Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender (LGBT) Individuals in the U.S.
Executive Summary
Lesbian, gay, bisexual, and transgender (LGBT) individuals often face challenges and barriers to accessing needed health services and, as a result, can experience worse health outcomes. These challenges can include stigma, discrimination, violence, and rejection by families and communities, as well as other barriers, such as inequality in the workplace and health insurance sectors, the provision of substandard care, and outright denial of care because of an individual’s sexual orientation or gender identity.1 ,2 ,3
While LGBT individuals have many of the same health concerns as the general population, they experience certain health challenges at higher rates, and also face several unique health challenges. In particular, research suggests that some subgroups of the LGBT community are more likely to suffer from certain chronic conditions and face higher prevalence and earlier onset of disabilities compared to heterosexuals. Other major health concerns include HIV/AIDS, mental illness, substance use, and sexual and physical violence. In addition to the higher rates of illness and health challenges, some LGBT individuals are more likely to experience challenges obtaining care. Barriers include gaps in coverage for certain groups, cost-related hurdles, and stigma, including poor treatment from health care providers.
Several recent changes within the legal and policy landscape have served to increase access to care and insurance for LGBT individuals and their families. Most notably these include the passage of the Affordable Care Act (ACA) and the Supreme Court’s overturning of a major portion of the Defense of Marriage Act (DOMA) in United States v. Windsor and subsequent ruling in Obergefell v. Hodges legalizing same-sex marriage nationwide. The ACA expands access to health insurance coverage for millions, including LGBT individuals, and contains specific protections related to sexual orientation and gender identity, although recent actions taken by the Trump Administration have sought to scale back some of these gains. The Supreme Court’s 2013 ruling on DOMA resulted in federal recognition of same-sex marriages for the first time and paved the way for recognition in many more states and its 2015 decision in Obergefell ruled that the Fourteenth Amendment requires a state to license same-sex marriages and to recognize such marriages performed out-of-state, thereby further expanding access and coverage across the country.
This issue brief provides an overview of what is known about LGBT health status, coverage, and access in the United States, and reviews the implications of the ACA, the Supreme Court rulings on marriage equality, and other recent policy developments for LGBT individuals and their families going forward.
Issue Brief: The Lgbt Community
While there is no single definition of the “LGBT community” – indeed, it is a diverse and multidimensional group of individuals with unique identities and experiences, and variations by race/ethnicity, income, and other characteristics – LGBT individuals share the common experience of often being stigmatized due to their sexual orientation, gender identity, and/or gender expression.4 In its landmark 2011 report, The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding, the Institute of Medicine defines sexual orientation as “an enduring pattern of or disposition to experience sexual or romantic desires for, and relationships with, people of one’s same sex, the other sex, or both sexes.”5 This definition incorporates elements of attraction, behavior, and identity. It is important to note that for some individuals, their sexual identity does not necessarily fall into any specific category but, rather, exists along a spectrum. In addition, not all persons who engage in same-sex behavior or experience same-sex attraction identify as lesbian, gay, or bisexual.
Gender Identity refers to “an individual’s internal sense of being male, female, or something else. Since gender identity is internal, one’s gender identity is not necessarily visible to others.”6 Additionally, gender expression and gender role conformity further describe the extent to which a person does or does not adhere to expected gender norms and roles. Transgender refers to individuals whose sex at birth is different from their identity as male, female, or elsewhere along the gender spectrum. People who identify as transgender may live their lives as the opposite gender, and may seek prescription pharmacologic therapy and/or surgical transformation. Transgender people may identify as heterosexual, lesbian, gay, or bisexual, or somewhere else along the spectrum of sexual identity.
Lastly, while sexual orientation and gender identity are important aspects of an individual’s identity, they interact with many other factors, including sex, race/ethnicity, and class. The intersection of these characteristics helps to shape an individual’s health, access to care, and experience with the health care system.
Population Characteristics
Assessing the health needs and barriers to care of the LGBT population has been challenging due to the historical lack of data collection on sexual orientation and gender identity. While some health surveys have asked about sexual orientation, it has not been routine to collect and analyze data on sexual orientation and gender identity in major health surveys, particularly nationally representative ones, meaning that much of the data available to date have been from smaller, non-representative studies and convenience samples. Where data have been collected, they have mostly focused on same-sex couples using data systems that collect information on relationship status.7 In addition, where data are available for individuals, there is more information about lesbian, gay, and bisexual persons than transgender individuals (sometimes due to design and other times due to sample limitations). There has been growing recognition of the need for research focused on the LGBT community, and the ACA instituted new federal data collection requirements on disparities, which include sexual orientation and gender identity (described below). The National Health Interview Survey (NHIS), a nationally representative survey and the principal source of information on the health of the U.S. population, began including a question on sexual orientation in its 2013 survey and the first round of findings were released in July 2014.
The latest data available on the size and characteristics of the LGBT population are as follows:
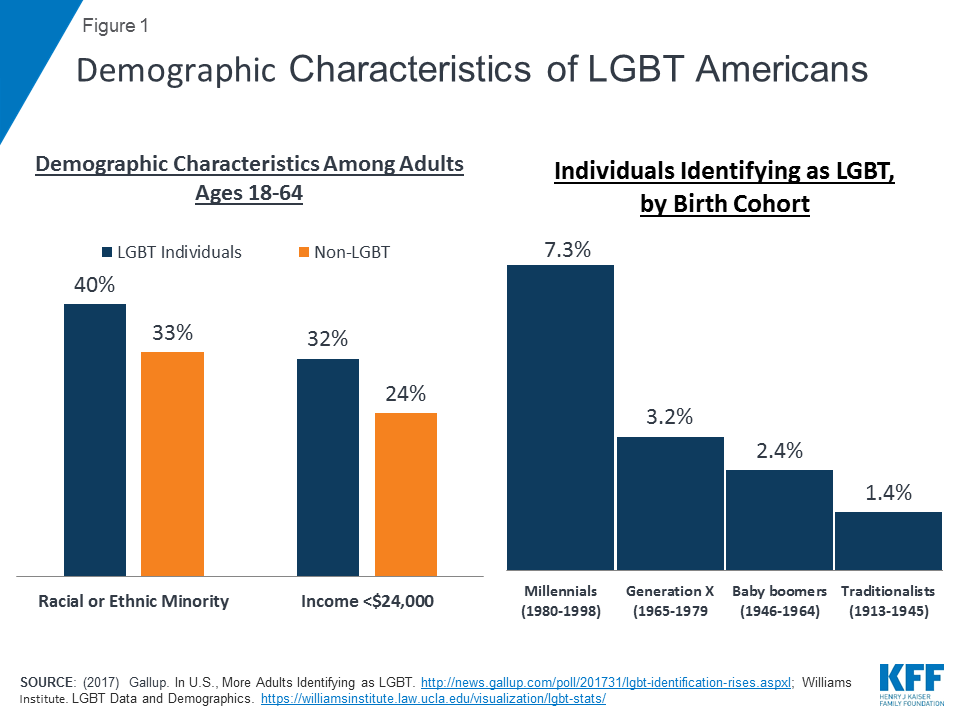
- Data on the size of the LGBT population in the United States range. The most recent data from the NHIS indicate that 2.8% of adults ages 18 and older in the U.S. identify as lesbian, gay, or bisexual, equating to more than 5.5 million people.8 Recent Gallup poll data have found slightly higher rates of LGBT identification of 4.1%, or about 10 million adults.9 Estimates may vary due to differing methodologies for data collection. Most of these surveys include only those who self-identify as LGB10 and do not include those who may have engaged in same-sex behavior or have same-sex attraction but do not identify as gay, lesbian, or bisexual. Other studies have looked beyond self-identification, to include behavior and attraction, and obtained higher estimates, including one that found that 10% of adults reported experience with same-sex partners.11 In addition, a recent analysis indicates that standard survey measures appear to significantly underestimate non-heterosexual identity and same-sex sexual experiences.12
- Racial and ethnic minorities, young people, and women are more likely than their counterparts to identify as LGBT (Figure 1).13
- The Youth Risk Behavior Surveillance System (YRBSS), a nationally representative survey of high school students, asks about sexual identity and sex of sexual contacts. It found that in 2015, 8% of high school students identified as LGB and 6.3% had same sex sexual contact. Demonstrating that sex of sexual contacts is not always an indication of sexual identity, among students who said they had sexual contact only with partners of the same-sex or both sexes, 25% identified as heterosexual.14
- Data on those who identify as transgender are limited but a recent study found that an estimated 0.6% of the U.S. population is transgender, equating to approximately 1.4 million people.15
- Estimates of self-identified LGBT individuals also vary by state. According to a 2017 Gallup poll, the share of adults who identify as LGBT ranges from a low of 2.0% in South Dakota to a high of 8.6% in the District of Columbia (followed by 5.3% in Vermont).16 This range could reflect local policies and societal attitudes regarding LGBT equality, which may be correlated with an individual’s willingness to self-identify as LGBT or live in a certain locale.
- Nearly one quarter (23%) of LGBT individuals indicate they are married (including those in opposite-sex and same-sex marriages).17 The share reporting that they are married to a same sex spouse has risen over time, from 7.9% in 2015, in the months prior to the Supreme Court’s Obergefell decision, to 10.2%, two years after the decision.18
- According to the 2016 American Community Survey, a smaller share of same-sex couples (17%) is raising children compared to heterosexual couples (39%). A greater share of female couples (23%) are raising children compared to male couples (10%).19
- Compared to the general population, LGBT people are disproportionately poor overall, although there is variation between subgroups. A 2013 Pew Research poll of LGBT individuals found that about 4 in 10 (39%) earned $30,000 or less per year, compared to 28% of the U.S. population overall.20 Poverty rates on average are higher among lesbian and bisexual women, young people, and African Americans.21 According to an analysis of the 2006-2010 National Survey of Family Growth, more than one-quarter (28%) of lesbian and bisexual women are poor, compared with 21% of heterosexual women. Just over 1 in 5 gay and bisexual men (23%) are poor, compared to 15% of heterosexual men. However, when comparing couples, lesbian couples have the highest poverty rates, followed by heterosexual couples and male same-sex couples. Further, a 2015 survey of 27,715 transgender people from across the U.S. found that one-third (32%) of respondents had an annual income of less than $10,000 compared to 23% of the US population.22
Issue Brief: Health Challenges
Health is shaped by a host of social, economic, and structural factors.23 For LGBT individuals, these factors include the experience and impact of discrimination, stigma, and ostracism which affect health outcomes, access, and interaction with the health system care.24 ,25 , 26 Research available to date finds that while LGBT people have many of the same health concerns as the general population, they experience some health challenges at higher rates, and face several unique health challenges.
Chronic Conditions
Studies have found that LGBT people experience worse physical health compared to their heterosexual and non-transgender counterparts.27 , 28
- A recent literature review found that self-identified LGB individuals are more likely than heterosexuals to rate their health as poor, have more chronic conditions, and have higher prevalence and earlier onset of disabilities. Overall, LGB people report more asthma diagnoses, headaches, allergies, osteoarthritis, and gastro-intestinal problems than heterosexual individuals.29
- Additionally, there are differences between subgroups within the LGBT community. Lesbian and bisexual women report poorer overall physical health and higher rates of asthma, urinary tract infections, and Hepatitis B and C than heterosexual women. Lesbian and bisexual women also report heightened risk for and diagnosis of some cancers and higher rates of cardiovascular disease diagnosis. Similarly, gay and bisexual men report more cancer diagnoses and lower survival rates, higher rates of cardiovascular disease and risk factors, as well as higher total numbers of acute and chronic health conditions such as headaches and urinary incontinence than heterosexual men.30
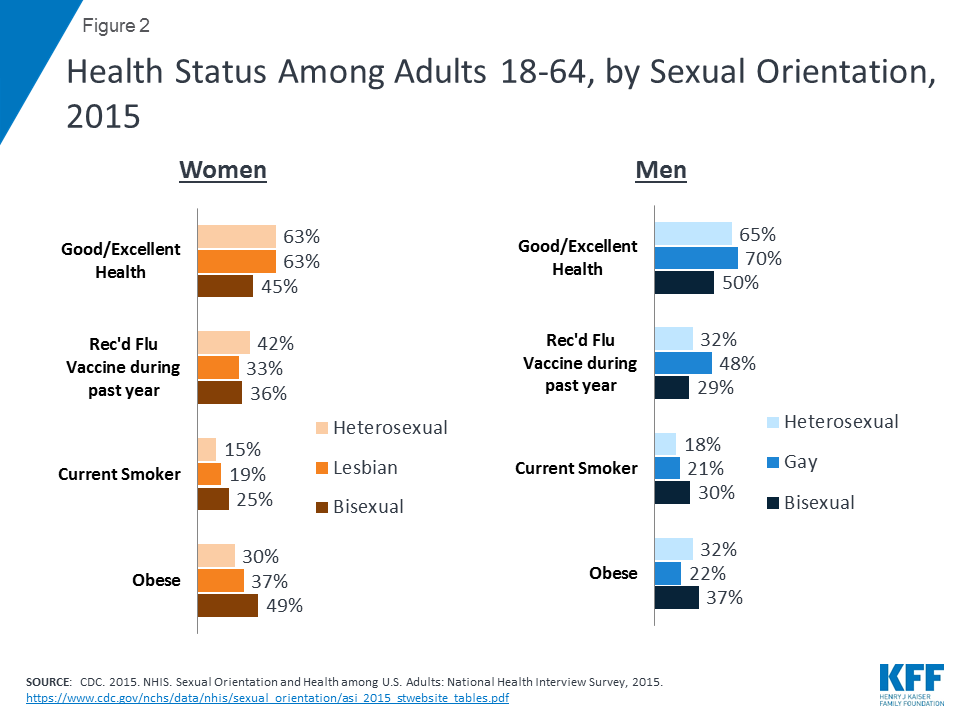
- According to data from the NHIS, fewer bisexual women reported excellent or very good health compared to heterosexual women and lesbians. Similarly, fewer bisexual men reported good/excellent health compared to gay or heterosexual men. (Figure 2)31 In a separate survey, fewer transgender individuals report very good or excellent health than the rates found in NHIS for LGB people.32 Similarly, a study of Massachusetts residents, transgender persons are the least likely among LGBT individuals to self-report their health as Excellent or Very Good (67% vs. 79%) and are twice as likely to report limitations in daily activities due to impairment of health problems (33% vs. 16%).33
- LGB individuals on average have higher rates of some risk factors for chronic illnesses. Obesity rates are higher among lesbian and bisexual women compared to heterosexual women, but are lowest among gay men. However, there were no significant differences by sexual orientation for women or men in rates of meeting physical activity guidelines.
HIV/AIDS and Sexually Transmitted Infections (STIs)
One of the most significant health challenges facing the LGBT community has been the HIV/AIDS epidemic’s impact on gay and bisexual men, and transgender women. After experiencing a dramatic rise in new infections in the 1980s, efforts by the gay community and public health officials helped to bring HIV incidence down; however, in recent years, new infections among gay and bisexual men in the U.S. have been on the rise, the only group for which infections are increasing (Figure 3).
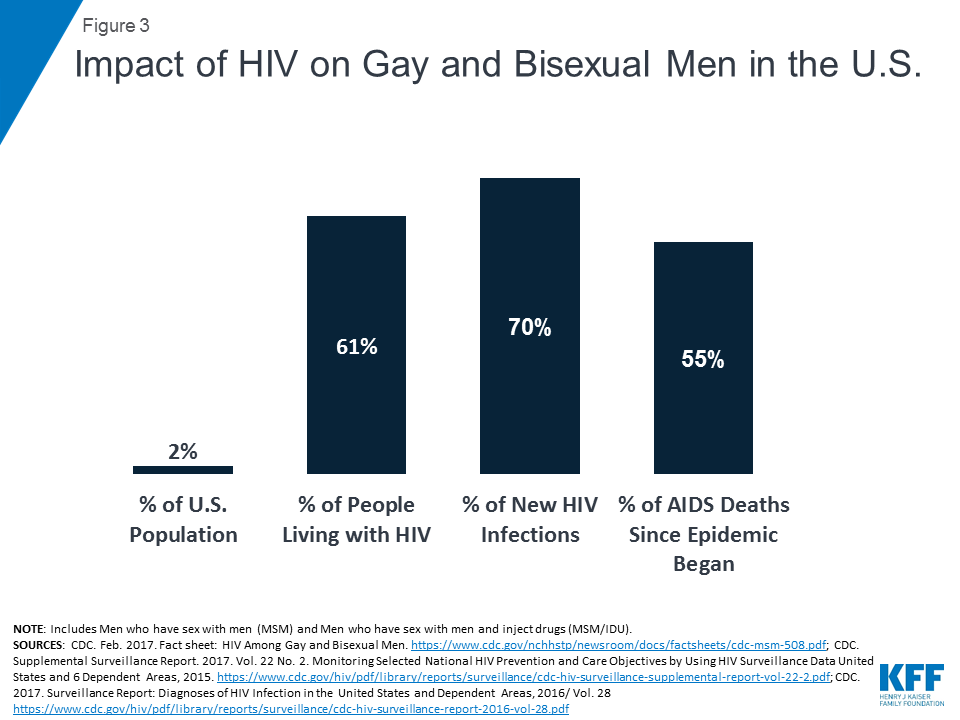
- In 2014, gay and bisexual men and other men who have sex with men (MSM), while representing an estimated 2% of the U.S. population, accounted for six in ten (61%) people living with HIV in the United States, and 70% of new HIV infections.34 ,35
- Between 2008 and 2014, annual HIV infections stabilized among all MSM but this trend was not observed among all racial/ethinic groups. HIV infections declined 18% among white MSM (from 9,000 to 7,400 infections), stabilized among black MSM (about 10,000 infections per year) but increased by 20% among Latino MSM (from 6,100 to 7,300 infections).36
- Despite a stabilizing in rates, young, black MSM accounted for more new diagnoses in 2015 than any other subgroup by race/ethnicity, age and sex.37
- Transgender women, particularly transgender women of color, are also at high risk of HIV. A 2013 study estimated HIV prevalence among transgender women to be 22%.38
- The CDC recommends routine HIV screening in health-care settings for all adults, aged 13-64, and repeat screening, at least annually, for those at high risk (e.g., that sexually active gay and bisexual men may benefit from more frequent testing, such as every 3 to 6 months).39 However, according to a nationally representative survey conducted by the Kaiser Family Foundation, many do not meet this level. While seven in ten gay and bisexual men say they have gotten an HIV test at some point in their lives, just 30 percent say they were tested within the past Three in ten (30%) say they have never been tested for HIV, rising to 44% of those under age 35. The leading reason that men give for not having had a recent test is that they do not consider themselves at risk for HIV.40
- Access to medical care is critical for the health of people with HIV. Among MSM diagnosed with HIV in 2014, 61% received care and 51% achieved viral suppression.41 In addition, according to the Kaiser survey, three in ten (31%) gay and bisexual men either say they don’t have a regular place to go for medical care or they don’t have a regular physician. These men (who tend to be younger, lower-income, and more racially diverse) are also less likely to report discussing HIV with doctors or getting tested for HIV.
- To date, there has only been one likely case of female-to-female sexual transmission of HIV in the United States.42 However, HIV is an issue that affects lesbians as well as bisexual women, since individuals who identify as lesbian may still have sexual relationships with men, and lesbians and bisexual women are also at risk of HIV via transmission modes that do not involve sexual contact (such as injection drug use).
- STI rates are higher among some LGB groups than heterosexuals, and rates have been increasing for some infections. For example, MSM account for more than eight in ten (82%) new gonorrhea and primary and secondary syphilis cases when the gender of sex partner is known. In addition, antibiotic-resistant gonorrhea
- may be higher among MSM.43 MSM also account for 10% of all new hepatitis A infections and 20% of new hepatitis B infections.44 Given the strong interaction between HIV and other STIs, this is a particular concern for MSM.
- Human Papillomavirus (HPV) is the most common STI and is a major cause of cervical, anal, and mouth cancers.45 MSM are 17 times more likely to develop anal cancer than men who only have sex with women.46 The HPV vaccine, which protects against certain strains of the virus that are associated with anal cancer, could reduce anal cancer rates among future generations of MSM
Behavioral and Mental Health
Research has found that LGBT individuals are at elevated risk for some mental health and behavioral health conditions, with studies finding that they are two and a half times more likely to experience depression, anxiety, and substance misuse.47 ,48 The history of discrimination and stigma, including lack of acceptance from family members, contributes to higher rates of mental illness.49 ,50 In fact, until the 1970s, homosexuality was considered a mental illness in the Diagnostic and Statistical Manual (DSM) of Mental Disorders and by various professional organizations. The diagnosis “gender dysphoria,” which has replaced the transgender diagnosis in the DSM, is intended to communicate the emotional distress that transgender people may experience as well as promote insurance coverage of services related to gender transition, such as counseling or hormone therapy, that typically have not been covered by insurance plans51 Further, stigma and prejudice against sexual and gender minorities remain pervasive and continue to have negative consequences for the mental health of the LGBT population.52
- The recent NHIS provides the first national comparisons of gay, lesbian and bisexual adults to heterosexual adults on alcohol consumption, smoking status, and one measure of mental health status (Table 1).
- Heavy consummation of alcoholic beverages during at least one day in the past year was reported by more bisexual (47%) and gay or lesbian (36%) adults than heterosexual adults (28%). Rates among men of all sexual orientations were substantially higher than for women.
- Smoking rates were higher among LGB adults compared to heterosexuals. A separate meta-analysis of several studies found that overall, LGBT people smoke cigarettes at 1.5 to 2.5 times the rate of heterosexual and non-transgender people.53
- Nearly one in six bisexual women experienced serious psychological distress in the past 30 days, more than three times the rate of heterosexual women. Approximately 3% of heterosexual men reported experiencing serious psychological distress.
- Other studies have used state-level data or sample populations to identify mental health trends among LGBT individuals. Nearly one fifth (19%) of bisexual adults in Massachusetts report they had recently seriously considered suicide, compared to 4% of lesbian and gay adults and 3% of heterosexuals.54 There are notable differences between subgroups, with the rate highest among bisexual women (26%), followed by bisexual men (11%), gay men (6%), and approximately 3% among all other subgroups. Another nationwide study found a reported 41% prevalence of suicide attempts among the transgender population.55
- Research suggests that MSM have higher use of certain substances. One study has estimated that MSM are more than 12 times as likely to use amphetamines and almost 10 times as likely to use heroin as heterosexual men. However, it’s important to note that research in this field is older and data are not necessarily comparable to the heterosexual population.56
Sexual Assault and Physical Violence
Sexual assault and physical violence can have lasting consequences for victims, families, and communities.57 LGBT individuals experience higher rates of sexual and physical violence compared to heterosexual and non-transgender individuals. Violence toward LGBT people has led to public policy responses. For example, federal legislation as well as some state laws allow for the classification of violence based on gender identity or sexual orientation bias as a “hate crime,” which has implications for penalties as well as funding to states and locales for deterrence and surveillance of these crimes.58 Key statistics include the following:
- A recent poll of LGBT adults found that two thirds had experienced some form of discrimination because of their sexual orientation or gender identity, including subjection to slurs, rejection by a friend or family member, being physically threatened or attacked, receiving poor service at a place of business or treated unfairly by an employer, or made to feel unwelcome at a place of worship; a full 30% said they had been physically threatened or attacked.59
- Many women and men have experienced some form of sexual violence, but the rates are significantly higher among some LGBT groups. It is estimated that almost half (46%) of bisexual women have been raped, as have 17% of heterosexual and 13% of lesbian women. More than four in ten heterosexual and lesbian women and the majority (75%) of bisexual women have experienced other forms of sexual violence, such as coercion or harassment. Six in ten (61%) bisexual women have encountered intimate partner violence (IPV), as have 44% of lesbian and 35% of heterosexual women (Figure 4).60
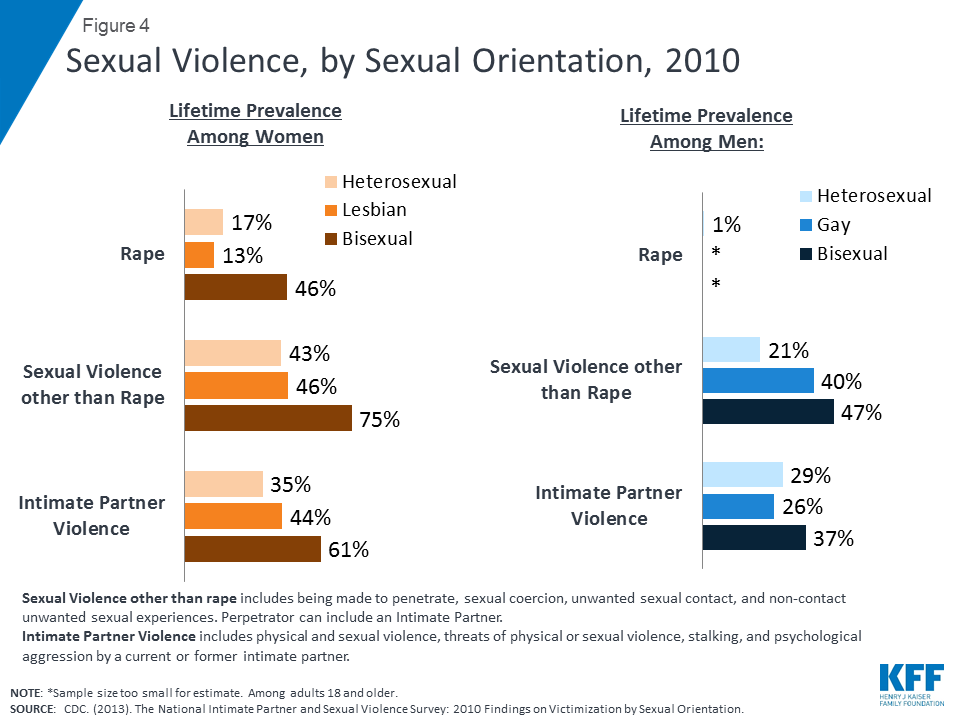
- While sexual violence rates are higher among women overall, bisexual and gay men experience significantly higher rates than heterosexual men. Four in ten gay men and nearly half of bisexual men have encountered sexual violence other than rape. More than one-third (37%) of bisexual men have faced partner violence. For both men and women, the perpetrators were predominantly male.
- Anti-LGBT bias also puts LGBT people at risk for physical violence. According to the FBI’s crime reporting surveillance, one in five single-bias incident hate crimes was due to sexual orientation bias.61 Studies using convenience samples have shown a significant number of LGBT individuals have been victims of physical and verbal assaults, as well as personal property damage, due to their sexual orientation or gender identity.62 One recent nationally representative study examined self-reported experiences with physical violence due to sexual orientation among gay men, lesbian women, and bisexual individuals, and found almost 8% of individuals have experienced physical violence once and 5.5% have experience physical violence at least twice. Gay men were the most likely to experience physical violence due to their sexual orientation.63 Transgender people, particularly transgender women and transgender people of color, are also at particular risk of physical violence.64 Statistics from the National Coalition of Anti-Violence Programs indicate that half of the victims of anti-LGBT bias-motivated murders in 2012 were transgender women and the majority were also people of color.65
Adolescent and Young Adult Health
Adolescence and young adulthood are often times when individuals begin to identify as LGBT and in fact high school students identify as LGB at higher rates than do adults in any age group.66 ,67 As mentioned above, the YRBS recently found that 89% of high school students identify as heterosexual, 2% as gay or lesbian, 6.0% bisexual, and 3% reported that they were unsure of their sexual identity.68 While these times can be challenging for many individuals, they are often especially so for LGBT youth. Despite growing societal acceptance and understanding, some young people still suffer discrimination at the hands of their family and friends and in their schools and communities, experiences which can lead to serious challenges, such as housing problems, that affect health. There is growing awareness about bullying and violence affecting LGBT youth, including dating and sexual violence. These include efforts to promote greater attention to fostering inclusive school climates, teaching youth about online safety, establishment of reporting processes in schools and communities when violence or bullying occur, and referring young people for professional mental and behavioral health services when needed. In addition, LGB high school students report engaging in some higher risk taking activities than do their heterosexual peers including with respect to actives such as drug, alcohol use and sexual behavior.69 Key statistics include the following:
- Like their adult counterparts, students who identify as lesbian, gay, or bisexual, experience higher rates of mental illness and suicidality. LGB students more likely to have felt sad or hopeless compared to their heterosexual peers (60% v. 26%), seriously considered suicide (43% v. 15%), or attempted suicide (29% v. 6%).70
- LGB students are also more likely to engage in certain risk taking activities, including having ever tried alcohol (75% v. 63%), marijuana (53% v. 38%), or cocaine (11% v. 4%). LGB students were also less likely to report condom use during last sexual intercourse than heterosexual students (48% v. 58%).71
- Like their adult counterparts, youth who identify as a sexual or gender minority experience higher rates of discrimination compared to the general population. Additionally, LGBT youth are more likely to be homeless and live in poverty than non-LGBT youth. Research has found that parental rejection can increase the likelihood that an LGBT youth will suffer from depression, attempt suicide, use illegal drugs, and/or engage in risky sexual behaviors.72
- Approximately 40% of homeless youth are LGBT, and the leading reasons for homelessness among this group are due to family rejection.73
- Almost two thirds (64%) of LGB students and 4 out of 10 (44%) transgender students report feeling unsafe at school because of their sexual orientation or gender identity.74
- LGB students experience higher rates of violence than do heterosexual students including having been threatened or injured with a weapon, been in a physical fight, or injured in a fight. The share of students who have experienced dating violence is two times higher among LGB students than heterosexual students (18% v 8%) and more than three times as many LGB youth report ever physically forced to have sexual intercourse against their will, compared to their heterosexual peers (18% vs. 5%).75
- Recent research estimates that 20,000 LGBT youth will receive conversion therapy from a licensed health care provider before the age of 18 and an additional 57,000 youth will receive “treatment” from a religious or spiritual advisor.76 This is contrary to the recommendation from professional medical organizations, including the American Psychological Association, American Medical Association, and America Association of Pediatrics, which oppose the practice citing its impact as harmful and ineffective.77
Insurance Coverage and Access to Care
Research has shown that LGBT populations have different patterns of health coverage and utilization of services and has begun to document gaps within the delivery system in meeting the needs of the LGBT population.
- While LGB individuals have similar rates of insurance coverage and uninsurance, and saw similar gains in coverage under the ACA (see below), in some cases access to care differs for this population. In particular, research finds that on some measures, bisexual individuals have more limited access to care while lesbian and gay individuals have rates comparable to heterosexual adults (Figure 5). In particular, bisexual adults fared poorer than other groups in terms of having a usual place to go for medical care and going without medical care due to cost.

- A separate 2013 survey found that among LGBT individuals estimated to have incomes under 400% of the federal poverty level (FPL), almost 4 in 10 had medical debt and more than 4 in 10 reported postponing medical care due to costs.78
- Research studies on same-sex couples find that LGB individuals have higher rates of unmet medical need because of cost and are less likely to have a regular provider. Research has also found that women in same-sex couples are less likely than heterosexual married women to have received timely medical care for both primary and specialty services. Among men in couples, gay men are three times as likely as their heterosexual counterparts to report delays in obtaining needed prescription medicines.79
- Marriage is tied to access to health insurance. Prior to the Supreme Court’s Windsor ruling, however, same sex married couples were only able to obtain coverage for their spouse as a domestic partner, if their employer provided such coverage, and these benefits were considered taxable income. Under the Windsor and Obergefell rulings, federal and state employees with same-sex married spouses are guaranteed the benefits afforded to opposite-sex married spouses but other employers may continue to elect to cover only opposite-sex married spouses (in states or localities without additional protections).
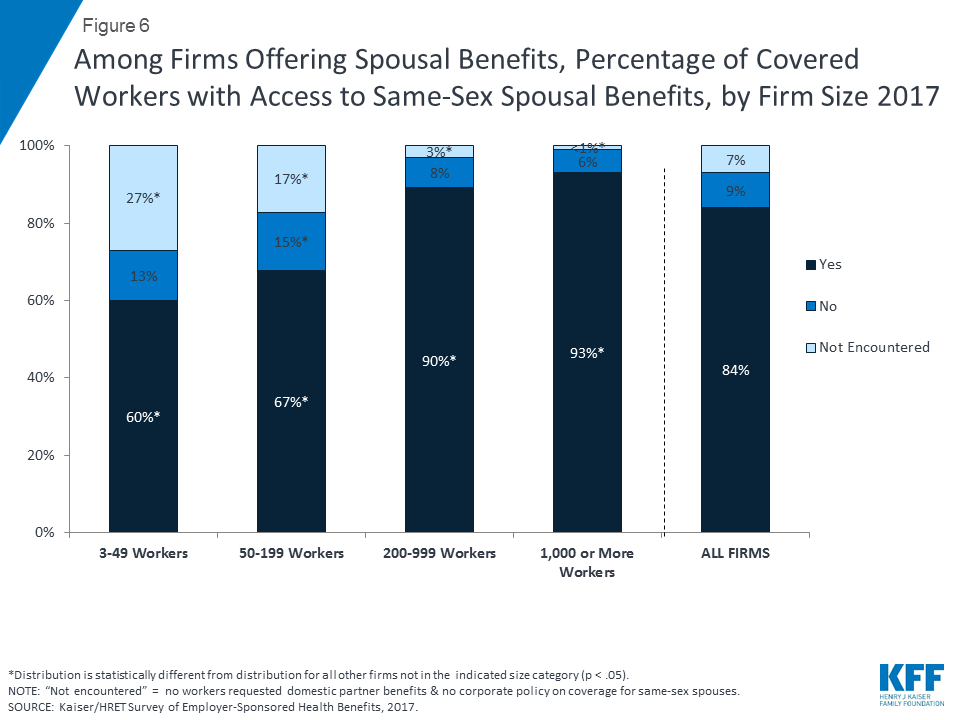
- Indeed, recent nationally representative research shows that in 2017 nearly six in ten (57%) firms that offer health benefits to opposite-sex spouses, offer coverage to same-sex spouses80 , that share is much higher (88%) among large employers (those with 200 or more workers) which is significant as most covered U.S. workers (71%) are employed by these firms.81 Because most covered workers are employed by large firms, which are more likely to offer the benefit overall, 84% of covered workers with access to opposite-sex spousal coverage also have access to same-sex spousal coverage. Almost all workers (93%) at firms with 1,000 or more employees have access to this benefit whereas fewer than two-thirds (64%) of workers at the smallest firms (between 3 and 49 employees) have access (see figure 6). 82 In addition, states have the option of enacting their own equal employment legislation protecting on the basis of sexual orientation. Beyond the requirements for state and federal employers, these Supreme Court rulings are through to have influenced the expansion of employment benefits, including health benefits, to same-sex spouses more broadly. Indeed, one study found that the legalization of same-sex marriage in New York was associated with an increase in employer-sponsored insurance among same-sex couples.83
- Some studies have found that lesbian women in couples have lower rates of breast and cervical cancer screenings than married heterosexual women.84 In addition to lower mammography rates, lesbian women on average have higher rates of some risk factors for breast cancer, including greater alcohol use and lower likelihood of childbearing. 85 ,86
- The transgender population is much more likely to live in poverty and less likely to have health insurance than the general population. Research reflects the impact of these barriers. In one survey of transgender individuals, nearly half (48%) of respondents postponed or went without care when they were sick because they could not afford it.87 In addition, many health plans include transgender-specific exclusions that deny transgender individuals coverage of services provided to non-transgender individuals, such as surgical treatment related to gender transition, mental health services, and hormone therapy.88
- An individual’s relationship with providers is another important component of access to care. Significant shares of LGBT individuals report negative experiences when seeking care, ranging from disrespectful treatment from providers and staff, to providers’ lack of awareness of specific health needs. In a survey of LGB people, more than half of all respondents reported that they have faced cases of providers denying care, using harsh language, or blaming the patient’s sexual orientation or gender identity as the cause for an illness.89 Fear of discrimination may lead some people to conceal their sexual orientation or gender identity from providers or avoid seeking care altogether.
- For transgender persons, discrimination may be as personal as refusing to use the patient’s chosen name or as structural as providers’ lack of knowledge about how to provide appropriate care to transgender people. For example, most transgender men still have a cervix and should be screened for cervical cancer, which requires a sensitive approach.90 Studies of the transgender community show that up to 39% of transgender people have faced some type of harassment or discrimination when seeking routine health care, and many report being denied care outright or encountering violence in health care settings.91 ,92
- Medical education does not routinely encompass LGBT health issues. More than half of medical schools and public health school curricula lack instruction about the health concerns of LGBT people beyond work related to HIV/AIDS.93 ,94 However, the medical community’s awareness of LGBT health needs has grown. Several professional medical societies have formed policies and guidance that advocate on behalf of fair treatment and access for LGBT patients and health providers.95 For example, the American Medical Association (AMA) has issued an explicit nondiscrimination policy as well as numerous other statements that recognize prior discriminatory practices in the medical setting, the importance of better understanding and addressing LGBT health needs, the impact of discrimination on health and well-being, and the need to include sexual orientation in research.
- The World Professional Association for Transgender Health also maintains a set of standards and principles to guide health care professionals in providing health care to transgender people.96 Additionally, in 2011, the Joint Commission, an independent non-profit national organization that accredits and certifies more than 20,000 health care organizations and programs in the U.S., began to require that hospitals prohibit discrimination based on sexual orientation, gender identity and gender
Issue Brief: Impact Of Changes In The Legal And Policy Landscape On Coverage And Access To Care
In addition to specific health needs, the health of and access to care for LGBT communities is shaped by federal and state policies on insurance, compensation and benefits, and marriage. The passage of the ACA in 2010, the Supreme Court’s ruling overturning DOMA in 2013, and subsequent ruling in Obergefell in 2015 (guaranteeing the right to same-sex marriage nationally), have significantly affected access to care and coverage for LGBT individuals and their families, expanded nondiscrimination protections, increased data collection requirements, and supported family caregiving. States and private organizations have also moved to add nondiscrimination protections and enhance coverage for LGBT individuals. While the Obama Administration supported expansion of many of these protections, the Trump Administration has sought to scale some of them back.
Impact of the ACA
The ACA makes far-reaching changes in health coverage and delivery of care for millions, including LGBT individuals. For LGBT populations, three major areas are of particular saliency: 1) expanded access to coverage and insurance market reforms, 2) “nondiscrimination” protections, and 3) requirements for data collection and research.
Coverage
- The ACA extends coverage to millions of uninsured persons through the expansion of Medicaid, in states that choose to expand, as well as the creation of new federally subsidized health insurance marketplaces in all states. In states that expanded their Medicaid programs, a new pathway to Medicaid eligibility is available based solely on income and immigration status, and is available to most individuals with incomes below 138% FPL regardless of their family or disability status. Uninsured individuals not eligible for Medicaid, can purchase coverage in insurance marketplaces, with subsidies available to most with incomes between 100% and 400% of FPL to help offset the costs of premiums. Additional subsidies are available to those between 100% and 250% FPL to help with other out-of-pocket costs.
- As of January 2014, individuals can no longer be denied most private market insurance due to a pre-existing condition, such as HIV, mental illness, or a transgender medical history. Additionally, new private plans are now required to cover recommended preventive services without cost sharing. This includes screenings for HIV, STIs, depression, and substance use. And, those who gain coverage through the Medicaid expansion or in the marketplace will have coverage for a set of essential health benefits, including prescription drugs and mental health services.
- A recent Kaiser Family Foundation study found that since implementation of the ACA, rates of uninsurance decreased significantly among LGB adults (dropping from 19% in 2013 to 10% in 2016), representing an estimated 369,000 fewer uninsured LGB individuals. In addition, Medicaid coverage increased (rising from 7% to 15% during the same period), representing an estimated 511,000 more LGB individuals with Medicaid coverage. These coverage changes were similar to those seen in the heterosexual population.97
Nondiscrimination Protections
- As described above, bias and discrimination in the health care system have been an unfortunate reality for many LGBT people.98 In addition to provider level discrimination, prior to the ACA, some policies in the insurance and financing system have disproportionately affected LGBT people, including pre-existing condition clauses permitting plans to deny insurance to people with conditions such as HIV, mental illness, or to transgender individuals, who may require specific health care services.99 Furthermore, some plans interpreted these exclusions broadly and used them to deny transgender people coverage for services that are not related to gender transition.100
- The ACA and subsequent federal regulations implementing the ACA prohibit such discrimination in many aspects of health care. For instance, federal regulations issued by the Department of Health and Human Services (DHHS) governing health insurance marketplaces101 as well as regulations governing any health plan offering essential health benefits102 bar discrimination in insurance provision based on sexual orientation and gender identity.
- The law (and implementing regulations) includes additional protections under Section 1557 including the prohibition of discrimination based on sex, defined to include gender identity and sex stereotypes, in any health program receiving federal funds (such as Medicaid, Medicare, and providers who receive federal funds). However, as part of an ongoing lawsuit, a federal court has issued an injunction halting enforcement of this provision’s protections around gender identity (and termination of pregnancy). HHS is currently reconsidering the final implementing rule that clarified these protections and has sent a draft proposed rule to OMB (a final step in the rulemaking process). Notably, while the injunction remains in place, it applies only to HHS’s authority to enforce this part of the regulation. Covered entities must still comply with the law and those that do not could be liable if someone files a discrimination claim in court under Section 1557 (rather than to seek remedy through HHS’ Office of Civil Rights (OCR)).103
- Federal regulations governing health plan marketing practices prohibit health insurance issuers offering non-grandfathered insurance coverage in the group or individual markets (including health care marketplaces) from employing marketing practices or benefit designs that discriminate on the basis of certain specified factors, including sexual orientation and gender identity.104 In 2014, the Centers for Medicare and Medicaid Services issued an FAQ105 clarifying that these regulations include coverage of same-sex married spouses. Per the FAQ, the regulations require health issuers who offer coverage to opposite-sex spouses to also offer coverage to same-sex married spouses, based on state of celebration, as of January 2015 However, the regulation does not apply to employers.
- In June 2016, CMS issues a proposed rule that would have required hospitals participating in the Medicare and Medicaid programs to establish non-discrimination policies that include prohibitions on discrimination on the basis of gender identity and sexual orientation.106 Given that the vast majority of hospitals participate in these programs, this rule could have widespread impact by extending protections on the basis of sexual orientation. This could be especially meaningful as sexual orientation protections remain unspecified under Section 1557 and because gender identity protections under 1557 are threatened by ongoing litigation. However, as of April 2018, the Trump Administration has taken no action to finalize this regulation.
- Since taking office, the Trump administration has sought to widen the availability of plans that may be exempt from key protections, including non-discrimination protections related to sexual orientation and gender identity. Of particular note, short-term limited duration (STLD) and association health plans may lack the protections or comprehensive design necessary to meet the needs of LGBT populations (and many others as well).107
- In addition, the Trump Administration has taken steps to provide conscience and religious exemptions for certain groups that could curb access to care and treatment for LGBT people. In 2018 HHS created a new unit at the HHS OCR called the “Conscience and Religious Freedom Division” with the stated purpose of protecting moral and religious convictions and issued a proposed rule aiming to ensure health care providers may refrain from participating in procedures incongruous with their moral or religious beliefs.108 LGBT advocates have said that the creation of this unit could suggest a move towards shielding healthcare workers from performing certain procedures or treating certain patients, such as transgender patients based on personal moral objections.109
Data Collection
- The ACA calls for the inclusion of routine data collection and surveillance on health disparities, which HHS and many other groups have recognized includes LGBT populations. Research on LGBT health has increased over time, and HHS has sponsored efforts to collect and report data on LGBT health, as evidenced with the inclusion of LGBT-specific data in publications such as the National Healthcare Disparities Report, the addition of Healthy People 2020 goals to increase routine data collection efforts on LGBT populations, and early efforts of collection and surveillance on sexual orientation and gender identity in national health care surveys.110 In fact, the Obama Administration worked to significantly expand the collection of LGBT data. The number of federal surveys and studies collecting sexual orientation data increased to 12 and 7 of these also collected data on gender identity.111 Since 2013, the NHIS has included a question on sexual orientation. In addition, several agencies within HHS have taken steps toward broader data collection. For example, the CDC has added sexual orientation and gender identity questions to the state-administered Behavioral Risk Factor Surveillance System surveys and the Substance Abuse and Mental Health Services Administration’s National Survey on Drug Use and Health. The Administration on Aging also added a sexual orientation and gender identity questions to the National Survey of Older Americans Act (OAA) Participants. However, it is still not routine for researchers and health data systems to collect and report data by individuals’ sexual orientation and gender identity. Additionally, since taking office, the Trump Administration has sought to roll back data collection on sexual orientation and gender identity in a several surveys including the questions in the OAA survey. It also reversed plans to add such questions to a disability survey out of The Administration for Community Living (ACL). However, in response to pressure from advocacy groups the sexual orientation (but not gender identity) question was added back into the OAA survey. No changes were made to the disability survey.112
- At the provider and patient level, some groups advocate for clinicians to collect patient information on sexual orientation and gender identity to better understand an individual’s health profile and needs. Some providers have expressed discomfort with and inadequate knowledge on soliciting this information. Advocates’ recommendations include being direct with patients about why questions on sexual orientation and gender identity are being asked, ensuring that confidentiality will be maintained, informing patients of the right to opt-out, and asking multiple questions to assess both sexual orientation and gender identity.113 In particular, the IOM recommends collecting such data in electronic medical records (EMRs), which are growing in use.114
- In October 2016, the NIH formally designated sexual and gender minorities (SGMs) as a health disparity population for research purposes. In doing so NIH recognized the health disparities faced by this population and that “the extent and causes of health disparities are not fully understood, and research on how to close these gaps is lacking.”115
Impact of Supreme Court Rulings
Spousal coverage is an important pathway to insurance and other health benefits and marriage offers legal protections for millions of people, particularly in the context of employer-sponsored health insurance. Until recently, the federal government did not recognize same-sex marriage due to DOMA and several states banned same-sex marriage. This limited the ability of LGBT individuals and families to access a wide range of benefits, including health coverage as a dependent spouse and the ability to make health care decisions for a married partner. Two rulings by the Supreme Court have fundamentally changed this landscape.
- United States v. Windsor116 : In June 2013, the Supreme Court’s ruling in United States v. Windsor overturned a portion of DOMA and required the federal government to recognize legal same-sex marriages for the first time. The ruling and subsequent Agency policy interpretations and guidance have resulted in expanded access for many LGB families to a range of benefits, including dependent health coverage and family and medical leave. However, the ruling did not require states to recognize same-sex marriage or end state-level bans. As such, while the federal government extended benefits to legally married same-sex couples based on “state of celebration”117 where possible, some benefits remained dependent on the legal status of same sex marriage in “state of domicile.”118 This led to a patchwork of coverage availability across the country until the Obergefell
- Obergefell v. Hodges119 : In June 2015, the Supreme Court ruled in Obergefell v. Hodges that the Fourteenth Amendment requires states to license same-sex marriages and to recognize such marriages lawfully licensed and performed out-of-state, resulting in legal recognition of same-sex marriage nationwide. This effectively ends the distinction between state of celebration and state of domicile and further expanded access to health coverage and care for LGBT individuals and families.
Specific changes that affect spousal coverage and benefits due to these rulings are as follows:
- Tax Implications: As a result of the Windsor ruling, the Internal Revenue Service (IRS) ruled that it recognized all legally married same sex couples, based on state of celebration, who could now file federal taxes as “married” and, where same-sex marriage was legal, state taxes as well. As a result of the Obergefell decision, same-sex couples can now file state taxes jointly in every state. Tax filing affects a number of health-related financial issues such as taxes on health benefits.120 For example, dependent coverage, including spousal coverage, is excluded from an employee’s taxable income. Prior to the Supreme Court’s Windsor ruling, coverage for a same-sex spouse was considered taxable income, which raised taxes for those who received this coverage. The same is true for state taxes in states that did not recognize same-sex marriage prior to the Obergefell These rulings mean that married same-sex couples no longer face this higher tax burden at the federal and state levels.121 ,122
- Federal Employees & Federal Contractors: The Supreme Court’s Windsor decision also prompted federal agencies to reverse previous limitations on spousal benefits in federal programs. Where the federal government determined it had jurisdiction to do so, such benefits were extended to all legally married same-sex couples based on state of celebration. For example, all federal employees who are legally married to a same-sex partner (regardless of where they live), were given the same eligibility for dependent spousal health coverage in the Federal Employees Health Benefits Program (FEHBP) as well as other dependent benefits, including dental and vision insurance, long-term care insurance, and flexible spending accounts.123 In addition, in 2014, President Obama issued an executive order124 adding sexual orientation and gender identity to the prohibited bases of discrimination in employment by federal contractors and subcontractors. As such, it requires contractors that provide spousal benefits to opposite-sex married couples to also provide them to same-sex married couples.125
- Members of the Military and Veterans: Following the Windsor decision, the Department of Defense recognized same-sex marriages based on state of celebration and extended spousal benefits, such as TRICARE health coverage, to the same-sex spouses of military service members and employees.126 However, several benefits for Veterans continued to be tied to state of domicile, which meant that eligibility for spousal benefits for Veterans was uneven between marriage equality and non-equality states until the ruling in Obergefell. As a result of that decision, the Department of Veterans Affairs now recognizes all same-sex marriages127 and will extend benefits to all same-sex spouses of Veterans, including CHAMPVA health coverage, survivor compensation, and burial benefits.
- State and Municipal Employees: While the Windsor decision resulted in eligibility for spousal coverage for all federal employees and contractor employees, a patchwork of policies remained for state and local public employees based on where they lived. As a result of the Obergefell ruling’s recognition of same-sex marriages in all states, spousal coverage benefits should be extended to state and municipal employees across the nation to the same degree as their heterosexual counterparts.
- Private Employers: Neither the Windsor nor Obergefell decisions are binding on employers. In addition, as mentioned above, ACA regulations regarding health issuers are also not binding on employers. Therefore, while employers in marriage equality states were largely expected to offer same-sex spousal coverage after Windsor, and in all states after Obergefell, there remains some question about whether employers can legally limit spousal coverage to opposite-sex spouses. Still, many experts believe that an employer that offers health benefits to opposite-sex spouses but refuses to offer such benefits to same-sex spouses would likely be in violation of Title VII of the Civil Rights Act, which prohibits discrimination based on sex. The Equal Employment Opportunity Commission (EEOC)128 and at least one federal court129 have found Title VII to have standing in such cases. Moreover, a recent EEOC decision found that “sexual orientation is inherently a ‘sex-based consideration” under Title VII.130 The EEOC ruling allows such cases from both private and public sector employees to be brought forward for its review and will also be considered by federal courts in their review of cases, although it is not binding on them. In addition to potential Title VII violations, employers who provide spousal coverage for opposite sex couples but not same-sex couples may be subject to state non-discrimination laws. Given the remaining uncertainties regarding employers, this will be an important area to watch going forward.
- ERISA Protections: The Department of Labor issued guidance131 on the implications of the Windsor ruling for health plans and plan sponsors governed by the Employee Retirement Income Security Act of 1974 (ERISA), the federal law that sets minimum standards for most voluntarily established pension and health plans. The guidance states that under ERISA, the definition of “marriage”, wherever it appears, will include same-sex marriage based on state of celebration. This makes clear that group health plans can extend certain protections to married same sex couples, most notably COBRA, the law that offers employees and their families a temporary extension of group health coverage following a job loss or other qualifying event. In addition, because ERISA requires group health plans that offer spousal coverage generally to permit special enrollment opportunities for newly-married spouses, this guidance makes clear that group health plans can extend special enrollment rights to same-sex marriages where spouses are otherwise eligible to participate. However, neither the guidance nor ERISA specifically addresses whether the employer that sponsors the group health plan is required to recognize a same-sex marriage.
- State-Level Insurance Protections: In addition to federal law, the number of states that have nondiscrimination policies in insurance coverage and employment has increased over time, although the majority of states do not have such protections. Twelve states (CA, CO, DE, HI, IL, ME, MN, NV, NY, OR, RI, VT, and WA) plus DC prohibit discrimination based on sexual orientation and gender identity in private health insurance.132 New Jersey provides protection on the basis of sexual orientation but not gender identity in private health insurance.133 Nineteen states (CA, CT, CO, DE, HI, IL, MA, MD, MI, MN, NJ, NV, NY, OR, PA, RI, VT, and WA) and DC prohibit transgender exclusions in health insurance through legislation or regulation.134 Twenty states (CA, CO, CT, DE, HI, IL, IA, ME, MD, MA, MN, NV, NJ, NM, NY, OR, RI, UT, VT, and WA) plus DC prohibit discrimination by private employers on the basis of sexual orientation and gender identity and another two states (NH and WI) prohibit discrimination based only on sexual orientation.135
- Health Insurance Marketplaces: Windsor also affected eligibility for assistance for same-sex couples in all ACA health insurance marketplaces (whether federally-facilitated or state based). Eligibility is based in part on an applicant’s family structure and income. Federal regulations were issued stating that insurance marketplaces must recognize same-sex marriages and base eligibility for tax credits on a couple’s income according to their tax filing.136 (It is important to note that when a couple’s income is used to determine eligibility for tax credits in the marketplace, it could mean they are more or less likely to qualify, depending on their specific situation).
- Medicaid and CHIP: Because Medicaid and the Children’s Health Insurance Program (CHIP) are federal-state partnerships, the federal government determined that Windsor did not allow it to require states to recognize same-sex marriages for the purpose of determining eligibility, although it encouraged them to do so.137 This meant that eligibility could vary based on state laws regarding same-sex marriage. With the Obergefell ruling, however, all states must now recognize legal same-sex marriages and state Medicaid agencies are expected to do so (as with marketplaces, eligibility may be impacted when income is counted jointly).
- Medicare: These decisions have also resulted in expanded access to Medicare for same-sex couples. After Windsor, DHHS issued guidance clarifying that same-sex married beneficiaries in Medicare Advantage plans who each need care in a skilled nursing facility can receive care at same facility, as applicable to married Medicare beneficiaries more generally.138 Also after Windsor, individuals in same-sex marriages became eligible for free Medicare Part A (hospital) premiums in marriage recognition states if their spouse had sufficient work history to qualify for Medicare benefits, even if they themselves did not.139 If they lived in a non-recognition state, however, they had access to reduced premiums only. Obergefell expanded access to free Part A premiums nationwide. In addition, a special enrollment period (SEP) for Medicare Part B (and Premium Part A) is available for an individual who gains and then loses insurance coverage related to spousal employment without facing a penalty (this was already based on state of celebration after Windsor).140 As with other means-tested programs, eligibility may be impacted when income is counted jointly.
Family Caregiving Issues
Caring for ill family members is another area of policy that has been evolving in recent years for LGBT people and their families. The Family Medical Leave Act (FMLA) provides workplace protections to employees if they take time off to care for a family member in the event of illness or birth of a child. Under DOMA, LGB individuals were not afforded the law’s protections to care for a spouse because the federal government did not recognize same-sex marriages; however, the Supreme Court’s decision extends the law to all legally married individuals at qualifying employers. While this is an important step, it does not cover all workers. Additionally there are still other barriers that can limit the reach of these new policies.
- After the Supreme Court’s Windsor ruling, the DOL expanded FMLA to include legally married same-sex spouses residing in states that recognized same-sex marriage.141 In February 2015, the DOL expanded the FMLA to include same-sex couples based on state of celebration, regardless of their state of residence.142
- In addition to workplace protections, visiting loved ones in the hospital or another health care setting has not always been guaranteed for LGBT people. However, federal regulations in effect since 2011 require hospitals participating in Medicare and Medicaid (virtually all hospitals in the U.S.) to adopt written policies and procedures regarding a patient’s rights to visit his or her same-sex partner (whether or not they are legally married) and state explicitly that discrimination based on sexual orientation and gender identity are prohibited.143
- Providers must sometimes communicate information or discuss medical decisions on a patient’s behalf with a patient “representative,” who is often a spouse. If finalized, Federal regulations proposed in 2014 would require that providers and suppliers, such as hospitals, hospices, community mental health centers, and laboratories, that participate in Medicare and Medicaid must recognize same-sex spouses (marriage legalized based on state of celebration) as patient representatives.144
- Concerns have also been raised about discrimination against older LGBT individuals and their families in long-term care facilities. Recent federal regulations now provide residents of long-term care facilities, such as nursing homes, the right to have visitors of their choice, including same-sex spouses and domestic partners.145
- However, in October 2017 the Trump admiration withdrew a proposed rule that would have required long term care facilities receiving federal funds to treat same-sex spouses the same as opposite-sex spouses.146 An HHS spokesperson stated that the Administration did not believe the rule needed to be finalized in light of the 2015 Obergefell ruling (requiring licensing and recognition of same-sex marriage in all states).147 However, Obergefell only address the right to marry, not whether institutions can legally treat married same-sex couples differently than married opposite-sex couples.
- In addition, there are still areas where LGBT individuals and families are not protected. For example, paid sick leave is an important benefit that many workers do not have. Because it has been legal in more than half the states to fire employees based on their sexual orientation or gender identity, LGBT employees without paid leave may be more reluctant to take time off when they or their family members are sick.148
Other Changes
- Medicaid is the primary payer of long-term care, and qualifying for Medicaid long-term services can result in exhaustion of financial resources for those who seek services as well as their spouses. The program’s “spousal impoverishment” protections aim to mitigate this by allowing a spouse who remains in the community to retain a certain level of income and assets without affecting eligibility. In 2011, states were given the option to extend these “spousal impoverishment” protections to married same-sex couples and domestic partners.149 After Windsor, such protections were required for married same-sex couples in marriage equality states. It is expected that with the Obergefell ruling, all states will be required to apply these protections to married same-sex couples.
- Coverage of transgender services has also been expanded in federal programs. In 2014, HHS invalidated a prior policy that had allowed Medicare plans to deny coverage for “transsexual surgery,” 150 and OPM has stated that, as of 2016, the Federal Employees Health Benefits Program (FEHBP) may not issue blanket exclusions for gender transition services.151 As a result, Medicare and FEHBP plans must cover gender transition services that are “medically necessary,” although the definition of medical necessity is in part at the discretion of providers and plans. Several employers have also moved to make their plan offerings more comprehensive by removing exclusions for transgender health services. Among major U.S. employers, there has been a five-fold increase in the number of businesses offering at least one health plan that includes coverage of transgender services such as counseling, hormone therapy, and surgical procedures.152
***
A number of health challenges disproportionately affect LGBT communities, particularly the HIV epidemic, stigma and violence, substance use, negative experiences in the health care system, and lack of insurance coverage. In addition to health outcomes, access to care has been a concern and intersects with many broader issues, including relationship recognition, legal identity recognition policies for transgender individuals, training and cultural competency of health professionals, as well as overarching societal and cultural issues, particularly a long history of stigma and discrimination. While many of these barriers persist recent policy and legal changes have served to mitigate some of these challenges, particularly the implementation of the ACA and the impacts of marriage equality. While this convergence of policy and legal breakthroughs holds promise for broader access to health services, coverage, and benefits for LGBT communities, actions taken by the Trump administration may threaten to destabilize some of the insurance market and individual protections gained over the past decade, and it will important to monitor these changes moving forward.
Tables
| Table 1: Alcohol Use, Cigarette Use, and Serious Psychological Distress Among Bisexual, Gay or Lesbian, and Heterosexual Adults ages 18-64, 2015 | |||
| Five (men)/four (women) or more alcoholic drinks in 1 day at least once in past year | Bisexual | Gay or Lesbian | Heterosexual |
| All adults | 47.2% | 36.2% | 27.5% |
| Women | 44.8% | 32.2% | 20.7% |
| Men | 52.9% | 39.6% | 34.5% |
| Current cigarette smoker | Bisexual | Gay or Lesbian | Heterosexual |
| All adults | 26.1% | 20.1% | 16.5% |
| Women | 24.7% | 18.7% | 14.9% |
| Men | 29.5% | 21.2% | 18.1% |
| Experienced serious psychological distress in past 30 days | Bisexual | Gay or Lesbian | Heterosexual |
| All adults | 15.0% | 4.6% | 3.7% |
| Women | 17.0% | 4.8%* | 4.3% |
| Men | N/A | 4.4* | 3.0% |
| NOTE: N/A- data not available due to unreliability. * Relative standard error >30% and less than or equal to 50% and should be used with caution.SOURCE: Centers for Disease Control and Prevention, National Health Statistics Reports. (2015). Data available; https://www.cdc.gov/nchs/data/nhis/sexual_orientation/asi_2015_stwebsite_tables.pdf | |||
| Table 2: Impact of Selected Federal Policy Changes on Coverage and Access to Care for LGBT Communities | |
| Policy | Key Provisions and Impact |
| The Patient Protection and Affordable Care Act (ACA)153 |
|
| Supreme Court Rulings on Marriage Equality: United States v. Windsor (2013) and Obergefell v. Hodges (2015) |
|
| Other |
|
Endnotes
- Institute of Medicine (IOM). (2011). The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. ↩︎
- Healthy People 2020: Lesbian, Gay, Bisexual, and Transgender Health. ↩︎
- Agency for Healthcare Research and Quality. (2012). 2012 National Healthcare Disparities Report. ↩︎
- IOM. (2011). The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. ↩︎
- Ibid. ↩︎
- National Center for Transgender Equality. (2009). Transgender Terminology. ↩︎
- Gates, G. (March 22, 2010). LGBT Demographics: Presentation to the Institute of Medicine. ↩︎
- Kaiser Family Foundation analysis of NHIS 2016 data available at: Dawson, L., Kates, J., and Damico, A. (2018). The Affordable Care Act and Insurance Coverage Changes by Sexual Orientation. Available at: https://modern.kff.org/disparities-policy/issue-brief/the-affordable-care-act-and-insurance-coverage-changes-by-sexual-orientation/ ↩︎
- Gates, G (2017). Gallup. In U.S., More Adults Identifying as LGBT. ↩︎
- Where data do not include transgender individuals, LGB (lesbian, gay, bisexual) is used. ↩︎
- IOM. (2011). The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. ↩︎
- Coffman, KB, Coffman, LC & Marzilli Ericson, KM. (2013). The Size of the LGBT Population and the Magnitude of Anti-Gay Sentiment are Substantially Underestimated, NBER Working Paper No. 19508. ↩︎
- Gates, G (2017). Gallup. In U.S., More Adults Identifying as LGBT. ↩︎
- Kann, L., et al. 2016. Centers for Disease Control and Prevention. MMWR. Sexual Identity, Sex of Sexual Contacts, and Health-Related Behaviors Among Students in Grades 9–12 — United States and Selected Sites, 2015. 65(9);1-202. ↩︎
- Flores, A., et al. The Williams Institute. How Many Adults Identify as Transgender in the United States? June 2016. Available at: http://williamsinstitute.law.ucla.edu/wp-content/uploads/How-Many-Adults-Identify-as-Transgender-in-the-United-States.pdf ↩︎
- Gates, G. Gallup. . (February 6, 2017.). Vermont Leads States in LGBT Identification. ↩︎
- Ibid. ↩︎
- Jones, J. Gallup. (June 22, 2017.) In U.S., 10.2% of LGBT Adults Now Married to Same-Sex Spouse. ↩︎
- Kaiser Family Foundation analysis of the 2016 American Community Survey. Data available here: https://www.census.gov/data/tables/time-series/demo/same-sex-couples/ssc-house-characteristics.html ↩︎
- Pew Research Center (June 2013). A Survey of LGBT Americans Attitudes, Experiences and Values in Changing Times. ↩︎
- Badgett, M.V., Durso, L.E. & Schneebaum, A. (2013). New Patters of Poverty in the Lesbian, Gay, and Bisexual Community. The Williams Institute. ↩︎
- James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality. ↩︎
- Agency for Healthcare Research and Quality. (2012). 2012 National Healthcare Disparities Report. ↩︎
- IOM. (2011). The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. ↩︎
- Healthy People 2020: Lesbian, Gay, Bisexual, and Transgender Health. ↩︎
- Agency for Healthcare Research and Quality. (2012). 2012 National Healthcare Disparities Report. ↩︎
- Lick, D., Durso, L.E., & Johnson, K.L. (2013). Minority Stress and Physical Health Among Sexual Minorities. Pers on Psychological Sci 8(5): 521-548. ↩︎
- Denney, J.T., Gorman, B.K. & Barrera, C.B. (2013). Families, Resources, and Adult Health: Where do Sexual Minorities Fit? Journal of Health and Social Behavior 54(1): 46-63. ↩︎
- Lick, D., Durso, L.E., & Johnson, K.L. (2013). Minority Stress and Physical Health Among Sexual Minorities. Pers on Psychological Sci 8(5): 521-548. ↩︎
- Ibid. ↩︎
- Centers for Disease Control and Prevention, National Health Statistics Reports. (July 2014). Sexual Orientation and Health Among U.S. Adults: National Health Interview Survey, 2013. ↩︎
- James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality. ↩︎
- Massachusetts Department of Public Health. (2009). The Health of Lesbian, Gay, Bisexual, and Transgender (LGBT) Persons in Massachusetts. ↩︎
- Centers for Disease Control and Prevention. (2016). Monitoring Selected National HIV Prevention and Care Objectives by Using HIV Surveillance Data United States and 6 Dependent Areas, 2015. Vol. 22. No 2. Available at: https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-supplemental-report-vol-22-2.pdf ↩︎
- Centers for Disease Control and Prevention. (2016). Diagnoses of HIV Infection in the United States and Dependent Areas, 2016. Vol. 28. https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2016-vol-28.pdf ↩︎
- Centers for Disease Control and Prevention (Feb. 2017). HIV Among Gay and Bisexual Men. https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/cdc-msm-508.pdf ↩︎
- Centers for Disease Control and Prevention (Sept. 2017), HIV Among Gay and Bisexual Men. https://www.cdc.gov/hiv/group/msm/index.html ↩︎
- Baral SD, et al. (2013). Worldwide burden of HIV in transgender women: a systematic review and meta-analysis. The Lancet Infectious Disease. 13(3): 214–222. ↩︎
- Centers for Disease Control and Prevention (2006). MMWR. Revised Recommendations for HIV Testing of Adults, Adolescents, and Pregnant Women in Health-Care Settings. 55(RR14); September 2006. ↩︎
- Kaiser Family Foundation, HIV/AIDS In The Lives Of Gay And Bisexual Men In The United States, 2014. ↩︎
- Centers for Disease Control and Prevention. (2016). Monitoring Selected National HIV Prevention and Care Objectives by Using HIV Surveillance Data United States and 6 Dependent Areas, 2015. Vol. 22. No 2. Available at: https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-supplemental-report-vol-22-2.pdf ↩︎
- Centers for Disease Control and Prevention. (2014). Likely Female-to-Female Sexual Transmission of HIV- Texas, 2012. ↩︎
- Centers for Disease Control and Prevention. (2016). https://www.cdc.gov/nchhstp/newsroom/2016/std-surveillance-report-2015-press-release.html ↩︎
- Centers for Disease Control and Prevention. (2012). Viral Hepatitis: Information for Gay and Bisexual Men. https://www.cdc.gov/hepatitis/Populations/PDFs/HepGay-FactSheet.pdf ↩︎
- Centers for Disease Control and Prevention (2013). HPV-Associated Cancers Statistics. ↩︎
- Centers for Disease Control and Prevention. (2012). HPV and Men- Fact Sheet. ↩︎
- Lick, D., Durso, L.E., & Johnson, K.L. (2013). Minority Stress and Physical Health Among Sexual Minorities. Pers on Psychological Sci 8(5): 521-548. ↩︎
- Cochran, S.D., Sullivan, J.G. & Mays, V.M. (2003). Prevalence of mental disorders, psychological distress, and mental health services use among Lesbian, Gay, and Bisexual adults in the United States. Journal of Consulting and Clinical Psychology 71(1): 53-61. ↩︎
- Institute of Medicine. (2011). The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. ↩︎
- Substance Abuse and Mental Health Services Administration. (2012). Top Health Issues for LGBT Populations: Information & Resources Kit. ↩︎
- Ford, Z. (December 3, 2012). APA Revises Manual: Being Transgender is no Longer a Mental Disorder. Think Progress. ↩︎
- Lick, D., Durso, L.E., & Johnson, K.L. (2013). Minority Stress and Physical Health Among Sexual Minorities. Pers on Psychological Sci 8(5): 521-548. ↩︎
- Lee J, Griffin G, Melvin C (2009). Tobacco use among sexual minorities in the USA, 1987 to May 2007: a systematic review. Tob Control. 18:275-282. ↩︎
- Cochran, S.D., Sullivan, J.G. & Mays, V.M. (2003). Prevalence of mental disorders, psychological distress, and mental health services use among Lesbian, Gay, and Bisexual adults in the United States. Journal of Consulting and Clinical Psychology 71(1): 53-61. ↩︎
- Grant JM, Mottet LA, Tanis J, Harrison J, Herman JL, Keisling M. (2011). Injustice at Every Turn: A Report of the National Transgender Discrimination Survey. Washington, DC: National Center for Transgender Equality and National Gay and Lesbian Task Force. ↩︎
- Ostrow, D.G. & Stall, R. (2008) Alcohol, tobacco, and drug use among gay and bisexual men. In Wolitski, R.J., Stall, R., & Valdiserri, R.O., Unequal opportunity: Health disparities affecting gay and bisexual men in the United States. New York: Oxford University Press. ↩︎
- Centers for Disease Control and Prevention. (2009). Sexual Violence: Consequences. ↩︎
- Human Rights Campaign, (2011). A Guide to State Level Advocacy Following Enactment of the Matthew Shepard and James Byrd, Jr. Hate Crimes Prevention Act. ↩︎
- Pew Research Center (June 2013). A Survey of LGBT Americans Attitudes, Experiences and Values in Changing Times. ↩︎
- Centers for Disease Control and Prevention. (2013). The National Intimate Partner and Sexual Violence Survey: 2010 Findings on Victimization by Sexual Orientation. ↩︎
- U.S. Department of Justice Federal Bureau of Investigation, (2016). Hate Crime Statistics 2016. ↩︎
- Herek, G.M. (2009). Hate Crimes and Stigma-Related Experiences Among Minority Adults in the United States: Prevalence Estimates from a National Probability Sample. Journal of Interpersonal Violence. ↩︎
- Ibid. ↩︎
- Lombardi E, et al. (2002). Gender violence: Transgender experiences with violence and discrimination. J Homosex 42(1). ↩︎
- National Coalition of Anti-Violence Programs. (2013). Lesbian, Gay, Bisexual, Transgender, Queer, and HIV-Affected Hate Violence in 2012. ↩︎
- Human Rights Campaign. (2012). National Coming Out Day Youth Report. ↩︎
- Kann L, Olsen EO, McManus T, et al. Centers for Disease Control and Prevention. Sexual Identity, Sex of Sexual Contacts, and Health-Related Behaviors Among Students in Grades 9–12 — United States and Selected Sites, 2015. MMWR. 2016;65(No. SS-9):1–202. Available at: http://dx.doi.org/10.15585/mmwr.ss6509a1 ↩︎
- Kann L, Olsen EO, McManus T, et al. Centers for Disease Control and Prevention. Sexual Identity, Sex of Sexual Contacts, and Health-Related Behaviors Among Students in Grades 9–12 — United States and Selected Sites, 2015. MMWR. 2016;65(No. SS-9):1–202. Available at: http://dx.doi.org/10.15585/mmwr.ss6509a1 ↩︎
- Kann L, Olsen EO, McManus T, et al. Centers for Disease Control and Prevention. Sexual Identity, Sex of Sexual Contacts, and Health-Related Behaviors Among Students in Grades 9–12 — United States and Selected Sites, 2015. MMWR. 2016;65(No. SS-9):1–202. Available at: http://dx.doi.org/10.15585/mmwr.ss6509a1 ↩︎
- Kann L, Olsen EO, McManus T, et al. Centers for Disease Control and Prevention. Sexual Identity, Sex of Sexual Contacts, and Health-Related Behaviors Among Students in Grades 9–12 — United States and Selected Sites, 2015. MMWR. 2016;65(No. SS-9):1–202. Available at: http://dx.doi.org/10.15585/mmwr.ss6509a1 ↩︎
- Kann L, Olsen EO, McManus T, et al. Centers for Disease Control and Prevention. Sexual Identity, Sex of Sexual Contacts, and Health-Related Behaviors Among Students in Grades 9–12 — United States and Selected Sites, 2015. MMWR. 2016;65(No. SS-9):1–202. Available at: http://dx.doi.org/10.15585/mmwr.ss6509a1 ↩︎
- Centers for Disease Control and Prevention. (2011). Lesbian, Gay, Bisexual, and Transgender Health: Youth. ↩︎
- The Williams Institute. (2012). Serving Our Youth: Findings from a National Survey of Service Providers Working with Lesbian, Gay, Bisexual, and Transgender Youth who are Homeless or At Risk of Becoming Homeless. ↩︎
- Gay, Lesbian & Straight Education Network. (2012). 2011 National School Climate Survey. ↩︎
- Kann L, Olsen EO, McManus T, et al. Centers for Disease Control and Prevention. Sexual Identity, Sex of Sexual Contacts, and Health-Related Behaviors Among Students in Grades 9–12 — United States and Selected Sites, 2015. MMWR. 2016;65(No. SS-9):1–202. Available at: http://dx.doi.org/10.15585/mmwr.ss6509a1. ↩︎
- William Institute. (2018). Conversion Therapy and LGBT Youth. https://williamsinstitute.law.ucla.edu/demographics/conversion-therapy-and-lgbt-youth/ ↩︎
- American Medical Association. Health Care Needs of Lesbian, Gay, Bisexual and Transgender Populations H-160.991. Available at: https://policysearch.ama-assn.org/policyfinder/detail/H-160.991%20?uri=%2FAMADoc%2FHOD.xml-0-805.xml; American Psychological Association. 2000. Position Statement on Therapies Focused on Attempts to Change Sexual Orientation (Reparative or Conversion Therapies). Available at: http://www.psychiatry.org/File%20Library/Advocacy%20and%20Newsroom/ Position%20Statements/ps2000_ReparativeTherapy.pdf.; and the American Academy of Pediatrics. PEDIATRICS Vol. 92 No. 4 October 1993. Available at: http://pediatrics.aappublications.org/content/pediatrics/92/4/631.full.pdf. ↩︎
- Center for American Progress. (2013). LGBT Communities and the Affordable Care Act: Findings from a National Survey. ↩︎
- Clift, J & Kirby J. (2012). Health care access and perceptions of provider care among individuals in Same-Sex Couples: Findings from the Medical Expenditure Panel Survey (MEPS). Journal of Homosexuality 59(6): 839-850. ↩︎
- Another 41% say they have not encountered this benefits issue and 16% say they do not offer the benefit. ↩︎
- Dawson, L., Kates, J. and Rae, M. (2017). The Kaiser Family Foundation. Access to Employer-Sponsored Health Coverage for Same-Sex Spouses: 2017 Update. . Available at: https://modern.kff.org/disparities-policy/issue-brief/access-to-employer-sponsored-health-coverage-for-same-sex-spouses-2017-update/ ↩︎
- Dawson, L., Kates, J. and Rae, M. (2017). The Kaiser Family Foundation. Access to Employer-Sponsored Health Coverage for Same-Sex Spouses: 2017 Update. . Available at: https://modern.kff.org/disparities-policy/issue-brief/access-to-employer-sponsored-health-coverage-for-same-sex-spouses-2017-update/ ↩︎
- Gonzales, G. (2015). Association of the New York State Marriage Equality Act with Changes in Health Insurance Coverage. JAMA. ↩︎
- Buchmueller, T.& Carpenter C. (2010). Disparities in health insurance coverage, access, and outcomes for individuals in same-sex versus different-sex relationships, 2000-2007. American Journal of Public Health 100(3): 489-495. ↩︎
- Kerker, B.D., Mostashari, F. & Thorpe, L. (2006). Health care access and utilization among women who have sex with women: Sexual behavior and identity. Journal of Urban Health 83(5): 970-979. ↩︎
- Cochran, SD, et al. (2001). Cancer-related risk indicators and preventive screening behaviors among lesbians and bisexual women. American Journal of Public Health 91(4): 591-597. ↩︎
- National Center for Transgender Equality and National Gay and Lesbian Task Force. (2011). Injustice at Every Turn: A Report of the National Transgender Discrimination Survey. ↩︎
- Center for American Progress. (2012). FAQ: Health Insurance Needs for Transgender Americans. ↩︎
- Lambda Legal, “When Health Care Isn’t Caring: Lambda Legal’s Survey on Discrimination Against LGBT People and People Living with HIV”. ↩︎
- The Fenway Institute. (2008). The Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health. ↩︎
- Lambda Legal, “When Health Care Isn’t Caring: Lambda Legal’s Survey on Discrimination Against LGBT People and People Living with HIV”. ↩︎
- Movement Advancement Project. (2009). Advancing Transgender Equality. ↩︎
- Tesar, C. & Rovi, S. (1998). Survey on Curriculum on Homosexuality/ Bisexuality in Departments of Family Medicine. Fam Medicine 30(4): 283-287. ↩︎
- Corliss, H.L., Shankle, M.D. & Moyer, M.B. (2007). Research, Curricula, and Resources Related to Lesbian, Gay, Bisexual, and Transgender Health in U.S. Schools of Public Health. American Journal of Public Health 97(6): 1023-1027. ↩︎
- GLMA, Health Professionals Advancing LGBT Equality. (2013). Compendium of Health Profession Association LGBT Policy & Position Statements. ↩︎
- World Professional Association for Transgender Health (2012). Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People. ↩︎
- L. Dawson, J. Kates, and A. Damico. (2018). Kaiser Family Foundation. The Affordable Care Act and Insurance Coverage Changes by Sexual Orientation. https://modern.kff.org/disparities-policy/issue-brief/the-affordable-care-act-and-insurance-coverage-changes-by-sexual-orientation/ ↩︎
- Lambda Legal, “When Health Care Isn’t Caring: Lambda Legal’s Survey on Discrimination Against LGBT People and People Living with HIV”. ↩︎
- Baker, K. & Cray, A. (2012). Ensuring Benefits Parity and Gender Identity Nondiscrimination in Essential Health Benefits. Center for American Progress. ↩︎
- Human Rights Campaign. Health Insurance Discrimination for Transgender People. ↩︎
- Department of Health and Human Services. Federal Register 77(59): March 27, 2012. ↩︎
- Department of Health and Human Services. Federal Register 78(37): February 25, 2013. ↩︎
- K. Keith. Health Affairs Blog. ACA Round-Up: Section 1557 Rule On Horizon; CSR And Medicaid Litigation Updates; Focus On Employer Mandate. February 19, 2018. https://www.healthaffairs.org/do/10.1377/hblog20180219.671383/full/ ↩︎
- Department of Health and Human Services. Federal Register 78(39): February 27, 2013. ↩︎
- Centers for Medicaid and Medicare Services (CMS). Frequently Asked Questions on Coverage of Same-Sex Spouses . March 14, 2014. ↩︎
- Department of Health and Human Services. Federal Register 81(116): June 16 2016. ↩︎
- Pollitz, K. (2018.) Kaiser Family Foundation. Understanding Short-Term Limited Duration Health Insurance. https://modern.kff.org/health-reform/issue-brief/understanding-short-term-limited-duration-health-insurance/ ↩︎
- HHS. 83 FR 2802. “Statement of Organization, Functions, and Delegations of Authority,” January 19, 2018. Available at https://www.gpo.gov/fdsys/pkg/FR-2018-01-19/pdf/2018-00820.pdf; HHS. 83 FR 3880. “Protecting Statutory Conscience Rights in Health Care; Delegations of Authority.” January 26, 2018. Available at https://www.gpo.gov/fdsys/pkg/FR-2018-01-26/pdf/2018-01226.pdf. ↩︎
- Lambda Legal. January 2018. Trump Administration Plan to Expand Religious Refusal Rights of Health Professionals: Legal Issues and Concerns. Available at: https://www.lambdalegal.org/sites/default/files/2018-01- 18_lambda_legal_analysis_re_hhs_ocr_special_religious_refusal_unit_jcp_issued.pdf ↩︎
- Department of Health and Human Services. (2013). HHS LGBT Issues Coordinating Committee 2013 Report. ↩︎
- Cahill, S., Geffen, S., and Wang, T. The Fenway Institute. One year in, Trump Administration amasses striking anti-LGBT record 2018. http://fenwayhealth.org/wp-content/uploads/The-Fenway-Institute-Trump-Pence-Administration-One-Year-Report.pdf ↩︎
- Cahill, S., Geffen, S., and Wang, T. The Fenway Institute. One year in, Trump Administration amasses striking anti-LGBT record 2018. http://fenwayhealth.org/wp-content/uploads/The-Fenway-Institute-Trump-Pence-Administration-One-Year-Report.pdf ↩︎
- The Fenway Institute. (2012). Policy Focus: How to gather data on sexual orientation and gender identity in clinical settings. ↩︎
- IOM. (2011). The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. ↩︎
- National Institutes of Health. National Institute on Minority Health and Health Disparities. Director’s Message. “Sexual and Gender Minorities Formally Designated as a Health Disparity Population for Research Purposes” October 6, 2016. Available at: http://www.nimhd.nih.gov/about/directors-corner/message.html. ↩︎
- Supreme Court of the United States, United States v. Windsor, June 26, 2013. ↩︎
- Their marriages were recognized as long as legally valid where performed and not dependent on whether the state they lived in recognized their marriage. ↩︎
- Where the couple lived when seeking the benefit. ↩︎
- Supreme Court of the United States, Obergefell v. Hodges, June 26, 2015. ↩︎
- Internal Revenue Service, Rev.Rul.2013-17. ↩︎
- Internal Revenue Service, Application of Windsor Decision and Rev. Rul. 2013-17 to Employment Taxes and Special Administrative Procedures for Employers to Make Adjustments or Claims for Refund or Credit ↩︎
- How Supreme Court Gay Marriage Ruling Affects Employee Benefit Plans, Insurance Journal, June 26 ,2015. ↩︎
- U.S. Office of Personnel Management, Guidance on the Extension of Benefits to Married Gay and Lesbian Federal Employees, Annuitants, and their Families, June 28, 2013. ↩︎
- The White House, Executive Order 13672, Further Amendments to Executive Order 11478, Equal Employment Opportunity in the Federal Government, and Executive Order 11246, Equal Employment Opportunity, July 21, 2014. ↩︎
- Department of Labor, Frequently Asked Questions: EO 13672 Final Rule, July 21, 2014. ↩︎
- Department of Defense, Extending Benefits to the Same-Sex Spouses of Military Members, August 13, 2013. ↩︎
- U.S. Department of Veterans Affairs, Statement Following Supreme Court Ruling in Obergefell v. Hodges, June 29, 2015. ↩︎
- Equal Employment Opportunity Commission (EEOC), Cote v. Walmart Stores, East, L.P., Notice of Right to Sue, May 29, 2015 ↩︎
- Hall et al v. BNSF Railway Company, No. 2:2013cv02160 – Document 37 (W.D. Wash. 2014). ↩︎
- EEOC, Opinion in Appeal No. 0120133080, July 15, 2015. ↩︎
- Department of Labor, Technical Release No. 2013-04, September 18, 2013. ↩︎
- Movement Advancement Project. Healthcare Laws and Policies. ↩︎
- Movement Advancement Project. Healthcare Laws and Policies. ↩︎
- Ibid. ↩︎
- Movement Advancement Project. Employment Non-Discrimination Laws. ↩︎
- Department of Health and Human Services, Guidance on Internal Revenue Ruling 2013-17 and Eligibility for Advance Payments of the Premium Tax Credit and Cost-Sharing Reductions , September 27, 2013. ↩︎
- Department of Health and Human Services, State Health Officer # 13-006, September 27, 2013. ↩︎
- Department of Health and Human Services, Impact of United States v. Windsor on Skilled Nursing Facility Benefits for Medicare Advantage Enrollees, August 29, 2013. ↩︎
- Social Security Administration. Program Operations Manual System (POMS): GN 00210.002 Same-Sex Marriage – Determining Marital Status for Title II and Medicare Benefits. TN 10 (06-14). Social Security Administration. Program Operations Manual System (POMS): GN 00210.706 Same-Sex Marriage – HI Premium Reduction for Aged and Disabled Individuals. TN 8 (05-14). ↩︎
- Social Security Administration. Program Operations Manual System (POMS): GN 00210.700 Same-Sex Marriage – Eligibility for Medicare Special Enrollment Period (SEP). TN 6 (04-14). ↩︎
- Department of Labor, Wage and Hour Division, Fact Sheet #28F: Qualifying Reasons for Leave under the Family and Medical Leave Act, August 2013. ↩︎
- Department of Labor, Wage and Hour Division, Fact Sheet: Final Rule to Amend the Definition of Spouse in the Family and Medical Leave Act Regulations, February 2015. ↩︎
- Department of Health and Human Services, Medicare finalizes new rules to require equal visitation rights for all hospital patients, November 17, 2010. ↩︎
- CMS. (2014). Medicare and Medicaid Program Revisions to Certain Patient’s Rights of Conditions of Participation and Conditions for Coverage. ↩︎
- CMS. (2013). Reminder: Access and Visitation Rights in Long Term Care (LTC) Facilities. ↩︎
- Department of Health and Human Services. Medicare and Medicaid Programs; Revisions to Certain Patient’s Rights Conditions for Participation and Conditions for Coverage; Withdrawal. Federal Register 82(191). ↩︎
- Mongan, E. October 4, 2017. “CMS withdraws proposal requiring LTC facilities to afford spousal rights to same-sex couples.” McKnight’s Long- Term Care News & Assisted Living. https://www.mcknights.com/cms-withdraws-proposal-requiring-ltc-facilities-to-afford-spousal-rights-to-same-sex-couples/printarticle/697715/ ↩︎
- National Gay and Lesbian Task Force, Nondiscrimination Laws Map, June 21, 2013. ↩︎
- CMS. (2011). State Medicaid Director Letter: Same Sex Partners and Medicaid Liens, Transfers of Assets, and Estate Recovery. ↩︎
- Department of Health and Human Services, Departmental Appeals Board, Appellate Division. NCD 140.3, Transsexual Surgery, Docket No. A-13-87, Decision No. 2576, May 30, 2014. ↩︎
- Office of Personnel Management, FEHBP Program Carrier Letter No. 2015-12, June 23, 2015. ↩︎
- Human Rights Campaign. (2013). Corporate Equality Index. ↩︎
- Department of Health and Human Services. Federal Register 77(59): March 27, 2012. ↩︎
- Department of Health and Human Services. Federal Register 81(96): May 18, 2016. ↩︎
- Department of Health and Human Services. Federal Register 77(59): March 27, 2012. ↩︎
- Department of Health and Human Services. Federal Register 78(39): February 27, 2013. ↩︎
- CMS. Frequently Asked Questions on Coverage of Same-Sex Spouses. March 14, 2014. ↩︎
- Supreme Court of the United States, United States v. Windsor, June 26, 2013. ↩︎
- Supreme Court of the United States, Obergefell v. Hodges, June 26, 2015. ↩︎
- Department of Justice, Attorney General Lynch Announces Federal Marriage Benefits Available to Same-Sex Couples Nationwide, July 9, 2015. ↩︎
- U.S. Department of the Treasury, All Legal Same-Sex Marriages Will be Recognized for Federal Tax Purposes, August 29, 2013. ↩︎
- U.S. Office of Personnel Management, Guidance on the Extension of Benefits to Married Gay and Lesbian Federal Employees, Annuitants, and their Families, June 28, 2013. ↩︎
- The White House, Executive Order 13672, Further Amendments to Executive Order 11478, Equal Employment Opportunity in the Federal Government, and Executive Order 11246, Equal Employment Opportunity, July 21, 2014. ↩︎
- Secretary of Defense, Extending Benefits to Same-Sex Spouses of Military Members, August 13, 2013. ↩︎
- Department of Veterans Affairs, Statement Following Supreme Court Ruling in Obergefell v. Hodges, June 29, 2015. ↩︎
- Department of Health and Human Services, Guidance on Internal Revenue Ruling 2013-17 and Eligibility for Advance Payments of the Premium Tax Credit and Cost-Sharing Reductions, September 27, 2013. ↩︎
- Department of Health and Human Services, State Health Officer # 13-006, September 27, 2013. ↩︎
- Social Security Administration. Program Operations Manual System (POMS): GN 00210.002 Same-Sex Marriage – Determining Marital Status for Title II and Medicare Benefits. TN 10 (06-14). Social Security Administration. Program Operations Manual System (POMS): GN 00210.706 Same-Sex Marriage – HI Premium Reduction for Aged and Disabled Individuals. TN 8 (05-14). ↩︎
- Social Security Administration. Program Operations Manual System (POMS): GN 00210.700 Same-Sex Marriage – Eligibility for Medicare Special Enrollment Period (SEP). TN 6 (04-14). ↩︎
- Department of Health and Human Services, Impact of United States v. Windsor on Skilled Nursing Facility Benefits for Medicare Advantage Enrollees, August 29, 2013. ↩︎
- Department of Labor, Wage and Hour Division. Federal Register 80(37): February 25, 2015. ↩︎
- Office of the Press Secretary, Presidential Memorandum- Hospital Visitation, April 15, 2010. ↩︎
- CMS. (2010). Medicare and Medicaid Programs: Changes to the Hospital and Critical Access Hospital Conditions of Participation to Ensure Visitation Rights for all Patients. ↩︎
- CMS. (2013). Access and Visitation Rights in Long Term Care (LTC) Facilities. ↩︎
- CMS. (2011). State Medicaid Director Letter #11-006: Same Sex Partners and Medicaid Liens, Transfers of Assets, and Estate Recovery. ↩︎
- Department of Health and Human Services, Departmental Appeals Board, Appellate Division. NCD 140.3, Transsexual Surgery, Docket No. A-13-87, Decision No. 2576, May 30, 2014. ↩︎
- Office of Personnel Management, FEHBP Program Carrier Letter No. 2015-12, June 23, 2015. ↩︎
- National Institutes of Health. (January 4, 2013). Statement by NIH Director Francis S. Collins, M.D., Ph.D., on opportunities for advancing LGBT health research. ↩︎
- The White House. Presidential Executive Order Promoting Healthcare Choice and Competition Across the United States. October 12, 2017. https://www.whitehouse.gov/presidential-actions/presidential-executive-order-promoting-healthcare-choice-competition-across-united-states/; HHS 83 FR 7437. “Short-Term, Limited-Duration Insurance.” February 21, 2018 https://www.gpo.gov/fdsys/pkg/FR-2018-02-21/pdf/2018-03208.pdf ↩︎
- HHS. 83 FR 2802. “Statement of Organization, Functions, and Delegations of Authority,” January 19, 2018. Available at https://www.gpo.gov/fdsys/pkg/FR-2018-01-19/pdf/2018-00820.pdf; HHS. 83 FR 3880. “Protecting Statutory Conscience Rights in Health Care; Delegations of Authority.” January 26, 2018. Available at https://www.gpo.gov/fdsys/pkg/FR-2018-01-26/pdf/2018-01226.pdf.; Lambda Legal. January 2018. Trump Administration Plan to Expand Religious Refusal Rights of Health Professionals: Legal Issues and Concerns. Available at: https://www.lambdalegal.org/sites/default/files/2018-01- 18_lambda_legal_analysis_re_hhs_ocr_special_religious_refusal_unit_jcp_issued.pdf ↩︎