Proposed Medicaid Federal Match Penalty for States that Cover Undocumented Immigrants with Their Own Funds: State-by-State Estimates

Introduction
The House reconciliation bill will substantially reduce federal Medicaid spending and coverage and increase the number of uninsured according to estimates from the Congressional Budget Office (CBO). The bill includes a provision that seeks to reduce federal Medicaid funding to states as a penalty for providing coverage to undocumented immigrants with their own state funds. Specifically, the bill proposes reducing the federal matching rate for the Affordable Care Act (ACA) Medicaid expansion population from 90% to 80% for states that either provide health coverage or financial assistance to purchase health coverage to individuals who are not lawfully residing in the United States. Pending changes to the bill would further expand the penalty to states that have taken up options in Medicaid and/or CHIP to expand coverage for lawfully residing children and/or pregnant women.
KFF data show that 14 states plus DC cover children regardless of immigration status, including 7 states plus DC who cover at least some adults regardless of status, that would be affected by the provision. In Utah and Illinois, the provision could result in federal funding and coverage losses for the entire ACA Medicaid expansion population, since the states have “trigger” laws that require them to terminate the expansion if federal funding decreases. An additional 19 states have taken up options to expand coverage for lawfully residing children and/or pregnant people in Medicaid and/or CHIP that could be affected by the pending expansion of the penalty; some of these states also have laws that would require termination of the Medicaid expansion if federal funding decreases.
This analysis examines the potential impacts of this policy change on state Medicaid spending, including state-by-state estimates of potential losses in federal financing (and increases in state spending) if states maintain their programs. It also presents enrollment data for state-funded coverage programs to estimate the number of people who may be at risk for coverage losses if states eliminate their programs based on KFF analysis of publicly available state enrollment data, budget documents, and media reports.
If states maintained their coverage programs, they would need to find ways to offset the loss of federal funding. This could include increasing state tax revenues, decreasing spending on non-Medicaid services such as education, or making other Medicaid cuts. If states eliminated their programs, there would likely be increased uninsured rates and barriers to care for immigrant families and negative impacts for the U.S. economy and workforce due to the role immigrants play.
Potential Impacts on State Spending if States Maintain Their
State-Funded Coverage Programs
The analysis assumes that, starting in FY 2027, expenditures for people eligible in the ACA Medicaid expansion would be matched at 80% instead of 90% in the 14 states and DC that offer coverage for people regardless of immigration status. This analysis does not make assumptions about specific state behavior and instead illustrates the potential impact on state Medicaid spending if all states maintained their undocumented coverage in response to this policy change. CBO projects that this provision will result in federal savings of $11 billion between 2025 and 2034 and a coverage loss of 1.4 million people, though CBO’s estimates account for assumptions about state behavioral responses and other secondary effects.
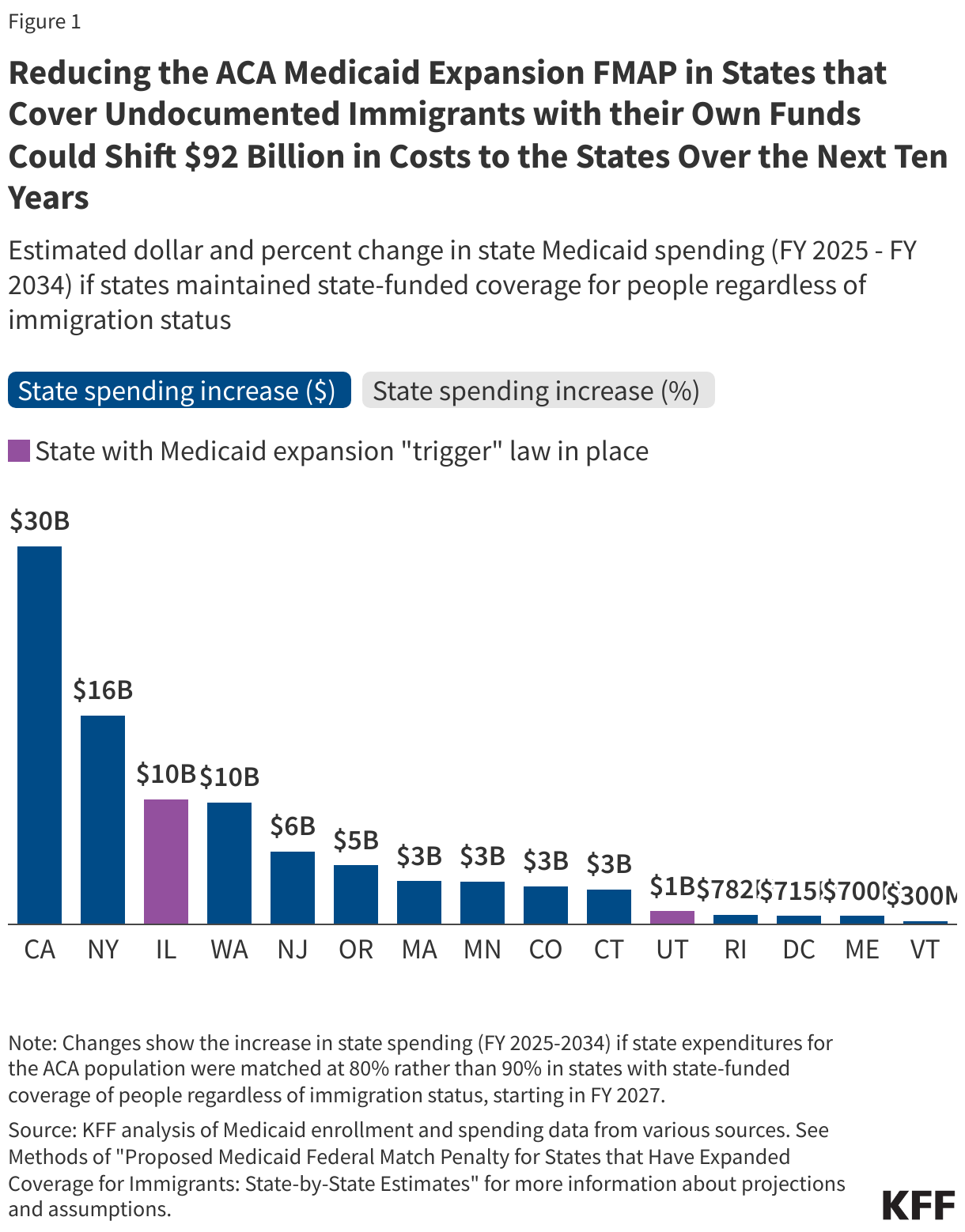
If the 14 states and DC maintain their state-funded coverage for people regardless of immigration status, a reduction in the expansion match rate or “FMAP” could shift $92 billion in costs from the federal government to the states over the next ten years. State Medicaid spending increases across the states range from $30 billion in California to $300 million in Vermont or from 8% in Oregon and Washington to 3% in Massachusetts, Vermont, New York, and Minnesota.
If states maintained their undocumented coverage, they would need to find ways to offset the loss of federal funding. This could include increasing state tax revenues, decreasing spending on non-Medicaid services such as education, which is the largest source of expenditures from state funds, or making other Medicaid cuts. Given the size of the federal Medicaid funding cuts in the reconciliation bill, states would likely face substantial challenges in efforts to replace the loss of federal funds and significant pressure to drop their current coverage of undocumented immigrants.
In addition, there would be large Medicaid spending and enrollment declines in Utah and Illinois if their ACA expansion coverage was eliminated per their current state “trigger” laws. Utah and Illinois are 2 of 12 states that have laws in place that automatically end expansion if the federal match rate were to drop, meaning the provision could result in funding and coverage losses for the entire ACA Medicaid expansion population in these states. Prior KFF analysis found that if states drop their ACA Medicaid expansion coverage altogether 78,000 (or 23% of Medicaid enrollees) could lose coverage in Utah and 840,000 (or 28% of Medicaid enrollees) could lose coverage in Illinois by FY 2034. This would result in a decrease of about $11 billion in federal Medicaid spending in Utah and $96 billion in Illinois over a ten-year period. It’s likely many of these expansion enrollees would become uninsured and gains in financial security, access to care, and health outcomes associated with Medicaid expansion would be reversed.
Potential Impacts on Coverage if States Eliminate Their State-Funded Coverage Programs
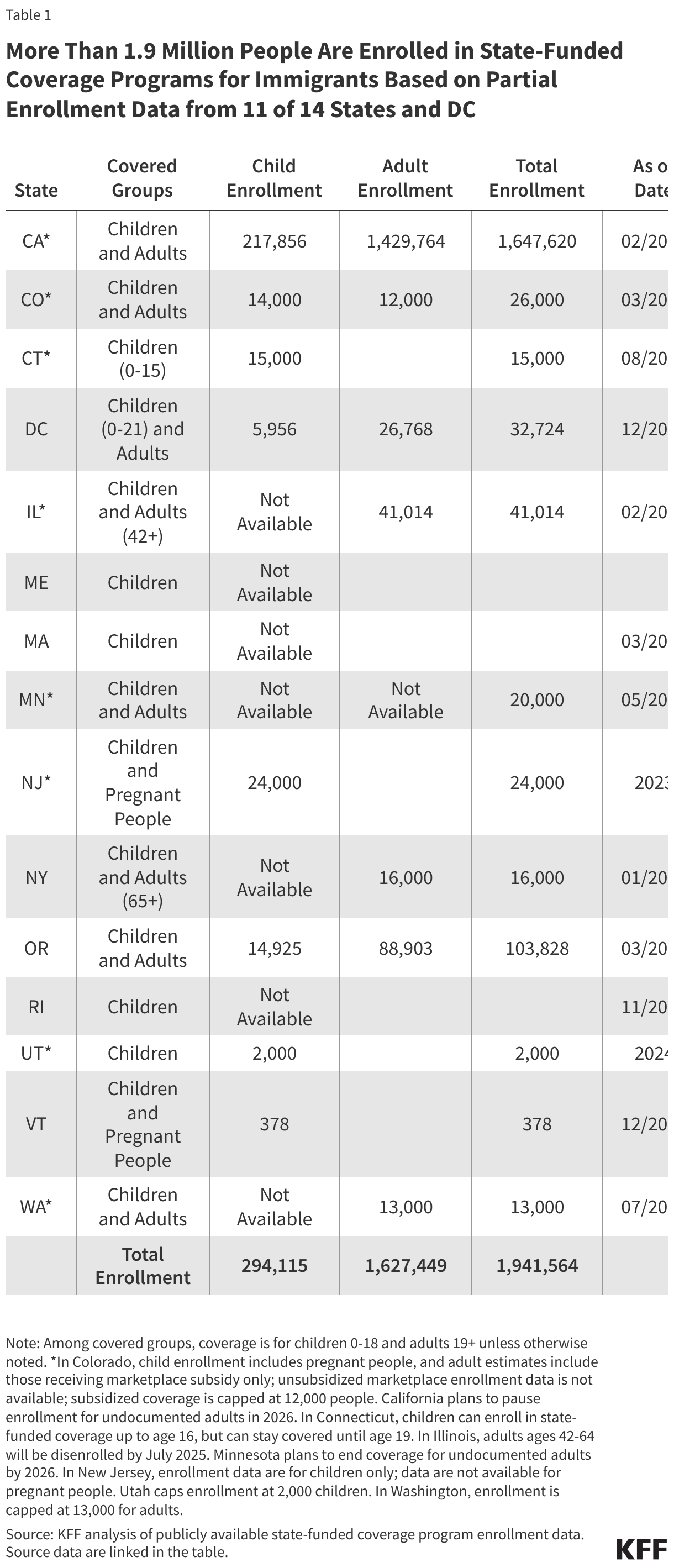
More than 1.9 million people could lose their health coverage if states eliminate their coverage in response to the penalty. About 1.9 million people are enrolled in state-funded coverage programs for immigrants based on enrollment data from 7 of the 14 states providing coverage to children and DC and 6 of the 7 states and DC providing coverage to at least some adults (Table 1). This includes roughly 1.6 million adults and about 300,000 children, although data are not available from six states that cover children (Illinois, Maine, Massachusetts, New York, Rhode Island, and Washington) and Minnesota does not report separate data for adults and children. As such, these data undercount the number of people enrolled in these programs and at risk for coverage losses. Moreover, the dates of the enrollment data vary across states. As noted, CBO estimates that 1.4 million people would become uninsured by 2034 due to this provision; this estimate represents a different time period than these enrollment data and makes assumptions about state behaviors in response to the provision.
If states eliminate their programs, there would be no federal savings, but there would likely be increases in the uninsured rate and barriers to accessing care among immigrant families. Although most immigrants are working, they are often employed in jobs that do not offer employer-sponsored health coverage and undocumented immigrants are prohibited from enrolling in federally funded coverage options. As such, without these programs most will not have access to an affordable coverage option and become uninsured. People who are uninsured often delay or go without needed care, which can contribute to health conditions becoming worse and more costly. Reduced coverage and access to care may also negatively impact the U.S. economy and workforce due to lost productivity since immigrants play an outsized role in many occupations including health care, construction, and agriculture.
Methods |
State spending estimates under the proposed policy change follow the methods outlined in a prior KFF analysis, with a few exceptions:
To determine the cost shift to states, the analysis calculates the difference in state Medicaid spending under the proposed policy change and KFF’s baseline projections of state Medicaid spending over the next ten years. |