Assessing Equity in PEPFAR Countries: Analysis of HIV Outcomes by Urban/Rural Residence, Wealth, Sex, and Age
PEPFAR, the U.S. global HIV program, is the largest commitment by any nation to address a single disease in history. As the program increasingly focuses on sustainability for the future, a key pillar of its current five year strategy is equity, defined by the program as a “fair and just opportunity for everyone to achieve their highest level of health”. More broadly, a focus on equity has long been a part of the HIV response,1 often serving as a model for global health and development efforts more generally. Still, disparities in HIV access and outcomes persist and the stakes have increased in recent years, with a growing HIV funding gap and other financial pressures, deteriorating human rights environment, and shrinking space for civil society, among other challenges.2,3 Better understanding how equitable the HIV response has been, and where equity gaps remain, can aid policymakers and program implementers in mitigating gaps and guiding PEPFAR’s future directions.
This analysis, adapted from a recent report, examines differences in HIV outcomes by urban/rural residence, wealth quintile, sex and age. Three HIV outcomes were examined: the share of people living with HIV who are aware of their HIV status, the share on antiretroviral treatment, and the share virally suppressed. Data were obtained from Population-based HIV Impact Assessment (PHIA) Project surveys, nationally representative household surveys of adults and adolescents aged 15 and older that have been completed in 15 PEPFAR countries. Changes over time were assessed in six countries with follow-up surveys (see methodology for more detail). While the demographic data examined here are important for assessing equity, PHIA surveys do not currently collect data on other subpopulation groups that also face equity challenges, particularly key populations –men who have sex with men, people who are transgender, sex workers, and people who inject drugs – who, as documented in a recent analysis, continue to be disproportionately impacted by HIV and experience poorer health outcomes.
Overall, this analysis finds that in the 15 PEPFAR countries analyzed, HIV equity gaps were found for some, but not all, subpopulation groups. In addition, some groups that generally have poorer health outcomes, such as those in rural areas and those with lower incomes, had better HIV outcomes than their counterparts in several countries. Finally, HIV outcomes improved across all groups and countries over time, and equity gaps narrowed in several cases. These findings point to areas where resources and attention can be directed to further reduce HIV equity gaps, and also identify examples of HIV “equity successes,” which may offer lessons going forward.
Key Take-Aways
- People living with HIV in rural areas were more likely to be on antiretroviral treatment and be virally suppressed in a greater number of PEPFAR countries than those in urban areas. For example, in seven countries, viral suppression rates in rural areas were better than in urban areas, compared to four countries where the opposite was found. In three countries, there were no differences.
- While people with HIV in the highest wealth quintile had better HIV outcomes than those in the lowest in eight PEPFAR countries, in five countries, the opposite was found and in two countries, there were no differences.
- There was a significant outcome gap by sex, with males faring more poorly than their female counterparts in all 15 PEPFAR countries and for all three HIV outcomes.
- There was also a significant gap by age in all 15 countries, with younger cohorts having poorer HIV outcomes across the board and in many cases, the differences were quite large and greater than for any other subpopulation examined.
- Over time, HIV outcomes improved across all groups in the six PEPFAR countries that have conducted two surveys. In addition, disparities narrowed in several cases, particularly by sex and age.
Findings
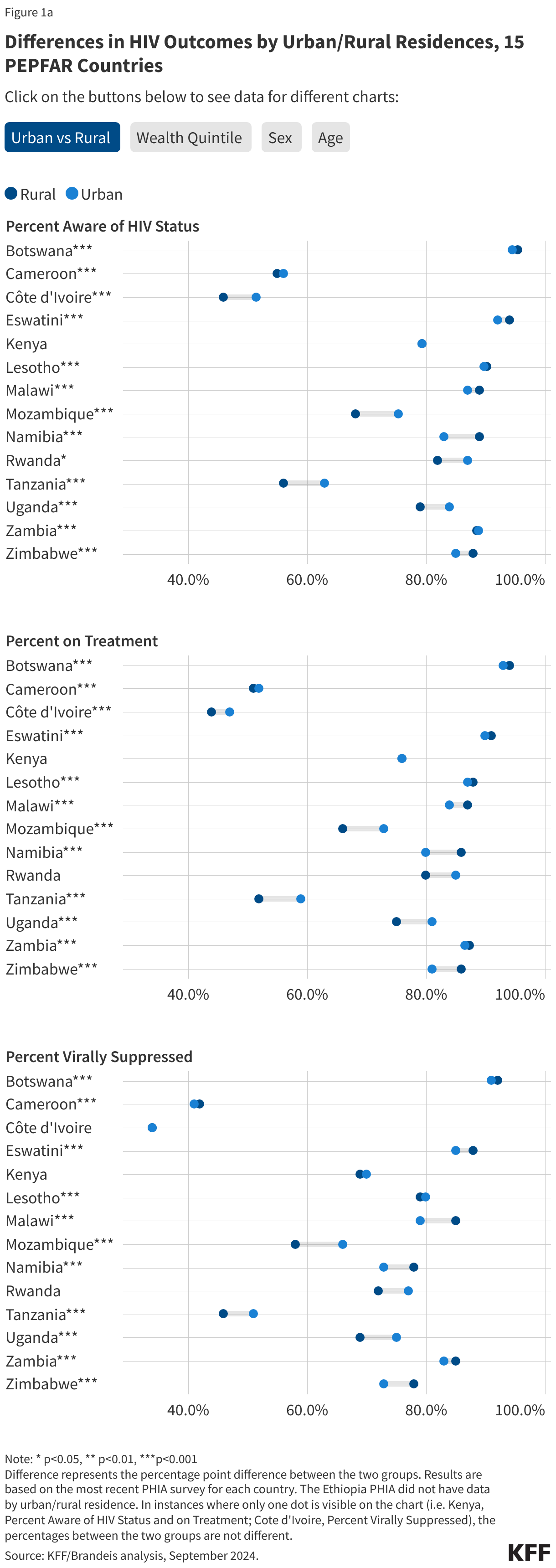
People with HIV in rural areas were more likely to be on antiretroviral treatment and be virally suppressed in a greater number of PEPFAR countries than those in urban areas. Differences, while significant, were generally small4 (see Figure 1a and Appendix Table 1).
- In six countries (Botswana, Eswatini, Lesotho, Malawi, Namibia, and Zimbabwe), people with HIV in rural areas had greater awareness of their HIV status than those in urban areas and in one country (Kenya), there was no difference. In seven countries (Cameroon, Côte d’Ivoire, Mozambique, Rwanda, Tanzania, Zambia, and Uganda) people with HIV in urban areas had greater HIV awareness.
- In seven countries, there were greater shares of people with HIV on antiretroviral treatment in rural areas (Botswana, Eswatini, Lesotho, Malawi, Namibia, Zambia and Zimbabwe) and in two countries (Kenya and Rwanda) there were no significant differences. Five countries (Cameroon, Côte d’Ivoire, Mozambique, Tanzania and Uganda) had higher shares on treatment in urban areas.
- Finally, seven countries (Botswana, Cameroon, Eswatini, Malawi, Namibia, Zambia and Zimbabwe) had higher HIV viral suppression rates among rural populations with HIV, and three countries (Côte d’Ivoire, Kenya and Rwanda) had no significant differences between rural and urban residents. Four had higher rates among urban populations (Lesotho, Mozambique, Tanzania, and Uganda).
- With few exceptions, the differences between rural and urban groups were five percentage points or less.
While people with HIV in the highest wealth quintile had better HIV outcomes than those in the lowest in a greater number of PEPFAR countries, in several countries, the opposite was found (see Figure 1b and Appendix Table 2).
- In eight of the 15 PEPFAR countries, people with HIV in the highest wealth quintile had better HIV awareness, treatment, and viral load suppression outcomes than those in the lowest wealth quintile (Cameroon, Ethiopia, Lesotho, Malawi, Mozambique, Tanzania, Uganda and Zambia) while in five countries (Botswana, Côte d’Ivoire, Eswatini, Namibia, and Zimbabwe), these outcomes were better among those in the lowest wealth quintile. Two countries—Kenya and Rwanda—showed no significant differences in outcomes between the lowest and highest wealth quintiles.
- Differences between groups ranged by country and in some cases were large. For example, the difference between the lowest and highest wealth quintiles in viral suppression rates was 10 percentage points or greater in seven countries (Cameroon, Côte d’Ivoire, Ethiopia, Mozambique, Namibia, Tanzania, and Uganda).
There was a significant disparity by sex, with males faring more poorly than their female counterparts in all 15 PEPFAR countries and for all three HIV outcomes (see Figure 1c and Appendix Table 3).
- In all 15 countries, males were significantly less likely to be aware of their HIV status, on antiretroviral therapy, or virally suppressed than females, and some countries, these equity gaps were 10 percentage points or higher.
- The gap in awareness of HIV status was 10 percentage points or higher in four countries (Côte d’Ivoire, Kenya, Ethiopia, and Tanzania).
- In five countries, there was at least a 10 percentage point gap in the share of males on antiretroviral treatment compared to females (Côte d’Ivoire, Ethiopia, Kenya, Namibia, and Tanzania).
- Similarly, the gap in the share virally suppressed was at least 10 percentage points in five countries (Côte d’Ivoire, Kenya, Namibia, Rwanda, and Tanzania).
There was also a significant gap by age in all 15 PEPFAR countries, with younger cohorts having poorer HIV outcomes across the board; in most cases, differences were quite large and greater than for any other subpopulation examined (see Figure 1d and Appendix Table 4).
- In all 15 countries, young people (ages 15-24) were significantly less likely to be aware of their HIV status, on antiretroviral therapy, and virally suppressed than those ages 25 and older and the equity gaps between age cohorts were greater than for other groups examined.
- The equity gap for awareness of HIV status and in antiretroviral treatment coverage was at least 20 percentage points in three countries (Cameroon, Mozambique, and Uganda).
- The gap in the share virally suppressed was at least 20 percentage points in five countries (Cameroon, Ethiopia, Mozambique, Uganda, and Zimbabwe).
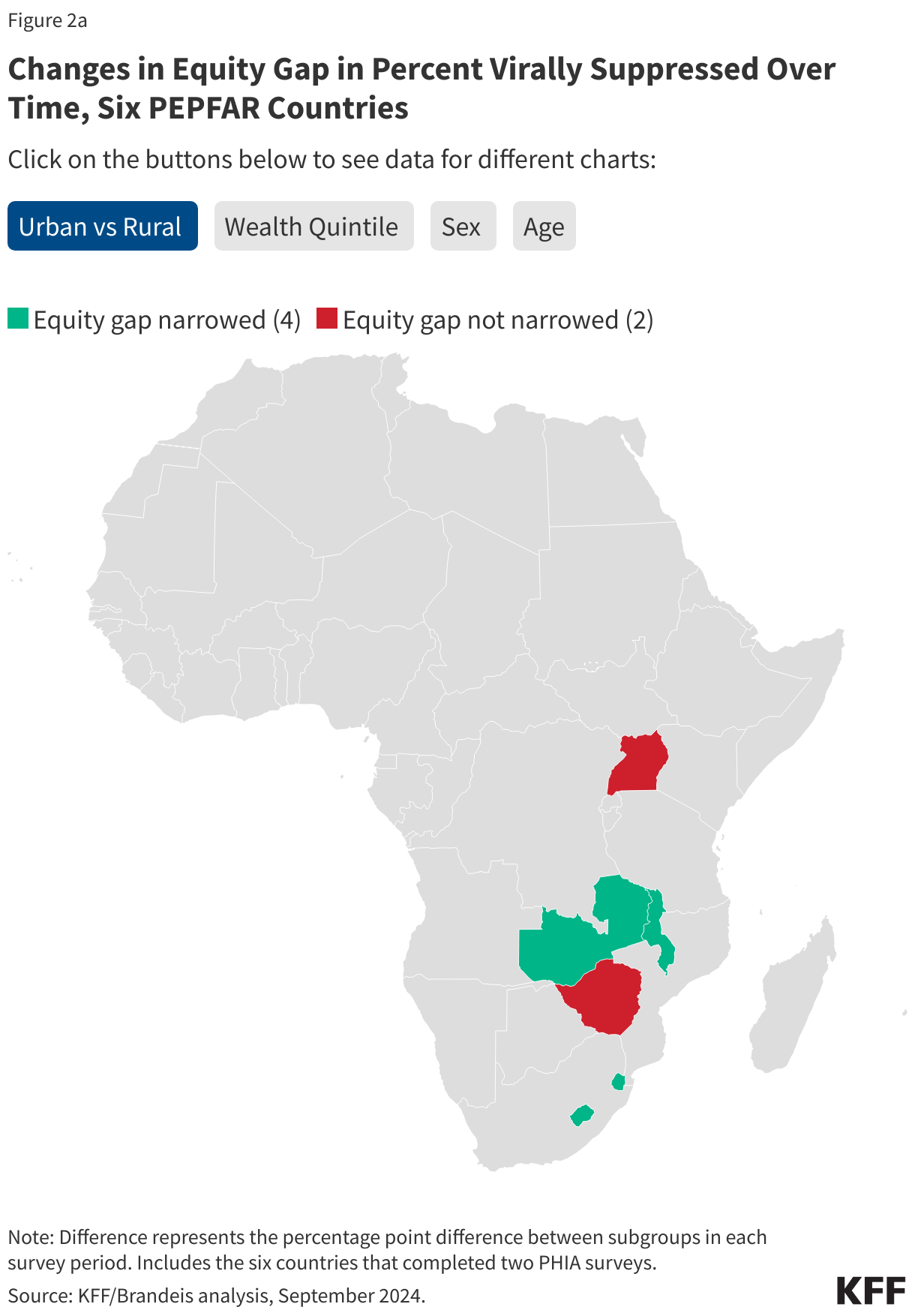
Over time, HIV outcomes improved across all groups in the six PEPFAR countries that completed two surveys. In addition, equity gaps narrowed in several cases, particularly by sex and age (see Figures 2a-d and Appendix Tables 5-6).
- Awareness of HIV status increased significantly for both urban and rural residents with HIV in each of the six countries. Increases were steepest for viral suppression rates. In three countries (Eswatini, Malawi, and Zambia), the equity gap between rural and urban residents narrowed across all three HIV outcomes, and the gap in viral suppression rates decreased in Zambia. Conversely, while overall outcomes improved, the gap between groups grew in Uganda and Zimbabwe.
- Both those in the highest and lowest wealth quintiles had increases in all HIV outcomes over time, particularly for viral suppression rates. Two countries (Eswatini and Zambia) narrowed the equity gap by wealth for all three HIV outcomes, and the gap narrowed for Lesotho for awareness of HIV status and treatment coverage and in Malawi for treatment coverage. The gap grew, however, in Uganda and Zimbabwe for all three HIV outcomes.
- Outcomes improved for females and males in all six countries, with the steepest improvements in viral suppression rates. In addition, the gap between males and females narrowed in all cases, except in Zambia where the disparity only narrowed for viral suppression rates.
- Finally, HIV outcomes also improved for both age cohorts and the equity gap narrowed in almost all cases (with the exception of viral suppression rates in Uganda, where the gap remained approximately the same, and in Zimbabwe, where the gap in viral suppression rates grew).
As this analysis shows, HIV equity gaps were found for some, but not all, groups examined in PEPFAR countries. It also finds that outcomes improved over time across the board and, in most cases, equity gaps narrowed. In addition to helping to identify areas in need of further resources and attention, these findings also point to examples of HIV equity successes, which could serve as models for other countries and populations. Future research could examine how equity was achieved in these countries, including the role played by PEPFAR funding and programming.
Methods |
| The analysis uses data from the Population-based HIV Impact Assessment (PHIA) Project, a series of cross-sectional, nationally representative household surveys funded by PEPFAR in PEPFAR countries, that are highly affected by HIV. To date, surveys have been completed in 15 PEPFAR countries with follow-up surveys done in six countries. Data from these countries were used to compare HIV outcomes among people living with HIV by the following characteristics available in the PHIA data: urban/rural residence, wealth quintile, sex, and age. Three HIV outcome measures were compared across groups: the share of people with HIV aware of their HIV status, share on antiretroviral treatment, and share virally suppressed. To measure equity, mean HIV outcome levels by subpopulation were compared. Statistical significance was assessed by performing Chi-squared and Fisher’s exact tests. Because surveys were conducted at different time periods by country, outcomes were not compared across countries in this analysis. It is important to note that findings from these 15 PEPFAR countries, or the six with follow-up data, may not be generalizable to other countries. In addition, while PHIA countries are PEPFAR countries, outcomes may not be attributable to PEPFAR alone, given that other funding sources and programs also support the HIV response. |