A National Survey of OBGYNs’ Experiences After Dobbs
Key Findings
Introduction
One year ago, the Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization overturned Roe v. Wade and opened the door for states to ban or severely restrict the availability of abortion care. Today, people seeking abortion in large swaths of the country must travel to other states to get abortion services or obtain medication abortion through self-managed or other means. In many states, abortion is not banned, but laws impose gestational limits and other restrictions that limit access to abortion. This has left large parts of the U.S., particularly in the South and Southeast, without meaningful abortion access. In the states where abortion remains available under most circumstances, abortion providers have had to take on additional patients traveling to their states to get an abortion. Furthermore, the situation in many states remains uncertain, with new bans being implemented that are often followed by legal challenges creating a complicated landscape to navigate for patients and clinicians, particularly those who provide services to pregnant people.
To understand the impact of the changing abortion landscape on clinical care, KFF conducted a nationally representative survey of office-based OBGYNs practicing in the United States who spend the majority of their working hours (60% or more) in direct patient care and provide sexual and reproductive health care to at least 10% of patients. The survey was fielded from March 17 to May 18, 2023, and responses were received from 569 OBGYNs. This survey examines the provision of sexual and reproductive health care provided by OBGYNs before and after the Dobbs decision, comparing the experiences of OBGYNs practicing in states where abortion is fully banned, states with gestational restrictions, and states where abortion remains available under most circumstances. All differences highlighted in the text of this report are statistically significant.
Key Findings
Abortion Access and Constraints on Care Since Dobbs
- Since the Dobbs decision, half of OBGYNs practicing in states where abortion is banned say they have had patients in their practice who were unable to obtain an abortion they sought. This is the case for one in four (24%) office-based OBGYNs nationally.
- Nationally, one in five office-based OBGYNs (20%) report they have personally felt constraints on their ability to provide care for miscarriages and other pregnancy-related medical emergencies since the Dobbs decision. In states where abortion is banned, this share rises to four in ten OBGYNs (40%).
- Four in ten OBGYNs nationally (44%), and six in ten practicing in states where abortion is banned or where there are gestational limits, say their decision-making autonomy has become worse since the Dobbs ruling. Over a third of OBGYNs nationally (36%), and half practicing in states where abortion is banned (55%) or where there are gestational limits (47%), say their ability to practice within the standard of care has become worse.
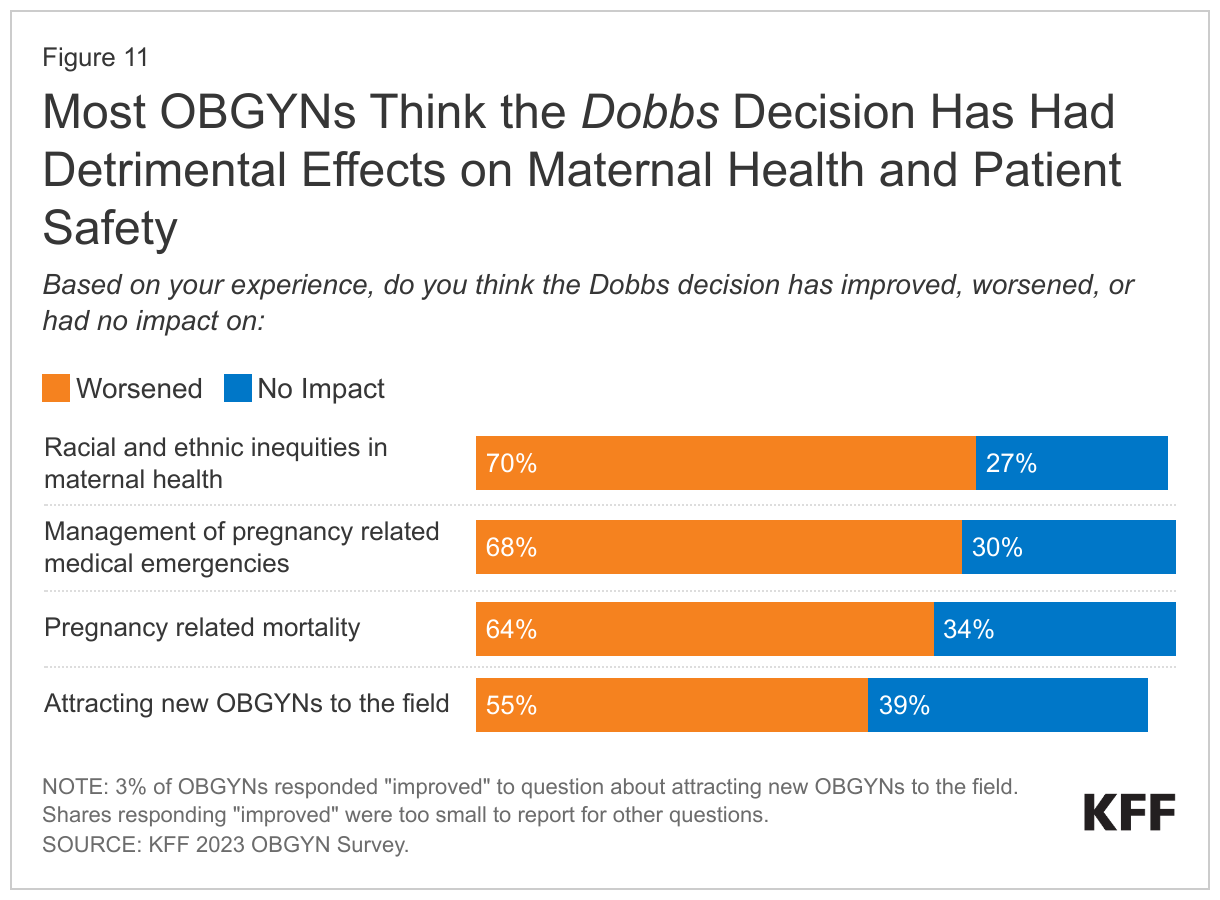
- Most OBGYNs (68%) say the ruling has worsened their ability to manage pregnancy-related emergencies. Large shares also believe that the Dobbs decision has worsened pregnancy-related mortality (64%), racial and ethnic inequities in maternal health (70%) and the ability to attract new OBGYNs to the field (55%).
Abortion Policies and Concern About Legal Risk
- Two-thirds of OBGYNs nationally (68%) say they understand the circumstances under which abortion is legal in the state they practice very well. However, among OBGYNs in states where abortion is restricted by gestational limits the share is lower (45%) compared to those practicing in states where abortion is available under most circumstances (79%) or banned (68%).
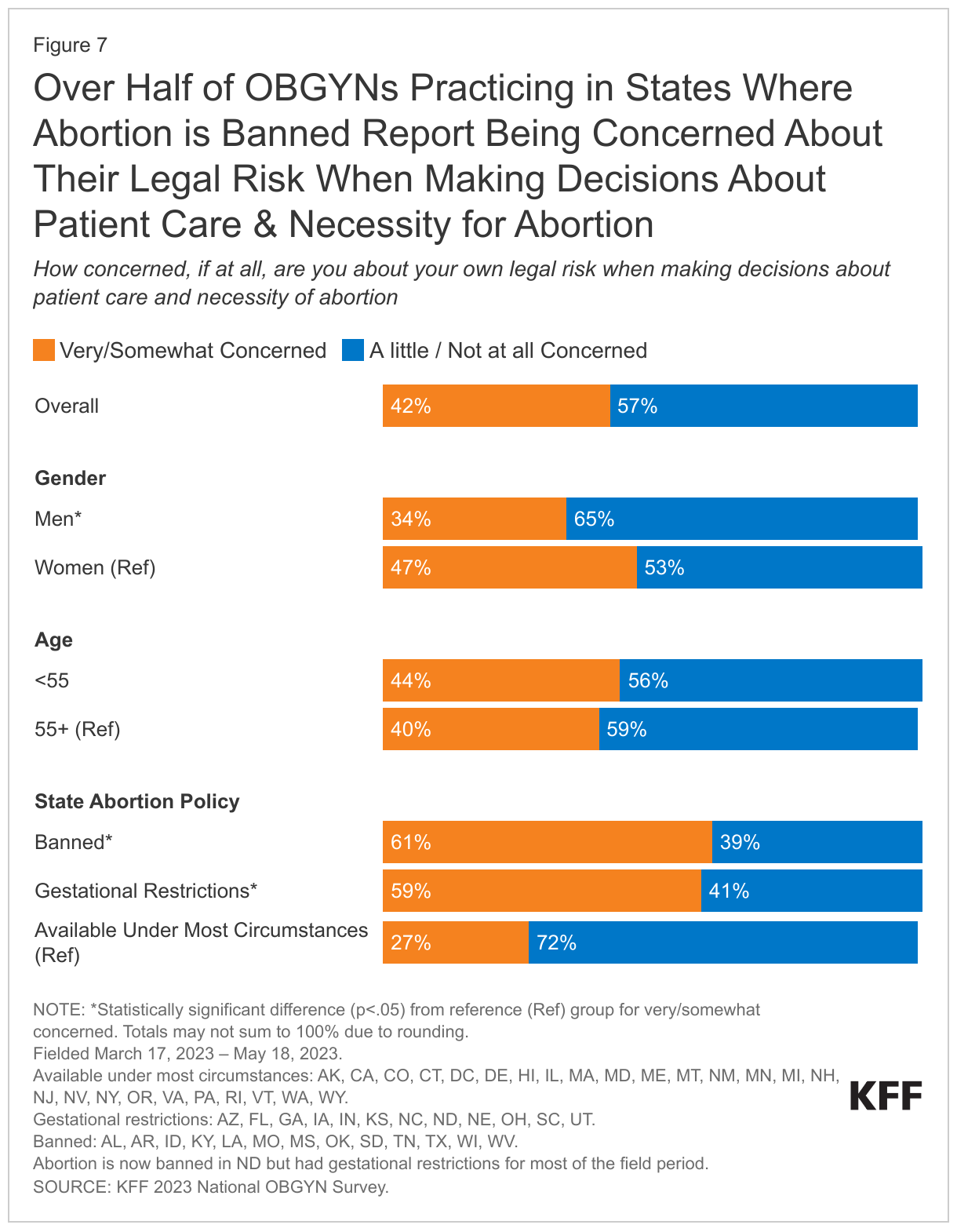
- Over four in ten (42%) OBGYNs report that they are very or somewhat concerned about their own legal risk when making decisions about patient care and the necessity of abortion. This rises to more than half of OBGYNs practicing in states with gestational limits (59%) and abortion bans (61%).
- Eight in ten OBGYNs approve of a recent policy change from the FDA that allows certified pharmacies to dispense medication abortion pills.
Abortion Services
- Nearly one in five (18%) officed-based OBGYNs nationally say that they are providing abortion services after the Dobbs About three in ten OBGYNs (29%) practicing in states where abortion is available under most circumstances offer abortion care, compared to just 10% in states with gestational restrictions. There were already large differences between states prior to the Supreme Court’s ruling. Many of the states that have abortion restrictions today had these or similar restrictions in place prior to the Dobbs decision.
- Nationally, 14% of OBGYNs say they provide in-person medication abortions, but only 5% say they provide telehealth medication abortions.
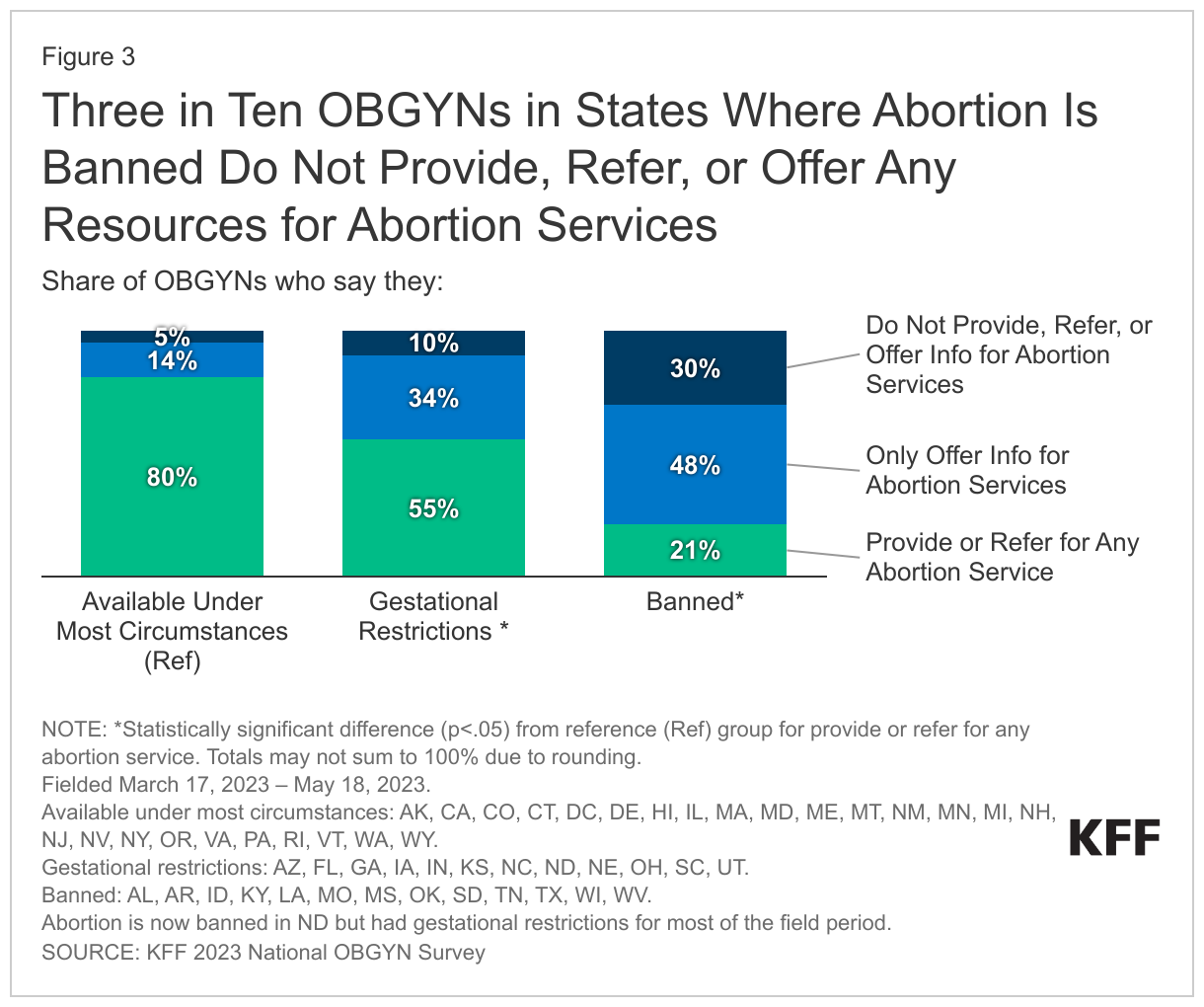
- In states where abortion is banned, essentially no OBGYNs offer abortions, except under very limited circumstances. Additionally, nearly half (48%) of OBGYNs in these states only offer information, such as online resources, to help patients seek out abortion services on their own, but 30% do not even offer their patients referrals to another clinician or any information about abortion.
Contraception
- More than half (55%) of OBGYNs nationally say they have seen an increase in the share of patients seeking some form of contraception since the Dobbs ruling, particularly sterilization (43%) and IUDs and implants (47%).
- Nearly all OBGYNs offer their patients some form of contraceptive care, but only 29% make all methods of contraception available to their patients, including all three methods of emergency contraception (copper intrauterine device (IUD), ulipristal acetate/Ella, and levonorgestrel/Plan B).
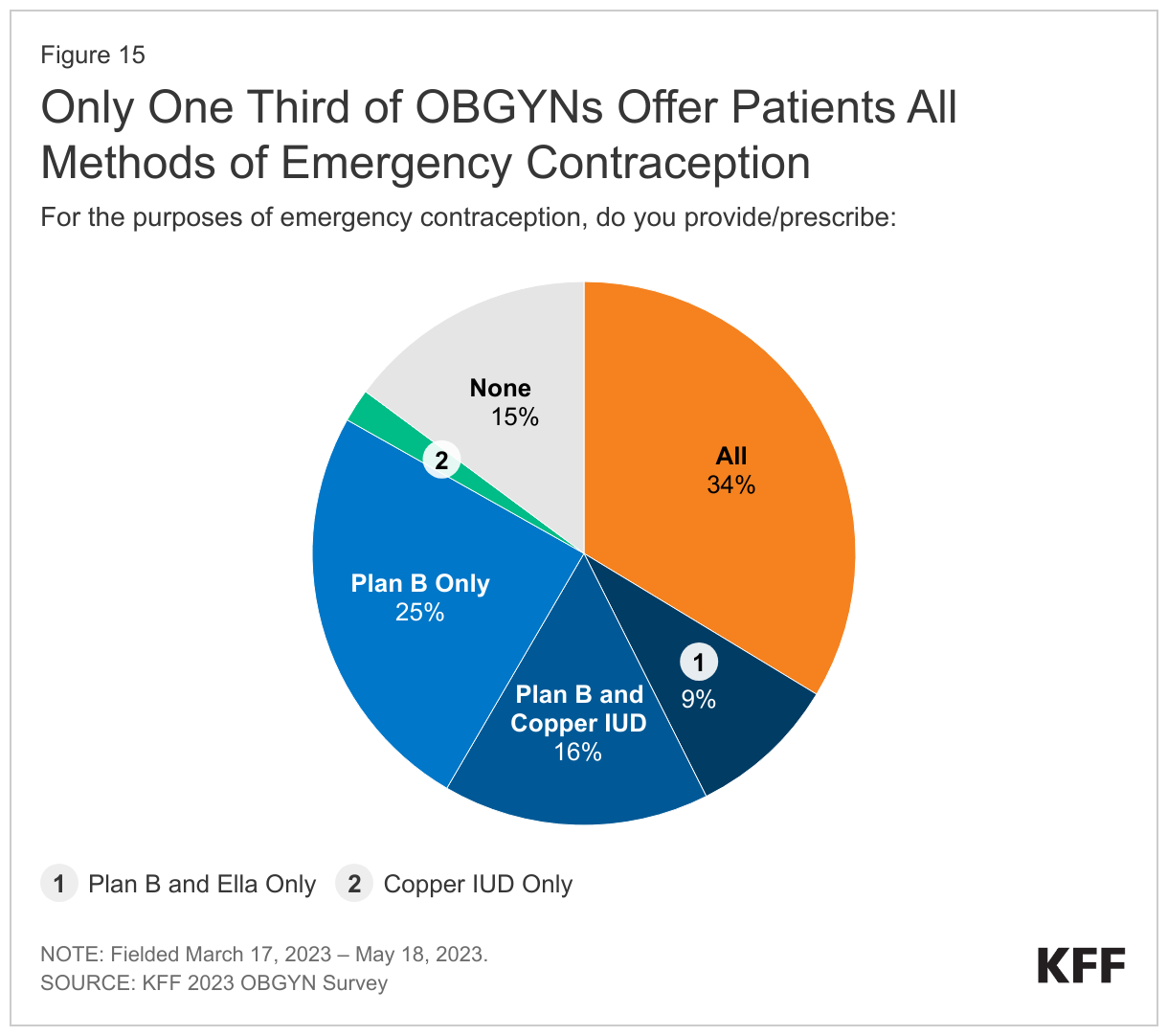
- Only one-third of OBGYNs (34%) prescribe or provide all three methods of emergency contraception and one in seven (15%) do not provide any methods of emergency contraception to their patients. A quarter of OBGYNS (25%) only prescribe or provide Plan B, which is available over the counter.
- Availability of care via telehealth expanded greatly after the onset of the COVID-19 pandemic. Today, almost seven in ten OBGYNs (69%) nationally say they provide at least some care via telehealth.
Report
Findings
ABORTION SERVICES
Provision of Abortion by U.S. OBGYNs
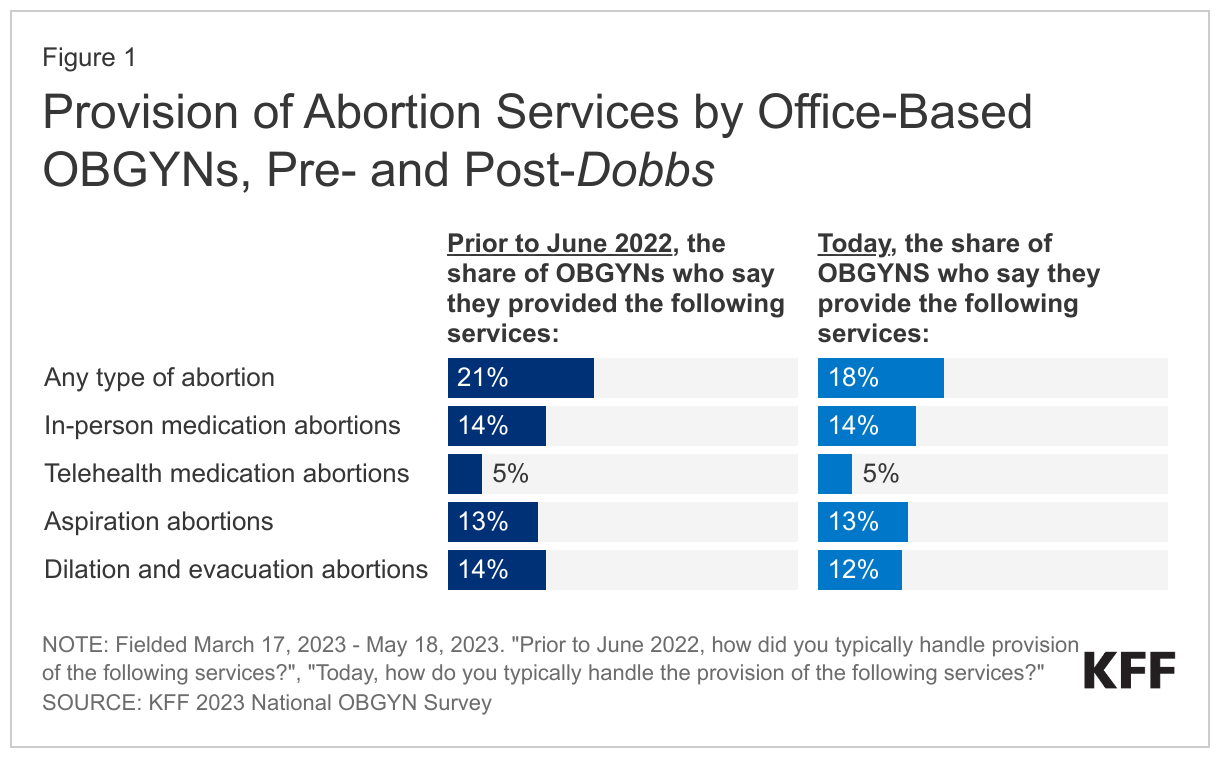
The KFF 2023 National OBGYN Survey finds one in five office-based OBGYNs (21%) say they provided any type of abortion prior to the Dobbs decision, which is statistically unchanged from the 18% that say they provide abortion services after the Dobbs decision.
Types of Abortion Services
Medication abortion, which accounts for more than half of abortions, is conducted by taking oral medications. In the U.S., the most common protocol uses two different drugs, Mifepristone and Misoprostol, which the Food and Drug Administration (FDA) has approved for use up to the first 10 weeks of pregnancy. Pills can be provided in-person or via telehealth depending on state policies.
Aspiration abortion is a minimally invasive and commonly used gynecological procedure and the most common form of procedural abortion. It can be used to conduct abortions up to 14-16 weeks of gestation.
Dilation and evacuation abortions (D&E) are usually performed after the 14th week of pregnancy.
Nationally, just over one in ten office-based OBGYNs (14%) provide in-person medication abortions, 13% provide aspiration abortions, 12% provide dilation and evacuation abortions, and only 5% provide telehealth medication abortions post-Dobbs (Figure 1).
The survey also looks at OBGYNs in states with very different policies on abortion access. Some states have outright banned abortion since the Dobbs ruling, some have limits on abortions between 6- and 22-weeks gestation, and in some states, abortion is largely available under most circumstances. Not surprisingly, there are substantial differences in the provision of abortion services depending on state abortion policies today, and there were already large differences between states prior to the Supreme Court’s ruling.
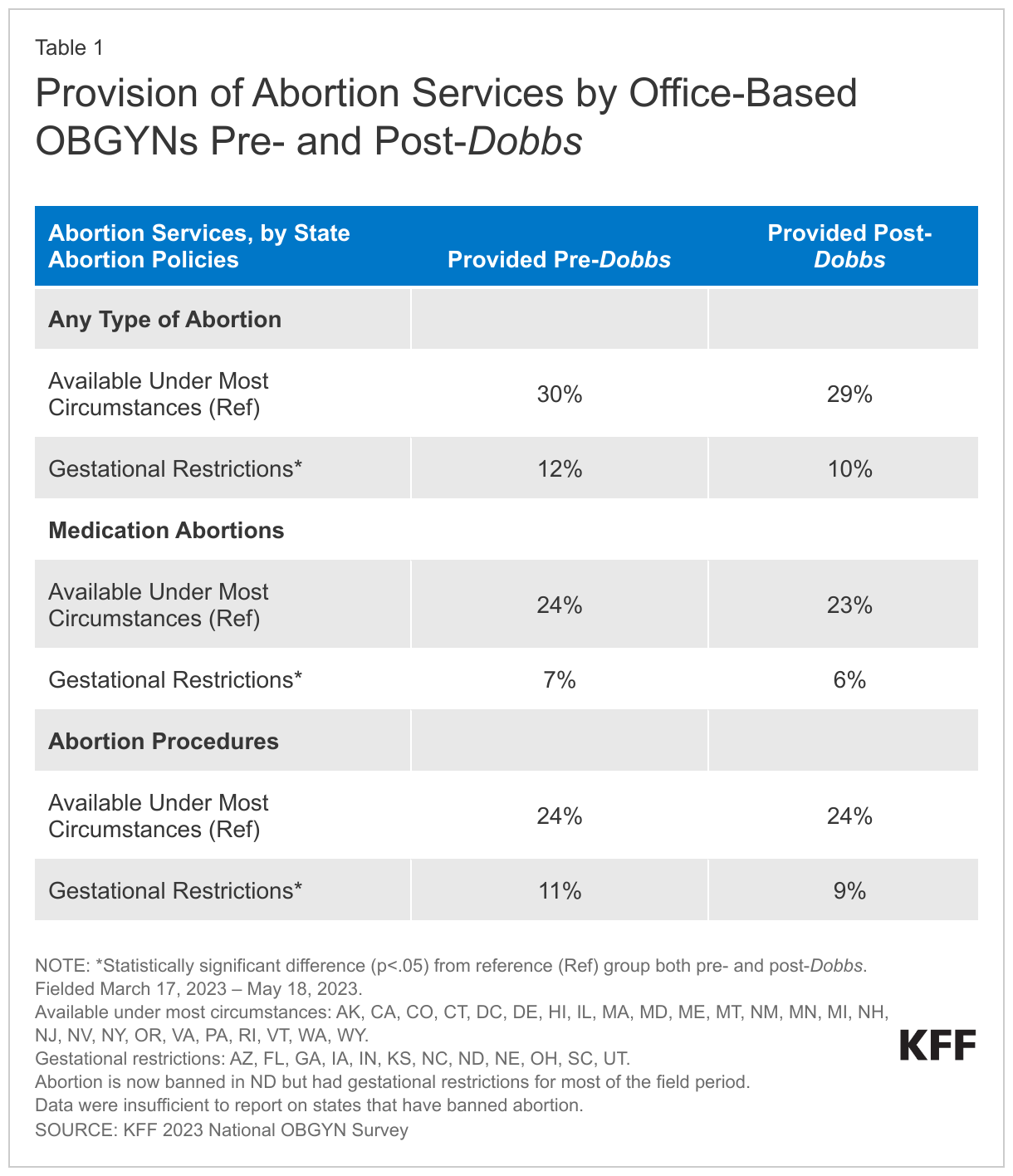
Many of the states that have gestational limits and bans now already had severe restrictions in place prior to the Dobbs ruling, which greatly limited abortion access and provision. As a result, just 12% of OBGYNs in states with gestational restrictions provided abortions before the Dobbs decision, compared to 30% in states where abortion remains available under most circumstances. The shares are similar today, with 29% of OBGYNs in states where abortion is available under most circumstances offering abortion care, compared to just 10% in states with gestational restrictions.
In states where abortion is now banned there were not sufficient shares of OBGYNs providing abortion services pre- and post-Dobbs to report. The shares of OBGYNs who perform abortions did not change substantially after the Dobbs decision in any of the state groupings (Table 1). In states with gestational limits only 6% of OBGYNs provide medication abortions and 9% provide abortion procedures. In contrast, in states where abortion is available under most circumstances, one quarter (23%) of OBGYNs say they provide medication abortions and abortion procedures (24%).
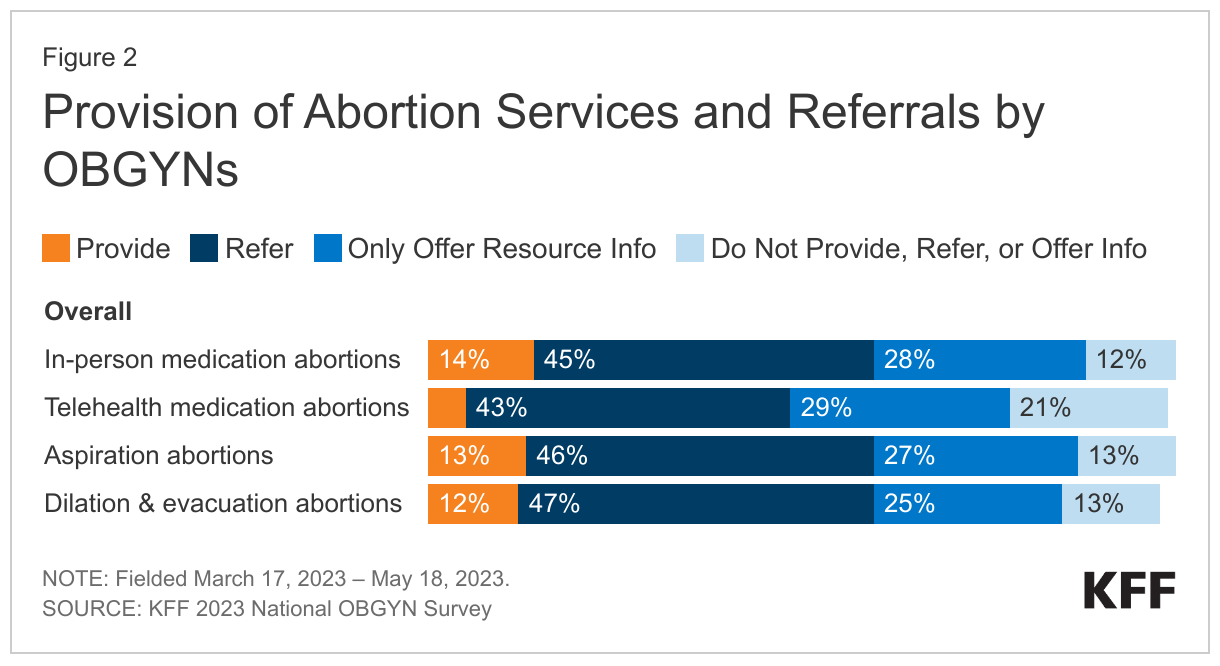
Many OBGYNs say they will refer their patients to another clinician for abortion services but don’t provide abortions themselves. Nearly three in ten OBGYNs say they do not provide nor refer their patients to abortion services, but they do share information about resources (e.g., a link to a website such as Abortion Finder or Plan C) (25-29% across different types of abortions). For most abortion procedures and in-person medication abortions, one in eight OBGYNs (12-13%) do not provide, refer, or offer information to their patients about abortion services. One in five (21%) do not provide, refer, or offer information to their patients about telehealth medication abortions (Figure 2).
In addition to lack of abortion availability in states with abortion bans, many OBGYNs in these states do not refer for abortion services either. They are more likely to say that they offer informational resources about abortion (e.g., a link to Abortion Finder or Plan C) than make referrals.
We looked at the characteristics of OBGYNs who specifically provide or refer for at least one abortion service since this offers patients a more direct connection to care. There were substantial differences between physicians who provide and refer compared to those who do not, based on the abortion policy in the state in which they practice. In states with abortion bans, 30% of OBGYNs do not even offer their patients referrals to another clinician or any information (such as online resources) about abortion, leaving those seeking abortion services without services and referrals, even if those referrals would be out of state (Figure 3).
This is not surprising in light of confusion in states like Idaho and Texas regarding the legality of abortion referrals. Texas’ SB8 prohibits aiding and abetting the provision of abortions, leaving providers afraid and reluctant to make abortion referrals. In Idaho, the Attorney General issued a letter saying Idaho law prohibits providers from referring a woman across state lines to access abortion services, but then withdrew the letter after being sued by abortion providers. Just under half (44%) of OBGYNs in states with restricted gestational limits do not provide or refer for abortion services compared to 19% in states where abortion is still available in most circumstances.
Reasons for Not Providing Abortion Services
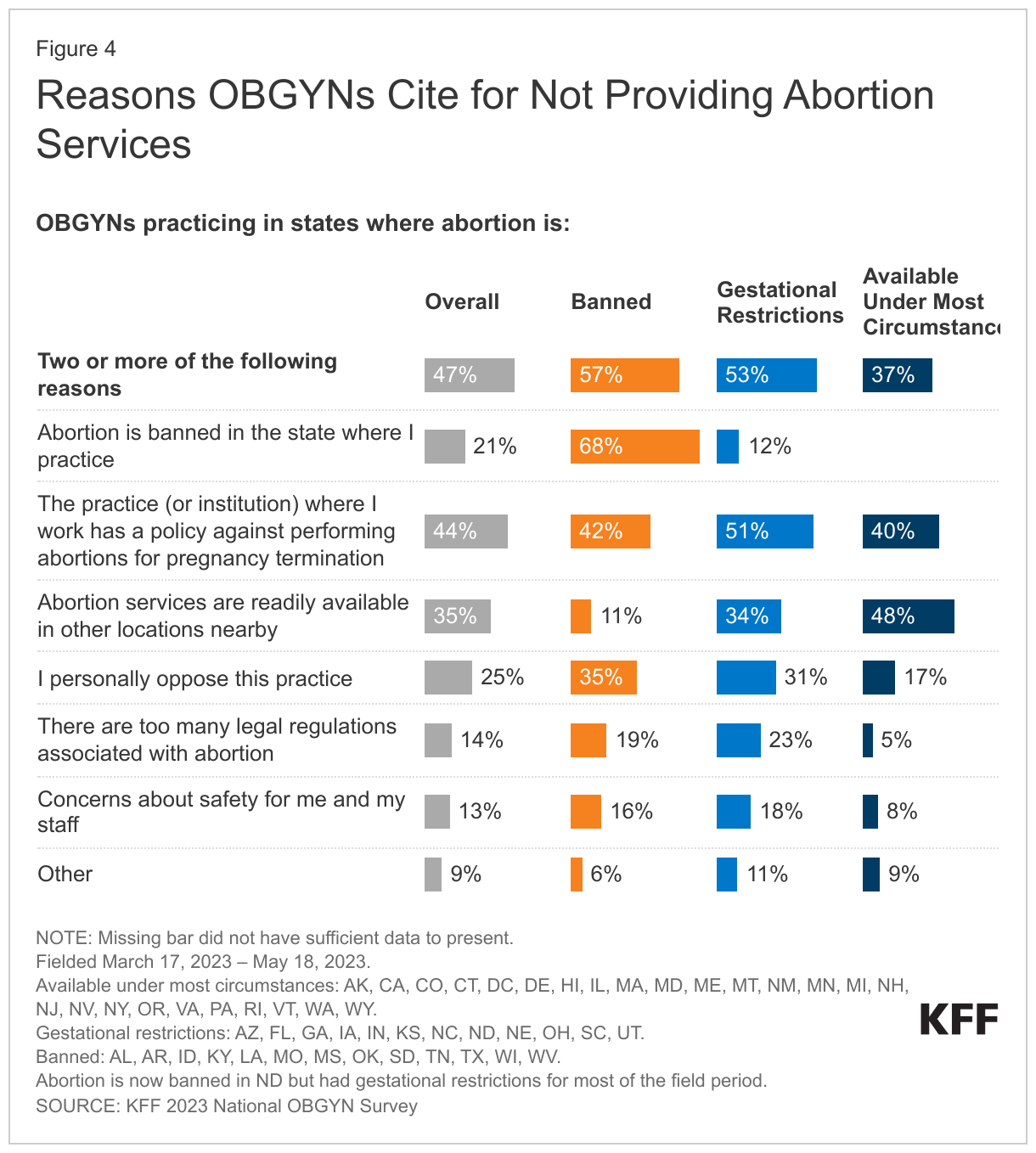
Overall, among OBGYNs who say they do not provide any type of abortion service, the top reason (44%) is that the practice or institution where they work has a policy against performing abortions for pregnancy termination (Figure 4). This share is similar across states where abortion is banned (42%) and states with gestational restrictions (51%). Not surprisingly, an abortion ban in the state where they practice is the leading reason OBGYNs in states with abortion bans cite for not providing abortions. Roughly three in ten OBGYNs who practice in states with abortion bans or restrictions who do not provide abortions say they personally oppose the practice, and one in five say there are too many legal regulations associated with abortion. Most OBGYNs that do not provide abortion services in states with bans or restrictions cite two or more reasons for not providing abortions. In states with gestational restrictions, just over a third of OBGYNs (34%) say the reason they do not provide abortion services is because abortion is readily available in other nearby locations.
Nationally, 13% OBGYNs cite safety concerns for themselves and their staff as a reason for not providing abortion services. This is higher among OBGYNs in states with bans (16%) and gestational restrictions (18%) compared to 8% in states where abortion is available under most circumstances.
Other reasons for why OBGYNs say they do not provide abortions include lack of training or religious reasons. Others say that they specialize in infertility and abortion services are not regularly desired by their patients.
MISCARRIAGE MANAGEMENT
Miscarriage Management among U.S. OBGYNs
Miscarriages are very common and an important aspect of many OBGYNs’ scope of practice, and sometimes involve the same procedures and medications that are used for abortions. Aspiration procedures, as well as mifepristone and misoprostol are also used to medically manage miscarriages. In early pregnancy, medical management for miscarriage with misoprostol and mifepristone allows a shorter time course than waiting for nonviable pregnancy tissue to pass on its own (expectant management) in patients without complications. Misoprostol alone can also be used for the medical management of miscarriage. Aspiration procedures are often used for individuals who are medically unstable or have an incomplete miscarriage after expectant or medical management or for patients who desire prompt resolution of their miscarriage.
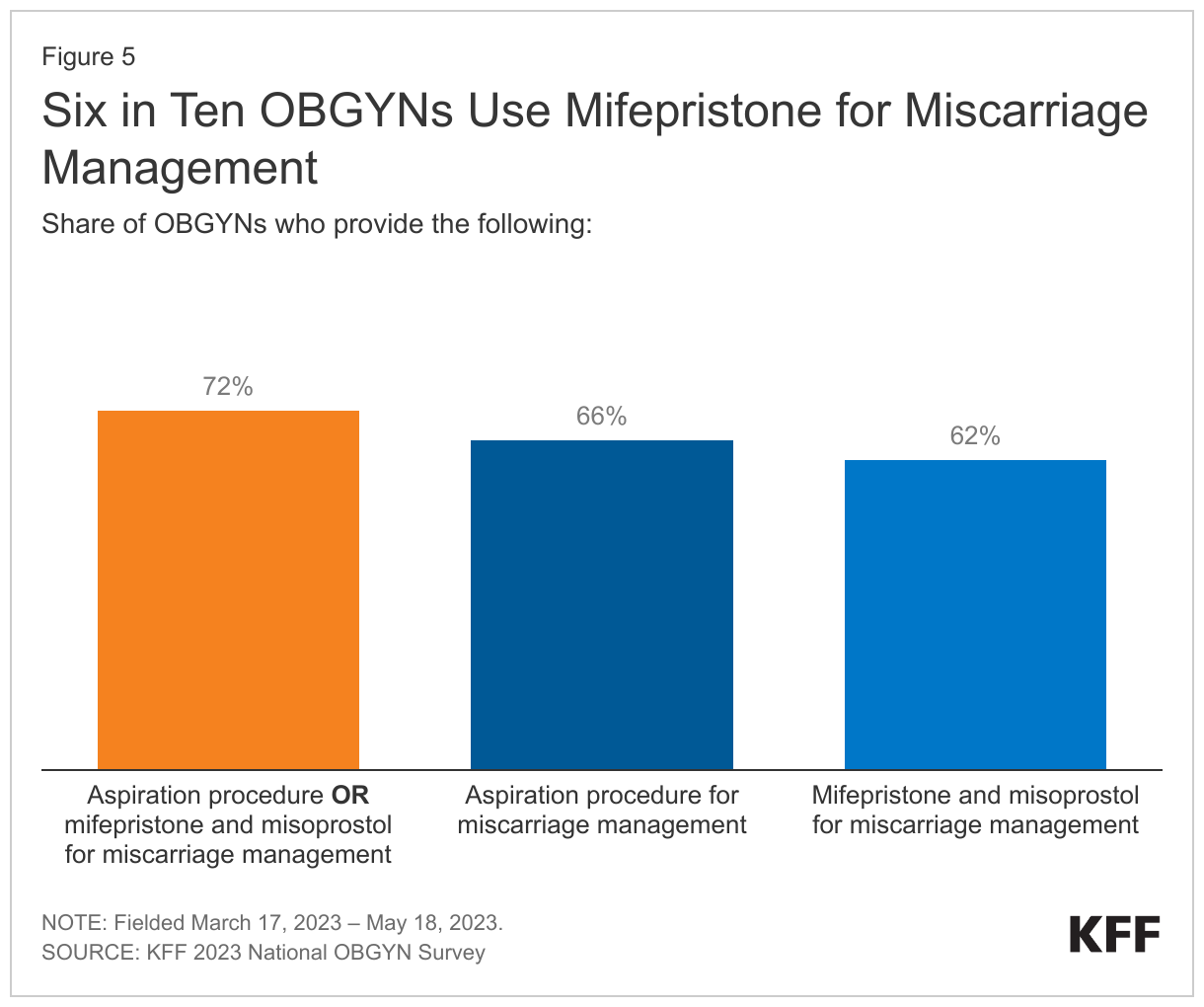
Three in four OBGYNs (72%) say they provide aspiration procedures or mifepristone and misoprostol for miscarriages, far more than those who provide abortion services (Figure 5). The shares of OBGYNs providing these services was similar pre- and post-Dobbs and there is very little variation by state abortion policy or demographic characteristics. Of note, six in ten (62%) OBGYNs use mifepristone with misoprostol for miscarriage management. However, the availability of mifepristone for miscarriage management could be greatly restricted if the current litigation challenging the FDA approval of the drug results in a reversal of the approval process.
UNDERSTANDING OF STATE ABORTION POLICIES AND CONCERNS ABOUT LEGAL RISK
Knowledge of State Abortion Laws
There are a wide variety of state laws and policies governing abortion access, availability, and provision, and since the Dobbs ruling, there have been numerous and often rapid changes in state policies. It is important for clinicians who provide sexual and reproductive health care to understand whether and when it is legal to offer abortion services. Even in states with abortion bans, there are limited exceptions, particularly for life-threatening medical emergencies, under which it should be legal to provide abortion services.
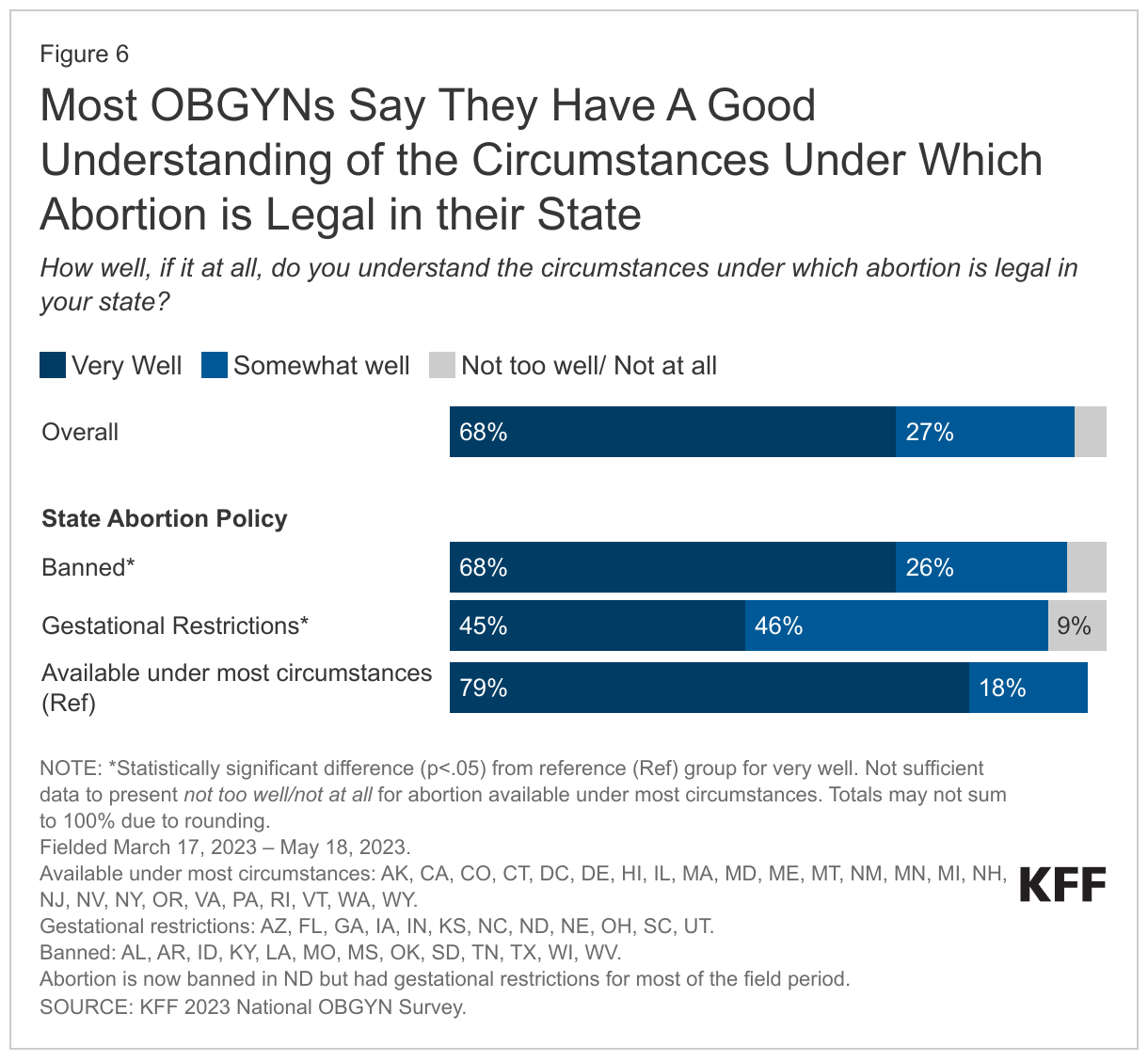
Nearly all OBGYNs (95%) say that they understand the circumstances under which abortion is legal in the state they practice—68% say they understand the circumstances very well and 27% say they understand somewhat well (Figure 6). Shares are similar across age, gender, and race/ethnicity groups. However, there is less clarity about policies among OBGYNs practicing in states with gestational restrictions where less than half say they understand the circumstances very well (45%), a lower share than those in states where abortion is banned (68%) altogether and where abortion remains available under most circumstances (79%).
Concern about Legal Risk
Abortion bans and restrictions can carry criminal penalties for clinicians that provide abortion care. Over four in ten (42%) OBGYNs report that they are very or somewhat concerned about their own legal risk when making decisions about patient care and the necessity of abortion. This is higher among OBGYNs identifying as women (47%), compared to men (34%). A higher share of OBGYNs practicing in states where abortion is banned (61%) and in states with gestational limits (59%) are concerned about their own legal risks compared to OBGYNs in states where abortion is available (27%) (Figure 7).
CONSTRAINTS ON CARE AS A RESULT OF DOBBS
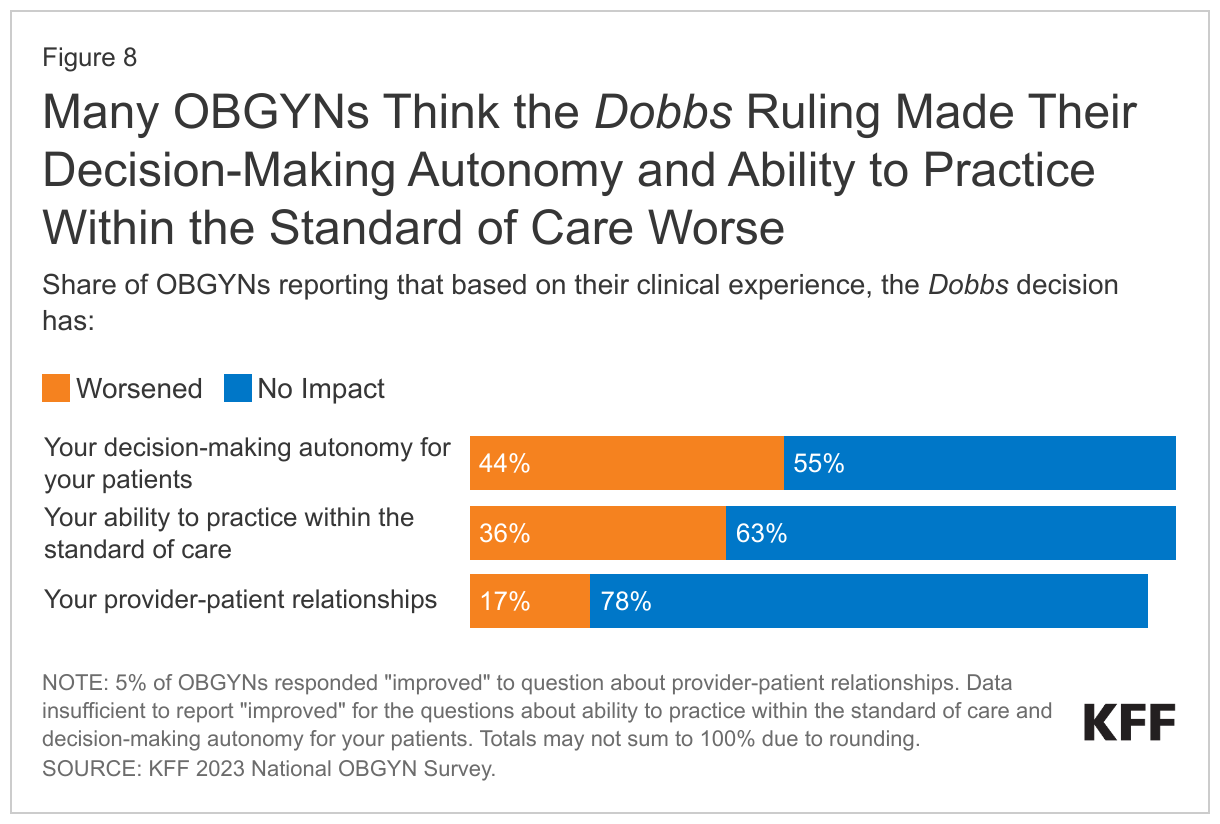
As OBGYNs worry about their legal risk, many report that Dobbs has affected their interactions with patients to the detriment of care (Figure 8). More than four in ten (44%) OBGYNs say their decision-making autonomy has become worse in the past year and over one-third (36%) say their ability to practice within the standard of care has deteriorated. Almost one in five (17%) OBGYNS say their provider-patient relationships have become worse since Dobbs. Overall, 16% of OBGYNs say the Dobbs decision has made all of these issues worse.
While many OBGYNs across the country have seen an impact of Dobbs on their practice, the effect on some of these measures varies widely between states (Figure 9). For example, 55% of OBGYNs in states with abortion bans and 47% in states with gestational limits say their ability to practice within the standard of care has worsened since Dobbs, much higher than 23% among OBGYNs in states where abortion is available under most circumstances. Similarly, three in ten OBGYNs in banned states (30%) and one in five in gestational limit states (20%) say their patient-provider relationships have worsened since Dobbs, compared to one in ten in states where abortion is available under most circumstances (11%).
A significant portion of OBGYNs say they have personally experienced limits on their professional care since the Dobbs ruling (Figure 10). Nationally, one in five say they have been constrained in providing care for miscarriages (20%) and pregnancy-related emergencies (19%) since the Dobbs ruling. About a quarter (24%) of OBGYNs say they have had a patient who tried to obtain an abortion and could not obtain one. However, all of these are more commonly reported among OBGYNs in states where abortion is banned or limited by gestational restrictions than in states where abortion is permitted under most circumstances. About four in ten OBGYNs in states where abortion is banned say they have been constrained in providing care for miscarriages (40%) and pregnancy-related medical emergencies (37%), compared to less than one in ten OBGYNs in states where abortion remains available under most circumstances. Fewer OBGYNs say a patient has asked them about how to have an abortion on their own (14%), but the share is slightly higher in states with gestational limits (18%).
Many OBGYNs also say that the Dobbs decision has had a negative impact on the broader field of maternity care. Pregnancy-related mortality (death within one year of pregnancy) has been recognized as a major public health tragedy and urgent priority for action. In particular, the share is 3-4 times higher among women who are Black, Native American, and NHOPI compared to White women. Reducing the overall rate and narrowing these disparities has been the focus of several efforts among clinicians, policymakers, and the public health community. Shortages in maternity care providers, particularly in certain regions, is one of many factors that affects pregnancy-related mortality and morbidity. These survey findings raise the alarming prospect that maternal health outcomes may worsen in the post-Roe world. Seven in ten OBGYNs say that since the Dobbs decision, racial and ethnic inequities in maternal health (70%) as well as management of pregnancy-related medical emergencies (68%) have gotten worse (Figure 11). Over half think that the ability to attract new OBGYNs to the profession has worsened (55%) and 64% think the same about pregnancy-related mortality. Interestingly, these concerns are shared by OBGYNs in states with different abortion policies. More than half of all OBGYNs across all state groupings say that these problems have become worse since Dobbs. A slightly higher share of those practicing in states where abortion is available (75%) under most circumstances say racial and ethnic inequities have worsened compared to those in states where abortion is banned (63%).
CONTRACEPTION
Provision of Contraception
Overall, 80% of OBGYNs provide reversible contraceptive methods (other than emergency contraception) (Figure 12). Nearly all OBGYNs report that they prescribe/provide oral contraceptive pills (99%), vaginal rings (96%), the patch (95%), contraceptive injections (Depo-Provera) (93%), and intrauterine devices (IUDs) (93%). Slightly fewer provide contraceptive implants (Nexplanon) (83%). Eight in ten also provide their patients with tubal ligation procedures (81%).
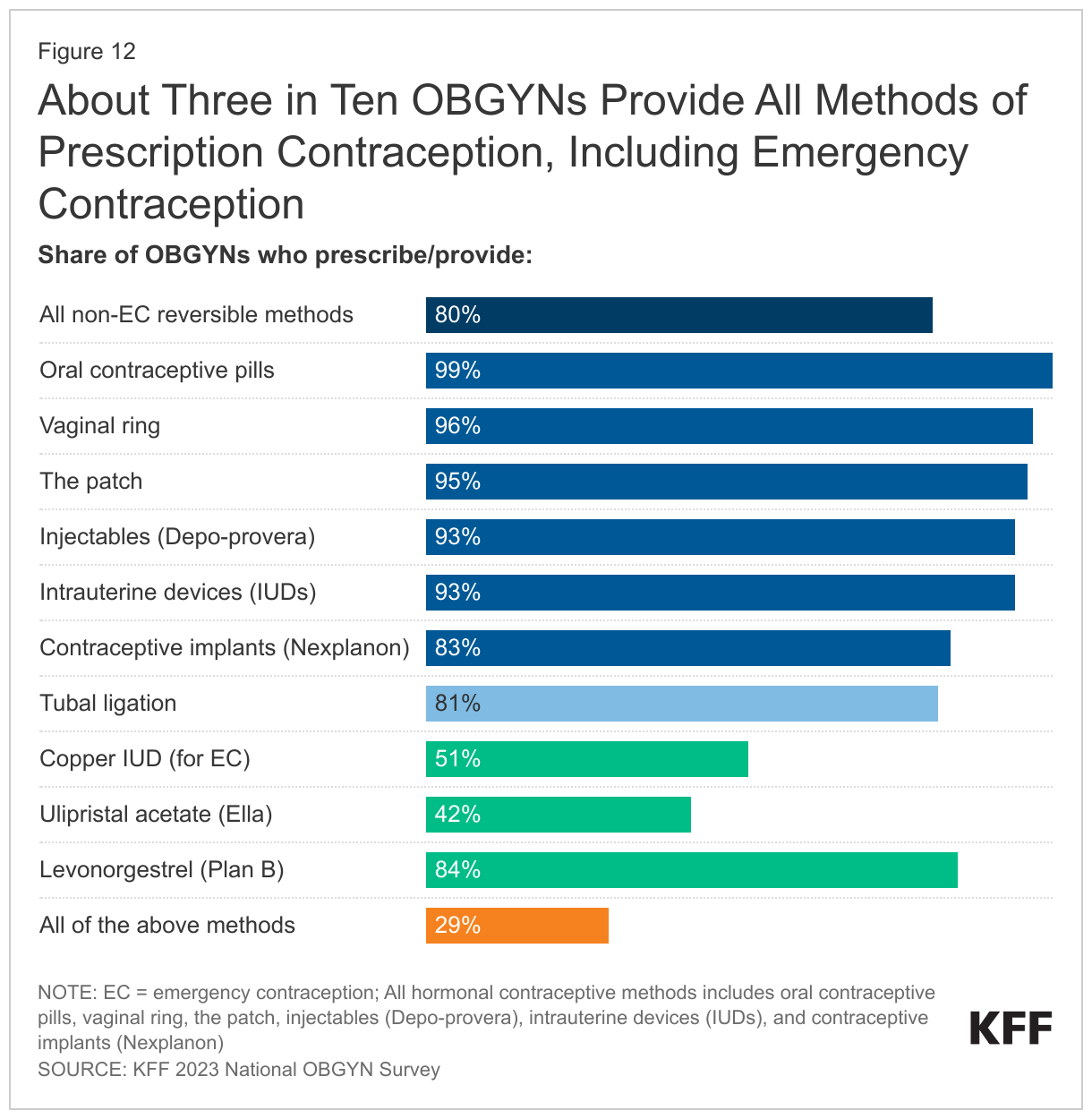
When including emergency contraception (discussed below), however, about three in ten (29%) OBGYNs reported prescribing or providing all ten of the contraceptive methods asked about, including all hormonal methods (pill, patch, ring, injection, IUD and implant), tubal ligation, and all three methods of emergency contraception (copper IUD, ulipristal acetate (Ella), and Plan B).
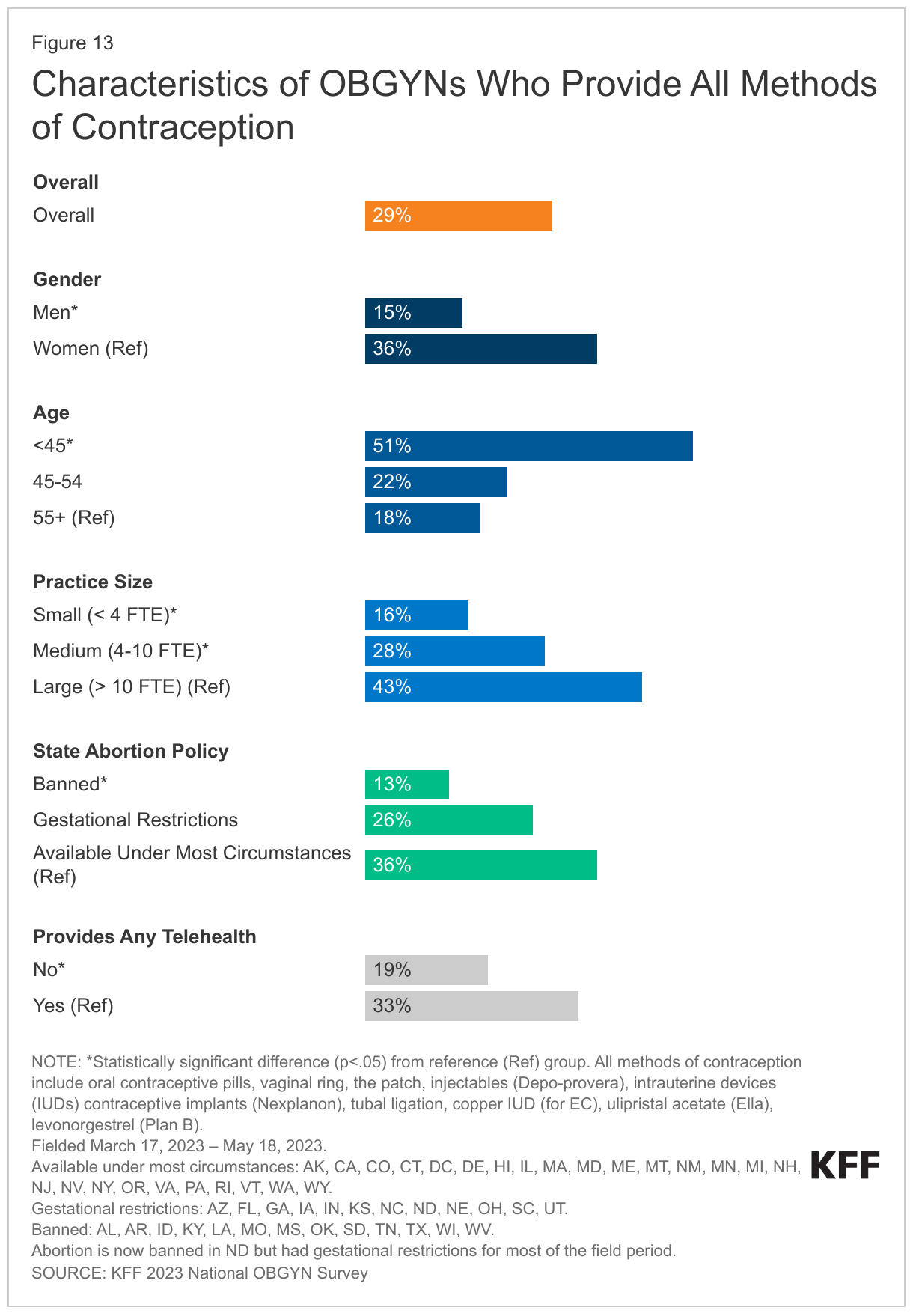
A higher share of OBGYNs who are women compared to men, younger compared to older, work in large practices compared to medium and small, and those who provide any telehealth compared to those who do not provide telehealth report providing all methods of contraception (Figure 13). Larger shares of OBGYNs practicing in states where abortion is available under most circumstances compared to states where abortion is banned say they provide all methods of contraception (36% vs. 13%).
Provision of Emergency Contraception
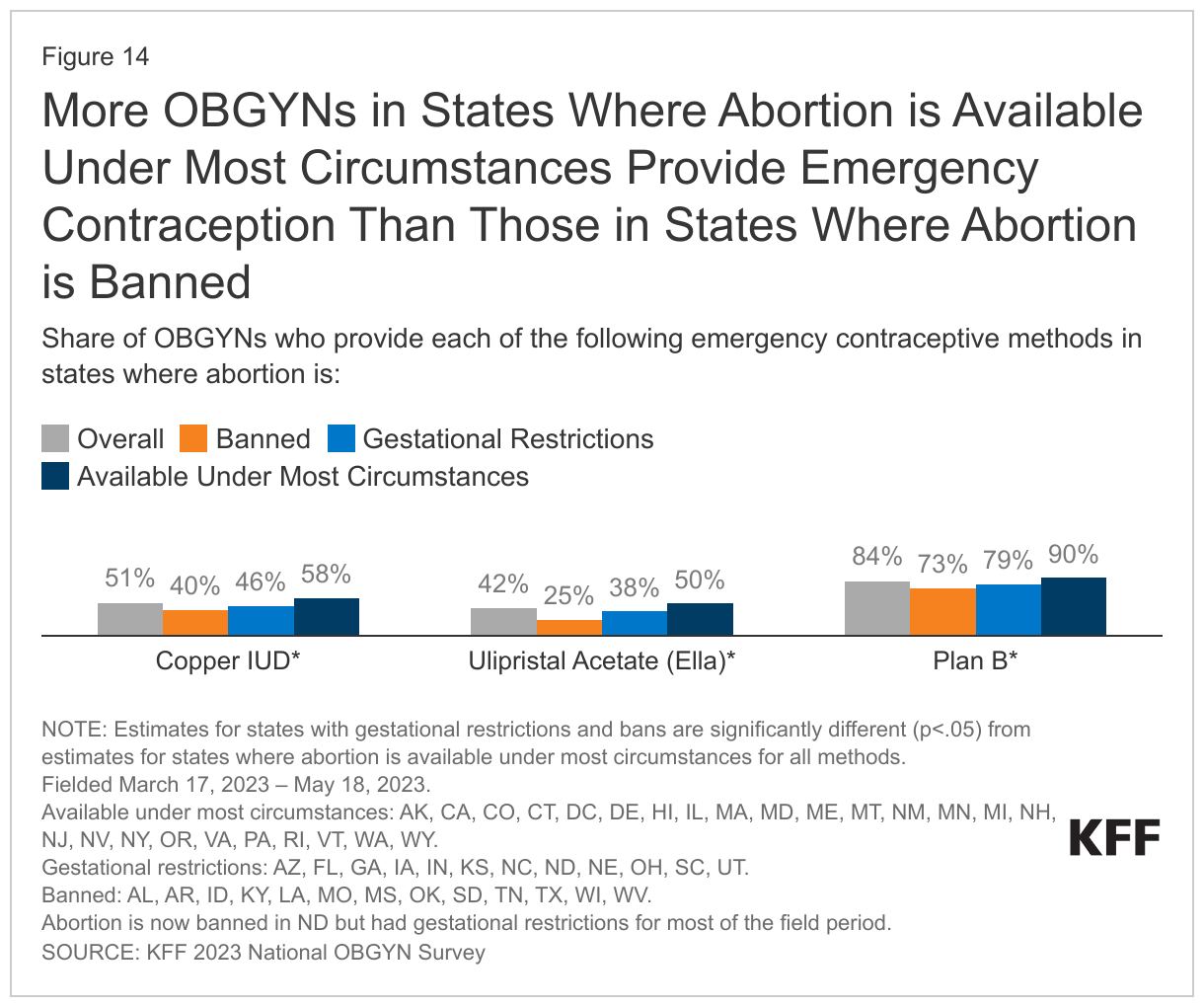
Among the three commonly used methods of emergency contraception (EC), the copper IUD and ulipristal acetate/Ella must be prescribed, and levonorgestrel/Plan B can be purchased over the counter. Just over half of OBGYNs provide copper IUDs (51%) for emergency contraception and less than half provide ulipristal acetate/Ella (42%) (Figure 14). Larger shares of OBGYNs who provide copper IUDs and ulipristal acetate/Ella for emergency contraception are women, younger, work in larger practices, and provide telehealth.
There are also notable differences in the availability of EC between states with and without abortion bans and restrictions. Notably, only a quarter (25%) of OBGYNs in states with abortion bans provide ulipristal acetate/Ella and only four in ten (40%) provide copper IUDs for emergency contraception, which is lower than in states where abortion is available under most circumstances. This means that in abortion ban states, not only is abortion unavailable, but there is also limited OBGYN provision of certain emergency contraception methods. While most OBGYNs provide levonorgestrel/Plan B, this share is also lower in states where abortion is banned (73%) compared to in states where abortion is available under most circumstances (90%). There are misconceptions, even among some OBGYNs that emergency contraception and IUDs cause abortion, which could result in their unwillingness to provide or prescribe emergency contraception.
Twice as many OBGYNs provide or prescribe levonorgestrel/Plan B than ulipristal acetate/Ella, which is surprising since Plan B can be purchased over the counter, while Ella requires a prescription from a clinician. Ella is also more effective among people who are overweight or obese and has a longer window of time for use. However, in most states, Plan B must be prescribed for it to be covered by insurance. Otherwise, someone would have to pay for it out of pocket, which typically costs between $35-$49. Obtaining a prescription from a clinician can also help alleviate some other barriers to obtaining Plan B pills, such as when stores do not stock it or lock it in a case.
Only a third of OBGYNs (34%) prescribe or provide all three methods of emergency contraception and one in seven (15%) do not provide any methods of emergency contraception. A quarter of OBGYNS (25%) only prescribe or provide Plan B (Figure 15).
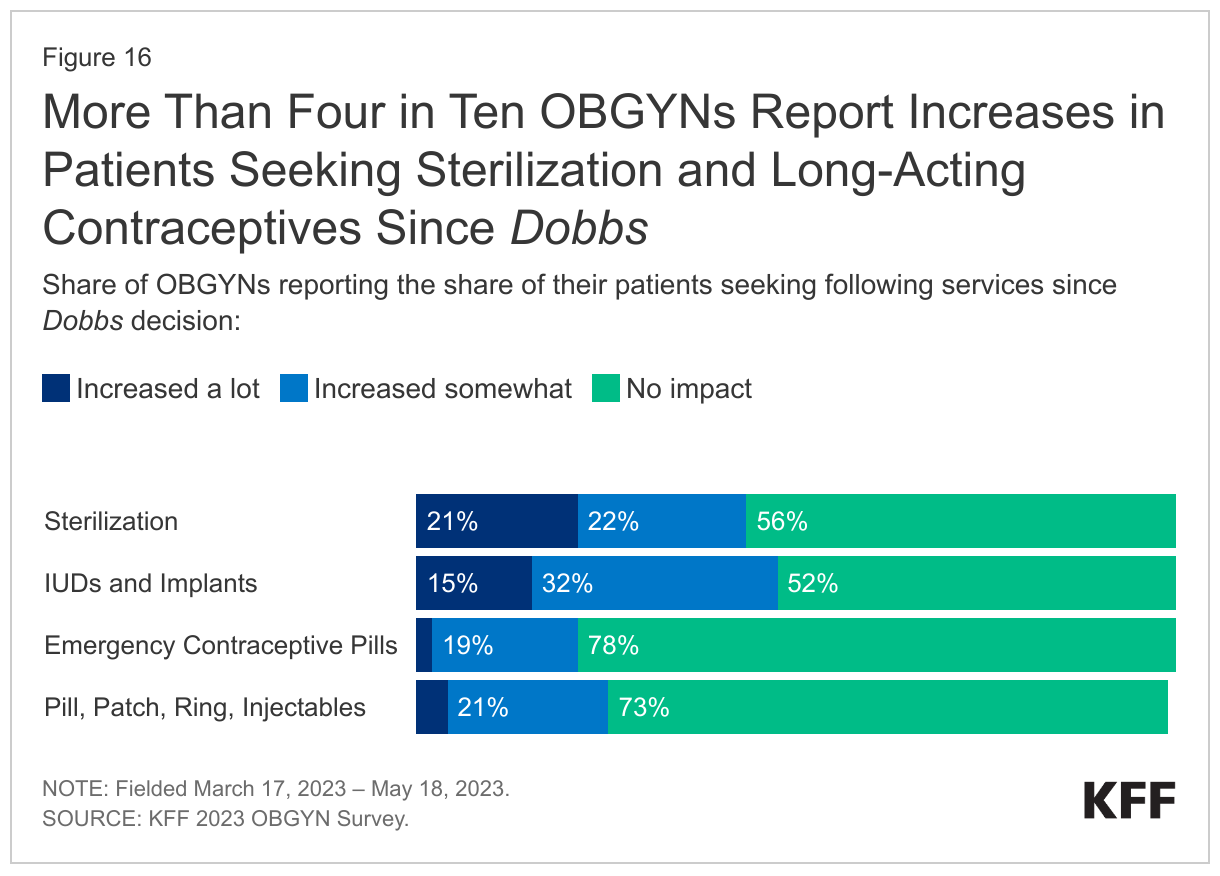
Many OBGYNs report that they have seen a rise in the share of their patients seeking contraception since the Dobbs ruling. Overall, more than half (55%) of OBGYNs say they have seen an increase in the share of patients seeking at least one form of contraception since the Dobbs ruling. In particular, a substantial share of OBGYNs report more patients are interested in sterilization and LARCs over the past year. One in five OBGYNs (21%) say that they have seen a lot of increase in the share of patients seeking sterilization and another one in five (22%) have seen some increase (Figure 16). More than one in ten (15%) say the share of patients seeking LARCs has increased a lot and another 32% say there has been some increase. Just over half (52%) though say there has been no change. OBGYNs report more modest rises in patients seeking EC pills (21% a lot or somewhat) and other hormonal methods, which include oral contraceptives, Depo injections, patch, and ring (25% a lot or somewhat). About three-quarters of OBGYNs say that there has been no change in the share of patients seeking EC (78%) or other hormonal methods (73%) since the Dobbs ruling.
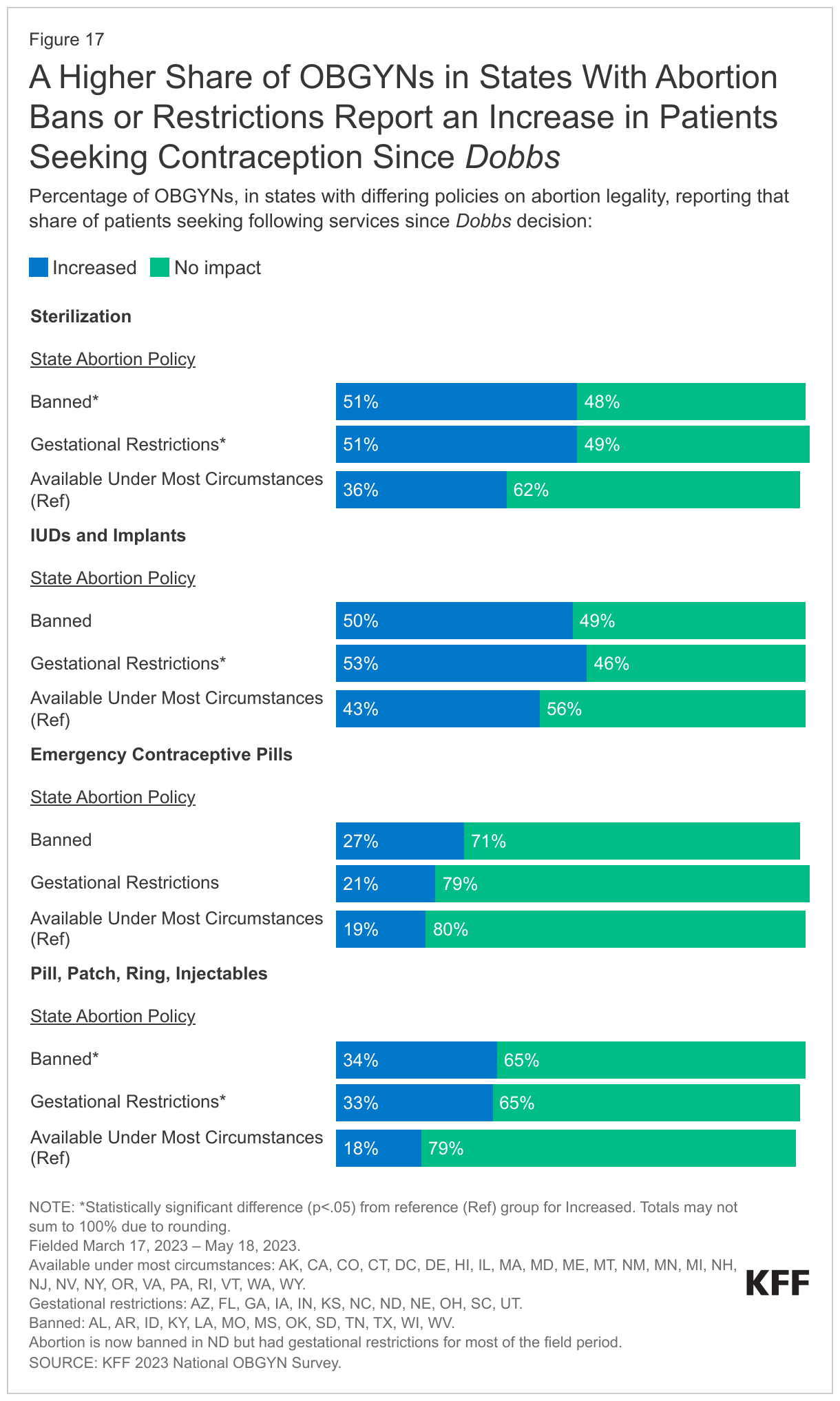
The increased interest in contraception is more pronounced in states where abortion is banned or greatly limited by gestational limits (Figure 17). For example, about half of OBGYNs in these states say the share of patients seeking sterilization has increased since Dobbs, higher than in states where abortion remains available under most circumstances. This pattern is similar for other hormonal methods too. About one-third of OBGYNs in states where abortion is banned or with gestational restrictions say they have seen an increase in patients seeking other hormonal methods, compared to 18% of OBGYNs in states where abortion is available under most circumstances.
ADDITIONAL AVENUES OF CARE
Telehealth
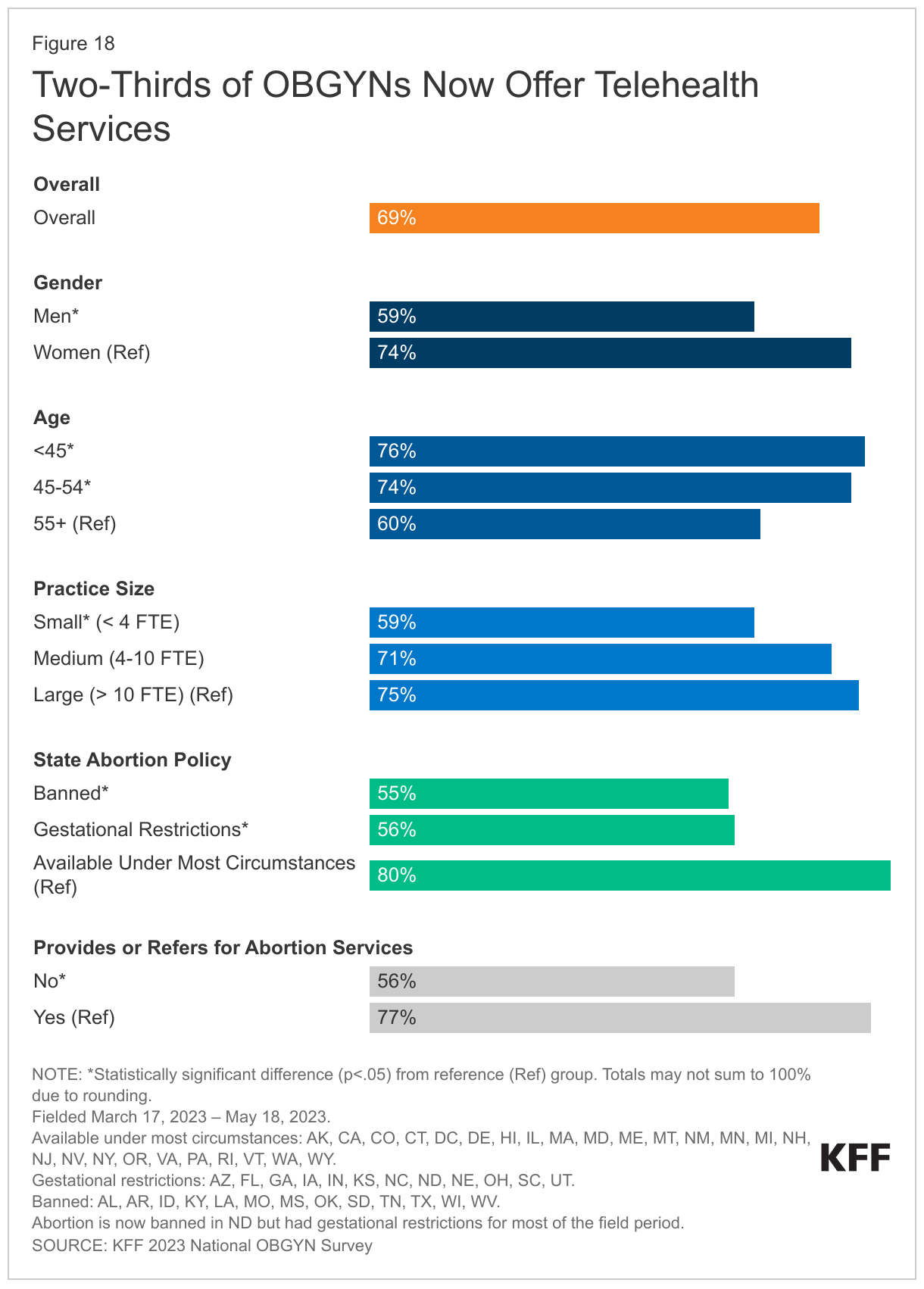
While the Dobbs decision has significantly changed the provision of health care, the COVID-19 pandemic also significantly expanded provider use of telehealth services. In 2020, the KFF National Physician Survey found that prior to March 1, 2020, just 12% of OBGYNs were using telehealth, which dramatically increased to 84% using telehealth by June 2020. In the 2023 survey we found 69% of OBGYNs were providing some services through telehealth, with about a third saying they did not (31%) provide any care via telehealth (Figure 18). Larger shares of OBGYNs who are women, younger, and provide or refer for abortion services, as well as practice in a state where abortion is available under most circumstances say they currently provide telehealth. Some patients that relied on telehealth services during the height of the pandemic may find that their provider is no longer providing telehealth services.
Pharmacy Dispensing of Medication Abortion
For many years, FDA policy required that mifepristone pills could only be dispensed by a clinician who was certified to prescribe the drug at an in-person medical appointment. However, in December 2021, the FDA adopted expanded the distribution to include certified pharmacies in addition to certified clinicians. This change removed the previous requirement to dispense the medication in person and expanded the opportunity for telehealth in states that have not banned abortion. Subsequently, on January 3, 2023, the FDA approved a protocol for pharmacies, allowing those that have been certified by the manufacturers to dispense mifepristone directly to patients. However, the FDA’s initial approval of mifepristone in 2000 is currently being challenged in federal courts.
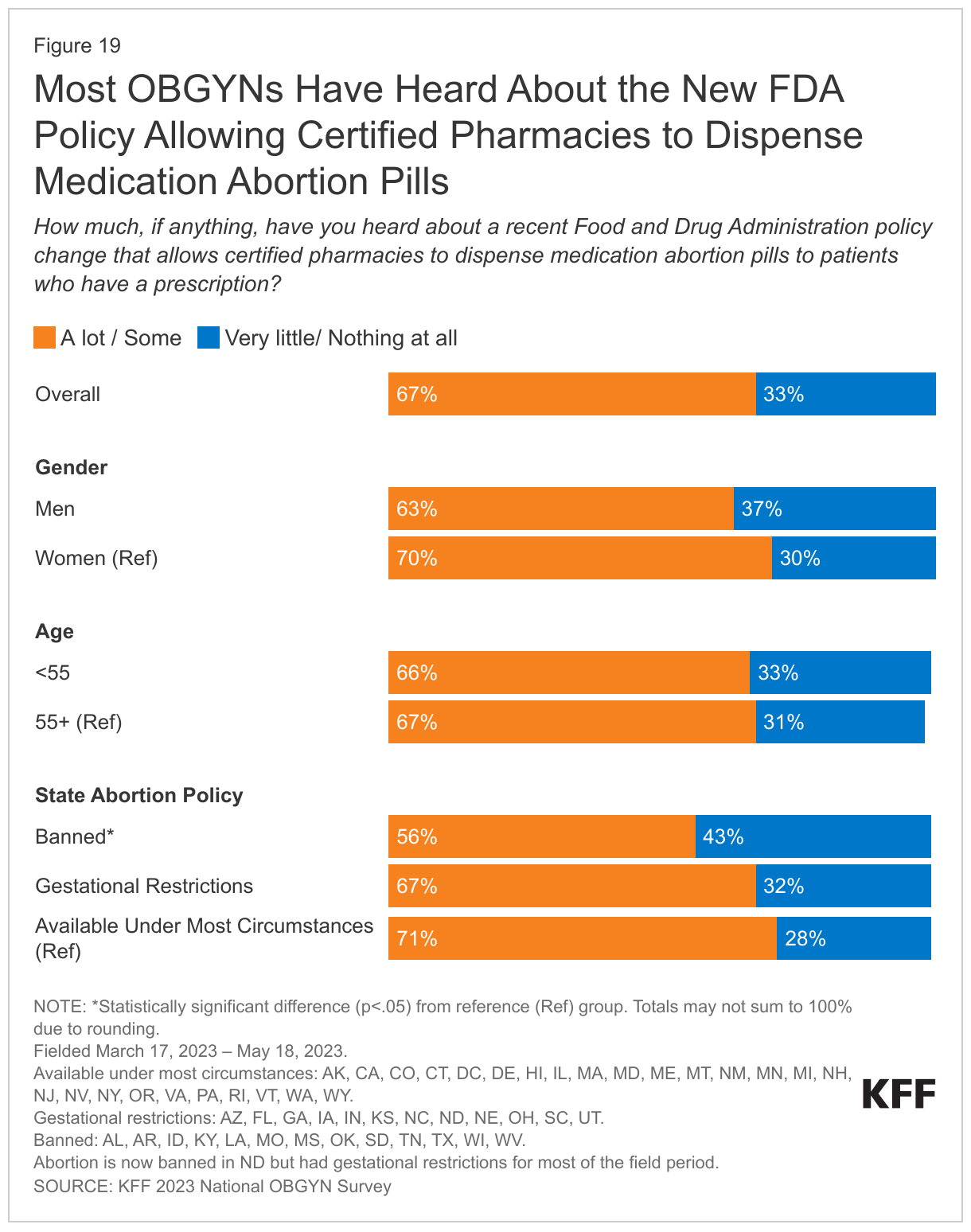
This survey asked OBGYNs if they had heard about the most recent FDA policy change allowing pharmacies to dispense medication abortion pills to patients. Two-thirds of OBGYNs (67%) report that they have heard a lot or some about the FDA’s policy change, and 33% have heard very little or nothing at all (Figure 19). Fewer OBGYNs practicing in states where abortion is banned (56%) report having heard of the policy change compared to OBGYNs practicing in states where abortion is restricted by gestational limits (67%) or is available (71%).
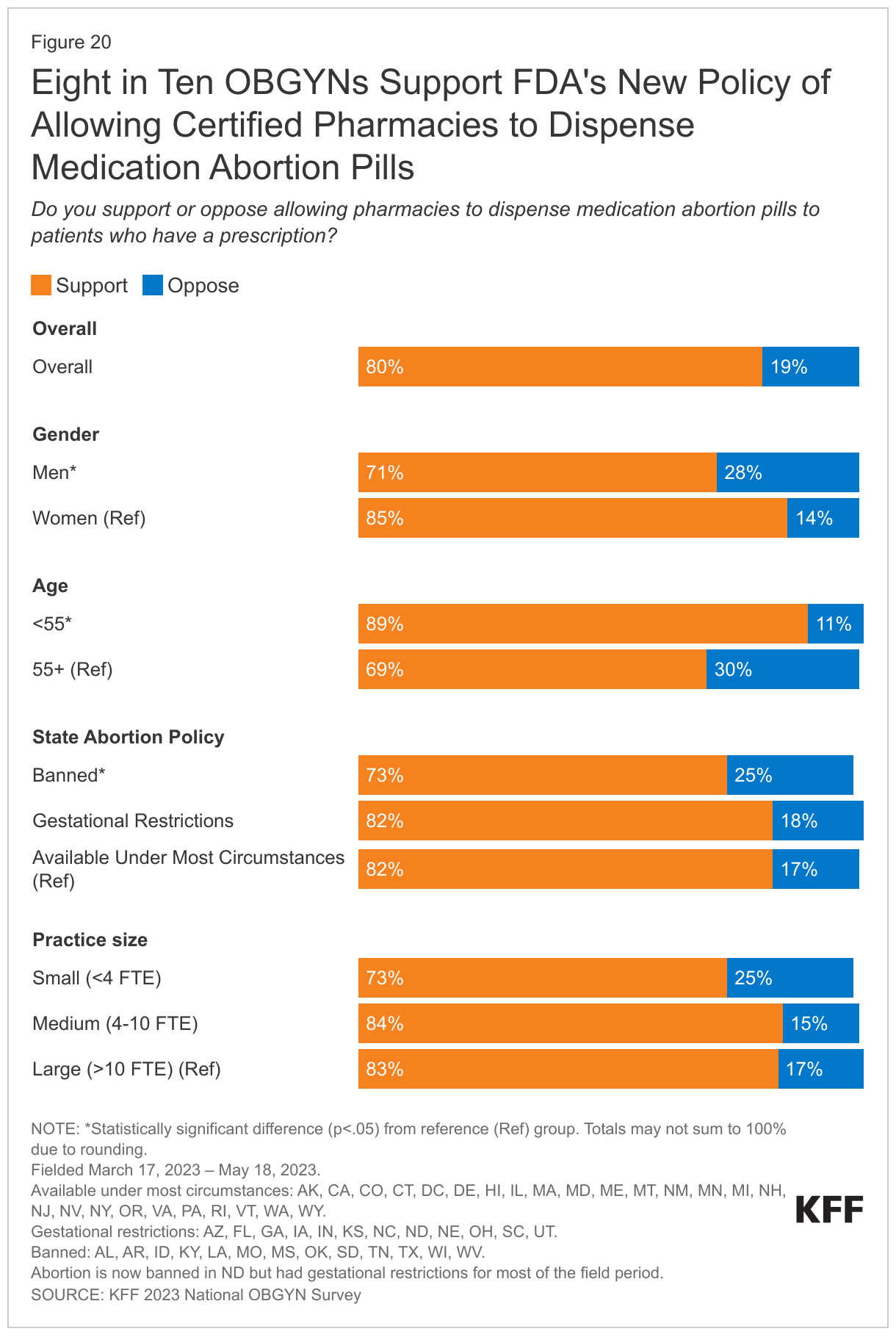
There is broad support among OBGYNs (80%) for the FDA change that allows certified pharmacies to dispense medication abortion pills to patients while 20% are opposed (Figure 20). Notably, support is consistently high across OBGYNs in states with differing abortion policies. Eight in ten OBGYNs practicing in states where abortion is available (82%) and in states where abortion is restricted (82%) support allowing pharmacies to dispense medication abortion as do 73% of those practicing in states where abortion is banned. Larger shares of OBGYNs under the age of 55 (89%), who are women (85%), or who work in midsize (84%) support this policy compared to OBGYNs who are over the age of 55 (69%), who are men (71%) or work in smaller practices (73%).
Looking Forward
The Supreme Court’s Dobbs decision not only affected abortion access, but it substantially changed many aspects of the provision of reproductive health care across the country. While the majority of OBGYNs do not provide abortion services, most OBGYNs do provide miscarriage management using the same procedures and medications that are used for abortions. Four in ten OBGYNs in states where abortion is illegal report constraints on their ability to manage miscarriages and pregnancy-related medical emergencies. Many also say their decision-making autonomy, the ability to practice within the standard of care, and their provider-patient relationships have been worsened by the Dobbs decision. Most are also concerned that pregnancy-related mortality and maternal health disparities have gotten worse as a result of the ruling. Some of the states with abortion bans and restrictions already had some of the poorest maternal and infant health outcomes.
The effects of the Dobbs decision on patient care are only beginning to be seen. In some states where abortion was not immediately banned, policymakers continue to pass laws to ban or seek to limit abortion services, leaving more patients without access and requiring longer travel distances for those that are not able to get abortion care where they live. These policies place additional demand on clinicians providing abortions in states where abortion is still available under most circumstances, but the share of OBGYNs that offer abortion services has not increased. Additionally, there has already been a decline in medical students applying to residencies in states where abortion is banned because they cannot receive the full spectrum of training. Over time, this could leave large parts of the country with shortages of trained OBGYNs that will affect not only abortion services but also other pregnancy-related services.
Methodology
Methods Summary
The KFF 2023 National OBGYN Survey obtained responses from a nationally representative sample of OBGYNs practicing in the United States who provide sexual and reproductive health care to patients in office-based settings. The survey was designed and analyzed by researchers at KFF, and an independent research company, SSRS, carried out the fieldwork and collaborated on questionnaire design, pretesting, sample design, and weighting. Survey responses were collected via paper and online questionnaires from March 17 to May 18, 2023 from 569 OBGYNs.
Providers were sent an up-front cash $20 incentive in the first mailing to encourage respondents to complete the survey.
The response rate for eligible OBGYNs was 29.9% and was calculated using AAPOR’s RR3. Overall, 39% of qualified OBGYNs completed the survey by web and 61% completed by mail.
The samples were weighted to match known demographics. Taking into account the design effect, the margin of sampling error for results based on total OBGYNs is +/- 5 percentage points at the 95% confidence level. Margins of sampling error for the state groupings are +/- 7% in states where abortion is available under most circumstances, +/- 7% in states with gestational limits, and +/- 7% in states where abortion is banned. Please see the attached topline for the full methodology report.
Sample Overview
We surveyed a nationally representative sample of 569 U.S. OBGYNs currently in clinical practice. Eligible physicians were board-certified OBGYNs who spend at least 60% of their time providing direct patient care and provide sexual and reproductive health care to at least 10% of their patients in an office-based setting. We compared survey responses by key physician and practice characteristics. Gender, age and race were determined by physician self-report. Practice size was determined by the number of full-time equivalent (FTE) physicians or advance practice clinicians (small <4, medium 4-10, large > 10). Sampling was conducted to ensure an adequate sample of OBGYNs in states where abortion was available under most circumstances, meaning that it is legal without pre-viability gestational limits, during the survey field period: AK, CA, CO, CT, DC, DE, HI, IL, MA, MD, ME, MI, MN, MT, NH, NJ, NM, NV, NY, OR, PA, RI, VA, VT, WA, WY; states with pre-viability gestational restrictions during the survey field period: AZ, FL, GA, IA, IN, KS, NC, ND, NE, OH, SC, UT; and states where abortion was banned during the survey field period: AL, AR, ID, KY, LA, MO, MS, OK, SD, TN, TX, WI, WV. During the field period, there was a change in policy in ND and abortion is now banned. ND remains in the gestational limits category for this analysis, as that was the status of the state’s policy for most of the field period.
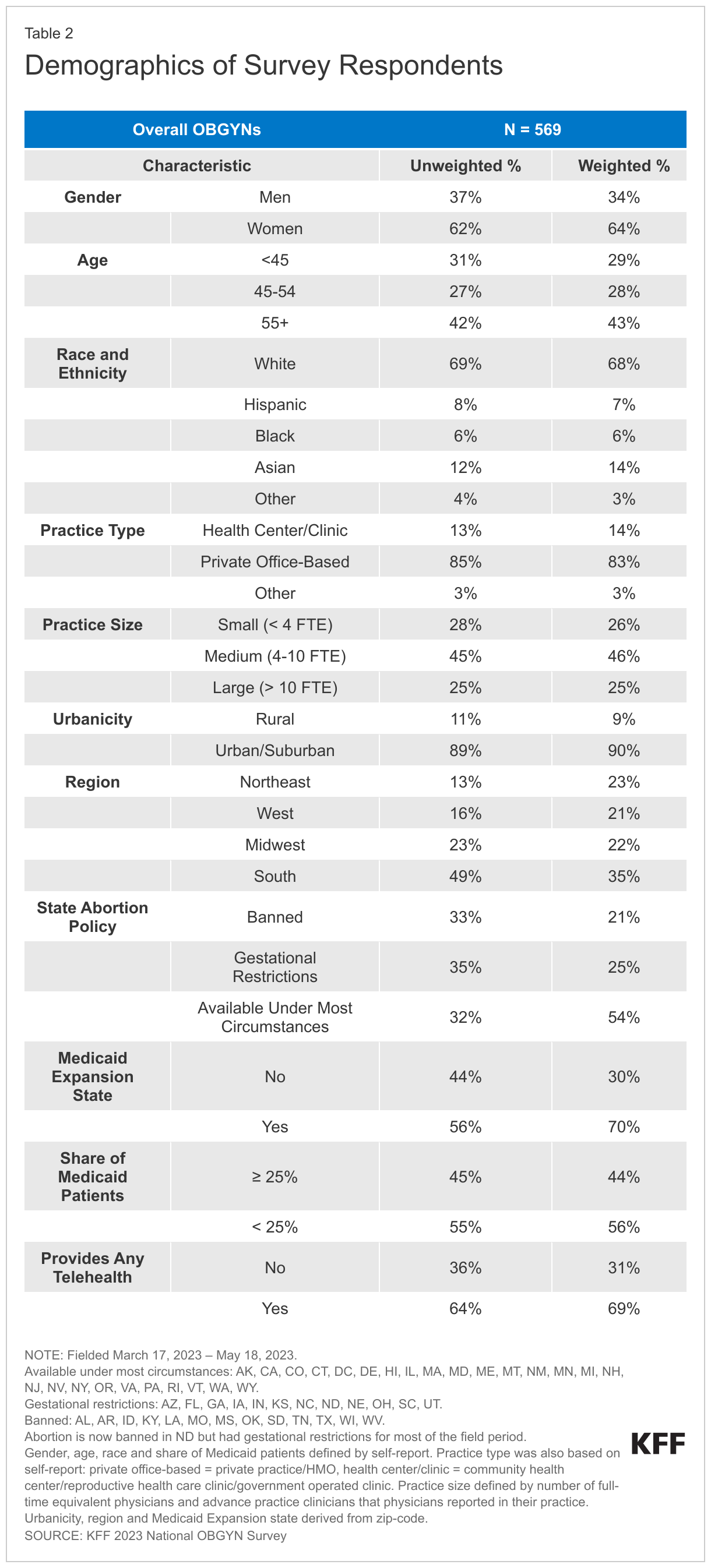
Characteristics of Survey Respondents
Table 2 shows the demographics of the survey respondents. More than six in ten are women (64%), most were under the age of 55 (57%), 68% are White, 14% Asian, 6% Black, and 7% Hispanic. The majority of OBGYNs surveyed work in private office-based practices (83% in solo, group or hospital owned private practice or HMOs and other private practices). A minority practiced in what was defined as a health center/clinic (14%). Just over four in ten (46%) OBGYNs work in medium size practices with 4-10 clinicians, and the majority practice in urban/suburban locations (90%). Half (54%) practice in states where abortion is available under most circumstances, 25% in states with pre-viability gestational restrictions, and 21% in states where abortion is banned.