measure concepts; to identify gaps in HCBS measures based on the framework; and to make recommendations for HCBS measure development efforts.16 17
| Exhibit 11: MLTSS Quality Measures, FY 2015, FY 2016, and FY 2017 | ||
| In Place FY 2015 | New/Expanded FY 2016 | New/Expanded FY 2017 |
| AZ, CA, DE, FL, IL, KS, MA, MN, NM, OH, TN, TX, VA |
AZ, CA, DE, IA, NJ, VA | AZ, CA, DE, TX, VA |
Table 12: Long-Term Care Expansions in All 50 States and DC, FY 2016 and FY 2017
| States | Waiver or SPA Expansions | Building Balancing Incentives in MLTSS | PACE Expansions | Downsize/Close Institution | Total States with HCBS Expansions | |||||
| 2016 | 2017 | 2016 | 2017 | 2016 | 2017 | 2016 | 2017 | 2016 | 2017 | |
| Alabama | X | X | X | X | ||||||
| Alaska | ||||||||||
| Arizona | X | X | X | X | ||||||
| Arkansas | X | X | X | X | X | X | ||||
| California | X | X | X | X | X | X | X | X | X | X |
| Colorado | X | X | X | X | X | X | ||||
| Connecticut | X | X | X | X | X | X | ||||
| Delaware | X | X | X | X | X | X | X | X | X | |
| DC | X | X | X | X | ||||||
| Florida | X | X | X | X | X | X | X | X | ||
| Georgia | X | X | ||||||||
| Hawaii | X | X | X | X | ||||||
| Idaho | X | X | X | X | ||||||
| Illinois | X | X | X | X | X | X | ||||
| Indiana | X | X | X | X | X | X | ||||
| Iowa | X | X | X | X | X | X | X | |||
| Kansas | X | X | X | X | X | X | ||||
| Kentucky | X | X | ||||||||
| Louisiana | ||||||||||
| Maine | X | X | X | X | ||||||
| Maryland | X | X | X | X | ||||||
| Massachusetts | X | X | X | X | X | X | X | X | ||
| Michigan | X | X | X | X | X | X | X | X | ||
| Minnesota | X | X | X | X | ||||||
| Mississippi | X | X | X | X | X | X | X | |||
| Missouri | X | X | X | X | ||||||
| Montana | X | X | X | X | X | X | ||||
| Nebraska | X | X | X | X | ||||||
| Nevada | X | X | X | X | ||||||
| New Hampshire | X | X | X | X | ||||||
| New Jersey | X | X | X | X | X | |||||
| New Mexico | X | X | X | X | ||||||
| New York | X | X | X | X | X | X | X | X | X | |
| North Carolina | X | X | X | |||||||
| North Dakota | X | X | X | X | X | |||||
| Ohio | X | X | X | X | X | X | ||||
| Oklahoma | X | X | X | X | X | X | ||||
| Oregon | X | X | X | X | X | X | ||||
| Pennsylvania | X | X | X | X | X | X | X | X | X | |
| Rhode Island | X | X | X | X | X | X | X | X | ||
| South Carolina | X | X | X | X | X | X | X | |||
| South Dakota | X | X | X | X | ||||||
| Tennessee | X | X | X | X | X | X | X | X | ||
| Texas | X | X | X | X | X | X | X | X | X | X |
| Utah | X | X | X | X | ||||||
| Vermont | ||||||||||
| Virginia | X | X | X | X | X | X | X | X | X | X |
| Washington | X | X | X | X | X | X | ||||
| West Virginia | X | X | X | X | ||||||
| Wisconsin | X | X | X | X | X | X | ||||
| Wyoming | X | X | X | X | X | X | ||||
| Totals | 42 | 41 | 19 | 18 | 23 | 18 | 14 | 9 | 46 | 47 |
| NOTES: “HCBS Waiver or SPA Expansions” include increases to the number of Section 1915(c) waiver slots, serving more people under existing waiver caps, or the addition of Section 1915(i) or Section 1915(k) state plan options to serve more individuals. In addition to the actions reported here, two states (IN and MA) also reported imposing a moratorium on construction of new nursing facility beds in FY 2016. SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2016. |
||||||||||
Table 13: Capitated MLTSS Models in all 50 States and DC, as of July 1, 2016
| States | Medicaid MCO | PHP | Medicare + Medicaid Demonstration | Any MLTSS | Statewide |
| Alabama | |||||
| Alaska | |||||
| Arizona | X | X | X | ||
| Arkansas | |||||
| California | X | X | X | ||
| Colorado | |||||
| Connecticut | |||||
| Delaware | X | X | X | ||
| DC | |||||
| Florida | X | X | X | ||
| Georgia | |||||
| Hawaii | X | X | X | ||
| Idaho | X | X | |||
| Illinois | X | X | X | ||
| Indiana | |||||
| Iowa | X | X | X | ||
| Kansas | X | X | X | ||
| Kentucky | |||||
| Louisiana | |||||
| Maine | |||||
| Maryland | |||||
| Massachusetts | X | X* | X | ||
| Michigan | X | X | X | X | |
| Minnesota | X | X* | X | X | |
| Mississippi | |||||
| Missouri | |||||
| Montana | |||||
| Nebraska | |||||
| Nevada | |||||
| New Hampshire | |||||
| New Jersey | X | X | X | ||
| New Mexico | X | X | X | ||
| New York | X | X | X | X | X |
| North Carolina | X | X | X | ||
| North Dakota | |||||
| Ohio* | X | X | X | ||
| Oklahoma | |||||
| Oregon | |||||
| Pennsylvania | |||||
| Rhode Island* | X | X | X | ||
| South Carolina | X | X | |||
| South Dakota | |||||
| Tennessee | X | X | X | ||
| Texas | X | X | X | X | |
| Utah | |||||
| Vermont | |||||
| Virginia | X | X | |||
| Washington | |||||
| West Virginia | |||||
| Wisconsin | X | X | X | ||
| Wyoming | |||||
| Totals | 18 | 5 | 10 | 23 | 15 |
| NOTES: States were asked whether they cover long-term services supports through any of the following managed care (capitated) arrangements as of July 1, 2016: Medicaid MCO (MCO covers Medicaid acute + Medicaid LTSS); PHP (covers only Medicaid LTSS); or Medicare + Medicaid Demonstration (Medicaid MCO covers Medicaid and Medicare acute + Medicaid LTSS). “Medicare + Medicaid Demonstration” – these states use Medicaid MCOs in Financial Alignment Demonstration (FAD) initiatives which involve care coordination for dually eligible beneficiaries. States were also asked whether MLTSS plans were operating in all regions of the state as of July 1, 2015 (statewide). *MA operates a FAD and another administrative alignment demonstration for dually eligible beneficiaries. *MN operates an administrative alignment demonstration (without financial alignment) for dually eligible beneficiaries. *RI is launching a FAD initiative in FY 2017. *OH offers a Medicaid MCO (MCO offers Medicaid acute + Medicaid LTSS) only in those counties where the FAD is offered; dually eligible seniors who opt out of the FAD must enroll in this Medicaid MCO model for Medicaid services. SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2016. |
|||||

Sections
Also of Interest
- The 16th Annual Kaiser 50-State Medicaid Budget Survey: Slowing Growth and Evolving Policies at a Forum with the National Association of Medicaid Directors
- Medicaid Enrollment & Spending Growth: FY 2016 & 2017
- Putting Medicaid in the Larger Budget Context: An In-Depth Look at Four States in FY 2016 and FY 2017
- 50-State Medicaid Budget Survey Archives