As an increasing share of older adults have adopted digital health technologies over the past several years, and with most expressing interest in using them to manage their health care, the Centers for Medicare & Medicaid Services (CMS) has introduced several initiatives to expand the use of digital health technologies in Medicare. Broadly speaking, these technologies include health-related applications (“apps”), online patient portals, and connected devices such as smartphones and wearable devices that can be used to measure or track health data.
A central component of CMS’s efforts in this area is the Health Tech Ecosystem, launched in 2025, through which CMS partners with private-sector organizations, including health care providers, payers, health app developers, and electronic health record vendors, to increase the availability of digital health tools and improve access to and exchange of electronic health information. While the initiative spans all CMS programs, people with Medicare gained access to the first wave of personalized health apps through the new Medicare app Library launched in April 2026, which allows beneficiaries to access third-party apps that have undergone independent review and meet certain requirements for privacy and security.
Separately, CMS introduced the ACCESS Model, a new Center for Medicare and Medicaid Innovation payment model scheduled to begin in July 2026 that aims to expand access to technology-enabled care for people in traditional Medicare with certain chronic conditions. CMS also enhanced the Medicare Plan Finder, the official online tool on Medicare.gov that helps beneficiaries compare and select Medicare coverage options.
This brief summarizes these digital health initiatives and draws on data from various surveys, including KFF Tracking Polls from September 2025 and March 2026, to highlight facts about recent experiences with and use of digital health tools among Medicare beneficiaries and older adults more generally.
The CMS Health Tech Ecosystem Aims to Expand Access to Patient-Facing Apps and Improve Health Data Exchange
As part of the CMS Health Tech Ecosystem, dozens of companies have pledged to develop patient-facing apps that support exchange of health data and enable connectivity to the new Medicare App library, where people with Medicare can access third-party apps that meet CMS’s privacy and security criteria. To support the use of these tools, participating app developers, health information networks, electronic health record vendors, and payers have agreed to adopt common standards that make it easier for patients and providers to access and exchange electronic health information through the apps. The Medicare App library that launched in April 2026 will feature apps that meet one of the following initial use cases:
- Supporting management and prevention of diabetes and obesity, such as features that enable medication management or include resources related to prediabetes.
- Integrating conversational artificial intelligence (AI) assistants to help people navigate their care options and manage aspects of their health care, such as checking symptoms.
- Allowing patients to securely share their health and identity information electronically at check-in instead of completing paper forms (so-called “kill the clipboard” apps). Patients can also receive a summary of their visit through the same platform.
As of June 2026, the Medicare app library lists five apps that are available to beneficiaries and an additional eight apps that are expected to be added soon. A search tool on the app library website enables a comparison of apps based on 13 key features, such as managing health records, connecting to wearable devices, or sharing information with caregivers or providers, as well as searching for apps tailored to a range of health conditions and by price, with some apps being free and others requiring a subscription or having paid features.
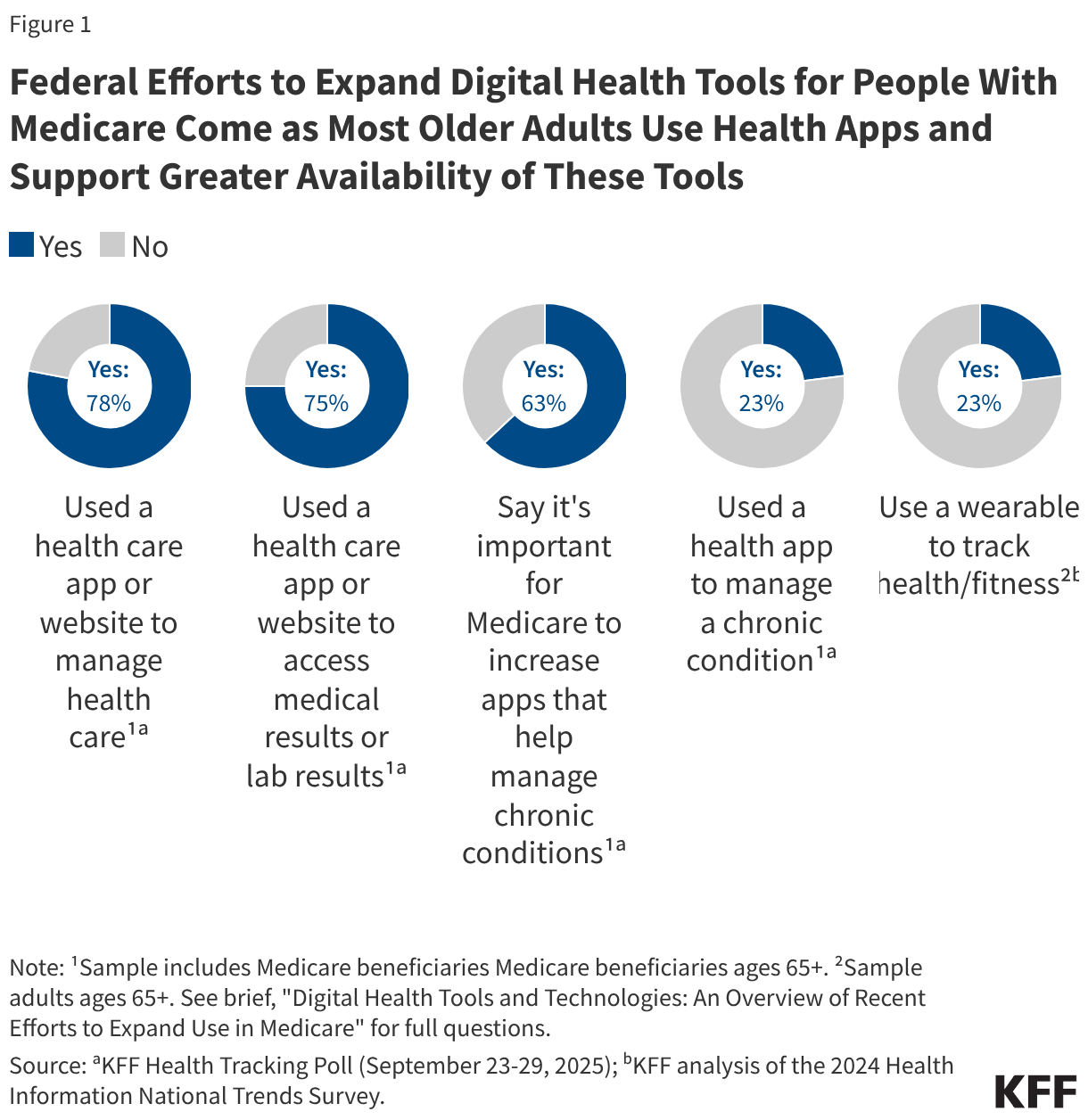
CMS’s efforts to expand the availability of health care apps that have been vetted by the agency and meet specified standards for privacy and security build on the popularity and appeal of these tools, including among older adults.In 2025, eight in 10 (78%) Medicare beneficiaries ages 65 and older used a health care app or website to manage their health care in the past year, and more than half (58%) said these tools make managing their health care easier, according to a September 2025 KFF Health Tracking Poll (Figure 1). Three-quarters (75%) say they have used a health care app or website to access their medical records or lab results, the most common reported use of health apps among Medicare beneficiaries.
In addition, nearly two-thirds (63%) of older adults on Medicare say it’s important for Medicare to increase the availability of apps that help manage chronic conditions with the help of a health care provider, but few older adults on Medicare—about one in four (23%)— say they have used a health app or website in the past year to manage a chronic condition with their health care provider.
The ACCESS Model Expands Access to Technology-Enabled Care for People in Traditional Medicare with Certain Chronic Conditions
The CMS Innovation Center launched the ACCESS Model in December 2025 to test a national, voluntary payment approach that uses technology-supported care options to help traditional Medicare beneficiaries prevent and manage a specified set of chronic conditions. These chronic conditions are grouped into an initial set of four clinical tracks, two of which target cardiovascular, kidney, or metabolic conditions (e.g., hypertension, diabetes), one that targets musculoskeletal conditions (e.g., chronic musculoskeletal pain), and another that targets behavioral health conditions (e.g., depression). About 7 in 10 Medicare beneficiaries have conditions that qualify for at least one track, though this estimate may change as CMS considers additional conditions and clinical tracks in the future.
The model is voluntary for both participating organizations and people in traditional Medicare, who need to enroll directly with participating organizations or through a referral from their provider. It will run for 10 years from July 2026 through June 2036, with organizations joining in cohorts on a rolling basis throughout the model period. Medicare beneficiaries may disenroll or switch participating organizations after 90 days of their enrollment, and participating organizations may withdraw with advance notice to CMS and beneficiaries.
To date, 190 organizations have been accepted as participants, including digital health companies, mental health organizations, health systems, and physician groups, most of which, according to CMS, have not previously served Medicare beneficiaries. These participants, who must enroll as Medicare Part B providers or suppliers, will receive monthly payments for managing beneficiaries’ qualifying conditions, with full payment tied to achieving certain health outcomes, such as helping a beneficiary with hypertension lower their blood pressure to a specific level. Currently, the vast majority of accepted applicants (151 organizations) have signed up for at least one of the two tracks focused on cardiovascular, kidney, or metabolic conditions, while 108 have signed up for the track on behavioral health conditions and 76 for the musculoskeletal track. Because organizations can participate in multiple tracks, these categories are not mutually exclusive.
Currently, it is unclear how broadly individual participants will operate geographically or the scope of services offered by each participant. CMS plans to launch a public directory of all ACCESS participants in July 2026, allowing people with Medicare and their providers to identify participating organizations, the conditions they treat, with risk-adjusted outcome measures for each organization expected to be added beginning in 2028. Organizations that participate in the model and also pledge to join the Health Tech Ecosystem will also be featured in the Medicare App Library as participants.
Participating organizations may use a variety of digital tools to deliver services under the Model, ranging from FDA-regulated medical devices such as continuous glucose monitors, to mobile applications, wearables, and non-FDA regulated software. CMS gives participants flexibility in selecting technologies and clinical tools that support the model. Some tools may be classified as clinical devices, including continuous glucose monitors, blood pressure cuffs, and wearable devices such as fitness trackers and smartwatches. Beneficiaries may receive these tools on either a loan or ownership basis from the participating organization or use their own devices. While participants generally may not require beneficiaries to purchase or rent devices classified as clinical, beneficiaries may still need access to non-clinical technologies, such as internet access, tablets, or smartphones to use technology-enabled services.
Variation in the technologies used under the ACCESS Model, as well as Medicare beneficiaries’ access to and familiarity with digital tools, may lead to differences in how people in traditional Medicare access and experience technology-supported care under this model. For example, some beneficiaries may enroll with participating organizations that incorporate the use of technologies already integrated into their care, such as Medicare-covered continuous glucose monitors. Others may enroll with participating organizations that incorporate technologies such as wearable fitness trackers that are generally not covered by Medicare and may be less widely adopted among beneficiaries. For example, in 2024, just under a quarter (23%) of adults ages 65 and older used an electronic wearable device to monitor or track their health or activity in the past year, based on KFF analysis of the Health Information National Trends Survey (Figure 1). However, among older adults who use wearable devices, the vast majority (85%) said they would be willing to share data from their device with their health care providers.
Medicare Advantage enrollees, who account for more than half of all Medicare beneficiaries, do not qualify for the ACCESS Model, but 16 insurers, including those serving Medicare Advantage enrollees, have pledged to adopt similar models of care to date. Many Medicare Advantage enrollees report having conditions being targeted by the ACCESS Model, including hypertension (64%), diabetes (35%), and depression (28%), based on a KFF analysis of the 2023 Medicare Current Beneficiary Survey (MCBS). Because details about the programs pledged by the 16 insurers are not yet available, it is unclear how they will be structured or the patient populations that will be targeted, though they may resemble existing supplemental benefits offered by Medicare Advantage plans. In 2026, 44% of enrollees are in individual Medicare Advantage plans that offer remote access technologies, which may include clinical devices such as continuous glucose monitors, and 95% are in plans that offer fitness benefits, which may include discounts on wearable devices. For example, some plans offered by Devoted Health, which has pledged to align with ACCESS, offer partial reimbursement for the purchase of a wearable device as part of a fitness benefit. While CMS collects data on use and spending on supplemental benefits in Medicare Advantage plans, such as the number and characteristics of enrollees who use these benefits, this data is currently unavailable to researchers and consumers.
Changes to the Medicare Plan Finder Could Make It Easier to Compare and Select Medicare Coverage Options
In 2025, CMS announced enhancements to the Medicare Plan Finder, the official tool on the Medicare.gov website that helps beneficiaries compare and select Medicare coverage options. These enhancements include the following updates:
- Offering Medicare Advantage provider directory information to help beneficiaries identify whether their doctors are in a plan’s network. Unlike traditional Medicare, most Medicare Advantage insurers use provider networks, which can change from year to year. Medicare beneficiaries say having access to their preferred providers is an important factor when selecting their Medicare coverage, yet in 2022, Medicare Advantage enrollees were in a plan that included just under half (48%) of all physicians available to traditional Medicare beneficiaries in their area. Prior to 2025, the Medicare Plan Finder did not include data on provider networks, resulting in beneficiaries’ going to each plan’s website or third-party sources to determine whether their preferred providers were in the network. Incorporating provider directory information in the Medicare Plan Finder may make it easier for beneficiaries to evaluate their coverage options, though the usability and completeness of this feature continue to evolve.
- Showing additional details on more than 30 supplemental benefits under Medicare Advantage. These details include in-network and out-of-network cost sharing amounts, whether prior authorization is required for each benefit, and whether there are limits on how much the plan will provide. Currently, most Medicare Advantage enrollees are in plans that offer supplemental benefits not covered by traditional Medicare, such as vision, hearing, and dental, and beneficiaries highlight the availability of extra benefits as a reason they choose to enroll in Medicare Advantage plans.
CMA also announced the launch of an “AI-powered” prescription drug search tool that will provide personalized cost comparisons across pharmacies. While prescription drug costs covered under Medicare Part D, including premiums and deductibles, can change from year to year and vary by plan, most enrollees in Medicare Advantage prescription drug plans (81%) and stand-alone prescription drug plans (69%) in 2023 did not compare their plans’ drug coverage with drug coverage offered by other plans in their area. According to CMS, the new prescription drug search tool will be available on Medicare.gov to users with an individual account but will not be incorporated in the Medicare Plan Finder. This tool could provide more individualized guidance to help Medicare beneficiaries lower their prescription drug costs beyond the prescription drug lookup tool that is already incorporated in the plan finder.
However, these enhancements will require beneficiaries to access the Medicare website and navigate the plan finder, even as just over half (53%) of Medicare beneficiaries said they hadn’t visited the Medicare website, according to KFF analysis of the 2023 MCBS, and it is unknown how many beneficiaries have used the Medicare Plan Finder specifically to compare coverage options or enroll in a plan. But with less than a third (28%) of Medicare beneficiaries comparing their coverage options during a previous open enrollment period for Medicare, enhancements to Medicare Plan Finder and Medicare.gov may help address some of the challenges beneficiaries face when evaluating their coverage options and comparing costs.