Civil Society Inclusion in a New Financial Intermediary Fund: Lessons from Current Multilateral Initiatives
Key Findings
Key Findings
Global leaders appear poised to approve the creation of a new financing mechanism for pandemic preparedness and response (PPR) activities. Support for such a mechanism grew as the profound fault lines exposed by the COVID-19 pandemic became clearer. The U.S. government has strongly supported the idea of creating a financial intermediary fund (FIF) for PPR at the World Bank, a proposal now endorsed by the G20, the WHO, and others, with the World Bank expected to vote on such a proposal this month. Despite this momentum, however, many questions remain about a new FIF including its governance and operations and the extent to which civil society will be formally included. A white paper on the FIF, recently released by the World Bank, contains a brief mention of civil society as potential observers to a FIF governing board, though some have critiqued that as insufficient. To help inform ongoing discussions, we sought to examine and draw lessons from existing institutions on how they engage with civil society formally, as part of their governance, as well as through other avenues. We analyzed 14 major multilateral global health and related institutions to assess how civil society, including from the global South, has been engaged in their governance, implementation/programming, and monitoring. We examined the following metrics of civil society inclusion to assess more formal engagement: board representation; voting rights; global South representation required; formal representation on committees; support for participation in governance; and requirements to fund civil society as part of program implementation. For those institutions that included formal board representation, we also looked at the share of seats reserved for civil society. Our key findings are summarized as follows:
- Civil society inclusion and engagement in the governance and operations of multilateral global health institutions has grown over time, especially since the Millennium Development Goals era, and as part of the global HIV movement in particular.
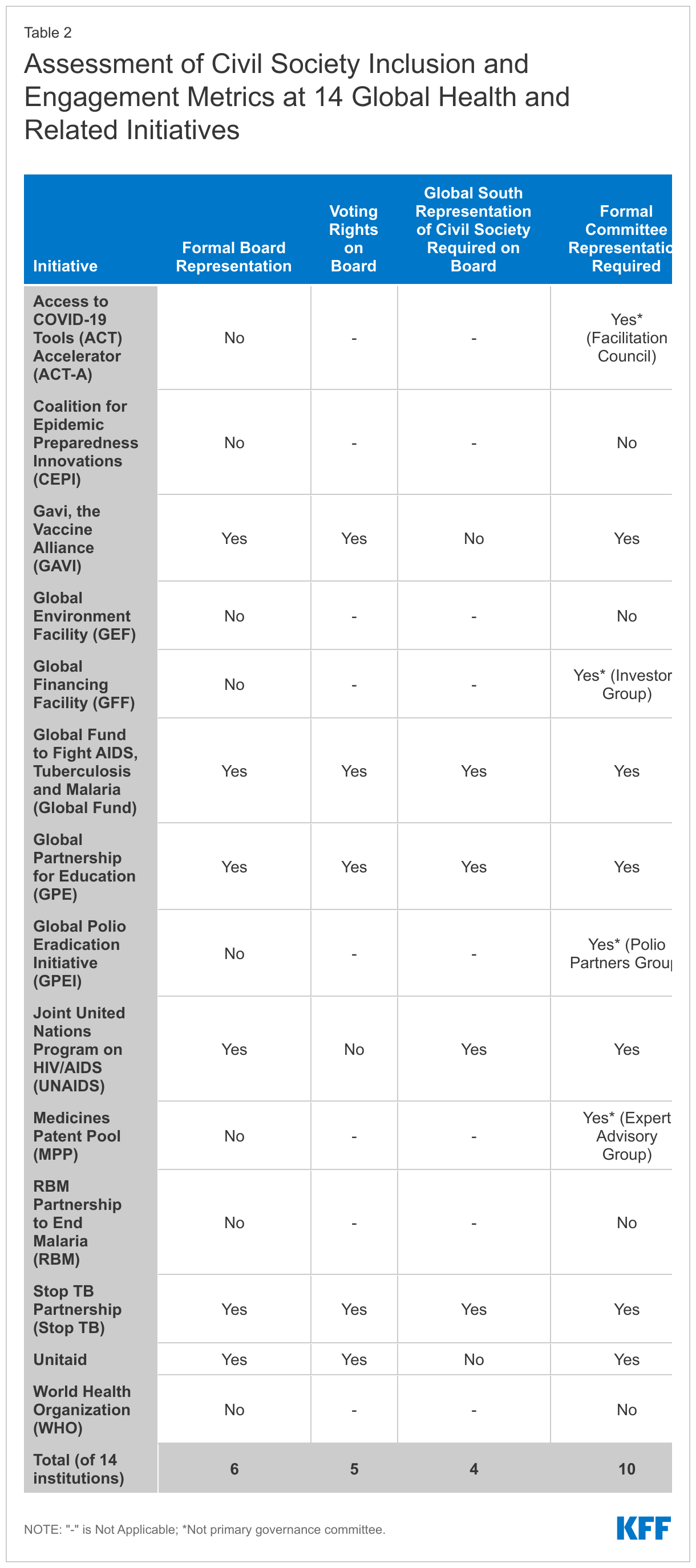
- The degree and nature of civil society engagement varies considerably. Three of the 14 institutions met all six metrics of formal civil society inclusion assessed (the Global Fund to Fight AIDS, Tuberculosis and Malaria; the Global Partnership for Education; and the Stop TB Alliance) and three met five metrics (GAVI, UNAIDS, and Unitaid). On the other end of the spectrum, three institutions met none (the Coalition for Epidemic Preparedness Innovations; the RBM Partnership to End Malaria; and the World Health Organization).
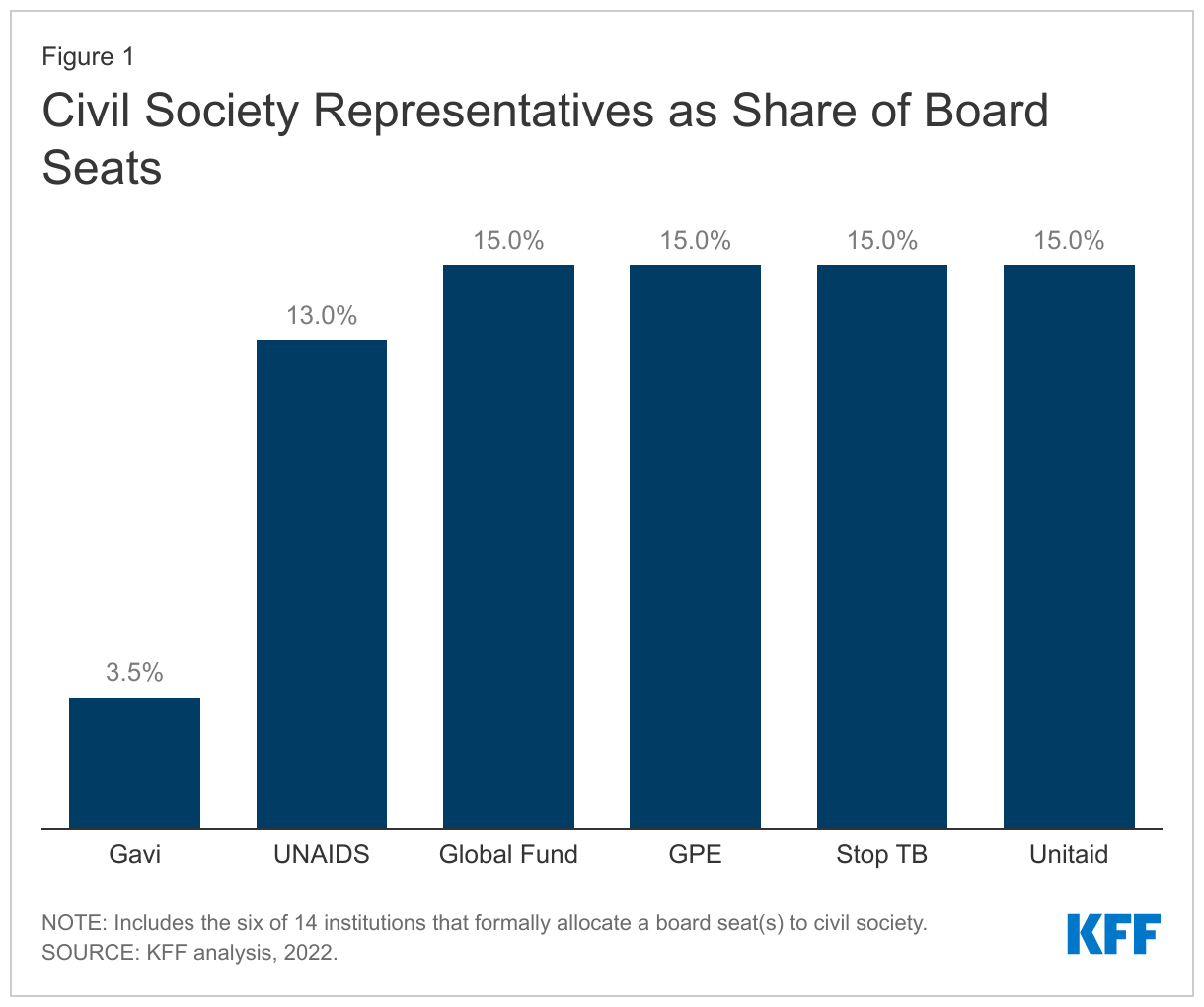
- On board representation specifically, six of the 14 institutions have formal seats for civil society, the strongest measure of inclusion, ranging from 3.5% to 15% of board seats. Five of the six provide voting rights, and four of the six specify that at least some portion of civil society representation be from the global South. In addition, the six with formal board seats also require civil society representation on their primary governance committee(s).
- All 14 multilateral global health initiatives, including those with no formal civil society representation on their governing board or committees, provide other opportunities for civil society engagement. Specific approaches and processes employed can bolster or limit civil society’s influence in governing decisions. For example, civil society representatives who are able to participate in advisory or working groups, or regional subgroups, can feed into and shape institutional governance. Other avenues, such as those that are more ad hoc, are seen as providing fewer opportunities for engagement or influence.
- At the same time, and even among those initiatives with formal representation on governing boards, civil society representatives confront a number of challenges, including a lack of financial and administrative support while managing a substantial burden of work, a steep learning curve for new representatives, and difficulties representing broad constituencies fairly and effectively.
- To address some of these challenges, some initiatives, but not all, have created mechanisms to directly support civil society engagement in governance, implementation and/or monitoring activities. Many of these have been instituted and expanded only in recent years.
Taken together, these findings offer new insights into how civil society has been included in major multilateral global health and related organizations that are in operation today, including the trend towards greater and more formal inclusion over time, and may inform ongoing global discussions about the creation of a new financing mechanism for PPR.
Introduction
Global leaders appear poised to approve the creation of a new financing mechanism for pandemic preparedness and response (PPR) activities. Support for such a mechanism, intended to coordinate and direct additional resources for PPR, particularly in low- and middle-income countries (LMICs), grew as the profound fault lines exposed by the COVID-19 pandemic became clearer. For its part, the Biden Administration has strongly supported the idea of creating a financial intermediary fund (FIF) for PPR at the World Bank and has already pledged $450 million and requested an additional $4.75 billion more from Congress. Support from other donors was pledged at the second Global COVID-19 summit, convened by the U.S. and several other governments, and the idea has been endorsed by the G20 and the World Health Organization. Most recently, the World Bank released a white paper outlining how a FIF might function and a proposal to establish the mechanism will be submitted for approval to the Executive Directors of the World Bank this month, after which the fund could begin to operate by the end of 2022.
Despite this momentum, however, many questions remain about a new FIF, including its governance and operations and how representative and inclusive it will be. Some global health stakeholders have raised questions as to whether and how civil society might be formally engaged in the governance of the FIF, as well as its design, implementation, and monitoring. The primary global health structure set up to respond to COVID-19 – the Access to COVID-19 Tools Accelerator, which includes COVAX, it’s vaccine arm designed to accelerate the development and manufacturing of COVID-19 vaccines and provide equitable access – has been critiqued for its lack of formal and meaningful civil society and community engagement, especially of representatives from the global South. In May of this year, the Independent Panel on Pandemic Preparedness and Response found that consultations to date with non-state actors on policy-making processes for pandemic preparedness have been “rushed, pro forma, and frankly, abysmal.”
In its white paper on the FIF, the World Bank states that it seeks to balance “inclusivity with simplicity and efficiency, to support streamlined and efficient decision-making and implementation”. The white paper contains a brief mention of civil society, as potential observers to the FIF governing board but not as formal members, as follows: “the observer pool could be broadened out, as needed, to include other multilateral institutions, civil society organizations (CSOs) and/or the private sector” and that “CSO observers could be included through a constituency-based approach”. The Bank solicited input on its white paper, and several critiques, including calls for ensuring substantive and formal civil society engagement in the governance and design of a FIF, have been submitted.1 The U.S. government, in its submitted comments, has been less clear on this point, saying that the FIF “should balance inclusivity and agility” and that non-governmental stakeholders could be included either as Board members or observers.
To help inform discussions regarding the creation and design of a global pandemic preparedness fund, we analyzed major multilateral global health and related institutions to assess how civil society, including global South organizations, has been engaged in their governance, implementation/programming, and monitoring. We examined 14 such institutions ranging from those that are affiliated with the United Nations, FIFs based at the World Bank, and/or independent organizations. For purposes of our analysis, we defined civil society to include representatives from non-profit or otherwise non-commercial actors who are not directly affiliated with a government and who are not acting in a solely individual capacity. Our analysis is based on a literature review, a review of official governance and other institutional documents, and interviews with a range of stakeholders (see methodology for more detail).
Methodology
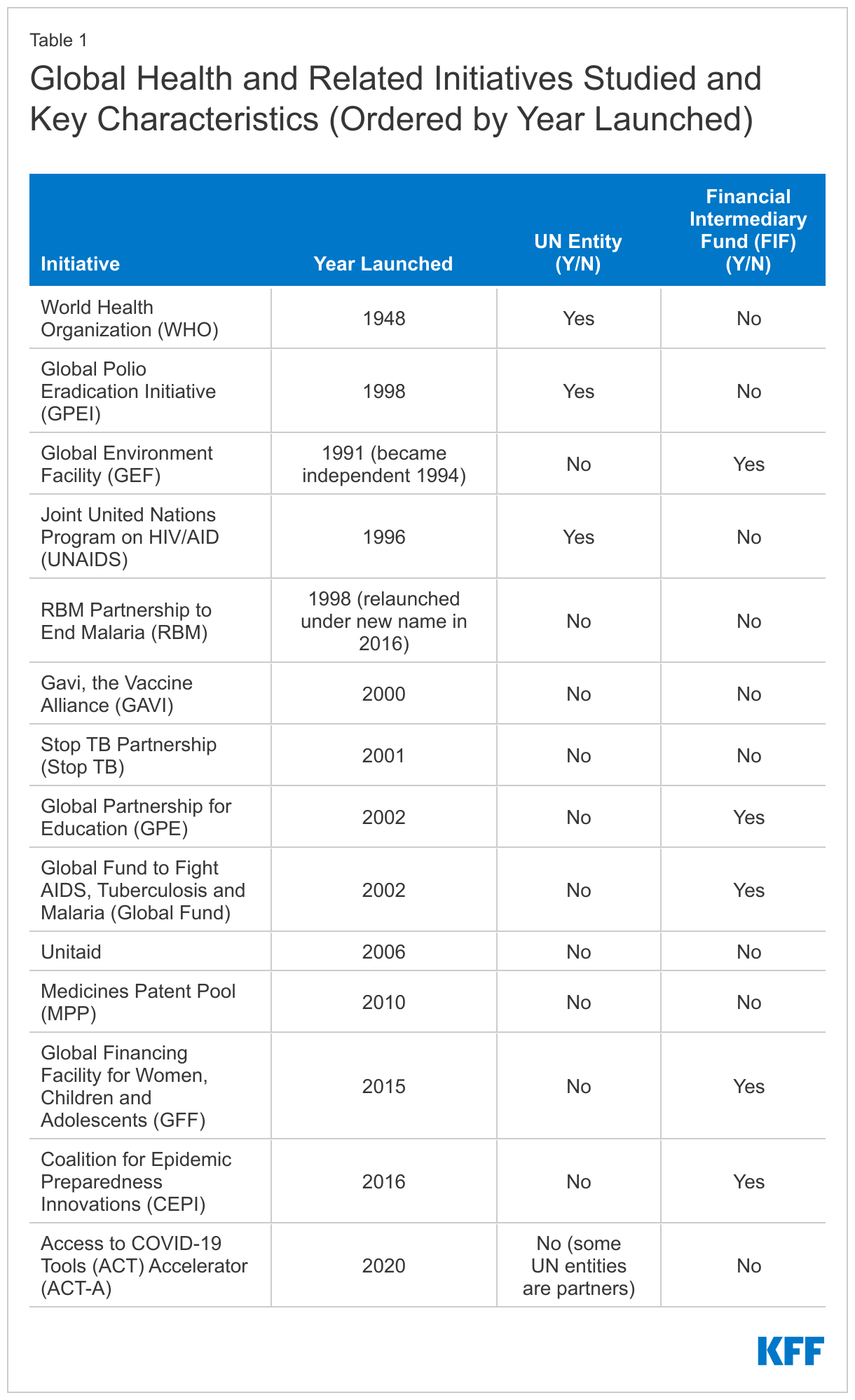
We performed a broad literature review on civil society and global health governance and identified 14 prominent, ongoing multilateral global health and related initiatives for inclusion in this analysis (see Table 1). Overall, five of the 14 models examined are FIFs housed in some manner at the World Bank. The others are multilateral efforts that are either independent (6) or part of the United Nations (3), although some of the independent entities are formally hosted by Unite Nations agencies. While we focused on multilateral initiatives, it is important to note that some bilateral donor governments have also made efforts to engage civil society in development planning and programming, including for global health. PEPFAR, the U.S. global HIV/AIDS program and largest initiative focused on a single disease, stands out in particular in this area, given both its size and because it has moved to enhance the engagement of civil society in its bilateral program implementation over time. As such, it also may offer some lessons and models for future PPR efforts (see Box 2).
For each of the global health initiatives included in this analysis, official governance documents (e.g. by-laws, terms of reference of governing bodies, website information regarding governing and advisory bodies) were studied to ascertain if, how, and to what extent civil society is officially included in the organization’s governance, implementation, and monitoring. This document review was supplemented by interviews with 22 individuals who are either involved in or have working knowledge of the governance processes of these organizations. The interviews provided additional details on the dynamics of the governing bodies, other avenues for civil society input into decision-making, particular challenges and opportunities experienced by civil society with respect to engagement in governance, and ways that civil society may be engaged (beyond governance). Both during the document review and key informant interviews, the analysis paid particular attention to the engagement of civil society representatives from the global South, which includes the bulk of countries that are the recipients of outside assistance. We examined the following metrics of civil society inclusion to assess more formal engagement: board representation; voting rights; global South representation required; formal representation on committees; support for participation in governance; and requirement to fund civil society as part of program implementation. For those institutions that included formal board representation, we also looked at the share of seats reserved for civil society.
For the purposes of this analysis, civil society was defined to include representatives from non-profit or otherwise non-commercial actors who are not directly affiliated with a government and who are not acting in a solely individual capacity. Multilateral institutions or public-private partnerships affiliated with multilateral bodies were not considered as civil society. Likewise, major private funders of organizations (such as private foundations) were not considered civil society for our purposes here. Organizations were deemed to have formally included civil society on their board only if governance documents specifically reserved seats for civil society representatives.
Issue Brief
Findings
- Civil society inclusion and engagement in the governance and operations of multilateral global health institutions has grown over time. A general trend in global health has been one of greater recognition over time of the importance of engaging with civil society actors.2 While older UN-based organizations such as WHO and GPEI feature little civil society role in their formal governance structures, even to this day, some of the institutions founded more recently, such as the Global Fund, Stop TB, Unitaid, and Gavi, engage civil society more prominently in their governance structures (see below). There are also a range of ways in which civil society actors engage in multilateral global health institutions, including both directly (through board participation, engagement in rule-making processes, and involvement in capacity-building for implementation) and indirectly (by helping set the global health agenda, generating knowledge and strategic information, and monitoring implementation of global health policies).3 The literature has found that civil society actors can play an important role in helping to ensure that global health policies and programs are informed by the lived experiences of the people most affected by health challenges, a view underscored by stakeholders interviewed. Official documents of many, but not all, of the initiatives included in this analysis reference a range of benefits derived from engagement with civil society (see Box 1).-The literature also supports the idea that civil society engagement improves global health processes and outcomes. Studies have found, for example, that civil society engagement has driven adoption of breakthrough innovations in health service delivery, including home management of malaria and community delivery of HIV treatment. Direct engagement of civil society in the governance of a global health organization may also help create a constituency that is invested in the organization’s success and will advocate on its behalf. For example, civil society engagement helps legitimize policies, mobilize resources for global health interventions and enhance the accountability of global health efforts (through its so-called “watchdog” role).4 In recent years, as the value of community-led health monitoring has become increasingly recognized, there has been a growing push to institutionalize and integrate civil society’s generation of strategic information within health monitoring and evaluation systems, such as, for example, with the Global Fund’s embrace of community-led monitoring for HIV.
Box 1: Multilateral Global Health Institutions: Reasons and Rationales for Engaging with Civil Society Organizations
Many of the initiatives examined here reference civil society engagement contributing to organizational success. For example, a number of initiatives (e.g. ACT-A, Gavi, Stop TB Partnership) highlight the role of civil society as advocates for policies, programs and funding to increase health service access. The Stop TB Partnership notes the value of civil society in monitoring health service access and outcomes and holding governments to account. Some initiatives (e.g. Gavi, GPE) tout the role of civil society in delivering services or technical assistance, and the Global Fund highlights how civil society can “serve as implementers of Global Fund grants and are often best placed to work with populations marginalized and excluded from mainstream health services.” In convening the Civil Society Task Force on TB, WHO cited civil society as the “driver for change,” helping translate WHO policies into practice and enhancing collaboration between governments and communities to improve health outcomes. The GEF says the “primary role of civil society…is to contribute to the development, implementation, monitoring and evaluation of GEF programs and projects on the ground.” CEPI’s articles of association state that “the CEPI Board shall be aware of take account of the views of different CEPI stakeholders such as…civil society” in order to “best support development of new vaccines and equitable access for affected people.”
Other initiatives emphasize that civil society can bring key community perspectives to the organization’s attention and shape governance, as well as muster support for the initiatives themselves. Unitaid’s Constitution advises that “[s]trong dialogue with NGOs and civil society is essential to ensure that the initiative is viable and addresses the needs of patients and communities.” UNAIDS governing documents state that civil society board representatives are “essential, respective stakeholders in decision-making processes”, representing the “perspectives of civil society, including living with HIV to the UNAIDS board.” The GFF says civil society helps ensure health assistance to countries is “evidence-based, reflective of community needs, and aligned with other issue-focused policies and strategies” while also “maintaining women’s, children’s and adolescents’ health high on the agenda for global leaders.” The Global Fund says civil society has an important role in “larger fundraising efforts with donor governments", which is also highlighted by a number of other initiatives, including Gavi and Stop TB.
- Multilateral global health institutions that arose during the Millennium Development Goals5 era, and from the HIV movement in particular, are more likely to prioritize civil society engagement. Previous analysis has found that intergovernmental institutions rooted more firmly in the global architecture that arose following World War II (such as United Nations entities and the World Bank) tend to be less likely to engage civil society in their governance compared to initiatives that arose after 2000, during the Millennium Development Goals (MDG) era (such as the Global Fund and Gavi). This pattern was confirmed by our analysis, as the entities least likely to formalize civil society involvement governance are either UN agencies (e.g. WHO) or certain financial intermediary funds housed at the World Bank (e.g. GEF, GFF). However, this pattern is not universal. UNAIDS, for example, is a UN body with five NGO representatives on its governing Programme Coordinating Board, but is unusual among UN organizations in this regard and its inclusion of civil society is firmly rooted in its origins in the HIV movement. It is also one of the more recently established UN agencies.-In some analyses of civil society engagement on global health governance, the response to HIV has been cited as a catalyst for greater attention to civil society engagement in the global health field. The Denver Principles, for example, articulated by people living with HIV in the earliest years of the HIV pandemic, as well as the endorsement in 1994 by 42 countries of commitments for the Greater Involvement of People Living with HIV/AIDS (GIPA), highlighted the right of people living with HIV to participate in decision-making processes that affect their lives. Among the initiatives examined here, those with a focus on HIV and TB tend to have greater engagement of civil society in governance, including through formal board representation, than global health initiatives focused on other health issues.
- The degree and nature of civil society engagement varies considerably, with three of the 14 institutions meeting all six metrics of formal civil society inclusion assessed, and three meeting none. The Global Fund, GPE, and Stop TB met all six metrics while GAVI, UNAIDS, and Unitaid met five. On the other end of the spectrum, CEPI, RBM, and WHO met none of the criteria (although they included less formal avenues of engagement). See Table 2.
- On board representation specifically, six of 14 have formal seats for civil society, the strongest measure of inclusion. The six are GAVI, the Global Fund, GPE, Stop TB, UNAIDS, and Unitaid. Five of these institutions (all but UNAIDS), provide voting rights. The Global Fund, GPE, Stop TB, and Unitaid each reserve 15% of voting seats for civil society representatives while Gavi reserves 3.5%. Although civil society representatives on the UNAIDS board do not have a formal vote, 13% of all board seats (including non-voting seats) are reserved for civil society representatives, as specified in governance by-laws. See Figure and Table 2.-The eight organizations that do not include civil society formally in their primary governance bodies are: ACT-A (no stand-alone governance mechanism, though its Principals Group includes some entities that do formally include civil society on their governing boards such as Gavi, the Global Fund and Unitaid); CEPI (which reserves one seat on its board for a non-profit/NGO investor, but not a civil society representative), GFF (no civil society representatives on the principal Trust Fund Committee), the GEF, GPEI, MPP, RBM Partnership to End Malaria, and WHO. Some of these eight organizations (e.g. MPP, RBM Partnership) have civil society members serving in their individual capacity on their current governing boards, but do not expressly dedicate a seat for civil society, and all do involve civil society in other ways (see below).
Several multilateral global health initiatives have seen their civil society engagement evolve over time. For example, at the earliest stages of its organizational development, affected communities did not have voting rights on the board of the Global Fund, but community representatives were granted full voting rights in 2004. In 2022, the Stop TB Partnership is restructuring its governance to ensure that representatives from the global South (including both government and civil society) occupy a majority of board seats and that robust representation of civil society and affected communities is further institutionalized.
- A subset of multilateral global health initiatives that formally include civil society on their boards (4 of 6) specifically reserve seats for civil society from the global South. GPE, the Global Fund, and Stop TB allocate one board seat for developed country NGOs and another for developing country NGOs. The five NGO delegations on the UNAIDS Programme Coordinating Board include three civil society representatives from the global South and two from high-income countries or countries in transition.
- Whether civil society is formally included on board committees, as required by 6 of the 14 institutions examined, is also an important determinant of civil society’s influence. According to key informants, much of the substantive work conducted by the governing boards of multilateral global health initiatives occurs in board committees and working groups. The six institutions that have board seats for civil society also require civil society representation on formal governance committees. The executive committee of the Stop TB Partnership board expressly reserves one seat for TB-affected communities. The NGO delegation of the UNAIDS Programme Coordinating Board has a seat on the PCB Bureau, which plans the board’s biannual meetings and oversees the board’s intersessional decision-making processes. Gavi mandates civil society representation on its governing board’s committees for governance and market-sensitive decisions. The Global Fund’s operating procedures require that each constituency be represented on at least one standing committee and all standing committees include both implementer and donor group members. GPE and Unitaid also require civil society representation on their main governance committee or committees. In addition to formal representation on primary governance committees, four other organizations – Act-A, the GFF, GPEI, and MPP – include civil society representation on an adjacent entity, such as an advisory group (e.g., Act-A’s Facilitation Council or MPP’s Expert Advisory Group).-The timing of board processes may occasionally affect the ability of civil society to influence the agenda of global health initiatives. In the case of the GFF, which has no civil society representation on its formal decision-making body (the Trust Fund), the Investors Group, which includes civil society, meets prior to regular meetings of the Trust Fund, enabling decisions on GFF funding by the Trust Fund to take account the findings and recommendations of the Investors Group. One key informant with experience working with the GFF advised that in part because of this, civil society is able to have some influence in GFF decision-making, even without a seat on the decision-making Trust Fund committee.
- All 14 multilateral global health initiatives, including those with no formal civil society representation on their governing board or committees, afford other opportunities for engagement. Beyond formal board representation, other avenues for engagement include a presence on committees (other than the primary governance committee), such as technical advisory working groups or other sub-committees, as well as involvement in temporary and issue-specific meetings and discussions. As mentioned above, while the GFF’s governing Trust Fund Committee includes no civil society representation on its board, its Investors Group, which advises the Trust Fund Committee and supports the GFF’s work at country level, includes two seats for civil society (one from an eligible country and one from a donor country) as well as one representative of the youth constituency. The GEF’s governance documents note the ability of civil society to participate in its civil society forum, workshops and meetings of GEF’s Country Support Program, and relevant task forces and working groups. ACT-A includes two civil society representatives on its Facilitation Council, which advises its Principals Group, and civil society representatives also participate in working groups for each of ACT-A’s four pillars (diagnostics, therapeutics, vaccines and health systems and response). Civil society representatives participate in MPP’s Expert Advisory Group and Scientific Advisory Panel. Unitaid’s consultative processes for its market-shaping interventions frequently include civil society. WHO has entered into official agreement with more than 200 non-state actors, who have the ability (within limits) to attend and speak at World Health Assembly meetings, and civil society organizations are frequently invited to participate in WHO processes to develop normative guidance on specific issues and topics. While these other avenues for collaboration and engagement are present in most initiatives, key informants have indicated that more informal participation is rarely as impactful as fixed representation on a governing board. They noted that the ability of civil society to speak at Health Assembly meetings is sharply limited, with civil society speakers limited to brief remarks regarding agenda items that they had no role in formulating. Informants advised that decisions of the Health Assembly are frequently negotiated in advance between Member States, further diminishing the meaningfulness of civil society input into decision-making by the body charged with setting global health norms.
- Among the five World Bank FIFs included in this analysis, civil society engagement also varies. The Bank is a trustee for numerous FIFs – ranging across development areas including prevention and treatment for communicable disease, climate change and food security. FIFs aim to leverage public and private resources to support international initiatives, including provision of global public goods. From FY2008 through FY2019, the number of FIFs at the World Bank rose from 12 to 27. The five FIFs included in this analysis – CEPI, GEF, the Global Fund, GPE, and the GFF – vary broadly in their models and in the degree of the Bank’s involvement in governance and decision-making. CEPI and the Global Fund, for example, effectively operate as independent entities, with the World Bank only providing financial services and serving on their governing boards as a non-voting member. By contrast, the Bank has a much more central role in the governance of some other FIFs. For example, the Bank chairs the Trust Fund Committee of the GFF. For the GPE, the Bank occupies a seat on the governing board that is reserved for multilateral and regional development banks. At the GEF, the World Bank helps mobilize resources, administers the trust fund, disburses funds, prepares financial statements, and monitors application of GEF funds.-Just as the FIFs have diverse operating models, FIFs also have broadly divergent modes of engaging with civil society. As mentioned above, 15% of GPE and Global Fund board seats are occupied by civil society, while CEPI, the GEF, and the GFF have none. Governance of the GEF, for example, is wholly intergovernmental, with ministerial officials representing a series of regional constituencies. Also, as noted earlier, all five FIFs do involve civil society in other ways, even the three that do not include civil society on their boards.
- Governance rules and practices, including whether board members represent constituencies or serve in their individual capacity, can affect civil society’s influence in multilateral global health initiatives. Civil society’s ability to influence multilateral global health institutions depends in part on having a critical mass of representation on the governing bodies that chart strategic directions and make decisions on behalf of these institutions. As noted, a number of multilateral global health initiatives have no civil society representatives on their governing boards, while others allow but do not mandate civil society inclusion. Governing rules or practices may affect the weight that civil society board representation has within a governing body. For example, the five NGO representatives on the UNAIDS governing board do not have voting power, although the Terms of Reference for the Programme Coordinating Board’s NGO delegation provides that “[t]hough technically NGOs do not have ‘the right to take part in the formal decision-making process’ of the PCB, in practice NGOs fully participate and are essential, respected stakeholders in the decision-making process.”-The capacity in which civil society representatives serve on governing boards varies among multilateral global health institutions. For most that have civil society on their governing body, board members represent constituencies. The Global Fund, Stop TB Partnership, and Unitaid reserve seats for representatives of communities affected by the diseases these organizations address, and the Global Fund reserves a board seat for NGO constituencies from developed and developing countries, respectively. UNAIDS reserves individual NGO seats for five regions (Africa, Asia/Pacific, Europe, Latin America and the Caribbean, and North America). In the case of the GPE, one civil society seat is set aside for the constituency of teachers. Where board seats are reserved for specific civil society constituencies, members are elected by their respective constituency and are expected to consult with their constituencies as part of their board responsibilities.-More rarely, civil society representatives serve on governing boards in their individual capacity. This is the case for the Medicines Patent Pool. UNAIDS governing rules also provide that NGO members serve in their individual capacity, although in practice, they operate as representatives of their respective regions and solicit considerable input from stakeholders in their respective regions.-The Global Fund’s unique model for formal decision-making serves to empower civil society to affect the organization’s funding decisions and strategic direction. Where a consensus cannot be reached on the board and a vote is called, Global Fund by-laws require that motions achieve a two-thirds majority in both the donor group (which includes eight donor countries plus one private sector seat and one private foundation seat) and the implementers group (which consists of seven developing county seats, two NGO seats, and the community representative). This effectively means the three civil society seats may, by persuading one of the developing country seats to vote with them, achieve a ”blocking minority” on any motion before the board. Informants cited this somewhat unusual arrangement as a key reason why civil society plays an especially influential role on the Global Fund board.
- At the same time, and even with formal involvement, civil society representatives on the governing bodies of multilateral global health initiatives confront a number of challenges. Key informants, many of whom are civil society representatives who are serving or have served on the governing boards of multilateral global health initiatives, cited an array of challenges that civil society board representatives face. Numerous informants pointed to the enormous time commitment required to serve on these boards, including review of voluminous board meeting materials and participation in board committees and working groups. Unlike the officials of national ministries and donor agencies, large philanthropic foundations, and multilateral agencies who serve on these boards, civil society representatives typically lack staff support to synthesize substantial bodies of data and analysis.-In addition, despite the substantial work burden associated with board membership in a multilateral global health body, civil society board members are often uncompensated for these efforts. Again, this distinguishes civil society representatives from most other board members, whose service on governing bodies is typically regarded as part of the job for which they are compensated. According to informants, uncompensated board work can be especially burdensome for civil society representatives from the global South, who often lack substantial institutional backing for such work. A group of civil society advocates who assessed the evolving global health architecture recommended that civil society and community engagement be specifically and adequately resourced, in order to enable civil society representatives to engage fully with governance processes and with their global constituencies.-According to key informants, civil society representatives who join the boards of multilateral global health initiatives often confront a sharp and daunting learning curve, and they sometimes receive limited training or ongoing support to help them navigate dynamic and often-complex governing processes. A common practice among global health initiatives with civil society membership on the board is to appoint two civil society representatives per seat – one serving as the formal board member, and one as alternate. This approach theoretically allows the alternate member to learn “on the job” before formally filling the board seat, although key informants said that the steady turnover in civil society board seats makes it difficult for civil society board blocs to cohere and become proficient in navigating board processes. Several key informants cited the civil society delegations to the Global Fund as examples of constituencies that have become sufficiently mature over time to wield considerable influence in institutional governance.-Where civil society members represent constituencies, the breadth and diversity of these constituencies can sometimes make it challenging for civil society board members to remain abreast of the full array of constituency issues and concerns. For example, the Global Fund board member representing affected communities is ostensibly representing people living on multiple continents and living with or affected by three diseases, each of which has a diversity of key affected populations.
- To address some of these challenges, several multilateral global health initiatives have created mechanisms to support civil society engagement in governance, implementation and/or monitoring. Multilateral global health initiatives have taken steps to support the engagement of civil society. While some of these initiatives focus specifically on enhancing the meaningfulness of civil society engagement in governance, most focus more broadly on facilitating greater civil society engagement in the respective work of these global initiatives. A recent review by the OECD, for example, found that development agencies are more likely to support civil society for project implementation than for joint planning, agenda-setting and decision-making.-UNAIDS funds a Communications and Consultation Facility to support NGO engagement in governance processes. This facility facilitates and coordinates communications within the NGO board delegation and between the NGO delegations and broader civil society. The Global Network of People Living with HIV (GNP+) currently oversees this mechanism for UNAIDS. A donor-funded effort supports a constituency bureau, based in Addis Ababa, to support the engagement of African board representatives on the governing boards of the Global Fund, and discussions are underway to leverage the bureau to support Africa civil society representatives on the boards of other global health initiatives.-For the Global Fund, formulation of national funding proposals for HIV, TB, malaria and health systems strengthening occurs within Country Coordinating Mechanisms (CCMs). The Global Fund mandates that CCMs set aside 15% of their administrative funding for non-governmental constituency engagement, with a particular focus on civil society and key and vulnerable populations.-Other support mechanisms created by global health initiatives focus primarily on engaging civil society in advocacy and program implementation, typically at country level. To improve civil society engagement in its work, GFF approved a civil society engagement framework for 2021-2025, with a specific focus on enhancing country-level engagement. GFF has committed $5 million over two years to implement the framework, which includes steps for communications, information sharing and engagement in strategic planning as well as creation of a civil society host to enable and support greater civil society engagement.-Gavi has earmarked 10% of funding from three Gavi funding windows to support civil society engagement in reaching communities currently missed by immunization programs. In April 2022, Gavi announced that Amref Health Africa would serve as the host of the Gavi CSO Constituency, responsible for mobilizing and supporting the efforts of more than 4000 civil society organizations to deliver immunization to underserved communities.
Box 2: The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) and Civil Society Engagement
PEPFAR is the U.S. government’s global HIV/AIDS program and largest commitment by any nation to address a single disease. While PEPFAR encompasses all of the U.S. government’s global HIV response, including financial support for and coordination with the Global Fund, the bulk of the program (approximately $5 billion per year) is for bilateral efforts – support provided directly to or on behalf of other countries.
Although the U.S. Department of State provides direct governance of PEPFAR, with oversight provided by Congress, the inclusion of civil society and community in PEPFAR country-level policy development and programming has been a hallmark of the program and one that has grown and become more formalized over time. Its importance was first identified in its 2003 authorizing legislation and first report to Congress. In its 2008 reauthorization, Congress specifically required PEPFAR to include civil society in the development of country “compacts”. In 2013, PEPFAR formally included civil society for the first time in the annual process for developing “Country Operational Plans” (COPs). COPs are prepared by multi-stakeholder country teams to document planned investments and results, and they serve as a basis for approval of final PEPFAR funding at the country level. Moreover, PEPFAR’s FY 2014 COP guidance specified that PEPFAR country teams must include a separate supplemental narrative documenting how civil society has been involved in COP development, comments made by civil society, and how these have been considered by country teams. Specifically, the guidance says that “As part of the COP process, PEPFAR teams are expected to expand their engagements with local civil society as a way to spur greater local civil society engagement by partner-country governments” and requires teams to include civil society at each major step of COP development. In addition, in 2018, PEPFAR set a goal that by the end of FY 2020, 70% of new funding going to partners must be local, including civil society and community organizations.
At the planning level, the Office of the Global AIDS Coordinator, which oversees PEPFAR, has begun providing draft COP guidance for input by civil society and other stakeholders and incorporating feedback into final guidance documents, which have reflected their recommendations and influenced country plans. At the country planning level, a recent analysis found that nearly 500 civil society recommendations were either fully or partially incorporated into PEPFAR annual country workplans during the COP 2020-2021 planning process. In addition, community involvement in COP development has been cited as an important factor in the implementation of innovations in HIV treatment programming in Malawi, Uganda, and Zimbabwe. Finally, civil society groups successfully advocated to have PEPFAR, and the Global Fund, adopt and support “community-led monitoring” (CLM), a process by which civil society groups are directly involved in data collection on HIV service quality and access primarily from actual beneficiaries of those services, and PEPFAR COP guidance now requires countries to establish CLM.
Sources: KFF, Key Issues and Questions for PEPFAR’s Future, September 2021, available at: https://www.kff.org/global-health-policy/issue-brief/key-issues-and-questions-for-pepfars-future/; State Department, PEPFAR 2022 Country and Regional Operational Plan (COP/ROP) Guidance for all PEPFAR-Supported Countries, January 2022, available at: https://www.state.gov/wp-content/uploads/2022/02/COP22-Guidance-Final_508-Compliant-3.pdf.
Since 2009, GPE has provided dedicated funding to civil society organizations through its Civil Society Education Fund. This mechanism aims to support civil society groups in influencing education policies, monitoring programs, and holding governments accountable for their commitments to ensure children’s access to quality education.
In addition to program implementation funding for civil society, some global health initiatives provide financing for civil society monitoring. For example, the Global Fund provides funding for community-based efforts to gather quantitative and qualitative data on the programs it funds and is working to stimulate inclusion of community-led monitoring in national funding proposals.
Implications
Our review highlights the spectrum of ways multilateral global health and related initiatives have incorporated civil society into their governance, operations, and other activities. The findings highlighted here may have relevance for the new global funding mechanism for pandemic preparedness and response – the FIF housed at the World Bank – that is being actively considered and whose governance structure is not yet decided. Several groups have already highlighted the importance of including civil society in pandemic preparedness, and the FIF specifically. For example, the Global Fund’s new strategic plan for 2023-2028 commits the organization to “champion community and civil society leadership in pandemic preparedness response, decision-making and oversight.” Advocacy and expert panel groups have provided feedback on the World Bank’s FIF white paper, as requested by the World Bank, calling for civil society to be “integral elements of the design” and expressing concern that the current approach “relegates civil society to an observer status…a far cry from the focused but inclusive multisectoral governance model.”
Our review identifies a clear trend in global health toward greater, more inclusive engagement of civil society in both governance and implementation, especially with respect to the meaningful involvement of civil society from the global South and affected constituencies. The ability of civil society to engage with and influence the programs and policies of multilateral global health initiatives appears most effective when the rules for inclusion of civil society constituencies are formalized and there exists a measure of institutional support to ensure the meaningfulness of civil society engagement. This is particularly the case when civil society has formal representation on governing boards as in the case of six of the 14 institutions analyzed here. While presence on governing bodies and committees is often important, it may not be sufficient in and of itself to create meaningful input and engagement with civil society. The details regarding how constituency-based representation is structured and how specific constituencies are identified and chosen, in addition to the availability of support mechanisms for civil society participation, often shape the meaningfulness of civil society involvement.
Many of our informants said civil society has important perspectives and insights that can strengthen efforts to address pandemic preparedness and response and other aspects of health system resilience. In particular, given the importance of building and maintaining trust in communities prior to and during pandemic response, civil society engagement may be a significant factor in the ultimate success of these efforts. Regarding a new FIF for PPR, many stakeholders have argued that inclusive governance should be emphasized for these reasons and to address existing power imbalances found in a more traditional donor-beneficiary framework.6 At the same time, as referenced in the World Bank’s white paper, some believe that a more inclusive governance structure could result in decision-making that is more complex and less efficient. It also requires existing decision-makers to relinquish some degree of power.
Taken together, these findings offer new insights into how civil society has been included in major multilateral health and related organizations that are in operation today and may inform ongoing global discussions about the creation of a new financing mechanism for PPR. As we find here, all 14 institutions examined include civil society in a range of ways, including several which mandate formal inclusion.
This work was supported in part by the Conrad N. Hilton Foundation. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Jen Kates and Josh Michaud are with KFF. Mike Isbell is an independent consultant.
Endnotes
- See, for example: Independent Panel for Pandemic Preparedness & Response, Comment on the World Bank’s White Paper on a Financial Intermediary Fund (FIF) for Pandemic Prevention Preparedness and Response, June 1, 2022, https://theindependentpanel.org/comment-on-the-world-banks-white-paper-on-a-financial-intermediary-fund-fif-for-pandemic-prevention-preparedness-and-response/; Friends of the Global Fight, Comments on World Bank White Paper on a proposed FIF for Pandemic Prevention, Preparedness and Response, June 2, 2022, https://www.theglobalfight.org/comments-on-world-bank-white-paper-on-a-proposed-fif-for-pandemic-prevention-preparedness-and-response/; WHO Council on the Economics of Health for All, A Proposed Financial Intermediary Fund (FIF) for Pandemic Prevention, Preparedness and Response Hosted by the World Bank – Elevating Ambitions Beyond Business as Usual, May 31, 2022, https://cdn.who.int/media/docs/default-source/council-on-the-economics-of-health-for-all/who-council-statement-31-may-2022.pdf?sfvrsn=97b00b6b_3&download=true; Pandemic Action Network, https://thedocs.worldbank.org/en/doc/b045141896aeb7483eabc2c7a8a33da0-0290032022/original/Pandemic-Action-Network-Review-and-Feedback.pdf; Global Preparedness Monitoring Board, https://thedocs.worldbank.org/en/doc/d441e976caa31d90cb06da27f2e03fc4-0290032022/original/WHO-Global-Preparedness-Board-Response.pdf; GFAN, May 31, 2022, https://thedocs.worldbank.org/en/doc/30d000fce96e1ca1cd18dc5c853436b6-0290032022/original/GFAN.pdf; Resolve to Save Lives, May 30, 2022, https://thedocs.worldbank.org/en/doc/cc924b3c66c0ab2b05a4c7e11bce8f37-0290032022/original/RESOLVE-TO-SAVE-LIVES.pdf. All comments are posted here: https://www.worldbank.org/en/projects-operations/products-and-services/brief/financial-intermediary-fund-for-pandemic-prevention-preparedness-and-response-engagement#comments. ↩︎
- See: Loewenson R, Annotated Bibliography on Civil Society Influence on Global Health Policy, Geneva: World Health Organization and Training and Research Center, 2003, https://www.researchgate.net/profile/Rene-Loewenson/publication/237459829_Annotated_Bibliography_on_Civil_Society_And_Health_Civil_society_influence_on_global_health_policy/links/5423df3f0cf26120b7a6f22e/Annotated-Bibliography-on-Civil-Society-And-Health-Civil-society-influence-on-global-health-policy.pdf; Lee K, “Civil Society Organizations and the Functions of Global Health Governance: What Role within Intergovernmental Organizations?” Glob Health Gov, 2010,3(2), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4888897/. ↩︎
- See: Gomez EJ, “Civil society in Global Health Policymaking: A Critical Review,” Globalization and Health 2018,14(1), https://globalizationandhealth.biomedcentral.com/articles/10.1186/s12992-018-0393-2; Smith SL, “Factoring Civil Society Actors into Health Policy Processes in Low- and Middle-income countries: A Review of Research Articles,” 1007-16, Health Policy Plan 2019, 34(1); Haas PM, Is There a Global Governance Deficit and What Should be Done About It? 2003, Berlin, Institute for International and European Environmental Policy. https://www.researchgate.net/publication/228423400_Is_there_a_global_governance_deficit_and_what_should_be_done_about_it. ↩︎
- See: Loewenson R, Annotated Bibliography on Civil Society Influence on Global Health Policy, Geneva: World Health Organization and Training and Research Center, 2003, https://www.researchgate.net/profile/Rene-Loewenson/publication/237459829_Annotated_Bibliography_on_Civil_Society_And_Health_Civil_society_influence_on_global_health_policy/links/5423df3f0cf26120b7a6f22e/Annotated-Bibliography-on-Civil-Society-And-Health-Civil-society-influence-on-global-health-policy.pdf; Lee K, “Civil Society Organizations and the Functions of Global Health Governance: What Role within Intergovernmental Organizations?” Glob Health Gov, 2010,3(2), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4888897/. ↩︎
- The MDGs were eight global goals, including health-related goals, that were agreed to in 2000 by all the world’s countries, with a target date of 2015. They have been succeeded by the Sustainable Development Goals. See: https://www.un.org/millenniumgoals/. ↩︎
- See: Mazzucato M, Donnelly A, “How to Design a Pandemic Preparedness and Response Fund,” Project Syndicate, April 20, 2022, https://www.project-syndicate.org/commentary/pandemic-financial-intermediary-fund-how-to-design-by-mariana-mazzucato-and-alan-donnelly-2022-04 (accessed June 15, 2022); Jarvis M, Glassman A, Kenny C, Governing New Pandemic Preparedness Financing – What’s Needed for Credibility, Legitimacy, and Effectiveness, Center for Global Development, September 21, 2021, https://www.cgdev.org/blog/governing-new-pandemic-preparedness-financing-whats-needed-credibility-legitimacy-and. ↩︎